Feb 18, 2026

What if you have been stressing about tirzepatide timing for no reason at all? That thought might sound reckless. It is not. The weekly injection schedule printed on your prescription label looks rigid, almost sacred, but the pharmacology behind tirzepatide tells a more flexible story than most people realize. Yes, you can take tirzepatide a day early. The medication allows a surprisingly forgiving window, provided you respect one critical threshold that separates safe early dosing from a nausea-inducing mistake.
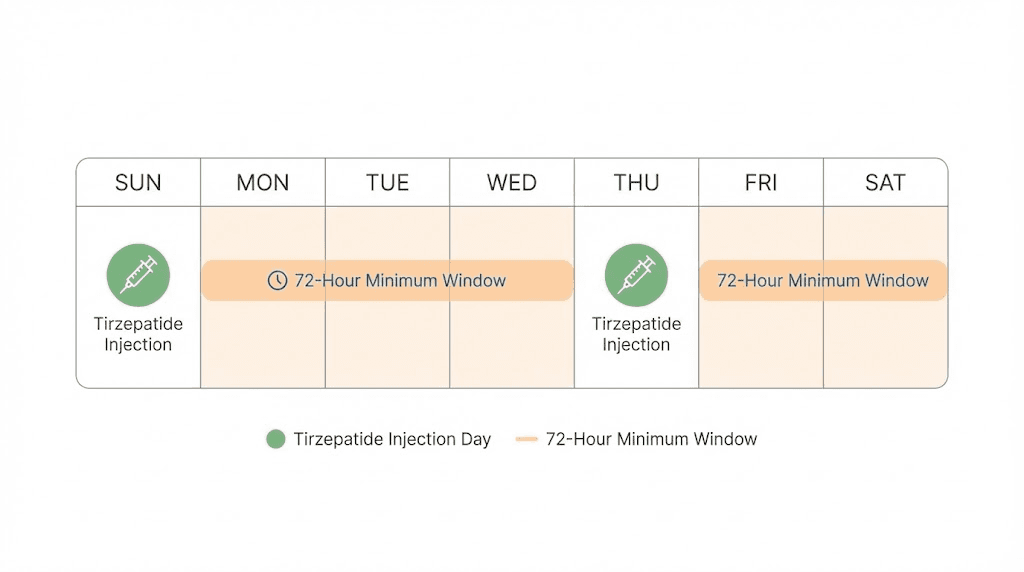
Here is the short version. At least 72 hours must pass between injections. That is the floor. Three full days. Anything less than that, and you are stacking active drug on top of active drug in a way your body was never meant to handle. But once you clear that 72-hour mark, you have genuine flexibility. You can shift your injection day forward. You can adjust for travel. You can accommodate a busy schedule without compromising your results or your safety.
The confusion around dose timing is understandable. Medical information online ranges from overly cautious to dangerously casual, and tirzepatide sits at the center of enormous public interest right now. People want to get this right. They want to know exactly what happens when life disrupts their weekly routine, when a flight lands on injection day, when they simply forget and wake up a day late. This guide answers every one of those questions with the pharmacological evidence behind each answer. Whether you are on your first tirzepatide dose or months into a protocol, understanding timing flexibility gives you something no rigid schedule can: confidence. And SeekPeptides has built an entire library of dosing resources to help you develop exactly that.
The short answer: yes, with one non-negotiable rule
You can take tirzepatide a day early. That is the direct answer.
But it comes with a condition that you cannot ignore. A minimum of 72 hours, three full days, must separate your current injection from your previous one. This is not a suggestion. It is not a conservative recommendation from overly cautious prescribers. It is a pharmacological boundary based on how tirzepatide behaves inside your body, how it accumulates, and how your gastrointestinal system responds to overlapping doses.
Think about what "a day early" actually means in practice. If you normally inject on Saturday mornings at 9 AM, taking your dose on Friday morning at 9 AM puts exactly 144 hours between your Thursday-of-last-week injection and your Friday injection. That is well above the 72-hour minimum. Perfectly safe. No issue at all. But if you normally inject on Tuesdays and you took your last dose on Sunday afternoon, injecting on Monday morning would only give you about 40 hours of separation. That is a problem.
The math matters more than the calendar. Do not think in terms of "days" as abstract concepts. Count the actual hours since your last injection. If that number is 72 or higher, you are cleared. If it is under 72, wait. It really is that simple, and understanding the tirzepatide dose chart principles makes the decision even clearer.
Most people who ask "can I take tirzepatide a day early" are already well within the safe zone. A day early on a weekly schedule means roughly 144 hours between doses instead of 168. That 24-hour difference is pharmacologically insignificant. Your body will not notice. Your results will not change. Your side effect profile will remain exactly what it would have been on your normal schedule.
Where people get into trouble is when "a day early" compounds over multiple weeks. Taking it a day early every single week gradually shifts your schedule forward. After seven weeks, you would have effectively eliminated an entire dose interval. That scenario is unlikely for most people, but it is worth understanding. The solution is straightforward: after moving your dose early, simply establish the new day as your regular injection day and maintain that 7-day rhythm going forward.
Why the 72-hour rule exists
Numbers without context are just numbers. Understanding why 72 hours matters requires a brief look at what tirzepatide does inside your body after injection, and that story starts with a concept called half-life.
Tirzepatide half-life and what it means for timing
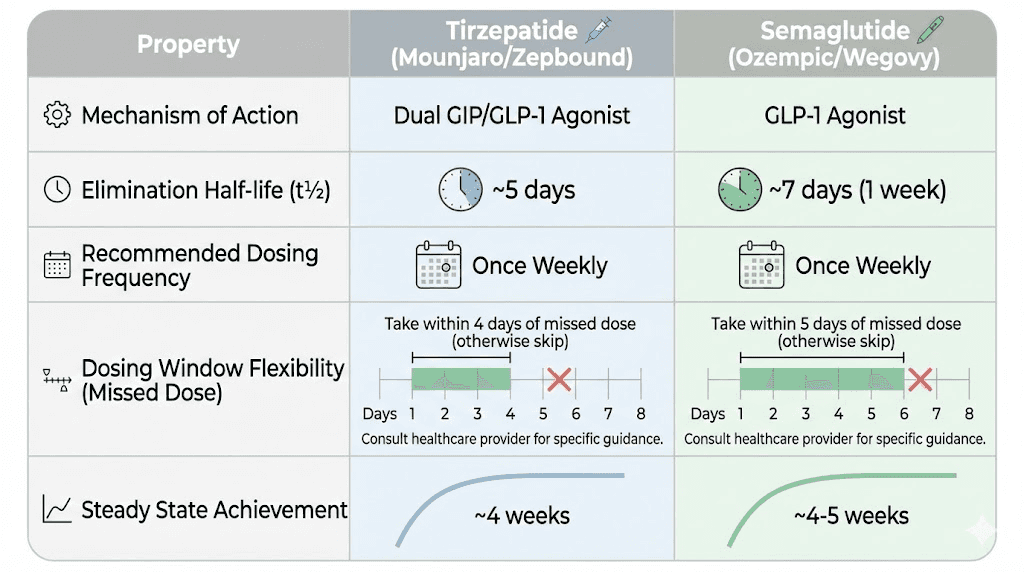
Tirzepatide has an elimination half-life of approximately 5 days, or about 120 hours. That is remarkably long compared to many medications. It means that 5 days after your injection, roughly half of the active drug remains circulating in your system. After 10 days, about a quarter remains. After 15 days, an eighth. The drug does not disappear when your next injection day arrives. Far from it.
This extended half-life is actually the reason tirzepatide works as a weekly injection in the first place. If the drug cleared your system in 24 hours, you would need daily injections. The long half-life creates sustained GLP-1 and GIP receptor activation throughout the entire week, maintaining appetite suppression, glucose control, and the metabolic benefits that drive tirzepatide before and after results people talk about.
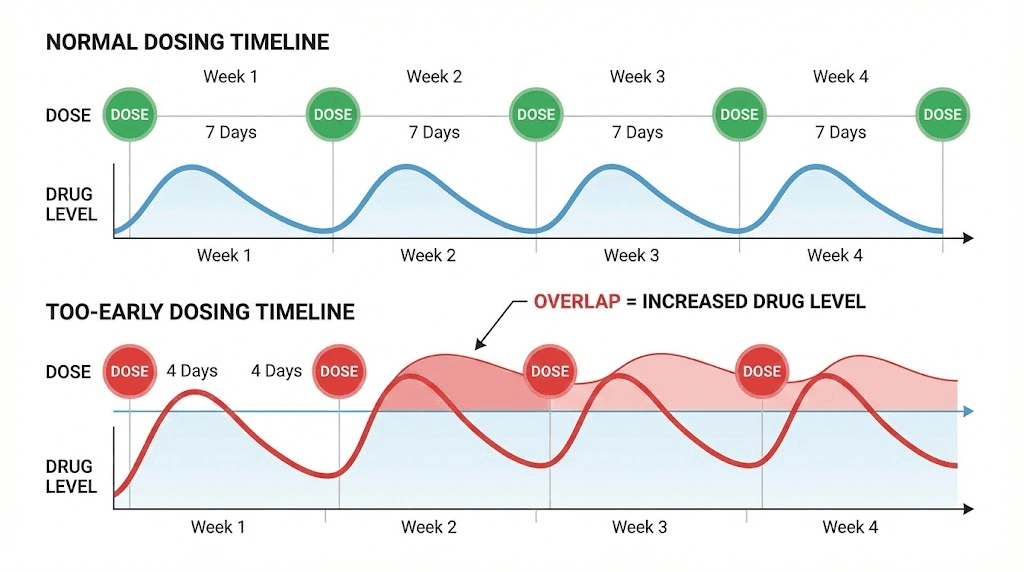
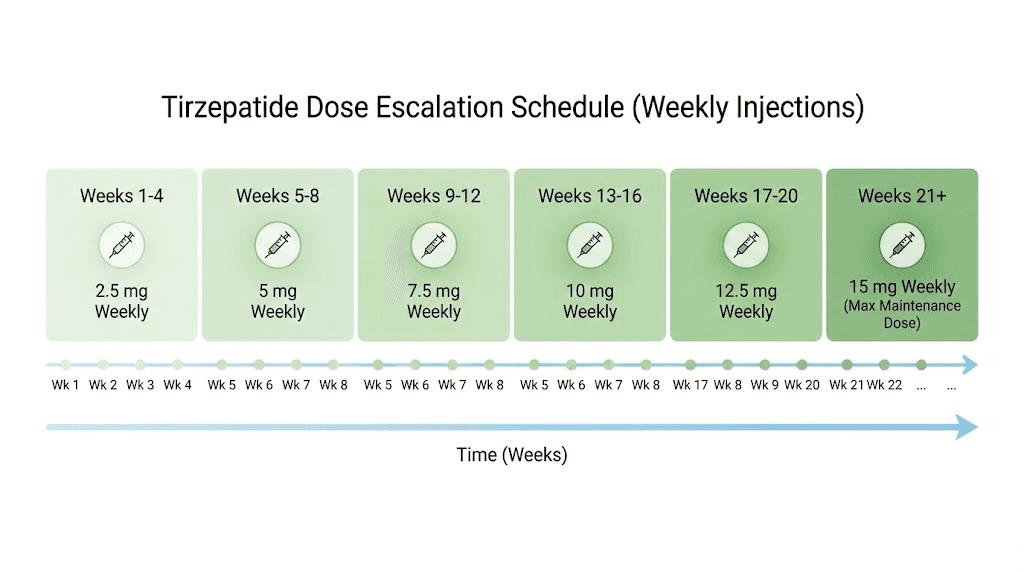
But this same long half-life creates an accumulation effect. When you inject your next dose, the previous dose has not fully cleared. Each weekly injection adds new drug on top of residual drug. After about four weeks of consistent weekly dosing, your body reaches what pharmacologists call "steady state," the point where the amount of drug entering your system each week equals the amount leaving. At steady state, tirzepatide shows approximately 1.6-fold accumulation. That means the total active drug in your body at any given time is about 60% higher than what a single dose alone would produce.
Now imagine injecting early, before that residual drug has had time to decline to its expected level. You are adding a full new dose on top of a higher-than-expected residual amount. The result is a temporary spike in active drug levels that your body was not prepared to handle. This is exactly why people who inject too early experience amplified side effects, particularly nausea, which is already the most common side effect of GLP-1 receptor agonists.
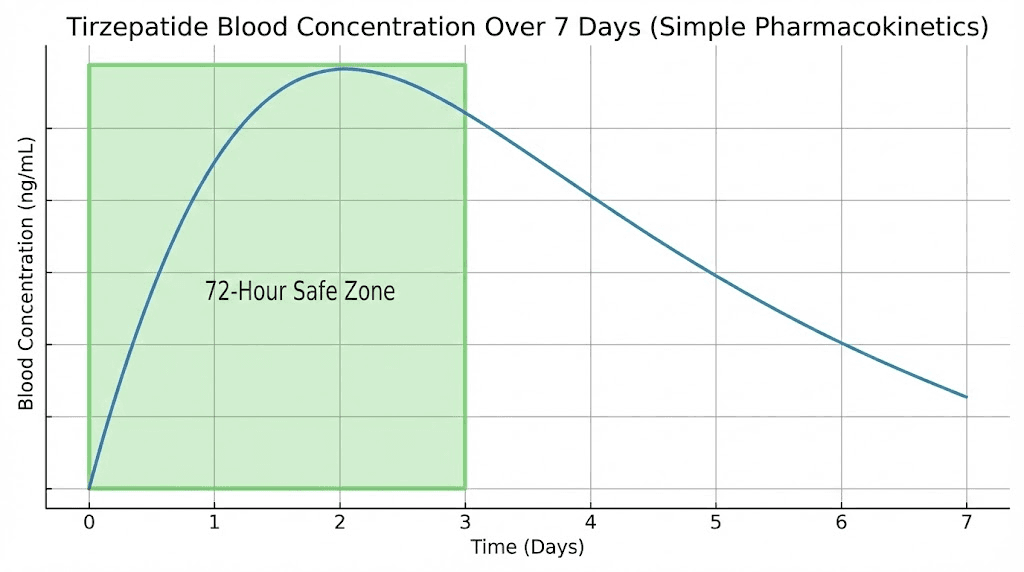
Peak concentration and the absorption window
After subcutaneous injection, tirzepatide does not hit peak blood levels immediately. The drug reaches its maximum concentration, known as Cmax, somewhere between 8 and 72 hours after injection. That is a wide window, and it varies based on injection site, individual metabolism, body composition, and dose amount. For most people, peak levels occur around 24 to 48 hours post-injection.
This absorption pattern has a direct implication for early dosing. If you inject your new dose while still within the peak concentration window of your previous dose, you are essentially doubling down on the highest drug levels your body experiences. That 8-to-72-hour Cmax window is precisely why the 72-hour minimum exists. It ensures that your previous dose has at least cleared its peak absorption phase before you introduce new drug.
The compounded tirzepatide dosage calculator can help you understand your specific dose in milligrams and units, which becomes relevant when calculating how much active drug is actually circulating at any given point in your weekly cycle. Higher doses mean higher peak levels, which means the consequences of injecting too early become more pronounced as you titrate up through the tirzepatide compound dosage chart.
How steady state changes the equation
The first few weeks of tirzepatide use are different from weeks five, ten, or twenty. During the initial loading phase, your body is still building up to steady state concentrations. Each dose adds to the accumulating total. Side effects tend to be most intense during this period, particularly during the first weeks of tirzepatide treatment and during each dose escalation.
Once you reach steady state, roughly four to five weeks at a consistent dose, your body has adapted. The 1.6-fold accumulation is expected. Your GI tract has adjusted. The receptors have downregulated slightly to accommodate the sustained stimulation. This is when most people report that initial side effects like nausea fade and the appetite-suppressing effects feel more natural and less forced.
Injecting early during the pre-steady-state phase is riskier than injecting early at steady state. During accumulation, your body is still adapting to rising drug levels. Adding an early dose accelerates that accumulation beyond the planned escalation rate. This is particularly relevant for people in their first month of treatment or within the first two weeks after a dose increase. If you are in either of those situations, adhere more strictly to the 7-day schedule and avoid early dosing unless absolutely necessary.
Step-by-step guide to taking tirzepatide early
Theory is useful. Practical guidance is better. Here is exactly how to handle the most common early-dosing scenarios, with the pharmacology translated into simple decisions.
Scenario 1: you want to take it one day early this week
This is the most common situation. Something about next week, travel, a medical appointment, a social event, makes your normal injection day inconvenient. You want to shift one day forward.
The process is simple. Count the hours since your last injection. If your last dose was at least 72 hours ago, inject now. If you normally inject on Sundays and want to inject on Saturday instead, that is approximately 144 hours between doses. Completely safe. No adjustment needed to your actual dose amount. You are simply compressing one interval by 24 hours, and the pharmacokinetics accommodate that compression without any meaningful change in drug levels.
After injecting early, you have a choice. You can either make this new day your permanent injection day, or you can return to your original day the following week. If you return to your original day, your next interval will be 8 days instead of 7. That longer gap is also completely fine. Tirzepatide remains active and effective across an 8-day interval thanks to its long half-life. Some people report slightly reduced appetite suppression on day 7 or 8, but this is generally minimal, especially at higher doses where you can reference the standard unit conversions to confirm your levels.
Scenario 2: you want to take it two days early
Two days early on a weekly schedule means a 5-day interval, or approximately 120 hours between doses. This is still above the 72-hour minimum, so it is technically safe. However, two days early is where you start to notice differences.
At 120 hours post-injection, more residual drug remains in your system compared to the usual 168-hour point. Your new dose is being added on top of a slightly higher baseline. For most people on stable doses, this produces no noticeable difference. But if you are sensitive to side effects, currently in the dose-escalation phase, or already experiencing tirzepatide fatigue or GI symptoms, the extra residual drug could amplify those effects temporarily.
If you need to inject two days early, consider these adjustments. Inject in the evening rather than the morning, as sleeping through the initial peak absorption can reduce perceived nausea. Eat a light, bland meal about an hour before injection. Stay well hydrated. And do not combine the early injection with any other changes to your protocol, like switching injection sites or introducing new supplements.
Scenario 3: repeated early dosing over multiple weeks
This is the scenario that actually requires caution. Taking tirzepatide one day early for a single week is a non-event. Taking it one day early every week for six weeks means you have compressed six 7-day cycles into six 6-day cycles. Over that period, you have administered six doses in 36 days instead of 42 days. That is one extra dose worth of drug accumulation spread across the period.
The practical impact depends on where you are in your titration. At the starting dose of 2.5 mg, the extra accumulation is minimal. At higher doses like 10 mg or 15 mg, the cumulative effect becomes more significant. If you find yourself consistently wanting to inject early, the better approach is to officially change your injection day and maintain a consistent 7-day rhythm from that new starting point.
Understanding your exact dosing in both milligrams and units helps here. Resources like the 2.5 mg unit conversion guide and the 5 mg unit conversion guide ensure you always know exactly how much medication you are administering, which becomes critical when evaluating whether timing shifts are clinically meaningful.
What happens if you take tirzepatide too early
Rules exist because breaking them has consequences. The 72-hour minimum is not arbitrary. Here is what actually happens in your body when you inject tirzepatide before sufficient time has passed since your last dose.
Amplified gastrointestinal side effects
Nausea is the most commonly reported side effect of tirzepatide, affecting roughly 40% to 70% of users at some point during treatment. Most nausea occurs during dose initiation and dose escalation, and it is caused by the slowed gastric emptying that GLP-1 receptor agonists produce. Your stomach empties more slowly. Food sits longer. The signals to your brain trigger a nausea response.
When you inject too early, you amplify this effect. More active drug means more aggressive gastric slowing. Food that would normally pass through your stomach in 3 to 4 hours might sit for 6 to 8 hours. The nausea can be intense, sometimes progressing to vomiting. This is the single most common consequence of premature dosing, and it is the one that people remember. It often turns a manageable side effect into a miserable 48-hour experience.
Beyond nausea, early dosing can worsen other GI symptoms. Constipation may intensify as gastric motility slows further. Some people experience increased bloating, abdominal discomfort, or acid reflux. These effects are temporary, resolving as the excess drug clears, but they can be genuinely uncomfortable. For people already managing GI side effects with careful dietary adjustments, early dosing can undo weeks of careful management.
Disrupted appetite suppression patterns
This one is counterintuitive. More drug should mean more appetite suppression, right? Not exactly. When drug levels spike above the expected range, the body sometimes responds with a compensatory rebound. Some people who inject too early report a period of intense appetite suppression followed by a stronger-than-usual return of hunger once the excess drug begins clearing. This creates an inconsistent pattern that makes meal planning difficult and can actually undermine the steady, predictable appetite control that makes tirzepatide effective for weight loss.
The goal is consistency. Steady drug levels produce steady appetite suppression. Steady appetite suppression produces predictable eating patterns. Predictable eating patterns produce sustainable weight loss. Breaking that chain by introducing irregular timing disrupts the entire cascade, even if the total drug amount over a month stays roughly the same.
Impact on dose escalation assessment
Here is a consequence people rarely consider. Your prescriber uses your response at each dose level to determine when and whether to escalate. If you are injecting at irregular intervals, your reported experience does not accurately reflect the dose you are supposed to be on. You might report breakthrough hunger that prompts a premature dose increase, when the real problem was inconsistent timing causing uneven drug levels.
Similarly, if early dosing causes amplified side effects, you might report that a dose is poorly tolerated when it would have been perfectly fine on a proper 7-day schedule. This could delay your escalation unnecessarily, extending the time it takes to reach your target dose and slowing your overall progress. Many people who feel tirzepatide is not working anymore are actually dealing with timing inconsistencies rather than true tolerance.
Changing your injection day permanently
Sometimes the issue is not a one-time schedule conflict. Sometimes your injection day just does not work. Maybe you started on a Tuesday but realized weekends are better. Maybe your work schedule changed. Maybe you simply want a different day. Good news: you can absolutely change your injection day permanently. The process is straightforward and safe as long as you follow one simple protocol.
How to shift your injection day forward
Shifting forward means injecting earlier than your current schedule. If you currently inject on Thursdays and want to switch to Mondays, your next interval would be 4 days instead of 7. Check the math: 4 days equals 96 hours, which clears the 72-hour minimum. So on your next dose, simply inject on Monday instead of Thursday. That Monday becomes your new permanent injection day. Maintain 7-day intervals from that new day going forward.
The key is making the shift in one move rather than gradually. Do not inch forward one day per week. That creates weeks of irregular intervals. Instead, make the jump all at once. One shortened interval followed by consistent weekly dosing is far better than four or five slightly shortened intervals spread over a month.
How to shift your injection day backward
Shifting backward means injecting later than your current schedule. If you currently inject on Mondays and want to switch to Fridays, your next interval would be 11 days instead of 7. This is inherently safer from a drug-accumulation standpoint since you are extending the gap, not compressing it. The concern here is different: will the extended interval cause breakthrough symptoms?
For most people on established doses, an 11-day gap between two specific injections produces minimal symptoms. You might notice slightly reduced appetite suppression on days 9 through 11, and some people report mild mood fluctuations as drug levels dip below their usual trough. But these effects are temporary and resolve immediately with your next injection on the new schedule. The long 120-hour half-life ensures that meaningful drug levels persist well beyond the standard 7-day interval.
Once you inject on your new day, maintain that 7-day rhythm. Your body will re-establish steady state within three to four weeks at the new schedule, and any symptoms from the transition will resolve during that period.
Documenting the change
Keep a record. Note your old injection day, the date of the transitional injection, and your new injection day. Inform your prescriber at your next appointment. This documentation helps ensure that any side effects or efficacy changes you report can be properly evaluated in the context of the schedule adjustment rather than misattributed to the medication itself.
The peptide calculator on SeekPeptides can help you track your dosing schedule and understand the pharmacokinetic implications of any timing changes. Precise tracking eliminates guesswork and gives you confidence that your protocol remains optimized.
Missed dose protocol: what to do when you forget
Forgetting a dose happens. Life gets busy. Routines break. The alarm does not go off. You remember at 11 PM when you are already in bed. What matters is not that you missed it but how you handle the recovery. And the protocol for missed tirzepatide doses is clearly defined.
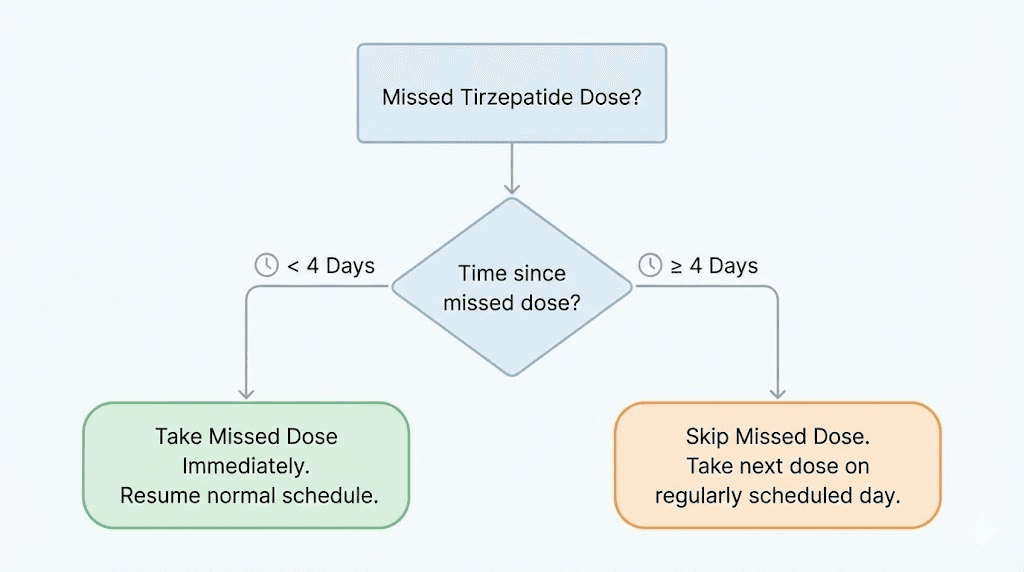
The 4-day window rule
If you miss your scheduled injection day, you have a 4-day window, 96 hours, to take the missed dose. During this window, simply inject as soon as you remember. Then resume your regular schedule from there. If your regular day is Wednesday and you remember on Saturday (3 days late), inject on Saturday and return to your usual Wednesday the following week. That gives you a 4-day interval followed by a 7-day interval. Both are within safe parameters.
If more than 4 days (96 hours) have passed since your missed dose was due, skip it entirely. Do not double up. Do not try to compensate. Simply wait until your next regularly scheduled injection day and take your normal dose. You will have gone roughly 14 days between injections, and while this is longer than ideal, the half-life characteristics of tirzepatide mean that some active drug remains in your system even at the 14-day mark. You will not be starting from zero.
What happens during a missed dose
The experience of a missed dose depends on how long you have been on tirzepatide and what dose you are taking. At lower doses early in treatment, a missed dose may produce minimal noticeable effects. At higher doses after months of treatment, you may notice a gradual return of appetite over days 5 through 10, along with potential blood sugar fluctuations if you are using tirzepatide for glycemic management.
Many people wonder how long tirzepatide takes to suppress appetite after a dose. When resuming after a missed dose, appetite suppression typically returns within 24 to 48 hours of the catch-up injection. The full steady-state level takes about three to four weeks to re-establish after any significant disruption, but the functional effects of each individual dose begin much sooner.
Do not panic if you miss a dose. One missed injection in the context of a months-long protocol is statistically insignificant. It will not derail your progress. It will not reset your tolerance. It will not undo weeks of metabolic adaptation. The key is getting back on schedule as quickly as possible within the allowed window.
When repeated missed doses require intervention
Missing one dose is nothing. Missing two consecutive doses, that changes things. If you miss two or more doses in a row, creating a gap of 21 or more days, contact your prescriber before resuming. Extended gaps can affect your tolerance, and restarting at your previous dose after a prolonged break may produce more intense side effects than expected. Your prescriber might recommend stepping down to a lower dose temporarily and re-titrating up, which is the same approach used during initial treatment. Understanding the full tirzepatide dosage structure in units helps when navigating these conversations with your healthcare provider.
Travel and schedule adjustments
Travel is the most common real-world reason people need to adjust tirzepatide timing. Flights, time zones, hotel refrigerators, security checkpoints, and unfamiliar routines all conspire to disrupt a carefully maintained weekly schedule. But travel does not need to derail your protocol. With some planning, you can maintain effective dosing across any itinerary.
Crossing time zones
When you cross time zones, the clock changes but your biology does not. If you normally inject at 8 AM Eastern time on Wednesdays and you fly to London (5 hours ahead), your body still expects the injection 168 hours after the last one. The local clock might say 1 PM, but your circadian drug metabolism does not care about Greenwich Mean Time.
The practical approach is simple. Count hours from your last injection, not calendar days. Use a timer on your phone if needed. As long as 72 or more hours have passed, you can inject at whatever local time is convenient. The exact hour of injection within a given day does not meaningfully affect tirzepatide pharmacokinetics. Morning, afternoon, evening, it does not matter. What matters is the interval between doses.
For extended international travel, some people find it helpful to shift their injection day before departure so it falls at a convenient point in the trip. Use the day-shifting protocol described above. Inject a day early before your trip, establish that new day as your temporary schedule, and shift back after you return if desired. This proactive approach beats trying to manage injections during transit or on your first jet-lagged day in a new time zone. You can find more detailed guidance on traveling with GLP-1 medications that applies to tirzepatide as well.
Keeping tirzepatide cold during travel
Dose timing matters, but so does medication integrity. Tirzepatide, whether pharmaceutical or compounded, requires proper temperature management. Understanding tirzepatide refrigeration requirements is critical for any travel scenario. The medication can tolerate brief periods at room temperature, but extended heat exposure degrades the active compound.
For short trips, a medical-grade cooling case with gel packs keeps your tirzepatide within acceptable temperature ranges for 24 to 48 hours. For longer trips, confirm that your hotel room has a refrigerator, and store the medication there upon arrival. Never leave tirzepatide in a car, in checked luggage exposed to cargo hold temperature extremes, or in direct sunlight. The question of how long compounded tirzepatide can be out of the fridge depends on the specific formulation and ambient temperature, but erring on the side of caution protects your investment and your results.
If you are worried about tirzepatide expiration during an extended trip, check the expiration date before departure and consider whether you will need a refill while traveling. Planning ahead prevents the stressful scenario of running out of medication far from your pharmacy.
Airport security and injection supplies
Traveling with injectable medications through airport security requires minimal preparation but causes maximum anxiety for first-timers. Tirzepatide pens and syringes are permitted through TSA and most international security checkpoints. Carry your medication in your carry-on bag, never in checked luggage. Bring a copy of your prescription or pharmacy label. Declare the medication if asked. In over a decade of GLP-1 medications being commonly prescribed, security issues with injectable medications are vanishingly rare.
Keep your supplies organized. Medication, syringes (if using compounded formulations), alcohol swabs, and a sharps container for used needles should all be together in a clear bag for easy screening. Understanding proper injection techniques is particularly important when traveling, as unfamiliar environments can make the process feel more complicated than it needs to be.
Best time of day to inject tirzepatide
A question that generates surprisingly passionate debate. Morning or evening? Before meals or after? With coffee or without? The research is clear, and the answer may disappoint people looking for a definitive winner.
The evidence on timing
Tirzepatide can be injected at any time of day. Clinical trials did not mandate a specific time, and the pharmacokinetic data shows no meaningful difference in absorption, peak levels, or efficacy based on injection timing. Morning injectors and evening injectors achieve the same blood concentrations, the same appetite suppression, and the same weight loss outcomes when all other factors are equal.
However. That word carries weight.
Individual experience often differs from population-level data. Many people report that injection timing affects their personal side effect experience, particularly nausea. The mechanism is not fully understood, but it likely relates to the interaction between tirzepatide absorption, meal timing, and the body circadian regulation of GI motility. Studies on the best time of day for GLP-1 injections suggest similar patterns across the medication class.
The case for morning injections
People who inject in the morning report several advantages. First, it establishes a consistent routine attached to an existing morning habit. You wake up, you inject, you start your day. The ritual becomes automatic. Second, morning injection means the initial absorption phase, the period most likely to produce nausea, occurs while you are active and upright. Being vertical and moving around seems to help some people tolerate the initial GI effects better than lying down.
Third, morning injection aligns the peak appetite-suppression window with the hardest part of many people diets: afternoon and evening snacking. If you inject at 7 AM, peak drug levels arrive between 15 and 55 hours later, covering you through the afternoon snack window and into the next evening. Many people following a tirzepatide diet plan find that morning dosing gives them the strongest willpower during the hours they need it most.
The case for evening injections
Evening injectors have their own arguments. The primary one is practical: if tirzepatide makes you nauseous, you can sleep through the worst of it. Injecting at 8 or 9 PM means the initial absorption peak occurs while you are in bed. You wake up the next morning past the nausea window, and the rest of the week proceeds normally. For people who experienced significant nausea during dose escalation, this strategy has genuine merit.
Additionally, some people report that evening injection reduces next-day fatigue. The theory, unproven but plausible, is that the body initial metabolic response to the injection benefits from the restorative processes that occur during sleep. By morning, the drug has been partially processed, and the most energy-intensive phase of absorption has passed.
With or without food
Tirzepatide can be injected with or without food. Clinical trials did not specify a relationship to meals, and absorption occurs through subcutaneous tissue, not the GI tract, so food in your stomach has no direct effect on how the drug enters your bloodstream. However, many prescribers recommend having a small, bland meal about an hour before injection, particularly during early treatment or dose escalation. The reasoning is that a partially full stomach may buffer some of the initial GI effects. Knowing what to eat on tirzepatide and what to avoid around injection time can make a meaningful difference in your comfort during the first 24 to 48 hours post-dose.
How dose timing affects weight loss results
Let us address the question people really want answered. Does taking tirzepatide a day early, a day late, or at a different time of day affect your weight loss? The answer is nuanced, but the bottom line is reassuring.
Consistency matters more than precision
Weight loss on tirzepatide is driven by sustained caloric deficit, which is driven by consistent appetite suppression, which is driven by steady drug levels. The key word is "steady." A single early or late injection does not meaningfully disrupt steady-state drug levels. The half-life is too long. The accumulation factor is too stabilizing. One 144-hour interval instead of one 168-hour interval simply does not create a pharmacologically significant dip or spike.
What does affect results is chronic inconsistency. Missing doses regularly. Varying your schedule by 2 to 3 days in both directions. Creating a pattern of unpredictable drug levels that prevents the smooth, sustained appetite suppression tirzepatide is designed to provide. If you are wondering why you are not losing weight on tirzepatide, irregular dosing schedule is one of the first things to evaluate before attributing the problem to the medication itself.
The compounding effect of perfect timing
There is a difference between "fine" and "optimal." Taking your dose a day early once is fine. Taking your dose within a 2-hour window on the same day every single week for months is optimal. That level of consistency produces the most uniform drug levels, the most predictable appetite suppression, and the most reliable weight loss trajectory.
People who achieve the most impressive tirzepatide weight loss results tend to share one characteristic beyond their dose: rigorous consistency. Same day, roughly same time, every week, without exception. They treat their injection schedule the way a musician treats practice, not as something that happens when convenient, but as something that happens on schedule because the results depend on it.
For men specifically, the data on male tirzepatide results shows that consistent dosing combined with resistance training and adequate protein intake produces the best body composition outcomes. Timing your injection to align with your weekly routine, rather than fighting against it, supports the behavioral consistency that drives long-term success.
Dose timing during titration versus maintenance
During dose titration, the escalation phase where you increase from 2.5 mg to 5 mg to 7.5 mg and beyond, timing precision matters more. Each dose increase introduces your body to a new drug level. Consistent 7-day intervals during this phase give your prescriber the cleanest data about how you tolerate each dose. Irregular intervals muddy the picture and can lead to premature escalation or unnecessary delays.
During maintenance, once you have reached your target dose and your weight loss has stabilized, timing flexibility increases. Your body has fully adapted. Steady state is well established. The difference between a 6-day and an 8-day interval is pharmacologically minimal. This is not permission to become cavalier about your schedule, but it is permission to relax about the occasional one-day shift.
If you want to understand exactly how your dose translates to units for precise measurement, the detailed guides on 20 units of tirzepatide in milligrams, 40 units of tirzepatide, and 7.5 mg in units provide the exact conversions you need.
Common dose timing mistakes and how to avoid them
After working through the pharmacology and the protocols, let us get practical. These are the timing mistakes people actually make, not hypothetical concerns, but real-world errors that affect real-world outcomes.
Mistake 1: counting days instead of hours
"I injected on Monday so I can inject again on Thursday because that is 3 days." No. Monday at 8 PM to Thursday at 8 AM is not 72 hours. It is 60 hours. The 72-hour rule counts hours, not calendar days. If your phone has a timer function, set it after each injection. When it reaches 72:00:00, you are cleared. This eliminates the mental math that trips people up.
Mistake 2: adjusting the dose because of timing changes
Some people, thinking they are being careful, reduce their dose when injecting early or increase it when injecting late. Do not do this. The prescribed dose is the prescribed dose regardless of timing. If you are cleared for 5 mg weekly, you take 5 mg whether your interval is 6 days or 8 days. Adjusting the dose without medical guidance introduces a variable your prescriber is not tracking, which makes it impossible to accurately assess your response to the medication.
If you are using compounded tirzepatide from a vial and drawing your own doses, accurate measurement is even more critical during schedule changes. The tirzepatide reconstitution guide covers proper preparation techniques, and using the compounded tirzepatide dosage calculator ensures your drawn volume matches your prescribed milligrams exactly.
Mistake 3: "making up" for a missed dose by doubling
Never take a double dose. This sounds obvious, but the temptation exists, especially when someone misses a dose and feels their appetite returning. A double dose of tirzepatide is a recipe for severe nausea, vomiting, and potentially dangerous drops in blood sugar for people using it for type 2 diabetes management. One dose, on schedule or within the recovery window. That is all. Ever.
Mistake 4: ignoring injection-day symptoms as timing clues
Your body provides feedback about dose timing, but many people ignore it. If you consistently feel nauseous on injection day, that is information. If your appetite returns strongly on day 6, that is information. If you experience headaches on day 2 post-injection, that is information. These patterns can help you optimize your timing, but only if you track them.
Keep a simple log. Date, time, injection site, and any symptoms in the 48 hours after. Over a few weeks, patterns emerge. Some people discover that evening injections eliminate their nausea. Others find that a specific day of the week, aligned with their lowest-stress period, produces the best tolerance. This data is invaluable for personalizing your protocol beyond the generic guidelines.
Mistake 5: stopping and restarting without guidance
Taking an unplanned break from tirzepatide, whether because of a supply issue, travel, or a decision to "take a week off," and then restarting without any dose adjustment is a common mistake. After gaps of two or more weeks, restarting at your previous dose can overwhelm a body that has partially de-adapted. The speed of tirzepatide onset after restarting depends on how long the gap was and what dose you left off at. Always consult your prescriber before restarting after extended breaks.
Mistake 6: combining timing changes with other protocol changes
Changed your injection day AND started a new supplement AND switched injection sites AND began a new diet all in the same week? You have created a situation where any positive or negative change cannot be attributed to any single variable. Make one change at a time. If you are shifting your injection day, keep everything else constant for at least two to three weeks before introducing additional changes. Whether you are exploring supplements to take with tirzepatide or adjusting your meal plan, introduce each change in isolation so you can evaluate its impact independently.
Dose timing and nutrition: what to eat and when
Timing your injection is only half the equation. What you eat and when you eat it relative to your injection creates a synergy that most people never optimize. The relationship between tirzepatide timing and nutrition planning deserves dedicated attention because it directly affects both side effect severity and weight loss outcomes.
The 24-hour nutrition window around injection
The 12 hours before and 12 hours after your injection represent the most critical nutrition window of your week. During this period, your body is transitioning from declining drug levels (pre-injection) to rapidly rising drug levels (post-injection). What sits in your stomach during this transition matters.
Before injection, eat a moderate meal that includes easily digestible protein and complex carbohydrates. Avoid high-fat meals, large portions, and foods known to cause GI distress independently. The goal is a partially full stomach with foods that will clear relatively quickly. A meal heavy in fat or fiber takes 4 to 6 hours to digest even without tirzepatide, and once the drug begins slowing gastric emptying after injection, that meal could sit for 8 to 10 hours. The result is bloating, nausea, and discomfort that people wrongly attribute to the medication itself when the real culprit is poor meal timing.
After injection, keep meals light for 24 hours. Small, frequent portions of bland, protein-rich foods work better than large meals. Avoid carbonated beverages, which add gas to an already sluggish stomach. Avoid alcohol, which compounds the GI effects and stresses the liver during a period of active drug absorption. The comprehensive foods to avoid on tirzepatide guide covers the specific items most likely to cause problems, and the optimal foods list for tirzepatide provides alternatives that work with, not against, the medication mechanism.
Weekly meal planning around injection day
Strategic meal planning built around your injection schedule produces better outcomes than generic diet advice. Here is a framework that aligns nutrition with the pharmacokinetic curve of tirzepatide through the week.
Days 1 to 2 post-injection represent peak drug activity. Appetite is at its lowest. Nausea risk is at its highest. Plan light, nutrient-dense meals that prioritize protein. This is not the time for elaborate dinners or social eating events. Keep it simple, keep it small, and focus on hydration. Many people find that 3 small meals and no snacks work perfectly during these days.
Days 3 to 5 post-injection represent the sweet spot. Appetite suppression is strong but the initial GI effects have subsided. This is when structured tirzepatide meal planning pays the biggest dividends. You can eat normally, in moderate portions, with a focus on hitting protein targets that preserve lean mass during weight loss. Meal prepping for these days ensures you eat intentionally rather than reactively.
Days 6 to 7 post-injection represent the waning period. Appetite begins returning for most people, and the temptation to overeat is strongest. This is where behavioral strategies matter most. Having pre-portioned meals ready, avoiding trigger foods in the house, and staying occupied during traditionally difficult hours (late afternoon, late evening) prevent the caloric surplus that undermines weekly progress. The downloadable tirzepatide meal plan provides day-by-day guidance specifically structured around this weekly cycle.
Hydration and timing
Dehydration amplifies every side effect of tirzepatide. Nausea gets worse. Constipation intensifies. Headaches appear. Fatigue deepens. And the risk of dehydration increases during tirzepatide treatment because reduced food intake often means reduced fluid intake, especially from foods with high water content.
Aim for a minimum of 80 to 100 ounces of water daily, with an emphasis on increasing intake during the first 48 hours post-injection. Electrolyte supplementation, particularly sodium, potassium, and magnesium, becomes important as well. Many of the recommended supplements for tirzepatide users specifically address electrolyte balance and the nutritional gaps that reduced caloric intake can create.
Alcohol timing relative to injection
This topic warrants additional emphasis beyond the brief mention in the special populations section. The interaction between tirzepatide and alcohol is not just about blood sugar. Tirzepatide slows gastric emptying, which means alcohol stays in your stomach longer, gets absorbed more slowly, but produces more prolonged intoxication effects. People who could previously handle two drinks comfortably often find that one drink produces unexpectedly strong effects while on tirzepatide.
If you choose to drink, timing your consumption for days 5 through 7 of your injection cycle, when gastric emptying has partially normalized, reduces the intensity of this interaction. Detailed guidance on drinking alcohol while on tirzepatide covers the specific considerations for different types of alcohol, recommended limits, and warning signs that indicate you should stop.
Injection technique and timing best practices
The physical act of injecting tirzepatide is straightforward. But technique details that seem minor, like injection site rotation, depth of injection, and skin preparation, can affect absorption rate and therefore indirectly affect dose timing considerations.
Injection site rotation and absorption variability
Tirzepatide is injected subcutaneously, meaning into the fatty tissue beneath the skin. The three approved injection sites are the abdomen (at least 2 inches from the navel), the front of the thigh, and the back of the upper arm. Each site has different subcutaneous fat thickness and blood supply, which produces slightly different absorption rates.
The abdomen generally provides the fastest and most consistent absorption. The thigh absorbs slightly more slowly. The upper arm falls somewhere in between but is harder to self-inject without assistance. These differences are small, usually within the 8-to-72-hour Cmax window, but they exist. If you notice that your side effect timing shifts when you change injection sites, absorption variability is likely the explanation.
For consistent pharmacokinetics and predictable timing, many prescribers recommend rotating between sides of the same injection area rather than rotating between different areas. For example, alternate between left and right abdomen week to week rather than switching between abdomen and thigh. This approach maintains consistent absorption while still preventing injection site reactions from repeated use of the same exact spot. The complete GLP-1 injection site guide provides detailed instructions with visual references for each location.
Preparing your injection properly
For people using compounded tirzepatide from multi-use vials, the preparation process adds steps that pharmaceutical pen users do not face. Proper reconstitution technique ensures consistent potency from the first draw to the last. Using bacteriostatic water rather than sterile water preserves multi-use vial integrity. And understanding proper storage after reconstitution prevents degradation between doses.
Timing the preparation is important too. Injecting immediately after reconstituting a new vial means the solution is fresh and at maximum potency. Drawing from a vial that was reconstituted weeks ago, or one that has been stored improperly, introduces uncertainty about actual dose delivered. For precise dosing, especially when making timing adjustments, knowing that your medication is at full potency removes one variable from an already complex equation. The comprehensive peptide storage guide covers temperature requirements, light exposure concerns, and shelf life for various formulations.
Understanding your dose in multiple formats
When discussing timing adjustments with your prescriber, being able to communicate your dose in both milligrams and units prevents miscommunication. Different pharmacies, different syringe types, and different formulation concentrations all use different measurement scales. Knowing that your 5 mg dose equals a specific number of units on your insulin syringe, and understanding how that translates to milligrams per unit, gives you the precision needed for informed timing decisions.
Resources covering specific conversions like 2.5 mg to units, 5 mg to units, 7.5 mg to units, and 50 units to milligrams eliminate the guesswork. And the semaglutide dosage calculator provides a parallel resource for people also taking or switching to that medication.
Dose timing for compounded versus pharmaceutical tirzepatide
The growing market for compounded tirzepatide introduces additional timing considerations that users of pharmaceutical brand-name products do not face. While the active molecule is the same, the formulation differences can affect pharmacokinetics in ways that matter for dose timing.
Pharmaceutical tirzepatide timing
Brand-name tirzepatide (Mounjaro, Zepbound) comes in pre-filled pens with precisely manufactured formulations. The pharmacokinetic data, the 120-hour half-life, the 8-to-72-hour peak absorption window, the 1.6-fold steady-state accumulation, all comes from studies of these pharmaceutical formulations. When you follow the timing guidelines in this article, you are following guidance that directly applies to these products.
The stability of pharmaceutical formulations also simplifies storage timing. Understanding how long tirzepatide lasts in the fridge is straightforward with commercial products because they come with specific storage guidelines and expiration dates from the manufacturer. These products maintain potency reliably within their stated shelf life, so timing your injections does not require worrying about whether the medication has degraded.
Compounded tirzepatide timing
Compounded tirzepatide, prepared by compounding pharmacies using bulk tirzepatide powder, introduces variables. Different pharmacies use different concentrations, different vehicles (the liquid the tirzepatide is dissolved in), and different stabilizers. Some compounded formulations use lyophilized (freeze-dried) powder that you reconstitute yourself. Others come pre-mixed in liquid form.
These formulation differences can theoretically affect absorption rate, which could influence the timing between the injection and peak drug levels. A formulation that absorbs slightly faster might produce a more pronounced peak and a steeper decline. A slower-absorbing formulation might produce a gentler curve. In practice, these differences are usually minor and fall within the range of individual variation, but they add a layer of uncertainty that pharmaceutical products do not have.
For compounded tirzepatide users, the 72-hour minimum rule still applies, but consider being slightly more conservative. If you are moving your dose up by a day, ensure you are closer to 96 hours than 72 hours to account for potential formulation variability. Many compounded formulations are available at various concentrations, and resources like the compounded tirzepatide dosage chart help you understand exactly what you are working with.
Compounded versions sometimes come in different delivery formats as well. Tirzepatide drops, oral formulations, and various injection preparations each have their own absorption characteristics. If you are considering switching between delivery methods, the oral versus injection comparison and the tablet versus injection analysis provide the detail you need to understand how timing recommendations may differ.
The role of additives in compounded formulations
Some compounded formulations include additional ingredients like B12, glycine, or niacinamide. These additions can affect the injection experience and, in some cases, absorption characteristics. Tirzepatide with B12 is one of the most popular combinations. Tirzepatide with glycine is another common formulation. And the triple combination of tirzepatide with glycine and B12 has gained significant popularity. The niacinamide formulation adds another option to the mix.
If you are using a compounded formulation with additives, the timing rules remain the same: 72-hour minimum between doses. The additives do not change tirzepatide half-life or accumulation characteristics. What they may change is your subjective experience on injection day, which could influence your preferred time of day to inject.
Sourcing and quality considerations
Timing is irrelevant if the medication itself is unreliable. Compounded tirzepatide quality varies dramatically between pharmacies. Some providers like those covered in our guides on Empower pharmacy tirzepatide, Peptide Sciences tirzepatide, and Lavender Sky tirzepatide have established track records for consistent quality. Others may produce formulations with variable potency that make dosing less predictable regardless of timing.
For people exploring affordable tirzepatide options or lower-cost compounded shots, understanding that price and quality are not always correlated is important. A cheaper formulation that delivers inconsistent potency will undermine even the most precise timing protocol. Choosing a reputable vendor and understanding peptide testing and verification protect your investment in ways that timing optimization alone cannot.
Tirzepatide timing compared to semaglutide timing
Many people have experience with semaglutide (Ozempic, Wegovy) before starting tirzepatide, or they are considering switching between the two medications. The timing rules are similar but not identical, and understanding the differences prevents confusion, especially during transitions.
Half-life comparison
Semaglutide has an elimination half-life of approximately 7 days, or 168 hours. Tirzepatide half-life is approximately 5 days, or 120 hours. This means semaglutide clears more slowly and has a longer effective duration per dose. Both medications are dosed weekly, but semaglutide maintains higher residual levels at the end of each dosing interval relative to its peak.
The practical implication: the 72-hour minimum applies to both medications, but semaglutide provides slightly more buffer if you inject late. A 9-day gap between semaglutide doses produces less of a "trough" than a 9-day gap between tirzepatide doses. Conversely, injecting either medication early within the 72-hour window carries similar risks of amplified side effects. The tirzepatide versus semaglutide dosage chart provides a detailed comparison of how the two medications relate from a dosing perspective.
Switching medications and timing
If you are transitioning from semaglutide to tirzepatide (or vice versa), timing becomes especially important. The standard recommendation is to wait at least one full dosing interval from your last injection of the old medication before starting the new one. That means waiting at least 7 days after your last semaglutide injection before your first tirzepatide injection.
Some prescribers recommend longer gaps, particularly for patients switching from higher semaglutide doses. The semaglutide to tirzepatide conversion chart maps the dose equivalencies and transition protocols. Understanding the core differences between semaglutide and tirzepatide helps contextualize why the transition requires careful management of timing, and why the side effect profiles differ. The side effect comparison between the two medications further clarifies what to expect during and after the switch.
New GLP-1 medications on the horizon
The GLP-1 receptor agonist space is evolving rapidly. Newer medications like retatrutide and mazdutide are in development or early commercialization, each with their own pharmacokinetic profiles and dosing schedules. The principles outlined in this article, understanding half-life, respecting minimum intervals, counting hours rather than days, apply to any injectable peptide medication. As the field expands, these foundational concepts will help you navigate new medications with confidence. Understanding retatrutide dosing protocols and GLP-1 plotter tools becomes increasingly valuable as options multiply.
Special populations and timing considerations
General timing guidelines apply to most people. But specific populations face unique considerations that deserve separate discussion.
Dose timing during pregnancy concerns
Tirzepatide is not approved for use during pregnancy, and it should be discontinued if pregnancy occurs or is planned. However, the timing of discontinuation matters because of the long half-life. If you stop tirzepatide, the drug remains active in your system for several weeks afterward. The general recommendation is to discontinue tirzepatide at least two months before planned conception to allow for thorough drug clearance.
For people who discover an unexpected pregnancy while on tirzepatide, the situation detailed in our guide on pregnancy on tirzepatide provides the specific guidance needed. Similarly, the question of GLP-1 medications during breastfeeding requires careful consideration of drug timing and clearance.
Dose timing with other medications
Tirzepatide slows gastric emptying, which can affect the absorption of other oral medications. This does not mean you need to change your tirzepatide timing, but you may need to adjust the timing of other medications relative to your injection. Birth control pills, thyroid medications, and blood pressure medications are among those most commonly affected by altered gastric motility.
The general strategy is to take time-sensitive oral medications at least one hour before your tirzepatide injection or at a consistent time each day regardless of your injection day. Since tirzepatide most strongly affects gastric emptying in the 24 to 72 hours post-injection, timing oral medications for the latter half of your injection cycle (days 4 through 7) may improve their absorption consistency.
Dose timing and alcohol
The question of drinking alcohol on tirzepatide relates to timing in two ways. First, alcohol can worsen the GI side effects of tirzepatide, so avoiding alcohol for 24 to 48 hours after injection is advisable. Second, alcohol can lower blood sugar, and combining alcohol with the blood-sugar-lowering effects of tirzepatide, especially shortly after injection, increases the risk of hypoglycemia in susceptible individuals.
If you plan to drink, timing your injection to maximize the gap between injection and alcohol consumption reduces your risk. Some people deliberately schedule their injection to begin a new 7-day cycle on Sunday evening, knowing that any weekend social drinking will occur in the later half of the cycle when drug levels are naturally declining.
Dose timing and exercise
Exercise timing relative to tirzepatide injection is a common concern for people using the medication alongside fitness programs. Intense exercise in the 12 to 24 hours after injection can exacerbate nausea, lightheadedness, and fatigue. The combination of vigorous physical activity and the initial GLP-1 receptor activation is simply uncomfortable for many people.
A practical approach: schedule your injection on your rest day or the day before a lighter training session. If you train Monday through Friday with rest days on weekends, a Saturday injection gives your body Sunday to process the initial absorption before returning to training on Monday. This alignment of injection timing with training schedule is one of the simplest optimizations available, and it is particularly relevant for people using tirzepatide alongside peptides for muscle growth or athletic performance protocols.
Managing side effects through strategic timing
Much of the conversation about tirzepatide timing focuses on "when is it safe to inject." But there is a more nuanced dimension: when is it optimal to inject for minimizing side effects and maximizing comfort? This is where individual experimentation, guided by pharmacological principles, produces genuinely personalized protocols.
Nausea management through timing
If nausea is your primary side effect concern, timing adjustments can make a meaningful difference. The nausea window typically spans 4 to 24 hours post-injection, with intensity peaking around 8 to 16 hours. By choosing your injection time strategically, you can align this window with periods when nausea is least disruptive.
Evening injection (8 to 10 PM) allows you to sleep through the initial peak. You may wake with mild residual nausea, but the worst has passed. Morning injection (6 to 8 AM) puts the nausea window during your active day, which some people prefer because movement and distraction reduce perceived nausea. The "worst" timing for nausea-prone individuals tends to be late morning or early afternoon (10 AM to 2 PM), which puts the peak nausea window right at dinner time when food aversion is most problematic.
Fatigue management through timing
Tirzepatide-related GLP-1 fatigue typically follows a predictable pattern. Energy dips most noticeably 12 to 36 hours post-injection, then gradually normalizes. For people who experience this fatigue pattern, injecting on Friday evening means the lowest-energy period falls on Saturday and early Sunday, when most schedules allow for rest. Injecting on Monday morning, by contrast, puts the fatigue window right in the middle of the workweek.
Think about your weekly rhythm. When can you afford to be less than 100%? Schedule your injection 12 to 36 hours before that window. This simple alignment does not eliminate fatigue, but it ensures that fatigue occurs when it is least consequential.
Muscle pain and injection site timing
Some users report muscle pain after tirzepatide injections. This is usually mild and localized, but it can be uncomfortable. If you rotate injection sites (abdomen, thigh, upper arm), consider timing your rotations to avoid using muscle groups you plan to train. Injecting into your left thigh on a day before an upper body workout, for example, avoids the discomfort of training a sore injection site.
Proper injection site selection and injection technique also reduce site-specific discomfort. A slow, steady injection into properly pinched subcutaneous tissue produces less soreness than a rushed injection into tense muscle. When you are adjusting your timing, take the extra 30 seconds to do the injection properly. Rushing an injection because you squeezed it in before leaving for work creates unnecessary discomfort that has nothing to do with the medication itself.
Building a bulletproof tirzepatide timing routine
All of this information converges on one practical goal: building a timing routine that is consistent, convenient, and resilient to disruption. Here is how to construct one.
Step 1: choose your anchor day
Pick the day of the week that is most consistently available in your schedule. Not the day you happen to have started on. Not the day your prescription was filled. The day that, week after week, month after month, offers the most reliability. For many people, this is a weekend day. For others, it is a specific weekday that reliably has the same structure.
Step 2: choose your anchor time
Morning or evening, based on your side effect profile and daily routine. If you have no strong preference, start with morning. Morning injections are easier to remember because they attach to the existing routine of waking up, and they allow you to observe your body response throughout the day rather than sleeping through it and wondering why you feel off in the morning.
Step 3: set non-negotiable reminders
A phone alarm is good. A recurring calendar event with a 1-hour and 1-day advance reminder is better. The most reliable approach is stacking the injection with an existing non-negotiable habit. If you always make coffee at 7 AM on Saturdays, tirzepatide happens at 6:55 AM before the coffee. The habit stack makes the injection automatic rather than requiring active decision-making each week.
Step 4: prepare for disruptions in advance
Know the rules before you need them. If you know you will be traveling on your injection day in three weeks, decide now whether you will inject early (72-hour minimum) or late (within 4 days). Make the decision when you are calm and can count the hours carefully, not when you are stressed in an airport.
Step 5: track everything
Date, time, dose, injection site, and brief notes on how you feel for 48 hours post-injection. After 8 to 12 weeks, you will have a dataset that reveals your personal optimal timing, your side effect patterns, and any correlations between timing variations and outcomes. This data makes you an active participant in optimizing your protocol rather than a passive recipient of generic guidelines.
SeekPeptides provides tracking tools and protocol guidance that make this process systematic rather than ad hoc. Members access structured frameworks for logging injection data, interpreting patterns, and making evidence-based adjustments to their dosing protocols. For people serious about optimizing their tirzepatide results, this kind of structured tracking makes the difference between good outcomes and exceptional ones.
Weight loss plateaus and the timing adjustment question
A question that surfaces repeatedly in online forums: "I have hit a weight loss plateau on tirzepatide. Should I change my injection timing?" The short answer is probably not. But the longer answer involves understanding what actually causes plateaus and whether timing plays any role.
What causes tirzepatide weight loss plateaus
Weight loss plateaus on tirzepatide result from metabolic adaptation, not timing issues. As you lose weight, your basal metabolic rate decreases. The body requires fewer calories to maintain a smaller mass. Eventually, the caloric deficit created by tirzepatide-induced appetite suppression narrows to the point where weight loss slows or stops. This is basic thermodynamics, not a medication failure.
Other factors contribute too. Reduced NEAT (non-exercise activity thermogenesis), hormonal shifts, water retention fluctuations, and changes in body composition all play roles. People who feel that tirzepatide is not working anymore are often experiencing one or more of these metabolic adaptations rather than a true medication failure. The solution usually involves adjusting caloric intake, increasing activity, or discussing a dose escalation with their prescriber, not changing injection timing.
That said, inconsistent timing can masquerade as a plateau. If your drug levels are fluctuating due to irregular injection intervals, your appetite suppression will be inconsistent, your eating patterns will be inconsistent, and your caloric intake will vary unpredictably from week to week. Tightening your injection timing, making it more consistent rather than simply different, sometimes resolves what appears to be a plateau. The underlying weight loss guidance in our troubleshooting article for tirzepatide weight loss covers the full range of plateau-breaking strategies.
Does energy expenditure fluctuate with dosing schedule
Some researchers theorize that the mild energy fluctuations throughout the weekly tirzepatide cycle, slightly higher metabolic rate during peak drug levels, slightly lower during the trough, could be optimized through strategic timing. The idea is that aligning peak drug levels with days of higher physical activity might marginally increase total weekly energy expenditure.
The evidence for this is weak at best. The metabolic impact of tirzepatide throughout its weekly cycle is far more gradual and sustained than the sharp peaks and troughs that would be needed to meaningfully shift daily energy expenditure. If you want to increase energy expenditure, exercise more. If you want to lose weight faster, tighten your nutrition. Timing your injection to coincide with gym days is not going to move the needle compared to those fundamental interventions.
For people who notice an energy boost or feel more motivated on certain days relative to their injection schedule, there is no harm in aligning training with those days. Some people report that tirzepatide gives them a subtle energy increase similar to what semaglutide users describe. But do not restructure your entire week around optimizing a marginal pharmacokinetic effect. The fundamentals, consistent dosing, adequate protein, regular exercise, and patience, matter infinitely more than micro-optimizing injection timing relative to workout schedules.
Understanding microdosing and timing flexibility
A growing number of people are exploring microdosing tirzepatide, which involves taking smaller doses more frequently than the standard weekly protocol. While this approach is not part of the FDA-approved prescribing information, it raises interesting timing considerations that are worth addressing.
Microdosing protocols typically involve splitting the weekly dose into two or more smaller injections spread across the week. For example, instead of 5 mg once weekly, someone might inject 2.5 mg twice weekly, separated by 3 to 4 days. The rationale is that smaller, more frequent doses may produce smoother drug levels with fewer peak-related side effects.
If you are following a microdosing protocol under medical supervision, the 72-hour rule applies to each injection as a minimum interval. Two injections of 2.5 mg separated by only 48 hours create a very different pharmacokinetic profile than two injections separated by 84 hours. The 72-hour minimum remains your safety floor regardless of the dose amount.
This is also where understanding your medication in precise units becomes essential. Guides on milligram-to-unit conversions and the semaglutide dosage equivalent in units help ensure you are measuring accurately when working with non-standard dosing schedules.
The role of GLP-1 receptor dynamics in timing
For those who want to understand the deeper science behind timing flexibility, GLP-1 receptor dynamics provide the explanation. Tirzepatide is a dual GIP and GLP-1 receptor agonist, and both receptor systems have characteristics that influence how the body responds to varying drug levels.
GLP-1 receptors undergo tachyphylaxis, a reduction in response with sustained stimulation. This is actually beneficial for timing flexibility, because it means your body does not respond to each dose as if it is the first time. By the time you reach steady state, the receptors have partially adapted. A slightly higher drug level from an early injection does not produce a proportionally amplified response. The receptor downregulation provides a built-in buffer against minor timing variations.
This is part of why understanding how peptides work at the receptor level gives you a more nuanced perspective on timing. The body is not a simple dose-response machine. It adapts, compensates, and modulates. This biological flexibility is what makes the 72-hour minimum rule workable, rather than requiring exact 168-hour intervals with zero tolerance for variation.
For a broader understanding of the GLP-1 medication class, the relationship explained in our guide on whether GLP-1 is the same as Ozempic clarifies how different medications in this category share fundamental timing principles while differing in their specific pharmacokinetic profiles.
Long-term considerations for dose timing
Tirzepatide is often prescribed for extended periods. Understanding how timing flexibility evolves over a long treatment course helps you plan for the months and years ahead.
Dose timing after significant weight loss
As you lose weight, your body composition changes. Less body fat means a different volume of distribution for the medication. In practical terms, the same dose may produce slightly different blood concentrations in a 200-pound body versus a 160-pound body. This does not change the 72-hour minimum rule, but it means that the side effect profile at a given dose may shift as your weight changes. If you notice that early dosing, which was previously well-tolerated, starts producing nausea after significant weight loss, the changing pharmacokinetics of your lighter body may be the explanation.
Transitioning off tirzepatide
When the time comes to discontinue tirzepatide, whether because you have reached your goal weight or for another reason, the long half-life means the drug does not leave your system overnight. After your final injection, meaningful drug levels persist for approximately three to four weeks. Appetite gradually returns during this period. Understanding this timeline helps you plan your transition. Many people experience withdrawal-like symptoms that are common across the GLP-1 class, and the timeline of symptom emergence follows the pharmacokinetic clearance curve. Knowing that duration of treatment varies by individual helps set realistic expectations.
Maintaining results after discontinuation
Dose timing during the discontinuation phase can ease the transition. Rather than stopping abruptly, some prescribers recommend gradually extending the interval between doses. Instead of weekly injections, move to every 10 days, then every 14 days, then stop. This tapering approach allows the body to gradually readjust to unmedicated appetite levels, reducing the rebound effect that many people experience with abrupt discontinuation.
Regardless of how you discontinue, the behavioral habits established during treatment, meal planning, portion awareness, regular exercise, become your primary tools for weight maintenance. The tirzepatide diet plan principles remain valuable even after the medication is stopped, because the underlying nutritional strategies support healthy eating independently of pharmacological appetite suppression.
Frequently asked questions
Can I take tirzepatide 2 days early?
Yes. Two days early on a weekly schedule means a 5-day (120-hour) interval between doses. This exceeds the 72-hour minimum and is pharmacologically safe. However, if you are in the dose-escalation phase or prone to GI side effects, the extra residual drug at the 120-hour mark may slightly amplify nausea. Consider injecting in the evening to sleep through any peak-absorption side effects. Check the tirzepatide dose chart to understand your specific dose parameters.
What happens if I accidentally take tirzepatide after 5 days instead of 7?
A 5-day interval is within safe parameters (above 72 hours). You may notice slightly stronger appetite suppression or mild GI effects compared to your usual 7-day interval, but these are typically minor and self-resolving. Simply resume your regular 7-day schedule from the early injection date, or return to your original day the following week, whichever is more convenient. Monitor your response with the compounded tirzepatide dosage calculator to ensure accuracy.
Does changing my injection day reset my progress?
No. One irregular interval does not reset steady-state concentrations, tolerance, or weight loss trajectory. Your body reaches steady state over approximately four weeks of consistent dosing. A single shorter or longer interval creates a minor, temporary fluctuation that resolves within days. Your overall progress, tracked through tools like the before and after tracking resources, reflects months of cumulative effort, not individual weekly intervals.
Can I switch from a weekday injection to a weekend injection?
Absolutely. Use the day-shifting protocol: make the jump in one move, ensuring at least 72 hours between your last weekday injection and your first weekend injection. Then maintain the 7-day rhythm from the new weekend day. Most people who switch to weekends report better adherence because weekend mornings are less rushed and more consistent.
Is it better to take tirzepatide in the morning or at night?
Neither is pharmacologically superior. The choice depends on your personal side effect experience. Morning injection aligns peak appetite suppression with afternoon and evening hours when overeating is most common. Evening injection allows you to sleep through peak nausea. Try both over several weeks and compare your experience. The approach that works for semaglutide timing often applies to tirzepatide as well, since the medications share the GLP-1 mechanism.
What if I miss my dose by 3 days?
Take it immediately. A 3-day delay (10 days between doses) is within the 4-day recovery window. Inject your normal dose as soon as you remember, then resume your regular schedule the following week. Expect slightly reduced appetite suppression during the extended gap and potentially a brief return of GI side effects as drug levels rebuild. Understanding how quickly tirzepatide restores appetite suppression helps set expectations for the days following a catch-up dose.
Can I take my tirzepatide dose early before surgery?
This requires guidance from your surgeon and prescribing physician. Tirzepatide slows gastric emptying, which is a concern for anesthesia and surgical procedures. Many surgeons require GLP-1 agonists to be held for 1 to 3 weeks before procedures involving general anesthesia, specifically because of the delayed gastric emptying and aspiration risk. Do not adjust your timing for surgery without direct medical guidance. The peptide safety guide covers additional perioperative considerations.
Does the 72-hour rule change at higher doses?
The 72-hour minimum applies at all dose levels. However, the consequences of violating it escalate with dose. At 2.5 mg, injecting at 60 hours instead of 72 might produce mild additional nausea. At 15 mg, the same premature injection could produce severe GI distress. Higher doses mean higher residual levels at any given time point, which means the excess from early injection is proportionally larger. For detailed unit-to-milligram conversions at each dose level, consult the 7.5 mg conversion guide or the 40-unit conversion guide.
Can I split my tirzepatide dose across two days instead of taking it all at once?
Splitting a single weekly dose across two separate injections on consecutive days is not recommended and fundamentally changes the pharmacokinetic profile of the medication. The drug was designed and tested as a single weekly injection, and the clinical trial data supporting its safety and efficacy is based on that dosing pattern. If you are interested in alternative dosing approaches like microdosing tirzepatide, discuss this with your prescriber so they can adjust the protocol appropriately and monitor your response under medical supervision.
Should I adjust my tirzepatide timing if I start exercising more?
Increased exercise does not require changing your injection schedule, but you may want to consider how your injection day aligns with your training week. Many active people prefer injecting on rest days or before lighter training days to avoid combining peak drug absorption with intense physical activity. If you are incorporating peptides for muscle growth or fat loss protocols alongside tirzepatide, strategic timing can reduce the likelihood that post-injection fatigue or nausea disrupts your training quality.
What if my prescriber says to take tirzepatide every 5 days instead of every 7?
Some prescribers individualize dosing intervals based on patient response. A 5-day interval (120 hours) is above the 72-hour minimum and can be clinically appropriate for patients who metabolize the drug faster or who experience inadequate coverage toward the end of a 7-day cycle. If your prescriber has recommended a shorter interval, follow their guidance. The 7-day standard applies to the general population, but individual pharmacokinetics vary, and your prescriber has information about your specific response that generic guidelines do not account for. Using the peptide calculator tools helps you stay precise regardless of your prescribed interval.
External resources
For people committed to optimizing every aspect of their tirzepatide protocol, from timing to nutrition to side effect management, SeekPeptides offers the most comprehensive resource available. Members access detailed dosing protocols, precision calculators, structured tracking tools, and a community of thousands who have navigated these exact questions. The difference between following generic guidelines and following a personalized, evidence-based protocol is often the difference between adequate results and exceptional ones.
In case I do not see you, good afternoon, good evening, and good night.
May your doses stay on schedule, your side effects stay manageable, and your results stay consistent.