Mar 25, 2026

What if the real reason your GLP-1 medication is not working the way you expected has nothing to do with the medication itself? What if the headaches, the muscle cramps, the crushing fatigue, and the brain fog that so many people blame on semaglutide or tirzepatide are actually caused by something far simpler? Something fixable. Something most guides completely ignore.
Electrolytes.
These tiny minerals control everything from your heartbeat to your muscle contractions to your ability to think clearly. And GLP-1 medications create the perfect storm for depleting them. Reduced food intake means fewer electrolytes coming in. Nausea and vomiting mean more electrolytes going out. The result is a deficit that compounds week after week, turning manageable side effects into miserable ones. Understanding which electrolytes your body needs, how much you need, and when to take them can transform your entire GLP-1 experience from something you barely tolerate to something that actually works the way the clinical trials promised.
This guide covers the specific electrolytes that matter most for people on GLP-1 receptor agonists, the exact dosages backed by research, the best forms and products to look for, the warning signs of deficiency you should never ignore, and the practical protocols that experienced users rely on to stay balanced throughout their treatment. Whether you are on compounded semaglutide, tirzepatide, or any other GLP-1 medication, this information applies directly to you.
Why GLP-1 medications deplete your electrolytes
GLP-1 receptor agonists work by mimicking a natural hormone called glucagon-like peptide-1. This hormone slows gastric emptying, reduces appetite, and enhances insulin secretion. Powerful effects. Genuinely transformative for weight management. But these same mechanisms create three distinct pathways for electrolyte loss that most people never think about until they are already deep in a deficit.
The first pathway is reduced intake. When your appetite drops by 30-50%, you eat less food. Less food means fewer dietary minerals. The average American gets approximately 3,400mg of sodium, 2,500mg of potassium, and 300mg of magnesium from food each day. Cut that food intake in half, and you have cut your electrolyte intake in half too. Simple math with serious consequences.
The second pathway is gastrointestinal losses. According to clinical data, nausea occurs in 15-44% of patients on GLP-1 medications. Diarrhea affects 8-30%. Vomiting impacts 5-24%. Each episode of vomiting or diarrhea strips away potassium, sodium, chloride, and bicarbonate. These are not small losses. A single bout of vomiting can deplete more potassium than an entire banana replaces.
The third pathway is renal excretion. GLP-1 receptor activation in the kidneys increases sodium excretion through inhibition of the sodium-hydrogen ion exchanger in the proximal tubule. Your kidneys are literally flushing sodium faster than usual. And when sodium goes, water follows, pulling other electrolytes along with it.
Three pathways. All running simultaneously. All depleting your mineral reserves from different directions. This is why fatigue on semaglutide and GLP-1 fatigue are so common. It is not always the medication causing problems. It is what the medication removes from your system.
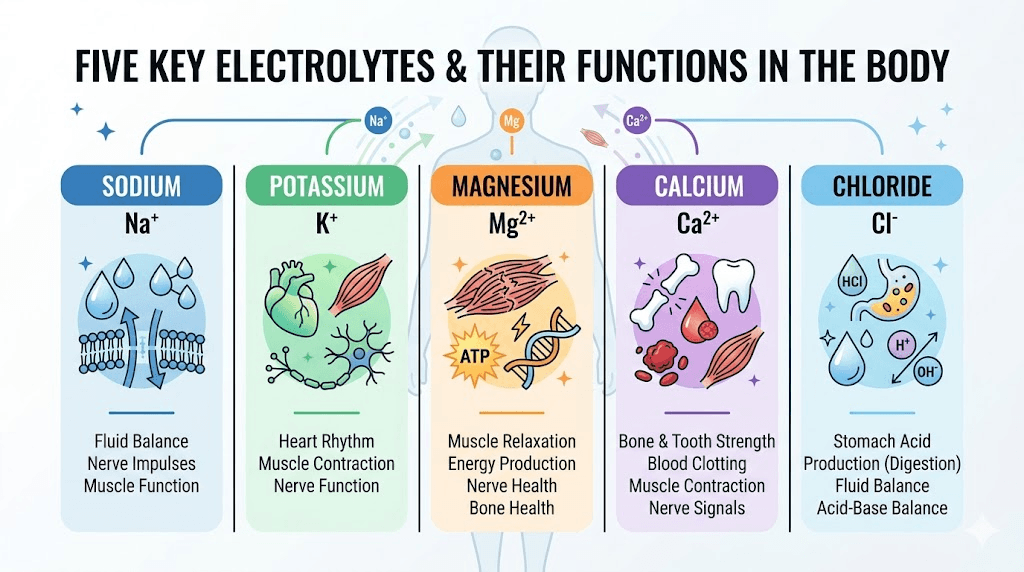
The five essential electrolytes and what each one does
Not all electrolytes matter equally when you are on a GLP-1 medication. Five deserve your attention. Understanding what each one does, and what happens when it runs low, helps you recognize problems before they become serious.
Sodium: the one everyone underestimates
Sodium gets a bad reputation. Years of public health messaging have trained people to avoid it. But when you are on a GLP-1 medication, eating less, and potentially losing fluids through GI side effects, sodium becomes critically important.
Your body needs sodium to maintain blood volume, regulate nerve impulses, and contract muscles. Normal blood sodium levels fall between 136-145 mEq/L. When levels drop below 130 mEq/L, symptoms appear. Below 125 mEq/L, the situation becomes dangerous.
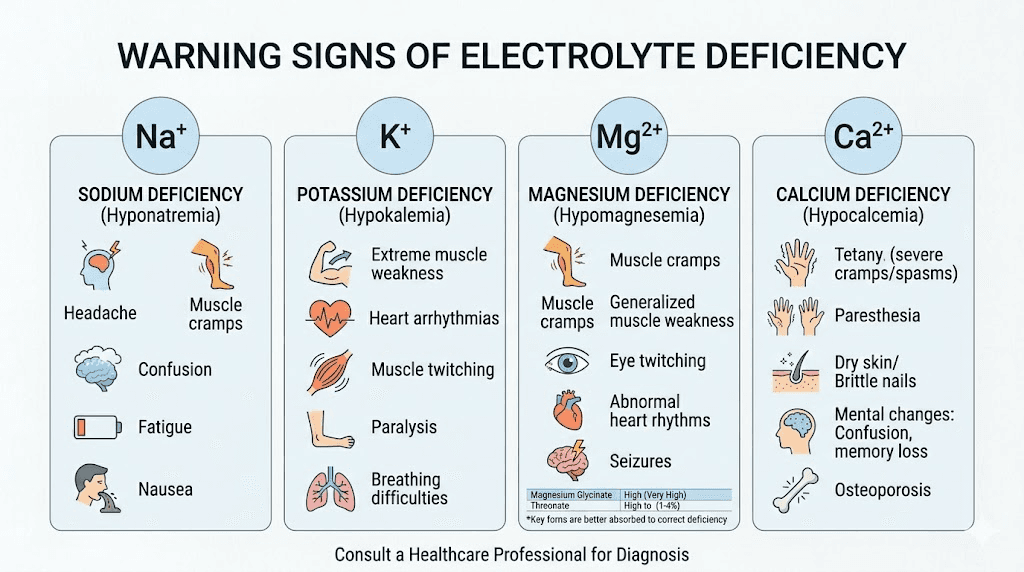
What does low sodium feel like? Headaches. Nausea that seems worse than it should be. Confusion. Dizziness. Fatigue that sleep does not fix. Many people assume these symptoms are just part of being on a GLP-1 medication. They are not. They are signs of hyponatremia, and they are fixable.
The recommended daily intake is 1,500-2,300mg for most adults. On a GLP-1 medication with reduced food intake, most people fall well below this range without supplementation. Bone broth, salted foods, and electrolyte drinks can help bridge the gap. If you are experiencing light-headedness on semaglutide, sodium is one of the first things to address.
Potassium: the muscle and heart mineral
Potassium controls your heartbeat. That is not an exaggeration. It regulates the electrical impulses that keep your heart rhythm steady, and it enables every muscle contraction in your body. Normal blood levels range from 3.5-5.0 mEq/L. Below 3.0 mEq/L requires urgent medical intervention.
The adequate intake for potassium is 4,700mg per day from all sources. Most Americans already fall short of this target even without appetite suppression. Add a GLP-1 medication that cuts food intake significantly, and the gap widens fast.
Low potassium symptoms include muscle cramps, weakness, constipation, heart palpitations, and fatigue. These overlap heavily with common GLP-1 side effects, which is why so many people never realize the actual problem. If you are dealing with constipation on tirzepatide that fiber supplements have not resolved, low potassium could be the underlying cause.
Important caution: potassium supplementation requires more care than other electrolytes. High-dose potassium supplements can be dangerous, especially for people with kidney disease or those taking certain medications like ACE inhibitors or potassium-sparing diuretics. Most over-the-counter potassium supplements max out at 99mg per serving for this reason. The safest approach is increasing potassium through food sources first, then supplementing conservatively if needed, always under medical guidance.
Magnesium: the most commonly deficient
Magnesium participates in over 300 enzymatic reactions in the body. It supports muscle relaxation, nerve function, bone health, blood sugar regulation, and sleep quality. Normal blood levels range from 1.7-2.2 mg/dL. But here is the problem: blood tests only measure the 1% of magnesium circulating in your bloodstream. The other 99% lives in your bones, muscles, and soft tissues. You can be significantly magnesium-deficient while blood tests show normal levels.
An estimated 50% of the general population does not get enough magnesium from diet alone. On a GLP-1 medication with reduced food intake, that percentage climbs even higher. The recommended dietary allowance is 310-420mg per day depending on age and sex.
Magnesium deficiency shows up as muscle pain, cramps, insomnia, anxiety, heart palpitations, and constipation. If you are experiencing sleep problems on semaglutide, magnesium supplementation should be one of your first steps.
The tolerable upper intake level for supplemental magnesium is 350mg per day for adults. Going above this amount can cause diarrhea, which defeats the purpose when you are already dealing with GI discomfort.
Calcium: beyond bone health
Calcium does more than build bones. It plays a critical role in muscle contractions, blood clotting, nerve signaling, and hormone secretion. The recommended daily intake is 1,000-1,200mg for adults.
GLP-1 medications present a unique calcium concern. Rapid weight loss, regardless of the method, increases the risk of bone density loss. Combined with reduced calcium intake from eating less, this creates a compounding risk. Studies on weight loss medications show that patients who supplement calcium and vitamin D during treatment maintain significantly better bone density than those who do not.
Symptoms of low calcium include numbness or tingling in fingers and toes, muscle aches, cramps, and in severe cases, confusion or memory problems. The connection between tirzepatide and bone loss makes calcium supplementation especially important for long-term users.
Chloride: the forgotten electrolyte
Chloride rarely gets attention in electrolyte discussions, but it matters. It works alongside sodium to maintain fluid balance, helps produce stomach acid for digestion, and assists in carbon dioxide transport. Normal blood levels range from 96-106 mEq/L.
Vomiting is the primary way GLP-1 users lose chloride. Stomach acid is rich in hydrochloric acid, so every episode of vomiting depletes both chloride and hydrogen ions. This can lead to metabolic alkalosis, a condition where blood pH rises above normal, causing headaches, muscle twitching, and confusion.
Most people get adequate chloride through table salt (sodium chloride) and food. If you are supplementing sodium properly, chloride typically comes along with it. But if you are experiencing frequent vomiting during dose escalation on tirzepatide or your first weeks on semaglutide, pay extra attention to chloride replacement.
Best forms of each electrolyte supplement
Not all supplement forms are created equal. The form of an electrolyte determines how well your body absorbs it, how well your stomach tolerates it, and whether it creates additional GI problems. When you are already dealing with the gastrointestinal effects of a GLP-1 medication, choosing the right form matters enormously.
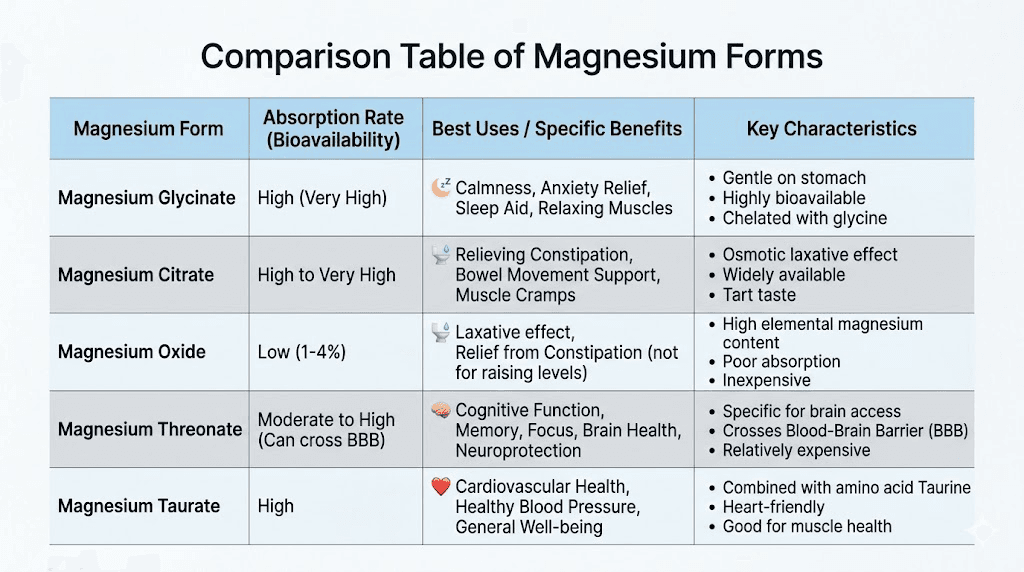
Magnesium forms ranked for GLP-1 users
Magnesium comes in many forms. Each one has different absorption rates and different effects on your gut. For people on GLP-1 medications, some forms work far better than others.
Magnesium glycinate (best overall). This is the form most experts recommend for GLP-1 users. It offers excellent absorption, minimal GI side effects, and has the added benefit of glycine, an amino acid that supports sleep quality and relaxation. Typical dosage: 200-400mg daily, taken with meals or before bed. If you are experiencing insomnia on tirzepatide, magnesium glycinate before bed is an excellent starting point.
Magnesium citrate (best for constipation). This form has a mild laxative effect, which can be beneficial if constipation is your primary GI complaint. However, it should be avoided if diarrhea is already a problem. Dosage: 250-420mg daily. Citrate form may absorb slightly better into muscle tissue, making it a good choice for people dealing with leg cramps on semaglutide.
Magnesium oxide (least recommended). Cheap and widely available, but poorly absorbed. Only about 4% of magnesium oxide actually makes it into your bloodstream. The rest passes through your digestive tract, often causing diarrhea. Avoid this form entirely if you are on a GLP-1 medication.
Magnesium threonate (best for brain function). This form crosses the blood-brain barrier more effectively than others. If brain fog on tirzepatide is your main complaint, magnesium threonate is worth considering. Dosage: 1,500-2,000mg of magnesium threonate, which provides approximately 144mg of elemental magnesium.
Magnesium taurate (best for heart health). Combines magnesium with taurine, an amino acid that supports cardiovascular function. A solid choice if heart palpitations are your primary concern. Dosage: 200-400mg daily.
Sodium supplementation strategies
You do not need a fancy supplement for sodium. Here are the most practical approaches.
Salt tablets or capsules. Simple, inexpensive, and precise. Each tablet typically provides 200-400mg of sodium. Take one with water when symptoms of low sodium appear, like headaches or dizziness.
Bone broth. One cup of bone broth provides approximately 400-500mg of sodium along with collagen, amino acids, and other minerals. It is gentle on the stomach, warm, and easy to consume even when appetite is suppressed. Many GLP-1 users find that sipping bone broth throughout the day is one of the most effective ways to maintain sodium levels without forcing solid food.
Electrolyte drink mixes. These combine sodium with other electrolytes in balanced ratios. Look for products with 200-300mg sodium, 100-200mg potassium, and 50-100mg magnesium per serving. Citrate-based formulas tend to sit better on sensitive stomachs.
Pink Himalayan salt or sea salt. Adding a pinch of quality salt to water or food provides sodium along with trace minerals. A quarter teaspoon of salt contains approximately 575mg of sodium. This is a simple hack that costs almost nothing and can make a real difference when you are eating much less than usual.
Potassium: food first, supplements second
Because potassium supplementation carries more risk than other electrolytes, dietary sources should be your primary strategy.
Top potassium-rich foods:
Avocado (one medium): 975mg
Baked potato with skin: 926mg
Sweet potato: 541mg
Banana: 422mg
Spinach (one cup cooked): 839mg
White beans (one cup): 1,004mg
Salmon (6oz): 683mg
Yogurt (one cup): 573mg
Coconut water (one cup): 600mg
Even when appetite is reduced, many of these foods can be consumed in small portions. A quarter avocado here. A few bites of baked potato there. Coconut water as your hydration base. Small additions compound over a full day. For people following a semaglutide diet plan or tirzepatide diet plan, building potassium-rich foods into every meal is one of the highest-impact changes you can make.
If supplementation is necessary, over-the-counter potassium gluconate or potassium citrate in 99mg doses is the safest option. Never exceed supplemental potassium without medical supervision, especially if you have kidney disease or take medications that affect potassium levels.
Calcium forms for GLP-1 users
Two forms dominate the calcium supplement market.
Calcium citrate. Better absorbed on an empty stomach. Does not require stomach acid for absorption, making it the superior choice for GLP-1 users since these medications reduce stomach acid production and slow gastric emptying. Take in divided doses of 500mg or less for optimal absorption.
Calcium carbonate. Requires stomach acid for absorption and should be taken with meals. Less ideal for GLP-1 users because of the reduced gastric acid environment. However, it is less expensive and contains more elemental calcium per tablet.
Always pair calcium supplementation with vitamin D (1,000-2,000 IU daily) for proper absorption. This combination is especially important for people experiencing hair loss on GLP-1 medications, as nutritional deficiencies including calcium and vitamin D contribute to hair thinning during rapid weight loss.
How to recognize electrolyte deficiency on GLP-1 medications
The tricky part about electrolyte deficiency during GLP-1 treatment is that the symptoms look almost identical to normal medication side effects. This means most people never investigate further. They assume the headaches and fatigue are just the cost of being on the medication. They push through. They suffer unnecessarily.
Knowing the difference between a normal side effect and an electrolyte deficiency can change everything.
Red flags that suggest electrolyte problems, not just medication side effects
Persistent fatigue that worsens over weeks. Normal GLP-1 fatigue tends to be worst during the first week or two and improves as your body adjusts. If you are getting more tired as time goes on, especially after the initial adjustment period, electrolyte depletion is a likely culprit. Many people dealing with tiredness on tirzepatide find that electrolyte supplementation provides more relief than rest does.
Muscle cramps, especially at night. Occasional minor cramps during dose escalation can be normal. But persistent cramps, especially nocturnal leg cramps or cramps that happen during light activity, strongly suggest magnesium or potassium deficiency. These are the body sending an unmistakable signal.
Heart palpitations or irregular heartbeat. This is a serious warning sign. Both low potassium and low magnesium can cause cardiac rhythm disturbances. If you experience palpitations, skipped beats, or a racing heart that is not related to physical activity or anxiety, contact your healthcare provider immediately. Do not wait.
Headaches that do not respond to hydration. If you are drinking plenty of water but still getting headaches, the problem might not be water volume. It might be electrolyte concentration. Plain water without electrolytes can actually worsen dilutional hyponatremia by further reducing blood sodium concentration. If headaches on tirzepatide persist despite drinking 2-3 liters of water daily, switch to electrolyte-enhanced water for a few days and see if the pattern changes.
Dizziness when standing up. Called orthostatic hypotension, this happens when blood pressure drops too quickly on standing.
Low blood volume from dehydration and sodium depletion is a common cause. If you experience this, it is a clear sign your sodium and fluid intake need attention. Light-headedness on semaglutide is often directly linked to this mechanism.
Constipation that fiber does not fix. Fiber is the standard first-line treatment for GLP-1 related constipation. But if fiber, water, and movement have not helped, low magnesium or low potassium could be the real issue. Both minerals are essential for normal bowel motility.
Tingling or numbness in hands and feet. This paresthesia can indicate low calcium, low magnesium, or both. It typically appears as a subtle tingling that many people dismiss. Do not dismiss it. It means mineral levels are low enough to affect nerve function.
When to get tested
Request a comprehensive metabolic panel (CMP) from your healthcare provider if you experience any of the warning signs above. This basic blood test measures sodium, potassium, chloride, calcium, and bicarbonate levels. For magnesium, you will need to specifically request a serum magnesium test, as it is not always included in standard panels.
Ideal timing for testing:
Before starting your GLP-1 medication (baseline)
4-6 weeks after starting treatment
After any dose increase
Quarterly during stable dosing
Immediately if warning symptoms appear
People at higher risk for electrolyte problems include those over 65, anyone with kidney disease, heart failure patients, people taking diuretics, and anyone with persistent GI symptoms lasting beyond the first 8-12 weeks of treatment. If you fall into any of these categories and are taking a GLP-1 injection, proactive monitoring is not optional. It is essential.
Complete electrolyte protocol for GLP-1 users
Theory is useful. Protocols are what actually change outcomes. Here are three evidence-based electrolyte protocols designed specifically for people on GLP-1 medications, ranging from minimal intervention to comprehensive coverage.
Protocol 1: the foundation (for mild or no GI symptoms)
Who this is for: People tolerating their GLP-1 medication well, with minimal nausea and no vomiting or diarrhea. Eating reduced portions but still maintaining reasonable food intake.
Daily targets:
Sodium: 1,500-2,000mg from food and supplementation
Potassium: 3,500-4,700mg primarily from food
Magnesium glycinate: 200-300mg supplemental
Calcium citrate: 500-600mg supplemental (if dietary intake is low)
Vitamin D: 1,000 IU daily
Implementation:
Morning: magnesium glycinate (200mg) with breakfast
Midday: electrolyte drink mix (one serving) or bone broth
Evening: calcium citrate (500mg) with vitamin D at dinner
Focus on potassium-rich foods at every meal
This protocol covers the basics. It addresses the most common deficiencies without overcomplicating your routine. For people who are in the early weeks of treatment, following the semaglutide week-by-week timeline or tirzepatide weight loss timeline, this protocol should start from day one.
Protocol 2: the enhanced protocol (for moderate GI symptoms)
Who this is for: People experiencing regular nausea, occasional vomiting, or periodic diarrhea. Eating significantly less than before treatment. Noticing symptoms like fatigue, headaches, or muscle cramps.
Daily targets:
Sodium: 2,000-2,500mg from food and supplementation
Potassium: 4,000-4,700mg from food and conservative supplementation
Magnesium glycinate: 300-400mg supplemental
Calcium citrate: 600-1,000mg supplemental (divided doses)
Vitamin D: 2,000 IU daily
Implementation:
Morning: magnesium glycinate (200mg) with food, electrolyte drink
Midday: bone broth (400-500mg sodium), potassium-rich snack
Afternoon: second electrolyte drink or salt tablet
Evening: magnesium glycinate (200mg), calcium citrate (500mg), vitamin D
Before bed: additional magnesium if experiencing cramps or insomnia
This protocol is appropriate during dose escalation phases when side effects typically peak. Many people find they can step back down to Protocol 1 once they stabilize on their target dose.
Protocol 3: the intensive protocol (for significant GI symptoms)
Who this is for: People with frequent vomiting (more than twice daily), persistent diarrhea (more than three times daily), or inability to maintain adequate oral intake. This protocol bridges the gap until symptoms improve. Medical supervision is required.
Daily targets:
Sodium: 2,500-3,000mg with medical guidance
Potassium: 4,700mg or more with medical monitoring
Magnesium glycinate: 350mg supplemental (upper limit)
Calcium citrate: 1,000-1,200mg supplemental (divided doses)
Vitamin D: 2,000 IU daily
Oral rehydration solution (ORS): As needed after each episode of fluid loss
Implementation:
Sip ORS continuously throughout the day
Small frequent electrolyte doses rather than large single doses
Bone broth as tolerated between meals
Magnesium and calcium in divided doses to maximize absorption
Daily symptom tracking including fluid intake, urine color, and episodes of vomiting or diarrhea
Contact provider if unable to keep fluids down for more than 24 hours
If you are on Protocol 3, talk to your healthcare provider about whether a dose adjustment is appropriate. Severe GI symptoms that prevent adequate nutrition and hydration may warrant temporarily reducing your dose until your body adjusts.
Best electrolyte products and what to look for
The electrolyte supplement market has exploded in recent years, especially with the growth of GLP-1 medications. Not all products are created equal. Some are basically sugar water with marketing. Others contain the wrong ratios. Here is what to look for and what to avoid.
What makes a good electrolyte product for GLP-1 users
Low or zero sugar. This is non-negotiable. Many traditional sports drinks contain 30-40 grams of sugar per serving. When you are on a GLP-1 medication for weight management, adding liquid sugar undermines the entire purpose. Look for products sweetened with stevia, monk fruit, or no sweetener at all.
Balanced mineral ratios. A good GLP-1-friendly electrolyte product contains approximately 200-300mg sodium, 100-200mg potassium, and 50-100mg magnesium per serving. Products that are almost entirely sodium with minimal other minerals are designed for extreme athletes, not for people managing medication side effects.
Citrate-based minerals. Sodium citrate and potassium citrate tend to sit better on nauseated stomachs than other mineral forms. If your primary concern is being able to actually keep the electrolytes down, citrate formulations are worth prioritizing.
No artificial colors or unnecessary additives. When your GI system is already sensitive from GLP-1 medications, the fewer unnecessary ingredients, the better. Simple formulas with clean ingredient lists reduce the risk of additional stomach irritation.
Types of electrolyte products
Electrolyte powder packets. These dissolve in water and provide a convenient, customizable way to increase electrolyte intake throughout the day. Most popular options come in single-serving packets that you can carry anywhere. They are typically the most cost-effective option per serving.
Electrolyte tablets. Effervescent tablets that dissolve in water. Convenient and portable but sometimes limited in mineral variety. Good as a secondary option when you are traveling with semaglutide or traveling with tirzepatide and need something compact.
Electrolyte capsules. Swallowed like any supplement. No taste, no mixing. The downside is that they do not contribute to fluid intake the way drink mixes do. Best used alongside adequate water consumption.
Coconut water. A natural electrolyte source providing approximately 600mg potassium, 252mg sodium, and 60mg magnesium per 16oz serving. Lower in sodium than ideal for GLP-1 users but excellent for potassium. Combine with a pinch of salt to balance the mineral ratio.
Bone broth. The all-star option for GLP-1 users. Provides sodium, potassium, calcium, magnesium, and collagen in a warm, easy-to-consume format. Ideal for days when solid food is difficult. One cup typically contains 400-500mg sodium, making it a significant contributor to daily sodium goals. It pairs well with the nutritional approach in a semaglutide food guide or tirzepatide food guide.
What to avoid in electrolyte products
High-sugar sports drinks like Gatorade or Powerade. They contain too much sugar and not enough electrolytes for this purpose. Diet versions are marginally better but still have poor mineral profiles.
Products with very high sodium and nothing else. Some electrolyte products marketed for athletes contain 1,000mg+ of sodium per serving with minimal potassium or magnesium. This is too aggressive for daily GLP-1 support and can cause water retention and bloating.
Products containing artificial sweeteners that trigger GI symptoms. Sucralose and sugar alcohols (sorbitol, maltitol, mannitol) can cause bloating and diarrhea in sensitive individuals. When your gut is already dealing with a GLP-1 medication, these sweeteners can amplify discomfort.

Electrolyte timing strategies that maximize absorption
When you take electrolytes matters almost as much as which electrolytes you take. Timing strategies can reduce nausea, improve absorption, and prevent the peaks and valleys that cause symptoms.
The morning foundation
Your body has been fasting for 8-10 hours overnight. Electrolyte levels are at their lowest point of the day. Starting your morning with electrolytes before food sets a strong foundation.
Within 30 minutes of waking: one serving of electrolyte drink mix in 16oz of water. Sip it slowly. Do not chug it, as large volumes of fluid consumed quickly can trigger nausea, especially on GLP-1 medications. This single habit addresses the overnight deficit and gives you a head start on the day.
If you take your semaglutide dose in the morning or your tirzepatide injection in the morning, have your electrolyte drink 30-60 minutes before or after the injection, not simultaneously.
The steady-state approach
The worst strategy for electrolytes is taking everything at once. Large single doses are poorly absorbed and more likely to cause stomach upset. The best strategy is small, frequent doses throughout the day.
Think of it like stoking a fire. Small amounts of fuel added regularly keep the fire burning steadily. One massive load dumped all at once smothers it.
A practical approach: divide your daily electrolyte intake into 4-6 smaller portions spread across the day. One electrolyte drink in the morning. Bone broth at midday. Another electrolyte serving in the afternoon. Magnesium at night. This steady approach maintains more consistent blood levels and is much gentler on the stomach.
Timing around meals
Magnesium and calcium are best absorbed when taken with food. Sodium and potassium can be taken with or without food. If you are planning your caloric intake on tirzepatide or figuring out how many calories to eat on semaglutide, building electrolyte-rich foods and supplements around your meals simplifies the entire process.
Take calcium and magnesium at different times of day. High doses of calcium can interfere with magnesium absorption and vice versa. Morning calcium, evening magnesium (or the reverse) works well for most people.
Timing around GI episodes
After any episode of vomiting or diarrhea, electrolyte replacement should happen within 30 minutes. Small sips of an oral rehydration solution or electrolyte drink are better than waiting until the next scheduled dose. The body loses electrolytes in real time during these episodes, and delays in replacement extend the period of deficiency.
If nausea prevents you from drinking, try:
Ice chips made from electrolyte solution
Frozen electrolyte popsicles
Tiny sips (1-2 tablespoons) every 5-10 minutes
Room-temperature fluids (cold can worsen nausea for some people)
Timing on injection day
Many GLP-1 users report that side effects peak in the 24-48 hours following their injection. Planning extra electrolyte support around injection day can reduce the impact. The day before your injection, the day of, and the day after should all include enhanced electrolyte intake. Think of it as pre-loading your mineral reserves before the most demanding period.
This is especially relevant during the early weeks of compounded tirzepatide or when starting semaglutide for the first time, when your body is still adapting to the medication.
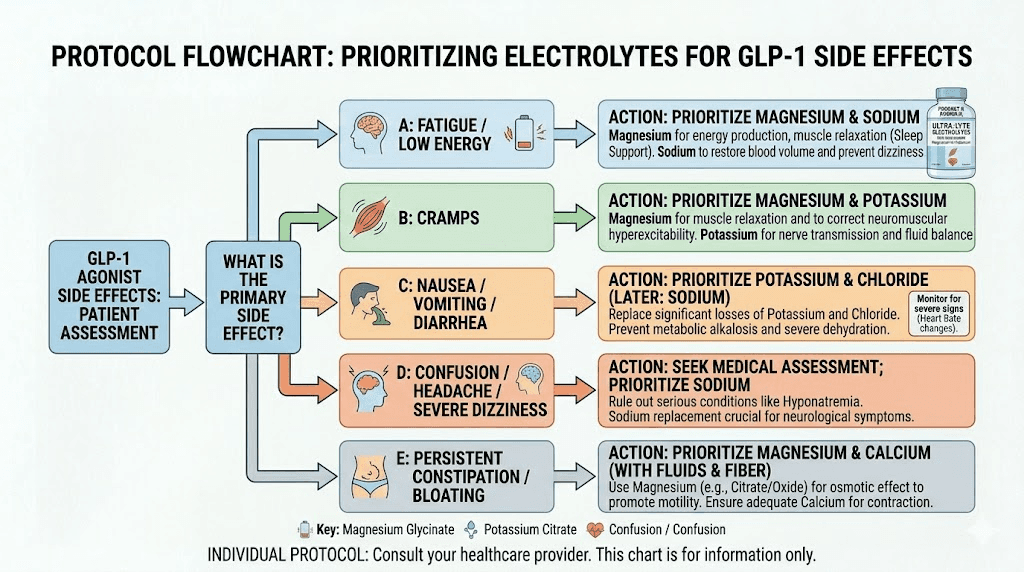
Electrolytes and specific GLP-1 side effects
Different side effects respond to different electrolyte interventions. Here is a targeted breakdown of which minerals to prioritize based on what you are experiencing.
For fatigue and low energy
Fatigue is the most common complaint among GLP-1 users, and it has multiple potential causes. From an electrolyte perspective, low sodium and low magnesium are the primary culprits.
First, check your sodium intake. Aim for at least 1,500mg daily from all sources. If you have been avoiding salt, this is the time to stop avoiding it. Second, ensure your magnesium intake is adequate. Third, rule out other nutritional causes. People on GLP-1 medications often develop vitamin B12 deficiency alongside electrolyte deficits, which also causes fatigue.
If supplementing with B12, electrolytes, and eating adequate protein does not resolve the fatigue, discuss further testing with your provider. Thyroid function, iron levels, and vitamin D status should all be evaluated. Understanding energy changes on semaglutide requires looking at the whole picture, not just one variable.
For nausea management
Electrolytes alone will not eliminate GLP-1-related nausea, but they can reduce its severity. Dehydration and low sodium both worsen nausea independently. Correcting these creates a less hostile internal environment.
Ginger combined with electrolytes is a powerful combination. Ginger root has well-documented anti-nausea properties. Many electrolyte products now include ginger for this reason. If yours does not, brewing ginger tea and adding a pinch of salt and a splash of coconut water creates an effective DIY anti-nausea electrolyte drink.
Small sips work better than large gulps. The best tips for managing semaglutide consistently include the advice to sip fluids slowly throughout the day rather than drinking large amounts at once.
For muscle cramps and body aches
Magnesium, potassium, and calcium all play roles in muscle contraction and relaxation. A deficit in any of them can cause cramps.
Start with magnesium glycinate (300-400mg daily) as it is the most common deficiency and the easiest to correct. If cramps persist after two weeks of consistent magnesium supplementation, add focused potassium intake through dietary sources. If they still persist, calcium deficiency should be investigated.
For muscle pain on tirzepatide that is more diffuse than localized cramps, a combined magnesium-potassium-calcium approach often works better than targeting a single mineral. Creatine supplementation alongside tirzepatide can also help with muscle function and may complement electrolyte supplementation.
For constipation
Magnesium citrate is the electrolyte hero for constipation. Its osmotic effect draws water into the intestines, softening stool and stimulating motility. Start with 200mg and increase gradually to 400mg as needed. Do not exceed 400mg per day without medical guidance.
Potassium also supports bowel motility. Ensuring adequate potassium through food sources complements magnesium supplementation. Combined with adequate water intake and fiber supplementation, this three-pronged approach addresses constipation from multiple angles simultaneously.
A comprehensive approach to GLP-1 constipation relief should always include electrolyte optimization as a foundational step.
For brain fog and cognitive symptoms
Brain fog on GLP-1 medications is often linked to a combination of dehydration, low sodium, and low magnesium. The brain is extremely sensitive to electrolyte imbalances. Even mild hyponatremia (low sodium) can cause confusion, difficulty concentrating, and mental sluggishness.
Address sodium first. Then ensure magnesium intake is adequate. If cognitive symptoms persist, consider magnesium threonate specifically, as it is the only form shown to effectively cross the blood-brain barrier and increase brain magnesium levels.
B vitamins also play a role in cognitive function. Many supplements recommended alongside tirzepatide include B-complex vitamins for this reason. Combining electrolyte optimization with adequate B vitamin intake addresses the two most common nutritional causes of brain fog during GLP-1 treatment.
For heart palpitations
Heart palpitations require immediate attention. Both low potassium and low magnesium can cause cardiac rhythm disturbances. If you experience palpitations:
Step one: contact your healthcare provider. Do not attempt to self-treat cardiac symptoms with supplements alone.
Step two: request bloodwork including a comprehensive metabolic panel and magnesium level.
Step three: while waiting for results, ensure adequate potassium and magnesium intake from food sources. Do not start high-dose supplementation without medical guidance, as both excessively high and excessively low levels of these minerals affect heart rhythm.
Magnesium taurate is often recommended for cardiovascular support because taurine itself has cardioprotective properties. But this recommendation should come from your provider, not from an internet guide.
Hydration and electrolytes: why water alone is not enough
This is one of the most misunderstood aspects of GLP-1 treatment. People hear "stay hydrated" and they drink water. Lots of water. Three liters a day. Four liters. And they still feel terrible.
Here is why. Water without electrolytes does not hydrate you properly. In fact, drinking large amounts of plain water when electrolytes are already low can make things worse by diluting blood sodium levels further. This condition, called dilutional hyponatremia, causes the exact same symptoms people are trying to fix: headaches, fatigue, nausea, and confusion.
True hydration requires both water AND electrolytes. The electrolytes enable your cells to actually absorb and retain the water you drink. Without them, much of that water passes straight through.
How much fluid do GLP-1 users actually need?
Most guidelines recommend 2-3 liters of total fluid per day for people on GLP-1 medications. But this should not all be plain water. A practical breakdown:
Plain water: 1-1.5 liters
Electrolyte-enhanced water or drinks: 0.5-1 liter
Bone broth, herbal tea, or other hydrating beverages: 0.5-1 liter
This distribution ensures you are getting both the fluid volume and the mineral content your body needs. The exact amounts depend on your body weight, activity level, climate, and the severity of any GI side effects.
The urine color test
One of the simplest ways to monitor hydration status. Pale yellow urine indicates adequate hydration. Dark yellow or amber urine suggests dehydration. Clear, colorless urine may actually indicate overhydration and potential electrolyte dilution.
Aim for pale straw-colored urine throughout the day. If it is consistently dark despite drinking adequate fluids, you likely need more electrolytes, not more water.
Hydration strategies for people who can barely eat
Some people on GLP-1 medications go through periods where eating feels nearly impossible. The appetite suppression is profound. During these times, hydration and electrolyte intake become even more critical because you are not getting any minerals from food.
Strategies that work:
Sipping bone broth throughout the day provides sodium, potassium, calcium, small amounts of protein, and collagen in liquid form. Many people find that warm bone broth is one of the few things they can consistently tolerate, even during peak nausea.
Coconut water with a pinch of salt provides a natural potassium-rich base with added sodium. Keep it room temperature if cold drinks worsen nausea.
Electrolyte popsicles made from diluted electrolyte solution can be easier to tolerate than drinks during severe nausea. The cold and the slow rate of consumption both help manage the nausea while getting minerals in.
Smoothies blended with spinach, banana, yogurt, and a pinch of salt pack multiple electrolytes into a few sips. Even a quarter cup provides meaningful mineral content during periods of extremely low intake. Protein shakes for GLP-1 users can serve double duty as both protein and electrolyte sources when made with the right ingredients.
Special considerations for different GLP-1 medications
While electrolyte principles apply across all GLP-1 medications, there are some differences worth noting between specific medications.
Semaglutide (Ozempic, Wegovy, compounded)
Semaglutide has a longer half-life than some other GLP-1 medications, meaning side effects can be more sustained throughout the week rather than concentrated in the days immediately following injection. This means electrolyte depletion tends to be more gradual and chronic rather than acute.
For semaglutide users, the steady-state approach to electrolyte supplementation works well. Consistent daily intake rather than reactive supplementation after symptoms appear. If you are following a semaglutide dosage chart for dose escalation, increase your electrolyte protocol with each dose increase.
Common semaglutide side effects that respond well to electrolyte management include fatigue, sulfur burps, acid reflux, and feeling cold. While electrolytes will not eliminate all of these, adequate mineral status reduces their severity in most cases.
Tirzepatide (Mounjaro, Zepbound, compounded)
Tirzepatide is a dual GIP/GLP-1 agonist, meaning it activates two receptor types instead of one. This dual mechanism tends to produce stronger appetite suppression and, in some cases, more pronounced GI side effects during dose escalation.
Tirzepatide users may need more aggressive electrolyte support during the initial dose escalation phase compared to semaglutide users. The tirzepatide dosing schedule involves increases every four weeks, and each increase can temporarily worsen GI symptoms and electrolyte losses.
The connection between tirzepatide and specific side effects like feeling cold, dry mouth, and bloating often has an electrolyte component. Addressing mineral deficits alongside other management strategies provides the best results.
Compounded versus brand-name medications
The electrolyte considerations are identical regardless of whether you are using brand-name or compounded semaglutide. The active medication works the same way. However, compounded formulations sometimes include additional ingredients like glycine, methylcobalamin (B12), niacinamide, or L-carnitine that may support overall nutritional status.
Similarly, compounded tirzepatide may include glycine and B12, niacinamide, or levocarnitine. These additions can reduce some side effects but they do not replace the need for electrolyte supplementation.
Electrolyte-rich meal planning on GLP-1 medications
Supplements are important, but food remains the best source of electrolytes. The challenge is getting enough from food when your appetite is significantly reduced. The solution is intentional meal planning that maximizes mineral density in every bite.
High-electrolyte breakfast options
Even a small breakfast can provide significant electrolytes if you choose the right foods.
Avocado toast with salt (2-3 bites worth): One-quarter avocado on whole-grain toast with a generous pinch of salt provides approximately 240mg potassium, 150mg sodium, and 15mg magnesium. Small, nutrient-dense, and usually tolerable even with reduced appetite.
Greek yogurt with banana and nuts: A half-cup of Greek yogurt with half a banana and a tablespoon of almonds delivers approximately 350mg potassium, 200mg calcium, 50mg magnesium, and 30mg sodium. Add a pinch of salt to boost sodium.
Smoothie foundation: Blend spinach, banana, yogurt, coconut water, and a pinch of salt. Even 8oz of this combination packs potassium, magnesium, calcium, and sodium into a drinkable format. Perfect for mornings when solid food feels impossible. Check out GLP-1 breakfast ideas for more options that prioritize both nutrition and tolerability.
High-electrolyte lunch and dinner ideas
Salmon with sweet potato and spinach: This combination is an electrolyte powerhouse. A 4oz salmon fillet provides 450mg potassium and 50mg magnesium. A small sweet potato adds 540mg potassium and 30mg magnesium. A cup of cooked spinach contributes 839mg potassium and 157mg magnesium. Season generously with salt.
White bean soup with bone broth base: Using bone broth as the soup base provides sodium and collagen. White beans add massive potassium (1,004mg per cup). Add vegetables for additional minerals. This one-bowl meal can be made in advance and reheated in small portions throughout the week. It fits perfectly into a GLP-1 dinner rotation.
Baked potato bar: A medium baked potato with skin provides 926mg potassium. Top it with a small amount of plain yogurt (instead of sour cream) for calcium, sprinkle with salt for sodium, and add steamed broccoli for magnesium. Simple, inexpensive, and extremely electrolyte-dense.
For more complete meal planning frameworks, the tirzepatide meal plan and best foods for semaglutide guides provide detailed day-by-day plans.
Snacks that pack electrolyte value
When you can only manage a few bites between meals, make those bites count.
Salted almonds (1oz): 76mg magnesium, 200mg potassium, 95mg sodium
Banana with peanut butter: 422mg potassium, 49mg magnesium
Edamame with salt: 676mg potassium, 99mg magnesium per cup
Dried apricots (5 pieces): 407mg potassium
Dark chocolate (1oz, 70%+): 64mg magnesium, 203mg potassium
Salted pumpkin seeds (1oz): 156mg magnesium, 261mg potassium
These snacks are small enough to eat even on days when appetite is minimal, yet they provide meaningful amounts of critical electrolytes. Keeping them accessible means you are never far from a mineral-rich option. Knowing which foods to avoid on tirzepatide is equally important, as some common choices can worsen GI symptoms and interfere with electrolyte absorption.
Electrolyte interactions with other supplements and medications
If you are taking other supplements or medications alongside your GLP-1, electrolyte timing and dosing may need adjustment.
Metformin and electrolytes
Many people take metformin alongside their GLP-1 medication. Metformin can reduce vitamin B12 absorption and may affect magnesium levels over time. If you are on both metformin and semaglutide or metformin and tirzepatide, pay extra attention to magnesium and B12 levels. More frequent testing is warranted.
Diuretics and electrolytes
Blood pressure medications like thiazide diuretics or loop diuretics actively deplete potassium, sodium, and magnesium. Combined with a GLP-1 medication, the electrolyte losses can be substantial. If you take any diuretic, your healthcare provider should be monitoring electrolyte levels closely and may recommend specific supplementation protocols.
Berberine and electrolytes
Some people take berberine alongside tirzepatide or berberine with semaglutide for additional metabolic support. Berberine can have its own GI side effects (diarrhea, nausea) that compound with GLP-1 side effects. If you are using both, increase electrolyte supplementation accordingly and monitor for signs of excessive fluid loss.
Phentermine and electrolytes
Some providers prescribe phentermine with semaglutide or phentermine with tirzepatide. Phentermine can reduce appetite even further and increase heart rate, making both adequate nutrition and electrolyte balance more important. Pay particular attention to potassium and magnesium, which both affect cardiac function.
Creatine and electrolytes
Creatine supplementation is increasingly popular among GLP-1 users for muscle preservation during weight loss. Creatine and GLP-1 medications can be taken together, but creatine pulls water into muscle cells, which can increase fluid requirements. Increase water and electrolyte intake by about 20% if you add creatine to your supplement routine.
Probiotics and electrolytes
GLP-1 medications alter gut motility, which can affect the microbiome. Probiotics for semaglutide users and products like Pendulum GLP-1 probiotic may help normalize GI function, which in turn can reduce electrolyte losses from diarrhea. Healthy gut bacteria also produce short-chain fatty acids that improve mineral absorption. Supporting gut health and electrolyte balance simultaneously creates a positive feedback loop.
Long-term electrolyte management
Electrolyte needs change as your GLP-1 treatment progresses. The strategies that work during month one may not be exactly what you need at month six or month twelve.
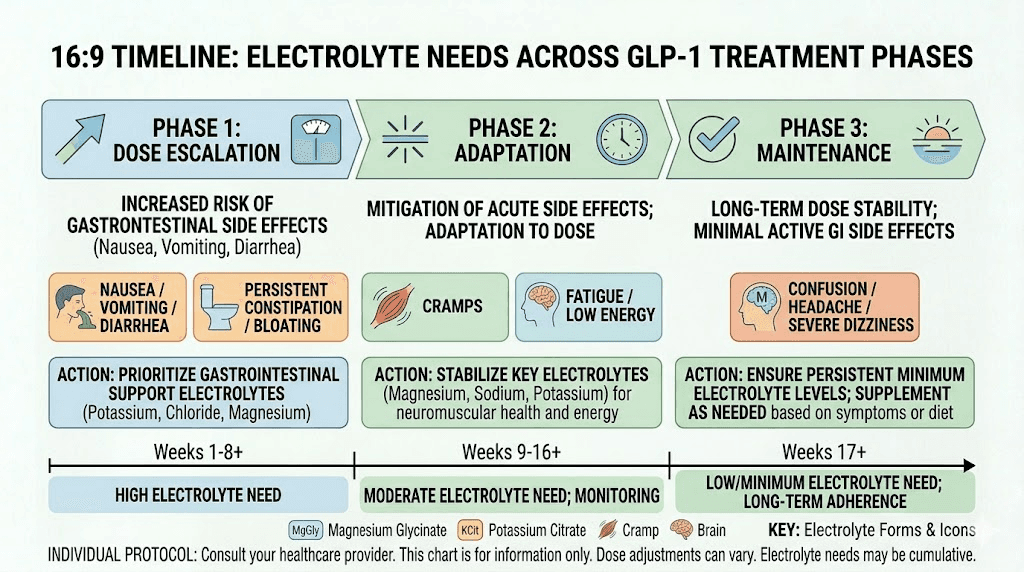
During dose escalation (months 1-4)
This is the most demanding period for electrolyte management. Each dose increase can temporarily worsen GI symptoms and reduce food intake further. Plan to use Protocol 2 or Protocol 3 during dose escalation, stepping back to Protocol 1 once you stabilize.
Track your symptoms daily during this phase. A simple journal noting energy levels, any cramps, headaches, or digestive symptoms helps you identify patterns and adjust supplementation proactively rather than reactively. Understanding what to expect in your first month on tirzepatide or semaglutide one-month results includes knowing that electrolyte needs are highest during this period.
During stable dosing (months 4+)
Once you are on a stable dose and side effects have lessened, Protocol 1 is usually sufficient. Your food intake has likely stabilized at a lower but consistent level, and GI symptoms have generally resolved or become manageable.
However, do not become complacent. You are still eating less than before treatment, which means ongoing electrolyte vigilance is necessary. Continue with at least baseline supplementation (magnesium and a daily electrolyte drink) indefinitely while on the medication.
Quarterly bloodwork including electrolyte levels helps catch any gradual deficiencies before they cause symptoms. This is especially true for long-term semaglutide use.
During weight maintenance
When you reach your goal weight and either reduce your dose or transition to a maintenance protocol, electrolyte needs shift again. If your food intake increases during maintenance, dietary electrolytes may cover more of your needs. But if you continue on the medication at any dose, some degree of supplementation is likely still beneficial.
For people exploring maintaining weight loss after tirzepatide or considering weaning off tirzepatide, maintaining good electrolyte habits during the transition protects against rebound symptoms.
If you stop treatment
When you discontinue a GLP-1 medication, whether through stopping tirzepatide or stopping semaglutide, appetite and food intake typically increase. This natural return of appetite usually resolves electrolyte deficits as dietary mineral intake rises. However, continuing magnesium supplementation is often worthwhile since most people are deficient regardless of medication status.
Semaglutide withdrawal symptoms can include increased appetite, blood sugar fluctuations, and weight regain. Maintaining stable electrolyte levels during this transition helps minimize additional disruption.
Electrolytes and alcohol on GLP-1 medications
Alcohol and GLP-1 medications have a complicated relationship. Many people wonder whether they can drink on semaglutide or whether alcohol is safe with tirzepatide. From an electrolyte perspective, alcohol makes everything harder.
Alcohol is a diuretic. It suppresses antidiuretic hormone (ADH), causing your kidneys to excrete more water and electrolytes than they normally would. One alcoholic drink can increase urine output by 320-950ml over the following hours. Each trip to the bathroom flushes sodium, potassium, and magnesium.
Combined with the fluid losses already happening from GLP-1 side effects, even moderate alcohol consumption can push electrolyte levels into problematic territory. The resulting dehydration and mineral depletion explain why hangovers feel significantly worse on GLP-1 medications than they did before.
If you do choose to drink, and your healthcare provider has approved it, the electrolyte strategy is straightforward. Before drinking, consume a full serving of electrolyte drink. Between each alcoholic beverage, have 8-12oz of electrolyte water. Before bed, take another serving of electrolytes with 16oz of water. The morning after, prioritize electrolyte-rich fluids before coffee or food.
For those choosing to drink on GLP-1 medications, understanding the best alcohol options on tirzepatide can help minimize the impact. Lower-sugar options with lower alcohol content create less disruption to electrolyte balance.
The role of electrolytes in preventing GLP-1 related hair loss
One of the most distressing side effects reported by GLP-1 users is hair thinning or loss. While the primary cause is telogen effluvium triggered by rapid weight loss and caloric restriction, nutritional deficiencies play a significant contributing role. And electrolyte imbalances are part of that picture.
Zinc, iron, and biotin get most of the attention in hair loss discussions. But magnesium and calcium deficiencies also affect hair growth. Magnesium helps regulate calcium levels, and calcium signaling is involved in hair follicle cycling. Low magnesium can disrupt normal hair growth patterns, contributing to increased shedding.
Ensuring adequate electrolyte intake will not prevent all GLP-1-related hair loss. The rapid weight loss component is the primary driver. But optimizing mineral status reduces one contributing factor and supports overall health during the weight loss process. For a comprehensive approach to this issue, the GLP-1 hair loss guide covers all the interventions worth considering, including the nutritional foundations that electrolytes support.
A balanced supplementation approach that includes magnesium, calcium with vitamin D, and a quality multivitamin addresses the most common nutritional gaps during GLP-1 treatment. Combined with adequate protein intake on semaglutide, this strategy gives hair follicles the best possible nutritional environment despite reduced caloric intake.
DIY electrolyte recipes for GLP-1 users
Commercial electrolyte products work well but they are not the only option. Homemade electrolyte solutions can be equally effective and allow you to control exactly what goes in.
Basic oral rehydration solution
Mix 1 liter of water with half a teaspoon of salt (1,150mg sodium), a quarter teaspoon of salt substitute (potassium chloride, approximately 650mg potassium), and 2 tablespoons of honey or maple syrup for palatability. This matches the WHO recommended oral rehydration formula and is ideal for days with significant fluid losses.
GLP-1 morning tonic
Combine 16oz of warm water with a quarter teaspoon of pink Himalayan salt (575mg sodium), juice of half a lemon (80mg potassium plus vitamin C), and a tablespoon of raw honey. Sip slowly over 30 minutes. The warmth helps settle the stomach, the salt replaces sodium lost overnight, and the lemon provides a small potassium boost with flavor.
Anti-nausea electrolyte drink
Brew 12oz of ginger tea using fresh ginger root. Let it cool to room temperature. Add a pinch of salt (approximately 300mg sodium), 4oz of coconut water (150mg potassium), and squeeze in a quarter of a lime. Ginger calms the stomach while the electrolytes replenish minerals. This combination specifically targets the dual challenge of nausea and electrolyte depletion that defines the GLP-1 experience for many people.
Electrolyte ice cubes
Prepare a batch of electrolyte solution and freeze it in ice cube trays. Pop two or three cubes into plain water throughout the day for a slow-release electrolyte delivery system. Or suck on the cubes directly during episodes of nausea when drinking feels impossible. This method provides tiny, consistent doses of minerals without overwhelming a sensitive stomach.
These homemade options cost pennies per serving compared to commercial products. They are customizable, use whole ingredients, and avoid the artificial additives that can irritate GLP-1-sensitive stomachs. Combined with the GLP-1 recipes designed for weight loss, they form part of a complete nutritional strategy.
Common mistakes people make with electrolytes on GLP-1 medications
After reviewing thousands of discussions in GLP-1 communities and analyzing the most common electrolyte-related complaints, these patterns emerge repeatedly.
Mistake 1: drinking only plain water
The most common mistake by far. People drink 3+ liters of plain water daily, feel terrible, and cannot figure out why. They are diluting their already-low electrolyte levels. The fix is simple: replace at least a third of daily water intake with electrolyte-enhanced fluids.
Mistake 2: avoiding sodium entirely
Years of "reduce your salt" messaging has trained many people to fear sodium. On a GLP-1 medication with reduced food intake, this fear becomes counterproductive. Your body needs sodium. Not excessive amounts, but adequate amounts. If you have been salting your food sparingly or not at all, this is the time to reconsider.
Mistake 3: taking all supplements at once
Swallowing magnesium, calcium, potassium, and a multivitamin all at the same time reduces absorption of each one. Calcium and magnesium compete for absorption. Iron inhibits calcium absorption. Spreading supplements throughout the day improves how much your body actually uses.
Mistake 4: using magnesium oxide
It is the cheapest and most widely available form, which is why people default to it. But with only 4% bioavailability, you are essentially paying for expensive diarrhea. Switch to glycinate, citrate, or any other form with better absorption.
Mistake 5: ignoring symptoms as "just the medication"
Chronic headaches, persistent fatigue, ongoing muscle cramps, and worsening brain fog are not normal features of GLP-1 treatment that you should just accept. They are often correctable signals of electrolyte deficiency. Treating them early prevents them from compounding into more serious problems.
Mistake 6: not adjusting during dose escalation
Electrolyte needs increase during each dose increase. The protocol that worked at 2.5mg of tirzepatide may not be adequate at 5mg or 7.5mg. Proactively increasing electrolyte support before each dose increase prevents reactive scrambling after symptoms appear.
Mistake 7: forgetting about food as a primary source
Supplements fill gaps, but food provides electrolytes in forms your body absorbs most efficiently, along with cofactors that enhance absorption. Even on reduced appetite, making every calorie count by choosing mineral-dense foods is the most effective long-term strategy. Whether you follow a specific semaglutide food guide or create your own plan, electrolyte density should be a primary criteria for food selection.
Frequently asked questions
Can I take too many electrolytes while on a GLP-1 medication?
Yes. Excessive electrolyte supplementation carries real risks. Too much potassium (hyperkalemia) can cause dangerous heart rhythm disturbances. Too much sodium can cause high blood pressure and fluid retention. Too much magnesium from supplements can cause diarrhea and, in extreme cases, cardiac complications. Follow recommended dosages, get baseline bloodwork, and work with your healthcare provider to determine what your body actually needs.
Should I take electrolytes on injection day or skip them?
Take them, and consider increasing your intake. Injection day and the 24-48 hours following are often when side effects peak and electrolyte losses are highest. Pre-loading electrolytes before your injection can reduce the severity of post-injection symptoms.
Do electrolyte supplements break a fast?
Most electrolyte supplements contain zero or minimal calories and do not break a fast. Electrolyte powders without sugar, salt tablets, and mineral capsules are all fine during fasting periods. Products containing sugar or significant calories will break a fast. Check labels carefully.
How soon after starting a GLP-1 medication should I start electrolyte supplementation?
Immediately. Do not wait for symptoms to appear. Start electrolyte supplementation on day one of your first week on semaglutide or first dose of tirzepatide. Proactive supplementation prevents deficits from developing. Reactive supplementation after symptoms appear means you are already behind.
Can electrolyte supplementation improve my weight loss results?
Indirectly, yes. When electrolyte levels are adequate, you feel better. Better energy means more physical activity. Less fatigue means more consistent medication adherence. Fewer side effects means less temptation to reduce your dose prematurely. While electrolytes do not directly cause weight loss, they create the conditions that allow your medication to work optimally. People who plateau on their medication, wondering why semaglutide is not working or why tirzepatide results have stalled, sometimes find that optimizing nutrition and electrolytes breaks the stall.
Are there electrolyte products specifically designed for GLP-1 users?
A growing number of products are being marketed specifically for GLP-1 medication users. Some are genuinely well-formulated with appropriate mineral ratios and gentle ingredients. Others are basic electrolyte products with a premium price tag and GLP-1 marketing. Read the ingredient labels and mineral amounts rather than relying on marketing claims. A well-formulated general electrolyte product at half the price often provides identical benefits.
Should I adjust electrolytes if I exercise while on a GLP-1 medication?
Absolutely. Exercise increases sweat losses, which deplete sodium, potassium, magnesium, and chloride. If you are exercising regularly on a GLP-1 medication, add a serving of electrolytes before and after workouts in addition to your baseline daily protocol. This is especially important for people maintaining active fitness routines alongside their weight loss treatment.
Can I get all my electrolytes from food alone?
In theory, yes. In practice, it is extremely difficult when appetite is significantly suppressed. The daily potassium target alone (4,700mg) is hard to reach even with normal appetite. With GLP-1-reduced appetite, supplementation is almost always necessary for at least sodium, magnesium, and often calcium. Use food as your foundation and supplements to fill the gaps.
External resources
For researchers serious about optimizing their GLP-1 experience, SeekPeptides provides comprehensive protocol guides, dosing calculators, and evidence-based resources that cover every aspect of peptide therapy, from electrolyte management to advanced stacking strategies. SeekPeptides members get access to personalized support, detailed protocols, and a community of experienced researchers who have navigated these exact challenges.
In case I do not see you, good afternoon, good evening, and good night. May your electrolytes stay balanced, your energy stay steady, and your GLP-1 results stay on track.