Feb 19, 2026

Before you dismiss that dull ache in your legs as "just getting older," read this. Tirzepatide is one of the most effective weight loss medications ever developed. It works. The clinical trials prove it. But somewhere around week two or three, a surprising number of users notice something the prescribing information barely mentions. Their body starts to ache.
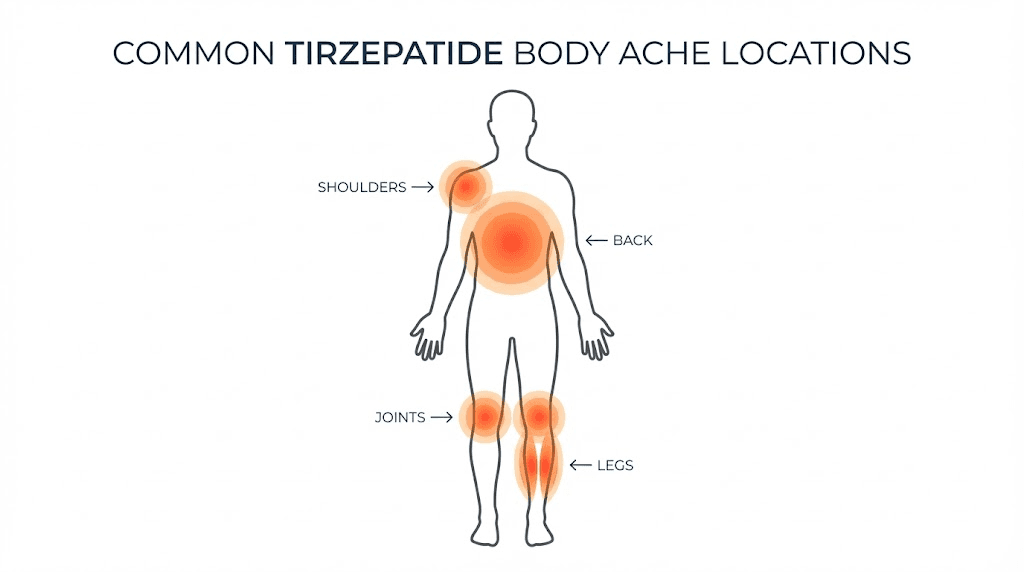
Not the sharp pain of an injury. Something different. A low-grade soreness that settles into muscles and joints like an unwelcome guest. Some describe it as feeling like they ran a marathon they never signed up for. Others say it reminds them of the body aches that come with a mild flu, except there is no flu. Just tirzepatide doing its job while the body scrambles to keep up with rapid metabolic changes.
Here is the good news. These aches are almost never a direct pharmacological effect of tirzepatide itself. The SURMOUNT-1 clinical trial, which tested tirzepatide for weight loss in adults without diabetes, found that musculoskeletal complaints like back pain, arthralgia, and myalgia did not occur at significantly higher rates in the tirzepatide group compared to placebo. That means something else is going on. And once you understand what that something is, you can fix it. This guide covers every type of body ache associated with tirzepatide treatment, the six mechanisms that actually cause them, and a complete protocol for prevention and relief. Whether you are on your first week at 2.5 mg or well into your weight loss dosing schedule, you will find specific, actionable solutions here.
What the clinical data actually says about tirzepatide and body aches
The first thing to understand is that body aches are not listed among the most common adverse effects in the FDA prescribing information for tirzepatide. The primary side effects documented in clinical trials are gastrointestinal, including nausea, diarrhea, vomiting, and constipation. These occur in 5% or more of patients. Musculoskeletal pain sits in a different category entirely.
Numbers tell the real story.
In the SURMOUNT-1 trial, which enrolled 2,539 participants across tirzepatide doses of 5 mg, 10 mg, and 15 mg, musculoskeletal complaints were reported at rates of roughly 1-2%. That is not zero. But it is not statistically different from the placebo group, which means tirzepatide itself may not be the direct cause. A separate analysis of real-world data from the FDA Adverse Event Reporting System found similar patterns. Body aches appear in post-marketing reports, but at rates that do not suggest a strong pharmacological link. The most commonly reported adverse events remain gastrointestinal by a wide margin, with constipation, headaches, and fatigue rounding out the list.
But here is what makes this interesting. A population-based study presented at the American College of Rheumatology examined tirzepatide and joint pain outcomes using a propensity score-matched design. The findings were surprising. Tirzepatide initiation was actually associated with a lower overall risk of joint pain, including lower back pain, hip pain, and knee pain. The likely explanation is straightforward: when you lose significant weight, you reduce mechanical stress on joints. The medication that causes temporary aches during the adjustment period may ultimately reduce chronic pain over time.
Community data paints a slightly different picture. A study analyzing posts from the r/Mounjaro subreddit found that 4.1% of users describing active tirzepatide use mentioned body aches or stiffness as a side effect. That is higher than the clinical trial figure, but self-reported online data skews toward people experiencing problems. Users who feel fine rarely post about it. The real prevalence likely falls somewhere between the clinical trial rate of 1-2% and the community-reported rate of 4-5%.
What does all of this mean for you? If you are experiencing tiredness and body aches on tirzepatide, you are not imagining things. The discomfort is real. But it is almost certainly caused by the downstream effects of the medication rather than the drug itself, and that distinction matters enormously when it comes to treatment. If the drug were directly causing pain through receptor activity, your options would be limited. Because the causes are indirect, they are fixable.
Six reasons tirzepatide causes body aches (and why most are indirect)
Understanding the mechanism behind your pain is the fastest path to resolving it. Tirzepatide works as a dual GIP and GLP-1 receptor agonist, meaning it activates two separate incretin pathways simultaneously. This dual action suppresses appetite, slows gastric emptying, improves insulin sensitivity, and promotes significant weight loss. Each of these effects can create secondary conditions that manifest as body aches. Six mechanisms account for the vast majority of cases.
Dehydration and electrolyte imbalances
This is the most common culprit. Tirzepatide reduces appetite dramatically. When food intake drops, water intake often drops with it, because a significant portion of daily hydration comes from food. Add in the gastrointestinal side effects that many users experience during dose escalation, including nausea, vomiting, and diarrhea, and the result is a fluid deficit that the body feels in its muscles and joints.
Even mild dehydration causes problems. A 2% drop in body water content is enough to trigger muscle cramping, stiffness, and a vague achiness that can be difficult to pinpoint. Electrolytes like sodium, potassium, and magnesium regulate muscle contraction and relaxation. When these minerals fall out of balance due to reduced food intake or fluid loss, muscles become prone to spasms and sustained tension.
The fix is not simply drinking more water. You need to replenish electrolytes too. Plain water without electrolyte supplementation can actually worsen the imbalance by diluting the minerals you have left. We will cover the exact hydration protocol later in this guide.
Rapid weight loss and musculoskeletal stress
Tirzepatide produces substantial weight loss. The SURMOUNT-1 trial demonstrated average reductions of 15-22.5% of body weight over 72 weeks, depending on dose. That kind of change does not happen without consequences for the musculoskeletal system. When you carry less weight, your body redistributes mechanical forces across joints and connective tissue. Ligaments, tendons, and joint capsules that adapted to a higher body weight need time to adjust to the new load pattern.
Think of it like this. If you wore a 50-pound weighted vest every day for years and then suddenly removed it, your body would feel strange for a while. Muscles that compensated for the extra load would need to recalibrate. Joints would experience different stress patterns. That recalibration process can feel like generalized achiness, particularly in weight-bearing joints like the knees, hips, and lower back. Users tracking their tirzepatide before and after results often notice that body aches peak during the periods of most rapid weight loss and then subside as the rate of change slows.
Muscle loss from inadequate protein intake
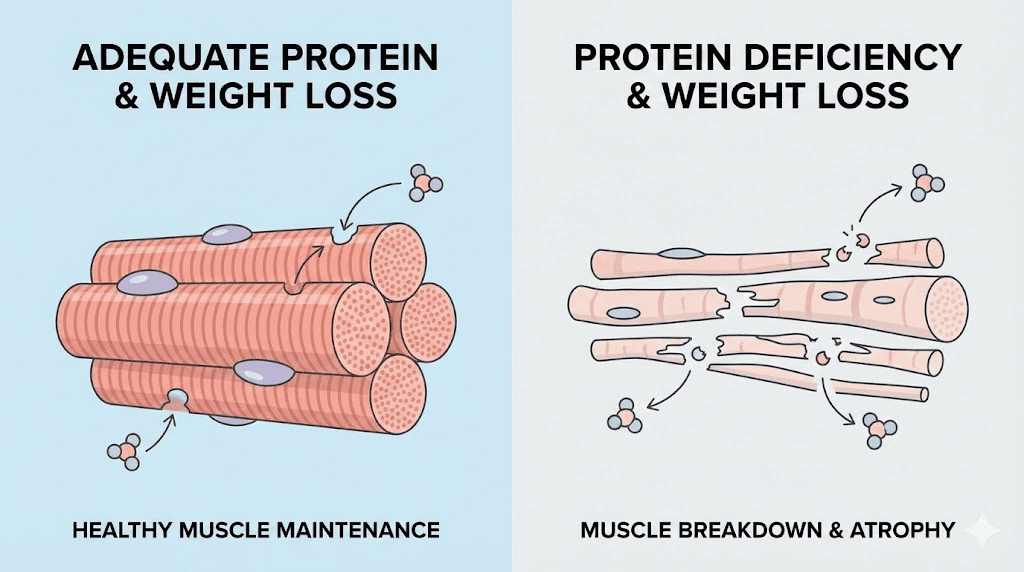
This one is serious and preventable. Tirzepatide suppresses appetite so effectively that many users dramatically undereat without realizing it. When caloric intake drops below a critical threshold and protein intake is insufficient, the body does not just burn fat. It also breaks down muscle tissue for energy and amino acids. The clinical term is sarcopenia, and it is the biggest risk of aggressive weight loss beyond body aches.
Muscle loss creates a cascade of problems. Weakened muscles provide less support for joints, increasing joint stress and pain. Reduced muscle mass lowers metabolic rate, making further weight loss harder. And the breakdown process itself generates inflammatory byproducts that contribute to generalized soreness. Research on GLP-1 receptor agonists suggests that without deliberate intervention, up to 20-40% of weight lost may come from lean mass rather than fat. That is why protein supplementation and dietary optimization are not optional on tirzepatide. They are essential.
Nutrient deficiencies beyond electrolytes
Reduced food intake does not just affect protein and electrolytes. It can create deficiencies across multiple micronutrients that play direct roles in muscle and joint health. Magnesium is the most common, affecting muscle relaxation and nerve signaling. Vitamin D influences calcium absorption and bone health. B vitamins support energy metabolism and nerve function. Omega-3 fatty acids modulate inflammation.
Magnesium deserves special attention. This mineral is required for over 300 enzymatic reactions in the body, including muscle contraction and relaxation. When magnesium levels drop, muscles cannot fully relax after contracting, leading to chronic tension, cramping, and soreness. Many Americans are already marginally deficient in magnesium before starting tirzepatide. The appetite suppression simply pushes them further into deficit. Users who add targeted supplements to their tirzepatide protocol often report significant improvement in body aches within the first week.
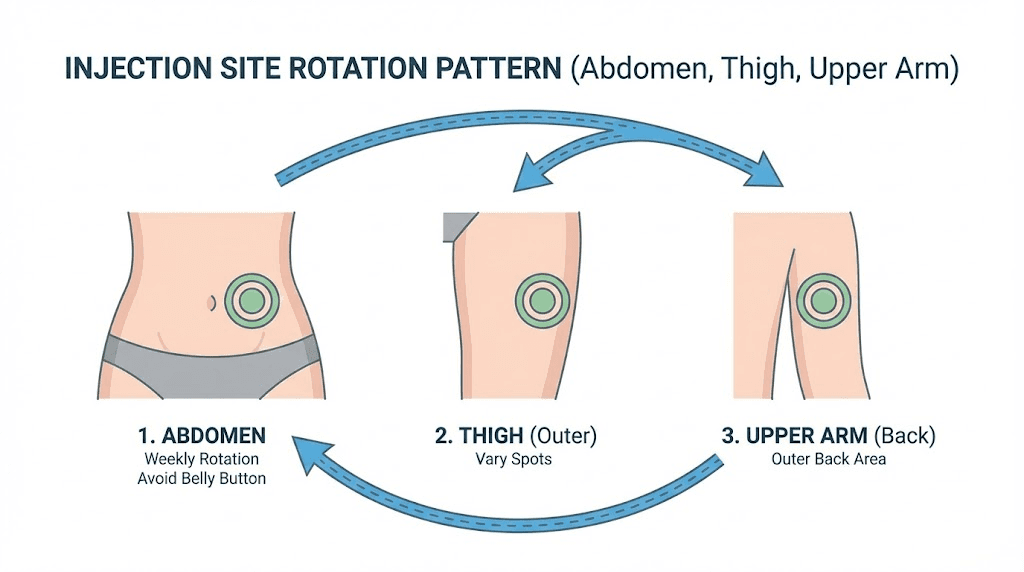
Injection site reactions and immune response
Some body aches are directly related to the injection itself rather than the medication systemic effects. Tirzepatide is administered as a subcutaneous injection, typically in the abdomen, thigh, or upper arm. The injection introduces a foreign protein into the body, and the immune system responds accordingly. This localized immune activation can occasionally produce flu-like symptoms, including generalized achiness, that last 24-48 hours after each injection.
Three published case reports highlight this pattern. In one case, a 37-year-old male developed new neck and back pain after increasing from 7.5 mg to 10 mg. Symptoms peaked at 48-72 hours post-injection and improved when the injection site was changed from the abdomen to the thigh. A second case involved bilateral neck and shoulder pain that resolved after switching the injection location to the arm. These cases suggest that injection site selection matters more than most users realize. Rotating between the abdomen, thigh, and upper arm may help reduce site-specific immune responses that contribute to body aches.
Increased physical activity and delayed onset muscle soreness
Weight loss creates energy. Users who previously felt too tired or heavy to exercise often find themselves motivated to move more once tirzepatide starts working. This is a positive development, but the body needs time to adapt to new physical demands. Starting or intensifying an exercise routine produces delayed onset muscle soreness, commonly called DOMS, which peaks 24-72 hours after the activity.
The challenge is distinguishing DOMS from medication-related aches. If your body aches started around the same time you began a new walking routine, gym program, or increased your daily step count, exercise is the more likely explanation than tirzepatide. The solution is not to stop exercising. It is to increase activity gradually and give your body adequate recovery time between sessions.
Different types of body aches on tirzepatide
Not all body aches are the same. The type, location, and pattern of your discomfort can reveal its underlying cause and point you toward the most effective treatment. Users report five distinct categories of body aches while on tirzepatide treatment. Understanding which category fits your experience helps you target your response precisely.
Joint pain and stiffness (arthralgia)
Arthralgia refers to pain within a joint itself, as opposed to the muscles surrounding it. On tirzepatide, joint pain most commonly affects the knees, hips, wrists, and fingers. It tends to be worse in the morning or after periods of inactivity and improves with gentle movement. The primary cause is the musculoskeletal adjustment to changing body weight, though inflammation from dehydration and nutrient deficiencies can amplify the sensation.
Users with pre-existing joint conditions like osteoarthritis often report initial worsening before long-term improvement. The temporary increase in pain makes sense biomechanically. As weight drops and load patterns change, the joint recalibrates. Once the body stabilizes at a new weight, most users experience significantly less joint pain than they had before treatment. Those interested in peptides that support bone and joint healing may find complementary approaches worth exploring.
Muscle soreness and cramping (myalgia)
Myalgia is pain originating in the muscles themselves. On tirzepatide, it most commonly manifests as a dull, diffuse soreness in the legs, arms, or trunk. Cramping, particularly in the calves and feet at night, is a telltale sign of electrolyte deficiency. Muscle soreness without cramping more often points to protein deficiency or exercise-related strain.
The distinction between cramping and general soreness matters for treatment. Cramping responds quickly to electrolyte supplementation, particularly magnesium and potassium. General soreness requires a broader approach that includes adequate protein intake, hydration, and sometimes adjustments to the tirzepatide dose or timing. If you are experiencing anxiety alongside muscle tension, the connection may be stress-related muscle guarding rather than a direct medication effect.
Back pain
Back pain is the most frequently reported musculoskeletal complaint across all GLP-1 receptor agonist classes, not just tirzepatide. The lower back bears the brunt of postural changes that accompany significant weight loss. As abdominal fat decreases, the center of gravity shifts, and the spinal musculature must adapt. This adaptation period commonly produces low-grade aching across the lumbar region.
Upper back and thoracic pain are less common but do occur, particularly in users who have changed their exercise habits. New resistance training, prolonged standing, or even changes in sleep position due to body composition changes can all contribute. Users dealing with persistent back discomfort may benefit from understanding approaches to spinal health that complement their weight loss protocol.
Neck and shoulder pain
The published case reports on tirzepatide adverse events highlight neck and shoulder pain as a specific pattern worth noting. In at least two documented cases, bilateral neck and shoulder pain emerged within 24 hours of injection and peaked at 48-72 hours. Both cases responded to injection site changes, suggesting a localized immune or inflammatory mechanism rather than a systemic cause.
If your neck and shoulder pain consistently appears 1-3 days after your injection and resolves before the next dose, try rotating your injection site. If you currently inject in the abdomen, switch to the thigh. If you use the thigh, try the upper arm. This simple change resolved symptoms completely in the documented cases.
General malaise and flu-like aching
Some users describe a whole-body achiness that feels similar to the early stages of a viral illness. No fever. No cough. Just that low-grade, everywhere-at-once discomfort that makes you want to lie down. This pattern is most common during the first 1-2 weeks on tirzepatide and during dose escalation periods.
The mechanism is likely a combination of the immune response to the injected protein and the metabolic shift that occurs as the medication takes effect. As your body adjusts to reduced caloric intake, altered insulin dynamics, and changes in gastric motility, the overall metabolic stress can manifest as generalized achiness. This type of body ache is usually the most transient, resolving within 2-3 weeks as the body adapts. Users wondering how quickly tirzepatide takes effect should understand that this initial adjustment period is a normal part of the process.
Timeline: when body aches start and when they stop
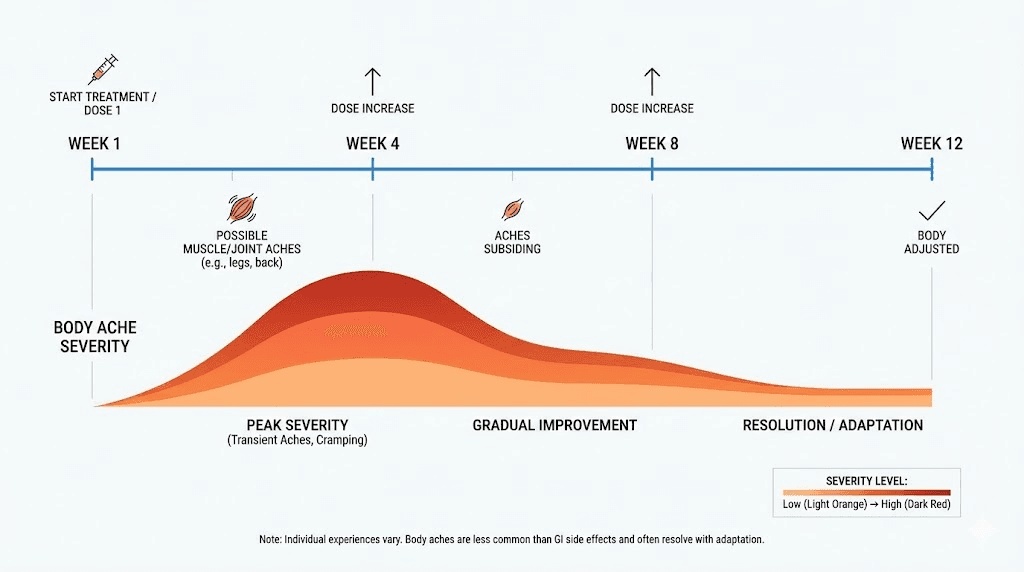
Timing is everything when evaluating body aches on tirzepatide. The pattern of onset and resolution reveals the underlying cause and helps you decide whether action is needed or patience is sufficient.
Week 1-2 (initiation at 2.5 mg): Mild body aches are common during this period. The body is adjusting to a new medication, reduced caloric intake, and shifting metabolic patterns. Most users describe this phase as feeling slightly "off" rather than being in significant pain. Aches during this period typically resolve on their own.
Week 3-4 (still at 2.5 mg or first escalation to 5 mg): This is when dehydration and electrolyte-related aches become most pronounced. By now, appetite suppression is firmly established, and many users have unconsciously reduced their fluid and mineral intake significantly. If aches worsen during this period, hydration and electrolytes are the first intervention to try.
Week 5-8 (dose escalation through 5 mg to 7.5 mg): Each dose increase can temporarily reintroduce body aches, particularly in the 48-72 hours following the new dose. This is normal and expected. The aches associated with dose changes typically resolve within a week as the body adjusts to the higher level. Users following a proper dose titration schedule experience fewer escalation-related aches than those who increase doses too rapidly.
Week 8-12 (higher doses, 10 mg to 15 mg): By this point, most initial body aches have resolved. If new aches appear at higher doses, they typically relate to more aggressive weight loss and the musculoskeletal adjustments that accompany it. Protein intake becomes critical at this stage.
Beyond week 12: Persistent body aches beyond three months warrant medical evaluation. While most tirzepatide-related aches resolve within the first 2-4 weeks, ongoing discomfort may indicate an unrelated condition, a nutrient deficiency that has not been addressed, or a need for protocol adjustments.
Most users report that body aches are worst during the first month and diminish steadily as the body adapts. By the 8-12 week mark, the majority of users who experienced early body aches report significant improvement or complete resolution. The key variable is whether they actively address the underlying causes or simply wait and hope.
How to prevent body aches on tirzepatide
Prevention is always easier than treatment. If you are just starting tirzepatide or preparing for a dose increase, implementing these strategies proactively can prevent body aches from developing in the first place. Even if aches have already started, these same interventions form the foundation of effective treatment.
Hydration protocol
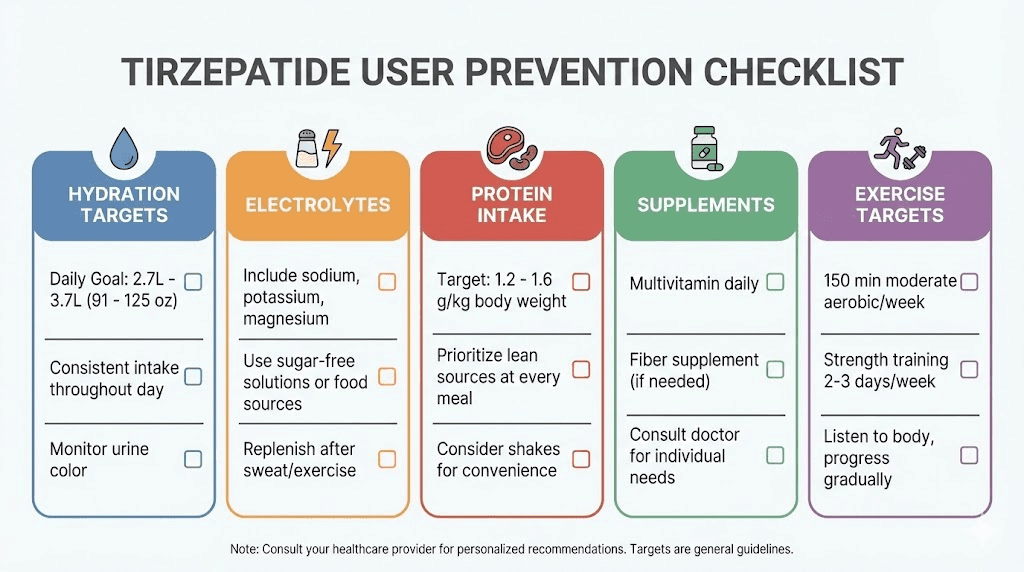
The minimum target is 8-10 glasses of water daily, but that number is misleading in isolation. Your actual hydration needs depend on body weight, activity level, climate, and how much fluid you are losing through tirzepatide side effects. A more useful guideline is to divide your body weight in pounds by two and drink that many ounces of water per day. A 200-pound person needs approximately 100 ounces, or about 12-13 glasses.
Spread your intake throughout the day rather than trying to drink large amounts at once. Sipping consistently is more effective for maintaining hydration than occasional large volumes. Set reminders on your phone if necessary. Many users find that the appetite suppression from tirzepatide also suppresses their thirst cue, making it easy to go hours without drinking anything.
Monitor your urine color. Pale yellow indicates adequate hydration. Dark yellow or amber signals dehydration. If your urine is consistently dark despite drinking water, you may need to increase your electrolyte intake, as the water is passing through without being properly retained.
Electrolyte management
Water alone is not enough. You need sodium, potassium, and magnesium in proper ratios to maintain muscle function and prevent cramping. The simplest approach is to add an electrolyte supplement to your daily routine. Look for products that provide at least 200-400 mg of sodium, 200-400 mg of potassium, and 60-120 mg of magnesium per serving.
Food-based sources work too, but only if you are eating enough. Bananas and avocados provide potassium. Leafy greens and nuts provide magnesium. Salt your food adequately. Many users on tirzepatide drastically reduce their sodium intake simply because they are eating less, and this contributes to the electrolyte imbalance. Your tirzepatide diet plan should specifically account for electrolyte-rich foods.
Protein optimization
Aim for a minimum of 0.7-1.0 grams of protein per pound of ideal body weight daily. This is the single most important nutritional target on tirzepatide, more important than total calories, carbohydrate ratios, or any other macronutrient consideration. Adequate protein preserves muscle mass, supports joint tissue, and provides the amino acids necessary for repair and recovery.
When appetite is suppressed and eating feels like a chore, liquid protein becomes your best friend. Protein shakes designed for GLP-1 users deliver 20-40 grams of protein in a form that is easier to tolerate than solid food. Prioritize protein at every meal. If you can only eat a small amount, make sure the majority of those calories come from protein. Good sources include chicken, fish, eggs, Greek yogurt, and whey protein isolate.
Track your intake for at least two weeks to establish a baseline. Many users are shocked to discover they are consuming 30-50 grams of protein daily when they need 100-150 grams. The gap between what you think you are eating and what you actually consume can be enormous when appetite is suppressed.
Targeted supplementation
Beyond electrolytes and protein, several supplements directly address the mechanisms behind tirzepatide body aches. Vitamin B12 supports nerve function and energy metabolism. Many compounded tirzepatide formulations already include B12, but if yours does not, supplementation at 1000-2000 mcg daily is reasonable. Vitamin D at 2000-5000 IU daily supports calcium absorption and bone health. Glycine is an amino acid that supports collagen synthesis and may help with joint and connective tissue health.
Magnesium glycinate is the preferred form for muscle-related complaints because it combines the benefits of magnesium with additional glycine. A dose of 200-400 mg of elemental magnesium at bedtime can significantly reduce nighttime cramping and morning stiffness. Users taking tirzepatide compounded with glycine and B12 may already receive some of these benefits, though additional supplementation may still be warranted.
Exercise and movement strategy
Movement prevents aches. That sounds counterintuitive if your body already hurts, but gentle activity improves circulation, delivers nutrients to muscles and joints, and prevents the stiffness that comes from inactivity. The key word is gentle. Intense exercise during the early weeks of tirzepatide treatment can worsen body aches rather than improve them.
Start with 10-15 minutes of walking twice daily. Add 5-minute gentle stretching sessions in the morning and evening, focusing on the areas where you experience the most discomfort. Resistance training is important for preserving muscle mass but should be introduced gradually, starting with body weight exercises or light resistance bands before progressing to heavier loads. Wait until you are at least 4-6 weeks into treatment and have stabilized your nutrition before beginning a new resistance training program.
How to treat body aches that have already started
If prevention came too late and body aches are already affecting your daily life, these interventions can provide relief. Start with the least invasive approaches and escalate only if needed.
Temperature therapy
Heat and cold serve different purposes. Heat increases blood flow, relaxes tense muscles, and reduces stiffness. It works best for chronic, dull aches and morning stiffness. Apply a heating pad or warm towel to affected areas for 15-20 minutes at a time, up to three times daily. Warm baths with Epsom salt, which contains magnesium sulfate, provide double benefits by combining heat therapy with transdermal magnesium absorption.
Cold therapy reduces inflammation and numbs acute pain. It works best for joint pain with swelling and sharp, localized discomfort. Apply an ice pack wrapped in a thin towel for 10-15 minutes at a time. Do not apply ice directly to skin.
For most tirzepatide-related body aches, heat tends to be more effective than cold because the underlying mechanism is typically muscular tension and dehydration rather than acute inflammation.
Over-the-counter pain relief
Acetaminophen (Tylenol) is generally the safest first-line option for tirzepatide users experiencing body aches. It does not interfere with the gastrointestinal system, which is already under stress from the medication. Standard dosing of 500-1000 mg every 6-8 hours, not exceeding 3000 mg daily, provides moderate pain relief for most users.
NSAIDs like ibuprofen (Advil) and naproxen (Aleve) are more effective for joint inflammation but carry a risk of gastrointestinal irritation that may compound existing GI side effects. If your primary symptom is joint pain with stiffness, a short course of NSAIDs may be appropriate, but consult your healthcare provider first. Long-term NSAID use is not recommended alongside GLP-1 receptor agonists without medical supervision.
Gentle stretching routine
A targeted 10-15 minute stretching routine performed twice daily can significantly reduce muscle-related body aches. Focus on the areas most commonly affected: the lower back, hips, quadriceps, hamstrings, calves, shoulders, and neck.
Hold each stretch for 20-30 seconds without bouncing. Breathe deeply and allow the muscle to relax into the stretch gradually. The goal is not flexibility improvement. It is circulation enhancement and tension release. If a particular stretch causes sharp pain, skip it and move to the next one. Mild discomfort during stretching is normal. Sharp pain is not.
Yoga and tai chi are excellent options for tirzepatide users because they combine gentle stretching with balance work and controlled breathing. Both practices have documented benefits for musculoskeletal pain management.
Injection site modifications
If your body aches follow a predictable pattern relative to your injection schedule, peaking 24-72 hours after each dose, injection site rotation may provide significant relief. The three standard injection sites for GLP-1 receptor agonist injections are the abdomen, thigh, and upper arm. Rotate between all three, using a different site each week.
Within each site, vary the exact location by at least one inch from the previous injection. This prevents localized tissue irritation that can amplify immune-mediated body aches. Keep a simple log of which site you used and when. Some users find that one particular site produces fewer body aches than others, and adjusting their rotation accordingly provides meaningful improvement. A quality injection pen can also help reduce tissue trauma at the injection site.
Dose titration adjustments
If body aches consistently worsen with dose increases and do not resolve within two weeks, discuss a slower titration schedule with your healthcare provider. The standard escalation from 2.5 mg to 5 mg occurs at 4 weeks, but some patients benefit from extending each dose level to 6-8 weeks before escalating. This gives the body more time to adapt and can reduce the severity of escalation-related side effects, including body aches.
Microdosing approaches, where the dose is increased in smaller increments than standard protocols, are another option gaining attention. While not part of the approved prescribing information, some healthcare providers use compounded formulations to create more gradual dose escalation curves for sensitive patients.
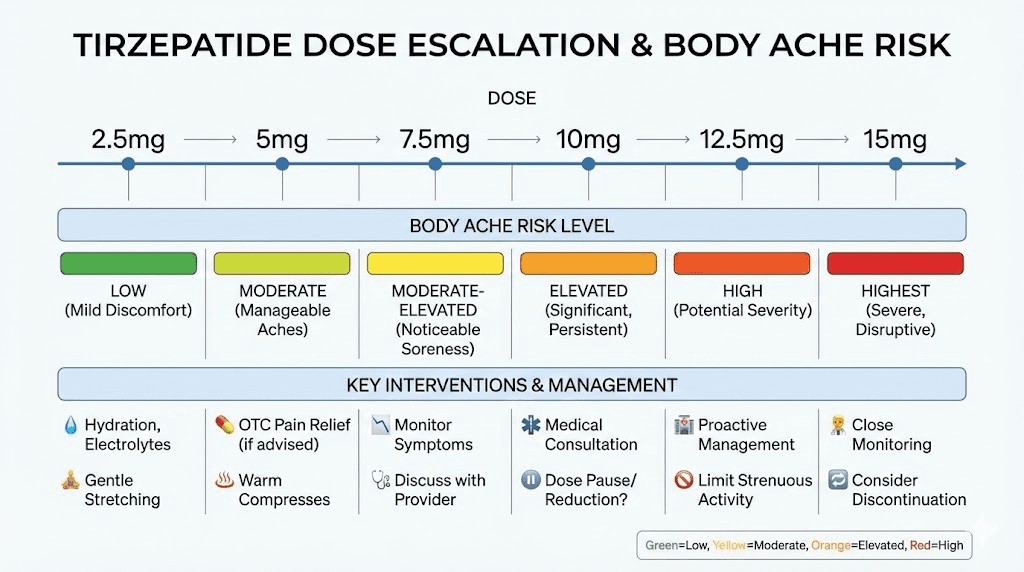
Body aches at different tirzepatide dose levels
Each tirzepatide dose produces a different side effect profile, and body aches follow a general pattern that correlates with dose level and the rate of weight loss it produces.
2.5 mg (starting dose): Body aches at this level are usually mild and transient, primarily related to the initial adjustment to the medication and reduced food intake. Most users report that any achiness at 2.5 mg resolves within 1-2 weeks. The standard dose chart recommends staying at 2.5 mg for at least 4 weeks before escalating.
5 mg (first therapeutic dose): This is where appetite suppression becomes pronounced and weight loss accelerates. Body aches become more common at 5 mg because caloric intake drops more significantly, increasing the risk of dehydration, electrolyte depletion, and protein insufficiency. Proactive nutritional management is important at this dose.
7.5 mg: The intermediate dose often represents a transition point where body aches either resolve or become more persistent. Users who have addressed hydration, electrolytes, and protein by this point typically experience minimal discomfort. Those who have not may find aches intensifying as weight loss continues.
10 mg: Higher doses produce more aggressive appetite suppression and weight loss. Body aches at 10 mg are more likely to stem from muscle loss and rapid musculoskeletal changes than from dehydration alone. Resistance training and protein supplementation become essential at this level.
12.5 mg and 15 mg (maximum doses): At these levels, the side effect profile is well-established for each individual. New body aches at maximum doses are uncommon if lower doses were tolerated. If they do appear, they typically relate to the continued pace of weight loss rather than new medication effects. Detailed dosage charts in units can help you understand exactly where you are in the escalation process.
Tirzepatide body aches versus semaglutide body aches
If you are comparing tirzepatide to semaglutide, you might wonder whether one causes more body aches than the other. The honest answer is that the data does not show a clear winner. Both medications produce similar rates of musculoskeletal complaints in clinical trials, with body aches reported in roughly 1-5% of users across both drug classes.
The mechanisms are identical. Both medications suppress appetite, both cause gastrointestinal side effects that can lead to dehydration, and both produce weight loss that stresses the musculoskeletal system. The key difference is that tirzepatide generally produces more weight loss, more quickly, which means the indirect causes of body aches may be more pronounced. Users on tirzepatide lose an average of 15-22.5% of body weight versus 10-15% on semaglutide at comparable durations.
Some users who experience fatigue on semaglutide find that tirzepatide produces less fatigue but more musculoskeletal discomfort, or vice versa. The side effect profiles are individual enough that switching between medications sometimes resolves specific complaints. Our guide to semaglutide versus tirzepatide side effects provides a detailed comparison across all symptom categories.
For users considering switching, the semaglutide to tirzepatide conversion chart outlines appropriate dose matching to minimize side effects during the transition.
When body aches signal something more serious
The vast majority of body aches on tirzepatide are benign and self-limiting. But certain symptoms require prompt medical attention because they may indicate a serious underlying condition. Knowing the red flags can prevent a treatable complication from becoming dangerous.
Rhabdomyolysis warning signs
Rhabdomyolysis is the rapid breakdown of skeletal muscle that releases muscle fiber contents into the bloodstream, including a protein called myoglobin that can damage the kidneys. While extremely rare, a case of rhabdomyolysis associated with tirzepatide use was published in a peer-reviewed journal. The warning signs include severe muscle pain that is disproportionate to any activity, dark brown or cola-colored urine, muscle weakness that prevents normal movement, and swelling in the affected muscle groups.
If you experience any combination of these symptoms, seek emergency medical care immediately. Rhabdomyolysis is treatable when caught early but can cause permanent kidney damage if untreated.
Pancreatitis symptoms
Pancreatitis is listed as a potential adverse event for all GLP-1 receptor agonists, including tirzepatide. While it does not typically present as body aches, the abdominal pain it causes can sometimes be mistaken for generalized abdominal or back discomfort. The distinguishing features of pancreatitis pain are severe, constant upper abdominal pain that radiates to the back, pain that worsens after eating, nausea and vomiting that does not improve with standard antiemetics, and a rigid or tender abdomen.
If abdominal pain is severe, constant, and accompanied by these features, contact your healthcare provider or go to an emergency room. Do not assume it is a normal side effect of the medication.
Severe dehydration warning signs
Moderate dehydration causes body aches. Severe dehydration is a medical emergency. Warning signs include dizziness or lightheadedness when standing, rapid heartbeat, little or no urine output, confusion or extreme fatigue, dry mouth with inability to produce tears, and sunken eyes. If gastrointestinal side effects from tirzepatide have prevented you from keeping fluids down for 24 hours or more, contact your healthcare provider. Intravenous fluid replacement may be needed.
Allergic reaction indicators
Rarely, body aches accompanied by hives, facial swelling, difficulty breathing, or rapid heart rate may indicate an allergic reaction to tirzepatide. These symptoms require immediate emergency care. If you experience generalized body aches with any signs of anaphylaxis after a tirzepatide injection, call emergency services without delay.
Real case reports of tirzepatide musculoskeletal symptoms
Published case reports provide valuable insight into how tirzepatide-related body aches present in clinical practice. While individual cases cannot establish causation, they reveal patterns that clinical trials may miss due to their structured reporting methods.
Case 1: A 38-year-old woman switched from semaglutide 2.4 mg to tirzepatide 5 mg. Within 24 hours, she developed paroxysmal palpitations that woke her from sleep, with a self-recorded heart rate of 130 beats per minute, accompanied by chest discomfort and generalized myalgia. Her blood pressure dropped to 90/58 mmHg. She discontinued tirzepatide, and all symptoms resolved within one week after switching back to semaglutide. This case highlights that some individuals may respond very differently to tirzepatide compared to semaglutide, even when the medications share similar mechanisms.
Case 2: A 37-year-old man developed new-onset neck and back pain after his tirzepatide dose was increased from 7.5 mg to 10 mg. Symptoms peaked at 48-72 hours post-injection and occurred consistently after each dose. When the injection site was moved from the abdomen to the thigh, symptoms became tolerable. He continued treatment successfully. This case supports the theory that injection site rotation can meaningfully reduce musculoskeletal symptoms.
Case 3: A 43-year-old man with type 2 diabetes initiated tirzepatide at 2.5 mg and developed bilateral neck and shoulder pain accompanied by morning headaches. After the injection site was changed to the arm, symptoms resolved completely. The dose was subsequently increased to 5 mg without recurrence. This case reinforces the injection site hypothesis and suggests that starting the medication at a low dose with the right injection site can prevent musculoskeletal complaints from the outset.
In all three cases, the temporal relationship between injection and symptom onset was clear, with symptoms appearing within 24 hours and peaking at 48-72 hours. Differential diagnoses including infection, structural pathology, anemia, thyroid dysfunction, and medication interactions were all excluded. These case reports underscore the importance of considering injection site modification as a first-line intervention for body aches that correlate with the injection schedule.
Supplements that help with tirzepatide body aches
Targeted supplementation addresses the nutritional deficiencies that cause most tirzepatide-related body aches. These six supplements have the strongest evidence base for reducing musculoskeletal discomfort during GLP-1 receptor agonist treatment. Always consult your healthcare provider before starting any new supplement, particularly if you take other medications.
Magnesium glycinate (200-400 mg elemental magnesium daily): The single most impactful supplement for body aches on tirzepatide. Magnesium glycinate is preferred because it has higher bioavailability than magnesium oxide and causes less gastrointestinal disturbance. Take it at bedtime to reduce nighttime cramping and improve sleep quality. Most users notice improvement in muscle tension within 3-7 days of consistent supplementation. Those already taking a comprehensive supplement stack should verify their magnesium dose is adequate.
Potassium (from food sources primarily, 2600-3400 mg daily total): Potassium supplementation in pill form is limited to low doses (99 mg per tablet) due to safety regulations. Meeting your needs through food is more effective. Bananas, potatoes, avocados, spinach, and coconut water are all potassium-rich options that can be consumed even when appetite is reduced. If your eating plan on tirzepatide does not include these foods regularly, consider an electrolyte supplement that provides potassium.
Vitamin D3 (2000-5000 IU daily): Vitamin D deficiency is widespread, affecting an estimated 35-40% of American adults. When combined with the reduced food intake from tirzepatide, deficiency risk increases further. Low vitamin D contributes to bone pain, muscle weakness, and generalized achiness. Take vitamin D3 with a meal containing fat for optimal absorption.
Vitamin B12 (1000-2000 mcg daily, methylcobalamin form): B12 supports nerve function and energy metabolism. Deficiency causes fatigue, muscle weakness, and neuropathic pain that can mimic body aches. Some compounded tirzepatide formulations include B12, but the dose may not be sufficient for everyone. Methylcobalamin is the active form and does not require conversion by the body, making it more immediately available. The connection between methylcobalamin and GLP-1 therapy is increasingly recognized as important.
Omega-3 fatty acids (2000-3000 mg combined EPA and DHA daily): Omega-3s modulate inflammation throughout the body and support joint health. They are particularly beneficial for users experiencing joint-predominant body aches. Fish oil or algae-based supplements are both effective options. Take with food to maximize absorption and minimize fishy aftertaste.
Collagen peptides (10-15 grams daily): Collagen provides the specific amino acids, primarily glycine, proline, and hydroxyproline, that the body uses to build and repair connective tissue, including tendons, ligaments, and cartilage. During rapid weight loss, collagen supplementation supports the integrity of these tissues as they adapt to changing mechanical loads. Add collagen powder to your morning protein shake for an easy, flavorless boost.
Your 4-week body aches management plan
If body aches are already affecting your quality of life, this structured 4-week plan provides a systematic approach to identifying and resolving the underlying causes. Each week builds on the previous one, progressively addressing the most common mechanisms behind tirzepatide-related musculoskeletal discomfort.
Week 1: assessment and hydration
Goal: Establish baseline and address the most common cause.
Daily actions:
Calculate your hydration target (body weight in pounds divided by 2 = ounces of water daily)
Track actual water intake using an app or marked water bottle
Add an electrolyte supplement to at least 2 glasses daily
Rate your body ache severity each morning on a 1-10 scale
Note the location, type, and timing of aches relative to injection day
Expected outcome: If dehydration is the primary cause, you should notice improvement within 3-5 days. If aches persist unchanged after a full week of optimal hydration, the cause lies elsewhere.
Week 2: nutritional optimization
Goal: Address protein and micronutrient deficiencies.
Daily actions (add to Week 1):
Track protein intake for 7 consecutive days (aim for 0.7-1.0 g per pound of ideal body weight)
Begin magnesium glycinate supplementation (200-400 mg at bedtime)
Begin vitamin D3 supplementation (2000-5000 IU with a meal)
If not already taking B12, add 1000 mcg methylcobalamin daily
Follow a structured meal plan designed for tirzepatide users
Expected outcome: Nutritional optimization typically produces noticeable improvement by day 10-14. Magnesium supplementation often reduces nighttime cramping within the first 3-4 nights.
Week 3: movement and recovery
Goal: Introduce therapeutic movement and recovery strategies.
Daily actions (add to Weeks 1 and 2):
Begin a 10-15 minute walking routine twice daily
Add a 5-minute stretching routine morning and evening
Use heat therapy (warm bath or heating pad) for 15-20 minutes on the most affected areas
If using Epsom salt baths, soak for 20 minutes 2-3 times weekly
Continue tracking ache severity daily
Expected outcome: Movement and heat therapy provide the most immediate relief for muscle-related aches. Many users report that their pain scores drop by 2-3 points within the first few days of consistent stretching and walking.
Week 4: fine-tuning and evaluation
Goal: Evaluate progress and address remaining issues.
Daily actions (maintain all previous interventions plus):
Review your 4-week pain log for patterns (does pain correlate with injection day, specific activities, or specific meals?)
If injection-related pattern exists, implement injection site rotation
If aches have improved 50% or more, maintain current protocol
If aches have improved less than 50%, discuss with healthcare provider about potential dose adjustment
Consider adding omega-3 fatty acids and collagen peptides if not already included
Expected outcome: By the end of week 4, most users with tirzepatide-related body aches will have experienced significant improvement. Those who have not should seek medical evaluation to rule out unrelated causes.
Users who want precision tracking throughout this process can use the SeekPeptides peptide calculator to monitor their dosage and track their response over time.
Frequently asked questions
Does tirzepatide directly cause body aches?
No. Clinical trial data from SURMOUNT-1 shows that musculoskeletal complaints did not occur at significantly higher rates in the tirzepatide group compared to placebo. Body aches on tirzepatide are caused by indirect effects including dehydration, electrolyte imbalances, rapid weight loss, and muscle-related nutritional deficiencies. This distinction is important because indirect causes are addressable and usually temporary.
How long do tirzepatide body aches last?
Most tirzepatide-related body aches resolve within 2-4 weeks of onset, particularly when the underlying causes are actively addressed with proper hydration, electrolyte supplementation, and adequate protein intake. Body aches that appear during dose escalation typically resolve within 7-10 days at each new dose level. Persistent aches beyond 3 months warrant medical evaluation.
Can I take ibuprofen for tirzepatide body aches?
Short-term ibuprofen use may be appropriate for tirzepatide-related joint pain, but consult your healthcare provider first. NSAIDs can increase the risk of gastrointestinal irritation, which may compound existing GI side effects from tirzepatide including constipation and nausea. Acetaminophen is generally considered the safer first-line option for tirzepatide users.
Do body aches get worse at higher tirzepatide doses?
Not necessarily. Body aches may temporarily reappear with each dose increase, but they typically resolve within 1-2 weeks. Users who proactively manage hydration, nutrition, and supplementation often tolerate higher doses with minimal musculoskeletal discomfort. The compounded tirzepatide dosage calculator can help you plan your escalation schedule.
Should I stop taking tirzepatide if I have body aches?
In most cases, no. Body aches alone are not a reason to discontinue tirzepatide unless they are severe enough to significantly impair daily function and do not respond to the interventions outlined in this guide. Stopping tirzepatide forfeits the metabolic benefits while the body aches resolve on their own anyway. However, if body aches are accompanied by dark urine, severe muscle weakness, high fever, or signs of an allergic reaction, contact your healthcare provider immediately.
Will switching from tirzepatide to semaglutide help with body aches?
It might. Some individuals tolerate one medication better than the other, even though both work through similar mechanisms. If body aches persist despite comprehensive management, discussing a trial of switching from tirzepatide to semaglutide with your healthcare provider is reasonable. The transition requires careful dose matching using a conversion chart to maintain therapeutic effect.
Are body aches a sign that tirzepatide is working?
Not directly. Body aches are not a marker of medication efficacy. However, they often coincide with the period of most active weight loss, which is when the medication is working hardest. Users who experience aches during the first few weeks and then see them resolve typically also report strong appetite suppression and steady weight loss during that same period. For a clearer picture of how long tirzepatide takes to start working, time-to-effect data is more useful than symptom monitoring.
Can I exercise if I have body aches from tirzepatide?
Yes, with modifications. Gentle movement like walking, swimming, and light stretching typically improves body aches rather than worsening them. Avoid intense exercise during the first month of treatment or during dose escalation periods. Once body aches have resolved, gradually introduce resistance training to preserve muscle mass. Users looking at energy levels on tirzepatide should find that as nutrition stabilizes, exercise tolerance improves significantly.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members get access to detailed side effect management guides, personalized dosing tools, and direct support from experienced researchers who understand what you are going through.
In case I do not see you, good afternoon, good evening, and good night. May your joints stay limber, your muscles stay nourished, and your tirzepatide protocol stay comfortable.