Feb 28, 2026

What if the injection site you have been using is quietly undermining your weight loss results?
It sounds dramatic. Maybe even a little paranoid. But here is the thing most people never consider when they start a GLP-1 injection protocol for weight loss: the FDA approves three different injection sites for every GLP-1 receptor agonist on the market. Three. And while the official guidance says they are all equivalent, the real-world experience of thousands of researchers tells a more nuanced story. Some sites absorb faster. Some cause fewer side effects. Some work better for people with more subcutaneous tissue, while others suit leaner body types. The difference between a good injection site and the optimal one might not show up in a single dose, but over weeks and months of consistent use, small advantages compound into meaningful outcomes.
This guide breaks down everything you need to know about choosing, rotating, and optimizing your GLP-1 injection site specifically for weight loss. Whether you are using semaglutide, tirzepatide, retatrutide, or liraglutide, the principles remain the same. You will learn which site absorbs fastest, which causes the least discomfort, how to rotate properly so your medication keeps working as intended, and what mistakes to avoid that could silently reduce your results. SeekPeptides members have been asking these questions for months, and the answers are more interesting than you might expect.
Why your injection site matters more than you think
Most injection guides treat site selection as an afterthought. Pick a spot. Inject. Move on. But the pharmacokinetics of subcutaneous peptide delivery depend on several factors that vary by location, and understanding these factors gives you an edge that compounds over time.
How subcutaneous absorption actually works
When you inject a GLP-1 medication subcutaneously, the drug enters the fatty tissue layer beneath your skin. From there, it gradually absorbs into your bloodstream through a network of tiny capillaries. The speed of this absorption depends on three things: local blood flow, the thickness of the subcutaneous fat layer, and the degree of lymphatic drainage in that area.
Blood flow matters most. Regions with higher blood flow deliver medication to your bloodstream faster, which means the active compound reaches peak concentration sooner. Research on subcutaneous peptide injections shows that abdominal subcutaneous blood flow runs roughly 30% higher than femoral (thigh) blood flow, and this difference persists for at least six hours after eating.
That is not a trivial difference.
For medications like semaglutide and tirzepatide, which have long half-lives measured in days rather than hours, the total amount absorbed remains essentially the same regardless of site. Eli Lilly confirmed this in their Phase 1 pharmacokinetic study: no clinically relevant differences in total tirzepatide exposure between the abdomen, thigh, and upper arm. But the absorption profile, how quickly the medication reaches peak levels and how gradually it tapers, does shift slightly depending on where you inject.
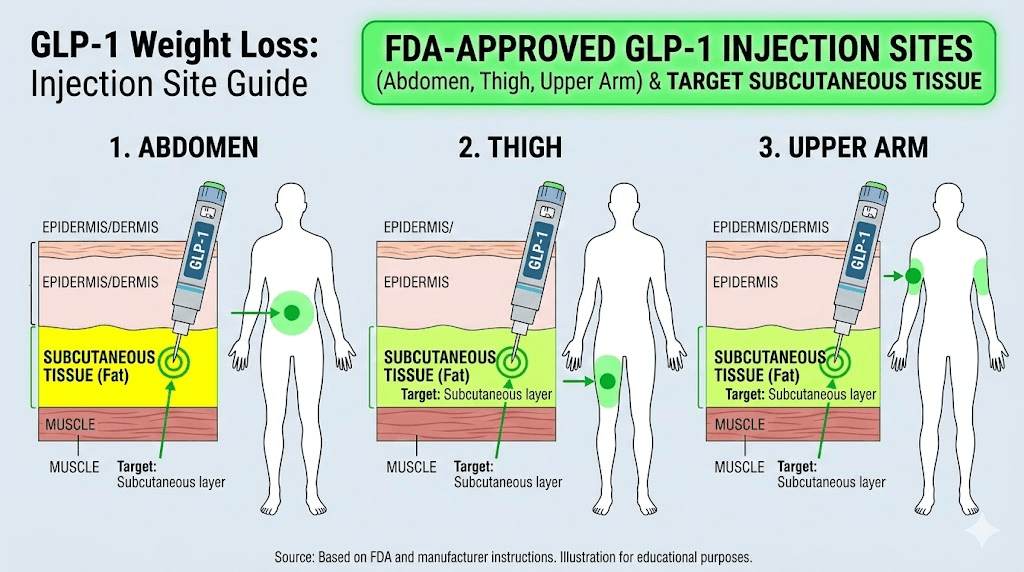
The three FDA-approved injection sites
Every GLP-1 receptor agonist currently approved for weight loss uses the same three injection sites. The abdomen. The front of the thigh. The back of the upper arm. These locations were selected because they provide adequate subcutaneous tissue depth for reliable absorption, easy access for self-administration, and relatively low risk of hitting blood vessels or nerves.
But "approved" does not mean "identical." Each site has distinct characteristics that affect comfort, absorption speed, side effect likelihood, and practical usability. Understanding these differences lets you make informed choices rather than random ones, and that matters when you are committing to a long-term weight loss protocol that may span months or even years.
The abdomen: the most popular GLP-1 injection site for weight loss
Ask experienced GLP-1 users where they prefer to inject, and the majority will point to their stomach. There are good reasons for this popularity, backed by both research and practical experience.
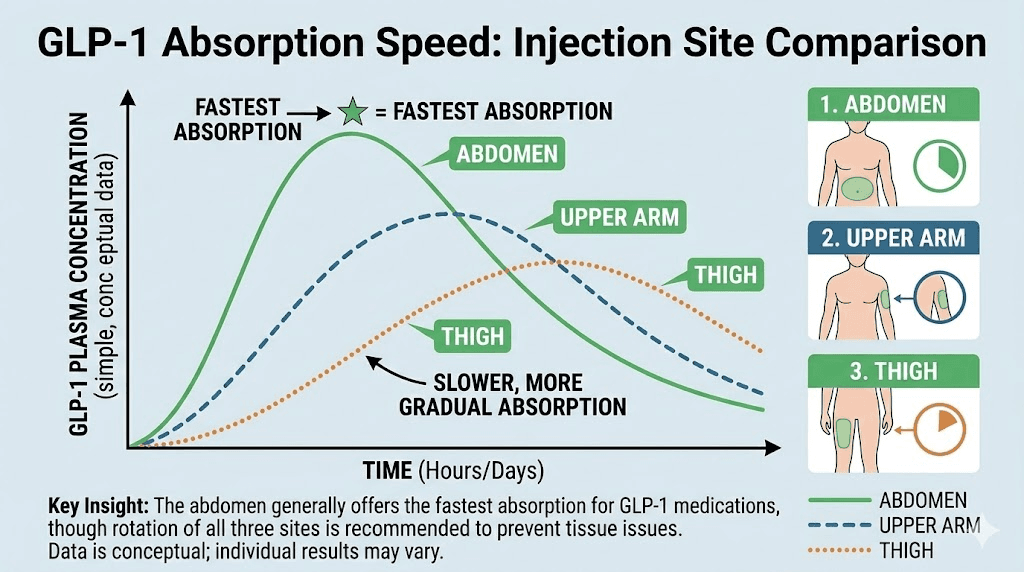
Absorption rate and blood flow advantage
The abdomen offers the fastest absorption of any approved injection site for subcutaneous medications. Studies on insulin, a closely related class of injectable peptides, show that peak concentration (Cmax) is approximately 28% higher and occurs more than twice as fast when injected in the abdomen compared to the thigh. Research on human growth hormone confirms the pattern: maximum serum concentration arrived at 4.26 hours from the abdomen versus 5.89 hours from the thigh.
Why? The abdominal wall has significantly higher subcutaneous blood flow. This means more capillaries carrying medication into your systemic circulation per unit of time. For GLP-1 medications specifically, this faster absorption can translate to a slightly quicker onset of appetite suppression after each dose, which is directly relevant when your goal is fat loss.
But faster is not always better. Some users report that abdominal injections of tirzepatide or semaglutide produce stronger initial nausea compared to thigh injections, likely because of this faster absorption profile. The medication hits the system more quickly, triggering gastrointestinal side effects more intensely in the first few hours after injection.
Proper abdominal injection technique
Getting the technique right matters as much as choosing the right site. For abdominal injections, follow these guidelines:
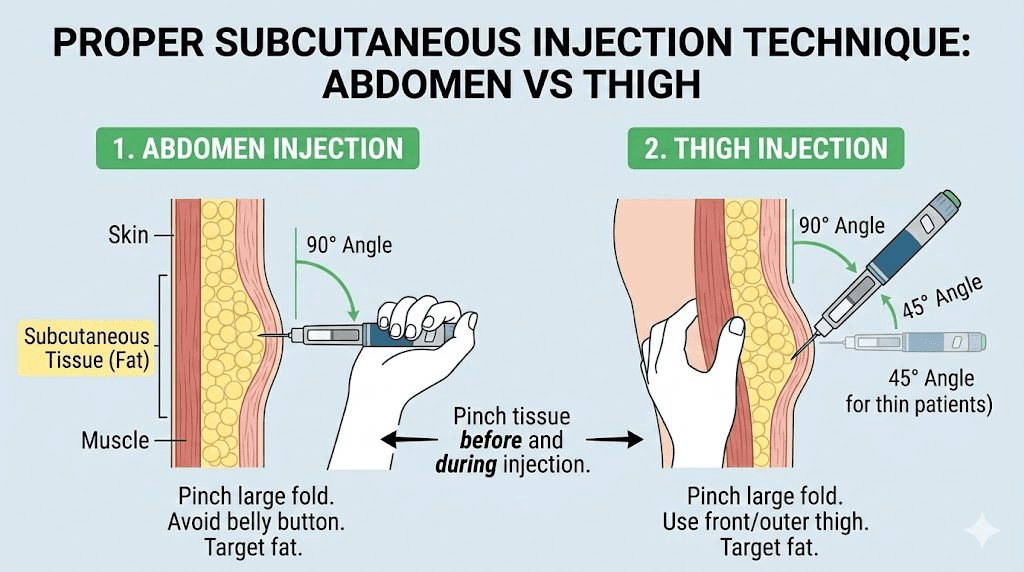
Stay at least two inches away from your belly button in all directions. The tissue directly around the navel is thinner and more vascular, which increases bruising risk and can lead to inconsistent absorption. The best zone forms a wide band across the lower and mid-abdomen, roughly from hip bone to hip bone.
Pinch the skin gently before inserting the needle. This lifts the subcutaneous layer away from the underlying muscle, ensuring the medication deposits into fat rather than muscle tissue. Intramuscular injection causes faster, less predictable absorption and more post-injection pain. A proper syringe injection technique keeps everything in the right layer.
Insert at a 90-degree angle for most body types. If you have very little abdominal fat, a 45-degree angle works better. Use a properly sized syringe with a 30-31 gauge needle, 4-6mm in length, for maximum comfort.
Who benefits most from abdominal injection
The abdomen works best for people with moderate to high levels of abdominal subcutaneous fat. If you can pinch at least an inch of tissue in the injection zone, this site will deliver consistent, reliable absorption. It is also the easiest site for self-administration since you have direct visual access and full range of motion with both hands.
People who are very lean in the abdominal area, particularly men with low body fat percentages, may find this site less comfortable and should consider the thigh as their primary site instead. As your weight loss progresses and abdominal fat decreases, you may need to transition to other sites or adjust your technique to maintain proper subcutaneous delivery.
The thigh: slower absorption with fewer side effects
The front of the thigh is the second most popular injection site, and it has advantages that make it the preferred choice for a significant subset of GLP-1 users.
Why some researchers prefer the thigh
Thigh injections produce a slightly slower, more gradual absorption curve compared to the abdomen. For some users, this translates to milder gastrointestinal side effects. Anecdotal reports across peptide research communities consistently note less nausea when injecting tirzepatide in the thigh versus the abdomen. The theory is straightforward: slower absorption means a gentler onset of the medication effects, reducing the sharp spike that can trigger bloating and nausea in sensitive individuals.
This matters. A lot.
Side effects are the number one reason people discontinue GLP-1 medications before achieving their weight loss goals. If thigh injection reduces nausea enough to keep you compliant with your protocol, the slightly slower absorption becomes irrelevant compared to the benefit of actually staying on treatment. Compliance beats optimization every single time.
Proper thigh injection technique
Use the front and outer portions of the thigh, roughly in the middle third between your hip and knee. Avoid the inner thigh entirely, as this area has more blood vessels and nerves, making injections more painful and increasing bruising risk. Also avoid injecting too close to the knee or too high near the hip crease.
The thigh typically has more subcutaneous tissue than people realize, even in relatively lean individuals. This makes it a reliable backup when abdominal fat decreases during your weight loss journey. Sit down and relax the leg muscle completely before injecting. Tension in the quadriceps can cause the needle to penetrate into muscle rather than fat, which changes the absorption profile and increases discomfort.
The same needle specifications apply: 30-31 gauge, 4-6mm length, inserted at 90 degrees with a gentle skin pinch. Make sure you are using the correct syringe technique for consistent results.
Thigh injection for different body types
The thigh is particularly well-suited for people who carry more fat in their lower body. Women, who tend to store more subcutaneous fat in the thighs and hips, often find this site more comfortable than the abdomen. The tissue depth provides excellent cushioning for the needle, and the larger surface area makes site rotation easier.
For men with athletic builds and low thigh fat, the outer thigh usually provides enough tissue depth. The key is finding spots where you can pinch at least half an inch of skin and fat. If you struggle to do this, the abdomen may be a better primary site for your body type.
As weight loss progresses, monitor your thigh tissue depth periodically. Some people lose significant thigh fat during GLP-1 treatment, particularly those on higher doses of tirzepatide or retatrutide, which can reduce the suitability of this site over time.
The upper arm: convenient but challenging for self-injection
The back of the upper arm is the third FDA-approved site, and it occupies a unique position in the site rotation discussion.
When the upper arm makes sense
The upper arm offers a middle ground in absorption characteristics, falling between the abdomen and thigh in most pharmacokinetic comparisons. It provides adequate subcutaneous tissue in the triceps area, and many users find it less sensitive to needle insertion than either the abdomen or thigh.
The catch? Self-injection in the upper arm is difficult. Reaching around to the back of your own arm with a syringe requires significant flexibility and coordination. You lose visual contact with the injection site, which increases the risk of hitting muscle tissue instead of the subcutaneous layer. For this reason, the upper arm is most practical when someone else administers the injection for you, or when you are using a pre-filled pen device that simplifies the process.
That said, if you have a partner willing to help with injections, or if you are comfortable with the technique, the upper arm provides valuable real estate for your injection rotation schedule. Having three viable sites instead of two gives your skin more recovery time between injections in the same area.
Upper arm technique tips
Target the fleshy area at the back of the upper arm, roughly midway between the shoulder and elbow. Avoid the deltoid area on top of the shoulder, which has less subcutaneous tissue and more muscle. The tissue should feel soft and pinchable, not firm or muscular.
If self-injecting, use your non-dominant hand to pinch the tissue while your dominant hand operates the syringe. Some users find it helpful to rest their arm against a table or doorframe to stabilize the tissue. Keep the muscle completely relaxed, as tensing the triceps will thin the subcutaneous layer and increase the chance of intramuscular injection.
The upper arm tends to be more visible than the abdomen or thigh for injection site reactions like redness or bruising. If cosmetic concerns matter to you, factor this into your rotation plan. Minor bruising that disappears in a day or two on your stomach might be more noticeable on a bare arm.
Head-to-head comparison: which site works best for weight loss?
Let us cut through the noise and compare all three sites directly. The honest answer is that no single site produces dramatically better weight loss outcomes than the others, but there are meaningful differences that should inform your strategy.
What the pharmacokinetic research shows
Eli Lilly published a Phase 1 study specifically examining tirzepatide absorption across all three injection sites. The results showed no clinically relevant differences in total exposure (AUC) between the abdomen, thigh, and upper arm. Peak blood concentration occurred between 8 and 72 hours post-injection regardless of location, and the total amount of medication entering the bloodstream was equivalent.
Semaglutide data tells a similar story. Clinical trials for both Ozempic and Wegovy demonstrated consistent weight loss outcomes without site-dependent variations. The best injection site for semaglutide pharmacokinetics appears to be the abdomen by a small margin, but the clinical difference is negligible.
So if total drug exposure is the same, why does site selection matter at all?
Because weight loss is not just about pharmacokinetics. It is about compliance, comfort, side effect management, and sustainable long-term habits. The site that keeps you injecting consistently, week after week, is the best site for weight loss. Period.
Site comparison table
Factor | Abdomen | Thigh | Upper arm |
|---|---|---|---|
Absorption speed | Fastest | Moderate | Moderate |
Total drug absorbed | Same | Same | Same |
Nausea likelihood | Higher | Lower | Moderate |
Self-injection ease | Easy | Easy | Difficult |
Pain level | Low-moderate | Low | Low |
Bruising risk | Moderate | Low-moderate | Moderate |
Available surface area | Large | Large | Small |
Visibility of reactions | Hidden | Mostly hidden | Visible |
Best for | Most users | Nausea-sensitive | Rotation |
The takeaway is clear. Start with the abdomen for most people. Switch to the thigh if nausea is a problem. Add the upper arm to your rotation once you are comfortable with the injection process. This three-site strategy gives you the best combination of effectiveness and sustainability for long-term fat loss.
The compliance factor
Here is something the research papers rarely discuss. The best injection site is the one you will actually use. Consistently. Week after week.
If abdominal injections make you anxious, if looking at the needle going into your stomach triggers dread, then the thigh is your best site regardless of what the pharmacokinetic data says. If you have been experiencing redness and itching at your injection site, switching locations might solve the problem entirely. Psychological comfort matters. Fear and anxiety around injections cause people to skip doses, delay their protocol, or quit altogether.
A skipped dose does far more damage to your weight loss results than choosing a slightly less optimal injection site ever could.
Injection site rotation strategies for sustained weight loss
Rotation is not optional. It is essential. And getting it wrong can directly impact how well your medication works over time.
Why rotation prevents absorption problems
Injecting repeatedly in the same spot causes localized tissue changes. The body responds to repeated needle trauma by forming fibrous tissue, tiny areas of scarring that alter the local architecture of the subcutaneous layer. Over time, these changes can develop into lipodystrophy, a condition where fatty tissue either builds up (lipohypertrophy) or wastes away (lipoatrophy) at the injection site.
Both forms are bad news for weight loss.
Lipohypertrophy creates hardened lumps that absorb medication unpredictably. Your dose might absorb fully one week and partially the next, leading to inconsistent appetite suppression and unpredictable appetite control. Lipoatrophy reduces the subcutaneous tissue available for injection, potentially forcing medication into muscle where absorption characteristics differ entirely. Either way, your carefully calibrated dosage protocol gets disrupted.
Research on insulin-dependent patients, who inject far more frequently than weekly GLP-1 users, shows that proper rotation reduces lipodystrophy incidence by over 80%. The principle applies equally to all injectable peptides.
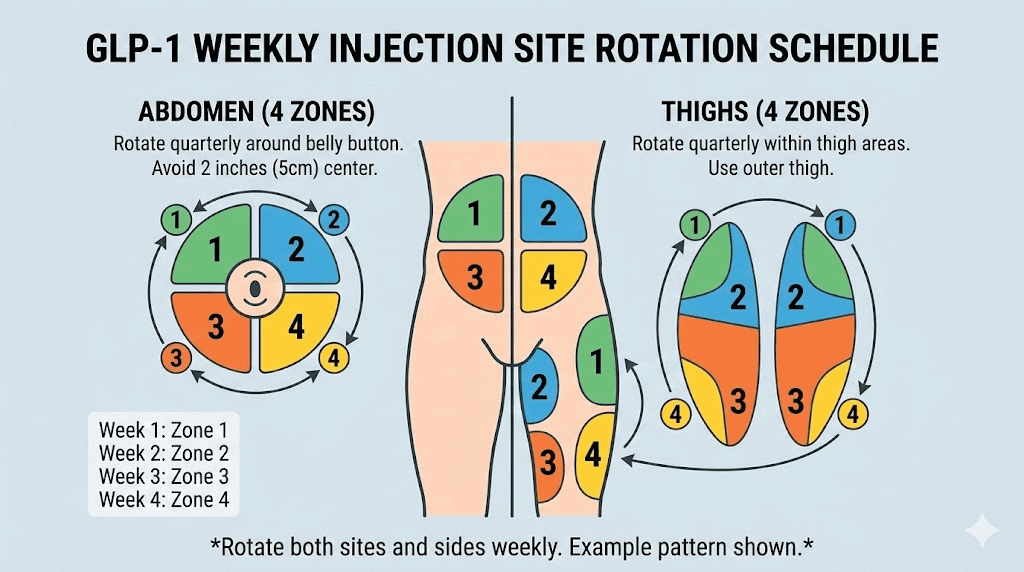
The three-zone rotation system
The simplest effective rotation system uses a three-zone approach. Divide your available injection area into three broad zones: left abdomen, right abdomen, and alternating thighs. If you also use the upper arm, you have four zones.
Rotate zones with each weekly injection. Week one: left abdomen. Week two: right thigh. Week three: right abdomen. Week four: left thigh. This gives each zone a full month of recovery between injections, more than enough time for complete tissue healing.
Within each zone, vary the exact spot by at least one inch from the previous injection in that area. Some people find it helpful to mentally divide each zone into a grid pattern, moving systematically from one grid square to the next. Others simply pick a different spot each time, making sure they maintain adequate distance from the last injection point.
Tracking your injection sites
Keep a simple log. Nothing complicated. Just record the date, the zone (left abdomen, right thigh, etc.), and any notes about comfort or reactions. This prevents you from accidentally favoring one site, a habit that develops more easily than you might think.
Some SeekPeptides members use a simple body diagram they print out and mark with each injection date. Others track it in a phone note. The format does not matter. What matters is that you rotate deliberately rather than defaulting to the same comfortable spot every week.
If you notice any area developing hardness, discoloration, or persistent tenderness, avoid that zone entirely for at least eight weeks. These are early signs of tissue changes that will worsen if you continue injecting there. Your injection technique might also need adjustment if you experience these issues frequently.
Rotation when switching medications
If you are switching between GLP-1 medications, maintain your rotation schedule without interruption. The tissue does not care which specific medication was injected there, only that it was punctured and exposed to a foreign substance. A spot that received tirzepatide last week needs the same recovery time before receiving semaglutide as it would before receiving another dose of tirzepatide.
The same principle applies when converting from semaglutide to tirzepatide or when transitioning between compounded and brand-name formulations. Rotation protects the tissue regardless of what you are injecting.
Common injection site problems that sabotage weight loss
Even with proper rotation, injection site issues can arise. Knowing how to identify and manage them quickly prevents disruptions to your weight loss protocol.
Lipodystrophy and nodule formation
Subcutaneous nodules can form after GLP-1 injections, particularly with longer-acting formulations. A study published in the Endocrine Society journals documented nodule formation with once-weekly exenatide, noting that nodules were typically 0.5 to 0.75 centimeters in diameter and tended to resolve on their own over time. The risk is considered small for semaglutide and tirzepatide, but it exists.
If you feel a firm lump under the skin at a previous injection site, do not inject into it or near it. Mark the area mentally and avoid it for at least two to three months. Injecting into a nodule produces unpredictable absorption, which means your carefully calibrated dose might deliver half or double the intended effect. Neither outcome helps your weight loss.
Lipohypertrophy, the buildup of fatty lumps from repeated injections, is more common in people who do not rotate adequately. These areas can grow from barely noticeable to marble-sized if the same spot keeps getting used. Treatment is simple: stop injecting there and wait. In severe cases, the tissue may need months to fully normalize.
Injection site reactions
Redness, itching, swelling, and minor bruising occur in approximately 1.4% of semaglutide users and 2.4% of tirzepatide users. These reactions are usually mild and self-limiting, resolving within a day or two. But they can affect absorption if inflammation alters local blood flow patterns.
To minimize reactions, let alcohol swabs dry completely before injecting. Wet alcohol entering the subcutaneous tissue causes stinging and local inflammation. Use a fresh needle every time, as reused needles develop microscopic burrs that tear tissue rather than puncturing cleanly. Apply gentle pressure for 30 seconds after removing the needle, but do not rub. Rubbing disperses the medication unevenly and increases bruising.
If you experience persistent injection site reactions, try switching to a different body region entirely. Some people react to abdominal injections but tolerate thigh injections perfectly, or vice versa. The local immune response can vary by location.
Bruising and its effect on absorption
Bruising at the injection site is mostly cosmetic, but large bruises can trap medication in the tissue, slowing absorption. People taking blood thinners like aspirin, warfarin, or apixaban are at higher risk for significant bruising. If you are on anticoagulant therapy, the thigh may be your best primary site since it tends to bruise less than the abdomen.
Cold application before and after injection reduces both bruising and discomfort. A systematic review found that applying a cold compress to the injection site for 30-60 seconds before injection significantly reduced bruising incidence and pain scores. This simple step costs nothing and takes barely a minute, yet most people skip it.
If you are experiencing frequent bruising despite proper technique, evaluate your needle gauge. Switching from a 29-gauge needle to a 31 or 32-gauge needle reduces tissue displacement and capillary damage. The thinner needle makes a smaller hole, which means less bleeding and less bruising. For semaglutide syringe injections, a 31-gauge needle at 4-6mm length is the sweet spot between comfort and reliability.
Technique optimization for maximum absorption
The difference between a good injection and a great one comes down to technique details that take seconds to execute but significantly impact results.
Needle selection for GLP-1 injections
Needle gauge and length directly affect comfort, accuracy, and absorption consistency. For all GLP-1 subcutaneous injections, the recommended specifications are:
Gauge: 30 to 32 gauge. Higher gauge numbers mean thinner needles. A 31-gauge needle is thin enough to minimize pain while strong enough to penetrate subcutaneous tissue reliably. Pre-filled pens like Ozempic and Mounjaro typically use 31 or 32-gauge needles. If you are using a vial and syringe for reconstituted semaglutide or reconstituted tirzepatide, select a 31-gauge insulin syringe.
Length: 4 to 8mm for most adults. Shorter needles (4-5mm) work well for most body types and reduce the risk of intramuscular injection. Longer needles (6-8mm) may be necessary for areas with very thick subcutaneous tissue. The goal is to deposit the medication in the middle of the fat layer, not too shallow (which causes leakage) and not too deep (which hits muscle).
The pinch technique
Pinching the skin before injection is not just about comfort. It serves a mechanical purpose. By lifting the subcutaneous tissue away from the muscle layer, you create a thicker target zone for the needle. This is especially important in leaner individuals or at sites with less natural fat padding.
Use your thumb and index finger to create a gentle fold of skin. Do not squeeze hard, as excessive pressure pushes blood out of the local capillaries and can alter absorption. The pinch should be firm enough to lift the tissue but gentle enough that the skin does not turn white from pressure.
Release the pinch after the needle is fully inserted but before pressing the plunger. This allows the tissue to return to its natural position around the needle tip, ensuring the medication deposits into the center of the subcutaneous layer rather than along the needle track.
Temperature matters
Cold medication stings more and may absorb slightly slower than room-temperature medication. If you store your GLP-1 medication in the refrigerator, remove it 15-30 minutes before injection to let it warm toward room temperature. Do not use a microwave, hot water, or any external heat source, as this can denature the active peptide.
This warming step reduces injection discomfort noticeably. Cold fluid entering warm tissue causes vasoconstriction (blood vessel narrowing) at the injection site, which can slow initial absorption and increase the sensation of pressure. Room-temperature medication flows more smoothly through the needle and disperses more readily in the tissue.
For tirzepatide storage and semaglutide storage, always follow the manufacturer guidelines regarding refrigeration versus room temperature storage. Most compounded formulations need refrigeration between uses but should be warmed briefly before injection.
Injection speed
Push the plunger slowly and steadily. Rapid injection forces medication into the tissue faster than it can accommodate, creating a pressurized pocket that causes pain and can push medication back out through the needle track. A slow, 5-10 second injection allows the tissue to expand gradually and accept the fluid without resistance.
After completing the injection, hold the needle in place for 5-10 seconds before withdrawing. This prevents medication from leaking back out through the needle hole. If you notice a drop of liquid on your skin after removing the needle, you either withdrew too quickly or injected too fast. Neither issue is dangerous, but both waste small amounts of medication that should be in your system working toward your fat loss goals.
How body composition affects your best injection site
Your body is not static. It changes as you lose weight, and those changes affect which injection site works best at different stages of your journey.
Starting at higher body weight
If you are beginning your GLP-1 protocol at a higher body weight, you likely have ample subcutaneous tissue at all three injection sites. This is actually an advantage. You have maximum flexibility in site rotation, plenty of tissue depth for reliable absorption, and lower risk of accidental intramuscular injection.
The abdomen is typically the best starting site at higher body weights. The abundant subcutaneous tissue ensures consistent medication delivery, and the large surface area makes rotation easy. Many people starting their first week on semaglutide or their starting dose of tirzepatide find abdominal injection the most straightforward and comfortable option.
During active weight loss
As you lose weight, subcutaneous fat distribution shifts. The abdomen typically loses fat faster than the thighs for men, while women often lose fat more evenly or lose thigh fat first. These changes mean your preferred injection site may need to change too.
Monitor the tissue depth at each site periodically. If the pinch test produces less than half an inch of tissue at your usual spot, consider transitioning to a site with more subcutaneous depth. For many people experiencing significant weight loss on tirzepatide compound protocols, the thigh becomes the primary injection site as abdominal fat decreases.
This transition is normal and expected. It does not mean anything is wrong. It simply means your body composition has changed enough to warrant adjusting your injection approach.
At maintenance weight
Once you reach your target weight and transition to a maintenance protocol, your available subcutaneous tissue may be noticeably less than when you started. This is when three-site rotation becomes most important. Using all three approved sites spreads the injection load across maximum available tissue, reducing the risk of localized problems at any single site.
Some people at maintenance weight find that certain sites no longer have adequate tissue depth. If you can not comfortably pinch half an inch of tissue at a site, remove it from your rotation and focus on the remaining sites. Two well-rotated sites are better than three sites where one consistently delivers medication into muscle.
Medication-specific injection site guidance
While all GLP-1 medications use the same three injection sites, each medication has subtle differences worth considering when choosing your primary site.
Semaglutide (Ozempic and Wegovy)
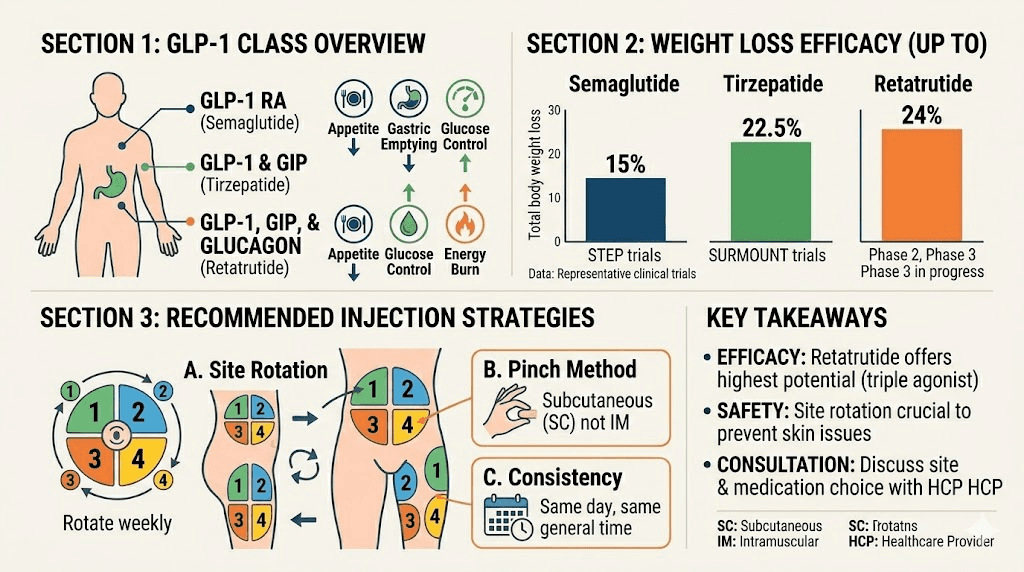
Semaglutide is the most widely used GLP-1 receptor agonist for weight loss. The STEP clinical trials demonstrated mean weight losses of 14.9% to 17.4% in participants with overweight or obesity, with 69% to 79% achieving at least 10% weight loss. These results were consistent across injection sites.
For semaglutide, the abdomen is generally the preferred starting site due to its faster absorption and ease of access. The medication is available as a pre-filled pen (Ozempic/Wegovy) or as a compounded vial formulation. Both deliver the same active peptide, but the injection technique differs slightly between pen and syringe.
If you are using the semaglutide dosage calculator to determine your dose, remember that the calculated amount remains the same regardless of injection site. The site does not change the dose, only the absorption characteristics.
Users who experience nausea during the dose escalation phase often benefit from switching to thigh injection during the transition weeks when side effects peak. Once your body adjusts to the higher dose, you can return to abdominal injection if preferred.
Tirzepatide (Mounjaro and Zepbound)
Tirzepatide is a dual GIP/GLP-1 receptor agonist that has shown even greater weight loss in clinical trials compared to semaglutide. The SURMOUNT trials demonstrated up to 22.5% mean weight loss at the highest dose. As a more potent peptide, side effects can be more pronounced, making site selection strategically important.
The thigh may be particularly advantageous for tirzepatide users experiencing gastrointestinal side effects. The slightly slower absorption from this site can moderate the initial impact of each dose, reducing nausea intensity. Multiple community reports support this observation, particularly during the higher-dose phases of the escalation schedule.
Tirzepatide is available in both pen (Mounjaro/Zepbound) and compounded formulations. Compounded versions may have slightly different viscosity than the brand-name product, which can affect how the injection feels at different sites. Thicker solutions benefit from slightly slower injection speeds and warmer temperatures.
For detailed guidance on tirzepatide injection in specific sites, see our tirzepatide thigh injection guide and stomach injection guide.
Retatrutide
Retatrutide is a triple agonist (GIP/GLP-1/glucagon receptor) currently in late-stage clinical trials that has shown remarkable weight loss results of up to 24% in Phase 2 studies. While not yet commercially available, researchers working with this peptide follow the same injection site principles.
Because retatrutide activates three receptor types simultaneously, its gastrointestinal side effect profile can be more intense than single or dual agonists. Thigh injection may be the optimal starting site for retatrutide initiation, with gradual introduction of abdominal injection as tolerance develops. The retatrutide dosage calculator can help determine appropriate starting doses regardless of injection site choice.
For those comparing these medications, our comprehensive comparison guide covers the differences in mechanism, efficacy, and side effect profiles across all three.
Liraglutide (Saxenda)
Liraglutide requires daily injection rather than weekly, which makes site rotation even more critical. With seven injections per week instead of one, each site gets used far more frequently. A strict rotation schedule between abdomen, both thighs, and both upper arms gives each zone adequate recovery time.
The same absorption principles apply. Abdominal injection absorbs fastest, thigh is slower with potentially fewer side effects, and the upper arm falls in between. The main practical difference is that daily injectors burn through their site rotation faster and need to be more disciplined about spacing.
Timing your injection and site choice for optimal weight loss
When you inject matters too. And the timing question intersects with site selection in ways that can optimize your results.
Morning versus evening injection
Clinical trials show no statistically significant difference in weight loss outcomes between morning and evening GLP-1 injections. The medication has a long half-life that provides consistent blood levels throughout the week regardless of injection time. But your subjective experience can vary dramatically.
Morning injectors often report that the initial wave of appetite suppression hits during the day when they are most active and most tempted by food. Evening injectors sometimes experience nausea while sleeping, which disrupts rest without providing any appetite-suppression benefit since they are not eating anyway.
The best time to take your GLP-1 injection is whichever time you can maintain consistently week after week. If you choose morning injection, the abdomen may be your most practical site since you can inject while standing at the bathroom mirror. Evening injectors often prefer the thigh since they can inject while seated and relaxed.
Injection timing relative to meals
For injectable GLP-1 medications (as opposed to oral formulations), meal timing does not significantly affect absorption. The subcutaneous depot releases medication gradually over days, independent of your digestive activity. However, some users report less injection-related nausea when they inject after a light meal rather than on an empty stomach.
This observation aligns with the absorption science. A light meal in your stomach provides a buffer against the initial wave of GLP-1 receptor activation. The effect is subtle, but for people struggling with nausea and bloating, it can make a meaningful difference in comfort.
Weekly consistency matters more than day optimization
Choose your injection day and stick with it. The seven-day interval is not arbitrary. It corresponds to the pharmacokinetic profile of weekly GLP-1 medications, maintaining blood levels within the therapeutic range. Injecting early one week and late the next creates fluctuations that can increase side effects and reduce appetite suppression consistency.
If you need to shift your injection day, move it by one day at a time over several weeks rather than making a sudden change. And if you take your injection a day early occasionally, it will not derail your results, but making it a habit is not ideal.
Advanced strategies for maximizing weight loss through injection optimization
Once you have mastered the basics, these advanced strategies can squeeze additional benefit from your GLP-1 protocol.
Strategic site selection during dose escalation
Dose escalation is when most side effects occur. Your body is adjusting to increasing levels of GLP-1 receptor activation, and the first few days after each dose increase tend to be the roughest. During these transition weeks, switching to thigh injection can moderate the side effect spike.
Here is a practical approach. Use abdominal injection during weeks when you are on a stable dose and tolerating it well. When you increase your dose, switch to thigh injection for that week and the following week. Once the new dose stabilizes and side effects subside, return to abdominal injection. This alternating strategy gives you the absorption benefits of abdominal injection most of the time while protecting against excessive side effects during transitions.
Combining site strategy with dietary timing
Your diet plan and injection site choice can work together. If you inject in the abdomen (faster absorption) on a day when you have social eating events planned, the stronger initial appetite suppression may help you make better food choices during meals. If you inject in the thigh (slower absorption) on a quiet day at home, the gentler onset allows you to ease into the medication effects without disrupting your routine.
This level of optimization is not necessary for most people. But for those who have plateaued and are looking for every possible advantage to push past a weight loss stall, these small adjustments can contribute to breaking through.
Exercise and injection site selection
Exercise increases blood flow to working muscles and surrounding tissue. If you inject in your thigh and then go for a run, the increased leg blood flow may speed up absorption from that site. Similarly, abdominal exercises after an abdominal injection could theoretically increase local absorption speed.
The practical impact is minimal for weekly GLP-1 injections since the total absorption over seven days remains the same. But if you consistently exercise at the same time you inject, be aware that the absorption spike may be faster than expected. This is more relevant for managing side effects than for weight loss optimization. If you find that exercising after injection consistently triggers nausea, try injecting in a non-exercised body region or adjusting your workout timing relative to injection day.
Supplements and injection site interaction
Certain supplements taken alongside GLP-1 medications can affect injection site comfort. Omega-3 fatty acids and vitamin E, both mild blood thinners, may increase bruising at injection sites. This does not mean you should stop taking them, just be aware that bruising risk increases and adjust your technique accordingly.
B12 supplementation is common among GLP-1 users, and many compounded formulations now include B12 in the blend or tirzepatide with B12. These combination formulations inject identically to standalone versions. The B12 does not alter injection site preferences or rotation needs.
Troubleshooting injection site issues that stall weight loss
Weight loss stalls happen. And sometimes the injection site is the culprit nobody suspects.
When your medication stops working as well
If you have been stalling on semaglutide or tirzepatide is not working anymore, your injection site could be part of the problem. When the same area receives repeated injections, scar tissue and lipodystrophy can develop beneath the skin surface, invisible to the eye but tangible to the touch. These tissue changes create a depot that traps medication, releasing it erratically rather than smoothly.
The fix is straightforward. Move to a completely fresh injection site that has not been used in at least two months. If you have been rotating between just two spots on your abdomen, expand to include the thighs and upper arms. Many people experiencing apparent medication tolerance are actually experiencing absorption inconsistency from overused injection sites.
Persistent pain or discomfort
Some amount of injection discomfort is normal. A brief sting, mild pressure, occasional minor bruising. But persistent pain lasting hours or sharp pain during injection suggests a technique problem.
Check your needle gauge. Switching from 29-gauge to 31-gauge needles makes a noticeable difference in comfort. Verify your injection depth by using the pinch test before every injection. And make sure you are storing your medication properly, as degraded peptides can cause more injection site irritation than fresh ones.
If one site consistently hurts more than others, your anatomy may have a nerve or blood vessel near the surface at that location. This is normal anatomical variation. Simply avoid that specific spot and use nearby areas instead. You do not need to abandon an entire region because one particular point is sensitive.
Medication leakage after injection
Seeing a drop of clear liquid on your skin after withdrawing the needle is frustrating. It means some of your dose did not make it into the subcutaneous tissue. While the amount lost is typically tiny, repeated leakage adds up over time.
Three things cause leakage. Injecting too fast creates back-pressure that pushes fluid out. Withdrawing the needle immediately after injection does not give the tissue time to seal around the puncture. And using a needle that is too short can deposit medication too close to the skin surface where it escapes easily.
To fix this: slow your injection speed to 10 seconds for the full dose, hold the needle in place for 10 seconds after completing the injection, and consider using a slightly longer needle (6mm instead of 4mm) if leakage persists. These adjustments solve the problem for the vast majority of users.
Building your personalized injection site protocol
Now let us put everything together into a practical, personalized strategy you can implement starting with your next injection.
Step 1: assess your body composition
Stand in front of a mirror and perform the pinch test at each of the three injection sites. Pinch the tissue at your lower abdomen (two inches from the navel), the front of your mid-thigh, and the back of your upper arm. Note where you have the most and least subcutaneous tissue. Rank your sites from most tissue to least.
Step 2: choose your primary site
For most people, the site with the most subcutaneous tissue and easiest self-access becomes the primary site. This is usually the abdomen. But if you have less abdominal fat or experience significant nausea, the thigh is an excellent primary choice. The getting started guide covers initial injection site selection in detail.
Step 3: establish your rotation schedule
Map out your first month of injections across all viable sites. Write it down. Commit to following the schedule rather than defaulting to your comfort zone. A simple four-week rotation might look like this:
Week 1: Right abdomen
Week 2: Left thigh
Week 3: Left abdomen
Week 4: Right thigh
If you have a partner who can assist with upper arm injections, add week 5 and 6 as left and right upper arm. Then repeat the cycle.
Step 4: monitor and adjust
Track three things after each injection: site used, any reactions or discomfort (rated 1-10), and nausea level over the next 24 hours. After four weeks, you will have clear data showing which sites work best for your body. Use this data to refine your rotation, spending more time on sites that produce the least side effects and best overall experience.
Remember, SeekPeptides provides comprehensive protocol guidance for members who want personalized support with their injection optimization, including access to detailed rotation tracking tools and expert recommendations tailored to individual body types.
Step 5: reassess every 20 pounds of weight loss
As your body composition changes, repeat the pinch test and recalibrate your site rankings. A site that was perfect at your starting weight may have insufficient tissue depth after significant weight loss. Conversely, sites you avoided initially might become viable as your comfort with injection technique improves.
If you are tracking your progress with before and after documentation, note your injection sites alongside your results. This creates a personal dataset that helps you correlate site choices with weight loss outcomes over time.
Special considerations for different GLP-1 delivery methods
Not all GLP-1 medications come as traditional injections, and the delivery method affects site selection considerations.
Pre-filled pen devices versus vial and syringe
Pre-filled pens (Ozempic, Wegovy, Mounjaro, Zepbound) simplify the injection process significantly. The needle is shorter, the injection depth is pre-set, and the dose is dialed rather than drawn. These pens work well at all three injection sites but are particularly convenient for abdominal injection.
Vial and syringe injections, common with compounded formulations, require more technique but offer greater flexibility. You can choose your needle gauge and length, adjust injection depth based on the site, and control injection speed more precisely. This flexibility is an advantage for people who have found their optimal technique through experimentation.
If you are using compounded tirzepatide with glycine and B12 or semaglutide with glycine and B12, the combined formulation injects identically to standalone versions. The additives do not change optimal injection sites.
Oral versus injectable GLP-1 formulations
Oral GLP-1 formulations like oral tirzepatide and oral semaglutide drops eliminate the injection site question entirely. However, oral bioavailability is significantly lower than injectable, and absorption depends heavily on an empty stomach. The comparison between oral and injectable tirzepatide shows that injectable delivery remains the gold standard for maximum weight loss efficacy.
For those considering a switch between delivery methods, our guide on tirzepatide tablets versus injections covers the tradeoffs in detail.
GLP-1 patches
Transdermal GLP-1 delivery through patches like Onmorlo GLP-1 patches represents a newer approach that bypasses injection entirely. Patches deliver medication through the skin over extended periods, with application site affecting absorption rate similar to injection sites. The abdomen and upper arm are the most common patch application sites.
Frequently asked questions
Does injection site actually affect how much weight you lose?
The total amount of medication absorbed is the same regardless of injection site. Clinical data from Eli Lilly and Novo Nordisk confirms equivalent pharmacokinetic exposure across abdomen, thigh, and upper arm. However, the injection site indirectly affects weight loss through side effect management and compliance. A site that causes less nausea helps you stay on protocol longer, which directly impacts long-term results.
Can I always inject in the same spot if it works well?
No. Even if one spot feels perfect, repeated injection in the same location causes lipodystrophy over time. This creates hardened tissue that absorbs medication unpredictably, potentially reducing the effectiveness of your dosage protocol. Always rotate between at least two to three different sites.
Should I switch injection sites if I experience nausea?
Yes, switching from abdomen to thigh often reduces nausea intensity. The thigh absorbs GLP-1 medications slightly slower, producing a gentler onset of effects. This is particularly helpful during dose escalation periods when side effects tend to peak.
Is it safe to inject in the stomach during pregnancy?
GLP-1 medications are not recommended during pregnancy. If you discover you are pregnant while on a GLP-1 protocol, contact your healthcare provider immediately. For those planning pregnancy after GLP-1 use, our guide covers GLP-1 considerations around pregnancy and breastfeeding.
What needle size should I use for GLP-1 injection?
For subcutaneous GLP-1 injections, use a 30 to 32 gauge needle with 4 to 6mm length. This combination minimizes pain and bruising while ensuring proper subcutaneous delivery. Pre-filled pens come with appropriately sized needles. For vial and syringe injections of reconstituted semaglutide or reconstituted tirzepatide, 31-gauge insulin syringes are the standard choice.
How do I know if I injected into muscle instead of fat?
Intramuscular injection typically causes sharper pain during injection, more bleeding afterward, and sometimes a dull ache that persists for hours. If you suspect you hit muscle, the dose will still work but may absorb faster than intended. Avoid repeating the same technique at that spot. Review the proper injection technique and adjust your pinch and angle for next time.
Can I use numbing cream before GLP-1 injection?
Topical numbing creams (lidocaine-based) are safe to use before GLP-1 injections and will not affect medication absorption. Apply the cream 20-30 minutes before injection and wipe the area clean with an alcohol swab before injecting. This approach is particularly helpful for people with injection anxiety or needle sensitivity.
Does the injection site affect how long it takes for GLP-1 to work?
The injection site has a minimal effect on overall timeline. Whether you inject in the abdomen, thigh, or arm, you should notice appetite suppression starting within the first week and meaningful weight loss within the first month. The site affects the absorption curve of each individual dose, not the long-term treatment trajectory.
External resources
ScienceDirect: Impact of injection sites on subcutaneous peptide pharmacokinetics
NEJM: Once-weekly semaglutide in adults with overweight or obesity
For researchers serious about optimizing every aspect of their GLP-1 protocol, SeekPeptides offers the most comprehensive resource available, with evidence-based injection guides, personalized protocol builders, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your injection sites stay healthy, your rotation stay consistent, and your weight loss stay steady.