Mar 21, 2026

Some people lose 15 pounds in their first month on a GLP-1. Others step on the scale after four weeks and wonder if the medication is even working. Both experiences are normal. Both are documented in clinical trials. And both can leave you confused about what "average" weight loss on a GLP-1 actually looks like.
The problem with averages is simple. They flatten thousands of individual experiences into a single number. A clinical trial might report 5% body weight loss at 12 weeks, but that number includes the person who lost 20 pounds and the person who lost 3. It includes the patient who started at 350 pounds and the one who started at 180. It includes people who overhauled their diet and people who changed nothing except adding a weekly injection.
So when you search for "GLP-1 average weight loss per month," you are really asking the wrong question. The better question is: what does the weight loss trajectory typically look like, what factors push results higher or lower, and where will you likely fall on that spectrum? That is exactly what we are going to break down here. Not vague promises. Not cherry-picked transformation photos. Real data from real clinical trials, organized month by month, medication by medication, so you can set expectations that actually match reality. SeekPeptides has compiled the most comprehensive breakdown available, pulling from every major GLP-1 clinical trial published to date. Whether you are considering semaglutide, tirzepatide, or liraglutide, the numbers below will give you a realistic roadmap for what to expect each month.
What "average" GLP-1 weight loss actually means
Before diving into monthly numbers, we need to address why the word "average" causes so much confusion. In clinical trials, researchers report mean weight loss across hundreds or thousands of participants. That mean includes outliers on both ends. It includes people who dropped out early. And it often includes data from the dose escalation phase, when patients are on sub-therapeutic doses.
This matters.
A study might report that participants lost an average of 14.9% of their body weight over 68 weeks on semaglutide. But within that trial, some people lost 25%. Others lost 5%. The distribution is not a neat bell curve, either. It skews based on adherence, starting BMI, dietary habits, and a dozen other variables we will cover later.
Clinical trial data vs. real world results
Clinical trials represent ideal conditions. Participants receive regular follow-ups, dietary counseling, and consistent medication supplies. They are motivated volunteers who agreed to be studied. Real world results tend to be slightly lower, though not dramatically so. A large retrospective study found that real world semaglutide patients lost an average of 14.1% of their body weight at one year, while tirzepatide patients lost 16.5%. Those numbers are close to, but slightly below, what the pivotal trials reported.
The takeaway? Clinical trial averages are a reasonable guide. They are not fantasy numbers. But your individual result will depend on factors specific to you.
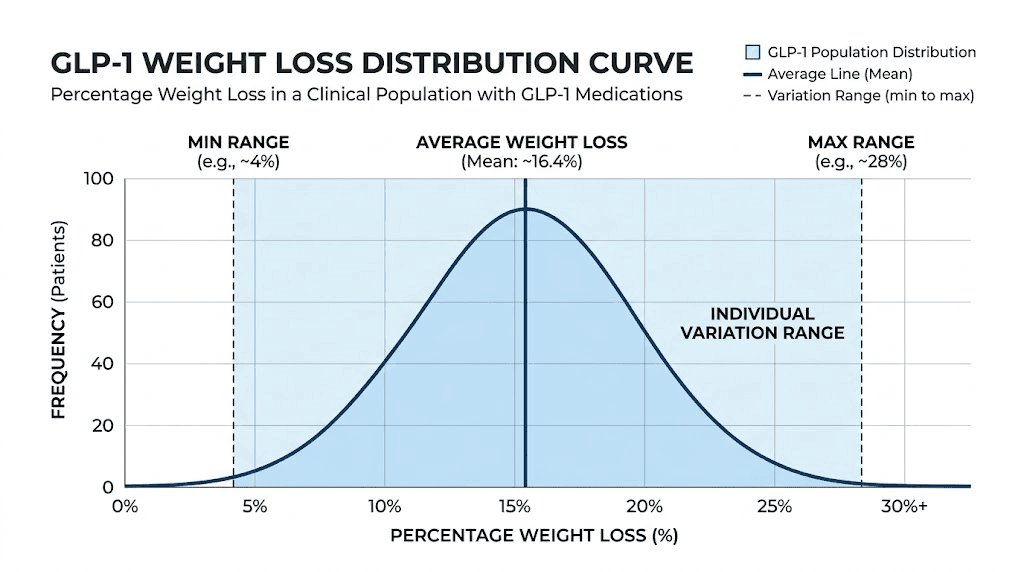
Why individual variation matters more than averages
A Johns Hopkins analysis of nearly 20,000 patients found that women lost an average of 10.88% of their initial body weight on GLP-1 medications, while men lost 6.78%. That is a significant gap. But the study also found that age, race, ethnicity, and starting BMI did not dramatically affect outcomes. The biggest predictors of success were adherence to the medication, dietary changes, and physical activity level.
If you take away one thing from this section, let it be this. Averages tell you what is possible. Your actions determine where you land within that range. Two people on the same medication, at the same dose, can have wildly different results based on what they eat, how they move, and how consistently they take their medication.
Month-by-month weight loss on semaglutide
Semaglutide is the most studied GLP-1 receptor agonist for weight management. The STEP trials, published in the New England Journal of Medicine, provide the most detailed weight loss trajectory data available. Here is what the numbers look like when broken down by month.
Month 1: the starting line
Most people beginning semaglutide start at 0.25 mg weekly for the first four weeks. This is a sub-therapeutic dose. It exists solely for tolerability, to let your gastrointestinal system adjust before the dose increases.
At this dose, weight loss is modest. Expect 2-4% of your body weight during the first month. For someone who weighs 200 pounds, that translates to roughly 4-8 pounds. For someone at 250 pounds, closer to 5-10 pounds.
Some of this initial loss is water weight and glycogen depletion, not pure fat. That is normal. It does not mean the medication is not working. It means your body is adjusting to a fundamentally different appetite and metabolic signaling pattern. You can read more about what to expect during your first week on semaglutide and how semaglutide makes you feel in our detailed guides.
Do not panic if your first month results seem underwhelming. You are still on the lowest dose.
Months 2-3: the acceleration phase
By month two, most patients have escalated to 0.5 mg weekly. By month three, many are at 1.0 mg. This is where appetite suppression becomes more noticeable, and the scale starts moving more consistently.
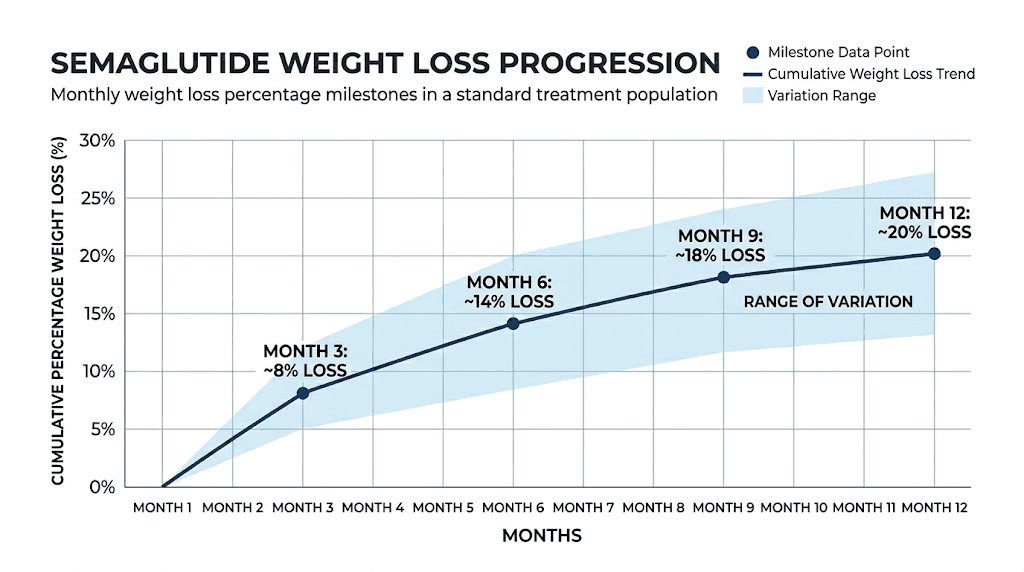
Cumulative weight loss by the end of month three typically reaches 5-8% of starting body weight. Clinical trial data shows a mean loss of approximately 6.7 kg (about 14.7 pounds) at the 12-week mark. For a 200-pound person, that is roughly 10-16 pounds total from baseline. For a 250-pound person, 12-20 pounds.
This phase is important because it often brings the most dramatic shift in appetite suppression. Many people report that food simply becomes less interesting. Cravings for high-calorie foods diminish. Portion sizes drop naturally. If you are not experiencing this effect, it may be worth discussing your dosage in units with your provider.
Months 4-6: steady state
Between months four and six, dose escalation typically continues toward the target dose of 2.4 mg weekly (for Wegovy). Weight loss continues at a steady pace, though the rate may slow slightly compared to the initial months.
By month six, cumulative weight loss averages 8-12% of starting body weight. Clinical data reports approximately 12.3 kg (about 27 pounds) of mean weight loss at the 6-month mark, equivalent to 10.9% of initial body weight. That translates to roughly 2-4 pounds per month during this period, or about 0.5-1 pound per week.
This is the phase where week-by-week results start to vary more. Some weeks you will lose two pounds. Other weeks the scale will not move. Some weeks you might even gain a pound due to water retention, hormonal fluctuations, or increased sodium intake. The trend line is what matters, not individual weigh-ins. Looking at monthly results rather than daily or weekly numbers provides a clearer picture.
Months 6-12: approaching the plateau
After six months, the rate of weight loss begins to decelerate for most people. This is not the medication failing. It is basic physics and biology working together. A smaller body requires fewer calories. Your metabolism has adjusted. The caloric deficit that produced rapid early losses now produces slower, steadier progress.
By month 12, cumulative weight loss on semaglutide averages 12-17% of starting body weight. The STEP 1 trial reported 14.9% mean weight loss at 68 weeks (approximately 16 months). Higher-dose studies have shown up to 17.4% at similar timepoints. The SELECT trial, which followed patients for up to four years, demonstrated that weight loss was maintained at -10.2% even at 208 weeks.
For a 200-pound starting weight, 14.9% means approximately 30 pounds lost by month 16. For a 250-pound starting weight, that is about 37 pounds. These are averages, remember. Some people lose significantly more. Understanding how fast you can realistically lose weight on semaglutide helps set appropriate expectations.
If your weight loss has slowed considerably or stopped, our guides on why you might not be losing weight on semaglutide and how to break through a semaglutide plateau cover the most common causes and solutions.
Month-by-month weight loss on tirzepatide
Tirzepatide is a dual GIP/GLP-1 receptor agonist, and the clinical data consistently shows it produces greater weight loss than semaglutide alone. The SURMOUNT trials provide the landmark data here.
Month 1: faster out of the gate
Tirzepatide starts at 2.5 mg weekly, which is already a more pharmacologically active starting dose compared to semaglutide 0.25 mg. As a result, many people experience more pronounced appetite suppression and weight loss from the very first month.
Expect 3-6% body weight loss in month one. For a 200-pound person, that is roughly 6-12 pounds. For a 250-pound person, 7-15 pounds. Some of this is water and glycogen, just as with semaglutide, but the proportion of fat loss tends to be higher from the start due to the dual-receptor mechanism.
If you want a deeper look at the early experience, our guide on what to expect after your first dose of tirzepatide covers the day-by-day and week-by-week experience. Understanding how long tirzepatide takes to suppress appetite also helps calibrate expectations during this initial adjustment period.
Months 2-3: aggressive loss
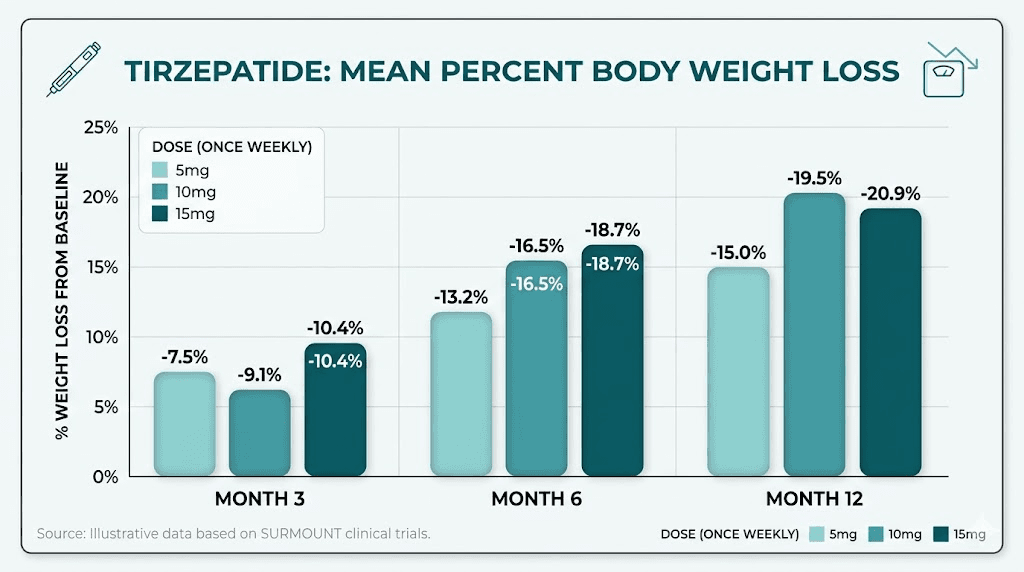
By week 12, participants in the SURMOUNT-1 trial had already lost an average of 6-8% of their body weight. That is on par with or slightly ahead of where semaglutide patients are at the same timepoint, even though tirzepatide dosing escalation is still ongoing.
At the end of month three, cumulative loss typically ranges from 6-10% of starting weight. For a 200-pound person, this means 12-20 pounds total. For a 250-pound person, 15-25 pounds. The dose is usually at 5 mg or 7.5 mg by this point, with further escalation planned. Checking the tirzepatide dosing for weight loss in units guide helps ensure you are tracking the right amounts.
Months 4-6: hitting stride
This is where tirzepatide really separates from other GLP-1 medications. Between months four and six, most patients reach the 10 mg or 15 mg target dose. Weight loss accelerates or maintains a strong pace.
Cumulative weight loss at six months averages 10-16% of starting body weight. For reference, the SURMOUNT-1 trial showed that patients on the 15 mg dose were already approaching 15-18% body weight loss by this timepoint. That is roughly 30-36 pounds for a 200-pound person, or 37-45 pounds for someone starting at 250.
The before and after results from tirzepatide at this stage can be dramatic. Clothing sizes change. Faces become visibly leaner. Energy levels often improve despite eating significantly less food. If you are curious about real world outcomes, our compilation of before and after tirzepatide weight loss results shows what the 6-month mark typically looks like.
Months 6-12+: the full picture
The SURMOUNT-1 trial ran for 72 weeks, approximately 17 months. At the end, the results broke down by dose. Patients on 5 mg lost an average of 16.0% of their body weight (about 35 pounds, or 16 kg). Patients on 10 mg lost 21.4% (about 49 pounds, or 22 kg). And patients on the highest dose of 15 mg lost 22.5% (about 52 pounds, or 24 kg).
To put that in monthly terms for the 15 mg group: 52 pounds over approximately 17 months equals roughly 3 pounds per month on average. But the actual trajectory is front-loaded. Monthly losses of 4-6 pounds in the first six months gradually taper to 1-2 pounds per month in the later stages.
The head-to-head SURMOUNT-5 trial provided even more compelling data. Tirzepatide patients lost an average of 20.2% of body weight compared to 13.7% for semaglutide patients over 72 weeks. That is a meaningful difference of about 17 pounds more with tirzepatide. Our detailed semaglutide vs. tirzepatide comparison breaks down all the differences beyond just weight loss numbers.
For a comprehensive view of the weight loss journey, the complete tirzepatide weight loss timeline maps out what to expect from week one through month 18 and beyond.
Month-by-month weight loss on liraglutide
Liraglutide (branded as Saxenda for weight management) was the first GLP-1 receptor agonist approved specifically for obesity treatment. It remains an option, though its results are notably lower than both semaglutide and tirzepatide.
The liraglutide trajectory
In the SCALE trial, liraglutide at 3.0 mg daily produced an average weight loss of approximately 8% of body weight over 56 weeks. In a direct head-to-head comparison with semaglutide, liraglutide produced only 6.4% weight loss compared to semaglutide at 15.8%.
Month by month, this translates to slower progress across the board. Month one typically sees 1-2% body weight loss. By month three, cumulative loss reaches 3-5%. At six months, 5-7%. And at 12 months, the average lands around 6-8%.
For a 200-pound person, liraglutide typically produces about 12-16 pounds of total weight loss over a year. That is roughly half of what semaglutide achieves and about one-third of what tirzepatide delivers.
There is one notable advantage to liraglutide, however. Research suggests it may be better at preserving lean muscle mass compared to semaglutide and tirzepatide. One meta-analysis found that liraglutide was the only GLP-1 receptor agonist to achieve significant weight reduction without significantly reducing lean mass. For people concerned about muscle loss, this is a meaningful consideration. Understanding the side effect differences between GLP-1 medications can help inform which option might be best suited to your situation.
Side-by-side comparison: all GLP-1 medications
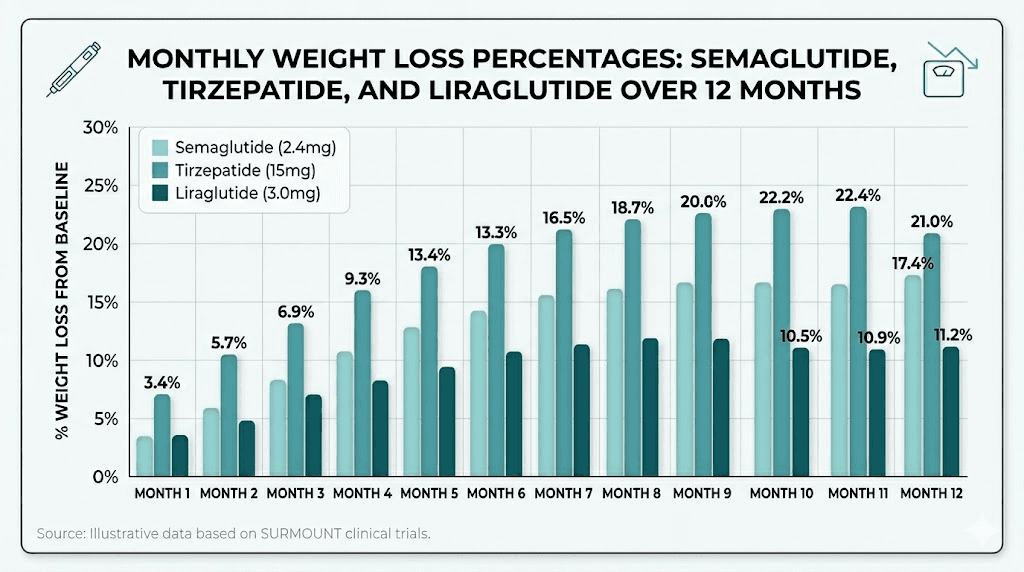
Numbers tell the clearest story when placed next to each other. The table below summarizes average weight loss by timepoint across all three major GLP-1 medications approved for weight management.
Timepoint | Semaglutide 2.4 mg | Tirzepatide 15 mg | Liraglutide 3.0 mg |
|---|---|---|---|
Month 1 | 2-4% (4-8 lbs) | 3-6% (6-12 lbs) | 1-2% (2-4 lbs) |
Month 3 | 5-8% (10-16 lbs) | 6-10% (12-20 lbs) | 3-5% (6-10 lbs) |
Month 6 | 8-12% (16-24 lbs) | 10-16% (20-32 lbs) | 5-7% (10-14 lbs) |
Month 12 | 12-17% (24-34 lbs) | 16-22% (32-44 lbs) | 6-8% (12-16 lbs) |
Month 16-18 | 14.9% (30 lbs) | 22.5% (52 lbs) | 8% (16 lbs) |
Based on a 200-pound starting weight. Individual results vary significantly based on dose, diet, exercise, and adherence.
The differences are stark. Tirzepatide consistently outperforms semaglutide by 5-8 percentage points, and both dramatically outperform liraglutide. If raw weight loss numbers are your primary goal, tirzepatide currently offers the most robust results. But medication choice involves more than just numbers. Comparing semaglutide, tirzepatide, and retatrutide provides a broader view of the evolving GLP-1 landscape.
You can also explore our tirzepatide vs. semaglutide dosage chart to understand how dosing protocols differ between the two most popular options.
Why your results might differ from the averages
Knowing the averages is useful. Understanding why you might land above or below them is critical. Here are the factors that most strongly influence monthly GLP-1 weight loss results.
Starting weight and BMI
People with higher starting weights tend to lose more absolute pounds but a similar percentage of body weight. Someone at 300 pounds losing 15% still loses 45 pounds. Someone at 180 pounds losing 15% loses 27 pounds. Percentage-based expectations are more useful than absolute pound targets.
The BMI requirements for GLP-1 prescriptions vary by medication and indication, so understanding where you fall on that spectrum affects both eligibility and expected outcomes.
Dose escalation speed
Both semaglutide and tirzepatide use gradual dose escalation protocols. If your provider moves you up slowly due to side effects, your early results will be lower. If you tolerate escalation well and reach the target dose quickly, your results will trend toward the higher end of the ranges.
Some patients stay at lower doses by choice or necessity. That is perfectly valid. Even the 5 mg dose of tirzepatide produced 16% weight loss in SURMOUNT-1. Understanding the optimal starting dose for compounded tirzepatide or checking a semaglutide dosage chart can help you track where you are in the escalation protocol.
Diet quality and protein intake
This is the single biggest modifiable factor. GLP-1 medications reduce appetite, but they do not control what you eat when you do eat. Two people on the same dose of semaglutide can have dramatically different results based on food choices.
Protein intake deserves special attention. Research recommends 1.2 to 1.6 grams of protein per kilogram of body weight for people losing weight on GLP-1 medications. For a 200-pound person (90 kg), that means 108-144 grams of protein daily. Hitting this target preserves muscle mass, keeps you satiated longer, and supports metabolism during weight loss.
Our guides on the best foods to eat on semaglutide and what to eat on tirzepatide break down specific food strategies. If you want a structured approach, the semaglutide diet plan and tirzepatide diet plan offer week-by-week meal guidance. You can also find practical GLP-1 breakfast ideas and GLP-1 recipes for weight loss that prioritize protein.
Exercise habits
Exercise has a smaller impact on the scale than most people expect, but a massive impact on body composition. Resistance training 2-3 times per week is the single most powerful intervention for preserving lean muscle mass during GLP-1-mediated weight loss.
People who combine GLP-1 medications with regular resistance training lose the same amount of total weight but retain significantly more muscle. The result is a better body composition, a higher resting metabolic rate, and a lower risk of weight regain after discontinuation.
Walking matters too. Aiming for 7,000-10,000 steps daily increases non-exercise activity thermogenesis (NEAT), which can add 200-400 calories of daily expenditure without structured exercise sessions. For those wondering if exercise is truly necessary, our guide on losing weight on semaglutide without exercise explores what happens when you rely on the medication alone.
Sleep and stress
Poor sleep disrupts hunger hormones, specifically ghrelin and leptin, even in people taking GLP-1 medications. Chronic stress elevates cortisol, which promotes visceral fat storage and can blunt the appetite-suppressing effects of GLP-1 receptor agonists.
Seven to nine hours of quality sleep per night and active stress management are not optional extras. They are foundational to maximizing your monthly weight loss results. If semaglutide is causing insomnia or tirzepatide is disrupting your sleep, addressing that issue should be a priority.
Genetics and metabolic factors
Some people are GLP-1 super-responders. Others respond modestly. Genetic variation in the GLP-1 receptor itself can influence how effectively you respond to medication. Thyroid function, insulin resistance severity, existing metabolic conditions, and even gut microbiome composition all play roles.
If you have Hashimoto thyroiditis or other autoimmune conditions, your response pattern may differ. These are not excuses for poor results but explanations for why your trajectory might not match the averages.
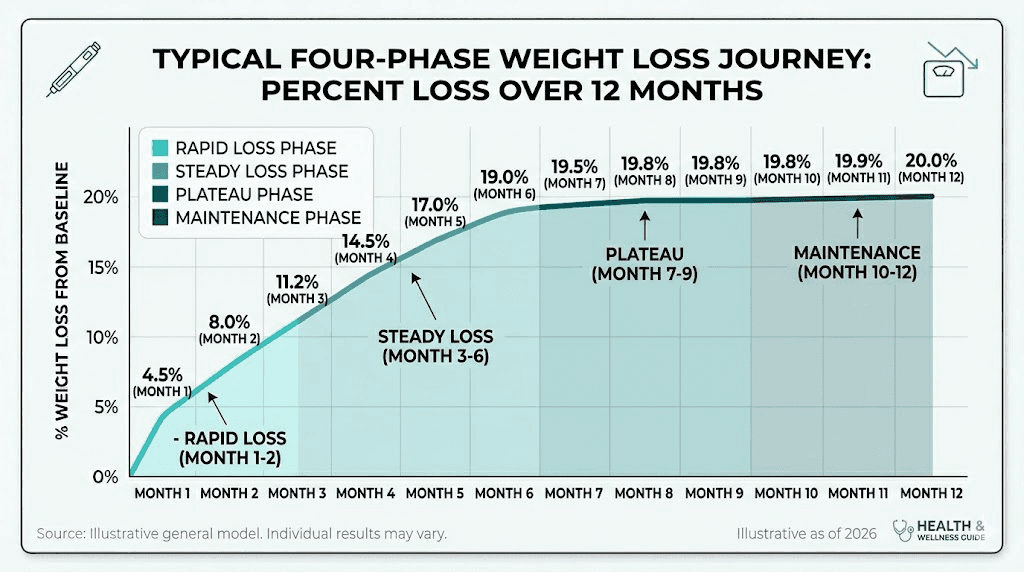
The weight loss curve explained
GLP-1 weight loss does not happen in a straight line. It follows a predictable curve with four distinct phases.
Phase 1: rapid initial loss (weeks 1-8)
The first two months produce the fastest weight loss. Part of this is genuine fat loss. Part of it is water weight and glycogen depletion as caloric intake drops. Part of it is the novelty effect, where the new appetite suppression is strongest because your brain has not yet adapted to the altered signaling.
During this phase, it is common to see 4-8 pounds of loss in some weeks. Do not expect this pace to continue. It is biologically unsustainable. If you are in this phase and wondering when the weight loss actually starts, know that most people see meaningful scale movement within the first 2-4 weeks.
Phase 2: steady loss (months 2-6)
After the initial rush, weight loss settles into a more predictable pattern. Expect 1-3 pounds per week on average, with significant week-to-week variation. This is the productive phase where most of your total weight loss accumulates.
The key during this phase is consistency. Take your medication on time. Prioritize protein. Keep moving. Do not let a slow week derail your commitment. Looking at results week by week can provide reassurance that variation is normal.
Phase 3: the plateau (months 6-12)
Nearly everyone hits a plateau. It typically arrives between months 6 and 12. The scale slows to a crawl. Some weeks it does not move at all. This is the most psychologically challenging phase, and it is also completely normal.
The plateau happens because your body has adapted. A smaller body burns fewer calories at rest. Your non-exercise activity often drops without you noticing. And your body ramps up appetite-promoting hormones in an attempt to defend its previous weight, a phenomenon researchers call metabolic adaptation.
If you are stuck, our guides on breaking through a semaglutide plateau and what to do when tirzepatide stops working offer actionable strategies. Sometimes the answer is a dose adjustment. Sometimes it is a dietary audit. Sometimes it is patience.
Phase 4: maintenance (month 12+)
After the active weight loss phase, you enter maintenance. This is not "done." It is a new phase where the goal shifts from losing to sustaining. GLP-1 medications help here by maintaining the appetite suppression that prevents regain.
The SELECT trial showed that patients on semaglutide maintained a 10.2% weight loss at 208 weeks (four years). That is encouraging. But discontinuing the medication typically leads to weight regain. Studies on tirzepatide discontinuation show that patients regain approximately two-thirds of their lost weight within a year of stopping.
Understanding how long to stay on semaglutide and how to maintain weight loss after tirzepatide is crucial for long-term planning. If you are considering discontinuation, how to properly wean off tirzepatide and the risks of semaglutide withdrawal symptoms are essential reading.
Body composition: fat loss vs. muscle loss
The number on the scale tells an incomplete story. What you lose matters as much as how much you lose.
The fat-to-muscle ratio
Research shows that approximately 70-75% of weight lost on GLP-1 medications comes from fat mass, while 25-30% comes from lean body mass (primarily muscle). This ratio is not unique to GLP-1 drugs. It is consistent with most forms of caloric restriction-driven weight loss.
However, the absolute amount of muscle loss can be significant when total weight loss is large. Someone who loses 50 pounds on tirzepatide might lose 12-15 pounds of lean mass along with 35-38 pounds of fat. That muscle loss affects metabolic rate, physical function, and long-term weight maintenance.
Some studies report even worse ratios, with lean mass loss comprising 40-60% of total weight in certain populations. Others show ratios as favorable as 85% fat to 15% lean mass. The difference? Exercise and protein intake.
Protecting your muscle mass
Three strategies have strong evidence for preserving lean mass during GLP-1-mediated weight loss.
Protein intake: Aim for 1.2 to 1.6 grams per kilogram of body weight daily. Spread this across meals, targeting 20-30 grams of high-quality protein per sitting. This creates the optimal stimulus for muscle protein synthesis. The best supplements to take with tirzepatide often include protein-focused options.
Resistance training: Even modest resistance training twice weekly shows significant benefits. You do not need to become a powerlifter. Bodyweight exercises, resistance bands, or light dumbbells are sufficient for most people. The stimulus of progressive overload tells your body to hold onto muscle even while in a caloric deficit.
Adequate calories: Eating too little is counterproductive. GLP-1 medications can suppress appetite so aggressively that some people eat dangerously few calories. Under 1,200 calories daily for women or 1,500 for men generally accelerates muscle loss without proportionally increasing fat loss.
Loose skin considerations
Rapid weight loss of 50+ pounds increases the risk of excess skin. The faster the loss, the less time skin has to adapt. Factors that influence skin elasticity include age, genetics, sun exposure history, hydration, and how long you carried the excess weight.
Preserving muscle mass helps fill out skin that would otherwise hang loose. Slow, steady weight loss (1-2 pounds per week) gives skin more time to contract. There is no guaranteed way to prevent loose skin with large weight losses, but these strategies improve outcomes.
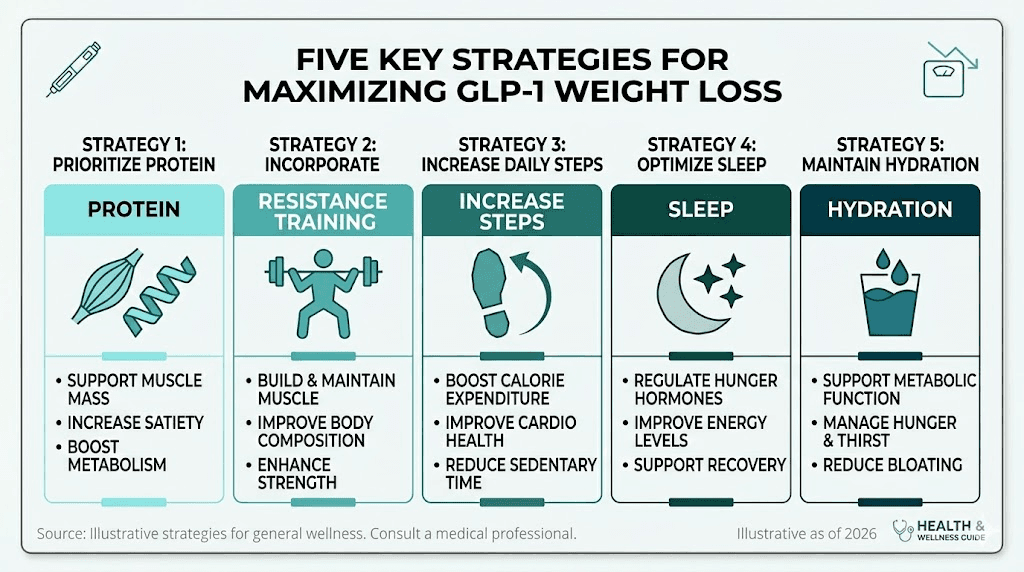
How to maximize your monthly weight loss on GLP-1
If you want to land on the higher end of the monthly weight loss ranges, these evidence-based strategies consistently produce better results.
Protein-first eating
At every meal, eat protein first. Before vegetables, before carbohydrates, before anything else. This ensures you hit your protein target even if appetite suppression limits total food intake. Good sources include chicken, fish, eggs, Greek yogurt, cottage cheese, and protein shakes.
Planning meals around protein is easier with structured guidance. Our list of foods to eat while on semaglutide and foods to avoid on tirzepatide can help you build a diet that supports maximum fat loss while preserving muscle.
Strategic supplementation
Several supplements support the weight loss process. Vitamin B12 is commonly added to compounded formulations because GLP-1 medications can reduce B12 absorption. Glycine supports collagen synthesis and may help with skin elasticity during weight loss. Probiotics can help manage the gastrointestinal side effects that sometimes limit adherence. And L-carnitine may support fat metabolism, though the evidence is less robust.
Timing and consistency
Take your injection at the same time each week. The best time to take semaglutide and the best time to take tirzepatide depend on your schedule and side effect pattern, but consistency matters more than the specific day or time.
If you are using compounded formulations, proper reconstitution of semaglutide or reconstitution of tirzepatide is essential for potency. Incorrect mixing can reduce effectiveness. Proper storage in the fridge and understanding refrigeration requirements protect your investment.
Injection technique
Proper injection technique ensures full absorption of the medication. Inject subcutaneously into the abdomen, thigh, or upper arm. Rotate injection sites to prevent lipodystrophy. Our guides on the best injection site for semaglutide, how to inject tirzepatide in the stomach, and where to inject GLP-1 cover technique in detail.
Movement beyond the gym
Structured exercise is important, but daily movement matters more than most people realize. Walking 7,000-10,000 steps per day, taking stairs, standing while working, and doing household chores all contribute to total daily energy expenditure.
This non-exercise activity thermogenesis (NEAT) can account for 200-500 calories per day. Over a month, that adds up to an additional 1-2 pounds of fat loss beyond what exercise alone provides.
Hydration
Dehydration is common on GLP-1 medications because reduced food intake also reduces water intake from food sources. Dehydration can cause dizziness, headaches, constipation, and fatigue. Aim for at least 64 ounces of water daily, more if you exercise or live in a hot climate.
When weight loss stalls: the GLP-1 plateau
Nearly every person on a GLP-1 medication experiences a plateau. Understanding why it happens and what to do about it is the difference between frustration and progress.
Why plateaus happen
Three mechanisms drive the GLP-1 plateau.
First, metabolic adaptation. As you lose weight, your basal metabolic rate drops. A body that once burned 2,400 calories at rest might now burn only 2,000. The caloric deficit that produced 2 pounds per week of loss now produces half a pound or less.
Second, behavioral drift. After months on medication, the initial dietary vigilance often relaxes. Portion sizes creep up. Snacking returns. High-calorie foods reappear. This is not failure. It is human nature. But it closes the caloric gap that drives weight loss.
Third, hormonal counter-regulation. The body fights weight loss. Ghrelin increases. Leptin decreases. Thyroid function may slow slightly. These hormonal shifts work to defend a weight setpoint that your body considers "normal" even if it is not healthy.
Breaking through the stall
Start with a food audit. Track every calorie for one week. Most people in a plateau are eating more than they think. Not from intentional overeating, but from unconscious portion increases and forgotten snacks.
Discuss dose adjustment with your provider. If you are on a sub-maximal dose, increasing may restart weight loss. If you have been on the same dose for months, your body may have partially adapted to its appetite-suppressing effects.
Increase protein to the upper end of the recommended range (1.6 g/kg body weight). Add or intensify resistance training. Prioritize sleep hygiene. Manage stress.
For specific strategies, our guides on what to do after four weeks with no weight loss, why you are not losing weight on tirzepatide, and why you are still hungry on tirzepatide address the most common plateau causes with actionable solutions.
If semaglutide has stopped working entirely, switching to tirzepatide might restart the process. Our guide on whether tirzepatide works when semaglutide does not explores this question in depth. And for those considering a medication change, the semaglutide to tirzepatide conversion chart provides dosing equivalency guidance.
Realistic expectations vs. social media
Social media is full of dramatic GLP-1 transformation stories. Someone posts a 100-pound weight loss in six months. Another shares a completely new body after 12 weeks. These stories are real but not representative.
Why transformation photos mislead
People who post transformation photos are, by definition, people with dramatic results. They are the outliers, the top 5-10% of responders. The other 90% of patients with solid but less photogenic results rarely post about their experience.
Additionally, photos can be manipulated through lighting, posture, clothing, and angles. A 20-pound weight loss can look like 40 pounds with the right photography. And many transformation photos span longer time periods than the captions suggest.
Our compilations of real semaglutide before and after results and GLP-1 before and after photos aim to show a range of outcomes, not just the most dramatic ones. For male-specific results, our men before and after tirzepatide guide provides relevant comparisons.
Non-scale victories that matter
Monthly weight loss numbers are important, but they are not everything. GLP-1 medications produce health improvements that often precede significant weight loss.
Blood sugar levels stabilize within weeks. Blood pressure drops. Inflammatory markers decrease. Joint pain improves as mechanical stress reduces. Sleep quality often improves. Energy levels increase as the medication affects energy regulation.
These benefits matter enormously for long-term health even if the scale is not moving as fast as you want.
When to talk to your provider
Not all weight loss trajectories are healthy, and not all slow results indicate a problem. Knowing when to seek guidance is important.
Losing too fast
Rapid weight loss, anything exceeding 3-4 pounds per week consistently, increases risks. Gallstone formation accelerates with rapid weight loss. Muscle loss becomes disproportionate. Nutritional deficiencies develop faster.
If you are losing more than 1-2% of your body weight per week after the initial month, discuss this with your provider. The dose may need reduction, or additional monitoring may be warranted. Issues like tirzepatide-related gallbladder concerns deserve attention if weight loss is very rapid.
Not losing enough
If you have been on a therapeutic dose for 12 or more weeks with less than 5% body weight loss, something may need adjustment. Options include dose escalation, medication switching, dietary intervention, or evaluation for underlying conditions that might limit response.
The question of how to qualify for semaglutide is one consideration, but if you are already on a GLP-1 and not responding, looking into switching between medications or exploring alternative dosing approaches like microdosing may be appropriate.
Side effects impacting adherence
Side effects that prevent you from eating enough or taking your medication consistently will reduce monthly weight loss. Common issues include constipation, bloating, sulfur burps, fatigue, and diarrhea. Most of these are manageable with dose adjustments, dietary modifications, or supportive treatments.
Some people experience less common side effects like anxiety, menstrual changes, hair loss, or feeling cold. Understanding what is normal and what requires medical attention helps you stay on track. Our guide on when semaglutide side effects typically appear can set your expectations.
Oral vs. injectable GLP-1 options
Not everyone wants to inject. Oral formulations of GLP-1 medications are available and under active development.
Oral semaglutide (Rybelsus) is currently available but produces less weight loss than the injectable form due to lower bioavailability. However, newer formulations and higher doses are in development. Our guides on oral semaglutide drops, oral tirzepatide, and how to take GLP-1 drops cover the current options and what is coming next.
For those using sublingual formulations, our sublingual semaglutide guide explains proper technique and expected results. There are also GLP-1 patches entering the market as an alternative delivery method.
The medication choice question
If your primary goal is maximum monthly weight loss, tirzepatide currently produces the best numbers. But medication selection involves more than just weight loss percentages.
Cost matters. Access matters. Side effect tolerance matters. Some people do better on semaglutide despite lower average weight loss numbers because they tolerate it better and maintain higher adherence.
Understanding whether GLP-1 is the same as Ozempic, comparing phentermine vs. semaglutide or phentermine vs. GLP-1, and exploring emerging options like retatrutide, survodutide, and mazdutide can help you make an informed decision. If you are considering combining medications, our guide on taking phentermine and semaglutide together or berberine and semaglutide together covers the safety considerations.
Special considerations
GLP-1 and alcohol
Alcohol contains empty calories and can reduce the effectiveness of your weight loss regimen. It also interacts with GLP-1 medications in ways that increase nausea and can cause rapid blood sugar drops. Our guides on drinking on semaglutide and drinking on tirzepatide explain the specific risks and how to minimize them if you choose to drink.
Travel and storage
Traveling with GLP-1 medications requires planning. Temperature control is critical because these are peptide-based medications that degrade with heat. Our guides on traveling with semaglutide and traveling with tirzepatide cover TSA regulations, cooling cases, and how to maintain your injection schedule across time zones.
Insurance and access
Coverage for GLP-1 medications varies widely. Some insurance plans cover them for obesity, others only for diabetes, and some do not cover them at all. Understanding Anthem GLP-1 coverage, Blue Cross Blue Shield GLP-1 coverage, and what to say when requesting GLP-1 options from your provider can improve your chances of getting coverage.
Compounded formulations offer an alternative pathway. Our compounded semaglutide guide explains the differences, costs, and considerations for compounded versions.
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members get access to detailed comparison tools, dosing calculators like the semaglutide dosage calculator, and expert-reviewed guidance that accounts for individual factors most resources ignore.
Frequently asked questions
How much weight will I lose in the first month on a GLP-1?
On semaglutide, expect 2-4% of your body weight in month one (4-8 pounds for a 200-pound person). On tirzepatide, expect 3-6% (6-12 pounds). On liraglutide, expect 1-2% (2-4 pounds). These numbers reflect the dose escalation phase, when you are on sub-therapeutic doses. Results accelerate in months 2-3 as doses increase. Our guide on semaglutide one month results provides a more detailed first-month breakdown.
Is tirzepatide faster than semaglutide for weight loss?
Yes. In the head-to-head SURMOUNT-5 trial, tirzepatide produced 20.2% weight loss compared to 13.7% for semaglutide over 72 weeks. Tirzepatide also tends to produce faster initial weight loss due to its dual GIP/GLP-1 receptor mechanism. However, both medications are effective, and choosing between them involves more factors than speed alone.
Why did I stop losing weight on GLP-1 after 3 months?
A slowdown at 3 months is common and usually reflects one of three things: metabolic adaptation as your body adjusts to a lower weight, the end of initial water weight loss, or behavioral changes like gradually eating more. Review your diet, ensure adequate protein, and discuss dose adjustment with your provider. Our semaglutide plateau guide covers strategies for breaking through a stall.
Can I lose weight on a low dose GLP-1?
Yes. Even the lowest therapeutic doses produce meaningful weight loss. Semaglutide at 1.0 mg produces approximately 10% weight loss, and tirzepatide at 5 mg produced 16% in the SURMOUNT-1 trial. Lower doses also have fewer side effects. Some people practice microdosing tirzepatide for this reason.
How much weight loss is too fast on GLP-1?
Losing more than 1-2% of your body weight per week consistently (after the first month) warrants a conversation with your provider. Very rapid weight loss increases the risk of gallstones, excessive muscle loss, nutritional deficiencies, and loose skin. If you are losing faster than expected, it may indicate that you are not eating enough, which creates its own health risks.
Do you gain weight back after stopping GLP-1?
Studies show that most people regain approximately two-thirds of their lost weight within a year of discontinuing GLP-1 medications. This is why many providers recommend long-term or indefinite treatment. If you are planning to stop, gradual tapering combined with established exercise and dietary habits offers the best chance of maintaining results. Our guides on stopping semaglutide cold turkey and weaning off tirzepatide explain the process and risks.
Does exercise make a difference in GLP-1 weight loss?
Exercise has a modest impact on the total number of pounds lost, but a massive impact on body composition. People who exercise regularly while on GLP-1 medications lose more fat and retain more muscle. Resistance training is particularly important. It also helps maintain metabolic rate and reduces the risk of weight regain after medication discontinuation.
Why do women lose more weight on GLP-1 than men?
A Johns Hopkins analysis found that women lost 10.88% of body weight compared to 6.78% for men across nearly 20,000 patients. The reasons are not fully understood but likely relate to hormonal differences, body composition (women carry proportionally more fat mass), and potentially different behavioral responses to appetite suppression.
External resources
Real-world weight loss effectiveness of GLP-1 agonists (PMC/NIH)
GLP-1 Agonists: What They Are, How They Work (Cleveland Clinic)
Long-term weight loss effects of semaglutide in obesity (Nature Medicine)
In case I do not see you, good afternoon, good evening, and good night. May your doses stay consistent, your protein stay high, and your progress stay steady.