Apr 3, 2026

Experienced researchers share one piece of advice more than any other. Get the setup right. Not the dosing. Not the brand.
Not the injection site. The setup. Because everything that follows, every result, every side effect, every moment of confusion or confidence, traces back to how well you prepared before that first injection ever touched your skin.
Most people skip this part. They order a vial, watch a two-minute video, and wing it. Then they wonder why their reconstitution looks cloudy, why their dose feels off, why results take longer than expected. The gap between people who see results in two weeks and people who struggle for months often comes down to preparation.
This is not a quick-start card. This is the guide that covers everything. Supplies. Reconstitution. Storage. Your first injection. Diet preparation. Side effect management. Ongoing protocol optimization. Whether you are starting semaglutide, tirzepatide, or retatrutide, the fundamentals of a proper GLP-1 setup remain the same. And getting them right from day one saves you weeks of frustration, wasted peptide, and second-guessing.
SeekPeptides members consistently report that thorough preparation before their first dose made the biggest difference in their overall experience. This guide distills that collective knowledge into a single, comprehensive resource.
Understanding your GLP-1 medication before you start
Before you open a single package, you need to understand what you are working with. GLP-1 receptor agonists mimic a hormone your body already produces called glucagon-like peptide-1. This hormone signals your pancreas to release insulin, slows gastric emptying, and communicates with your brain to reduce appetite. The medications amplify this natural process.
Three main GLP-1 medications dominate the research landscape right now. Each works slightly differently, and understanding those differences shapes your entire setup process.
Semaglutide
Semaglutide targets the GLP-1 receptor exclusively. It is the most widely studied of the three, with extensive clinical trial data supporting its efficacy for weight management. Most compounded semaglutide comes in 3mg, 5mg, or 10mg vials as a lyophilized powder requiring reconstitution. The standard protocol involves weekly subcutaneous injections, starting at a low dose and titrating upward over several weeks.
For detailed dosing information, the semaglutide dosage in units guide breaks down exactly how to calculate your dose. The semaglutide dosage chart provides visual reference for each titration step.
Tirzepatide
Tirzepatide is a dual-action peptide. It targets both the GLP-1 receptor and the GIP receptor, which is glucose-dependent insulinotropic polypeptide. This dual mechanism often produces more pronounced appetite suppression and potentially greater weight loss compared to semaglutide alone. Compounded tirzepatide typically comes in 10mg, 15mg, 30mg, or 60mg vials.
The tirzepatide dosage in units guide covers the complete titration schedule, and the tirzepatide dosage chart makes unit calculations straightforward. If you are deciding between the two, our semaglutide vs tirzepatide comparison covers the key differences.
Retatrutide
Retatrutide goes one step further. It is a triple agonist, targeting GLP-1, GIP, and glucagon receptors simultaneously. Early clinical data suggests it may produce the most significant weight loss of the three, though it is newer to the research space and less widely available. Compounded retatrutide typically comes in 10mg or 20mg vials.
The retatrutide dosage chart for weight loss outlines the recommended titration, and you can learn more about the differences between tirzepatide and retatrutide if you are weighing your options.
Compounded vs. brand-name medications
Most researchers using GLP-1 medications at home work with compounded versions. These come as lyophilized (freeze-dried) powder in vials rather than pre-filled pens. This means you handle the reconstitution, dosing calculations, and injection preparation yourself. It sounds intimidating. It is not, once you understand the process.
The compounded semaglutide guide and compounded tirzepatide starting dose guide cover the specifics of working with compounded formulations.
The complete GLP-1 supply list
Getting your supplies organized before your medication arrives prevents scrambling and mistakes. Here is everything you need, broken into categories.
Essential supplies you cannot skip
Your GLP-1 medication vial. This is the lyophilized powder that contains your peptide. Verify the label matches what you ordered. Check the expiration date. Inspect the vial for cracks or damage. The powder should appear as a white or off-white cake at the bottom of the vial.
Bacteriostatic water (BAC water). This is your reconstitution diluent. Bacteriostatic water contains 0.9% benzyl alcohol, which prevents bacterial growth and allows you to draw multiple doses from the same vial over time. Do not use sterile water for multi-use vials. Sterile water lacks the preservative, meaning bacteria can grow after the first needle puncture. Our bacteriostatic water for peptides guide explains why this distinction matters.
Insulin syringes. You need two types. A larger syringe (1mL or 3mL) with a longer needle (18-21 gauge) for drawing bacteriostatic water and injecting it into the vial during reconstitution. And smaller insulin syringes (0.3mL or 0.5mL, 29-31 gauge) for your actual injections. The 31-gauge needle is the thinnest and causes the least discomfort. Most researchers prefer 0.5mL 29-gauge or 31-gauge insulin syringes for daily dosing.
Alcohol swabs. You will use these to clean the rubber stoppers on both your medication vial and bacteriostatic water vial before every puncture. You will also clean your injection site before every injection. Buy in bulk. You will go through more than you expect.
Sharps container. Every used needle goes directly into a sharps container. Never recap needles. Never throw loose needles in the trash. A proper sharps container has a one-way opening that prevents accidental needle sticks. You can purchase dedicated sharps containers from any pharmacy, or use a thick-walled plastic container with a secure lid as a temporary solution.
Strongly recommended supplies
A small cooler or insulated bag. Useful for transport, whether you are picking up your medication or traveling with semaglutide or traveling with tirzepatide. You also want a dedicated GLP-1 travel case if you plan to move your medication between locations regularly.
A kitchen scale or body composition scale. Weight-based dosing calculations require knowing your current weight. A body composition scale that tracks muscle mass and body fat percentage gives you much better data for tracking progress beyond just the number on the scale.
A dosing journal or tracking app. Record every injection: date, time, dose, injection site, and any side effects. This data becomes invaluable for troubleshooting and optimizing your protocol. The how to track GLP-1 injections guide covers the best methods.
A pill organizer or calendar system. GLP-1 injections happen on specific days. Missing doses or injecting at irregular intervals undermines the medication steady-state levels your body needs to build. A visual reminder system prevents skipped doses.
Nice-to-have supplies
Cotton balls or gauze pads. For applying light pressure to the injection site after withdrawing the needle. Some people experience minor bleeding or bruising at the injection site. A cotton ball for 10-15 seconds resolves this.
A peptide injection pen can make the injection process more comfortable if you prefer the pen format over manual syringes. Not required, but some researchers find them easier to handle.
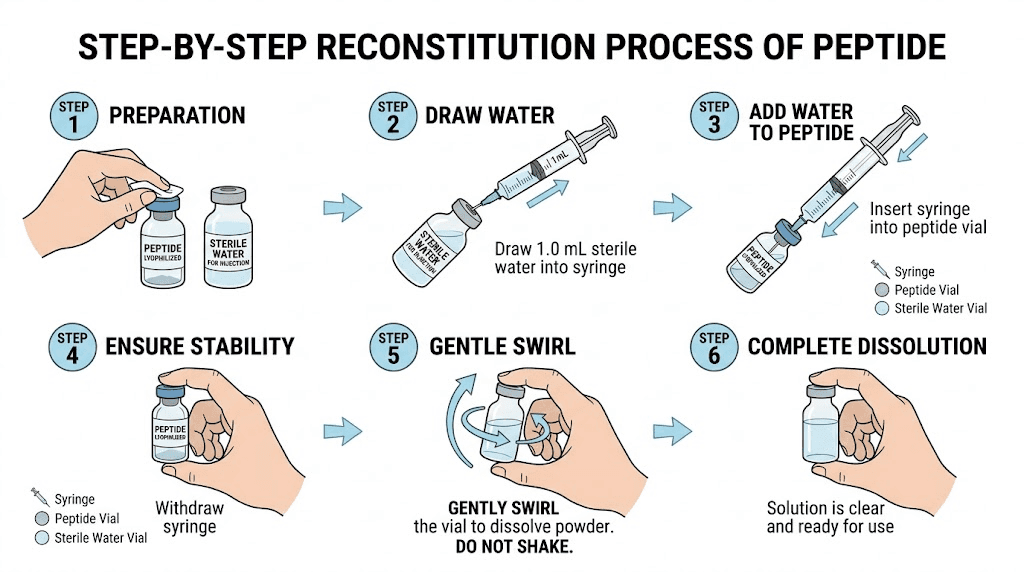
Reconstitution: mixing your GLP-1 medication step by step
Reconstitution is the process of adding bacteriostatic water to your lyophilized peptide powder to create an injectable solution. This is the step that intimidates most beginners. But it is straightforward once you understand the logic.
Before you begin
Wash your hands thoroughly with soap and water. Dry them completely. Set up a clean, flat workspace. Gather all supplies within reach. You want the medication vial, bacteriostatic water, your reconstitution syringe (the larger one), alcohol swabs, and a clean surface.
Remove your medication vial from the refrigerator and let it reach room temperature for about 15-20 minutes. Cold vials can cause the powder to dissolve more slowly and may increase air bubble formation.
Step 1: Clean the vials
Tear open an alcohol swab. Wipe the rubber stopper on your medication vial with the alcohol swab. Use firm pressure and a circular motion. Let it air dry for 10-15 seconds. Do not blow on it or wave it dry.
Repeat with a fresh alcohol swab on the rubber stopper of your bacteriostatic water vial.
Step 2: Draw bacteriostatic water
Using your reconstitution syringe (the larger gauge needle), draw back the plunger to the amount of bacteriostatic water you need. This creates an air bubble in the syringe that equals your target water volume.
How much water to add depends on your vial size and desired concentration. This is where a peptide reconstitution calculator becomes essential.
Common reconstitution ratios:
Semaglutide 5mg vial: Add 2mL BAC water for a 2.5mg/mL concentration. See the full guide for mixing 5mg semaglutide.
Semaglutide 10mg vial: Add 2mL BAC water for a 5mg/mL concentration. The 10mg semaglutide mixing guide walks through this precisely.
Tirzepatide 10mg vial: Add 2mL BAC water for a 5mg/mL concentration. The 10mg tirzepatide mixing guide details the process.
Tirzepatide 30mg vial: Add 3mL BAC water for a 10mg/mL concentration. See the 30mg tirzepatide reconstitution guide.
Retatrutide 10mg vial: Add 2mL BAC water for a 5mg/mL concentration. The retatrutide mixing guide covers the details.
Insert the needle through the rubber stopper of the bacteriostatic water vial. Push the air in. Invert the vial. Draw the water slowly to your target volume. Remove air bubbles by gently tapping the syringe and pushing them back into the vial.
Step 3: Add water to the peptide vial
This is the most important step. Do it wrong and you damage the peptide.
Insert the needle through the rubber stopper of your medication vial. Here is the critical part: aim the needle at the glass wall of the vial, not directly at the powder. Depress the plunger slowly. You want the water to trickle down the inside wall of the vial and gently reach the powder at the bottom.
Never shoot the water directly onto the powder. The force can denature (damage) the peptide molecules, reducing potency. Slow and gentle wins here.
Step 4: Mix gently
After adding all the water, remove the needle. Now gently swirl the vial in a circular motion. Think of it like swirling a glass of wine. Roll it between your palms. Tilt it at slight angles.
Do not shake the vial. Shaking creates air bubbles and can denature the peptide through mechanical stress. The powder should dissolve completely within 1-3 minutes of gentle swirling. If small particles remain, set the vial down for 5 minutes and swirl again.
The final solution should be completely clear. No cloudiness. No particles floating. No visible residue on the vial walls. If the solution is cloudy or contains particles after 10 minutes of intermittent gentle swirling, do not use it.
Step 5: Label and store
Write the following on the vial or on a label you attach to it: the reconstitution date, the concentration (mg/mL), and the discard-by date (typically 28-60 days after reconstitution depending on the medication). Our guides on storing peptides after reconstitution and general peptide storage cover best practices in detail.
Place the vial in the refrigerator immediately. More on storage specifics in the next section.
For complete step-by-step visual guides specific to each medication, see our dedicated reconstitution articles: how to reconstitute 5mg semaglutide, the full semaglutide reconstitution guide, and how to reconstitute tirzepatide.
Storage: keeping your GLP-1 medication potent
Proper storage is not optional. GLP-1 peptides are proteins. They degrade when exposed to heat, light, or bacterial contamination. Poor storage does not just reduce effectiveness. It can render your medication completely useless.
Before reconstitution
Unopened lyophilized vials should be stored in the refrigerator at 36-46 degrees Fahrenheit (2-8 degrees Celsius). Most peptide powders are stable for months or even years when stored properly in this temperature range. Keep the vial in its original packaging to protect it from light.
If your vial arrives at room temperature during shipping, that is usually fine. Lyophilized peptides tolerate brief temperature fluctuations better than reconstituted solutions. But get it into the refrigerator as soon as possible.
After reconstitution
Once reconstituted, the rules become stricter.
Store the reconstituted vial in the refrigerator at 36-46 degrees Fahrenheit. Place it in the middle of the fridge, not in the door. Door shelves experience the most temperature fluctuation from opening and closing. The middle shelf, toward the back, maintains the most consistent temperature.
Never freeze reconstituted GLP-1 medication. Freezing causes ice crystals to form within the solution, which physically damages the peptide structure. A frozen and thawed vial should be discarded.
Keep the vial upright when possible. This minimizes contact between the solution and the rubber stopper, reducing the chance of leaching contaminants from the stopper material over time.
For specific storage timelines: how long semaglutide lasts in the fridge and how long tirzepatide lasts in the fridge provide detailed breakdowns. General shelf life information is covered in the semaglutide shelf life guide and tirzepatide shelf life guide.
What happens when medication gets warm?
If your reconstituted vial sits out at room temperature briefly (under 30 minutes), it is generally fine. Return it to the fridge immediately.
Extended room temperature exposure is a different story. Most compounded GLP-1 medications can tolerate up to 72 hours at controlled room temperature (below 77 degrees Fahrenheit), but potency degrades the longer it stays warm. If your vial has been out for more than a few hours, check the solution for cloudiness or particles before using it.
For specific scenarios, check our guides on how long compounded semaglutide can be unrefrigerated, how long compounded tirzepatide can be out of the fridge, and whether GLP-1 must be refrigerated.
Signs your medication has gone bad
Discard the vial immediately if you notice any of the following: cloudiness or haziness in the solution, visible particles or floaters, color changes (most GLP-1 solutions should be clear and colorless), unusual smell when you remove the cap, or if the solution has been past its labeled discard-by date.
When in doubt, discard and reconstitute a fresh vial. The cost of a new vial is far less than the cost of injecting degraded or contaminated medication. For more on this topic, read about compounded semaglutide expiration and compounded tirzepatide expiration dates.
Calculating your dose
Dose calculation is where many beginners make their first real mistake. It involves converting milligrams to units on an insulin syringe. This sounds complicated. It is not, once you understand the relationship between concentration and syringe markings.
The concentration formula
After reconstitution, your vial has a specific concentration measured in milligrams per milliliter (mg/mL). For example, if you added 2mL of bacteriostatic water to a 10mg semaglutide vial, your concentration is 5mg/mL.
An insulin syringe measures in units, where 100 units equals 1mL. So at 5mg/mL:
10 units = 0.1mL = 0.5mg
20 units = 0.2mL = 1.0mg
50 units = 0.5mL = 2.5mg
The semaglutide dosage calculator and compounded tirzepatide dosage calculator automate these calculations completely. Enter your vial size, water added, and desired dose, and they tell you exactly how many units to draw.
Starting doses by medication
Semaglutide: Most protocols begin at 0.25mg per week for the first four weeks. This allows your body to adjust to the medication gradually, minimizing side effects. After four weeks, the dose typically increases to 0.5mg per week for another four weeks, then continues titrating upward. The semaglutide 5mg dosage chart and compounded semaglutide dose chart lay out the full schedule.
Tirzepatide: Standard starting dose is 2.5mg per week for the first four weeks. Titration then moves to 5mg, 7.5mg, 10mg, and potentially higher depending on tolerance and response. The compound tirzepatide dosing chart and tirzepatide dosing guide provide complete titration schedules.
Retatrutide: Starting doses in clinical trials ranged from 1mg to 4mg per week, with 1mg being the most conservative. The starting dose of retatrutide guide and the retatrutide dosage chart detail the recommended approach.
Common dosing unit conversions
These conversion guides answer the most common questions researchers have when reading their syringes:
Bookmark the peptide calculator for quick calculations whenever you reconstitute a new vial or adjust your dose.
Your first injection: a complete walkthrough
You have reconstituted your medication. You know your dose. Now comes the moment that makes every beginner nervous. The actual injection.
Take a breath. Subcutaneous injections use tiny needles, 29 to 31 gauge, which are thinner than a standard sewing needle. Most people describe the sensation as a slight pinch that lasts less than a second. Many feel nothing at all.
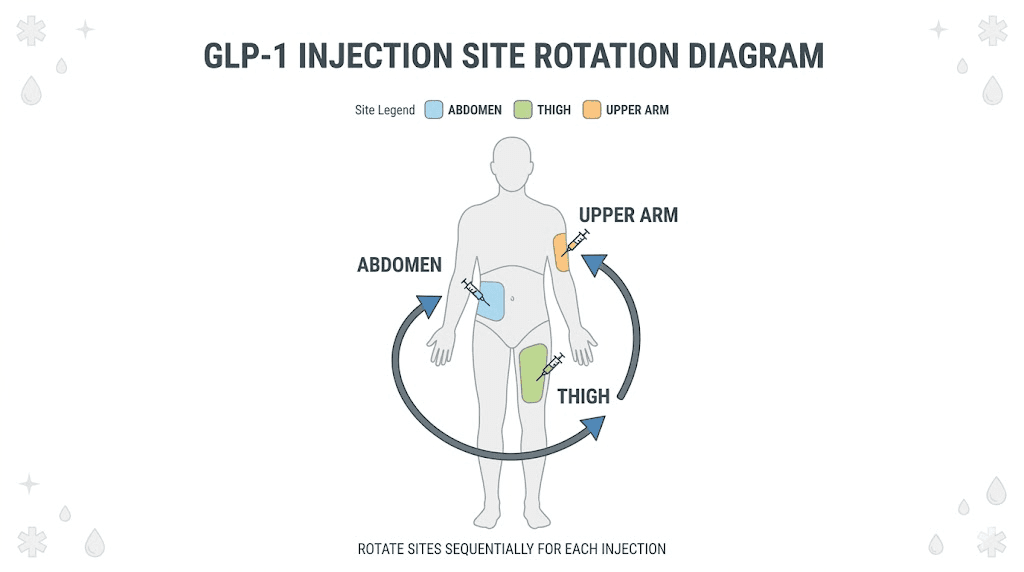
Choose your injection site
Three areas of the body work well for subcutaneous GLP-1 injections.
The abdomen is the most popular choice. Inject into the fatty tissue at least two inches away from your navel. Avoid the area directly around the belly button. The abdomen offers easy access, good visibility, and consistent absorption rates. Our guide to injecting tirzepatide in the stomach covers abdominal injection technique in detail.
The front or outer thigh is a good alternative, especially if you prefer to rotate away from the abdomen. Inject into the middle third of the thigh, on the front or outer side. Avoid the inner thigh where blood vessels are closer to the surface. The tirzepatide injection site thigh guide explains proper technique and positioning.
The back of the upper arm works if someone else can administer the injection for you, as it is difficult to self-inject in this area with proper technique.
For a comprehensive overview of all injection site options, see where to inject GLP-1 and the best GLP-1 injection site for weight loss.
Prepare the injection
Step 1: Wash your hands thoroughly with soap and water.
Step 2: Clean the rubber stopper of your reconstituted medication vial with an alcohol swab. Let it dry.
Step 3: Take a new insulin syringe (your smaller, injection syringe). Pull back the plunger to draw in air equal to your dose volume.
Step 4: Insert the needle into the vial through the rubber stopper. Push the air into the vial. This equalizes pressure and makes it easier to draw medication.
Step 5: Invert the vial so the stopper faces down. Slowly pull the plunger to draw your dose. Draw slightly more than you need.
Step 6: With the syringe still in the vial, tap the barrel gently to move air bubbles to the top near the needle. Push the plunger up slowly until the air is expelled and you reach your exact dose.
Step 7: Remove the syringe from the vial. Set the vial down. Your syringe is loaded and ready.
Administer the injection
Step 1: Clean your chosen injection site with a fresh alcohol swab. Let it dry completely. Injecting through wet alcohol can sting.
Step 2: Pinch a fold of skin between your thumb and index finger. You want about two inches of skin and subcutaneous fat gathered in this pinch. This ensures the needle enters fatty tissue rather than muscle.
Step 3: Hold the syringe like a dart or pencil at a 90-degree angle to your skin. In one smooth motion, insert the needle fully into the pinched skin fold.
Step 4: Release the skin pinch. Slowly depress the plunger to inject the medication. Take about 5-10 seconds to inject the full dose. Rushing can cause discomfort.
Step 5: After the plunger is fully depressed, hold the needle in place for 5-6 additional seconds. This allows the full dose to deposit in the tissue and prevents medication from leaking back through the needle track.
Step 6: Remove the needle in one smooth motion at the same angle you inserted it. If there is a small drop of blood or medication at the site, press a cotton ball or gauze gently against it for 10-15 seconds. Do not rub.
Step 7: Dispose of the used syringe immediately in your sharps container. Never recap the needle.
For medication-specific injection guides with additional detail, see how to give a semaglutide injection with a syringe, how to inject tirzepatide with a syringe, how to inject retatrutide, and the general how to inject GLP-1 guide.
Tips for a painless injection
Let the medication warm to room temperature for 15-30 minutes before injecting. Cold medication straight from the refrigerator stings noticeably more.
Use a fresh needle every time. Reused needles become dull after a single use, which increases pain and infection risk. Under a microscope, a used needle tip looks like a fish hook compared to the smooth point of a new one.
Rotate injection sites consistently. Using the same spot repeatedly causes lipohypertrophy, which is a buildup of hardened fatty tissue under the skin. These lumps reduce absorption and make future injections more uncomfortable. Give each injection site at least a week of rest before returning to it.
If you accidentally inject into muscle instead of fat, it is not dangerous, but absorption rates change. The guide on accidental intramuscular injection explains what to expect.
Timing your injections for best results
When you inject matters almost as much as how you inject. Consistency is the most important factor, but there are strategic advantages to certain timing patterns.
Pick a day and stick to it
GLP-1 medications are typically administered once weekly. Choose a specific day each week for your injection. Many researchers pick a day when they will be home and relatively relaxed, such as Friday evening or Saturday morning. This gives them the weekend to manage any side effects that tend to be strongest in the 24-48 hours after injection.
The best time to take your GLP-1 shot guide covers timing strategies in detail. For medication-specific timing, see the best time of day to take semaglutide and the best time to take a tirzepatide shot.
What if you miss your injection day?
If you miss your scheduled day by 1-2 days, inject as soon as you remember and then resume your regular schedule the following week. If you are more than 3-4 days late, skip that week and inject on your next scheduled day.
Some researchers wonder if they can take tirzepatide a day early or take their GLP-1 a day early. The general consensus is that a day early is fine, while consistently shortening the interval between doses is not recommended as it increases side effect risk.
Morning vs. evening injections
There is no definitive research showing a significant difference between morning and evening injections for GLP-1 medications. However, practical considerations matter.
Morning injections work well for people who want to get it done early and benefit from appetite suppression throughout the day. Evening injections suit people who experience nausea as a side effect, since sleeping through the peak nausea window (typically 4-8 hours after injection) makes it more tolerable.
Experiment during your first few weeks to find what works for your body and schedule.
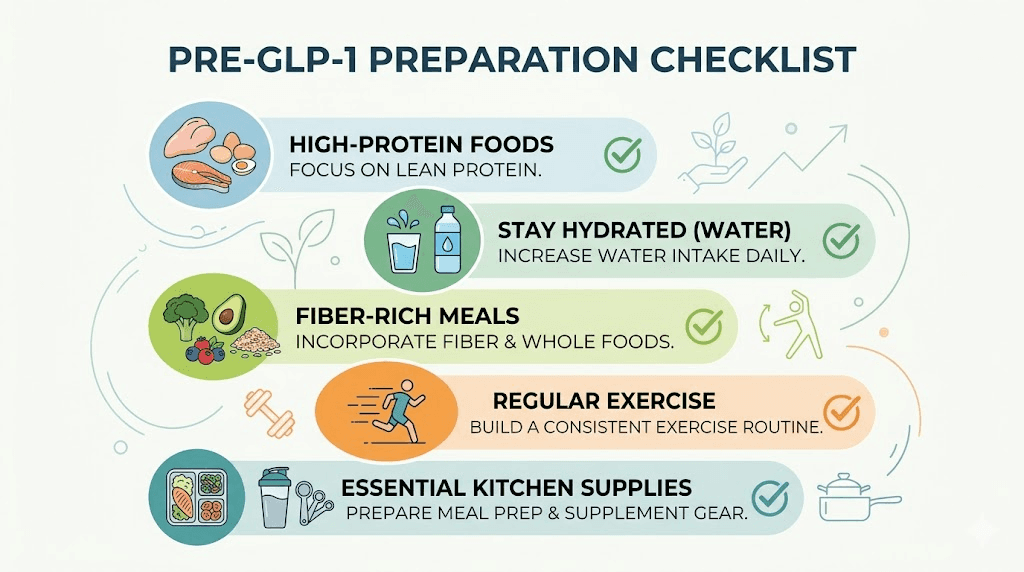
Preparing your body before starting GLP-1 medication
The physical preparation you do before your first injection significantly impacts your experience. Most side effects during the first few weeks are gastrointestinal: nausea, constipation, reduced appetite, and occasionally diarrhea. You can dramatically reduce the severity of these side effects by preparing your body in advance.
Start increasing protein intake two weeks before
GLP-1 medications reduce appetite significantly. When appetite drops, total food intake drops. If your diet is not already protein-rich, you risk losing muscle mass along with fat. Muscle loss slows metabolism, reduces strength, and produces a less healthy body composition even at a lower weight.
Aim for 0.7-1.0 grams of protein per pound of body weight daily. Start hitting this target at least two weeks before your first injection, while you still have normal appetite to make it easier. Good protein sources include eggs, chicken breast, fish, Greek yogurt, cottage cheese, lean beef, tofu, and whey protein.
The how much protein on semaglutide guide provides detailed recommendations. For meal planning help, see GLP-1 friendly meals and GLP-1 recipes for weight loss.
Gradually increase fiber intake
Constipation is one of the most common GLP-1 side effects because the medication slows gastric motility. If you suddenly increase fiber after starting the medication, you compound the problem. Instead, gradually increase fiber over the two weeks before you start.
Add an extra serving of vegetables to each meal. Switch to higher-fiber bread or cereal. Introduce a fiber supplement if needed. The best fiber supplement for GLP-1 guide compares your options. For managing constipation if it does occur, see GLP-1 constipation relief.
Hydrate aggressively
GLP-1 medications reduce thirst along with hunger. Many researchers forget to drink water because they simply do not feel thirsty. Dehydration worsens constipation, fatigue, headaches, and dizziness.
Establish a hydration habit before starting. Aim for at least half your body weight in ounces of water daily. If you weigh 200 pounds, that is 100 ounces. Get a large water bottle and keep it visible. Set phone reminders if needed. Making hydration automatic before your appetite changes makes it much easier to maintain after.
Consider adding electrolytes to your water, especially in the first few weeks. The best electrolytes for GLP-1 guide covers which supplements work best.
Stock your kitchen with GLP-1-friendly foods
When your appetite drops dramatically, you will not want to cook elaborate meals. Having pre-prepared, easy-to-eat, nutrient-dense foods on hand prevents the cycle of eating nothing (muscle loss, nutrient deficiency) or eating whatever is easiest (usually processed carbs).
Stock up on: pre-cooked chicken or rotisserie chicken, Greek yogurt, hard-boiled eggs, pre-cut vegetables, protein shakes, bone broth, cottage cheese, and frozen vegetables that microwave in minutes.
For comprehensive food guides, see best foods to eat on semaglutide, what to eat on tirzepatide, and foods to avoid on semaglutide. The tirzepatide foods to avoid guide covers similar ground for that medication specifically.
Full meal planning resources include the semaglutide diet plan and tirzepatide diet plan, along with ideas for GLP-1 breakfasts and GLP-1 dinners.
Start a basic exercise routine
You do not need to become an athlete before starting GLP-1 medication. But having some form of regular movement established before you begin helps in two ways. First, it preserves muscle mass during rapid weight loss. Second, it establishes a habit while your energy levels are still normal, since some people experience fatigue during the first few weeks of treatment.
Walking 20-30 minutes daily is a solid starting point. Add two to three resistance training sessions per week if possible. Even bodyweight exercises help. The building muscle while on GLP-1 guide covers exercise strategies specifically for people on these medications.
Managing side effects during your first weeks
Almost everyone experiences some side effects during the first 2-4 weeks and after each dose increase. This is normal. The side effects typically peak within 48 hours of injection and gradually diminish as your body adjusts. Understanding what to expect and how to manage each side effect transforms the experience from alarming to manageable.
Nausea
The most commonly reported side effect. GLP-1 medications slow gastric emptying, meaning food stays in your stomach longer. This produces a feeling of fullness that can tip into nausea, especially after eating too much or too quickly.
Management strategies:
Eat smaller, more frequent meals (5-6 small meals instead of 3 large ones)
Eat slowly and chew thoroughly
Avoid high-fat, greasy, or fried foods, especially on injection day
Ginger tea, ginger chews, or ginger supplements can help
Peppermint tea or candies often provide relief
Stay upright after eating (do not lie down for at least 30 minutes)
If nausea is severe, consider timing your injection before bed so you sleep through the worst of it
Constipation
Slowed gastric motility affects the entire digestive tract. Constipation is the second most common complaint and often the most persistent.
Management strategies:
Increase water intake beyond your normal amount
Add a magnesium supplement (magnesium citrate works well)
Use a fiber supplement daily (psyllium husk or methylcellulose)
Eat probiotic-rich foods (yogurt, kefir, sauerkraut)
Stay physically active, as walking helps stimulate bowel motility
If persistent, ask about stool softeners
For detailed guidance, see semaglutide constipation treatment and tirzepatide constipation treatment.
Fatigue and low energy
Some researchers report feeling tired during the first few weeks, particularly if caloric intake drops significantly. This usually resolves as the body adapts.
Management strategies:
Ensure adequate caloric intake (extreme restriction worsens fatigue)
Prioritize sleep (7-9 hours)
Maintain light exercise (walking, stretching)
Check hydration and electrolyte levels
B-vitamin supplementation may help some people
Detailed guides on fatigue include GLP-1 fatigue, semaglutide fatigue, and does tirzepatide make you tired.
Headaches
Often linked to dehydration or rapid changes in blood sugar. More common in the first week or two.
Management strategies:
Increase water intake significantly
Eat regular meals (do not skip meals, even if appetite is low)
Monitor caffeine intake (do not suddenly increase or decrease)
Over-the-counter pain relief is generally safe if needed
See the GLP-1 headache guide for more detailed troubleshooting.
Dizziness and lightheadedness
Typically related to blood sugar fluctuations, dehydration, or caloric under-eating. More common during rapid dose escalation.
The semaglutide dizziness guide and semaglutide lightheaded guide cover this topic comprehensively. Ensure you eat at least three small meals per day, even when appetite is suppressed.
Injection site reactions
Redness, mild swelling, itching, or a small bump at the injection site are common and usually resolve within 24-48 hours.
Management strategies:
Rotate injection sites consistently
Allow alcohol to dry completely before injecting
Inject at room temperature (not cold from the fridge)
Use a fresh needle every time
If reactions persist or worsen, see injection site reaction with tirzepatide, tirzepatide injection site red and itchy, and tirzepatide injection site reaction treatment.
Other side effects worth knowing about
Less common but still reported side effects include acid reflux, heartburn, bloating, dry mouth, insomnia, and changes in menstrual cycles. Most resolve within the first month as the body adapts to the medication.
Supplements to support your GLP-1 protocol
The right supplement stack can meaningfully reduce side effects and protect against the nutritional gaps that reduced food intake creates.
Essential supplements
A quality multivitamin. Reduced food intake means reduced micronutrient intake. A comprehensive multivitamin provides baseline coverage for vitamins and minerals you might otherwise miss.
Electrolytes. Sodium, potassium, and magnesium levels can drop when fluid balance shifts during rapid weight loss. The best electrolytes for GLP-1 guide compares products and dosing. Magnesium citrate specifically helps with both electrolyte balance and constipation.
Fiber supplement. Psyllium husk or methylcellulose supports regular bowel movements when dietary fiber drops due to reduced food intake.
Protein powder. When you cannot eat enough whole food protein, a quality whey or plant-based protein powder fills the gap. Essential for muscle preservation.
Beneficial additions
Some GLP-1 medications come compounded with additional ingredients that may enhance results or reduce side effects. Vitamin B12 is one of the most common additions, and for good reason, as it supports energy production and may reduce fatigue. Read more about semaglutide with B12 and tirzepatide with B12.
Other common compounded additions include glycine with semaglutide, glycine with tirzepatide, niacinamide with semaglutide, niacinamide with tirzepatide, and L-carnitine with semaglutide.
For a broader overview of supportive supplements, the supplements to take with GLP-1 guide provides a complete breakdown.
Supplements that may interact
Some researchers combine GLP-1 medications with other weight management supplements. Phentermine and semaglutide and phentermine and tirzepatide are common combinations people ask about. Metformin with semaglutide and metformin with tirzepatide are also frequently discussed. Always research interactions thoroughly before combining medications.
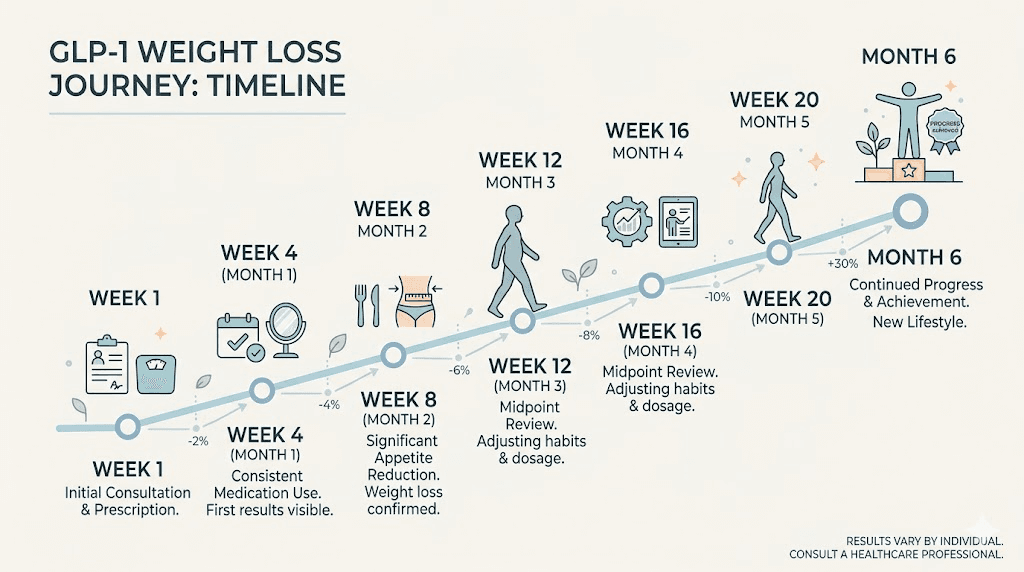
What to expect week by week
Setting realistic expectations prevents discouragement. GLP-1 medications are not overnight solutions. They work progressively over weeks and months. Here is what most researchers report at each stage.
Week 1
The starting dose is intentionally low. You may notice subtle appetite reduction, or you may notice nothing at all. Some people experience mild nausea, a slight headache, or fatigue. Others feel completely normal. Both responses are typical.
This is your body adjusting to the medication. Do not increase your dose because you are not feeling effects. The starting period exists specifically to let your gastrointestinal system adapt gradually.
The first week on semaglutide guide and what to expect after your first dose of tirzepatide provide detailed timelines of what happens in those initial days.
Weeks 2-4
Appetite suppression becomes more noticeable. You may find yourself eating smaller portions naturally, thinking about food less frequently, and feeling satisfied sooner during meals. Some researchers lose 2-5 pounds during this period, primarily from reduced caloric intake and water loss.
Side effects that appeared in week one often diminish by week three as your body adapts. If they persist, review the management strategies above and consider whether your hydration, protein, and electrolyte intake are adequate.
Weeks 5-8 (first dose increase)
After four weeks at the starting dose, most protocols call for the first dose increase. This is when results typically accelerate. Appetite suppression becomes stronger. Weight loss increases. But side effects may briefly return or intensify for a few days as your body adjusts to the higher dose.
The pattern repeats with each subsequent dose increase: a brief period of adjustment followed by adaptation.
Months 2-3
By this point, you are into a rhythm. Injection preparation feels routine. Side effects have largely resolved or become manageable. Weight loss is steady, typically averaging 1-3 pounds per week depending on the medication, dose, and individual factors.
This is when tracking becomes especially valuable. Record your weight weekly (same day, same time, same conditions), track your measurements, and note how your clothes fit. The scale fluctuates daily, but the trend over weeks tells the real story.
For timeline-specific guides, see tirzepatide weight loss timeline, semaglutide results week by week, and when you start losing weight on semaglutide.
Months 3-6 and beyond
This is where patience and consistency pay off. The compounding effect of sustained caloric reduction produces significant body composition changes. Many researchers report their most dramatic visible changes during this period, even if the rate of scale weight loss slows slightly.
If progress stalls, do not panic. Plateaus happen. The semaglutide plateau guide, why you are not losing weight on semaglutide, and why you are not losing weight on tirzepatide cover proven strategies for breaking through stalls. The 4 weeks on semaglutide with no weight loss guide addresses the specific scenario of early-stage plateaus.
Common mistakes beginners make and how to avoid them
After helping thousands of researchers navigate their GLP-1 setup, SeekPeptides has identified the mistakes that appear over and over. Knowing these in advance saves you from learning them the hard way.
Mistake 1: Skipping the priming step
When using a new vial, the first draw from the syringe may pull more air than medication. Some researchers skip priming (drawing a small amount and pushing it back, or tapping out air bubbles thoroughly) and end up injecting mostly air for their first dose. The result is no appetite change that week and confusion about whether the medication works.
Always prime carefully. Ensure you see a clear, bubble-free column of medication in the syringe before injecting.
Mistake 2: Shaking the vial during reconstitution
Shaking denatures the peptide. It is one of the most common causes of cloudy solution and reduced effectiveness. Swirl gently. Roll between your palms. Never shake. Refer back to the reconstitution section above and our dedicated guides for how to mix peptides with BAC water.
Mistake 3: Not eating enough protein
The appetite suppression is powerful. Many researchers celebrate eating very little without realizing they are losing significant muscle along with fat. Inadequate protein intake during GLP-1 therapy is arguably the single biggest mistake you can make for long-term body composition.
Prioritize protein at every meal. Use protein shakes to fill gaps. Track your intake for at least the first month. The calorie guide for semaglutide and calorie guide for tirzepatide provide nutrition targets.
Mistake 4: Increasing dose too quickly
Impatience drives this one. The starting dose feels like it is doing nothing, so people jump to a higher dose ahead of schedule. This dramatically increases side effect severity without meaningfully speeding up results. Trust the titration schedule. Your body needs time to adapt.
Mistake 5: Inconsistent injection timing
Injecting three days late one week, then two days early the next disrupts the medication steady state. Drug levels spike and crash rather than maintaining a consistent therapeutic level. This increases side effects and reduces efficacy. Pick a day. Stick to it.
Mistake 6: Storing medication incorrectly
Leaving reconstituted medication on the counter, storing it in the fridge door, or freezing it accidentally all compromise potency. Review the storage section above. The how long peptides last at room temperature guide gives you exact timelines for temperature exposure.
Mistake 7: Not rotating injection sites
Using the same spot repeatedly causes lipohypertrophy, which means hardened fatty lumps under the skin. These lumps reduce medication absorption. Your effective dose drops even though you are injecting the same amount. Rotate between abdomen, thighs, and different spots within each area. Our guide on where to inject tirzepatide and best injection site for semaglutide shows rotation patterns that prevent this.
Mistake 8: Ignoring hydration
GLP-1 medications reduce thirst alongside hunger. You stop feeling thirsty, so you stop drinking enough water. Dehydration causes headaches, constipation, dizziness, fatigue, and muscle cramps. All of which get blamed on the medication when the real cause is simply not drinking enough water. Make hydration proactive, not reactive.
For a comprehensive list of beginner mistakes beyond GLP-1 specifically, see our common peptide mistakes beginners make guide and the getting started with peptides overview.
Setting up your ongoing protocol
The initial setup gets you started. But optimizing your protocol over time is what produces exceptional results. Think of the first month as the foundation. Everything after that is refinement.
Titration schedule
Your dose should increase gradually according to a planned titration schedule. Do not increase your dose based on how you feel on a given day. Follow the timeline your protocol specifies.
A typical semaglutide titration:
Weeks 1-4: 0.25mg once weekly
Weeks 5-8: 0.5mg once weekly
Weeks 9-12: 1.0mg once weekly
Weeks 13-16: 1.7mg once weekly
Week 17 onward: 2.4mg once weekly (maximum maintenance dose)
A typical tirzepatide titration:
Weeks 1-4: 2.5mg once weekly
Weeks 5-8: 5.0mg once weekly
Weeks 9-12: 7.5mg once weekly
Weeks 13-16: 10mg once weekly
Week 17 onward: 12.5-15mg once weekly (if needed)
Some researchers find their optimal dose well below the maximum. If side effects are manageable and results are progressing at a moderate dose, there is no requirement to keep increasing. The GLP-1 maintenance dose guide covers how to identify your sweet spot.
When to consider switching medications
If one GLP-1 medication is not producing results after adequate time at therapeutic doses, switching may be worth exploring. The switching from tirzepatide to semaglutide and switching from semaglutide to tirzepatide dosage chart provide conversion guidelines. The switching from tirzepatide to retatrutide guide covers the newer option.
Alternative delivery methods
Not everyone prefers injections. Alternative options are emerging. Oral tirzepatide is becoming available in some formulations. Sublingual semaglutide offers another non-injection route. The tirzepatide oral vs injection comparison helps you evaluate whether an alternative delivery method might work for your situation.
Microdosing approaches
Some researchers use lower-than-standard doses for specific purposes such as anti-inflammatory benefits or autoimmune support rather than weight loss. The microdosing tirzepatide chart, microdose tirzepatide schedule, and microdosing GLP-1 for autoimmune conditions explore this approach.
GLP-1 setup checklist: everything in one place
Use this as your reference before and during your first week.
Two weeks before starting:
Order your GLP-1 medication, bacteriostatic water, syringes, alcohol swabs, and sharps container
Increase protein intake to 0.7-1.0g per pound of body weight daily
Gradually increase fiber intake
Begin hydrating at 0.5oz per pound of body weight daily
Stock your kitchen with GLP-1-friendly foods
Start a basic exercise routine (walking plus resistance training)
Weigh yourself and take baseline measurements
Day your medication arrives:
Inspect packaging for damage
Verify the medication label matches your order
Check the expiration date
Store unreconstituted vials in the refrigerator immediately
Organize all supplies in one clean, accessible location
Reconstitution day:
Wash hands and prepare clean workspace
Let the vial reach room temperature (15-20 minutes)
Clean both vial stoppers with alcohol
Calculate BAC water amount using the reconstitution calculator
Add water slowly against vial wall (never directly onto powder)
Swirl gently until clear (never shake)
Label vial with date, concentration, and discard-by date
Store immediately in the middle of the refrigerator
First injection day:
Eat a light, balanced meal 1-2 hours before
Remove reconstituted vial 15-30 minutes before injection (room temperature)
Calculate dose using the peptide calculator
Clean vial stopper and injection site with alcohol
Draw dose, remove air bubbles, verify amount
Pinch skin, insert needle at 90 degrees, inject slowly
Hold 5-6 seconds, remove, apply light pressure
Dispose of syringe in sharps container
Log the injection: date, time, dose, site, any notes
First week ongoing:
Maintain protein and hydration targets
Eat smaller, more frequent meals
Avoid greasy foods and alcohol for 48 hours after injection
Track any side effects (type, severity, duration)
Continue light exercise (walking minimum)
Do not increase dose yet, regardless of how you feel
Special considerations
Certain situations require additional planning during your GLP-1 setup.
Traveling with GLP-1 medication
If you need to travel while on a GLP-1 protocol, you need a plan for keeping your medication cold and your injection schedule consistent. The traveling with semaglutide guide and traveling with tirzepatide guide cover everything from TSA considerations to maintaining cold chain during flights and road trips. A quality GLP-1 travel case is essential.
Alcohol and GLP-1 medications
Many researchers ask about drinking on semaglutide and drinking on tirzepatide. Alcohol interacts with GLP-1 medications in several ways. It compounds nausea, increases blood sugar fluctuations, adds empty calories, and can slow weight loss progress. If you choose to drink, do so minimally and not within 48 hours of your injection. The best alcohol to drink on tirzepatide guide offers harm reduction strategies.
Pregnancy and breastfeeding
GLP-1 medications should be discontinued before attempting pregnancy. These are important safety considerations that researchers should understand before starting. See semaglutide while trying to get pregnant, tirzepatide while breastfeeding, and GLP-1 while breastfeeding for detailed guidance.
Stopping and maintaining
Eventually, you may want to discontinue GLP-1 medication. This requires a plan. Abrupt cessation often leads to rapid appetite return and weight regain. The how to wean off tirzepatide and how to maintain weight loss after tirzepatide guides cover tapering strategies and long-term maintenance planning. The getting off GLP-1 guide provides a comprehensive overview of the transition process.
Frequently asked questions
How long does it take for GLP-1 medication to start working?
Most researchers notice subtle appetite changes within the first week, though some feel nothing at the starting dose. More noticeable effects typically appear within 2-4 weeks. Weight loss usually begins within the first month. See our detailed timeline guides for how long GLP-1 takes to start working, how fast semaglutide works, and how fast tirzepatide works.
Can I use sterile water instead of bacteriostatic water?
For single-use vials (one reconstitution, one injection, then discard), sterile water is acceptable. For multi-use vials where you draw multiple doses over days or weeks, you must use bacteriostatic water. The benzyl alcohol preservative prevents bacterial growth. Using sterile water for multi-dose vials creates contamination risk. See our bacteriostatic water for peptides guide.
What gauge needle should I use for GLP-1 injections?
Use 29-31 gauge insulin syringes for subcutaneous injections. The 31-gauge is thinnest and least painful. For reconstitution (drawing and injecting BAC water), use a larger gauge (18-21) syringe to move water more efficiently. Never use the same needle for both reconstitution and injection.
How much weight can I expect to lose?
Results vary significantly based on medication, dose, starting weight, diet, and exercise. Clinical trial averages show semaglutide users losing 10-15% of body weight over 68 weeks, and tirzepatide users losing 15-22% of body weight over 72 weeks. The GLP-1 average weight loss per month guide provides more granular data.
Do I need to take GLP-1 medication forever?
This depends on your goals and how you manage the transition off medication. Some researchers use GLP-1 medications for a defined period to reach their goal weight, then taper off while maintaining lifestyle changes. Others use a GLP-1 maintenance dose long-term. Research suggests weight regain is common after complete discontinuation without adequate lifestyle modification, which is why a structured taper and maintenance plan matters.
Can I combine creatine with GLP-1 medication?
Yes. Creatine and GLP-1 are frequently combined. Creatine supports muscle preservation and performance during the caloric deficit that GLP-1 medications create. There are no known interactions between creatine and GLP-1 receptor agonists. See also creatine and semaglutide and creatine and tirzepatide.
Is it normal to feel nothing on the starting dose?
Completely normal. Starting doses are intentionally subtherapeutic for weight loss. Their purpose is to let your gastrointestinal system adjust. Many researchers feel no appetite change at all during the first 2-4 weeks. This does not mean the medication is not working, as it is building up in your system. The does semaglutide suppress appetite immediately guide explains the timeline.
External resources
PMC - Ten top tips for GLP-1 receptor agonist management in primary care
Novo Nordisk Medical - GLP-1 storage and stability reference
For researchers serious about optimizing their GLP-1 protocol from the very first dose, SeekPeptides provides the most comprehensive resource available. Members access detailed dosing protocols, reconstitution calculators, expert-reviewed guides, and a community of thousands who have navigated every question covered in this guide and many more that arise along the way.
In case I do not see you, good afternoon, good evening, and good night. May your reconstitution stay clear, your injections stay painless, and your setup stay flawless from day one.