Feb 27, 2026

Scroll through the listings at any weight loss clinic and you will notice something. The vials do not just say tirzepatide anymore. They say tirzepatide with levocarnitine. Or tirzepatide plus L-carnitine. Or some variation that makes the simple compounded tirzepatide you researched last month sound almost outdated. Compounding pharmacies have been adding ingredients to their GLP-1 formulations for a while now, but the levocarnitine blend has become one of the most marketed combinations on the market. It promises faster fat burning. Greater muscle preservation. Better energy. A more complete weight loss solution in a single injection.
That sounds compelling. It also raises questions.
Does adding levocarnitine to tirzepatide actually improve outcomes? Is there clinical evidence behind these claims, or is this another case of compounding pharmacies bundling ingredients to justify premium pricing? What does the research say about L-carnitine for fat loss on its own, and does combining it with a GLP-1 receptor agonist change the equation? These are the questions that matter, and the marketing materials from clinics and pharmacies rarely address them with the specificity you need. This guide covers what the tirzepatide levocarnitine blend actually is, how each ingredient works independently, what happens when they are combined, the current evidence for and against this formulation, practical dosing considerations, side effects to watch for, and the regulatory landscape that determines whether you can even access this combination legally. SeekPeptides built this resource because the information gap around compounded GLP-1 blends is enormous, and making informed decisions requires more than a pharmacy product page.
What is the tirzepatide levocarnitine blend?
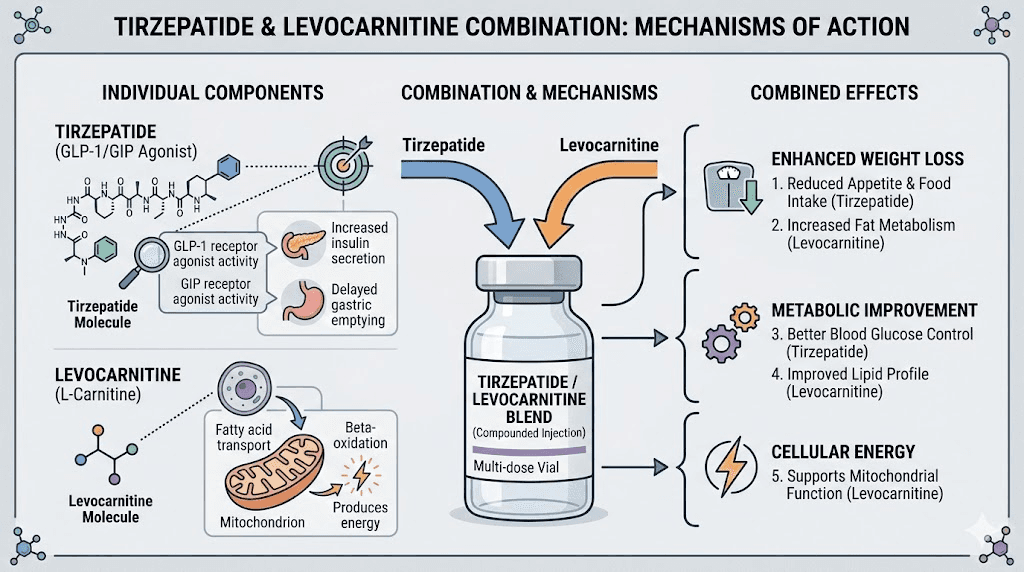
The tirzepatide levocarnitine blend is a compounded medication that combines two distinct ingredients into a single injectable formulation. The first ingredient, tirzepatide, is a dual GIP/GLP-1 receptor agonist originally developed by Eli Lilly and approved by the FDA under the brand names Mounjaro (for type 2 diabetes) and Zepbound (for chronic weight management). It works by mimicking two incretin hormones simultaneously, reducing appetite, slowing gastric emptying, improving insulin sensitivity, and promoting significant weight loss in clinical trials.
The second ingredient is levocarnitine, which is the pharmaceutical name for L-carnitine. This is a naturally occurring amino acid derivative that plays a critical role in fatty acid metabolism. Your body produces it. You also get it from food, primarily red meat and dairy products. Its primary function is transporting long-chain fatty acids across the inner mitochondrial membrane so they can be oxidized and converted into cellular energy through beta-oxidation.
When a compounding pharmacy creates the tirzepatide levocarnitine blend, they are mixing these two ingredients into a single vial or syringe at specific concentrations. The idea is straightforward. Tirzepatide reduces how much you eat. Levocarnitine theoretically helps your body burn more of the fat it is already breaking down. Together, the combination is marketed as a more effective weight loss tool than tirzepatide alone.
How tirzepatide works on its own
Before evaluating the blend, you need to understand what each component does independently. Tirzepatide is not just another GLP-1 drug. It is the first approved dual GIP and GLP-1 receptor agonist, which means it activates two separate incretin pathways that single-agonist medications like semaglutide cannot reach. The GIP receptor activation adds an additional metabolic dimension that appears to enhance fat oxidation and improve insulin sensitivity beyond what GLP-1 activation alone achieves.
Clinical trial data tells a clear story. In the SURMOUNT-1 trial, participants taking the highest dose of tirzepatide (15 mg weekly) lost an average of 22.5% of their body weight over 72 weeks. That is roughly 52 pounds for someone starting at 230 pounds. The tirzepatide weight loss timeline typically shows measurable results within the first four to eight weeks, with the most dramatic changes occurring between months three and six as doses titrate upward.
The mechanism involves multiple pathways working simultaneously. Appetite suppression reduces caloric intake, often dramatically. Delayed gastric emptying means food stays in the stomach longer, extending feelings of fullness after meals. Improved insulin signaling helps the body process glucose more efficiently, reducing the tendency to store excess energy as fat. And emerging research suggests direct effects on adipose tissue metabolism that may shift the body toward preferentially burning fat stores rather than lean muscle.
That last point is important for this discussion. One of the concerns with any rapid weight loss, whether from GLP-1 medications, calorie restriction, or surgery, is the loss of lean body mass alongside fat. Roughly 25-40% of weight lost during aggressive calorie restriction can come from muscle tissue. Tirzepatide before and after data from clinical trials suggests the lean mass loss percentage may be lower than with some other interventions, but it is still a legitimate concern. This is where levocarnitine enters the conversation.
How levocarnitine works in the body
Levocarnitine is not exotic. It is one of the most studied nutritional compounds in metabolic research, with decades of clinical data behind it. Your body synthesizes approximately 75% of the L-carnitine it needs from the amino acids lysine and methionine, primarily in the liver and kidneys. The remaining 25% comes from dietary sources. Healthy adults with adequate nutrition rarely develop a clinical deficiency.
The primary role of L-carnitine is acting as a shuttle. Long-chain fatty acids cannot cross the inner mitochondrial membrane on their own. They need a carrier, and L-carnitine is that carrier. Through a system involving the enzymes carnitine palmitoyltransferase I (CPT-I) and carnitine palmitoyltransferase II (CPT-II), L-carnitine binds to fatty acid molecules, transports them into the mitochondrial matrix, and releases them for beta-oxidation, the process that breaks fatty acids down into acetyl-CoA units for energy production in the citric acid cycle.
Think of it this way. Fat is fuel. But fuel sitting in a gas station does nothing for your car. It needs to get into the engine. L-carnitine is the truck that delivers fatty acids to the mitochondrial engine where they can actually be burned.
Beyond fatty acid transport, L-carnitine has several other documented functions. It helps remove toxic acyl groups from cells, preventing their accumulation. It serves as a buffer for the acyl-CoA/CoA ratio, which is critical for normal cellular metabolism. It may have anti-inflammatory properties. And some research suggests it supports cardiovascular function by improving the efficiency of cardiac energy metabolism. The compound also exists in several forms, including acetyl-L-carnitine (ALCAR), which crosses the blood-brain barrier more readily and is studied for cognitive benefits, and L-carnitine L-tartrate, which is commonly used in athletic performance contexts for exercise recovery.
What the weight loss research shows for L-carnitine alone
A systematic review and meta-analysis published in Clinical Nutrition ESPEN analyzed 37 randomized controlled trials with 2,292 participants. The findings showed that L-carnitine supplementation significantly decreased body weight by an average of 1.21 kg, BMI by 0.24 kg/m2, and fat mass by 2.08 kg. The effects were most pronounced in overweight and obese individuals and when combined with lifestyle modifications like diet and exercise.
That is real. But it is modest.
A dose-response analysis from the same research suggested that 2,000 mg per day provides the maximum weight loss effect in adults, with a non-linear relationship meaning that taking more than 2,000 mg does not produce proportionally greater benefits. Most positive clinical trials used 1-2 grams daily for 8-24 weeks.
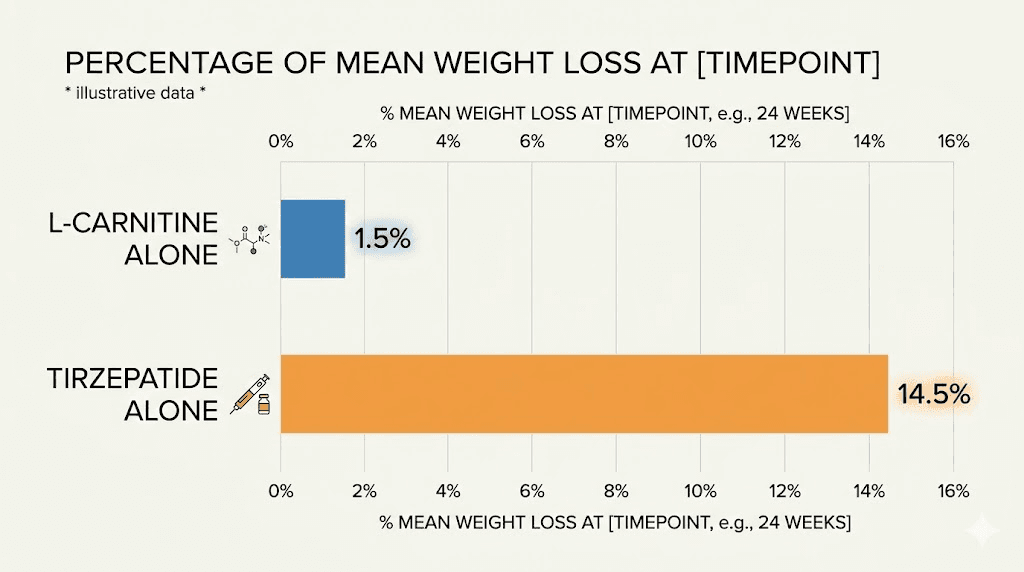
To put this in perspective, L-carnitine alone might help you lose an extra 2-4 pounds over several months. Tirzepatide alone can produce 50+ pounds of weight loss over the same period. The scale of effect is dramatically different. This does not mean L-carnitine is worthless, but it does mean that anyone expecting it to dramatically amplify how fast tirzepatide works needs to calibrate their expectations against the actual data.
The theory behind combining tirzepatide with levocarnitine
The rationale for the tirzepatide levocarnitine blend rests on a logical premise, even if the clinical evidence for the specific combination is limited. The argument goes like this.
When you take tirzepatide, your caloric intake drops significantly. Your body responds to this energy deficit by increasing the mobilization of fatty acids from adipose tissue. These fatty acids enter the bloodstream and become available for oxidation. But availability does not automatically equal utilization. If the mitochondrial transport system becomes a bottleneck, if there is not enough carnitine to shuttle all those mobilized fatty acids into the mitochondria for burning, then some of that fat may not get oxidized efficiently.
Adding levocarnitine, in theory, ensures that the transport system never becomes the limiting factor. More fatty acids get into the mitochondria. More fat gets burned. The proportion of weight lost from fat (rather than muscle) potentially improves. Energy levels may stay higher because the body is more efficiently converting fat stores into usable cellular energy rather than breaking down muscle protein for gluconeogenesis.
This is a reasonable hypothesis. It is also largely theoretical when applied specifically to the tirzepatide combination.
What we know and what we do not
There is strong evidence that L-carnitine plays a critical role in fatty acid oxidation. Nobody disputes the biochemistry. There is moderate evidence that L-carnitine supplementation can modestly reduce body weight and fat mass in overweight individuals. There is some evidence that L-carnitine may help preserve lean muscle mass during calorie restriction, though the data is mixed and the effect sizes are small.
What does not exist, at least as of the current published literature, is a clinical trial specifically studying the combination of tirzepatide plus levocarnitine versus tirzepatide alone. No head-to-head comparison has been conducted. No randomized controlled trial has isolated the additive effect of levocarnitine when given alongside tirzepatide. The claims being made by clinics and compounding pharmacies about this specific blend are based on extrapolation from independent research on each ingredient, not on evidence from the combination itself.
This distinction matters. Combining two individually beneficial interventions does not always produce additive or synergistic results. Sometimes the effects overlap rather than stack. Sometimes one intervention makes the other redundant. And sometimes there are interactions that reduce effectiveness or increase side effects. Without specific combination data, we are operating in the territory of informed speculation rather than proven science.
Dosing protocols for the tirzepatide levocarnitine blend
The dosing for the tirzepatide component in the blend follows the same general escalation pattern as standard compounded tirzepatide. Most protocols start at 2.5 mg per week and increase by 2.5 mg increments every four weeks based on tolerability and response. The maximum dose typically reaches 15 mg per week, matching the FDA-approved upper limit for brand-name tirzepatide products.
Standard titration schedule
The tirzepatide dosing chart for the levocarnitine blend typically follows this pattern. Weeks one through four use 2.5 mg of tirzepatide with a set amount of levocarnitine. Weeks five through eight increase to 5 mg. Weeks nine through twelve move to 7.5 mg. From there, the dose can continue increasing to 10 mg, 12.5 mg, and ultimately 15 mg if needed and tolerated. Each step usually involves a minimum four-week hold to assess tolerance before moving up.
The levocarnitine component in compounded blends varies significantly between pharmacies. Some formulations include 100 mg of levocarnitine per injection. Others include 200 mg, 500 mg, or even higher amounts. There is no standardized concentration because these are compounded products, not FDA-approved drugs with fixed formulations. The amount of levocarnitine you receive depends entirely on which pharmacy compounds your blend and what your prescribing provider orders.
This variability is worth understanding. The meta-analysis research suggesting optimal L-carnitine dosing around 2,000 mg daily studied oral supplementation, not injectable administration. Injectable L-carnitine has significantly higher bioavailability than oral forms, which means smaller injectable doses may achieve comparable blood levels to larger oral doses. However, the exact pharmacokinetic equivalence is not well established for the concentrations typically used in these compounded GLP-1 blends.
How reconstitution works for the blend
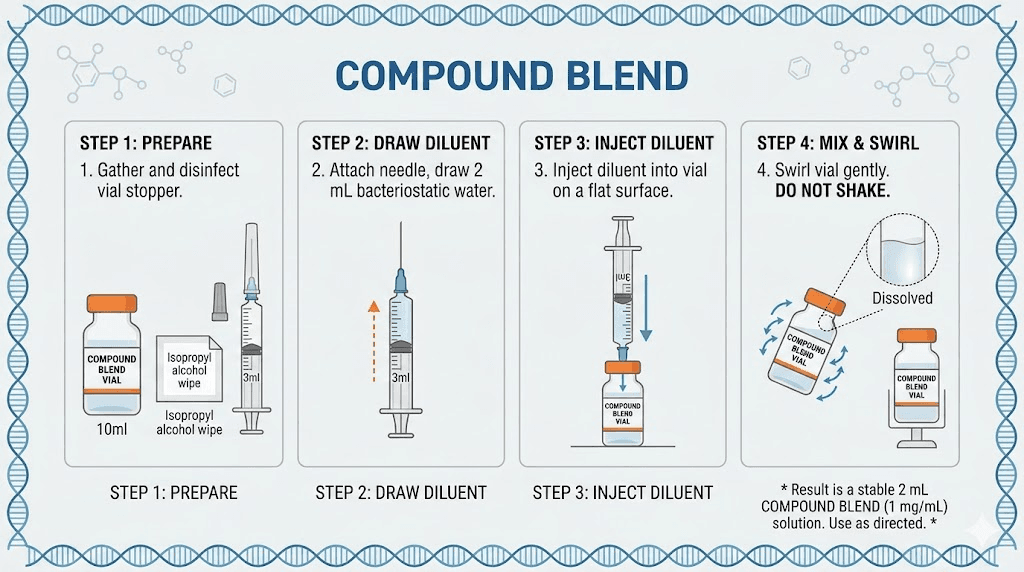
If your tirzepatide levocarnitine blend comes as a lyophilized (freeze-dried) powder, you will need to reconstitute tirzepatide with bacteriostatic water before injection. The process is identical to reconstituting standard compounded tirzepatide. You inject a specific volume of bacteriostatic water into the vial, swirl gently (never shake), and allow the powder to dissolve completely. The resulting solution concentration determines how many units you draw for each dose.
Use the compounded tirzepatide dosage calculator to determine exact volumes based on your vial concentration and target dose. The math works the same regardless of whether levocarnitine is included in the formulation. What changes is that the reconstituted solution now contains both active ingredients at their respective concentrations.
Some pharmacies ship the blend pre-mixed in liquid form, eliminating the need for reconstitution entirely. These ready-to-inject vials typically come with a concentration printed on the label (for example, tirzepatide 5 mg/mL with levocarnitine 200 mg/mL), and you simply draw your calculated dose using an insulin syringe. Check the tirzepatide syringe dosage guide for proper technique.
Comparing tirzepatide additive options
Levocarnitine is not the only ingredient that compounding pharmacies add to tirzepatide. Several other additives are commonly offered, each with a different theoretical justification. Understanding how they compare helps you make a more informed decision about which formulation, if any, is right for your situation.
L-carnitine versus B12
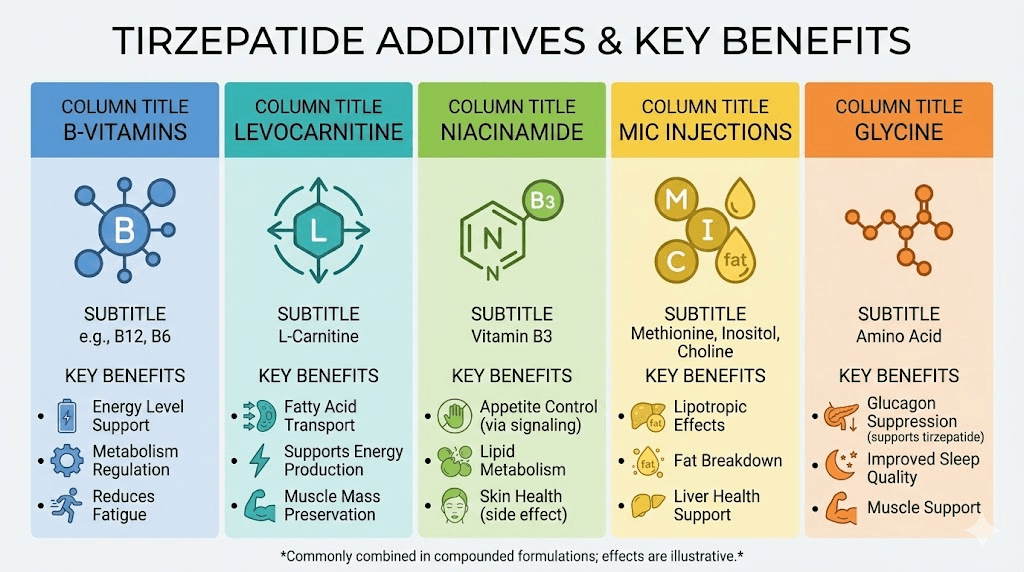
Tirzepatide with B12 is probably the most common compounded combination. Vitamin B12 (cyanocobalamin or methylcobalamin) supports red blood cell production, nerve function, and energy metabolism. The rationale for adding it to tirzepatide is that calorie restriction and GI side effects from GLP-1 medications can reduce B12 absorption, potentially leading to deficiency over time. Adding B12 directly to the injection bypasses the digestive system entirely.
The evidence base for B12 supplementation is stronger than for L-carnitine in the context of GLP-1 medications, at least in terms of addressing a documented risk (B12 deficiency during prolonged GLP-1 use). However, B12 is not directly involved in fat metabolism the way L-carnitine is. If your primary concern is maximizing fat oxidation and preserving muscle, the theoretical advantage goes to L-carnitine. If your concern is preventing nutritional deficiency and supporting general energy levels, B12 has the stronger case. The tirzepatide methylcobalamin combination uses the more bioavailable form of B12.
L-carnitine versus glycine
Tirzepatide with glycine takes a different approach. Glycine is the simplest amino acid, and adding it to GLP-1 formulations is thought to improve stability and reduce injection site reactions. Some practitioners also cite glycine role in collagen synthesis, detoxification pathways, and sleep quality. The tirzepatide glycine blend addresses different concerns than the levocarnitine version, focusing more on tolerability and compound stability than on metabolic enhancement.
L-carnitine versus niacinamide
The tirzepatide niacinamide combination adds a form of vitamin B3 that supports NAD+ production, cellular energy, and skin health. Niacinamide has anti-inflammatory properties and may help with some of the skin-related side effects that can occur with rapid weight loss. It addresses a completely different set of concerns than levocarnitine.
Triple and multi-ingredient blends
Some pharmacies take it further with triple blends. The tirzepatide glycine B12 compound is one of the most popular multi-ingredient formulations. You may also encounter blends that include NAD+, B6 (pyridoxine for nausea reduction), or even combinations of four or five additives in a single vial. More ingredients does not necessarily mean better results. Each addition introduces potential for interactions, stability concerns, and cost increases.
The comparison table below summarizes the key differences.
Additive | Primary purpose | Evidence level | Best for |
|---|---|---|---|
L-Carnitine | Fat oxidation, muscle preservation | Moderate (for fat loss alone) | Maximizing fat burning ratio |
B12 | Energy, nerve function, deficiency prevention | Strong (for deficiency prevention) | General wellness during GLP-1 use |
Glycine | Stability, tolerability, collagen | Moderate (for compound stability) | Reducing injection reactions |
Niacinamide | NAD+, skin health, anti-inflammatory | Moderate (individually) | Skin concerns during weight loss |
B6 | Nausea reduction | Moderate (for nausea) | Managing GI side effects |
Muscle preservation during GLP-1 weight loss
This is the argument that sells the most tirzepatide levocarnitine blends. The fear of losing muscle alongside fat is legitimate, and it is one of the most searched concerns among people considering GLP-1 medications for weight loss.
Here is the reality. When you create a caloric deficit significant enough to lose 20-25% of your body weight, some muscle loss is virtually inevitable. The body does not exclusively target fat stores during periods of severe energy restriction. It pulls from protein stores as well, breaking down muscle tissue for gluconeogenesis (making glucose from amino acids) when dietary protein intake and exercise stimulus are insufficient to fully protect lean mass.
Data from the SURMOUNT trials showed that participants losing significant weight on tirzepatide experienced approximately 33-39% of total weight loss from lean body mass. That means for every 10 pounds lost, roughly 3-4 pounds came from muscle and other lean tissue. This ratio is actually comparable to or slightly better than what is seen with aggressive diet-only interventions, but it is still a meaningful amount of muscle to lose.
What actually preserves muscle during weight loss
The interventions with the strongest evidence for preserving muscle during rapid weight loss are, in order of evidence strength, resistance training, adequate protein intake (1.0-1.6 grams per kilogram of body weight daily), and possibly creatine supplementation. These are the foundations. Everything else is secondary.
L-carnitine theoretical contribution to muscle preservation is indirect. By enhancing fatty acid oxidation, it may reduce the body need to break down protein for energy. If more fat is being efficiently converted to fuel, there is less metabolic pressure to cannibalize muscle tissue. Some small studies suggest that L-carnitine supplementation during calorie restriction may improve the ratio of fat loss to lean mass loss, but the effect sizes are small and not all studies agree.
A critical point that the marketing materials rarely address: the most important factors for preserving muscle during tirzepatide use have nothing to do with what is in the vial. They depend on what you do outside of the injection. Lifting weights two to three times per week. Eating sufficient protein at every meal. What to eat on tirzepatide matters enormously for body composition outcomes, and no additive in the world can compensate for a protein-deficient diet and a sedentary lifestyle during rapid weight loss.
That said, if someone is already training, already eating adequate protein, and wants to optimize every possible variable, adding L-carnitine is not unreasonable. It is just unlikely to be the difference-maker that marketing materials suggest.
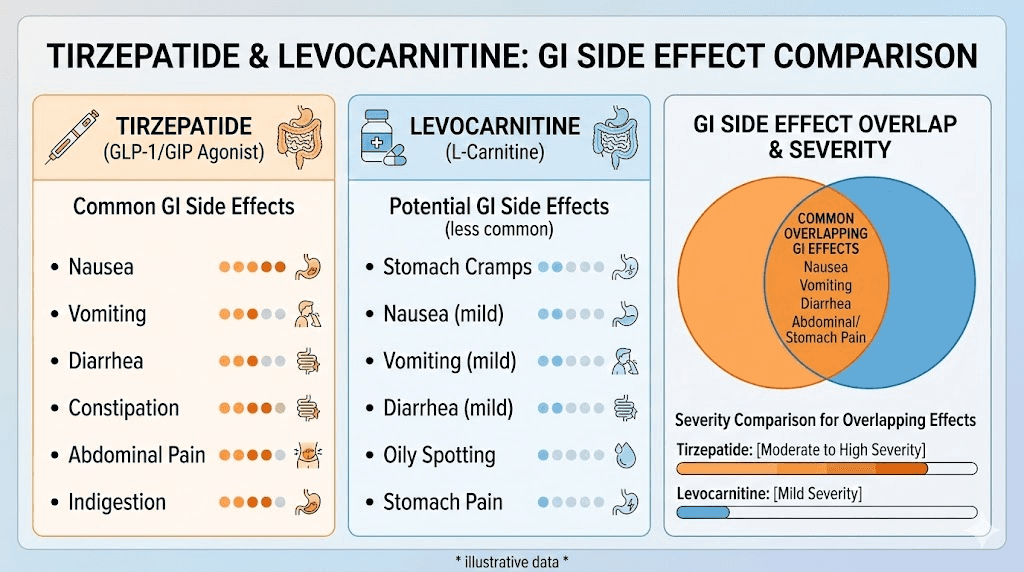
Side effects and safety considerations
The side effect profile of the tirzepatide levocarnitine blend is primarily driven by the tirzepatide component. The most common adverse effects include nausea, vomiting, diarrhea, constipation, decreased appetite, and abdominal discomfort. These gastrointestinal effects are typically most pronounced during the first few weeks at each dose level and tend to improve as the body adjusts. See the tirzepatide constipation treatment guide and the tirzepatide diarrhea guide for management strategies.
Tirzepatide side effects to monitor
The side effect comparison between tirzepatide and semaglutide shows broadly similar profiles with some differences in severity. Common tirzepatide side effects that people report include headaches, fatigue, body aches, anxiety, insomnia, muscle pain, dry mouth, and injection site reactions. Most of these resolve with continued use and proper dose titration. Starting low and increasing slowly is the single most effective strategy for minimizing GI side effects.
Levocarnitine side effects
L-carnitine is generally well tolerated at typical supplemental doses. Side effects tend to be dose-dependent and include nausea, vomiting, abdominal cramps, diarrhea, and a fishy body odor. These GI effects overlap with tirzepatide common side effects, which raises a legitimate concern. Combining two ingredients that both have GI side effect potential could theoretically worsen tolerability, particularly during the early dose titration phase when the body is still adjusting to tirzepatide.
At doses above 3,000 mg daily, L-carnitine side effects become more common. Most compounded blends contain well below this threshold per injection, but the exact amount varies by pharmacy and formulation. Ask your prescriber to confirm the levocarnitine content in your specific blend.
A longer-term concern that has received attention in the cardiology literature involves trimethylamine N-oxide (TMAO). Some research suggests that chronic high-dose L-carnitine supplementation may increase TMAO levels via gut bacteria metabolism, and elevated TMAO has been associated with increased cardiovascular risk in observational studies. This finding is still debated and the clinical significance for people taking moderate injectable doses (which bypass gut metabolism) is unclear. But it is worth discussing with your healthcare provider, especially if you have existing cardiovascular risk factors.
Drug interactions
L-carnitine can interact with certain medications. It may enhance the effects of warfarin and other blood thinners, potentially increasing bleeding risk. It can interact with thyroid hormones. And it may affect the metabolism of certain seizure medications. If you are taking any prescription medications alongside your tirzepatide levocarnitine blend, make sure your prescribing provider has a complete medication list. Also review the supplements to take with tirzepatide guide for a broader look at what pairs safely with GLP-1 medications.
FDA status and compounding regulations
This section is critical because the regulatory landscape around compounded tirzepatide, including the levocarnitine blend, has changed dramatically in recent months.
During the tirzepatide shortage period (roughly mid-2023 through late 2024), compounding pharmacies were permitted under FDA enforcement discretion to produce copies of commercially available tirzepatide to help meet patient demand. This is how the entire compounded tirzepatide market, including levocarnitine blends, B12 combinations, and other additive formulations, grew so rapidly.
In October 2024, the FDA determined that the tirzepatide injection shortage (covering both Mounjaro and Zepbound) was resolved. This meant that the legal basis for most compounding of tirzepatide essentially disappeared. The FDA issued a declaratory order in December 2024 reaffirming this decision and established grace periods for pharmacies to wind down their compounded tirzepatide operations.
Current compounding status
As of the current regulatory framework, 503A pharmacies (traditional compounding pharmacies that fill individual prescriptions) were given until February 2025 to stop compounding tirzepatide. 503B outsourcing facilities had until March 2025. After these deadlines, compounding tirzepatide is only permitted in limited circumstances, specifically when a prescriber determines that a compounded product provides a clinical difference for a specific patient that cannot be met by commercially available FDA-approved products, with that determination documented on an individual patient basis.
What does this mean for the tirzepatide levocarnitine blend specifically? Some legal arguments suggest that because the levocarnitine blend is a distinct formulation that does not exist as a commercially available product, it could potentially be compounded under different provisions. This legal territory is actively being tested and contested. Some compounding pharmacies have pivoted to emphasizing the "clinically meaningful difference" angle, arguing that the addition of levocarnitine makes their product sufficiently different from commercial Mounjaro/Zepbound to justify continued compounding.
The situation remains fluid. Court challenges are ongoing. State pharmacy boards are interpreting federal guidance differently. And enforcement priorities continue to evolve. If you are currently using or considering a tirzepatide levocarnitine blend, verify with your pharmacy that they are operating within current legal requirements. The grey market tirzepatide landscape has become increasingly complex, and purchasing from non-compliant sources carries both legal and safety risks.
The semaglutide levocarnitine comparison
It is worth noting that the levocarnitine additive concept is not unique to tirzepatide. The semaglutide L-carnitine combination has been available from compounding pharmacies as well, and many of the same claims and considerations apply. The choice between a tirzepatide-based or semaglutide-based blend depends on factors beyond the L-carnitine addition, including which GLP-1 your body responds to better, side effect tolerance, cost, and prescriber preference.
Tirzepatide dual-agonist mechanism (GIP + GLP-1) may provide stronger weight loss results on average compared to semaglutide single-agonist (GLP-1 only) approach. The semaglutide versus tirzepatide comparison covers this head-to-head data in detail. If the base medication is more effective, the relative contribution of the levocarnitine additive becomes proportionally smaller in terms of overall impact.
Some practitioners recommend starting with a semaglutide-based blend for patients who are GLP-1 naive, since semaglutide has a longer track record and may be easier to titrate. Others prefer starting directly with tirzepatide for its superior efficacy data. The levocarnitine addition does not fundamentally change this decision calculus. It is the same additive regardless of which base GLP-1 it is combined with.
Who the tirzepatide levocarnitine blend is designed for
Not everyone needs a compounded blend with additives. Understanding who might actually benefit helps separate marketing from medicine.
Potential candidates
People with documented L-carnitine deficiency (rare but does occur, particularly in individuals with certain genetic conditions, kidney disease, or those on dialysis) have a clear medical rationale for L-carnitine supplementation. If you happen to also need tirzepatide for weight management, a combined formulation could simplify your medication regimen.
Individuals prioritizing body composition over scale weight, meaning people who are specifically concerned about the ratio of fat loss to muscle loss rather than just total pounds lost, represent the theoretical target market. Athletes, fitness enthusiasts, and bodybuilders who are using GLP-1 medications while trying to maintain training performance and muscle mass fall into this category.
Older adults (over 60) losing weight on GLP-1 medications face higher risks from muscle loss because age-related sarcopenia is already reducing their lean mass. Any intervention that might improve muscle preservation has proportionally greater value in this population, even if the absolute effect is modest.
Who probably does not need it
People who are primarily interested in total weight loss and are not focused on body composition metrics will likely see negligible benefit from the levocarnitine addition. The extra cost (compounded blends with additives typically cost more than plain compounded tirzepatide) is hard to justify when the additive contribution to total weight loss is measured in single-digit pounds at most.
People who are already taking oral L-carnitine supplements separately do not need it in their injection as well. If you are supplementing with 1,000-2,000 mg of oral L-carnitine daily, you are likely already achieving the blood levels needed for any potential metabolic benefit. Adding more via injection may not produce additional effects and could increase side effect risk.
And anyone who is not simultaneously addressing the fundamentals, adequate protein intake, resistance training, sufficient sleep, and proper hydration, is unlikely to notice any meaningful difference from the levocarnitine additive. These basics drive 90%+ of body composition outcomes during weight loss. The remaining marginal gains from supplements and additives are only detectable against a backdrop of solid fundamentals.
Storage and handling for the blend
Proper storage of the tirzepatide levocarnitine blend follows the same principles as standard tirzepatide storage. Refrigerate at 36-46 degrees Fahrenheit (2-8 degrees Celsius). Do not freeze. Keep the vial protected from direct light. Once reconstituted, use within the timeframe specified by your pharmacy, typically 28-42 days depending on the formulation.
The addition of levocarnitine does not significantly change storage requirements, but it may affect stability in some formulations. L-carnitine is generally stable in aqueous solution at refrigerator temperatures, but the combined formulation stability depends on the specific concentrations, pH, and excipients used by each compounding pharmacy. Always follow the storage instructions provided with your specific product. The tirzepatide shelf life guide covers general storage principles in greater detail.
If you need to travel with tirzepatide, the same cold chain requirements apply to the levocarnitine blend. Insulated travel cases with gel packs keep the medication within proper temperature ranges. Avoid leaving the blend at room temperature for extended periods, and check the what happens if tirzepatide gets warm guide if you suspect a temperature excursion.
If your blend changes color unexpectedly, develops cloudiness, or shows particles, do not use it. The tirzepatide color guide can help you identify what normal looks like for various formulations. Compounded blends may have a slightly different appearance than plain tirzepatide depending on the levocarnitine concentration and any other additives included.
Injection technique and administration
The tirzepatide levocarnitine blend is administered as a subcutaneous injection, typically once weekly. The injection technique is identical to standard tirzepatide. Use an insulin syringe to draw the calculated dose from the vial, select an injection site (abdomen or thigh are most common), pinch the skin, insert the needle at a 45-90 degree angle, and inject slowly.
For detailed injection guidance, see the how to inject tirzepatide with syringe guide. Preferred injection sites include the thigh and stomach areas. Rotate sites to reduce the risk of injection site reactions, which can include redness, swelling, and itching.
Some people report that levocarnitine-containing injections produce slightly more injection site irritation than plain tirzepatide. This is anecdotal and not universally experienced, but if you notice increased redness and itching at the injection site, the levocarnitine may be contributing. Injecting slowly, using the proper needle gauge, and ensuring the solution is at room temperature (let the vial sit out for 15-20 minutes before injecting) can help minimize discomfort.
The best time to take your GLP-1 shot does not change with the addition of levocarnitine. Most people find that injecting on a consistent day each week, often in the morning before meals, produces the best results and easiest routine compliance.
What to eat while using the blend
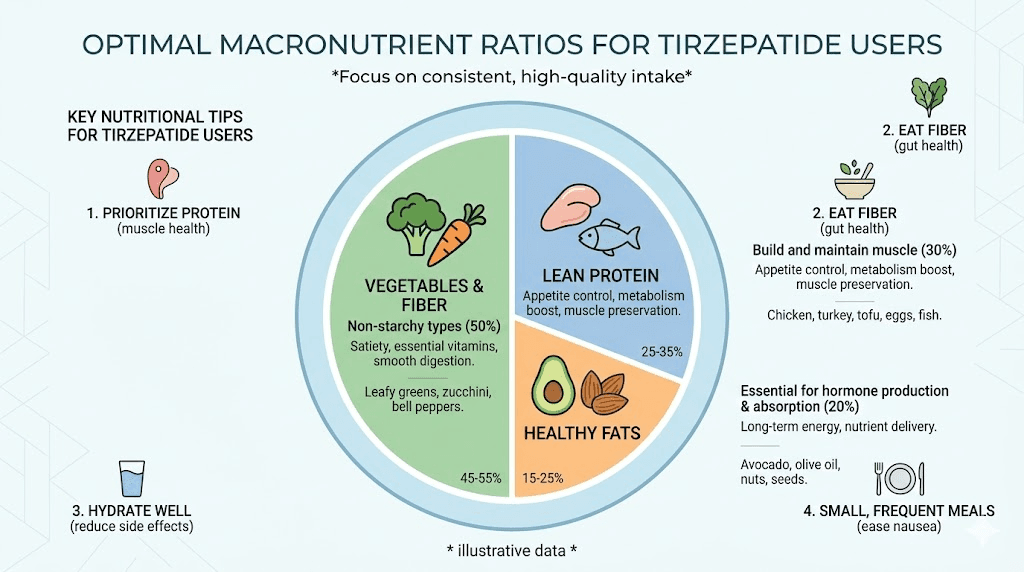
Nutrition while using the tirzepatide levocarnitine blend is arguably more important than the blend itself when it comes to determining your outcomes. The appetite suppression from tirzepatide can dramatically reduce your food intake, which means every meal needs to count. Prioritizing protein is essential, both for muscle preservation and for general health during rapid weight loss.
The tirzepatide diet plan guide provides comprehensive nutritional guidance, and the tirzepatide foods to avoid article covers items that commonly cause problems during GLP-1 therapy. High-fat, greasy foods tend to exacerbate nausea. Large portions overwhelm a stomach that is already emptying more slowly than usual. And simple carbohydrates provide empty calories that crowd out the protein and nutrients you actually need.
Aim for 1.0 to 1.6 grams of protein per kilogram of body weight daily. For a 200-pound person, that means 90-145 grams of protein each day. This is challenging when your appetite is significantly reduced, which is why protein shakes for GLP-1 users have become such a popular solution. A high-quality protein shake can deliver 30-50 grams of protein in a small volume that even a suppressed appetite can handle.
The tirzepatide meal plan provides structured daily eating templates. The list of foods to eat on GLP-1 medications gives you a comprehensive grocery guide. And the best foods for GLP-1 users article highlights the highest-impact choices.
If you are taking the levocarnitine blend specifically for its fat-oxidation benefits, note that L-carnitine works best when there are fatty acids available to transport. This does not mean you should eat a high-fat diet. It means your body natural fat mobilization during a caloric deficit provides the substrate. Regular physical activity, especially during fasting periods or before meals, increases fatty acid mobilization and creates the conditions where enhanced carnitine-mediated transport could theoretically make a difference.
Exercise considerations with the blend
Exercise is not optional if you care about body composition during weight loss. No additive, whether levocarnitine or anything else, can replace the muscle-preserving stimulus of resistance training. The people who maintain the most lean mass during GLP-1-assisted weight loss are consistently the ones who combine their medication with structured exercise.
Resistance training two to three times per week provides the primary signal that tells your body to preserve muscle tissue even in the face of significant caloric deficit. Compound movements like squats, deadlifts, presses, and rows recruit large muscle groups and produce the strongest anabolic stimulus. You do not need to train like a competitive bodybuilder. Moderate loads (60-80% of your one-rep max) for 3-4 sets of 8-12 repetitions per exercise, covering all major muscle groups twice per week, is sufficient for most people.
Cardiovascular exercise provides additional calorie burning and cardiovascular health benefits but does relatively little for muscle preservation compared to resistance training. Walking 30-60 minutes daily is an excellent baseline activity that complements tirzepatide appetite-suppressing effects without overtaxing recovery capacity.
The theoretical benefit of levocarnitine in the exercise context relates to L-carnitine well-documented role in exercise metabolism. Some research suggests that L-carnitine supplementation can reduce exercise-induced muscle damage, decrease muscle soreness, improve recovery, and enhance exercise performance, particularly in trained individuals. A study published in the Journal of Physiology found that 24 weeks of L-carnitine supplementation (combined with carbohydrates to enhance uptake) increased muscle carnitine content by 21% and improved exercise performance by increasing work output by 11% while reducing muscle lactate accumulation.
However, this research used oral supplementation protocols very different from the weekly injectable doses found in compounded tirzepatide blends. Whether the intermittent, lower-dose levocarnitine exposure from a weekly injection produces comparable effects to daily oral supplementation is unknown.
If tirzepatide gives you enough energy to train consistently, the exercise itself will do far more for body composition than the levocarnitine in the blend. Focus on showing up to train and eating enough protein. Those are the high-impact variables. The levocarnitine is a potential marginal optimization on top of an already effective foundation.
Cost considerations
Compounded tirzepatide with levocarnitine typically costs more than plain compounded tirzepatide. The premium varies by pharmacy but generally ranges from $20-80 additional per month for the levocarnitine addition. Some pharmacies charge significantly more, bundling the blend into proprietary "weight loss packages" that include additional services, consultations, and monitoring.
When evaluating cost, consider this math. If L-carnitine supplementation at optimal doses (2,000 mg daily) costs roughly $15-30 per month as an over-the-counter oral supplement, and the injectable blend charges $50-80 more per month for a potentially lower total dose of L-carnitine, the economic argument for the blend over separate supplementation becomes thin. The convenience of a single injection is real. But so is the cost difference.
The affordable tirzepatide guide and the cheap compounded tirzepatide article cover cost-reduction strategies that apply regardless of which additive you choose. Comparing prices between pharmacies is essential because compounded medication pricing varies dramatically. The peptide cost calculator can help you estimate and compare total treatment costs across different providers and formulations.
Also factor in the cost of the fundamentals that matter more than the blend. A gym membership, high-quality protein sources, and potentially a personal trainer or nutritionist consultation will produce larger body composition improvements than switching from plain tirzepatide to the levocarnitine blend. Allocate your budget accordingly.
What experienced users report
Online forums and weight loss communities include numerous anecdotal reports from people using the tirzepatide levocarnitine blend. These reports are not scientific evidence, but they do reflect real-world experience that can be informative when combined with the clinical data.
Common positive reports include feeling more energetic during the day, subjectively better exercise performance, and a perception of "losing more fat and less muscle" compared to plain tirzepatide. Some users report that the levocarnitine blend seems to reduce the fatigue that is common with GLP-1 medications, which is plausible given L-carnitine role in energy metabolism. The GLP-1 fatigue guide discusses this issue comprehensively.
Common negative reports include increased injection site discomfort, slightly more GI upset (particularly during the first few weeks), and disappointment when the dramatic results promised by marketing materials do not materialize. Several users note that they saw similar results after switching to plain tirzepatide with a separate oral L-carnitine supplement, which cost significantly less.
The most balanced user reports consistently emphasize that the fundamentals, diet, exercise, protein intake, sleep, hydration, drove the majority of their results, and that the levocarnitine addition felt like a minor enhancement at best.
Alternatives to the compounded blend
If you want the potential benefits of L-carnitine alongside your tirzepatide therapy but do not want to use a compounded blend, several alternatives exist.
Separate oral supplementation
Taking oral L-carnitine or acetyl-L-carnitine as a standalone supplement while using standard tirzepatide (whether compounded or brand-name) is the most straightforward alternative. Oral L-carnitine has lower bioavailability than injectable forms (approximately 15-25% absorption versus near-complete absorption for injectables), which is why oral doses need to be higher. The standard oral dose for weight management is 1,000-2,000 mg daily, typically split into two doses taken with meals.
The advantage is flexibility and cost. You can adjust the L-carnitine dose independently of your tirzepatide dose. You can stop it without changing your tirzepatide formulation. And over-the-counter L-carnitine supplements are significantly cheaper than the compounded blend premium.
Separate injectable L-carnitine
Some providers offer standalone injectable L-carnitine (often as intramuscular injections) alongside GLP-1 therapy. This approach allows independent dosing and scheduling while providing the higher bioavailability of injectable administration. The downside is an additional injection, which some people find burdensome.
Dietary sources
Red meat (especially beef and lamb) is the richest dietary source of L-carnitine, providing roughly 56-162 mg per 3-ounce serving. Fish, poultry, and dairy products also contribute smaller amounts. Vegetarian and vegan individuals have lower average L-carnitine levels but typically do not develop deficiency because the body synthesizes sufficient amounts endogenously.
If you are eating adequate protein from animal sources during your tirzepatide therapy, you are likely getting a baseline of dietary L-carnitine that, combined with endogenous production, may be sufficient. The question of whether additional supplementation provides meaningful benefit on top of adequate dietary intake and normal endogenous production is exactly where the evidence gets thin.
Questions to ask your provider
If you are considering the tirzepatide levocarnitine blend, going into the conversation with your healthcare provider prepared improves the quality of guidance you receive. Here are specific questions worth asking.
How much levocarnitine is in each dose of the blend? This matters because dosing varies dramatically between pharmacies, and without knowing the amount, you cannot evaluate whether it is in the range shown to be effective in research (1,000-2,000 mg daily oral equivalent).
What specific clinical evidence supports using this combination over plain tirzepatide? A knowledgeable provider will be honest about the limitations of the evidence rather than repeating marketing claims.
Is the compounding pharmacy operating within current FDA regulations? Given the rapidly changing regulatory landscape, this question protects you from unknowingly using a product from a non-compliant source.
Can I achieve the same potential benefit by taking oral L-carnitine separately? If the provider cannot articulate a clear advantage of the injectable blend over separate supplementation, the added cost may not be justified.
What is the cost difference between the blend and plain compounded tirzepatide? Transparency about pricing allows you to make an informed cost-benefit decision.
How are my lab results and body composition being monitored? Any provider prescribing compounded GLP-1 formulations should be tracking your progress with periodic bloodwork and, ideally, body composition measurements (DEXA scan or bioimpedance) rather than relying solely on scale weight.
The providers worth trusting are the ones who present the evidence honestly, acknowledge the limitations, and focus on the fundamentals rather than upselling additives.
The bottom line on tirzepatide levocarnitine blends
The tirzepatide levocarnitine blend is not a scam and it is not a breakthrough. It is a compounded formulation that combines a proven, powerful weight loss medication with a well-studied but modestly effective metabolic supplement. The tirzepatide component does the heavy lifting. The levocarnitine component may provide a marginal enhancement, particularly for fat oxidation efficiency and potentially for lean mass preservation, but the evidence for the specific combination is theoretical rather than proven.
The strongest version of the argument for this blend is that L-carnitine has documented effects on fatty acid transport and oxidation, tirzepatide creates a metabolic state where enhanced fatty acid oxidation could theoretically be beneficial, and combining them in a single injection is convenient. The weakest part of the argument is that no clinical trial has ever tested this specific combination, the additive effect of levocarnitine on top of tirzepatide substantial metabolic impact may be negligible, and the cost premium is not clearly justified by the expected benefit.
If you are using this blend and feeling good about your results, there is no compelling reason to switch away from it. If you are considering it and the cost is not a barrier, it is unlikely to harm you and may provide a small benefit. But if budget is a consideration, the same potential L-carnitine benefit can be achieved more cheaply through oral supplementation alongside standard tirzepatide.
For researchers serious about optimizing their weight loss protocols, SeekPeptides provides comprehensive guides, evidence-based protocols, and detailed analysis of every major compounded GLP-1 formulation. The platform gives members access to dosing calculators, comparison tools, and a community of experienced researchers who have navigated these exact decisions.
Frequently asked questions
Is the tirzepatide levocarnitine blend FDA approved?
No. The blend is a compounded formulation, not an FDA-approved product. While tirzepatide itself is FDA-approved (as Mounjaro and Zepbound), the combination with levocarnitine is a compounded product that has not undergone FDA review for safety or efficacy. Compounded medications are prepared by pharmacies under state and federal regulations, but they are not held to the same approval standards as commercially manufactured drugs.
How much weight can I lose on the tirzepatide levocarnitine blend?
Weight loss expectations should be based primarily on the tirzepatide component. Clinical trials show average weight loss of 15-22.5% of body weight over 72 weeks with tirzepatide alone. The levocarnitine addition may modestly enhance the proportion of weight lost from fat versus muscle, but it is not expected to significantly increase total weight loss. See the tirzepatide weight loss timeline for detailed month-by-month expectations.
Can I take oral L-carnitine instead of using the compounded blend?
Yes. Oral L-carnitine supplementation at 1,000-2,000 mg daily can achieve similar blood levels, though oral bioavailability is lower (15-25%) compared to injectable forms. Many people choose this approach because it is cheaper and allows independent dosing. The supplements to take with tirzepatide guide covers compatible supplementation strategies.
Does the levocarnitine prevent muscle loss during tirzepatide use?
L-carnitine may modestly improve the ratio of fat loss to muscle loss by enhancing fatty acid oxidation, reducing the body reliance on protein breakdown for energy. However, the evidence is limited and the effect size is small. Resistance training and adequate protein intake (1.0-1.6 g/kg/day) are far more effective strategies for muscle preservation during weight loss.
What are the side effects of the tirzepatide levocarnitine blend?
Side effects are primarily driven by tirzepatide and include nausea, vomiting, diarrhea, constipation, decreased appetite, and abdominal discomfort. Levocarnitine may add mild GI effects, increased injection site irritation, and rarely a fishy body odor at higher doses. The overlapping GI side effect profiles mean some users experience slightly worse tolerability than with plain tirzepatide.
How much does the tirzepatide levocarnitine blend cost?
The blend typically costs $20-80 more per month than plain compounded tirzepatide. Exact pricing varies significantly between pharmacies. Compare this premium to the cost of separate oral L-carnitine supplementation ($15-30/month) when evaluating whether the convenience of a single injection justifies the added expense.
Can I switch from plain tirzepatide to the levocarnitine blend?
Yes, if your prescriber supports the switch and a compliant compounding pharmacy offers the formulation. The tirzepatide dose should remain the same during the switch. You would simply be adding levocarnitine to your existing tirzepatide protocol. Monitor for any changes in side effects during the first few weeks after switching.
Is the tirzepatide levocarnitine blend better than tirzepatide with B12?
They serve different purposes. The levocarnitine blend targets fat metabolism and potential muscle preservation. The B12 blend addresses vitamin deficiency risk and general energy support. Neither has strong evidence proving superiority over plain tirzepatide. Your choice should depend on your specific concerns, symptoms, and health profile.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your protocols stay optimized, your muscle stay preserved, and your fat oxidation stay efficient.