Mar 3, 2026

You ate half a meal. Maybe less. And somehow your stomach feels like you swallowed a basketball. The pressure sits there, heavy and uncomfortable, pushing outward against your waistband. You expected nausea on tirzepatide. Everyone warned you about that. But this relentless, expanding, impossible-to-ignore bloating? Nobody mentioned this part.
You are not imagining things. And you are definitely not alone.
Bloating is one of the most common yet least discussed side effects of tirzepatide treatment. Clinical trials from the SURPASS program show that gastrointestinal adverse events affect a significant percentage of users, with nausea hitting 13-22% and diarrhea affecting 14-19% depending on dose. Abdominal distension, the clinical term for bloating, appears at rates below 5% in formal trial data, but real-world experiences suggest the actual prevalence is considerably higher. Many users do not report bloating as a standalone complaint. They absorb it as part of the general discomfort package. They push through. They wonder if something is wrong with them specifically.
Nothing is wrong with you. The bloating has a clear biological mechanism, a predictable timeline, and a set of management strategies that actually work. This guide covers all of it. From the cellular reasons your stomach feels like a balloon to the specific dietary changes, supplement protocols, and dose adjustment strategies that bring genuine relief. Whether you are on your first dose of tirzepatide or deep into dose escalation, the information here applies. SeekPeptides has compiled the most comprehensive resource available on this topic, drawing from clinical research, community experiences, and evidence-based management approaches.
Why tirzepatide causes bloating in the first place
Understanding the mechanism changes everything. When you know exactly why your stomach feels this way, you stop worrying about whether something has gone wrong. You start making targeted adjustments instead of random guesses.
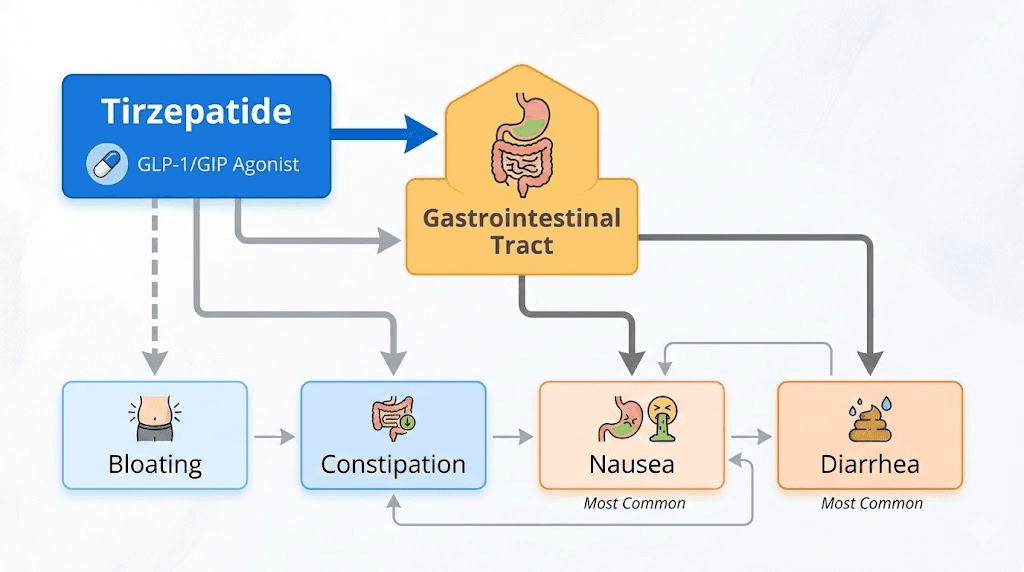
Tirzepatide is a dual GIP and GLP-1 receptor agonist. That dual action is what makes it more effective than pure GLP-1 receptor agonists like semaglutide for weight loss. But that same dual mechanism also affects your digestive system in specific, predictable ways.
Delayed gastric emptying explained
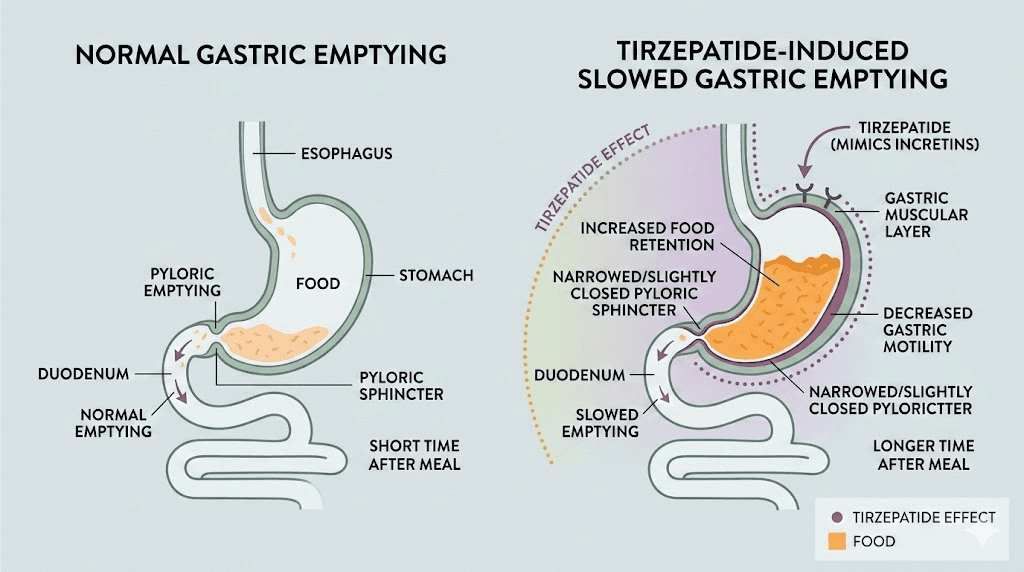
The primary reason for bloating is delayed gastric emptying. Under normal conditions, your stomach processes a meal and moves it into the small intestine within 2-4 hours. Tirzepatide slows this process substantially. Food sits in your stomach longer. Sometimes much longer.
Research published in the Journal of Clinical Endocrinology and Metabolism confirms that GLP-1 receptor agonists and tirzepatide both produce dose-dependent slowing of gastric emptying. The effect is most pronounced during early treatment and during dose escalation periods. Here is the critical detail that most guides miss: the slowing effect shows some attenuation over time with continued use. Your body adapts. Not completely, but meaningfully.
When food remains in the stomach longer than expected, several things happen simultaneously. Gas production increases because bacteria in the upper GI tract have more time to interact with partially digested food. The stomach stretches beyond its typical post-meal volume. Pressure builds against the abdominal wall. The result is that uncomfortable, distended feeling that makes you wonder if your pants shrank overnight.
The GLP-1 and GIP dual mechanism
Pure GLP-1 agonists like semaglutide cause similar digestive effects. But tirzepatide adds the GIP receptor component. Glucose-dependent insulinotropic polypeptide, the GIP part, has its own effects on gut motility and nutrient absorption. The combined activation of both receptor systems creates a more complex digestive impact than either system alone.
This is actually a feature, not a bug. The delayed gastric emptying is part of why tirzepatide works so well for weight loss. You feel full longer. Your appetite drops. You eat less without fighting constant hunger. The bloating is the uncomfortable side of that same coin.
Mouse studies showed something interesting. Tirzepatide delayed gastric emptying to a similar degree as semaglutide acutely. But after two weeks of continuous treatment, the acute inhibitory effects were abolished. This suggests that the digestive system does adapt to the medication, which aligns with the clinical observation that GI side effects tend to diminish over time.
What happens in your gut during a bloating episode
Picture the sequence. You eat a meal. Under normal circumstances, your stomach begins rhythmic contractions called peristalsis, pushing food toward the pyloric sphincter and into the duodenum. Tirzepatide reduces the frequency and strength of these contractions. The pyloric sphincter stays more constricted for longer periods.
Food pools. Liquid separates from solid matter. Gas that would normally pass through quickly gets trapped. The stomach wall stretches. Stretch receptors fire signals to the brain that register as fullness, pressure, and discomfort. Meanwhile, partially fermented food produces additional gas through bacterial interaction. The compounding effect creates the balloon sensation.
Understanding this helps with management. The bloating is not random. It follows predictable patterns based on what you eat, how much you eat, and when you eat relative to your injection schedule. Those patterns become leverage points for relief.
How common is tirzepatide bloating really
Clinical trial numbers and real-world experience tell different stories. Both matter.
What the SURPASS trials show
Across the SURPASS-1 through SURPASS-5 clinical trials involving 6,263 participants, the most commonly reported gastrointestinal adverse events were nausea (12-24%), diarrhea (12-22%), and vomiting (2-13%). These numbers are dose-dependent. At the 5mg dose, nausea hits about 13.7% and diarrhea about 14%. At the 15mg dose, nausea jumps to 22.4% and diarrhea to 19.2%.
Abdominal distension specifically, the closest clinical analog to what people call bloating, was reported at rates comparable to placebo in meta-analysis. That means formally, bloating did not reach statistical significance as a tirzepatide-specific side effect in controlled trials.
But here is where it gets complicated.
Clinical trials capture adverse events through specific reporting frameworks. A participant who experiences bloating alongside nausea might have both symptoms logged under "nausea" or "GI discomfort" rather than "abdominal distension" specifically. The categorization matters. Dyspepsia, which includes bloating as a component symptom, showed up at 7.13% in tirzepatide groups versus 3.31% in comparators. That is more than double the rate.
Real-world prevalence
Outside of controlled trials, the bloating picture looks different. Community reports from tirzepatide users consistently identify bloating as one of the top three most bothersome side effects, alongside constipation and nausea. Many users report bloating without formal medical reporting, especially those using compounded formulations.
The disconnect between trial data and user experience likely comes down to reporting thresholds. In a clinical trial, mild bloating might not trigger an adverse event report. In daily life, that same mild bloating affects clothing choices, social comfort, sleep quality, and overall satisfaction with the medication.
A reasonable estimate puts the real-world prevalence of noticeable bloating somewhere between 20-40% of tirzepatide users, with the severity ranging from mild inconvenience to significant daily disruption. The good news: for the vast majority, it resolves or becomes manageable within weeks.
The timeline: when does tirzepatide bloating start and stop
This is what everyone really wants to know. When does it end?
Week by week breakdown
The pattern is remarkably consistent across users. Bloating tends to follow a predictable arc that mirrors the dose escalation schedule.
Week 1-2 (initial dose, typically 2.5mg): Mild to moderate bloating begins, usually appearing 12-48 hours after the first injection. Some users feel almost nothing. Others notice immediate digestive changes. The variability is wide, but the bloating at this stage tends to be manageable. Your first week on a GLP-1 agonist is an adjustment period for the entire digestive system.
Week 3-4 (continuing at 2.5mg or first dose increase to 5mg): If you escalated to 5mg, expect a temporary spike in bloating for 3-7 days. The body had just started adapting to 2.5mg. Now it needs to recalibrate. If you stayed at 2.5mg, bloating should be noticeably improved from week 1.
Week 5-8 (dose escalation period): This is typically the peak bloating window. Each dose increase resets the adaptation clock partially. Users report that the 5mg to 7.5mg transition and the 7.5mg to 10mg transition produce the most noticeable bloating spikes. Your body is adjusting to increasingly potent gastric emptying delays.
Week 8-12 (reaching maintenance dose): For most users, bloating begins significantly improving once they reach a stable maintenance dose and stop escalating. The digestive system has time to fully adapt. About 80-90% of GI adverse events in the SURPASS trials occurred during the dose escalation period. Once escalation ends, so does most of the bloating.
Week 12+ (maintenance): By this point, the majority of users report minimal or no bloating. Some experience occasional flares related to specific foods or eating patterns, but the constant background bloating resolves.
Why dose escalation is the critical variable
The SURPASS and SURMOUNT trial data confirms what users experience intuitively. Slower dose escalation results in lower incidence of GI side effects including bloating. Healthcare providers can select slower or more flexible escalation schedules based on individual GI tolerability.
Maintaining a lower dose for a longer period before escalating helps improve GI tolerability and the overall treatment experience. If you are following a standard tirzepatide dosing schedule and experiencing severe bloating, discuss slowing the escalation with your provider. An extra 2-4 weeks at your current dose before moving up can make a dramatic difference in comfort.
Some practitioners now use microdosing approaches to minimize GI side effects entirely. Rather than jumping from 2.5mg to 5mg, they use intermediate steps. This strategy sacrifices some speed of weight loss for dramatically better tolerability.
When bloating does not resolve: warning signs
Most bloating is temporary and benign. But persistent, severe bloating that does not improve after 8+ weeks at a stable dose warrants medical evaluation. Potential concerns include gastroparesis (a more serious form of delayed gastric emptying), small intestinal bacterial overgrowth (SIBO), gallbladder issues, or paralytic ileus in rare cases.
Contact a healthcare provider if bloating is accompanied by severe abdominal pain, inability to pass gas, vomiting that does not stop, or fever. These symptoms suggest something beyond typical tirzepatide adjustment effects.
Diet strategies that actually reduce tirzepatide bloating
This is where you get the most control. Dietary modifications produce the fastest, most noticeable improvement in bloating symptoms. Not vague advice about eating healthy. Specific, evidence-based changes that target the exact mechanisms causing the problem.
The small, frequent meals approach
This single change helps more than anything else. When gastric emptying is already delayed, dumping a large meal into the system overwhelms it completely. The stomach simply cannot process a full plate of food at its current reduced processing speed.
Instead of three standard meals, split your intake into 5-6 smaller portions throughout the day. Each portion should be roughly the size of your fist. This keeps a manageable volume moving through the digestive system without triggering the extreme distension that comes from overloading a slow-emptying stomach.
Think of it like a highway bottleneck. You cannot widen the road (speed up gastric emptying while on tirzepatide). But you can reduce the number of cars entering at once. Fewer cars, less traffic jam. Smaller meals, less bloating.
Foods that make bloating worse
Certain food categories dramatically worsen tirzepatide bloating. Understanding why helps you make targeted choices rather than randomly restricting your diet. Our comprehensive tirzepatide foods to avoid guide covers this in detail, but here are the biggest offenders for bloating specifically.
Carbonated beverages: This should be obvious but it catches people constantly. Carbonation introduces gas directly into an already gas-prone environment. Every sip of sparkling water, soda, or carbonated drink adds volume to an already distended stomach. Switch to flat water, herbal teas, or still beverages entirely during the adjustment period.
High-fat foods: Fat slows digestion even without tirzepatide. Add a medication that further delays gastric emptying, and high-fat meals can sit in the stomach for an extraordinarily long time. This is double the delay, double the fermentation, double the bloating. Fried foods, heavy cream sauces, fatty cuts of meat, and butter-heavy dishes are the worst offenders. This does not mean eliminating fat entirely. It means reducing concentration per meal and choosing leaner preparations.
Gas-producing vegetables: Cruciferous vegetables like broccoli, cauliflower, Brussels sprouts, and cabbage produce significant gas during digestion under normal circumstances. When digestion is slowed by tirzepatide, that gas production extends over a longer period and creates more total volume. You do not need to eliminate these foods permanently. But during the initial dose escalation period, reducing intake can provide meaningful relief.
Beans and lentils: Similar to cruciferous vegetables, legumes contain oligosaccharides that the human gut ferments into gas. The extended gastric transit time means more fermentation time and more gas production.
Sugar alcohols: Xylitol, sorbitol, mannitol, and other sugar alcohols found in sugar-free products are notorious gas producers. If you switched to sugar-free gum, sugar-free candy, or protein bars with sugar alcohols after starting tirzepatide, these could be a major contributor to bloating.
Dairy (for some): If you have any degree of lactose intolerance, tirzepatide will amplify the bloating effects. Lactose that would normally cause mild discomfort can produce severe distension when gastric emptying is compromised. Consider a temporary trial of dairy elimination to assess whether it improves symptoms.
Foods that help reduce bloating
Just as some foods worsen bloating, others actively help. A well-planned tirzepatide diet plan incorporates these strategically.
Ginger: Research supports ginger as a gastric motility enhancer. It helps speed up gastric emptying, which directly counteracts the mechanism causing bloating. Ginger tea, fresh ginger in meals, or ginger supplements (500-1,000mg) taken 30 minutes before meals can provide measurable relief. This is not folk medicine. Studies consistently show ginger accelerates gastric emptying and reduces nausea.
Peppermint: Peppermint relaxes the smooth muscle of the GI tract, which can help trapped gas pass through more easily. Peppermint tea between meals is a simple, effective strategy. Enteric-coated peppermint oil capsules work for some people but can cause heartburn in others. Start with tea and assess tolerance.
Lean proteins: Protein is the macronutrient that produces the least gas during digestion. Chicken breast, fish, egg whites, and lean turkey move through the digestive system relatively cleanly. Building meals around lean protein with moderate portions of easily digestible carbohydrates creates less bloating pressure.
Cooked vegetables over raw: Cooking breaks down the cellular structure of vegetables, making them easier to digest. Raw vegetables require significantly more gastric processing. During the bloating-heavy dose escalation period, favor cooked or steamed vegetables over raw salads.
Fermented foods: Yogurt (if dairy tolerant), kimchi, sauerkraut, and kefir provide beneficial bacteria that can support healthier fermentation patterns in the gut. The evidence for fermented foods specifically in tirzepatide users is limited, but the general GI health benefits are well-established.
Meal timing relative to injections
When you eat relative to your tirzepatide injection timing matters more than most people realize. The medication effect peaks at different times depending on when it was administered. Many users report that bloating is worst in the 24-72 hours following their weekly injection.
During that peak window, keep meals especially small and easily digestible. This is not the time for a large family dinner or a heavy restaurant meal. Plan your injection timing so the peak GI effect period falls on days when you can control your eating environment and food choices.
Some users inject in the evening so the worst GI effects hit overnight and during the following morning when eating less feels natural anyway. Others prefer morning injections so they can monitor symptoms throughout the day. Experiment with timing to find what produces the least bloating disruption for your schedule.
Supplements and OTC remedies for tirzepatide bloating
Beyond dietary changes, several supplements and over-the-counter products can provide additional relief. Some have strong evidence. Others have limited support but widespread anecdotal use. Our comprehensive supplements guide for tirzepatide covers the full picture, but here are the most relevant options for bloating specifically.
Simethicone (Gas-X)
Simethicone works by breaking up gas bubbles in the GI tract, making them easier to pass. It does not reduce gas production, but it reduces the volume and pressure of existing gas. For tirzepatide users experiencing acute bloating episodes, simethicone provides relatively fast symptomatic relief.
The standard dose is 125-250mg taken after meals or when symptoms flare. Simethicone has an excellent safety profile with virtually no drug interactions and minimal side effects. It is a reasonable first-line option for managing bloating.
One important caveat: simethicone treats the symptom, not the cause. It is a useful tool for acute relief, but it does not address the underlying delayed gastric emptying. Use it as part of a comprehensive strategy, not as a standalone solution.
Ginger supplements
As mentioned in the diet section, ginger has solid research backing for gastric motility enhancement. In supplement form, 500-1,000mg of ginger root extract taken 30 minutes before meals has been shown to accelerate gastric emptying and reduce nausea. For tirzepatide users, this partially counteracts the medication-induced slowing of digestion.
Look for standardized ginger extract rather than raw ginger powder for more consistent dosing. Some compound formulations include B6 alongside tirzepatide specifically to help with nausea, and adding ginger targets the bloating component as well.
Probiotics
The evidence for probiotics in tirzepatide users is still emerging, but the theoretical basis is sound. Probiotics can synthesize digestive enzymes, promote nutrient absorption, and modify fermentation patterns that contribute to gas production. Research suggests that combined probiotic supplementation may assist tirzepatide in reducing gastrointestinal adverse effects, though evidence specific to tirzepatide remains limited.
If you want to try probiotics, look for strains with specific evidence for bloating reduction. Lactobacillus and Bifidobacterium species have the most research support for GI symptom management. The Pendulum GLP-1 probiotic is specifically marketed toward GLP-1 agonist users, though the evidence base is still developing. Start with a standard multi-strain probiotic and give it 2-4 weeks to assess effectiveness.
Digestive enzymes: do they actually help?
This is one of the most common questions, and the answer may surprise you. Digestive enzyme supplements are generally not necessary or particularly effective for tirzepatide-related bloating. The bloating is not caused by enzyme deficiency. No evidence shows that tirzepatide lowers digestive enzyme production. The symptoms stem from slower gastric emptying and gut hormone changes, not from an inability to break down food.
Enzyme supplements are not routinely recommended for GLP-1 or GIP side effects, and evidence for general bloating relief is mixed. The one exception is alpha-galactosidase (Beano), which can help specifically with gas from beans and certain vegetables by breaking down the oligosaccharides that human enzymes cannot process. If your diet includes significant amounts of legumes or cruciferous vegetables and you do not want to reduce them, Beano taken before those specific meals may help.
Fiber considerations
Fiber is complicated when it comes to tirzepatide bloating. On one hand, adequate fiber supports healthy bowel movements and can help prevent the constipation that often accompanies bloating. On the other hand, too much fiber too quickly in an already-compromised digestive system can worsen gas production.
If you are adding fiber to address constipation-related bloating, increase gradually. Start with an additional 5 grams per day and work up over 2-3 weeks. Soluble fiber sources like psyllium tend to produce less gas than insoluble fiber. Osmotic laxatives like polyethylene glycol (MiraLAX) are an alternative for constipation-related bloating that bypasses the gas production issue entirely.
Peppermint oil capsules
Enteric-coated peppermint oil capsules have clinical evidence for reducing bloating and gas in IBS patients. The mechanism, smooth muscle relaxation in the GI tract, is relevant to tirzepatide users as well. The enteric coating ensures the peppermint oil reaches the intestines rather than dissolving in the stomach, which reduces the risk of heartburn.
Standard dosing is 200mg of enteric-coated peppermint oil, 1-2 capsules before meals. Results typically appear within a few days if peppermint oil is going to help. Not everyone responds, but for those who do, it can be a significant bloating reducer.
Physical strategies for managing bloating
Diet and supplements are not the only tools. Physical strategies can provide surprisingly effective relief, especially during acute bloating episodes.
Walking after meals
Walking for 10-15 minutes after eating is one of the most effective and underutilized bloating remedies. The gentle movement stimulates peristalsis, helping food move through the digestive system more effectively. It also helps trapped gas pass. This is not intense exercise. A slow, comfortable walk around the block is sufficient.
Research on post-meal walking consistently shows benefits for gastric emptying, blood glucose management, and GI comfort. For tirzepatide users specifically, the gastric motility boost from walking partially compensates for the medication-induced slowing. Make it a habit. Walk after every meal during the dose escalation period.
Abdominal massage
Gentle clockwise massage of the abdomen can help move trapped gas and stimulate digestive movement. The clockwise direction follows the path of the colon. Apply gentle to moderate pressure in large circular motions around the navel for 5-10 minutes. Many users find this helpful during acute bloating episodes, especially before bed.
Yoga and stretching
Certain yoga poses are specifically effective for releasing trapped gas and stimulating digestive motility. The wind-relieving pose (pavanamuktasana), child pose, and supine twists are the most commonly recommended. Even a 5-minute gentle stretching routine after meals can improve gas passage and reduce abdominal pressure.
Body positioning
Avoid lying flat immediately after eating. Keep your upper body elevated for at least 30-60 minutes after meals. Lying flat slows gastric emptying further and can increase the sensation of fullness and bloating. If bloating is particularly bad at night, consider using a wedge pillow or elevating the head of your bed.
Left-side sleeping positioning can also help. The anatomical arrangement of the stomach and colon means that lying on the left side facilitates gas passage through the digestive tract.
Dose adjustment strategies for severe bloating
When dietary changes and supplements are not enough, dose management becomes the most powerful tool. This requires working with a healthcare provider, but understanding the options helps you have an informed conversation.
Slower dose escalation
The standard tirzepatide escalation schedule moves from 2.5mg to 5mg after 4 weeks, then increases by 2.5mg every 4 weeks until reaching the target maintenance dose. This pace works well for many people but is too aggressive for those with significant GI sensitivity.
Clinical data from the SURPASS trials confirms that slower dose escalation reduces GI adverse events. Starting with lower doses and using smaller escalation increments resulted in lower incidence of nausea, diarrhea, and vomiting. The same principle applies to bloating.
Options for slower escalation include spending 6-8 weeks at each dose level instead of 4 weeks, using intermediate doses like 3.75mg between the standard steps, or using microdosing protocols that break each dose level into smaller steps.
The trade-off is slower weight loss progress. But if severe bloating is causing you to consider quitting tirzepatide entirely, a slower escalation that keeps you on the medication is far better than a fast escalation that drives you off it.
Splitting doses
Some practitioners recommend splitting the weekly tirzepatide dose into two smaller injections. Instead of one 5mg injection per week, you would take 2.5mg twice per week. This maintains the same total weekly dose but reduces the peak concentration, which can significantly reduce GI side effects including bloating.
This approach is not officially recommended in prescribing guidelines, but it has growing support among practitioners who manage GLP-1 side effects aggressively. Discuss it with your provider if standard dosing produces intolerable bloating.
Temporary dose reduction
If bloating becomes truly unbearable after a dose increase, returning to the previous dose level for an extended period is a reasonable option. Your body may need more time at the lower dose before it can tolerate the next step up.
This is not failure. It is responsive dose management. The tirzepatide dosage chart is a guide, not a rigid prescription. Individual variability in GI tolerance is enormous, and the right dose escalation speed is the one your body can handle while maintaining quality of life.
Finding your effective minimum dose
Not everyone needs to reach 15mg. Many users achieve excellent weight loss results at 5mg or 10mg with significantly fewer side effects. The weight loss timeline may be slightly slower at lower doses, but the reduced bloating and improved quality of life often make this trade-off worthwhile.
If you have reached a dose that produces good appetite suppression and steady weight loss but your provider wants to increase further, discuss whether the additional dose is truly necessary. Sometimes the effective minimum dose is lower than the maximum recommended dose, and there is no benefit to pushing beyond what is already working.
Tirzepatide bloating versus other GI side effects
Bloating does not exist in isolation. It often appears alongside other digestive symptoms, and understanding the relationships between them helps with targeted management.
Bloating versus nausea
Nausea is the most commonly reported tirzepatide side effect, and it frequently coexists with bloating. However, the management strategies differ. Tirzepatide fatigue and nausea often improve with different interventions than bloating alone.
Nausea responds well to ginger, vitamin B6, eating crackers before rising, and avoiding strong smells. Bloating responds better to meal size reduction, carbonation elimination, and physical movement. When both are present, a combined approach works best. Small bland meals with ginger supplementation address both simultaneously.
The tirzepatide with B6 compound formulation was developed specifically to address nausea. If nausea is your primary complaint with bloating as a secondary issue, this formulation may be worth discussing with your provider.
Bloating versus constipation
Constipation and bloating feed each other in a vicious cycle. Slowed gastric emptying leads to slowed colonic transit. Stool moves more slowly through the colon. Water is absorbed more thoroughly, making stool harder. Hard stool is more difficult to pass. Retained stool increases abdominal pressure. Abdominal pressure feels like bloating.
Our tirzepatide constipation treatment guide covers this in detail. The key point for bloating management: if you are constipated, addressing the constipation will likely improve bloating even without additional bloating-specific interventions. Adequate hydration, fiber supplementation, and osmotic laxatives when needed are the first line for constipation-related bloating.
Bloating versus diarrhea
Interestingly, some tirzepatide users experience diarrhea rather than constipation, and this can also coexist with bloating. When the gut is processing food irregularly, alternating between slow transit and rapid transit, both bloating and loose stools can occur.
Diarrhea-associated bloating often responds to reducing FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) in the diet temporarily. A low-FODMAP approach eliminates the most common dietary triggers for both gas production and osmotic diarrhea simultaneously.
Bloating versus acid reflux
Delayed gastric emptying increases the risk of gastroesophageal reflux. When food sits in the stomach longer, there is more opportunity for stomach acid to splash upward into the esophagus, especially when lying down or bending over. The resulting heartburn can overlap with bloating sensations.
If you experience burning along with bloating, elevating your upper body after meals becomes even more important. Antacids or proton pump inhibitors may help with the reflux component. The bloating and reflux often improve together as the body adapts to tirzepatide.
Compound formulations and bloating differences
Not all tirzepatide is created equal when it comes to bloating. The formulation matters.
Standard tirzepatide versus compound formulations
Brand-name Mounjaro and Zepbound deliver tirzepatide in a standardized formulation. Compounded versions may include additional ingredients designed to improve tolerability. Common additions include vitamin B12, vitamin B6, glycine, niacinamide, and methylcobalamin.
The B6 addition is specifically targeted at reducing nausea and may have secondary benefits for bloating by supporting healthy neurotransmitter function in the GI tract. The glycine B12 combination aims to support overall GI function and energy levels during treatment.
While compound formulations cannot eliminate bloating entirely (the core mechanism of delayed gastric emptying remains), some users report meaningfully better GI tolerability with certain compound blends compared to standard tirzepatide. This is difficult to study formally, but the anecdotal pattern is consistent enough to be worth considering.
Oral and sublingual tirzepatide
Oral tirzepatide and tirzepatide drops offer alternative administration routes. The question of whether delivery method affects bloating is still being studied. Theoretically, oral delivery could produce different GI effects because the medication encounters the digestive system directly rather than reaching it through systemic circulation after injection.
Early reports on orally disintegrating tablet (ODT) formulations suggest similar GI side effect profiles to injectable versions, but the data is limited. If injectable tirzepatide causes intolerable bloating and your provider offers an alternative delivery option, it may be worth trying, but do not expect dramatically different GI outcomes.
Bloating at different tirzepatide doses
The relationship between dose and bloating is not perfectly linear. Understanding the dose-response pattern helps set expectations.
2.5mg: the starting dose
Most users experience mild or no bloating at the starting dose. The GI effect is present but typically manageable. This is by design. The 2.5mg starting dose exists specifically to allow the body to begin adapting to tirzepatide gastric effects before the therapeutic dose is reached.
If you experience significant bloating at 2.5mg, discuss extending the initial dose period with your provider before escalating. Your GI system may need more adaptation time than average.
5mg: the first therapeutic dose
The transition from 2.5mg to 5mg is where many users first notice meaningful bloating. This dose doubles the medication concentration and produces a noticeable increase in gastric emptying delay. Bloating at this level typically peaks in the first 1-2 weeks after the increase and begins improving by weeks 3-4.
For many users, 5mg provides meaningful appetite suppression and weight loss initiation while keeping side effects manageable. If 5mg produces good results with tolerable bloating, discuss staying at this dose rather than escalating further.
10mg: the moderate therapeutic dose
The jump to 10mg often produces the most significant bloating spike. Users who tolerated 5mg well sometimes find 10mg substantially more challenging digestively. The 10mg dose represents a point where GI adaptation becomes more demanding.
Bloating at 10mg follows the same pattern as lower doses but may take longer to resolve. Allow 6-8 weeks for full adaptation rather than the 4 weeks typical at lower doses. Aggressive dietary management during this period helps significantly.
15mg: the maximum dose
At 15mg, bloating is most pronounced but also most responsive to management strategies because users have typically been on the medication long enough to have identified their personal triggers and effective remedies. The overall GI adaptation that occurred at lower doses carries forward, so the incremental increase in bloating from 10mg to 15mg is usually less dramatic than the jump from 5mg to 10mg.
Special situations and bloating
Bloating and exercise
Exercise affects bloating in complicated ways. Moderate exercise like walking, swimming, and cycling tends to reduce bloating by stimulating digestive motility. Intense exercise, especially high-impact activities or heavy weightlifting, can temporarily worsen bloating because blood flow diverts away from the digestive system.
The benefits of tirzepatide extend well beyond weight loss, and maintaining an exercise routine is important. Time your workouts relative to meals. Exercising on a full stomach when gastric emptying is already delayed is a recipe for severe bloating and discomfort. Wait at least 2-3 hours after eating before intense exercise. Light walking is the exception and can be done immediately after meals.
Bloating and alcohol
Drinking on tirzepatide introduces several bloating risk factors. Alcohol irritates the GI lining, increases acid production, and can alter gut motility independently. Combined with tirzepatide delayed gastric emptying, even moderate alcohol consumption can produce significant bloating. Carbonated alcoholic beverages like beer and sparkling wine are especially problematic.
If you choose to drink, follow the best alcohol choices for tirzepatide users. Avoid carbonated options entirely. Keep portions small. Eat a small amount of food with alcohol rather than drinking on a completely empty stomach.
Bloating and menstrual cycles
For women, tirzepatide bloating can compound with hormonal bloating during certain phases of the menstrual cycle. Progesterone naturally slows GI motility, and the luteal phase (post-ovulation) already produces bloating in many women. Adding tirzepatide delayed gastric emptying on top of hormonal GI slowing can create particularly uncomfortable weeks.
Tracking your cycle alongside your tirzepatide injection schedule helps identify patterns. Some women find that adjusting their injection day to avoid overlapping with the luteal phase reduces total bloating burden. Our guide on how tirzepatide affects menstrual cycles covers the broader hormonal interactions in detail.
Bloating during travel
Travel adds multiple bloating risk factors: disrupted eating schedules, different food options, dehydration from flying, reduced physical activity during transit, and stress. If you are traveling with tirzepatide, plan proactively. Bring familiar snacks that you know do not trigger bloating. Prioritize hydration especially during flights. Schedule walking into your travel days. Consider timing your injection so you are not in the peak GI effect window during travel days.
Bloating and pregnancy
Tirzepatide is not recommended during pregnancy. If you experience bloating while on tirzepatide and suspect pregnancy, contact your healthcare provider immediately. Some users have become pregnant on tirzepatide, and bloating is one of many overlapping symptoms between early pregnancy and GLP-1 side effects that can cause confusion.
Comparing bloating across GLP-1 medications
If bloating is a primary concern, understanding how it compares across different medications helps inform treatment decisions.
Tirzepatide versus semaglutide bloating
The semaglutide versus tirzepatide comparison is relevant here. Both medications cause bloating through delayed gastric emptying, but the profiles differ somewhat. Our detailed semaglutide bloating guide covers the semaglutide side specifically.
Semaglutide users report similar rates of bloating, with some studies suggesting the GI side effect profile is roughly comparable between the two medications. The dual GIP/GLP-1 mechanism in tirzepatide does not appear to produce substantially more bloating than pure GLP-1 agonism, though individual responses vary widely.
For users who experienced severe bloating on semaglutide and are considering switching to tirzepatide, the bloating pattern may or may not improve. There is no reliable predictor of which medication will produce less bloating for a specific individual. Some users find tirzepatide easier on the GI system. Others find the opposite.
Tirzepatide versus retatrutide bloating
Newer triple agonists like retatrutide add a glucagon receptor component to the GLP-1 and GIP activity. Early data suggests similar or slightly higher GI side effect rates compared to tirzepatide. Users considering whether retatrutide is better than tirzepatide should not expect a major bloating advantage from the newer medication.
When switching medications for bloating
If bloating on tirzepatide is intolerable despite aggressive management, switching to a different GLP-1 medication is a reasonable option. The GI response to GLP-1 agonists has significant individual variability. A medication that causes severe bloating for one person may be well-tolerated by another, even when the mechanism is similar.
Discuss switching strategies with your provider. A direct switch with appropriate dose conversion is typically the approach. Allow 4-6 weeks on the new medication before judging the bloating response, as adaptation time is needed for any GLP-1 agonist.
Building your personal bloating management protocol
Generic advice only goes so far. The most effective bloating management is personalized. Here is how to build a protocol tailored to your specific situation.
Step 1: identify your specific bloating pattern
For one week, track the following after each meal: what you ate, how much you ate, how long after your injection you ate, bloating severity on a 1-10 scale, and what (if anything) helped. This simple tracking exercise reveals patterns that are invisible without documentation.
Most users discover that 2-3 specific triggers are responsible for the majority of their bloating. Eliminating those specific triggers produces disproportionate improvement compared to making broad dietary changes.
Step 2: implement the foundational changes
These apply to virtually everyone on tirzepatide.
Reduce meal size to fist-sized portions. Eliminate carbonated beverages entirely. Walk for 10-15 minutes after every meal. Stay aggressively hydrated with flat water, aiming for at least 8-10 glasses per day. Avoid eating within 3 hours of bedtime.
These foundational changes alone resolve or significantly improve bloating for about 60-70% of users. Give them a full 2 weeks before adding additional interventions.
Step 3: add targeted supplements
If foundational changes are not sufficient, add supplements in order of evidence strength. Start with ginger (500mg before meals). If needed, add simethicone (125-250mg after meals as needed). If constipation is contributing, add a gentle osmotic laxative. Consider a probiotic supplement if the above combination is not adequate.
Add one supplement at a time with 5-7 days between additions. This lets you identify which interventions actually help rather than throwing everything at the problem simultaneously and not knowing what worked.
Step 4: optimize timing and dose management
If steps 1-3 produce meaningful but insufficient improvement, look at timing and dose factors. Adjust your injection timing to minimize bloating during important days or events. Discuss dose escalation speed with your provider. Consider whether your current dose is actually necessary or whether a lower dose with less bloating would serve you better overall.
Step 5: evaluate whether switching is appropriate
If you have worked through steps 1-4 for at least 8-12 weeks at a stable dose and bloating remains significantly impactful on quality of life, discuss switching medications with your provider. Intolerable side effects that persist despite aggressive management are a legitimate reason to try a different approach.
SeekPeptides members access detailed protocol builders and personalized guidance for optimizing GLP-1 therapy while minimizing side effects like bloating. The combination of evidence-based approaches and community experience provides a comprehensive toolkit that no single guide can fully replicate.
The gut microbiome connection
Emerging research suggests that the gut microbiome plays a role in how individuals respond to tirzepatide, including the severity and duration of GI side effects.
How tirzepatide affects gut bacteria
Delayed gastric emptying changes the environment in which gut bacteria operate. Slower transit means different fermentation patterns, altered pH levels in various gut segments, and shifts in bacterial populations. Some bacterial strains thrive in the altered environment while others decline. These shifts can influence gas production, bowel habits, and bloating severity.
Users with healthier, more diverse baseline microbiomes may adapt to tirzepatide GI effects more quickly. This is speculative but consistent with broader research showing that microbiome diversity predicts GI resilience.
Supporting your microbiome during treatment
Diverse dietary fiber from multiple sources supports microbiome diversity. Fermented foods introduce beneficial bacteria. Avoiding unnecessary antibiotics preserves existing microbiome populations. These general microbiome-supporting practices may help reduce bloating duration and severity during tirzepatide treatment.
The relationship between GLP-1 agonists and the gut microbiome is an active area of research. Future treatment protocols may incorporate microbiome assessments to predict GI tolerability and customize management strategies, but current practice relies on the empirical approaches outlined in this guide.
Long-term outlook for tirzepatide bloating
The long-term picture is reassuring for most users.
Chronic versus acute bloating
The acute bloating associated with dose initiation and escalation is time-limited. It resolves for the overwhelming majority of users. Chronic, persistent bloating that lasts beyond 3-6 months at a stable dose is uncommon and warrants medical evaluation.
For users on long-term GLP-1 therapy, occasional bloating flares may occur in response to dietary indiscretions, stress, or illness, but the baseline level of bloating typically remains far lower than what was experienced during the initial adjustment period.
Does bloating affect weight loss outcomes
Many users worry that bloating means the medication is not working properly. In fact, bloating has no negative correlation with weight loss outcomes. Some degree of GI response actually indicates that the medication is active and producing the expected physiological effects.
SURPASS trial data showed no meaningful difference in weight loss between participants who experienced GI side effects and those who did not. The bloating is uncomfortable, but it does not indicate treatment failure or reduced effectiveness. Users who follow their tirzepatide diet plan and management protocol while tolerating mild bloating often achieve excellent long-term results.
After stopping tirzepatide
If you eventually discontinue tirzepatide or begin weaning off, bloating resolves completely as gastric emptying returns to normal speed. The digestive effects are entirely medication-dependent and do not represent permanent changes to GI function.
For those planning to maintain weight loss after stopping tirzepatide, the bloating management skills developed during treatment, smaller meal sizes, mindful eating, regular walking after meals, become valuable maintenance habits regardless of medication status.
Frequently asked questions
How long does tirzepatide bloating last?
For most users, significant bloating lasts 4-8 weeks during the active dose escalation period. Once a stable maintenance dose is reached, bloating typically resolves within 2-4 additional weeks. About 80-90% of GI adverse events in clinical trials occurred during dose escalation. If bloating persists beyond 12 weeks at a stable dose, consult your healthcare provider.
Does tirzepatide bloating mean the medication is working?
Bloating indicates that tirzepatide is producing its expected physiological effects, including delayed gastric emptying and appetite suppression. However, absence of bloating does not mean the medication is not working. GI response varies widely between individuals. Focus on appetite changes and weight loss progress rather than side effect presence as indicators of effectiveness.
Is tirzepatide bloating dangerous?
Typical bloating from tirzepatide is uncomfortable but not dangerous. It reflects the medication slowing gastric emptying as intended. However, severe bloating accompanied by intense abdominal pain, inability to pass gas or stool, persistent vomiting, or fever could indicate a more serious condition and requires immediate medical evaluation.
Can I take Gas-X with tirzepatide?
Yes. Simethicone (Gas-X) has no known interactions with tirzepatide and is safe to use for bloating relief. The standard dose is 125-250mg after meals or when symptoms occur. It works by breaking up gas bubbles rather than reducing gas production, so it provides symptomatic relief without affecting the medication mechanism.
Should I stop eating when bloated on tirzepatide?
You should not skip meals entirely, as this can disrupt blood sugar regulation and overall nutrition. Instead, reduce portion sizes significantly during bloating episodes. Choose easily digestible foods like lean proteins, cooked vegetables, and simple carbohydrates. Eat very small amounts more frequently rather than skipping meals and then overeating when hungry.
Does tirzepatide bloating get worse at higher doses?
Bloating can temporarily increase with each dose escalation, but the relationship is not strictly dose-dependent. Many users experience less bloating at 15mg than they did during the initial 5mg escalation because their bodies have had months to adapt to the gastric effects. Slower dose escalation reduces the severity of bloating spikes at each step.
What is the difference between tirzepatide bloating and gastroparesis?
Tirzepatide causes temporary, dose-dependent slowing of gastric emptying that improves over time and resolves when the medication is discontinued. Gastroparesis is a chronic condition where the stomach empties abnormally slowly regardless of medication use. If bloating and fullness persist indefinitely, worsen over time despite stable dosing, or are accompanied by frequent vomiting of undigested food hours after eating, gastroparesis evaluation is appropriate.
Can probiotics help with tirzepatide bloating?
Some evidence suggests probiotics may help by modifying gut fermentation patterns that contribute to gas production. Look for multi-strain formulations containing Lactobacillus and Bifidobacterium species. The Pendulum GLP-1 probiotic is specifically formulated for GLP-1 users. Allow 2-4 weeks for probiotics to show effects, as gut microbiome changes take time.
External resources
PMC: Tirzepatide-induced gastrointestinal manifestations systematic review
Diabetes, Obesity and Metabolism: GI adverse events in SURPASS trials
Journal of Clinical Endocrinology: Delayed gastric emptying with GLP-1 agonists
For researchers serious about optimizing their GLP-1 protocols while minimizing side effects, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven management strategies, and a community of thousands who have navigated these exact challenges successfully.
In case I do not see you, good afternoon, good evening, and good night. May your digestion stay comfortable, your doses stay effective, and your progress stay consistent.