Feb 19, 2026

Three weeks in, the scale had barely moved. Two pounds. Maybe three on a good morning. And the nausea from that first injection was still a fresh memory, sitting heavy in your mind right alongside the question everyone asks but nobody answers honestly.
Is this actually working?
That question haunts almost every person who starts semaglutide for weight loss. The clinical trials report averages of 15% body weight reduction. The before-and-after photos online show dramatic transformations. But those are endpoints, final results after months or even a full year of treatment. Nobody talks about the messy, uncertain, sometimes frustrating reality of month one.
Here is the truth that most guides skip over entirely. The first month on semaglutide is not about dramatic weight loss. It is about adaptation. Your body is meeting a new molecule, adjusting its hunger signals, recalibrating the speed at which food moves through your digestive system, and rewiring decades of eating patterns. The starting dose of 0.25 mg exists specifically for this purpose, not to melt fat, but to teach your body how to tolerate the medication without making you miserable.
And that is where the disconnect happens. People expect the fireworks from day one. They see the STEP trial data showing 14.9% average body weight loss and assume the trajectory starts steep. It does not. The first four weeks are a slow burn, a quiet foundation being laid beneath the surface while your GLP-1 receptors learn to respond to something new.
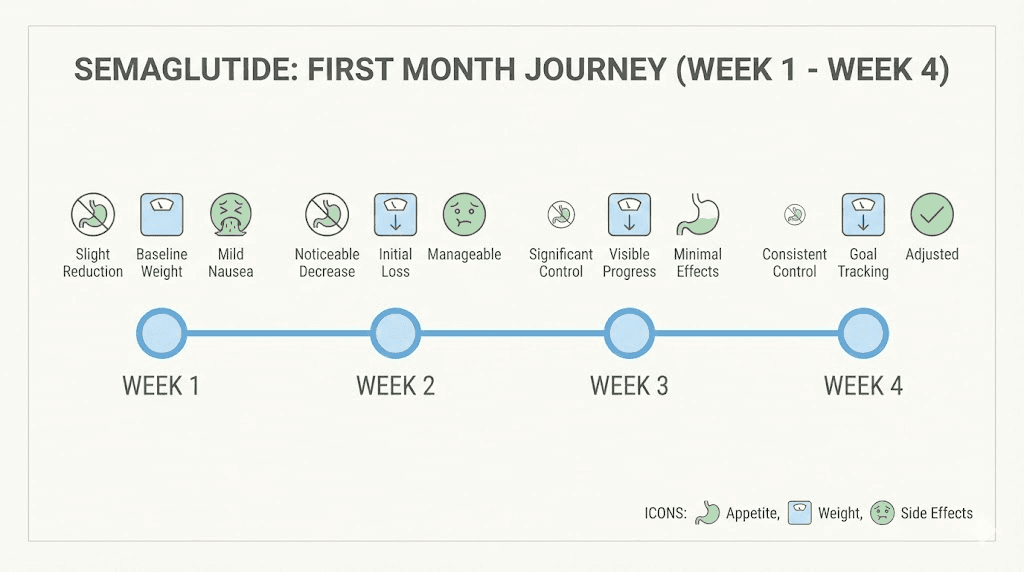
This guide breaks down exactly what happens during those first 30 days, week by week, backed by clinical trial data from the STEP program, real-world outcome studies, and the practical realities that research papers never capture. You will learn what is normal, what is concerning, and what specific strategies can help you get the most out of your first month on semaglutide. SeekPeptides has analyzed thousands of protocols, and the patterns in month one are remarkably consistent once you know what to look for.
What the clinical data actually shows for month one
Before diving into the week-by-week breakdown, you need to understand what the science says about early semaglutide results. Not the marketing. Not the social media highlights. The actual published data from controlled clinical trials involving thousands of participants.
The STEP 1 trial, published in the New England Journal of Medicine, enrolled 1,961 adults with BMI of 30 or higher. Participants received once-weekly injections starting at 0.25 mg, with dose escalation every four weeks until reaching the maintenance dose of 2.4 mg at week 16. Weight loss was already measurable by the first assessment at week 4, but it was modest compared to what came later.
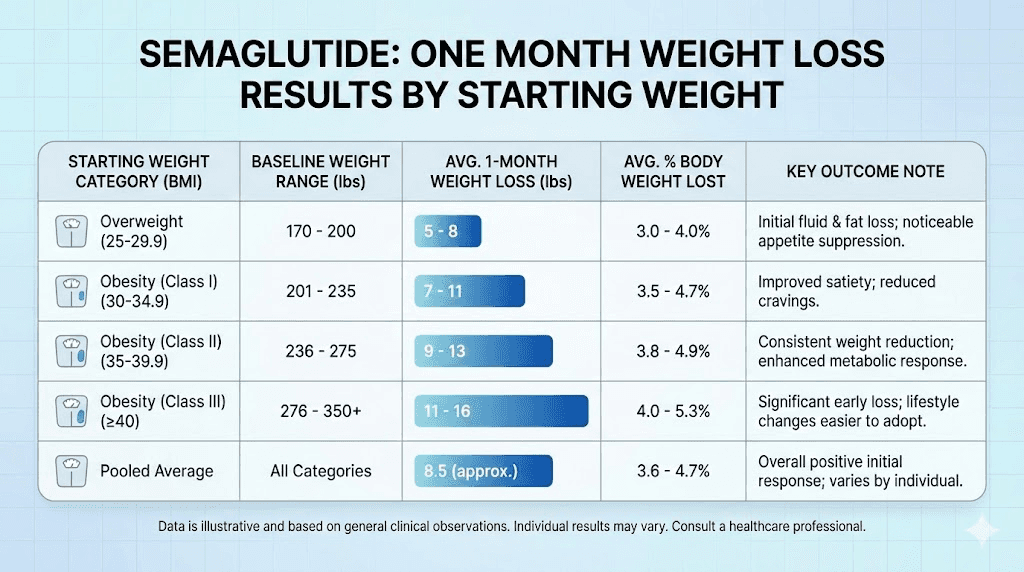
A real-world analysis published in JAMA Network Open examined weight loss outcomes across multiple clinical settings. Patients lost approximately 2% of their body weight per month during the first six months, then about 1% per month for the following six months. That means in month one, you are looking at roughly 2% of your starting weight. For someone weighing 200 pounds, that is about 4 pounds. For someone at 250 pounds, roughly 5 pounds.
Those numbers might feel small.
They are not.
A 2% reduction in body weight during the adaptation phase, while taking a dose that is one-tenth of the maintenance dose, signals that the medication is engaging your appetite regulation pathways correctly. The weight loss accelerates significantly once you reach higher doses, typically between weeks 8 and 20. Month one is the runway, not the takeoff.
The dose escalation schedule and why it matters
Semaglutide follows a carefully designed titration schedule. You do not jump straight to the effective dose. The progression looks like this:
Weeks 1 through 4: 0.25 mg weekly
Weeks 5 through 8: 0.5 mg weekly
Weeks 9 through 12: 1.0 mg weekly
Weeks 13 through 16: 1.7 mg weekly
Week 17 onward: 2.4 mg weekly (maintenance)
This gradual increase exists because GLP-1 receptor agonists can cause significant gastrointestinal side effects when introduced too quickly. The 0.25 mg starting dose allows your body to adjust to the medication with minimal discomfort while still beginning to shift your hunger signals.
Understanding this schedule reframes what month one means. You are on the lowest possible dose for the entire first month. Expecting dramatic results at this dose is like expecting to run a marathon after your first training jog. The foundation matters more than the speed.
How first-month results compare to later months
The weight loss trajectory on semaglutide is not linear. It follows a curve that starts slow, accelerates through months 2 through 6, and then gradually plateaus as you approach your new set point. Here is what the data shows across the full treatment timeline:
Time Period | Average Weight Loss | Dose | Primary Driver |
|---|---|---|---|
Month 1 | 2 to 4% of body weight | 0.25 mg | Appetite adaptation |
Months 2 to 3 | 5 to 8% cumulative | 0.5 to 1.0 mg | Significant appetite suppression |
Months 4 to 6 | 10 to 14% cumulative | 1.7 to 2.4 mg | Full metabolic effects |
Months 7 to 12 | 14 to 17% cumulative | 2.4 mg maintenance | Sustained energy deficit |
The participants in the STEP 1 trial who completed 68 weeks lost an average of 14.9% of their body weight with semaglutide compared to 2.4% with placebo. But the distribution was not even. Some participants lost over 20% of their body weight. Others lost less than 5%. Your first month gives you clues about where you might fall on that spectrum, but it is not the whole story.
What matters most in month one is not the number on the scale. It is the shift in your relationship with food. The reduced appetite. The ability to stop eating when satisfied rather than when the plate is empty. These behavioral changes, driven by semaglutide acting on your brain hunger centers, are the real indicators that the medication is working as designed.
Week 1: the adjustment begins
Your first injection is a milestone. It is also, for most people, somewhat anticlimactic. You push the plunger, apply a bandage, and wait. And then you wait some more.
The pharmacokinetics of semaglutide tell an important story here. After a single subcutaneous injection, semaglutide reaches its peak concentration in your blood between 24 and 72 hours. But that first dose is 0.25 mg, which is genuinely tiny. It takes approximately four to five weeks of consistent dosing for semaglutide to reach steady-state levels in your bloodstream, meaning the drug needs time to accumulate before its full effects emerge.
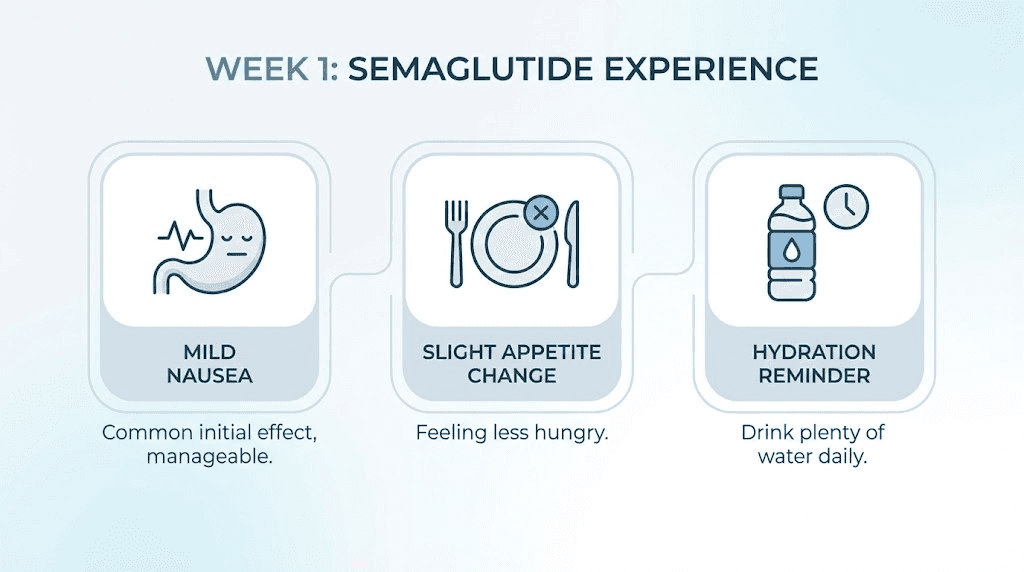
What most people feel in week 1
Appetite changes in the first week are subtle for most people. Some notice a slight decrease in hunger by day 2 or 3. Others feel almost nothing different until later in the month. Both responses are completely normal. The timeline for appetite suppression varies significantly between individuals based on factors like body composition, metabolic rate, and individual receptor sensitivity.
Side effects in week 1 tend to be mild when they appear at all. The most common reports include:
Mild nausea: Approximately 16 to 20% of people experience some nausea in the first week, usually lasting a few hours after injection
Fatigue: Your body is adjusting to eating less, and reduced caloric intake can cause temporary tiredness
Injection site reactions: Minor redness, swelling, or itching at the injection site that typically resolves within 24 hours
Headaches: Often related to mild dehydration as appetite decreases and people forget to drink enough water
Weight change in week 1 is typically minimal. Zero to one pound is the norm. Some people actually see a slight increase due to water retention or the stress response of starting a new medication. Do not panic if this happens. It means nothing about your long-term trajectory.
Week 1 strategies that matter
The decisions you make in week 1 set the tone for your entire first month. Focus on these fundamentals:
Hydration becomes critical. When semaglutide reduces your appetite, it also tends to reduce your natural thirst cues. Aim for at least 64 ounces of water daily, and consider adding electrolytes if you experience headaches or dizziness. Dehydration is the most common preventable side effect trigger in the first week.
Your food choices matter more than food quantity right now. Smaller, more frequent meals reduce nausea risk. Lean proteins, vegetables, and complex carbohydrates are easier to tolerate than heavy, greasy, or highly processed foods. This is not the time for a cheeseburger challenge, even if your appetite seems unchanged.
Track your injection timing relative to your side effects. Many people find that injecting in the evening minimizes daytime nausea because the peak drug concentration occurs during sleep. Others prefer morning injections so they can monitor their response throughout the day. There is no universally correct answer, but finding your optimal injection day and time during week 1 pays dividends for the rest of your treatment.
Week 2: subtle shifts take hold
By the second injection, semaglutide levels in your bloodstream are building. You still have not reached steady state, but the accumulation is enough that most people start noticing genuine changes in their hunger patterns.
The most commonly reported change in week 2 is not weight loss. It is a shift in how food feels. People describe feeling satisfied with smaller portions. The drive to snack between meals diminishes. That nagging background hunger that used to follow you through the afternoon starts to quiet down. These are the GLP-1 receptors in your hypothalamus responding to the medication, slowing gastric emptying and signaling satiety to your brain earlier than your body normally would.
The appetite shift explained
Semaglutide works through multiple mechanisms that all contribute to appetite reduction. Understanding these helps you recognize what is happening in your body during week 2:
Delayed gastric emptying. Food stays in your stomach longer, creating a sustained feeling of fullness. This is why meals that once disappeared in 15 minutes now take 30 to 45 minutes to finish, and why you might feel uncomfortably full if you try to eat at your previous pace.
Central appetite suppression. Semaglutide crosses the blood-brain barrier and acts on GLP-1 receptors in the hypothalamus, the brain region that controls hunger and satiety. This creates a top-down reduction in food-seeking behavior that feels qualitatively different from simply being full. People describe it as food noise turning down, like someone lowered the volume on a constant background craving.
Reduced reward signaling. Early research suggests semaglutide dampens the reward response to highly palatable foods. That slice of cake still tastes good, but the compulsive desire for it, the feeling of needing it, diminishes significantly.
If you are not feeling these effects strongly in week 2, that does not mean the medication is failing. Individual variation in GLP-1 receptor density and sensitivity means some people respond later. The full appetite suppression effect often does not emerge until weeks 3 through 6 for some individuals.
Weight changes in week 2
By the end of week 2, most people have lost between 1 and 3 pounds from their starting weight. Some have lost more, particularly those who had significant water retention before starting. Others hover at zero or show only fractional changes.
A study published in JAMA Network Open found that the rate of weight loss during the dose escalation phase was approximately 0.5% of body weight per week. At a starting weight of 200 pounds, that translates to about 1 pound per week, or roughly 2 pounds by the end of week 2. This aligns with what most people experience, though the range extends from no change to 4 or 5 pounds in either direction.
What you should NOT do in week 2 is drastically cut calories. Your appetite is naturally decreasing, and that caloric reduction is sufficient. Stacking aggressive calorie restriction on top of the medication-induced appetite suppression leads to excessive muscle loss, nutrient deficiencies, and a metabolic slowdown that works against you long term. Let the medication do its job. Eat when hungry, stop when satisfied, and prioritize nutrient-dense foods.
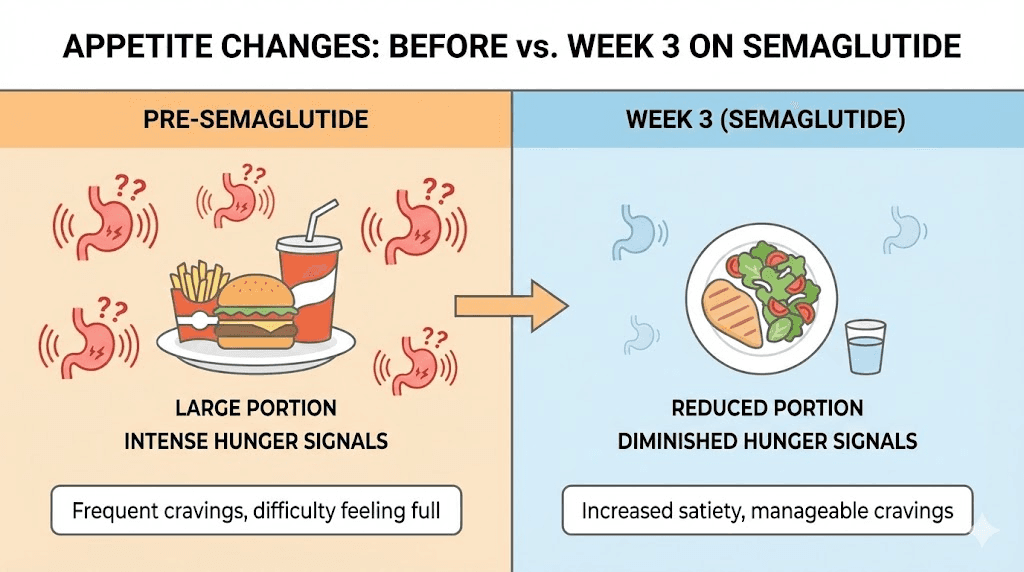
Week 3: the turning point for many
Something changes for most people around week 3. The semaglutide levels in your blood are approaching steady state. The side effects from the initial injection have typically subsided or become manageable. And the appetite changes that were subtle in weeks 1 and 2 become more pronounced.
Week 3 is often when people first say, "I think this is actually working."
The meal sizes shrink noticeably. Where you once ate an entire sandwich, you now eat half and feel done. The evening snacking habit that seemed impossible to break suddenly feels optional. You walk past the break room donuts without the usual internal negotiation. These are not willpower improvements. They are pharmacological effects, the medication changing the signals your brain sends about food.
The emotional component
An underreported aspect of semaglutide at the three-week mark involves the emotional relationship with food. For many people, eating is not just about hunger. It is comfort, stress relief, social bonding, habit, and identity. When semaglutide removes the physical hunger drive, these emotional eating patterns become visible in a way they never were before.
Some people find this liberating. Without the constant pull of physical hunger, they can finally see which eating behaviors are emotional and address them directly.
Others find it unsettling. Food was a coping mechanism, and without the drive to eat, they feel a void they did not expect. This is a normal response and does not mean the medication is wrong for you. It means you are uncovering patterns that were hidden beneath the noise of physical hunger.
SeekPeptides members frequently report that week 3 is when they begin to understand the difference between physical hunger and emotional hunger for the first time. This awareness, more than the weight loss itself, often becomes the most valuable outcome of the first month.
Side effects at week 3
For most people, the initial gastrointestinal side effects have improved significantly by week 3. The nausea that peaked after the first or second injection has typically subsided. Constipation, if it appeared, has either resolved naturally or been managed with increased fiber and targeted interventions.
However, some people develop a new concern around week 3: fatigue. This often results from eating significantly less than before without adjusting hydration, sleep, or protein intake to compensate. The solution is not to eat more just for the sake of calories. Instead, focus on protein-rich meals that sustain energy, adequate hydration, and consistent sleep patterns.
If fatigue persists beyond a few days, check whether you are getting enough protein. A minimum of 0.7 grams per pound of body weight is recommended while on semaglutide to preserve lean muscle mass. For a 180-pound person, that means at least 126 grams of protein daily, which requires intentional effort when appetite is suppressed.
Week 4: your first real checkpoint
Week 4 marks the end of the introductory dose phase. You have completed four injections at 0.25 mg, and your body has had a full month to adapt to semaglutide. This is the point where you take stock of what has happened and prepare for the first dose increase.
Realistic weight loss expectations at day 30
Based on clinical trial data and real-world outcome studies, here is what one month of semaglutide results typically look like:
Starting Weight | Expected Loss (Conservative) | Expected Loss (Average) | Expected Loss (Above Average) |
|---|---|---|---|
150 lbs | 1 to 2 lbs | 3 to 4 lbs | 5 to 7 lbs |
180 lbs | 2 to 3 lbs | 4 to 5 lbs | 6 to 8 lbs |
200 lbs | 2 to 4 lbs | 4 to 7 lbs | 7 to 10 lbs |
220 lbs | 3 to 4 lbs | 5 to 8 lbs | 8 to 12 lbs |
250 lbs | 3 to 5 lbs | 6 to 9 lbs | 9 to 14 lbs |
280 lbs | 4 to 6 lbs | 7 to 10 lbs | 10 to 15 lbs |
These ranges account for the variability seen in clinical practice. The "conservative" column represents the lower end of the data, often seen in people with type 2 diabetes or those who are less responsive to GLP-1 agonists. The "above average" column reflects individuals who respond strongly to appetite suppression and have made concurrent dietary adjustments.
A critical note about the scale. Weight fluctuates daily by 2 to 5 pounds based on water retention, sodium intake, bowel contents, and hormonal cycles. A single morning weigh-in tells you almost nothing. The trend over multiple weeks is what matters. If you weigh 198 pounds on day 1 and 195 pounds on day 30, but you also hit 200 pounds on day 12 and 193 pounds on day 22, your overall trend is downward even though individual data points look chaotic.
Non-scale victories that matter more
The most meaningful first-month results often have nothing to do with the number on the scale. SeekPeptides members consistently report these non-scale changes during their first 30 days:
Portion control becomes automatic. Instead of forcing yourself to stop eating, you naturally lose interest in food midway through a meal. This is the GLP-1 effect working as designed, and it is arguably the most important indicator that semaglutide is effective for you.
Food noise decreases. The constant mental chatter about what to eat next, when to eat, whether you should eat, and guilt about eating fades to a whisper. For people who have spent years battling intrusive food thoughts, this quiet is transformative.
Blood sugar stabilization. Even without significant weight loss, semaglutide improves glycemic control rapidly. People with prediabetes or insulin resistance often notice fewer energy crashes, more stable mood, and reduced afternoon drowsiness within the first two to three weeks.
Reduced cravings for hyperpalatable foods. The pull toward sugary, salty, and fatty foods weakens. Not because you are white-knuckling through willpower, but because the neurological reward pathway that made those foods irresistible has been dampened at the receptor level.
Preparing for the dose increase
At the end of week 4, your dose increases from 0.25 mg to 0.5 mg. This doubling of the dose is the first real step toward the therapeutic range, and it brings both enhanced effects and potential side effect recurrence.
The nausea, constipation, or other gastrointestinal symptoms you experienced in week 1 may return briefly when you increase the dose. This is normal and expected. Your body adapted to 0.25 mg, and now it needs to adapt to 0.5 mg. The adjustment period is typically shorter the second time around, usually lasting 2 to 4 days rather than a full week.
Strategies for a smooth dose transition include:
Continue eating smaller, more frequent meals for the first 3 days after the increase
Stay hydrated, as dehydration amplifies nausea and headache risk
Avoid heavy, high-fat meals on injection day and the following day
Keep ginger tea or ginger supplements on hand for nausea management
Do not skip meals entirely, even if appetite is very low, since some food helps buffer gastrointestinal effects
Why some people lose more in month one and others lose less
The range of first-month results is enormous. Some people step on the scale after 30 days and see 12 pounds gone. Others see 2 pounds. Both can be completely normal responses, but understanding why this variation exists helps you set appropriate expectations and avoid unnecessary frustration.
Factors that accelerate first-month results
Higher starting weight. People with more weight to lose tend to lose more absolute pounds in the first month. This is partly mathematical, since 2% of 280 pounds is more than 2% of 160 pounds, and partly physiological, since larger bodies have more metabolic flexibility.
No diabetes diagnosis. Research published in JAMA Network Open shows that patients without type 2 diabetes lost approximately 6.3% of body weight in the first three months, while those with diabetes lost about 3.9%. Insulin resistance appears to moderate the weight loss response, at least initially.
Concurrent lifestyle changes. People who combine semaglutide with a structured eating plan and regular exercise consistently outperform those who take the medication without changing other behaviors. The STEP 1 trial included lifestyle intervention counseling for all participants, which likely contributed to the strong results.
Strong appetite suppression response. Some people are highly sensitive to GLP-1 receptor agonists. Their appetite drops dramatically from the first dose, naturally creating a large caloric deficit without any conscious effort. If you fall into this category, your first-month results will be above average.
Water weight loss. People who consumed high-sodium diets, carried significant glycogen stores, or had hormonal water retention before starting semaglutide may see a larger initial drop that includes water loss alongside fat loss. This is real weight loss, but the rate will normalize in subsequent months.
Factors that slow first-month results
Type 2 diabetes. As noted above, diabetic patients tend to lose weight more slowly on semaglutide. The medication is still effective, but the timeline extends.
Medications that promote weight gain. If you are taking medications known to cause weight gain, like certain antidepressants, corticosteroids, or insulin, semaglutide has to overcome that pharmacological headwind. Weight loss still happens, but it may start slower.
Previous GLP-1 use. People who have previously used other GLP-1 receptor agonists like liraglutide may have some degree of receptor desensitization. This can moderate the initial appetite suppression effect, though it typically resolves as semaglutide levels build.
Inadequate protein intake. Without sufficient protein, your body loses lean muscle along with fat. Muscle loss does not always show on the scale as dramatically, and it can slow your metabolic rate, reducing the caloric deficit that drives weight loss.
Hormonal factors. Thyroid function, cortisol levels, and reproductive hormones all influence weight loss velocity. Women may notice more week-to-week variability due to menstrual cycle fluid shifts that mask underlying fat loss.
Not tracking accurately. Some people eat more than they realize, especially in the form of liquid calories, cooking oils, or unconscious snacking. While semaglutide reduces appetite, it does not eliminate all eating, and the calories you do consume still count.
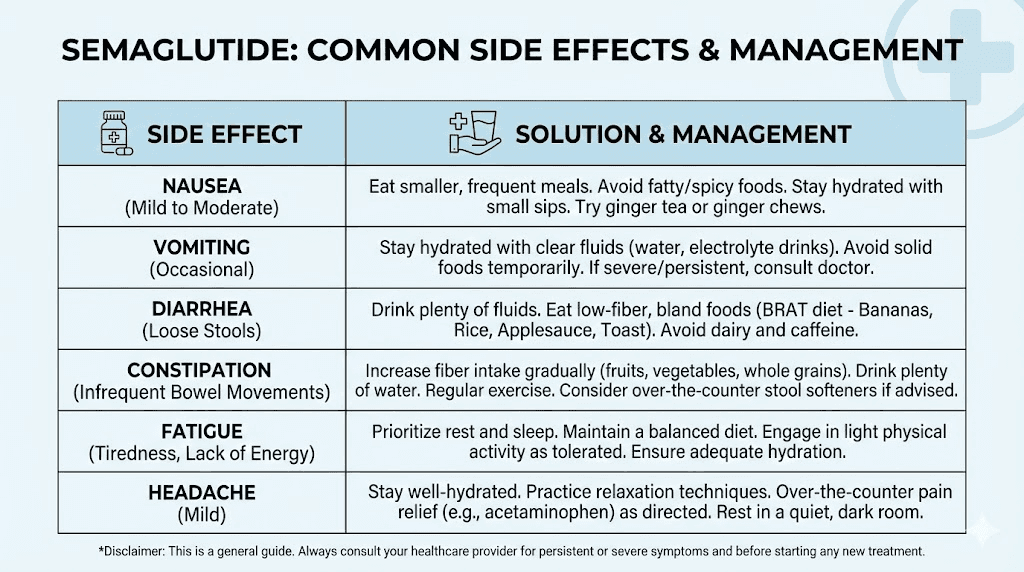
Managing side effects during the first month
Gastrointestinal side effects are the primary complaint during semaglutide initiation. The STEP trials reported nausea in approximately 44% of participants over the full treatment period, with the highest incidence during dose escalation phases. Most first-month side effects are mild to moderate, transient, and manageable with simple strategies.
Nausea management protocol
Nausea is the most common side effect in month one. It typically appears within 24 to 48 hours after injection and lasts anywhere from a few hours to 2 to 3 days. For most people, it resolves by the third injection as the body adapts.
Effective management strategies include:
Meal timing and composition. Eat small portions every 3 to 4 hours rather than 2 to 3 large meals. Prioritize bland, easy-to-digest foods when nausea is present. Rice, toast, bananas, plain chicken breast, and broth-based soups tend to be well tolerated.
Ginger in multiple forms. Ginger has established antiemetic properties. Ginger tea, ginger chews, ginger capsules, or even flat ginger ale can reduce nausea severity. Aim for the equivalent of 1 gram of ginger daily during the first week after each injection.
Peppermint. Peppermint tea or peppermint oil capsules can soothe gastrointestinal discomfort. Some people find that simply inhaling peppermint essential oil during waves of nausea provides temporary relief.
Injection timing optimization. If nausea disrupts your daily activities, try injecting in the evening before bed. The peak drug concentration occurs during sleep, and by morning, the worst of the nausea has often passed. Conversely, if nighttime nausea disrupts your sleep, switch to a morning injection.
Avoid lying flat after eating. This worsens nausea by increasing gastric pressure. Stay upright for at least 30 minutes after meals, especially on injection day.
Constipation solutions
Semaglutide slows gastric emptying, which can extend to the entire digestive tract and cause constipation. This affects roughly 5 to 25% of users in the first month. Unlike nausea, constipation may persist or worsen as doses increase.
Prevention and treatment involve a multi-layered approach:
Fiber intake. Aim for 25 to 35 grams of fiber daily from vegetables, fruits, legumes, and whole grains. If your appetite is too suppressed for that much food, a fiber supplement like psyllium husk can help bridge the gap. Start with a small dose and increase gradually to avoid bloating.
Hydration. Fiber without adequate water makes constipation worse, not better. A minimum of 64 ounces of water daily is essential, and more is better when fiber intake is high. See our complete constipation management guide for detailed protocols.
Movement. Light to moderate physical activity, even a 20-minute walk, stimulates intestinal motility. Sedentary behavior combined with reduced food intake and slowed gastric emptying creates a perfect storm for constipation.
Magnesium supplementation. Magnesium citrate or magnesium oxide at 200 to 400 mg before bed can promote bowel regularity. This also supports sleep quality, which tends to improve weight loss outcomes.
Other first-month side effects
Headaches are common in the first two weeks and almost always resolve with adequate hydration and consistent meal timing. If you skipped breakfast because you were not hungry and then developed a headache by noon, that is a hydration and blood sugar issue, not a dangerous side effect.
Fatigue affects some people during the first month, particularly those who significantly reduce caloric intake without adjusting their nutrient density. Managing semaglutide fatigue involves maintaining adequate protein, staying hydrated, getting 7 to 9 hours of sleep, and not cutting calories below sustainable levels.
Dizziness upon standing can occur due to dehydration or low blood sugar. This is more common in people who skip meals entirely. Eating regular, small meals even when appetite is low helps prevent this.
Injection site reactions like mild redness, swelling, or itching are typically harmless and resolve within 24 to 48 hours. Rotating injection sites between the abdomen, thigh, and upper arm reduces the likelihood of persistent reactions.
Burping and acid reflux can emerge as delayed gastric emptying keeps food in the stomach longer. Eating slowly, avoiding carbonated beverages, and not lying down immediately after meals can minimize these symptoms.
What to eat during your first month on semaglutide
Nutrition during the first month requires a different approach than what most diet plans recommend. Your appetite is changing. Your stomach capacity feels smaller. And your body needs specific nutrients to function well even though you are eating less overall.
Protein: the non-negotiable nutrient
If there is one nutritional priority during your first month on semaglutide, it is protein. Reduced caloric intake combined with weight loss creates a risk of lean muscle loss. Adequate protein intake protects your muscle mass, supports your metabolic rate, and keeps you feeling satisfied with smaller portions.
Target at least 0.7 to 1.0 grams of protein per pound of body weight daily. For a 200-pound person, that means 140 to 200 grams of protein. This sounds like a lot, especially when appetite is suppressed, but it is achievable with strategic food choices:
Greek yogurt (15 to 20 grams per cup)
Eggs (6 grams each)
Chicken breast (31 grams per 4 ounces)
Fish and seafood (20 to 30 grams per serving)
Cottage cheese (14 grams per half cup)
Protein shakes as supplements when solid food is difficult
Eating protein first at every meal ensures you get this critical nutrient even if you cannot finish the entire plate. When your appetite tells you to stop, you want the protein already consumed rather than still sitting on the side.
Foods that minimize side effects
Certain foods work better than others during the semaglutide adaptation period. Your food selection during month one can dramatically influence your comfort level:
Foods that tend to be well tolerated:
Lean proteins (grilled chicken, fish, turkey)
Non-starchy vegetables (broccoli, spinach, zucchini)
Complex carbohydrates in small amounts (sweet potatoes, quinoa, brown rice)
Fresh fruits, especially berries and melons
Broth-based soups
Smoothies with protein powder, greens, and fruit
Foods to approach with caution:
Fried and heavily processed foods (worsen nausea)
High-fat meals (delay gastric emptying further)
Very large portions of anything
Carbonated beverages (increase bloating and burping)
Extremely spicy foods (can aggravate reflux)
Alcohol, especially on an empty stomach
The relationship between semaglutide and alcohol deserves special attention. Many people find their tolerance decreases significantly because food stays in the stomach longer, altering alcohol absorption rates. What used to be two drinks might now feel like four. Caution is warranted, especially during the first month when you are still learning how your body responds.
Meal timing and structure
The traditional three-meals-a-day structure often does not work during semaglutide initiation. Your stomach feels smaller, meals take longer to digest, and the hunger cues you relied on to time your eating may be absent or dramatically reduced.
A more effective approach for month one:
Eat 4 to 5 smaller meals spaced 3 to 4 hours apart. This keeps nutrient intake consistent without overwhelming your slower-moving digestive system. Each meal should be roughly the size of your fist or slightly larger.
Front-load protein. Start every meal with protein before adding vegetables and then carbohydrates. When fullness hits, you want the most critical nutrient already consumed.
Set meal reminders. Without hunger cues prompting you to eat, it is easy to accidentally skip meals and then crash later with fatigue, dizziness, or headaches. Set phone alarms for your meal windows until a new eating pattern establishes itself.
Keep easy protein available. Pre-cooked chicken, hard-boiled eggs, protein bars, and Greek yogurt cups require zero preparation. When appetite is low and motivation to cook is even lower, these grab-and-go options prevent extended periods without food.
Exercise during the first month: how much is too much
Exercise during month one on semaglutide requires a balanced approach. You want to stay active to support weight loss and preserve muscle, but your body is adjusting to reduced caloric intake and a new medication simultaneously. Pushing too hard creates problems. Doing nothing also creates problems.
The right intensity for month one
Walking is the foundation. Aim for 7,000 to 10,000 steps daily, or 30 to 45 minutes of brisk walking. This level of activity supports cardiovascular health, promotes energy levels, stimulates digestion, and burns calories without placing excessive stress on a body that is adapting to eating less.
Strength training 2 to 3 times per week. This is critical for preserving lean muscle mass during weight loss. Focus on compound movements like squats, deadlifts, rows, and presses with moderate weight. You do not need to set personal records this month. The goal is muscle preservation, not muscle building.
Avoid extreme exercise on injection day. Your body is processing the medication, and high-intensity activity combined with potential nausea is a recipe for a miserable workout. Light activity or rest on injection day and the following day is reasonable.
Listen to your body. If fatigue is significant, reduce intensity rather than skipping exercise entirely. A 15-minute walk is infinitely better than doing nothing because a 60-minute gym session feels impossible.
The muscle preservation priority
Research consistently shows that weight loss from GLP-1 receptor agonists includes some lean muscle loss alongside fat loss. The ratio of fat to muscle lost depends heavily on protein intake and resistance training. Without both, up to 40% of weight lost can be lean tissue. With adequate protein and regular strength training, muscle loss can be minimized to less than 15% of total weight lost.
This matters because muscle mass drives your resting metabolic rate. Losing muscle means burning fewer calories at rest, which can lead to faster weight loss plateaus and easier weight regain if you discontinue the medication.
The combination of semaglutide plus resistance training plus adequate protein is the evidence-based trifecta for maximizing fat loss while preserving the metabolic engine that keeps your results sustainable long term.
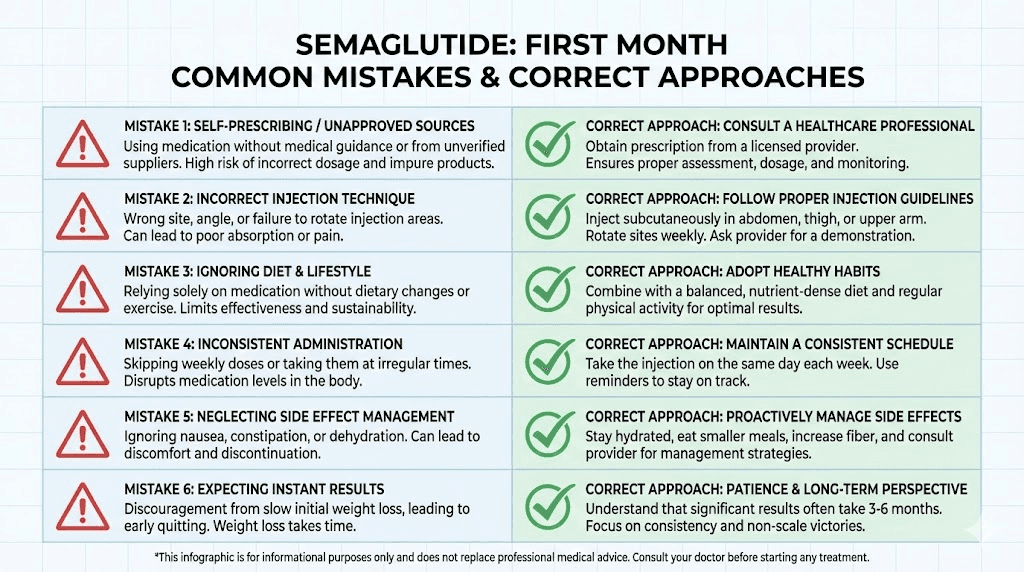
Common mistakes people make in the first month
Certain mistakes show up repeatedly among people starting semaglutide. Avoiding these can significantly improve your first-month experience and set you up for better long-term outcomes.
Mistake 1: obsessing over daily scale readings
The scale lies. Not because it is inaccurate, but because it measures total body weight, which includes water, food in your digestive tract, glycogen stores, and hormonal fluctuations that have nothing to do with fat loss. A person can lose half a pound of fat overnight but gain two pounds of water weight from a salty dinner, and the scale shows a 1.5-pound gain.
Weigh yourself once per week, at the same time, under the same conditions (morning, after using the bathroom, before eating). Better yet, take body measurements with a tape measure. Waist circumference often changes before the scale does.
Mistake 2: eating too little
This sounds counterintuitive for a weight loss medication, but consistently eating under 1,000 calories per day during month one is counterproductive. Extreme caloric restriction triggers metabolic adaptation, increases muscle loss, depletes essential nutrients, and often leads to binge episodes when the restriction becomes unsustainable.
Semaglutide naturally reduces your intake to a sustainable deficit. Trust the process. If the medication is suppressing your appetite to the point where eating feels impossible, focus on calorie-dense, nutrient-rich foods like nuts, avocado, olive oil, and protein shakes to maintain a minimum intake.
Mistake 3: skipping protein
Already covered above, but it bears repeating. Protein is not optional. Without adequate protein, you lose muscle, slow your metabolism, compromise your immune function, and set yourself up for disappointing long-term results. Make protein your number one nutritional priority every single day.
Mistake 4: expecting linear progress
Weight loss does not proceed in a straight line. You will have days where the scale goes up. You will have weeks where nothing changes despite doing everything right. This is normal physiology, not a sign that semaglutide has stopped working.
The trend over 4 to 8 weeks matters. Individual days do not. If your average weight is lower at the end of month one than at the beginning, the medication is working regardless of the ups and downs in between.
Mistake 5: comparing yourself to others
Your coworker lost 15 pounds in her first month. Your neighbor barely lost 3. Social media is full of dramatic transformations that represent outlier results. Your body, your metabolism, your starting point, and your response to the medication are unique. Comparing your week 3 results to someone else's curated highlight reel serves no purpose except to undermine your confidence in a process that takes time.
Mistake 6: discontinuing too early
Some people decide after 4 weeks that semaglutide is not working because they have only lost a few pounds. This is the single most counterproductive decision you can make. The first month is the adaptation phase at the lowest dose. The weight loss accelerates substantially at 0.5 mg, 1.0 mg, and particularly at 1.7 and 2.4 mg. Quitting at 0.25 mg is like leaving a movie after the opening credits and declaring it boring.
Give semaglutide at least 3 to 4 months, through the full dose escalation, before evaluating its effectiveness. The recommended treatment duration is a minimum of 12 to 16 weeks to see meaningful results.
When to be concerned: red flags versus normal adjustment
Most first-month symptoms are normal adaptation responses. But some warrant medical attention. Knowing the difference prevents both unnecessary anxiety and dangerous complacency.
Normal and expected
Mild to moderate nausea for 1 to 3 days after injection
Reduced appetite, even dramatically reduced appetite
Occasional constipation or loose stools
Mild headaches, especially in the first 2 weeks
Mild fatigue during weeks 1 and 2
Injection site redness or mild swelling
Changes in food preferences
Weight fluctuations day to day
Burping or mild acid reflux
Warrants medical attention
Severe, persistent vomiting that prevents you from keeping down fluids for more than 24 hours
Severe abdominal pain that is constant, worsening, or radiating to the back (potential pancreatitis concern)
Signs of dehydration: dark urine, dizziness, rapid heartbeat, confusion
Allergic reactions: hives, difficulty breathing, swelling of face or throat
Gallbladder symptoms: severe upper right abdominal pain, especially after fatty meals
Vision changes in people with diabetes (semaglutide can temporarily worsen diabetic retinopathy)
Significant mood changes: persistent depression, anxiety, or suicidal thoughts
The serious side effects are rare, particularly at the 0.25 mg starting dose. But awareness allows early intervention if they occur. Do not dismiss severe or persistent symptoms as normal adjustment. When in doubt, contact your prescribing physician.
Tracking your progress effectively
What you measure during month one shapes your expectations and your motivation for the months ahead. Most people track the wrong things, or they track the right things in the wrong way.
The metrics that matter
Weekly weight trend. Not daily. Weekly. Weigh yourself every Monday morning under identical conditions and record the number. Then calculate a 4-week average at the end of the month. This smooths out daily fluctuations and gives you a reliable trend.
Body measurements. Waist circumference, hip circumference, and chest measurement, taken once every 2 weeks. These often change before the scale does, especially if you are exercising and building muscle while losing fat.
Appetite rating. On a scale of 1 to 10, rate your hunger level before each meal. Track how this changes over the month. A declining trend in pre-meal hunger ratings confirms that semaglutide is engaging your appetite pathways correctly.
Food journal. Not for calorie counting, but for awareness. Note what you eat, how much, and how you felt afterward. Patterns emerge quickly, like certain foods worsening nausea or specific meal timing reducing fatigue. This information becomes invaluable as you continue treatment.
Side effect log. Note any side effects, their severity (1 to 10), duration, and what helped. This creates a personal database that guides your management strategies and gives your healthcare provider useful information at follow-up appointments.
Energy and mood. A brief daily note about your overall energy level and mood state. These subjective markers often improve before objective weight loss becomes significant, providing early evidence that the medication is working.
Tools and resources for tracking
The GLP-1 plotter tool can help visualize your progress over time. Simple apps like a notes app or a dedicated weight tracking app work well for daily logging. The key is consistency, not complexity. Use whatever tracking method you will actually maintain every day.
A useful approach is the weekly check-in format:
Current weight versus last week
How hunger levels have changed
Side effects experienced and severity
Foods that worked well and foods that did not
Activity level and energy
Overall assessment: better, same, or worse than last week
This structured reflection takes 5 minutes per week and creates a detailed record that shows your trajectory more accurately than any single data point ever could.
Setting expectations for months 2 through 6
Understanding what comes after month one helps you contextualize your first-month results. The trajectory ahead is substantially more dramatic than what you have experienced so far, and knowing that provides patience during the slow start.
Month 2: the acceleration begins
At 0.5 mg, appetite suppression typically intensifies noticeably. Most people report that the appetite effects they experienced at 0.25 mg double or triple in magnitude. Meal sizes shrink further. The window between feeling hungry and feeling full narrows. Weight loss accelerates to 1 to 2 pounds per week for most individuals.
Side effects may briefly return with the dose increase, but they tend to be milder and shorter than the initial onset. Your body has already adapted to semaglutide; it just needs to recalibrate to the higher level.
Month 3: hitting your stride
At 1.0 mg, you are at the lower end of the therapeutic dose range. Many people describe month 3 as the point where semaglutide truly feels like it is working. Weight loss is consistent, appetite management feels natural rather than forced, and the side effects have largely resolved.
By the end of month 3, cumulative weight loss typically reaches 5 to 8% of starting body weight. For a 200-pound person, that is 10 to 16 pounds. The visual changes are becoming noticeable, clothes fit differently, and the feedback loop of results driving motivation begins to turn positive.
Months 4 through 6: maximum velocity
At 1.7 mg and then 2.4 mg, you reach the full maintenance dose. This is where the STEP trial participants achieved their most rapid weight loss. The combination of maximum appetite suppression, optimized gastric emptying delay, and months of accumulated caloric deficit creates a period of significant body composition change.
Monthly weight loss during this phase averages 2 to 3% of body weight, though individual variation remains substantial. By month 6, cumulative losses of 10 to 14% of starting body weight are typical for responsive individuals.
This context matters for your first month because it shows that the slow start is not a failure. It is the beginning of a curve that steepens dramatically. The foundations you build in month one, good eating habits, consistent tracking, effective side effect management, adequate protein intake, determine how well you ride that curve when the acceleration comes.
Compounded semaglutide: does the first month differ
Many people start their semaglutide journey with compounded formulations rather than brand-name Wegovy or Ozempic. The first-month experience with compounded semaglutide has some unique considerations worth understanding.
Compounded semaglutide contains the same active molecule but may differ in concentration, formulation, and the additional ingredients included in the preparation. Some compounding pharmacies add vitamin B12 or glycine to their formulations, which can influence the first-month experience.
The dosing protocol for compounded semaglutide follows the same general escalation pattern, but the concentration of the vial may require different reconstitution procedures and different unit measurements on your syringe. Understanding exactly how to convert milligrams to units for your specific vial concentration is critical for accurate dosing. Mistakes here, taking too little or too much, can significantly alter your first-month experience.
The semaglutide dosage calculator at SeekPeptides helps ensure your dose calculations are accurate regardless of vial concentration. Entering your vial size, concentration, and target dose gives you the exact number of units to draw, eliminating guesswork from the equation.
Storage requirements for compounded semaglutide, once reconstituted, also differ from pre-filled pens. Proper refrigeration and handling are essential for maintaining potency throughout your first month. A vial that has been improperly stored may deliver inconsistent doses, leading to unpredictable results and side effects.
Semaglutide versus tirzepatide: comparing first-month results
If you are deciding between semaglutide and tirzepatide, or if you are curious how your experience compares to people on the other medication, the first-month differences are worth examining.
Tirzepatide is a dual GIP/GLP-1 receptor agonist, meaning it activates two appetite-related receptor pathways compared to semaglutide's one. In head-to-head clinical trials (the SURPASS program), tirzepatide produced greater weight loss than semaglutide at equivalent timepoints.
Metric | Semaglutide (Month 1) | Tirzepatide (Month 1) |
|---|---|---|
Starting dose | 0.25 mg weekly | 2.5 mg weekly |
Average weight loss | 2 to 4% body weight | 3 to 5% body weight |
Appetite suppression onset | Week 1 to 3 | Week 1 to 2 |
Nausea incidence | 16 to 44% | 12 to 24% |
Constipation incidence | 5 to 25% | 6 to 12% |
Time to maintenance dose | 16 weeks | 16 to 20 weeks |
The differences in month one are modest. Both medications are in their introductory dose phase and producing similar adaptation responses. The gap widens significantly at higher doses, particularly at the maintenance doses where tirzepatide's dual mechanism creates more pronounced effects.
For a comprehensive analysis of how these medications compare across all metrics, see our detailed side effect comparison and dosage comparison chart. If you are considering switching between the two medications, understanding the conversion protocols is essential.
The role of lifestyle factors in first-month outcomes
Semaglutide is not a magic injection that works in isolation. The lifestyle context surrounding your first month dramatically influences your results. Two people on identical doses can have vastly different outcomes based on what they do outside of their weekly injection.
Sleep quality
Poor sleep undermines weight loss through multiple mechanisms. It increases cortisol, which promotes fat storage. It disrupts leptin and ghrelin, the hormones that regulate hunger and satiety. It reduces insulin sensitivity. And it depletes willpower, making every food decision harder.
During your first month on semaglutide, prioritize 7 to 9 hours of quality sleep. This means consistent bed and wake times, a dark sleeping environment, no screens for 30 minutes before bed, and avoiding large meals within 2 to 3 hours of sleep.
Stress management
Chronic stress elevates cortisol, which promotes visceral fat storage and increases cravings for high-calorie comfort foods. Even with semaglutide suppressing appetite, stress can override the medication's effects through cortisol-driven metabolic changes.
Simple stress management strategies that support first-month results include daily walks, meditation or deep breathing exercises, limiting news consumption, maintaining social connections, and creating boundaries around work hours.
Hydration
Hydration affects virtually every aspect of your first-month experience. Adequate water intake reduces nausea severity, prevents constipation, supports energy levels, minimizes headaches, and helps your body process the metabolic byproducts of fat breakdown.
The minimum recommendation is 64 ounces daily, but most people on semaglutide benefit from 80 to 100 ounces. If your urine is consistently pale yellow to clear, your hydration is adequate. Dark yellow urine is a signal to drink more.
Social support
Telling at least one trusted person about your semaglutide journey provides accountability, emotional support, and practical help. A partner who understands why you are eating smaller portions is less likely to push food on you. A friend who knows about your side effects can offer encouragement during difficult days.
Online communities can also provide support, though they should be approached with discernment. Not all advice shared in forums is accurate or appropriate for your situation. SeekPeptides provides a community of researchers and users who share evidence-based experiences and protocols, offering more reliable guidance than anonymous social media posts.
Month one for specific populations
Your starting point influences your first-month experience in ways that generic guides rarely address. Here is how different populations tend to respond during the initial 30 days.
People with type 2 diabetes
If you have type 2 diabetes and are starting semaglutide (as Ozempic) for blood sugar management with weight loss as a secondary goal, your first-month trajectory differs from non-diabetic users. Weight loss tends to be slower, averaging about 1 to 2% of body weight in the first month. However, blood sugar improvements are often rapid and significant, with HbA1c reductions beginning within the first few weeks.
Blood sugar monitoring becomes especially important during month one, as semaglutide can cause hypoglycemia when combined with sulfonylureas or insulin. If you are on these medications, your prescriber may need to adjust their doses as semaglutide begins to improve your glycemic control.
Women and hormonal considerations
Women may notice more week-to-week weight variability during the first month due to menstrual cycle fluid shifts. Estrogen and progesterone fluctuations cause water retention patterns that can mask fat loss on the scale. A woman might lose 4 pounds of fat during month one but show only 1 pound of net weight loss because of a 3-pound water retention increase during her luteal phase.
Tracking measurements and considering your cycle phase when interpreting weight data helps avoid discouragement from hormonal water weight. The fat loss is happening even when the scale does not reflect it.
Women who are breastfeeding or pregnant should not use semaglutide. The medication has not been studied in these populations, and the effects on fetal development or breast milk are unknown.
People over 60
Older adults may experience more pronounced side effects during month one, particularly nausea and fatigue, due to naturally slower metabolism and reduced digestive efficiency. Starting at a lower dose or extending the time at 0.25 mg before escalating can help.
Muscle preservation is even more critical for this population, as age-related muscle loss (sarcopenia) compounds the lean tissue loss associated with rapid weight reduction. Higher protein intake (1.0 grams per pound of body weight) and consistent resistance training are non-negotiable for people over 60 using semaglutide.
People with a history of eating disorders
Semaglutide's appetite suppression can interact with disordered eating patterns in complex ways. People with a history of restrictive eating may find the medication triggers familiar patterns of restriction without the normal hunger safeguards. Those with binge eating disorder may experience significant relief as compulsive eating urges diminish.
Medical supervision and mental health support are especially important for this population during month one. The medication changes the physical experience of hunger and fullness, and processing that change within the context of an eating disorder history requires professional guidance.
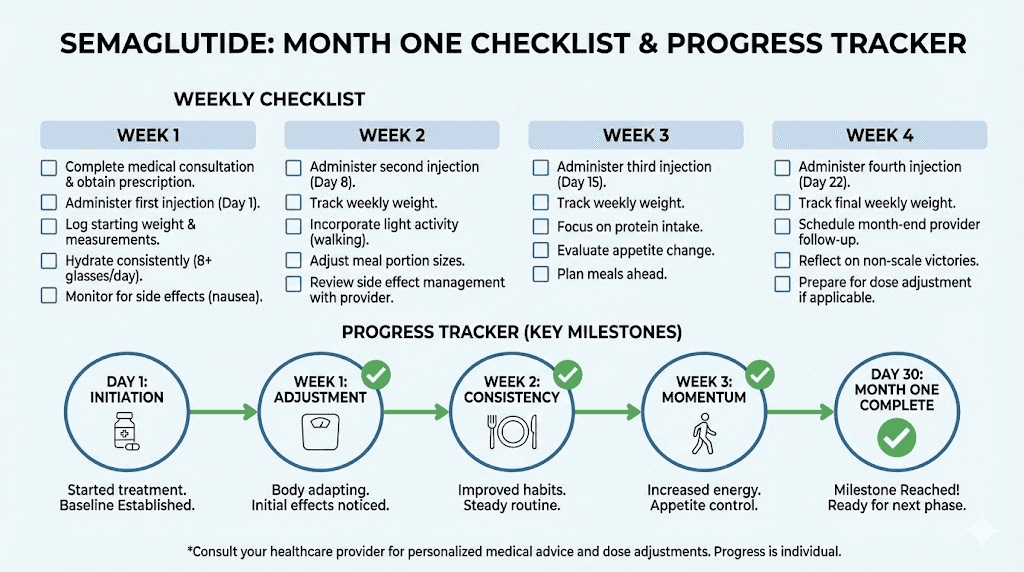
Your month one action plan
Here is a concrete, day-by-day framework for maximizing your first month on semaglutide. This is not theoretical. It is built from clinical protocols and the collective experience of thousands of semaglutide users.
Before your first injection
Take baseline measurements: weight, waist circumference, hip circumference
Photograph yourself (front, side, back) for future comparison
Stock your kitchen with protein-rich, easy-to-prepare foods
Set up your tracking system (app, journal, or spreadsheet)
Record your current appetite level, energy, and any existing health metrics
Choose your injection day and approximate time
Days 1 through 7
Inject your first 0.25 mg dose
Focus on hydration (80 or more ounces of water daily)
Eat small, frequent meals with protein at every one
Note any side effects and their timing relative to injection
Walk 20 to 30 minutes daily
Do not weigh yourself more than once this week
Days 8 through 14
Second injection at 0.25 mg
Continue tracking appetite changes on a 1 to 10 scale
Begin or continue light strength training (2 sessions this week)
Take body measurements
Adjust meal timing based on week 1 observations
Continue hydration and protein priorities
Days 15 through 21
Third injection at 0.25 mg
Notice and record the appetite shifts that typically emerge around this time
Evaluate which foods work best and which cause discomfort
Maintain exercise consistency
Weigh yourself at week 3 and record
Check protein intake and adjust if below target
Days 22 through 30
Fourth injection at 0.25 mg
Complete month-end assessment: weight, measurements, photos
Review your tracking data and identify trends
Prepare for dose increase to 0.5 mg
Stock up on nausea management supplies (ginger, peppermint)
Schedule follow-up with your prescribing physician
Celebrate non-scale victories alongside any weight loss
Frequently asked questions
How much weight should I lose in the first month on semaglutide?
Clinical data shows average first-month weight loss of 2 to 4% of starting body weight. For a 200-pound person, that is roughly 4 to 8 pounds. Results vary based on starting weight, diabetes status, diet quality, and individual medication response. Some people lose more, others less, and both can be normal.
Is it normal to not lose weight in the first month on semaglutide?
Yes. Some people see minimal scale movement during the first month, especially at the 0.25 mg starting dose. The medication is still working, adjusting appetite signals and metabolic processes, but visible weight loss may not appear until the dose increases. See our guide on what to do when semaglutide results seem slow.
When does semaglutide start suppressing appetite?
Most people notice subtle appetite changes within the first 1 to 2 weeks. Significant appetite suppression typically emerges by weeks 2 through 4. The full appetite suppression effect builds over the first 4 to 5 weeks as semaglutide reaches steady-state levels in your bloodstream.
Should I exercise during the first month on semaglutide?
Yes, but at moderate intensity. Walking 30 to 45 minutes daily and strength training 2 to 3 times per week supports fat loss while preserving muscle mass. Avoid extreme exercise during the first week as your body adjusts. Focus on consistency over intensity.
What should I eat during my first month on semaglutide?
Prioritize protein at every meal (0.7 to 1.0 grams per pound of body weight daily), eat smaller and more frequent meals, choose lean proteins and vegetables as the foundation, and avoid high-fat, fried, or heavily processed foods that worsen gastrointestinal side effects. See our complete food guide for semaglutide users.
Will the nausea get better?
For most people, yes. Nausea typically peaks during the first 1 to 2 weeks and gradually diminishes as your body adapts. It may briefly return with each dose escalation but is usually milder and shorter each time. Eating small meals, staying hydrated, and using GI management strategies helps significantly.
Can I drink alcohol during my first month on semaglutide?
Alcohol is not contraindicated, but caution is warranted. Semaglutide slows gastric emptying, which can alter alcohol absorption rates and increase intoxication effects. Alcohol tolerance often decreases on semaglutide. Start with smaller amounts than usual and monitor your response carefully.
When does semaglutide weight loss accelerate?
Weight loss typically accelerates during months 2 through 4 as the dose increases from 0.5 mg to 1.7 mg. The most significant weight loss velocity occurs between months 3 and 6 at the higher therapeutic doses. Full results develop over 12 to 18 months of consistent treatment, as documented in the STEP clinical trial program.
External resources
STEP 1 Trial: Once-Weekly Semaglutide in Adults with Overweight or Obesity (NEJM)
Weight Loss Outcomes Associated with Semaglutide Treatment (JAMA Network Open)
Semaglutide Side Effects and Dosage Information (Mayo Clinic)
Once-Weekly Semaglutide for Weight Management: Clinical Review (PMC)
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, proven protocols, dosage calculators, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay balanced, your progress stay consistent, and your patience stay strong.