Feb 23, 2026

Some people lose 5 percent of their body weight over three months and consider it a victory. Others lose 20 percent over a year and feel like they have only just started. The difference is not willpower. It is not genetics, though genetics play a role. The difference, increasingly, comes down to which medication class a person chooses, how that medication interacts with their specific biology, and whether the treatment timeline matches their actual goals. Phentermine and GLP-1 receptor agonists represent the two dominant pharmacological approaches to weight loss, and they could not be more different in how they work. One acts from the top down, stimulating the central nervous system to suppress hunger signals before they reach conscious awareness. The other works from the bottom up, mimicking a gut hormone that slows digestion, regulates blood sugar, and quietly rewires the appetite centers of the brain. Both produce real results. But the gap between those results, the side effect profiles, the costs, and the long-term sustainability of each approach has grown so wide that choosing the wrong one for your situation could mean years of frustration. If you have been comparing phentermine against specific GLP-1 medications or trying to figure out whether the newer injectable treatments are worth the price tag, this comparison will give you everything you need. Not opinions. Not marketing. Just the clinical data, the practical realities, and the honest trade-offs that nobody puts in the advertisements. Whether you are a clinician weighing options for patients or someone standing in a pharmacy wondering which prescription to fill, the next several thousand words will walk you through every angle of this decision, because getting it right matters more than most people realize.
What phentermine is and how it works
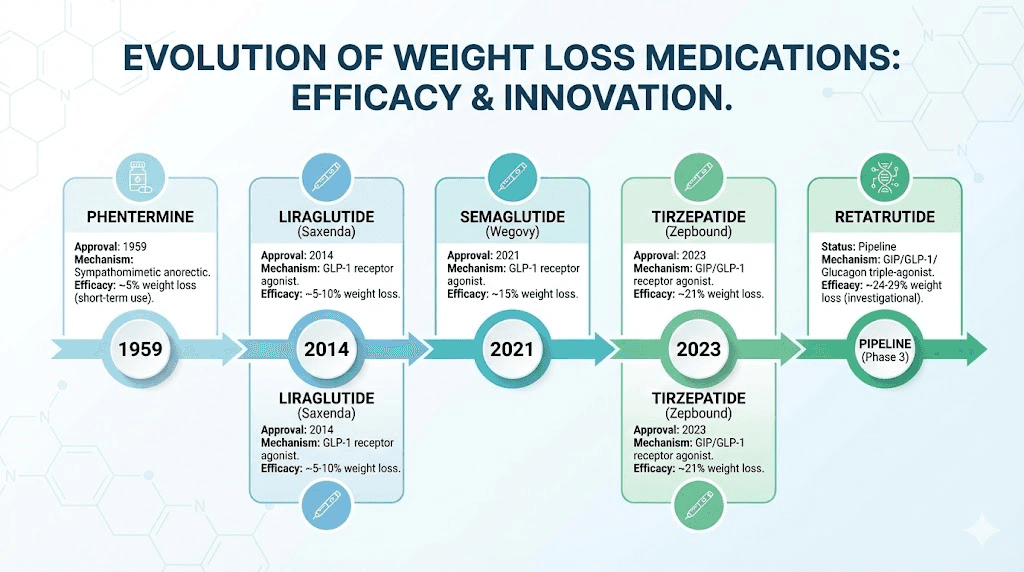
Phentermine is old. It has been around since 1959, making it one of the longest-standing FDA-approved weight loss medications in the United States. It belongs to a class of drugs called sympathomimetic amines, which means it mimics the effects of your sympathetic nervous system, the same system responsible for your fight-or-flight response. The FDA classifies phentermine as a Schedule IV controlled substance due to its stimulant properties and potential for dependence, though actual addiction rates remain low when the medication is used as prescribed.
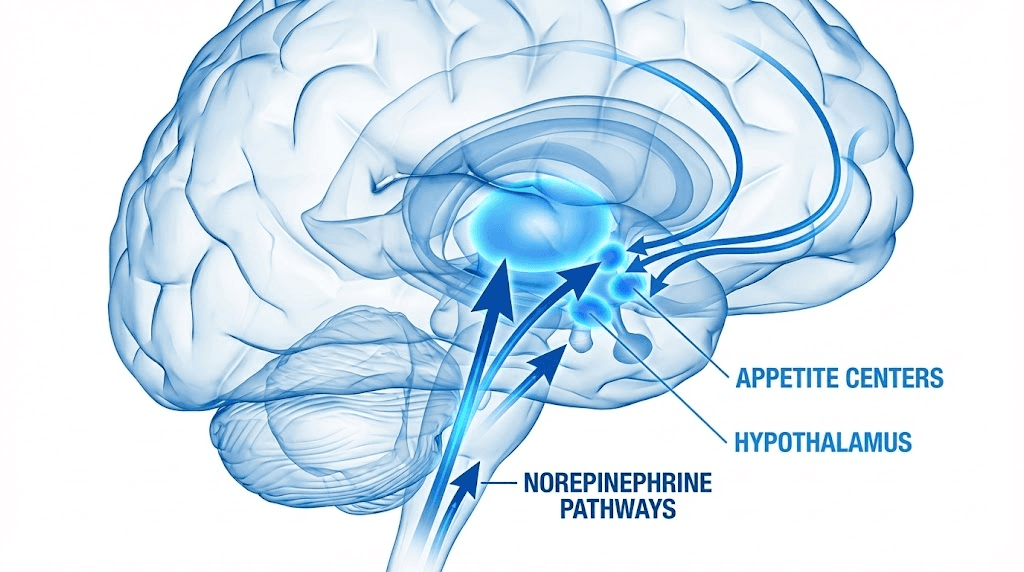
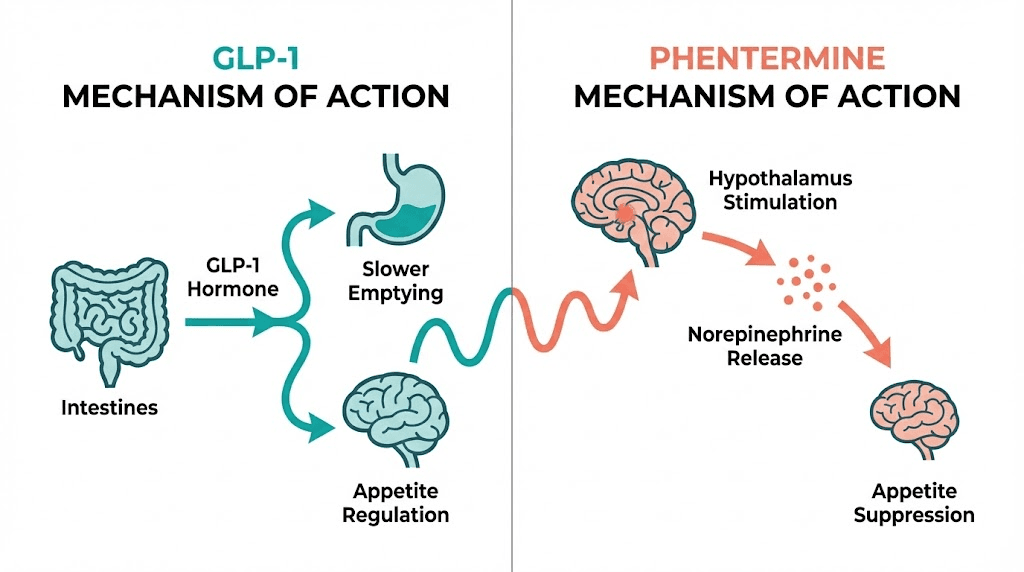
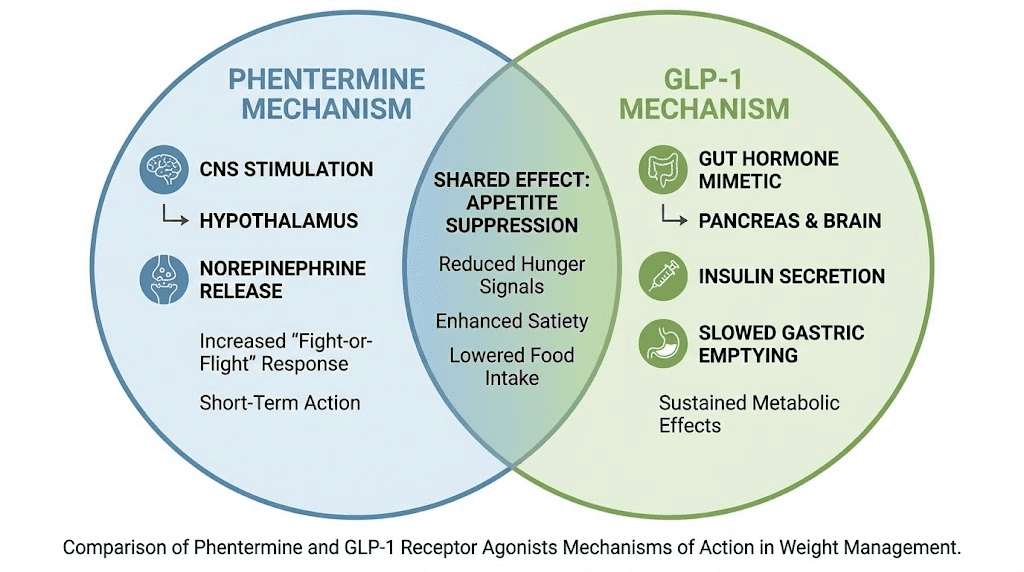
The mechanism is straightforward. Phentermine triggers the release of norepinephrine in the brain, and to a lesser extent dopamine and serotonin. Norepinephrine is your alertness neurotransmitter. When levels rise, appetite drops. You feel less hungry. You feel more energetic. Food loses some of its pull. This is a top-down approach to weight management because the drug acts directly on the central nervous system, essentially telling the brain to quiet down its hunger signals before they ever reach the conscious decision-making level.
The standard dosing protocol starts at 15mg daily and can increase to a maximum of 37.5mg once per day, usually taken in the morning to avoid insomnia. Most physicians prescribe it as a morning dose, sometimes as a split dose with a smaller tablet taken in the early afternoon. The drug reaches peak concentration in the blood within three to four hours and has a half-life of roughly 20 hours, which explains why a single morning dose can suppress appetite through most of the day.
Here is the critical limitation. Phentermine carries FDA approval only for short-term use, defined as up to 12 weeks. That is three months. The reasoning behind this restriction ties back to concerns about cardiovascular effects and the potential for tolerance, where the drug becomes less effective over time as the body adapts to elevated norepinephrine levels. Some clinicians prescribe phentermine for longer periods in an off-label capacity, cycling patients on and off the medication, but the official guidance remains firmly in the short-term camp.
In clinical trials, the results are modest but real. A 28-week study showed that the 15mg dose produced an average body weight loss of 7.38 percent compared to 2.28 percent with placebo. A separate 12-week trial at 30mg showed an average loss of 8.1 kilograms, with 95.8 percent of participants achieving at least 5 percent body weight loss. Translated into practical terms, most people can expect to lose three to five pounds per month on phentermine, with the most significant losses occurring in the first few weeks before tolerance begins to develop.
Phentermine is a blunt instrument. It works fast, it works cheaply, and then it stops working. That pattern defines the entire phentermine experience, and understanding it upfront prevents a lot of disappointment down the road. If you are exploring peptide-based approaches to fat loss, you will notice a fundamentally different philosophy at work, one built around sustained biological signaling rather than short bursts of stimulant-driven appetite suppression.
One detail worth understanding is that phentermine tolerance develops unevenly across patients. Some people maintain strong appetite suppression for the full 12 weeks. Others notice the effect weakening by week four or five. This variability is one reason clinicians sometimes cycle the medication, prescribing it for a few weeks, pausing, then restarting. The cycling approach lacks strong clinical evidence but persists in practice because some patients report that it helps maintain effectiveness over a longer period.
The patient experience on phentermine is also distinctly different from what people expect. Many first-time users describe a burst of energy and focus in the first week that they mistake for the appetite suppression itself. What actually happens is a broader sympathomimetic activation that makes everything feel slightly heightened. Colors seem brighter. Tasks feel more manageable. The appetite reduction is real, but it is layered on top of this general stimulant effect. By week three or four, the stimulant sensation fades while the appetite effect may persist at a reduced level. Managing these shifting expectations is part of using phentermine effectively.
What GLP-1 medications are and how they work
GLP-1 receptor agonists represent a completely different philosophy of weight management. Instead of forcing the brain to ignore hunger, they replicate a hormone your body already produces, glucagon-like peptide-1, and they do it at concentrations high enough to create dramatic shifts in appetite, digestion, and metabolic function.
Your gut produces natural GLP-1 every time you eat. The hormone signals the pancreas to release insulin, tells the stomach to slow down gastric emptying, and communicates with appetite centers in the brain to create a feeling of fullness. The problem is that natural GLP-1 breaks down within minutes. It is destroyed by an enzyme called DPP-4 almost as fast as the body makes it. GLP-1 medications solve this by using modified versions of the hormone that resist enzymatic breakdown, maintaining elevated levels for days or even a full week depending on the formulation.
The approach works from the bottom up. Rather than overriding hunger signals through stimulant activity, GLP-1 receptor agonists work with the body existing regulatory systems. They slow gastric emptying so food sits in the stomach longer, creating a physical sensation of fullness. They modulate blood sugar levels to prevent the spikes and crashes that trigger cravings. And they act on the hypothalamus and brainstem to reduce the reward value of food, a subtle but profound shift that many patients describe as simply not thinking about food the way they used to.
Several GLP-1 medications are now available, each with different profiles.
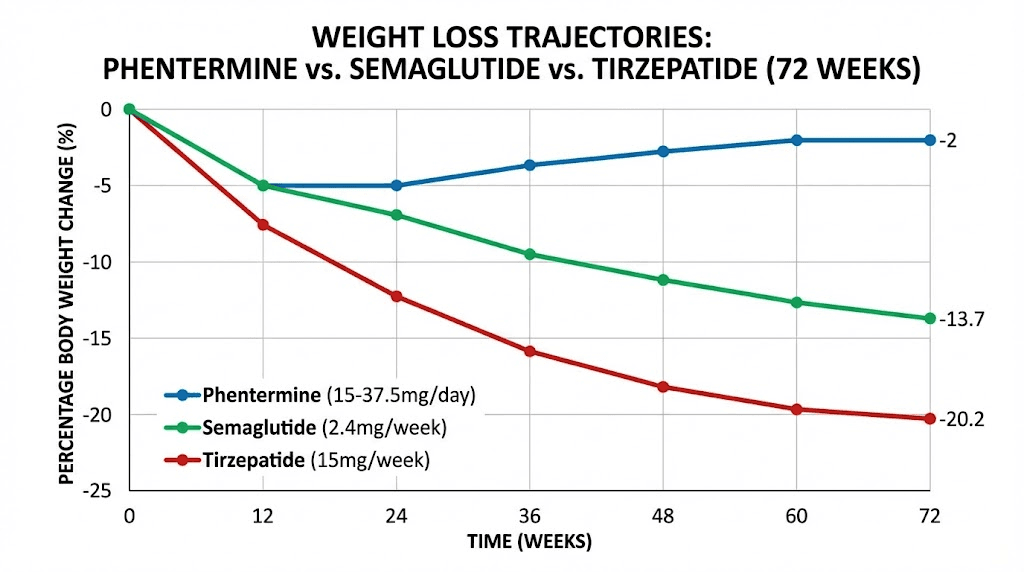
Semaglutide is the most widely recognized. Sold as Ozempic for type 2 diabetes and Wegovy for weight management, it is administered as a once-weekly injection. Clinical trials demonstrated 13.7 percent average body weight loss at 72 weeks, with many participants exceeding 15 percent. The dosing protocol involves a gradual titration over several months, starting low to minimize gastrointestinal side effects and increasing to the target maintenance dose. You can use the semaglutide dosage calculator to understand exact dosing schedules and conversions.
Tirzepatide takes the concept further. Rather than activating only GLP-1 receptors, it is a dual agonist that also targets GIP (glucose-dependent insulinotropic polypeptide) receptors. The result is even more pronounced weight loss. The SURMOUNT-1 trial showed average weight loss of 20.2 percent at 72 weeks on the highest dose, a figure that stunned the medical community when it was first published. If you are curious about the tirzepatide weight loss timeline, results typically begin appearing within the first month, with the most dramatic changes occurring between months three and nine. The dosing schedule follows a similar gradual titration to minimize side effects.
Liraglutide, sold as Saxenda for weight loss, requires daily injections rather than weekly ones. It produces more modest results than semaglutide or tirzepatide, typically around 8 percent body weight loss, but it was the first GLP-1 to receive FDA approval specifically for weight management and remains a viable option for patients who prefer a shorter-acting medication or who experience intolerable side effects on the more potent formulations.
On the horizon, retatrutide is an investigational triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. Phase 2 data showed weight loss exceeding 24 percent at 48 weeks, potentially making it the most powerful weight loss medication ever developed. When comparing retatrutide against semaglutide or looking at the broader landscape of emerging treatments, the trend is clear: each generation of GLP-1 based medications pushes the efficacy ceiling higher.
Unlike phentermine, every major GLP-1 medication carries FDA approval for long-term use. There is no 12-week cutoff. Patients can remain on these medications indefinitely, and the clinical data supporting long-term use extends to multiple years. This distinction alone fundamentally changes the treatment calculus, because chronic conditions typically require chronic treatment, and obesity is a chronic condition.
The learning curve with GLP-1 medications involves understanding injection technique, managing the initial adjustment period where gastrointestinal side effects peak, and following proper injection site rotation. Resources from SeekPeptides can help you navigate these practical aspects, from reconstitution guides to timing recommendations that help maximize effectiveness while minimizing discomfort.
Weight loss results compared head to head
Numbers do not lie. And in the comparison between phentermine and GLP-1 medications, the numbers tell a story that is difficult to argue with.
Phentermine at its best produces approximately 5 to 10 percent total body weight loss over a few months. The 15mg dose in a controlled 28-week trial yielded 7.38 percent loss. The higher 30mg dose over 12 weeks produced 8.1 kilograms of loss, with nearly 96 percent of participants hitting the clinically meaningful threshold of 5 percent body weight reduction. These are legitimate results for a medication that costs a fraction of what GLP-1 drugs cost.
But then look at the GLP-1 data.
Semaglutide at the 2.4mg weekly dose produced 13.7 percent body weight loss at 72 weeks in the STEP 1 trial. That is roughly double what phentermine achieves, sustained over a period more than three times as long. The early results on semaglutide are encouraging too, with most patients seeing measurable changes within the first four to eight weeks, though the full effect takes longer to manifest. If you are wondering how fast semaglutide works, the appetite suppression often begins within days, but meaningful scale changes typically appear by week four.
Tirzepatide pushes the ceiling even higher. The 15mg dose in the SURMOUNT-1 trial produced 20.2 percent average body weight loss at 72 weeks. More than a third of participants lost 25 percent or more of their starting weight. For a 250-pound person, that represents 50 or more pounds, results that were previously achievable only through bariatric surgery. Tirzepatide begins working on a similar timeline to semaglutide, with some patients reporting appetite changes almost immediately and significant weight changes becoming visible by weeks six through twelve.
Metric | Phentermine (15-37.5mg daily) | Semaglutide (2.4mg weekly) | Tirzepatide (15mg weekly) |
|---|---|---|---|
Average total body weight loss | 5-10% | 13.7% | 20.2% |
Trial duration | 12-28 weeks | 72 weeks | 72 weeks |
Participants achieving 5%+ loss | ~96% (30mg, 12 weeks) | ~87% | ~91% |
Participants achieving 10%+ loss | Limited data | ~70% | ~79% |
Participants achieving 20%+ loss | Rare | ~32% | ~57% |
Monthly rate of loss | 3-5 pounds | 4-8 pounds | 5-10 pounds |
FDA-approved duration | Up to 12 weeks | Long-term | Long-term |
The comparison becomes even more stark when you consider the trajectory of weight loss over time. Phentermine works best in the first few weeks, then efficacy tapers as tolerance develops. GLP-1 medications show the opposite pattern. Results start modestly and accelerate as the dose is titrated upward, with peak weight loss often occurring between months six and twelve. The GLP-1 onset timeline rewards patience, which is the opposite of what most people expect from a weight loss medication.
One important nuance. The clinical trials compare medications against placebo, not directly against each other in most cases. Head-to-head phentermine versus GLP-1 trials are limited. The data we have comes largely from comparing separate trial populations, which introduces variables like differences in baseline BMI, diet and exercise protocols, and participant demographics. Still, the magnitude of the difference, double to quadruple the weight loss percentage, is too large to dismiss as a statistical artifact. Looking at before and after results on semaglutide or tirzepatide before and after transformations makes the clinical percentages feel concrete and real.
For those who find themselves not losing weight in the early weeks on semaglutide, patience and dose optimization are usually the answer. Similarly, if tirzepatide seems to stop working, adjustments to dosing, diet, or exercise can often restart progress. The point is that GLP-1 medications offer more room for optimization because the treatment window is measured in years, not weeks.
Side effects and safety profiles
Every medication is a trade-off between benefit and harm. The side effect profiles of phentermine and GLP-1 medications are fundamentally different because the drugs operate through entirely different mechanisms, and understanding these differences is essential for making an informed choice.
Phentermine side effects
Phentermine is a stimulant. Its side effects reflect that reality. Increased heart rate is the most common cardiovascular effect, followed by elevated blood pressure. For someone with well-controlled blood pressure, a modest increase may be clinically insignificant. For someone with existing hypertension or cardiovascular disease, it could be dangerous.
The stimulant profile extends beyond the heart. Insomnia affects a significant percentage of users, which is why morning dosing is standard. Dry mouth is nearly universal at therapeutic doses. Restlessness and anxiety can emerge, particularly in the first week as the body adjusts to heightened norepinephrine activity. Some patients experience headaches, constipation, and an unpleasant taste in the mouth.
The more serious concern with phentermine is the cardiovascular risk associated with prolonged use. Historical precedent matters here. Phentermine was half of the infamous fen-phen combination (fenfluramine-phentermine) that was pulled from the market in the 1990s after causing heart valve damage and pulmonary hypertension. The fenfluramine component was identified as the primary culprit, but the association left a lasting shadow over phentermine as well. Rare cases of pulmonary hypertension have been reported with phentermine alone, though the absolute risk appears low. Phentermine is contraindicated in patients with cardiovascular disease, hyperthyroidism, glaucoma, and a history of drug abuse.
GLP-1 side effects
GLP-1 side effects cluster in the gastrointestinal system. This makes sense because the drugs work by modulating gut function. Nausea is the most frequently reported side effect, affecting 40 to 50 percent of patients at some point during treatment, typically during dose escalation. It usually subsides within days to weeks as the body adjusts. Constipation and diarrhea are also common, though they tend to be mild to moderate and manageable with dietary modifications.
Some patients experience sulfur burping on semaglutide, which while not medically serious can be socially uncomfortable and distressing. Dizziness, headaches, and fatigue appear in the clinical data as well. Semaglutide-related fatigue is often related to reduced caloric intake rather than a direct drug effect, and adjusting protein intake or meal timing can help. For tirzepatide users, constipation management, diarrhea duration, and fatigue follow similar patterns.
Injection site reactions occur in a small percentage of patients, including redness, swelling, or itching at the injection site. These are usually mild and resolve within days. Proper injection site reaction management for tirzepatide and technique can minimize these issues. Less common but more concerning side effects include pancreatitis (rare but documented), gallbladder disease, and potential thyroid tumor risk based on animal studies, though human data has not confirmed the thyroid concern.
Hair thinning is another side effect that has gained attention. GLP-1 related hair loss appears to be connected to rapid weight loss itself rather than a direct drug effect, a phenomenon called telogen effluvium that can occur with any rapid weight change.
The cardiovascular divide
Here is where the safety profiles diverge most dramatically. Phentermine raises cardiovascular risk markers. GLP-1 medications lower them. The SELECT trial demonstrated that semaglutide reduced major adverse cardiovascular events (heart attack, stroke, cardiovascular death) by 20 percent in overweight and obese adults with established cardiovascular disease. This is not a neutral finding. It means the drug actively protects the heart beyond what weight loss alone would explain.
GLP-1 medications also reduce blood pressure, improve lipid profiles, decrease systemic inflammation, and show renal protective effects. Tirzepatide has demonstrated similar cardiovascular benefits in ongoing trials. This anti-inflammatory and cardioprotective profile has led some researchers to suggest that GLP-1 agonists are not just weight loss drugs, they are metabolic therapies with wide-ranging systemic benefits.
For anyone with cardiovascular risk factors, and the majority of people with obesity have at least one, this distinction between a medication that raises cardiovascular stress and one that reduces it is arguably more important than the weight loss difference itself.
The mental health dimension of side effects deserves attention too. Phentermine stimulant properties can exacerbate anxiety disorders, trigger panic attacks in susceptible individuals, and create a cycle of stimulant-dependent energy followed by afternoon crashes. Some patients describe feeling "wired but tired," a state where the body feels energized but the mind feels frayed. GLP-1 medications generally do not produce these psychological effects, though the rapid change in relationship with food can create its own psychological adjustment. Patients sometimes report a sense of loss when food no longer provides the same emotional comfort, an effect that is more existential than pharmacological but worth anticipating.
The side effect timelines also differ in important ways. Phentermine side effects tend to be most intense in the first week, then gradually diminish as the body adapts, though they may return if the dose is increased. GLP-1 side effects follow a different curve, worsening with each dose increase during the titration period, then gradually improving once the maintenance dose is reached and the body fully adjusts. Understanding these patterns helps patients push through the difficult early period of either medication without abandoning treatment prematurely. The tirzepatide adjustment timeline and the general GLP-1 onset period both illustrate that temporary discomfort often precedes significant benefit.
Cost and accessibility
Cost is where phentermine wins. It wins decisively, and for many people this single factor determines the entire decision.
Generic phentermine costs between $20 and $75 per month. Some pharmacies fill it for even less with discount cards. It is one of the most affordable prescription medications in existence. Insurance coverage is variable but often unnecessary because the out-of-pocket cost is so low. A three-month course, which covers the full FDA-approved treatment window, might cost less than a single month of a GLP-1 medication.
GLP-1 medications exist in a different financial universe. Brand-name semaglutide (Wegovy) carries a list price of approximately $1,300 to $1,500 per month. Tirzepatide (Zepbound) falls in a similar range. Without insurance coverage, a year of GLP-1 treatment can cost $15,000 to $18,000. That is a significant financial commitment by any measure.
Insurance coverage for GLP-1 medications has been expanding but remains inconsistent. Some plans cover them with prior authorization. Others exclude weight loss medications entirely. Medicare historically has not covered anti-obesity medications, though legislative efforts are underway to change this. The coverage landscape shifts frequently, and what is denied today may be approved tomorrow.
Compounded semaglutide has emerged as a lower-cost alternative, with prices ranging from $150 to $500 per month depending on the pharmacy and dosage. Resources like the peptide cost calculator can help you estimate actual monthly costs for various protocols. Similarly, affordable tirzepatide options including compounded formulations have expanded access for many patients. The compounding landscape involves its own complexities, from pharmacy-specific guides for semaglutide to tirzepatide compounding resources.
Newer delivery methods are also changing the cost conversation. Oral semaglutide drops, sublingual semaglutide, oral tirzepatide, tirzepatide drops, and even GLP-1 patches represent alternatives that may shift pricing dynamics as competition increases.
Cost factor | Phentermine | GLP-1 medications |
|---|---|---|
Monthly cost (no insurance) | $20-$75 | $900-$1,500 (brand), $150-$500 (compounded) |
Annual cost (no insurance) | $60-$225 (12 weeks) | $10,800-$18,000 (brand), $1,800-$6,000 (compounded) |
Insurance coverage | Widely covered | Variable, often requires prior authorization |
Generic availability | Yes, widely available | No (brand-name only for FDA-approved versions) |
Cost per pound lost | ~$5-$10/pound | ~$20-$50/pound (brand), ~$5-$15/pound (compounded) |
The financial analysis shifts when you factor in the long-term perspective. Phentermine is cheap for three months but produces modest, often temporary results. GLP-1 medications are expensive but produce substantially greater weight loss with documented health benefits beyond the scale. If a year of GLP-1 treatment prevents a cardiovascular event, a diabetes diagnosis, or a joint replacement surgery, the cost-benefit equation looks very different. But those are theoretical long-term savings, and the monthly bill arrives right now.
The economics of compounded preparations deserve closer examination. Compounded semaglutide and tirzepatide are manufactured by compounding pharmacies rather than the original drug manufacturers. Prices vary widely. Some pharmacies charge $150 per month. Others charge $500 for what they claim is the same medication at the same concentration. The variation reflects differences in pharmacy overhead, testing protocols, ingredient sourcing, and profit margins. Vendor-specific guides like the Direct Meds semaglutide review and the Olympia pharmacy semaglutide guide can help you navigate quality differences between compounding sources. The key is verifying that any compounded medication comes from a licensed 503B outsourcing facility or a 503A pharmacy with appropriate oversight.
FSA and HSA eligibility add another financial dimension. Some patients wonder whether weight loss medications qualify for these tax-advantaged health accounts. The answer varies by plan and by medication. Prescription medications generally qualify, but not all employers include weight loss drugs in their covered expenses. Checking with your plan administrator before assuming coverage can save frustration at the pharmacy counter.
Duration of treatment and long-term outcomes
This is where the philosophical divide between these two medication classes becomes most apparent.
Phentermine is designed to be temporary. Twelve weeks. That is the window. Some physicians extend treatment through off-label prescribing, alternating months on and months off, or using lower doses for longer periods. But the FDA has never approved phentermine for long-term continuous use, and the data supporting extended protocols is thin. The drug was conceived as a short-term jumpstart, a way to break inertia and establish new eating patterns while the medication provides a window of reduced appetite.
The problem with this philosophy is that obesity is not a short-term condition. It is chronic. The biological mechanisms that drive weight regain, including hormonal adaptations, metabolic rate reduction, and neurological changes in appetite regulation, persist indefinitely. A 12-week medication course addresses none of these underlying drivers in a permanent way. When the medication stops, the biological pressures that caused weight gain in the first place reassert themselves.
GLP-1 medications were designed with chronicity in mind. Clinical trials extend to 72 weeks and beyond. Extension studies have followed patients for multiple years with continued efficacy and safety. The treatment paradigm mirrors how we approach other chronic conditions: you take the medication as long as you need it, potentially for life. This framing is uncomfortable for many people who view medication as something you take temporarily until a problem resolves, but it aligns with the biological reality of obesity as a chronic disease with chronic neurohormonal underpinnings.
The long-term outcome data heavily favors GLP-1 medications. In addition to sustained weight loss, long-term use is associated with continued cardiovascular protection, maintained glycemic control, and progressive improvements in metabolic markers. Patients who remain on semaglutide or tirzepatide for years tend to maintain their weight loss, with some continuing to lose additional weight even after the first year.
For phentermine, long-term outcome data is sparse precisely because the drug was never intended for long-term use. What data exists suggests that weight is typically regained after discontinuation, often rapidly. The question is not whether phentermine works during the 12 weeks you take it. It does. The question is what happens during the 52 weeks after you stop.
Understanding how long people stay on semaglutide helps frame realistic expectations. Many patients remain on treatment for a year or longer. The full timeline for semaglutide to work extends well beyond the first few weeks, with continued weight loss often occurring through the first 12 to 18 months of treatment.
The psychological impact of treatment duration should not be overlooked. Phentermine creates urgency. You know you have 12 weeks, so every pound matters, every slip feels catastrophic, and the ticking clock adds stress to an already difficult process. GLP-1 treatment removes that pressure. With an open-ended timeline, a bad week is just a bad week. A plateau is something to wait out, not panic over. This shift in temporal framing often produces better adherence and less disordered eating behavior during treatment.
Medication storage and handling also differs between the two classes, and this affects long-term convenience. Phentermine is a pill you keep in a bottle at room temperature. Simple. GLP-1 medications often require refrigeration, careful handling, and awareness of storage requirements for tirzepatide and semaglutide fridge shelf life. Some formulations can be kept at room temperature for limited periods, but exceeding these limits compromises potency. For travelers, understanding what happens when semaglutide gets warm becomes a practical concern. These logistics are manageable but represent a real difference in daily treatment burden between an oral pill and an injectable biologic.
Weight regain after stopping
This section matters more than any other in this article. Weight regain is the defining challenge of obesity treatment, and the pattern after stopping medication tells you more about a drug utility than the weight loss it produces while you are taking it.
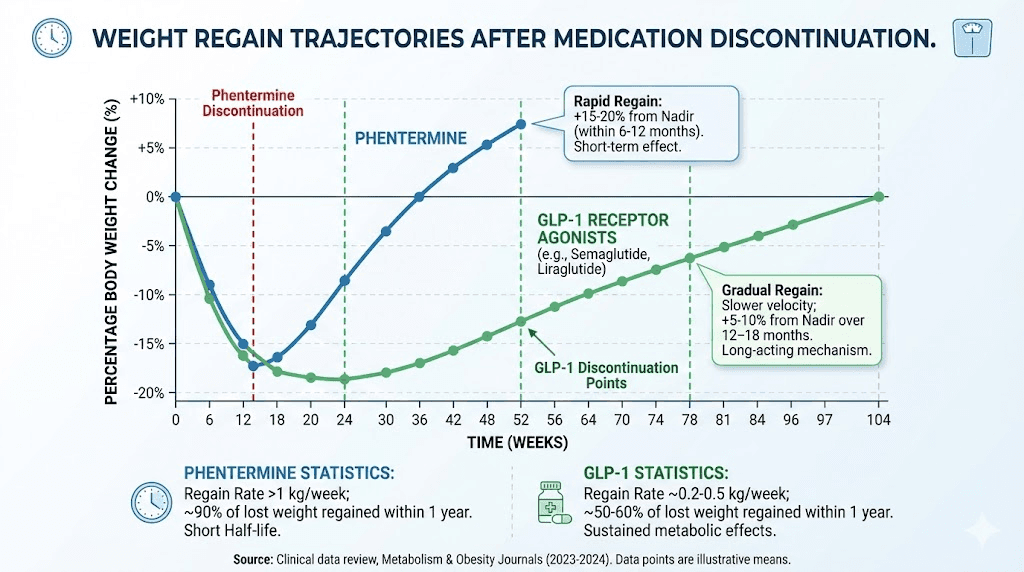
The data on GLP-1 withdrawal is sobering. After stopping semaglutide, patients regain an average of 5.63 kilograms. The rate of regain averages about 0.8 kilograms per month. By 18 months after discontinuation, most patients have returned to their baseline weight, erasing the majority of their progress. Semaglutide withdrawal symptoms extend beyond simple weight regain, with many patients reporting a return of intense food cravings and appetite increases that feel overwhelming after months of suppressed hunger.
Phentermine follows a similar pattern of regain, though the data is less precisely quantified because the shorter treatment duration and older study designs make direct comparisons difficult. The general finding is that weight regain after stopping phentermine is common and expected. Without the appetite-suppressing effect of elevated norepinephrine, hunger returns to pre-treatment levels, and weight creeps back up.
An interesting finding has emerged regarding the transition between medications. One study found that patients who switched from a GLP-1 medication to phentermine were 29 percent less likely to regain all of their lost weight compared to patients who stopped GLP-1 treatment entirely without any replacement medication. This suggests a potential role for phentermine as a maintenance or bridge therapy after GLP-1 discontinuation, though the evidence remains preliminary.
The weight regain problem is not a medication failure. It is a biological reality. Weight loss triggers a cascade of hormonal adaptations designed to restore the body to its previous weight. Ghrelin increases. Leptin decreases. Metabolic rate drops. These adaptations persist for years, possibly permanently, after weight loss. Medication can counteract these biological pressures while you are taking it. When you stop, the pressures return in full force. This is why the long-term treatment model of GLP-1 medications, for all its costs and inconveniences, may ultimately prove more effective than the short-term burst approach of phentermine.
The semaglutide plateau phenomenon also deserves mention here. Many patients experience a period where weight loss stalls before either resuming or stabilizing at a new weight. This is distinct from regain and is a normal part of the adaptation process. Similarly, patients on tirzepatide may encounter periods where weight loss seems to stall, and understanding the difference between a temporary plateau and true treatment failure helps prevent premature discontinuation.
Who should choose phentermine
Phentermine is not the wrong choice for everyone. For specific situations, it may actually be the better option.
Cost is the most obvious consideration. If you cannot afford GLP-1 medications and do not have insurance coverage, phentermine provides real appetite suppression at a fraction of the cost. Losing 5 to 10 percent of body weight, even temporarily, carries meaningful health benefits. It reduces blood pressure, improves blood sugar levels, decreases joint stress, and can provide the psychological momentum needed to establish healthier habits. For someone on a tight budget who needs immediate results, $20 to $75 per month is orders of magnitude more accessible than $900 to $1,500.
Short-term goals also favor phentermine. If you need to lose weight before a surgical procedure, for a specific medical reason on a defined timeline, or as a bridge to another treatment, phentermine short-term approval window aligns perfectly with a short-term need. You take it, you lose weight, you achieve the clinical goal, and the question of long-term maintenance becomes secondary.
Phentermine may suit individuals who respond poorly to GLP-1 side effects. Some people cannot tolerate the gastrointestinal effects of GLP-1 medications despite gradual titration and supportive measures. For these individuals, the stimulant-based side effect profile of phentermine, while different, may be more manageable. Insomnia is addressable with morning dosing. Dry mouth is uncomfortable but not debilitating. Mild increases in heart rate are tolerable in otherwise healthy individuals.
People who prefer oral medications over injections have historically leaned toward phentermine. Though this advantage is narrowing as oral GLP-1 formulations become available, including the GLP-1 six-in-one oral liquid and various tablet formulations like tirzepatide tablets, injection aversion remains a real barrier for many patients.
Phentermine accessibility extends beyond cost. It is available at virtually every pharmacy in the country, requires no special handling or refrigeration, and prescriptions can often be obtained through telemedicine platforms with minimal friction. GLP-1 medications, by contrast, may face supply shortages, require specialty pharmacy fulfillment, and involve navigating prior authorization processes that can delay treatment by weeks. When time is a factor, phentermine ability to go from prescription to first dose within 24 hours has real clinical value.
Finally, phentermine can serve as a test of medication-assisted weight loss. If you have never tried pharmacological weight management and want to see how your body responds to appetite suppression before committing to a more expensive long-term protocol, a short course of phentermine provides useful information. If you respond well to appetite suppression as a mechanism, that response is likely to be amplified with GLP-1 medications. If you find that appetite suppression alone does not change your eating behaviors, that is equally valuable information that can guide future treatment decisions.
Who should choose a GLP-1
The clinical evidence supports GLP-1 medications as the superior choice for most people seeking significant, sustained weight loss. That is a strong statement, but the data backs it up.
Anyone with a BMI of 30 or above, or 27 with at least one weight-related comorbidity, meets the standard prescribing criteria for GLP-1 therapy. The BMI thresholds for GLP-1 prescribing are well-established and provide a clinical framework for initiating treatment. But beyond the formal criteria, several specific situations make GLP-1 medications particularly compelling.
If you have type 2 diabetes or prediabetes, GLP-1 medications address both weight and glycemic control simultaneously. This dual action is not available with phentermine, which has no meaningful effect on blood sugar regulation. The insulin-sensitizing and glucose-lowering properties of GLP-1 agonists make them a first-line consideration for anyone in the diabetes spectrum.
Cardiovascular risk changes the calculation entirely. If you have a history of heart disease, stroke, or multiple cardiovascular risk factors, phentermine is not just suboptimal, it is contraindicated. GLP-1 medications, by contrast, actively reduce cardiovascular risk. Choosing between a medication that increases heart rate and blood pressure versus one that reduces MACE events by 20 percent is not a close call when cardiovascular health is a concern.
If you need to lose a substantial amount of weight, GLP-1 medications are simply more powerful tools. Phentermine efficacy ceiling of 5 to 10 percent body weight loss is insufficient for someone who needs to lose 30 percent or more. Tirzepatide, with its demonstrated ability to produce 20+ percent weight loss, reaches into territory that phentermine cannot approach. Tirzepatide before and after weight loss results demonstrate what these percentages look like in practice, and for people with significant weight to lose, the visual transformations are striking.
People who have tried phentermine and regained weight are also strong candidates for GLP-1 therapy. If the short-term approach has already failed you, repeating it is unlikely to produce a different outcome. GLP-1 medications offer a fundamentally different mechanism with a long-term treatment framework that addresses the chronicity phentermine cannot.
If long-term health optimization is your primary goal rather than short-term weight reduction, the metabolic benefits of GLP-1 medications extend well beyond the scale. Anti-inflammatory effects, renal protection, cardiovascular risk reduction, and improved metabolic markers create a comprehensive health improvement that phentermine does not provide. SeekPeptides provides resources to help you understand these broader metabolic effects and how different peptide-based approaches interact with your overall health profile.
Even the process of how quickly appetite suppression begins on semaglutide can help set expectations. While phentermine appetite suppression is immediate and intense, GLP-1 appetite modulation builds gradually, often feeling more natural and sustainable. Patients frequently describe it as a quiet reduction in food noise rather than a forced suppression of hunger.
For men specifically, the weight loss data on GLP-1 medications is particularly interesting. Men tend to lose weight faster than women on both medication classes, likely due to higher baseline metabolic rates and greater lean mass. Men who have used tirzepatide report dramatic body composition changes that often exceed the averages reported in mixed-gender clinical trials. The combination of significant fat loss with muscle preservation, particularly when exercise is maintained, produces visible changes that many men describe as transformative.
Nutritional support during GLP-1 treatment cannot be overstated. Because these medications reduce overall food intake, the quality of every calorie consumed becomes more important. GLP-1 companion supplements and nutritional support help fill the gaps that reduced eating creates. Protein intake deserves particular attention because insufficient protein during rapid weight loss accelerates muscle loss, which in turn slows metabolism and undermines long-term results. Many clinicians recommend 1.0 to 1.2 grams of protein per kilogram of goal body weight as a minimum during GLP-1 treatment.
Can you combine phentermine and GLP-1 medications
This question comes up constantly. If phentermine works through one mechanism and GLP-1 medications work through another, would combining them produce additive or even synergistic weight loss? The answer is more complicated than you might hope.
The theoretical case for combination is straightforward. Phentermine suppresses appetite through central norepinephrine release. GLP-1 agonists suppress appetite through peripheral gut hormone signaling and central satiety pathways. These mechanisms are largely non-overlapping, which suggests potential for additive benefit. Some clinicians have adopted this reasoning and prescribe both medications off-label, particularly phentermine combined with semaglutide or phentermine combined with tirzepatide.
The evidence, however, does not strongly support this approach. A small human study examining the addition of phentermine to liraglutide found no meaningful additional weight loss compared to liraglutide alone. The study was limited, involving only 45 participants, and used liraglutide rather than the more potent semaglutide or tirzepatide. But the null finding is notable because it suggests that GLP-1 appetite suppression may already be near the ceiling of what appetite reduction can achieve, leaving little room for phentermine to add benefit.
Animal studies paint a mixed picture. Combination treatment produced the largest absolute weight reduction in rodent models, but it also raised cardiovascular concerns. The stimulant effects of phentermine (increased heart rate, elevated blood pressure) combined with the cardiovascular changes produced by GLP-1 medications created a physiological profile that researchers flagged for further investigation. This does not mean combination therapy is dangerous in humans, but it does mean the safety profile has not been adequately characterized.
The practical reality is that many patients end up on combination therapy not by design but by circumstance. A patient starts phentermine, achieves some weight loss, then transitions to a GLP-1 medication for sustained management. During the overlap period, they are effectively on both medications. Other patients start on a GLP-1 medication and add phentermine during a plateau to attempt to restart weight loss. These real-world scenarios happen frequently in clinical practice, even though the evidence base supporting them is thin.
If you are considering combining these medications, the fundamental differences between phentermine and GLP-1 mechanisms are worth understanding deeply. They are not the same type of drug, they are not interchangeable, and combining them requires careful medical supervision with particular attention to cardiovascular monitoring. Blood pressure and heart rate should be checked frequently, and any signs of cardiovascular stress should prompt immediate reassessment.
The broader peptide landscape offers other potential combination strategies as well. Some researchers are exploring whether compounds like AOD-9604 combined with tirzepatide might offer complementary mechanisms without the cardiovascular concerns of stimulant addition. The peptide stack calculator on SeekPeptides can help you explore how different compounds interact, though any combination protocol should be developed with a qualified healthcare provider.
Individual GLP-1 medications compared to phentermine
Rather than treating GLP-1 medications as a monolithic category, it helps to examine how each individual GLP-1 drug stacks up against phentermine on its own terms. The differences within the GLP-1 class are significant enough to affect clinical decision-making.
Semaglutide versus phentermine
The phentermine versus semaglutide comparison is the most commonly discussed matchup because semaglutide is the most widely prescribed GLP-1 for weight loss. Semaglutide roughly doubles the weight loss percentage of phentermine (13.7% versus 5-10%) over a much longer treatment duration. The semaglutide versus tirzepatide comparison further contextualizes where semaglutide sits in the overall hierarchy.
Semaglutide comes in multiple formulations. The injectable form (Wegovy for weight loss, Ozempic for diabetes) is the most studied and most commonly prescribed. Understanding the semaglutide dosage chart helps you follow the titration schedule. Proper reconstitution technique for compounded formulations is essential for those using non-brand preparations, and tools like the unit-to-milligram conversion guides and the comprehensive units-to-mg calculator eliminate dosing confusion.
The side effect trade-off is clear. Phentermine causes stimulant-related effects (insomnia, elevated heart rate, anxiety). Semaglutide causes gastrointestinal effects (nausea, constipation, diarrhea). For most patients, the GI effects are more manageable than cardiovascular stress, but individual tolerance varies. Detailed side effect comparisons between semaglutide and tirzepatide can help you anticipate what to expect from each specific medication.
Dietary compatibility also differs. On phentermine, the reduced appetite is non-specific, you simply eat less. On semaglutide, specific food choices matter more. Understanding foods to avoid while taking semaglutide, building a proper semaglutide diet plan, and knowing the best foods to eat on semaglutide all contribute to better outcomes and fewer side effects. The question of alcohol on semaglutide comes up frequently as well, since many people find their alcohol tolerance changes dramatically.
Tirzepatide versus phentermine
Tirzepatide represents an even larger gap. At 20.2 percent average body weight loss versus phentermine 5-10 percent, tirzepatide produces roughly three to four times the weight loss. The dual GIP/GLP-1 mechanism appears to be more effective than GLP-1 alone, which is why researchers continue developing multi-receptor agonists. The tirzepatide dose chart and compounded tirzepatide dosage information provide practical dosing guidance.
Tirzepatide carries a similar gastrointestinal side effect profile to semaglutide, though some patients report milder nausea. Headaches, sleep disturbances, body aches, and anxiety are reported side effects that should be weighed against the significant weight loss benefits. Joint pain and muscle pain have also been reported, though these may be related to rapid body composition changes rather than direct drug effects.
The dietary component of tirzepatide treatment parallels semaglutide. Having a tirzepatide diet plan, understanding what to eat on tirzepatide, and knowing foods to avoid all contribute to better outcomes. Supplements that complement tirzepatide can address nutritional gaps that emerge from reduced food intake. Combinations like tirzepatide with B12 and tirzepatide with glycine have gained attention for their potential to enhance outcomes, and guides on the triple compound of tirzepatide, glycine, and B12 provide practical implementation details.
The question of alcohol with tirzepatide mirrors the semaglutide conversation, as both medications affect how the body processes alcohol. For women specifically, understanding how tirzepatide affects menstrual cycles is important, as hormonal shifts during rapid weight loss can alter cycle regularity. The same applies to semaglutide effects on menstruation.
Liraglutide versus phentermine
Liraglutide is the closest GLP-1 to phentermine in terms of efficacy, producing around 8 percent body weight loss at its approved dose. This makes it a more interesting comparison point. The weight loss difference between liraglutide and phentermine is smaller than with semaglutide or tirzepatide, which means the other factors, cost, side effects, duration of treatment, and long-term outcomes, carry more relative weight in the decision.
Liraglutide requires daily injections, which some patients find burdensome compared to phentermine daily pill. However, liraglutide offers the cardiovascular and metabolic benefits common to all GLP-1 medications, which phentermine does not. For patients who need modest weight loss with metabolic benefits and have access to insurance coverage, liraglutide can be a reasonable middle ground between phentermine affordability and semaglutide maximum efficacy.
One advantage liraglutide holds over the more potent GLP-1 options is the ability to fine-tune dosing on a daily basis. If a patient experiences significant nausea after increasing the dose, they can drop back to the previous level the very next day. With weekly semaglutide or tirzepatide, a bad dose means seven days of waiting before the next adjustment opportunity. This flexibility appeals to patients who are sensitive to medication changes or who want more granular control over their treatment. The trade-off is that daily injections require more discipline and create more opportunities to miss doses, which can reduce effectiveness.
Emerging medications versus phentermine
The next generation of GLP-1 based medications will make the comparison with phentermine even more lopsided. Retatrutide, the triple agonist targeting GLP-1, GIP, and glucagon receptors, showed 24+ percent weight loss in phase 2 trials. If these results hold in phase 3, retatrutide will produce weight loss approaching five times what phentermine delivers. The cost considerations for retatrutide and availability timeline are still being determined, but the efficacy trajectory is unmistakable.
Other pipeline medications like CagriSema (semaglutide plus cagrilintide), survodutide, and orforglipron (an oral GLP-1) continue to push the boundaries of what pharmacological weight loss can achieve. Mazdutide and other dual agonists in development further expand the options. Each of these makes phentermine look increasingly outdated by comparison, though phentermine cost advantage remains durable for now.
Making the right decision for your situation
There is no universal right answer. There is only the right answer for you, right now, given your specific circumstances. Here is a framework for thinking through the decision.
Start with your health status. If you have cardiovascular disease, the choice is already made. Phentermine is contraindicated, and GLP-1 medications offer active cardiovascular protection. If you have type 2 diabetes, GLP-1 medications address both weight and blood sugar, making them the clearly superior option. If you are metabolically healthy with no cardiovascular risk factors, you have more flexibility in choosing between the two classes.
Consider how much weight you need to lose. If your goal is to lose 10 to 15 pounds for a specific purpose on a defined timeline, phentermine efficacy may be sufficient, and its 12-week treatment window may actually align with your needs. If you need to lose 50 pounds or more, phentermine will not get you there. You need the greater potency and longer treatment duration of a GLP-1 medication.
Be honest about your budget. If GLP-1 medications are financially out of reach and compounded alternatives are not available to you, phentermine producing 5 to 10 percent weight loss is infinitely better than no treatment at all. Do not let the perfect be the enemy of the good. Some weight loss, even if modest and potentially temporary, provides health benefits.
Think about your timeline. Are you looking for a short-term boost or a long-term solution? If three months of appetite suppression is what you need, phentermine delivers that affordably. If you are looking at weight management as a multi-year or lifelong endeavor, GLP-1 medications match that timeline.
Factor in your side effect tolerance. If you are sensitive to stimulants, experience anxiety, have trouble sleeping, or have a history of hypertension, phentermine side effect profile may be problematic. If you have a sensitive stomach, the GI adjustment period of GLP-1 medications may be challenging. Neither side effect profile is objectively worse, they are just different, and your individual tolerance matters.
Evaluate your previous experience. If you have tried phentermine before and the weight came back, there is no reason to expect a different outcome the second time. If you have tried a GLP-1 and did not tolerate it, phentermine offers a genuinely different mechanism that may work for you. Your history is the best predictor of your future response.
Explore the broader landscape. Beyond these two medication classes, the peptide world offers a range of compounds that support weight management through various mechanisms. Peptides for fat loss include compounds that work through growth hormone pathways, metabolic optimization, and other routes that complement or provide alternatives to traditional appetite-suppressant approaches. Peptides for muscle growth can help preserve lean mass during weight loss, which is critical for maintaining metabolic rate. Even peptides for anti-aging may play a role in overall metabolic health optimization. Tools like the peptide calculator and reconstitution calculator from SeekPeptides provide practical support for anyone exploring these options.
Frequently asked questions
Is phentermine or a GLP-1 better for quick weight loss?
Phentermine produces faster initial weight loss because it starts working at full strength immediately and does not require dose titration. Most patients notice reduced appetite within the first few days and may lose 3 to 5 pounds in the first week, much of which is water weight. GLP-1 medications start with low doses that gradually increase over weeks, meaning the full appetite-suppressing effect takes longer to develop. However, the total weight lost on GLP-1 medications far exceeds phentermine by the end of treatment. For a detailed look at how quickly semaglutide produces results, early changes in appetite typically begin within the first week, with significant scale changes by month two.
Can I switch from phentermine to a GLP-1 medication?
Yes, and this is a common treatment pathway. Many patients begin with phentermine due to its accessibility and low cost, then transition to a GLP-1 medication for long-term management. There is no required washout period between stopping phentermine and starting a GLP-1, though your physician may want to confirm that cardiovascular parameters (heart rate, blood pressure) have returned to baseline before initiating new treatment. The transition from phentermine to GLP-1 is well-established in clinical practice, and patients who responded well to appetite suppression on phentermine typically respond even better to GLP-1 medications.
Do GLP-1 medications work if phentermine did not work for me?
Possibly. Because the mechanisms are completely different, a poor response to phentermine does not predict a poor response to GLP-1 medications. Phentermine failures can occur because the appetite suppression was insufficient, because tolerance developed too quickly, or because the patient eating patterns were driven by factors other than hunger (emotional eating, habit, environment). GLP-1 medications address some of these limitations by modulating the reward value of food and slowing gastric emptying, which creates physical fullness independent of appetite suppression. The reasons people do not lose weight on semaglutide are usually different from the reasons phentermine fails, which is why cross-class switching can produce different outcomes.
What happens if I stop taking my GLP-1 medication?
Weight regain is the most likely outcome. Clinical data shows an average regain of 5.63 kilograms after stopping semaglutide, with most patients returning to near-baseline weight by 18 months post-discontinuation. The rate of regain averages about 0.8 kilograms per month. Semaglutide withdrawal also commonly involves a return of heightened appetite and food cravings. Some clinicians manage discontinuation by gradually tapering the dose rather than stopping abruptly, and others transition patients to phentermine or other medications to blunt the regain.
Are there people who should not take either medication?
Yes. Pregnant or breastfeeding women should avoid both phentermine and GLP-1 medications. The question of GLP-1 use during breastfeeding has specific considerations that require medical consultation. People with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 should not use GLP-1 medications. Individuals with uncontrolled hypertension, cardiovascular disease, or hyperthyroidism should avoid phentermine. Anyone with a history of eating disorders should use either medication class with extreme caution and close psychiatric monitoring.
Is phentermine a GLP-1 agonist?
No. This is a common misconception. Phentermine is not a GLP-1 medication. It is a sympathomimetic amine that works through norepinephrine release in the central nervous system. GLP-1 receptor agonists work through an entirely different mechanism involving gut hormone signaling. The two drug classes share the goal of weight loss but achieve it through fundamentally different biological pathways, which is precisely why they have different efficacy profiles, side effects, and treatment durations.
Can I exercise on phentermine or GLP-1 medications?
Exercise is recommended with both medication classes and can significantly enhance weight loss results. On phentermine, the stimulant effect may actually increase exercise capacity and motivation, though patients should monitor heart rate carefully during workouts. On GLP-1 medications, exercise is both safe and beneficial, and it may help preserve lean muscle mass during weight loss. While some patients wonder whether they can lose weight on semaglutide without exercise, combining medication with physical activity produces better body composition outcomes and helps maintain metabolic rate. Protein supplementation during GLP-1 treatment can further support muscle preservation.
How do GLP-1 medications compare to each other for weight loss?
The hierarchy based on current clinical data places tirzepatide at the top (20.2% average loss), followed by semaglutide (13.7% average loss), then liraglutide (approximately 8% average loss). The semaglutide versus tirzepatide comparison is detailed and nuanced, with differences in side effect profiles, dosing convenience, and insurance coverage all playing a role. Emerging medications like retatrutide may eventually surpass all current options, and the precise dosing comparisons between medications help clinicians optimize individual treatment plans.
External resources
Understanding the full landscape of weight loss medication options is the first step toward making a decision you will not regret. Whether you lean toward phentermine simplicity and affordability or the greater potency and long-term viability of GLP-1 receptor agonists, the most important thing is that you make the choice based on your actual health profile, your financial reality, and your honest assessment of what you need this medication to do.
For anyone researching peptide-based weight management approaches, SeekPeptides offers comprehensive tools, calculators, and educational resources that go far beyond what a single article can cover. Membership provides access to detailed protocols, compound combination guides, ingredient interaction details, methylcobalamin combination protocols, and community support from others navigating the same decisions. Whether you are just beginning to explore your options or ready to optimize a protocol you have already started, the depth of information available through the platform can make the difference between a good outcome and a great one. Practical guides for traveling with medications, storage information, temperature stability data, and expiration guidelines round out the kind of practical, daily-use knowledge that turns a prescription into a sustainable practice.
In case I do not see you, good afternoon, good evening, and good night. May your protocols stay optimized, your results stay lasting, and your decisions stay informed.