Feb 22, 2026

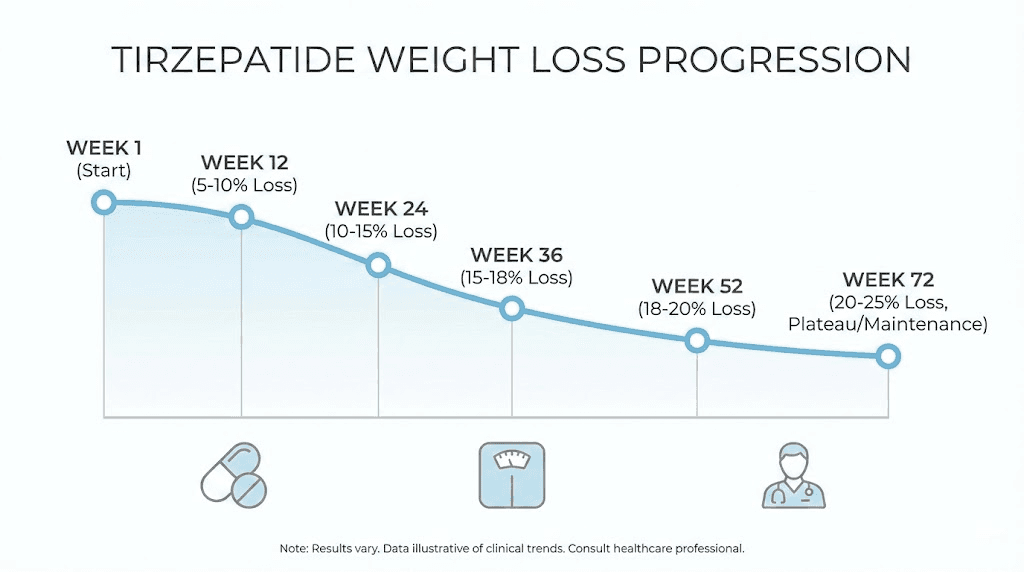
Week one. Nothing happens. Maybe a flicker of reduced appetite, barely noticeable, easy to dismiss. Week four, you step on the scale and the number has shifted. Not dramatically. But enough. By week twelve, people start noticing. Your clothes fit differently. Your face looks leaner. And by month six, you are standing in front of a mirror wondering how this is the same body you started with.
That is the tirzepatide weight loss timeline in broad strokes. But the reality is far more nuanced, more interesting, and more important to understand than any summary can capture. Because what happens between those milestones, the stalls, the surges, the side effects that come and go, the dose adjustments that restart progress, determines whether your experience falls on the exceptional end of the spectrum or the frustrating one.
This guide maps the entire journey. Week by week. Month by month. Drawing from real tirzepatide before and after results, clinical trial data from the SURMOUNT program involving over 5,000 participants, and the accumulated experience of thousands of people who have documented their progress. You will learn exactly what to expect at each phase, what side effects arise and when they resolve, how dose escalation affects the rate of weight loss, and what separates the people who achieve 20%+ body weight reduction from those who plateau early. SeekPeptides has compiled every relevant data point so you can walk into this process with clear expectations rather than hopeful guesses.
How tirzepatide drives weight loss over time
Before mapping the timeline, understanding the mechanism explains why weight loss follows the specific pattern it does. Tirzepatide is a dual GIP and GLP-1 receptor agonist. That means it activates two separate incretin pathways simultaneously, something semaglutide and other GLP-1 only medications do not do. This dual mechanism is precisely why tirzepatide produces greater weight loss than single-receptor drugs in head-to-head comparisons.
The GLP-1 pathway reduces appetite by slowing gastric emptying, signaling fullness to the brain, and reducing food reward pathways. You simply feel less hungry. Food becomes less interesting. The portions that used to seem normal start feeling excessive.
The GIP pathway adds something different. It improves fat metabolism, enhances insulin sensitivity, and appears to influence how the body partitions energy between fat storage and fat oxidation. Working together, these two pathways create a caloric deficit that the body sustains week after week without the metabolic adaptation that typically derails conventional dieting.
This is why the speed of tirzepatide results depends heavily on dose. At the starting dose of 2.5 mg, appetite suppression is mild. As doses increase every four weeks, the effect intensifies. Weight loss accelerates not in a straight line but in a curve, steeper through the middle months, then gradually flattening as the body reaches a new equilibrium.
Understanding this pattern prevents two common mistakes. First, giving up too early because the initial weeks produce modest results. Second, panicking when weight loss slows after month six, mistaking normal deceleration for failure. Both reactions stem from not knowing what the actual timeline looks like.
The dose escalation schedule and why it matters
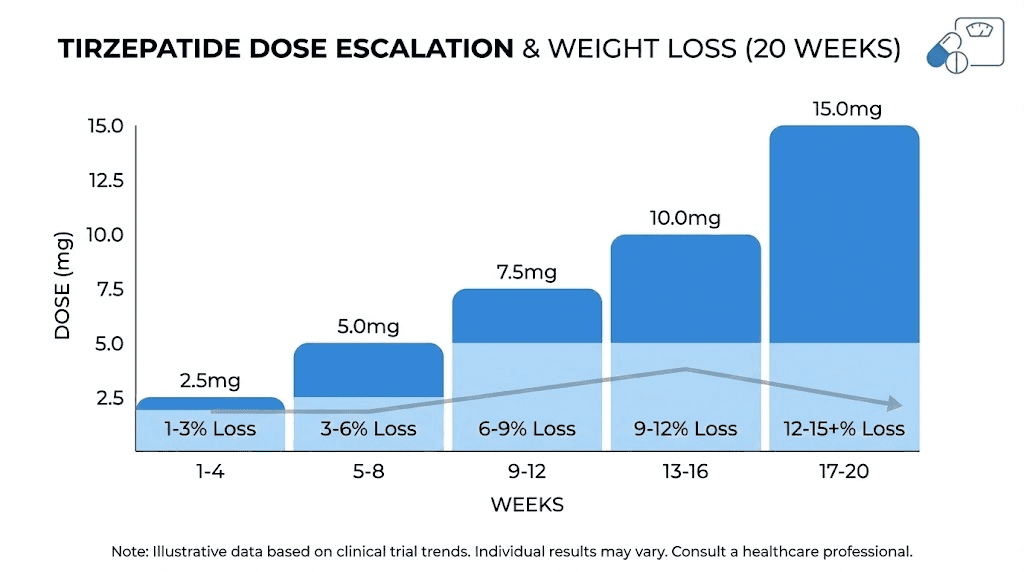
The tirzepatide dosing schedule directly shapes the weight loss timeline. You do not start at the therapeutic dose. Instead, doses increase gradually over a minimum of 20 weeks to reach the maximum, and this escalation period explains why results are modest early on.
Standard FDA-approved escalation
The protocol moves in 2.5 mg increments, each held for at least four weeks:
Weeks 1 to 4: 2.5 mg once weekly (initiation dose, not therapeutic)
Weeks 5 to 8: 5 mg once weekly (first therapeutic dose)
Weeks 9 to 12: 7.5 mg once weekly
Weeks 13 to 16: 10 mg once weekly
Weeks 17 to 20: 12.5 mg once weekly
Week 21 onward: 15 mg once weekly (maximum dose)
Not everyone reaches 15 mg. Some people achieve their goals at 5 mg or 10 mg. Others need the full dose. The tirzepatide dosage calculator can help determine what dose range corresponds to specific weight loss targets, but the body ultimately decides through its response at each level.
This escalation schedule explains a pattern that confuses many people. They hear about 20% weight loss from clinical trials but see only 2-3 pounds drop in the first month. That is completely normal. The 2.5 mg starting dose exists primarily to let the gastrointestinal system adapt, not to drive major weight loss. Real momentum begins at 5 mg and accelerates through 10 mg and 15 mg.
Compounded tirzepatide escalation
For those using compounded tirzepatide, the escalation may look slightly different. Some providers start at lower doses or use smaller increments. The microdosing tirzepatide approach has gained popularity, where people use sub-therapeutic doses initially and increase very slowly. This can reduce side effects but extends the timeline before significant weight loss begins.
Regardless of the specific escalation path, the principle remains. The weight loss timeline is inseparable from the dose timeline. Higher doses produce more appetite suppression, greater caloric deficits, and faster results.
Weeks 1 through 4: the adjustment phase
The first month on tirzepatide is about adaptation, not transformation.
At 2.5 mg, the body is meeting this molecule for the first time. The dual receptor activation begins, but at a level designed to be gentle. Most people notice subtle changes rather than dramatic ones.
What happens in your body
Gastric emptying slows slightly. Food moves through the digestive system more slowly, which creates a mild sense of fullness that lingers longer after meals. Appetite suppression begins within the first week for some people, though others barely notice it at this dose.
Blood sugar levels stabilize. Even in people without diabetes, the improved insulin signaling reduces the energy crashes and cravings that follow high-carbohydrate meals. This effect is subtle but meaningful. You might find yourself reaching for snacks less often without consciously deciding to eat less.
Weight loss expectations
Realistic week one through four weight loss: 0 to 4 pounds.
Some people lose nothing. Others drop 3 to 4 pounds, mostly from reduced food intake and some water weight redistribution. Clinical trial data from SURMOUNT-1 shows that the 2.5 mg dose produces minimal weight reduction on its own, which is expected since this dose is specifically labeled as an initiation dose rather than a maintenance dose.
Do not compare your first month to someone else who is three months in at 10 mg. That comparison is meaningless and discouraging. The time it takes for tirzepatide to work varies based on individual metabolism, starting weight, and dose progression.
Common side effects
The most common experience during weeks one through four involves gastrointestinal adjustment. Mild nausea affects roughly 12 to 24 percent of people, depending on individual sensitivity. This usually peaks one to two days after each injection and fades as the week progresses.
Other possible effects include:
Mild diarrhea that typically resolves within days
Headaches as the body adjusts to changed blood sugar patterns
Slight bloating or a feeling of food sitting in the stomach longer than usual
Fatigue in the first few days after injection
These side effects are transient. Most resolve within the first two to three weeks. Eating smaller, lighter meals and avoiding foods that worsen GI symptoms helps considerably.
Weeks 5 through 8: the first therapeutic dose
This is where things start to change.
At 5 mg, tirzepatide reaches its first therapeutic dose. The appetite suppression becomes more noticeable. Food interest drops more clearly. Portions shrink naturally, not because you are forcing willpower, but because your brain is receiving stronger satiety signals.
What changes at 5 mg
The shift from 2.5 mg to 5 mg represents a meaningful jump in pharmacological effect. GLP-1 receptor activation increases, further slowing gastric emptying. GIP receptor signaling strengthens, improving how the body handles dietary fat and glucose. Together, these changes create a more pronounced caloric deficit.
Most people notice they can eat about half to two-thirds of what they previously consumed before feeling full. The desire for seconds disappears. Late-night snacking drops off dramatically. What you eat on tirzepatide matters more now, because the reduced volume of food means every meal needs to deliver adequate nutrition in a smaller package.
Weight loss expectations
Cumulative weight loss by week eight: 3 to 8 pounds for most people.
The SURMOUNT-1 trial showed approximately 3 to 4 percent body weight loss by week eight across all dose groups. For someone starting at 250 pounds, that translates to roughly 7 to 10 pounds. For someone starting at 180 pounds, expect 5 to 7 pounds.
The rate typically accelerates compared to the first month. You might see 1 to 2 pounds per week at this stage, though weight loss is rarely linear. Some weeks bring 3-pound drops. Others show no movement at all. The GLP-1 plotter tool can help visualize this non-linear pattern and set realistic expectations.
Side effects at this dose
People who tolerated 2.5 mg well usually handle 5 mg without major issues. Those who experienced nausea at the initial dose may see a brief return of symptoms when stepping up, typically lasting two to three days. Comparing tirzepatide side effects to semaglutide, many users report that tirzepatide produces somewhat less nausea at equivalent efficacy levels, likely due to the dual-receptor mechanism distributing the physiological burden across two pathways.
This is a good time to establish nutrition habits that will serve you throughout the process. A tirzepatide diet plan focused on protein, fiber, and nutrient density helps maintain lean mass while the caloric deficit does its work.
Weeks 9 through 12: visible momentum
Three months in. This is typically when progress becomes visible to other people.
At 7.5 mg (or continuing at 5 mg if that dose is sufficient), the pattern established in the previous phase intensifies. Appetite suppression is now a consistent daily experience. You are eating less without struggling. The caloric deficit accumulates into meaningful body composition changes.
The three-month milestone
Clinical data from the SURMOUNT-1 trial reveals a critical finding about the twelve-week mark. Researchers categorized participants as either early responders (5% or more weight loss by week twelve) or late responders (less than 5% weight loss by week twelve). Both groups ultimately achieved clinically meaningful results, but the trajectory differed.
Early responders had already lost 5 to 8 percent of body weight by week twelve. They were clearly on an accelerating path. Late responders had lost less than 5 percent but, crucially, 90 percent of them went on to achieve 5 percent or greater weight loss by week 72. The lesson: being a slow starter does not predict a poor final outcome.
Weight loss expectations
Cumulative weight loss by week twelve: 5 to 12 percent of starting body weight for most people.
At 250 pounds starting weight, that means roughly 12 to 30 pounds lost. At 180 pounds, roughly 9 to 22 pounds. The range is wide because individual variation is significant at this point. Factors like starting BMI, metabolic health, activity level, and dietary choices all influence the rate.
This is also when the tirzepatide before and after transformations start becoming photographic. Faces look thinner. Waistlines shrink noticeably. Clothes that were tight now fit comfortably or become loose.
Body composition at three months
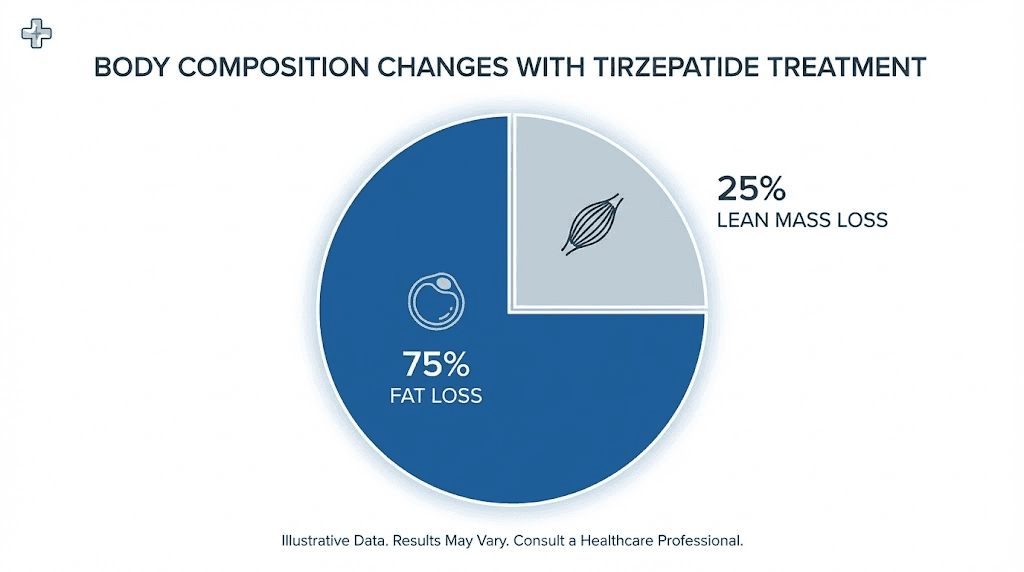
Research from the SURMOUNT-1 body composition sub-study shows that by twelve weeks, approximately 75 percent of weight lost is fat mass and 25 percent is lean mass. This ratio holds remarkably consistent across all dose groups and is comparable to what occurs with any form of caloric restriction, whether pharmaceutical or dietary.
To minimize lean mass loss, supplementing with key nutrients while on tirzepatide becomes important. Protein intake should stay at 0.7 to 1.0 grams per pound of target body weight. Resistance training helps preserve muscle. Protein shakes designed for GLP-1 users can make hitting protein targets easier when appetite is significantly reduced.
Weeks 13 through 20: peak acceleration
This is where tirzepatide earns its reputation.
Months four and five represent the steepest portion of the weight loss curve for most people. Doses are climbing through 10 mg, 12.5 mg, and potentially reaching 15 mg. Appetite suppression is at or near its maximum. The caloric deficit is substantial. And the body has not yet fully adapted its metabolic rate to the lower caloric intake.
The accelerating curve
Between weeks 13 and 20, many people experience their fastest rate of weight loss on the entire tirzepatide journey. The tirzepatide dosing for weight loss conversion shows that the jump from 7.5 mg to 10 mg, and then to 12.5 mg, produces meaningful increases in appetite suppression and energy expenditure.
Weekly weight loss of 2 to 3 pounds is common during this phase. Some weeks bring even more. The body is responding to both the increasing dose and the cumulative metabolic effects that have been building since week one.
But not every week is a winner. Stalls happen. Water retention masks fat loss. Hormonal fluctuations in women can cause the scale to jump up temporarily. Tirzepatide can affect menstrual cycles, which in turn affects water retention and scale weight. The trend matters more than any single weigh-in.
Weight loss expectations
Cumulative weight loss by week twenty: 10 to 18 percent of starting body weight.
For a person who started at 250 pounds, this means roughly 25 to 45 pounds lost. For someone at 200 pounds, roughly 20 to 36 pounds. These numbers align with the SURMOUNT trial data, which showed that the steepest decline in body weight occurs between months three and six.
Managing the dose increases
Each dose increase can bring a brief return of gastrointestinal side effects. Nausea that had resolved at 7.5 mg may reappear for two to three days at 10 mg. Body aches and sleep disturbances occasionally occur during dose transitions. These are typically mild and resolve within the first week at the new dose.
Timing your injection strategically helps. Many people find that injecting on a day when they can afford to eat lightly and rest minimizes the impact. The best time to take your GLP-1 shot depends on your schedule, but consistency matters more than the specific day.
Proper injection technique also affects tolerability. Subcutaneous injection into the abdomen, thigh, or upper arm should rotate sites weekly to prevent lipodystrophy and ensure consistent absorption. For detailed injection guidance, the injection site guide covers best practices.
Nutritional priorities during peak loss
During this rapid loss phase, nutritional quality becomes critical. The body is shedding weight quickly, and without adequate nutrition, you risk excessive lean mass loss, micronutrient deficiencies, fatigue, and hair thinning that sometimes accompanies GLP-1 medications.
A structured tirzepatide meal plan should prioritize:
80 to 120 grams of protein daily (minimum)
Adequate hydration (at least 64 ounces of water)
Fiber from vegetables and whole grains
A quality multivitamin to cover micronutrient gaps
Omega-3 fatty acids for metabolic support
The tirzepatide with B12 combination has become popular because B12 supports energy production, which can offset the fatigue some people experience during rapid weight loss. Glycine and B12 compound formulations offer additional benefits for metabolism and liver health.
Weeks 21 through 36: sustained progress and potential plateaus
By week 21, most people have reached or are approaching their maximum dose. The question shifts from escalation to maintenance and optimization.
What the SURMOUNT data shows
The SURMOUNT-1 trial at the 36-week mark shows average weight loss of approximately 15 to 17 percent of body weight on the 10 mg and 15 mg doses. The SURMOUNT-4 trial, which used an open-label design, showed a mean weight reduction of 20.9 percent after 36 weeks of maximum dose treatment.
These numbers are averages. Some people exceed them significantly. Others fall below. The variance is normal and expected.
Weight loss expectations
Cumulative weight loss by week 36: 15 to 22 percent of starting body weight for those on higher doses.
For a 250-pound starting weight: 37 to 55 pounds lost. For 200 pounds: 30 to 44 pounds lost. At this point, the change is dramatic. Most people have dropped multiple clothing sizes. Health markers, including blood pressure, blood sugar, cholesterol, and inflammatory markers, have typically improved substantially.
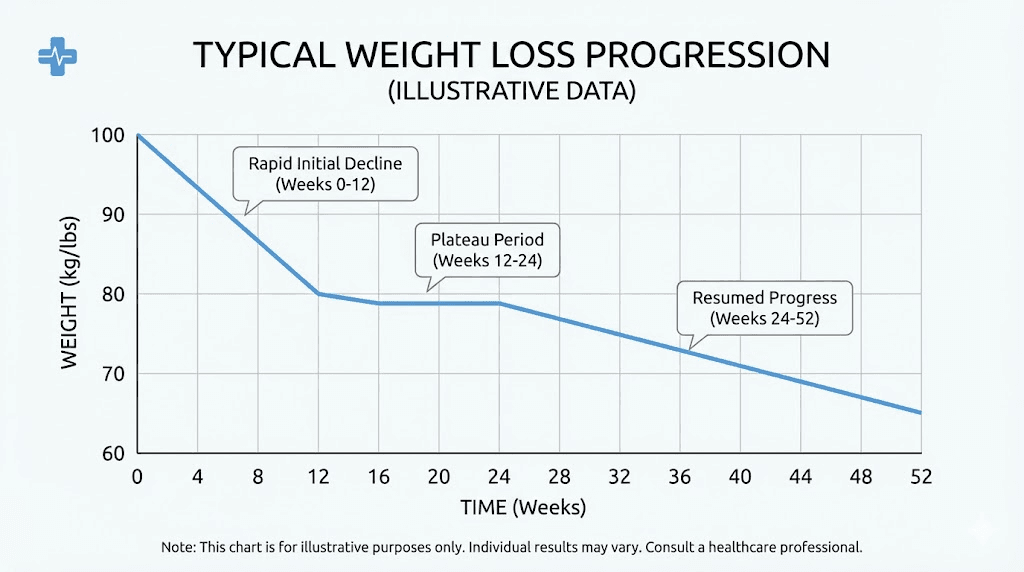
The plateau phenomenon
Somewhere between weeks 24 and 36, many people encounter their first significant plateau. Weight loss slows markedly or stops entirely for two to four weeks, sometimes longer. This is one of the most psychologically challenging parts of the journey, and understanding why it happens is essential.
The plateau occurs because the body has adapted. Resting metabolic rate decreases as body weight drops. The same dose of tirzepatide produces the same appetite suppression, but the caloric deficit narrows because a lighter body needs fewer calories. The math changes.
This does not mean tirzepatide has stopped working. It means the body has reached temporary equilibrium between caloric intake and expenditure. The sense that tirzepatide is no longer working is almost always this metabolic adaptation rather than medication failure.
If you find yourself in this position, the troubleshooting guide for tirzepatide weight loss stalls covers the most common causes and solutions. Often, small adjustments, adding resistance training, increasing protein, improving sleep quality, or a dose adjustment, restart the process.
Weeks 37 through 72: the long game
Most articles about tirzepatide stop at six months. The real story continues well beyond that.
The SURMOUNT-1 trial ran for 72 weeks, and the data from this extended period reveals something important. Weight loss continues, albeit more slowly, for most people well past the six-month mark. The curve flattens but does not go to zero.
Weight loss between months 9 and 18
After the initial rapid phase, weight loss settles into a slower, steadier rhythm. One to two pounds per month is typical during this period. That sounds modest, but it adds up. Over twelve months of slow loss, that is an additional 12 to 24 pounds on top of what was already achieved.
The SURMOUNT-1 final results at 72 weeks showed mean weight loss of:
5 mg dose: 16.0 percent of body weight
10 mg dose: 21.4 percent of body weight
15 mg dose: 22.5 percent of body weight
For context, 22.5 percent of 250 pounds is 56 pounds. That is transformative. And many participants lost more than the average.
Body composition at 72 weeks
The extended body composition data is encouraging. The fat-to-lean mass ratio improved from 0.93 at baseline to 0.70 at week 72 in the tirzepatide group, compared to 0.95 to 0.88 in the placebo group. This means tirzepatide preferentially improves body composition, shifting the ratio in favor of lean mass even as total weight decreases.
Studies examining muscle quality using MRI found that tirzepatide significantly reduced muscle fat infiltration, meaning the muscle that remains is leaner and healthier than before. Muscle-related concerns on tirzepatide are valid but often overstated. The lean mass loss that occurs is proportionally similar to any weight loss method. Resistance training and adequate protein can minimize it substantially.
When does weight loss actually stop?
Research suggests that most people on tirzepatide reach weight stability between 36 and 72 weeks. People with higher starting BMIs tend to continue losing longer. Those with lower starting BMIs plateau sooner.
The plateau is not failure. It is the body finding a new set point with the medication on board. At this stage, the goal shifts from weight loss to weight maintenance, body composition optimization, and health marker improvement.
What happens if you stop tirzepatide
The SURMOUNT-4 trial directly addressed this question, and the answer is sobering but important to understand upfront.
After 36 weeks of open-label tirzepatide treatment producing an average 20.9 percent weight loss, participants were randomized to either continue tirzepatide or switch to placebo. The results were stark. Among those who continued tirzepatide, 89.5 percent maintained at least 80 percent of their weight loss. Among those switched to placebo, only 16.6 percent maintained that level.
Weight regain after discontinuation is not a personal failure. It is biology. The appetite suppression, improved insulin signaling, and metabolic benefits of tirzepatide require ongoing medication to sustain. This is consistent with how we understand obesity as a chronic condition requiring chronic treatment, similar to how blood pressure medication manages hypertension rather than curing it.
For this reason, understanding the long-term treatment commitment is essential before starting. Many people plan from the beginning to use tirzepatide indefinitely at a maintenance dose, often lower than the maximum dose used during the active weight loss phase.
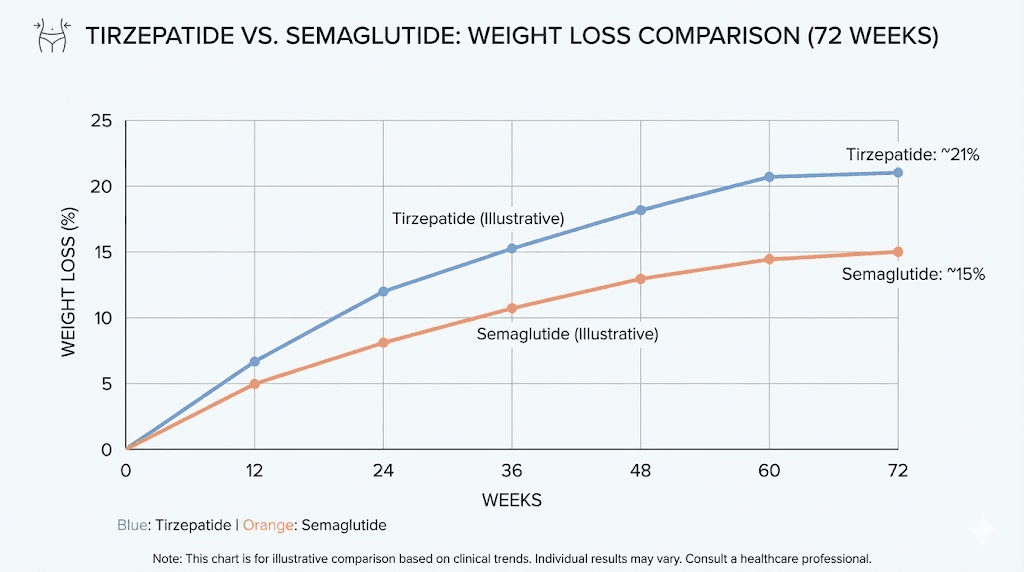
Tirzepatide versus semaglutide: timeline comparison
Many people considering tirzepatide want to know how its timeline compares to semaglutide, the other major GLP-1 medication. The comparison is instructive.
Speed of initial weight loss
Both medications show similar initial timelines. Semaglutide starts working within the first one to two weeks with appetite suppression, and meaningful weight loss begins around weeks four to eight. Tirzepatide follows a similar early pattern.
The divergence appears after month three. Tirzepatide produces consistently greater weight loss than semaglutide at every timepoint measured. By 72 weeks, the difference is substantial: 22.5 percent body weight loss for tirzepatide 15 mg versus approximately 15 to 16 percent for semaglutide 2.4 mg.
Side effect timeline comparison
The side effect profiles differ slightly between the two medications. Both cause gastrointestinal symptoms primarily during dose escalation. Tirzepatide has a longer escalation period (20 weeks to maximum versus 16 weeks for semaglutide), which means the GI adjustment period extends over more time but may be less intense at each step.
For people who have tried semaglutide and want to understand the transition, the semaglutide to tirzepatide conversion chart provides dose equivalency guidance. Switching between the two medications is possible but requires careful dose management.
Timepoint | Tirzepatide (15 mg) | Semaglutide (2.4 mg) |
|---|---|---|
Week 4 | 1-2% body weight | 1-2% body weight |
Week 12 | 5-8% body weight | 5-6% body weight |
Week 24 | 12-17% body weight | 10-13% body weight |
Week 36 | 17-21% body weight | 13-15% body weight |
Week 72 | 20-22.5% body weight | 15-16% body weight |
The advantage of tirzepatide becomes more pronounced over time. By one year, it has produced roughly 40 to 50 percent more weight loss than semaglutide. This is the benefit of dual-receptor agonism.
Factors that speed up or slow down your timeline
No two people follow the same tirzepatide weight loss timeline. Understanding what accelerates or decelerates the process helps set realistic expectations and identify areas for optimization.
Factors that accelerate weight loss
Higher starting BMI. People with more weight to lose typically lose faster, especially in the first six months. A person starting at 300 pounds will almost certainly lose weight faster than someone starting at 200 pounds. The absolute numbers are larger, and the metabolic effects of the medication have more substrate to work with.
Reaching higher doses. The relationship between dose and weight loss is clear in clinical data. Those who tolerate and remain on 15 mg lose more than those who stay at 5 mg. If your provider recommends dose escalation and you tolerate it, the higher doses produce better outcomes.
Adequate protein intake. This seems counterintuitive, eating more of something does not sound like a weight loss strategy. But adequate protein preserves lean mass, maintains metabolic rate, improves satiety, and supports the thermogenic effect of food. The foods that work best with GLP-1 medications are consistently protein-rich and nutrient-dense.
Resistance training. Exercise does not drive weight loss directly (the caloric deficit from tirzepatide does the heavy lifting), but resistance training preserves lean mass, increases resting metabolic rate, and prevents the metabolic slowdown that causes plateaus. Even two sessions per week makes a measurable difference.
Quality sleep. Poor sleep increases ghrelin (hunger hormone), decreases leptin (satiety hormone), and promotes insulin resistance. All of these work against tirzepatide. Seven to nine hours of quality sleep amplifies the medication effects.
Factors that slow weight loss
Alcohol consumption. Drinking on tirzepatide is not prohibited, but alcohol provides empty calories, impairs judgment around food choices, disrupts sleep, and slows fat oxidation. Even moderate drinking can meaningfully slow the timeline.
Inadequate protein. When protein intake drops below 0.5 grams per pound of body weight, the body breaks down muscle tissue for amino acids. This accelerates lean mass loss, slows metabolism, and can cause the scale to stall as the body resists further muscle depletion.
Certain medications. Some medications promote weight gain or interfere with the metabolic effects of tirzepatide. Beta blockers, certain antidepressants, corticosteroids, and insulin can all slow the weight loss timeline. Combining tirzepatide with other weight loss medications like phentermine is an option some providers use to accelerate results, though this should only be done under medical supervision.
Chronic stress. Elevated cortisol promotes visceral fat storage, increases appetite for calorie-dense comfort foods, and disrupts sleep. Stress management is an underappreciated component of the weight loss timeline.
Irregular injection timing. Taking tirzepatide early or late occasionally is fine, but consistently irregular dosing leads to fluctuating drug levels, inconsistent appetite suppression, and suboptimal results. Keeping a consistent weekly schedule maximizes the steady-state drug concentration.
Side effects timeline: when they start and when they stop
Side effects follow their own timeline, and knowing when to expect what reduces anxiety and prevents premature discontinuation.
Week 1 through 4 side effects
Mild nausea (12 to 15 percent of users), occasional diarrhea, and headaches. These are the most common early side effects and typically resolve within two to three weeks.
Dose escalation side effects (recurring)
Each dose increase can bring a brief return of GI symptoms. This is normal and expected. The body adapts to each new dose within one to two weeks. The side effects at higher doses are not necessarily worse than at lower doses, just recurring.
Month 2 through 4 side effects
Fatigue can occur as the body adjusts to significantly reduced caloric intake. This is not the medication itself causing tiredness but rather the energy deficit. Adequate protein, hydration, and micronutrient supplementation usually resolve this. Some people actually report increased energy as weight drops and metabolic health improves.
Constipation becomes more common as appetite drops and food volume decreases. Less food means less fiber, less bulk, and slower transit. Increasing water intake, adding a fiber supplement, and incorporating vegetables at every meal prevents this in most cases.
Month 4 through 6 side effects
By this point, most GI side effects have resolved. The body has adapted to both the medication and the new eating patterns. Hair thinning may become noticeable around months four to six, a result of the caloric deficit and rapid weight loss rather than a direct drug effect. This is usually temporary and resolves as weight stabilizes.
Mood changes are occasionally reported, ranging from mild anxiety to changes in emotional eating patterns. For people who used food as an emotional coping mechanism, the loss of that outlet can create psychological adjustment challenges that deserve attention.
Long-term side effect profile
After six months, the side effect profile stabilizes significantly. Most people are on their maintenance dose, the body has fully adapted, and the remaining experience is primarily the therapeutic benefit (reduced appetite, ongoing weight loss or maintenance) without the adjustment symptoms.
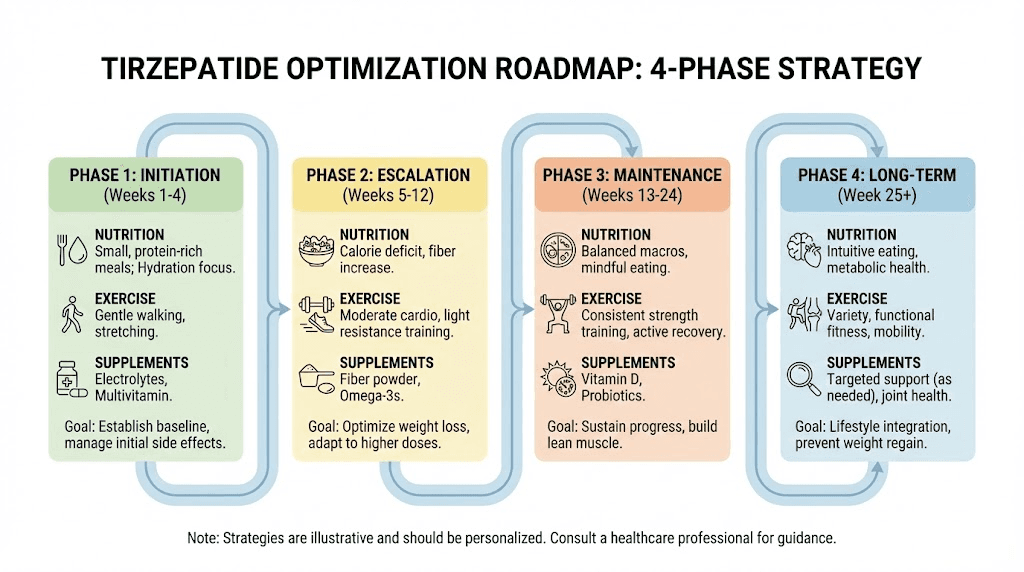
Optimizing results at each phase of the timeline
Knowing what to do at each stage of the tirzepatide weight loss timeline maximizes outcomes and minimizes setbacks.
Phase 1: weeks 1 through 8 (build the foundation)
Focus on establishing habits rather than chasing scale numbers.
Nutrition: Begin tracking protein intake. Aim for at least 80 grams daily. Start each meal with protein. Cut back on fried foods, heavy sauces, and large portions that exacerbate GI side effects. The foods to avoid on tirzepatide include greasy meals, carbonated drinks, and high-sugar items that worsen nausea and bloating.
Exercise: Start or maintain a basic exercise routine. Walking 30 minutes daily is sufficient. Do not launch into intense training while your body is still adjusting to the medication.
Mindset: Accept that weight loss will be modest during this phase. The medication is building in your system, your body is adapting, and the dose is not yet at a therapeutic level. Patience here pays off later.
Phase 2: weeks 9 through 20 (ride the wave)
This is the acceleration phase. Lean into it.
Nutrition: Increase protein to 100 to 130 grams daily. Add key supplements including a multivitamin, omega-3, vitamin D, and magnesium. Consider a glycine supplement or glycine-enhanced formulation for liver support during rapid fat mobilization.
Exercise: Add resistance training two to three times per week. This is non-negotiable for preserving lean mass during rapid weight loss. Compound movements (squats, deadlifts, rows, presses) are most effective. Even bodyweight exercises provide meaningful stimulus.
Tracking: Take measurements (waist, hips, chest, thighs) in addition to weighing. During rapid loss, the scale can temporarily stall while body composition continues improving. Measurements and progress photos capture what the scale misses.
Phase 3: weeks 21 through 36 (push through plateaus)
Plateaus are expected. Strategies to break them:
Caloric cycling: Instead of eating the same amount every day, vary intake. Slightly higher on training days, slightly lower on rest days. This prevents the metabolic adaptation that causes stalls.
Increase activity variety: If you have been only walking and doing weights, add interval training once weekly. The metabolic stimulus from high-intensity work can restart stalled weight loss.
Review medication adherence: Ensure injections are given at consistent times, properly stored (tirzepatide storage requirements must be followed), and that the medication has not expired.
Consider dose adjustment: If you are not yet at the maximum dose and have hit a plateau, a dose increase often restarts weight loss. Discuss this with your provider.
Phase 4: weeks 37 and beyond (maintain and optimize)
Long-term success requires shifting from a weight loss mindset to a health optimization mindset.
Focus on body composition: The scale matters less than how your body looks, feels, and functions. Continue resistance training. Prioritize protein. Consider using a DEXA scan to track body composition changes directly.
Maintain the medication: Do not discontinue abruptly. If cost is a concern, discuss dose reduction with your provider. Affordable tirzepatide options exist, including compounded formulations that cost significantly less than brand-name versions. The microdose tirzepatide maintenance approach is something some people use successfully at lower ongoing doses.
Monitor health markers: Regular blood work to track metabolic health, thyroid function, liver enzymes, and nutrient levels ensures the weight loss is producing health benefits and not creating new problems.
Special populations and timeline variations
The standard timeline applies to most people, but certain populations experience different patterns.
Men versus women
Men typically lose weight faster than women on tirzepatide, particularly in the first six months. This mirrors general weight loss patterns and relates to differences in lean mass, metabolic rate, and hormonal environment. The men before and after tirzepatide results often show larger absolute numbers but similar percentage losses when adjusted for starting weight.
Women face additional variables. Menstrual cycle fluctuations cause temporary weight increases that mask fat loss. Tirzepatide affects menstrual timing and flow for some women, adding another layer of complexity to tracking progress. Women approaching or in menopause face unique challenges with weight loss that require adjusted expectations.
Higher starting BMI
People with a BMI above 40 tend to lose weight faster in absolute terms and sustain the loss trajectory longer before plateauing. The SURMOUNT data shows that the plateau occurs later for higher BMIs, sometimes not until month eight or nine rather than month six. Total percentage weight loss is also often higher.
People with type 2 diabetes
Those with type 2 diabetes typically lose weight more slowly on tirzepatide than non-diabetic users. The SURPASS trials (studying tirzepatide for diabetes) showed approximately 5 to 13 percent weight loss over 40 to 52 weeks, compared to 16 to 22.5 percent in the SURMOUNT obesity trials. Insulin resistance and diabetes medications can affect the rate of weight loss.
Transitioning from semaglutide
People who switch from semaglutide to tirzepatide after a plateau often experience renewed weight loss. The conversion chart for switching helps ensure an appropriate starting dose. Many experience an additional 5 to 10 percent body weight loss after switching, though the timeline for this additional loss varies.
How to track your personal timeline
Knowing the general timeline is valuable. Tracking your specific progress is essential.
What to measure and when
Weekly: Body weight (same day, same time, same conditions). Record it but do not react to single data points. The GLP-1 plotter can help visualize the trend line rather than fixating on daily or weekly fluctuations.
Biweekly: Body measurements (waist, hips, chest, thighs, arms). These catch changes the scale misses, especially during periods of body recomposition where fat loss coincides with lean mass preservation.
Monthly: Progress photos (front, side, back, in same lighting and clothing). The mirror lies because it shows you the same image you see every day. Monthly comparison photos reveal changes that daily observation cannot detect.
Quarterly: Blood work (comprehensive metabolic panel, lipids, HbA1c, thyroid, vitamin D, B12, iron). These health markers tell the deeper story of what the weight loss is doing for your metabolic health.
When to be concerned versus patient
Normal: Two to three weeks with no scale movement. This is common and typically followed by a sudden drop (often called the "whoosh effect").
Worth investigating: Four or more weeks with zero scale movement AND no measurement changes. Review medication storage, injection technique, dietary intake (calorie creep is real), and sleep quality.
Discuss with provider: Consistent weight gain despite good adherence to medication and nutrition. This could indicate a thyroid issue, medication interaction, or need for dose adjustment.
Comparing tirzepatide to other weight loss approaches
Understanding where tirzepatide fits in the broader landscape of weight loss interventions helps frame expectations appropriately.
Tirzepatide versus diet and exercise alone
Conventional diet and exercise typically produces 5 to 8 percent body weight loss over six months. Tirzepatide produces 15 to 22.5 percent over the same period. More importantly, diet-alone approaches have a relapse rate exceeding 80 percent within five years. Tirzepatide, when continued, maintains weight loss in nearly 90 percent of users.
Tirzepatide versus bariatric surgery
Roux-en-Y gastric bypass produces average weight loss of 25 to 30 percent. Tirzepatide at 15 mg produces 22.5 percent. The gap is narrowing, and tirzepatide avoids the surgical risks, recovery time, and permanent anatomical changes of bariatric surgery. For many people, tirzepatide represents a viable alternative to surgery.
Tirzepatide versus other GLP-1 medications
Against semaglutide, tirzepatide produces approximately 40 percent greater weight loss at maximum doses. Against survodutide and orforglipron, data is still emerging but tirzepatide remains the benchmark for dual-agonist weight loss medications. Newer triple-agonists like retatrutide show promise for even greater results, but are not yet FDA-approved for obesity.
The cost timeline: budgeting for tirzepatide
Weight loss timelines are inseparable from financial timelines. Understanding the cost structure helps with planning.
Affordable tirzepatide options vary widely. Brand-name Zepbound carries a list price that can be prohibitive without insurance. Compounded tirzepatide offers a significantly lower cost alternative, though availability and quality vary by pharmacy.
When budgeting, plan for a minimum of six months to see substantial results. Twelve months produces near-maximum results. Some people continue indefinitely at a maintenance dose for weight regain prevention. The cost calculation should include not just the medication but also supplements, reconstitution supplies (if using compounded), and periodic blood work.
Delivery format and timeline differences
The format in which you take tirzepatide can affect the weight loss timeline.
Injectable tirzepatide
The standard subcutaneous injection remains the most studied and most predictable format. Bioavailability is consistent, dose accuracy is high, and the clinical trial data directly applies. Proper injection technique ensures optimal absorption and minimizes injection site reactions.
Oral tirzepatide
Oral tirzepatide is in clinical trials and shows promise. The oral versus injection comparison suggests similar efficacy at equivalent doses, but absorption variability may affect individual timelines. Sublingual tirzepatide drops and tablet formulations offer convenience but may have slightly less predictable absorption compared to injection.
Combining tirzepatide with other compounds
Some people combine tirzepatide with other compounds to enhance weight loss or address specific concerns. Understanding how these combinations affect the timeline is important.
Tirzepatide with B12 is the most common combination, primarily for energy support. B12 does not directly affect the weight loss timeline but can improve energy levels and overall well-being during the process.
Tirzepatide with niacinamide targets metabolic health markers alongside weight loss. Niacinamide supports NAD+ production and may improve insulin sensitivity further.
AOD-9604 combined with tirzepatide is used by some for targeted fat loss, though clinical evidence for the combination is limited.
Cagrilintide added to tirzepatide represents a more advanced combination targeting the amylin pathway in addition to GLP-1 and GIP. This is primarily seen in research settings and may produce faster or greater weight loss, but the safety profile of the combination is not yet fully established.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Reconstitution and storage: protecting your timeline
For those using compounded tirzepatide, proper handling directly affects whether the medication works as expected throughout your timeline.
Reconstituting tirzepatide correctly is the first step. Incorrect reconstitution can result in inaccurate dosing, which disrupts the entire dose escalation schedule and weight loss trajectory. Use the tirzepatide reconstitution chart to calculate exact volumes.
Storage requirements must be followed strictly. Tirzepatide should be refrigerated and kept between 36 and 46 degrees Fahrenheit. Time outside the fridge should be minimized. Degraded medication produces weaker appetite suppression and slower weight loss, creating the illusion that the medication has stopped working when in reality it has been compromised.
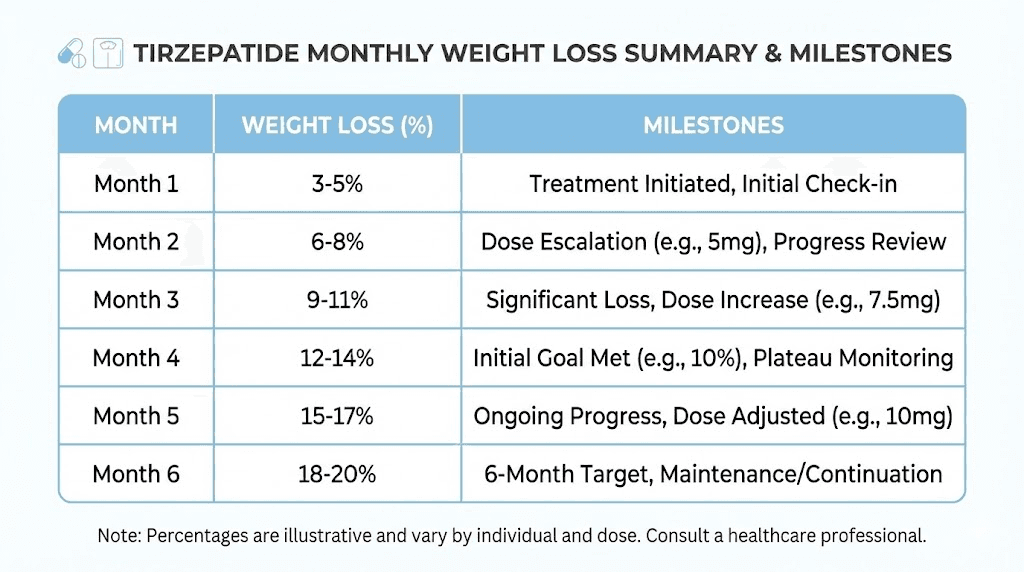
Realistic expectations: a month-by-month summary
Here is the consolidated view of what to expect, distilled from clinical trials and real-world data:
Timepoint | Typical weight loss | Key events |
|---|---|---|
Month 1 | 0-2% body weight | Appetite changes begin, GI adjustment, building dose |
Month 2 | 2-4% body weight | Noticeable appetite suppression, first therapeutic dose effects |
Month 3 | 5-8% body weight | Visible changes, clothes fit differently, others notice |
Month 4-5 | 8-15% body weight | Peak acceleration, fastest weekly losses, approaching max dose |
Month 6 | 15-18% body weight | Major milestone, health markers improve significantly |
Month 9 | 18-21% body weight | Potential first plateau, slower but continuing loss |
Month 12 | 20-22% body weight | Near maximum effect, body composition still improving |
Month 18 | 20-23% body weight | Weight stable, focus shifts to maintenance and optimization |
These ranges assume eventual dose escalation to 10 to 15 mg. Results at lower maintenance doses (5 to 7.5 mg) will be lower, typically 10 to 16 percent body weight loss at 72 weeks.
What the SURMOUNT clinical trials actually showed
The clinical trial data is the gold standard for understanding the tirzepatide weight loss timeline. Here are the specific findings that matter most.
SURMOUNT-1: the landmark trial
This 72-week trial enrolled 2,539 adults with obesity (BMI 30 or higher) or overweight (BMI 27 or higher) with at least one weight-related comorbidity. Participants who did not have diabetes were randomized to tirzepatide 5 mg, 10 mg, 15 mg, or placebo.
Results at 72 weeks:
Placebo: 3.1% weight loss
Tirzepatide 5 mg: 16.0% weight loss (35.3 pounds average)
Tirzepatide 10 mg: 21.4% weight loss (49.7 pounds average)
Tirzepatide 15 mg: 22.5% weight loss (52.3 pounds average)
The percentage of participants achieving 5% or more weight loss was 89% (5 mg), 96% (10 mg), and 96% (15 mg). For 20% or more weight loss, the numbers were 35% (5 mg), 57% (10 mg), and 63% (15 mg). Nearly two-thirds of people on the highest dose lost more than a fifth of their body weight.
SURMOUNT-4: the maintenance question
This trial demonstrated that continuing tirzepatide after achieving weight loss maintained the results, while stopping led to substantial regain. It established that tirzepatide is a chronic treatment, not a temporary intervention with lasting effects.
The late responder finding
Perhaps the most important finding for someone reading this article: 90 percent of participants who had lost less than 5 percent of their body weight by week 12 ("late responders") went on to achieve clinically meaningful weight loss by week 72. If you are reading this at month three feeling disappointed by your results, the data strongly suggests better outcomes ahead.
Frequently asked questions
How much weight will I lose in the first month on tirzepatide?
Most people lose 0 to 4 pounds in the first month. The starting dose of 2.5 mg is an initiation dose, not a therapeutic one. Real weight loss begins at the 5 mg dose in month two. The speed of tirzepatide results depends heavily on dose escalation and individual factors.
When will other people notice my weight loss on tirzepatide?
Most people report that others begin commenting on their appearance between weeks 8 and 12, when cumulative loss reaches 5 to 10 percent of body weight. Before and after comparisons typically show clearly visible changes by the three-month mark.
Is it normal to not lose weight the first few weeks?
Yes. The 2.5 mg starting dose is deliberately sub-therapeutic for weight loss. Its purpose is to let your gastrointestinal system adjust. Some people do not lose any weight until they reach 5 mg or even 7.5 mg. This does not predict your final outcome.
What if I am losing weight slower than the clinical trial averages?
Trial averages include both fast and slow responders. Your individual timeline depends on starting weight, dose, adherence, diet, activity, sleep, and genetic factors. If you are losing weight at all, the medication is working. Review the reasons for slow tirzepatide weight loss to see if any modifiable factors apply.
How long do I need to stay on tirzepatide?
Current evidence suggests tirzepatide should be used long-term for weight maintenance. The duration of GLP-1 medication use is ideally indefinite, though some people maintain with lower doses or explore microdosing protocols for ongoing maintenance.
Can I speed up my tirzepatide weight loss timeline?
Within safe limits, yes. Prioritizing protein intake, adding resistance training, ensuring quality sleep, managing stress, and adhering consistently to the injection schedule all maximize results. The optimal diet plan for tirzepatide users focuses on nutrient density and adequate protein to support faster fat loss while preserving lean mass.
Does tirzepatide increase metabolism?
Tirzepatide has metabolic effects that go beyond appetite suppression. The GIP pathway improves fat oxidation and energy expenditure. However, the primary weight loss mechanism is still reduced caloric intake through appetite suppression. Metabolic rate does decrease as weight drops, which is a normal physiological response.
What happens to loose skin after tirzepatide weight loss?
Loose skin depends on the amount of weight lost, age, genetics, and skin elasticity. Rapid weight loss from any method, including tirzepatide, can leave excess skin. The slower loss rate in the later months allows some skin remodeling. Skin tightening peptides and collagen-supporting compounds may help, though expectations should be realistic for larger weight losses.
Can I take tirzepatide while breastfeeding or pregnant?
Tirzepatide is not recommended during pregnancy or breastfeeding. The breastfeeding considerations include potential transfer of the medication to breast milk. Women who become pregnant on tirzepatide should discontinue immediately and consult their healthcare provider.
External resources
SURMOUNT-4 Trial: Continued Treatment With Tirzepatide for Maintenance of Weight Reduction (JAMA)
Body Composition Changes During Weight Reduction With Tirzepatide in SURMOUNT-1 (PMC)
For researchers serious about building an effective weight loss protocol, SeekPeptides provides comprehensive guides, evidence-based protocols, and a supportive community that has helped thousands navigate their peptide research journey with confidence and clarity.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay consistent, your progress stay visible, and your patience stay rewarded.