Feb 13, 2026

You have done everything right. You filled the prescription, took the injection on schedule, and waited four full weeks for the scale to budge. Nothing. Maybe a pound down one morning, then back up the next day. Maybe the number has not moved at all. And now you are wondering whether semaglutide even works, whether you wasted your money, whether something is wrong with your body that makes you different from all those people posting dramatic before-and-after photos online.
Stop. Take a breath. What you are experiencing is far more common than the internet would have you believe. The clinical trials that got semaglutide approved for weight loss tell a story that most people never hear. At the four-week mark, participants on the starting dose of 0.25 mg lost an average of just 2% of their body weight. For someone weighing 200 pounds, that is about 4 pounds. For someone at 250 pounds, roughly 5 pounds. Barely noticeable on a standard bathroom scale. And that average includes people who lost nothing at all during those first 30 days.
The truth is that four weeks on semaglutide is not enough time to judge whether the medication works. Not even close. You are on the lowest possible dose, your body is still building steady-state drug levels, and the real weight loss phase has not even started. This guide will explain exactly why you are not seeing results yet, what is happening inside your body right now, what the clinical data actually shows about early semaglutide outcomes, and precisely when you should expect the scale to start cooperating. We will also cover the specific situations where four weeks of no weight loss might actually signal a problem that needs addressing, because sometimes the issue is real, and knowing the difference matters.
Why 0.25 mg is not a weight loss dose
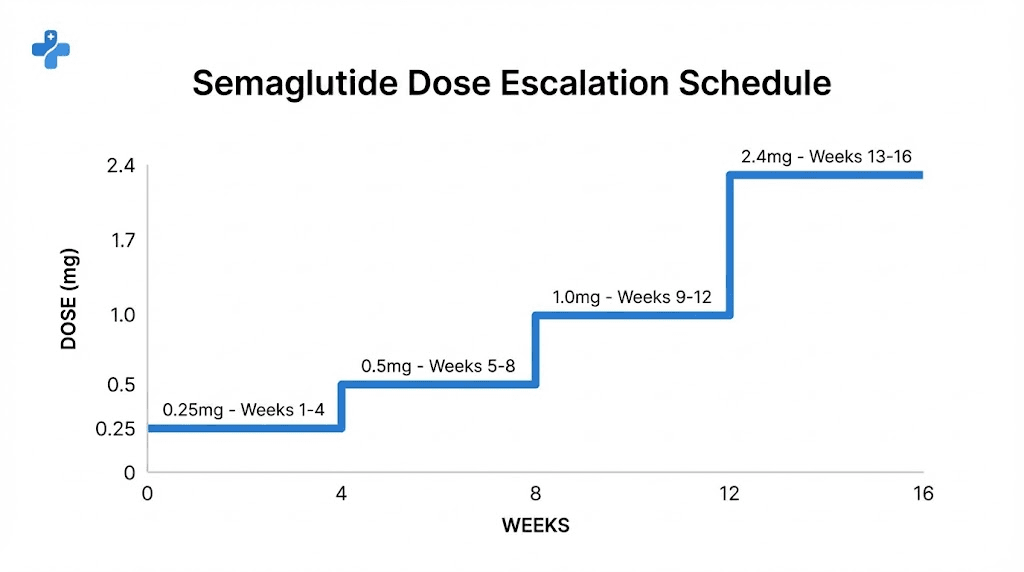
Here is something your prescriber may not have explained clearly. The starting dose of semaglutide, 0.25 mg per week, is not designed to make you lose weight. It exists for one reason: to let your gastrointestinal system adjust to the medication without making you violently nauseous. That is it. The semaglutide dosage schedule follows a careful five-step escalation that takes 16 to 20 weeks before you reach the full therapeutic dose.
Think about what that means. At four weeks, you have completed exactly one step of a five-step process. You are taking roughly 10% of the dose that produced the headline results in clinical trials. Expecting significant weight loss at this point is like expecting to run a marathon after training for one week. The foundation is being laid, but the real work has not started.
The complete dose escalation schedule works like this. Weeks 1 through 4, you take 0.25 mg weekly. Weeks 5 through 8, you move to 0.5 mg. Weeks 9 through 12, the dose increases to 1.0 mg. Weeks 13 through 16, you take 1.7 mg. And finally, from week 17 onward, you reach the maintenance dose of 2.4 mg per week. Each increase happens every four weeks, and each step gives your body time to adapt before the next escalation. Some people need even longer at each step, spending 8 weeks instead of 4 at a given dose if side effects are severe.
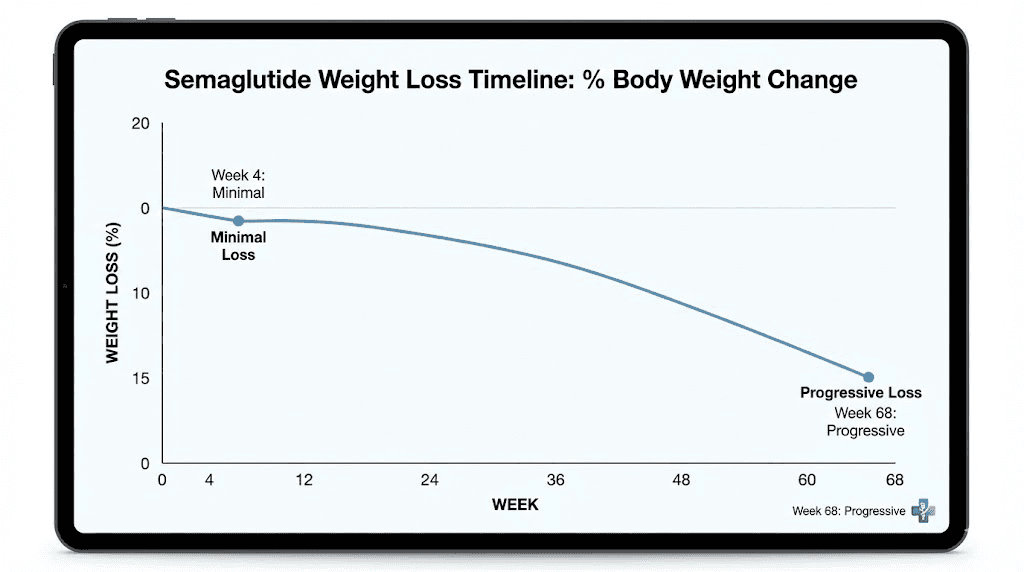
The STEP 1 trial, published in the New England Journal of Medicine, enrolled 1,961 adults and followed them for 68 weeks. The average weight loss at the full 2.4 mg dose was 14.9% of body weight, compared to just 2.4% with placebo. But those results came after months at the highest dose. At week 4, participants were still on 0.25 mg, and the weight loss was minimal for most. The trial specifically noted that weight loss was observed from the first assessment at week 4 onward, but the significant, visible, life-changing results did not appear until participants had been at higher doses for several weeks.
So when you search "4 weeks on semaglutide no weight loss" and find yourself panicking, remember this. You are not on the weight loss dose yet. You are on the preparation dose.
What is actually happening in your body right now
Even though the scale is not moving, semaglutide is doing things. Important things. Understanding what is happening beneath the surface can help you stay patient during these early weeks when visible results are absent.
GLP-1 receptor activation is ramping up
Semaglutide works by mimicking a hormone called GLP-1, which your gut naturally produces after eating. This hormone signals your brain to feel full, slows stomach emptying, and influences how your pancreas manages blood sugar. At 0.25 mg, you are introducing a synthetic version of this hormone at very low levels. Your appetite suppression mechanisms are just beginning to activate.
Research shows that semaglutide can reduce energy intake by approximately 40% compared to people not taking the medication. But that reduction does not happen overnight at the starting dose. It builds gradually as drug levels accumulate in your bloodstream. The half-life of semaglutide is approximately one week, which means it takes 4 to 5 weeks of consistent dosing to reach what pharmacologists call "steady state," the point where the amount entering your body each week roughly equals the amount being eliminated. At four weeks, you are only just reaching steady state at the lowest dose.
Your brain is recalibrating hunger signals
One of the most significant changes happening during these early weeks involves the hypothalamus, the brain region that regulates appetite and energy balance. Semaglutide crosses the blood-brain barrier and directly affects neurons that control hunger and satiety. This recalibration takes time.
Many people report subtle shifts in their relationship with food during the first month, even without weight loss. Portions feel slightly more satisfying. The urge to snack between meals weakens. Cravings for high-calorie foods become less urgent. These changes often precede weight loss by several weeks. If you are noticing any reduction in appetite, even a small one, the medication is working. The weight loss will follow.
Blood sugar regulation is improving
Even at 0.25 mg, semaglutide is already improving your GLP-1 receptor function. Your pancreas is receiving clearer signals about when to release insulin, and your blood sugar levels after meals are becoming more stable. This metabolic improvement creates the foundation for fat burning that will accelerate at higher doses. You may not see it on the scale, but your metabolic machinery is being tuned.
The clinical data on early semaglutide results
Let us look at what the actual research says about weight loss in the first month, because the numbers tell a very different story than social media.
STEP 1 trial early results
The landmark STEP 1 trial, the study that led to Wegovy approval, showed weight loss beginning from the first assessment at week 4. But the curve was shallow in the early phase and steepened dramatically as doses increased. By week 68 on the full 2.4 mg dose, 86.4% of participants had lost at least 5% of their body weight. That means roughly 14% of people, even on the highest dose for over a year, did not hit the 5% threshold. The percentage who saw meaningful results at week 4, on 0.25 mg, was substantially smaller.
The timeline for semaglutide to work follows a predictable pattern across clinical trials. Minimal weight loss in weeks 1 through 8, moderate loss in weeks 8 through 16 as doses increase, and the steepest weight loss between weeks 16 and 40 when patients reach and maintain the therapeutic dose. Results typically plateau between weeks 40 and 60, with the nadir, or lowest weight, occurring around week 60.
What "average" actually means
When you read that the average first-month weight loss is 2% to 3.8% of body weight, remember that averages hide enormous variation. Some people in the trials lost 8 pounds in the first month. Others gained weight. The average of those wildly different experiences is the 2% number you keep seeing. Your personal result at week 4 might fall anywhere on that spectrum, and it tells you almost nothing about where you will end up at week 20 or week 40.
A separate analysis of the STEP trials found that early response, meaning the amount of weight lost in the first 4 to 8 weeks, was a weak predictor of long-term outcomes. People who lost nothing in the first month sometimes went on to lose 15% or more of their body weight by the end of the trial. The early phase simply does not predict the final result with any reliability.
The 20-week milestone
Multiple studies and clinical guidelines point to 20 weeks as the first meaningful checkpoint. The reason is simple. By week 20, most patients have been on the full 2.4 mg dose for at least 4 weeks, giving the medication enough time to reach steady state at the therapeutic level. Before that point, drawing conclusions about effectiveness is premature.
The NICE (National Institute for Health and Care Excellence) guidelines recommend reassessing semaglutide after 6 months. If a patient has not lost at least 5% of their body weight by that point, the recommendation is to discontinue. But six months. Not four weeks. The difference between those timelines is everything.
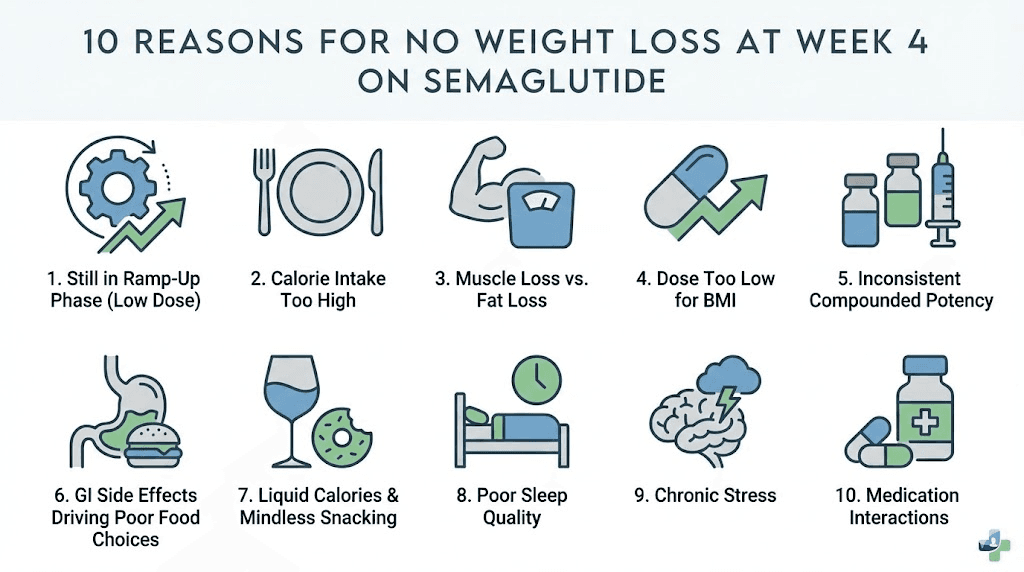
10 specific reasons your scale is stuck at week 4
While the most likely explanation for no weight loss at four weeks is simply that it is too early, there are specific factors that can contribute to a slow start. Some are fixable. Others require patience. All of them are worth understanding.
1. You are still on the sub-therapeutic dose
We have covered this, but it bears repeating because it is the single most important factor. At 0.25 mg weekly, the semaglutide concentration in your bloodstream is simply too low to drive significant appetite suppression in most people. The medication is working, but like a volume dial turned to 1 out of 10, the effect is barely perceptible. Each dose increase over the coming weeks will turn that dial higher.
2. Water retention is masking fat loss
This is more common than most people realize, especially in the first month. Starting a new medication can trigger temporary fluid shifts in your body. Hormonal fluctuations, changes in sodium intake (which often shift when appetite changes), and even the stress of starting a new treatment can cause water retention of 2 to 5 pounds. You might actually be losing fat tissue while simultaneously holding extra water, resulting in a flat or even slightly higher scale reading.
Signs that water retention is a factor include puffy fingers (rings feeling tighter), swollen ankles, weight fluctuations of 2 or more pounds between morning and evening, and feeling bloated despite eating less. If this sounds familiar, do not panic. Water weight is temporary and will resolve as your body adjusts. Staying hydrated, moderately reducing sodium, and being patient are the best responses.
3. You are not in a calorie deficit
Semaglutide is not magic. It reduces appetite, but it does not force you to eat less. If you are consuming the same number of calories as before, whether because your appetite has not significantly decreased at this low dose, or because you are eating calorie-dense foods in smaller volumes, you will not lose weight regardless of the medication. The research is clear: semaglutide works by helping you eat less, and if that reduction has not happened yet, neither will weight loss.
This is particularly relevant for people who eat out of habit rather than hunger. Semaglutide primarily reduces physical hunger signals, but it has less effect on emotional eating, boredom eating, or habitual snacking. If your eating patterns are driven more by routine than by actual hunger, the medication may need time and higher doses to shift those patterns. A thoughtful semaglutide diet plan can help bridge this gap while doses are still being escalated.
4. Your starting weight affects the timeline
People with lower starting BMIs often see slower initial results on semaglutide. This makes biological sense. When you have less excess weight to lose, your body defends its current weight more aggressively, and the calorie deficit needed to move the scale must be more precise. Someone starting at 300 pounds may notice results sooner than someone starting at 200 pounds, even though both are responding to the medication equally well from a metabolic standpoint.
5. You are gaining muscle while losing fat
If you started an exercise routine around the same time you began semaglutide, particularly a strength training program, you may be experiencing body recomposition. Muscle is denser than fat, so gaining muscle while losing fat can result in a stable or even slightly higher scale weight, despite visible changes in how your clothes fit and how your body looks.
This is actually a best-case scenario. Research published in multiple journals shows that weight loss with preserved muscle mass leads to better long-term outcomes, lower rebound risk, and improved metabolic health. If your clothes are looser, your energy is better, or you notice visual changes even without scale movement, body recomposition is likely happening.
6. Menstrual cycle fluctuations
For women, the menstrual cycle can mask weight loss by causing 2 to 7 pounds of water retention in the luteal phase (the two weeks before menstruation). If your four-week weigh-in happens to fall during this phase, your actual fat loss could be completely hidden by cyclical water retention. Tracking weight across a full cycle, rather than at a single point, gives a much more accurate picture.
7. Medications that counteract weight loss
Several common medications can slow or prevent weight loss, even when semaglutide is working correctly. These include certain antidepressants (particularly SSRIs like paroxetine and mirtazapine), beta-blockers used for blood pressure, corticosteroids like prednisone, insulin and certain oral diabetes medications, and some anti-seizure medications. If you take any of these, discuss the interaction with your prescriber. The solution is not to stop your other medication, but to set realistic expectations and potentially adjust your weight loss timeline.
8. Thyroid dysfunction
An underactive thyroid (hypothyroidism) can significantly impair weight loss. If you have undiagnosed or undertreated hypothyroidism, semaglutide will work less effectively because your basal metabolic rate is suppressed. Common signs include fatigue, cold intolerance, constipation, and dry skin. A simple blood test for TSH and free T4 can rule this out. If you have not had your thyroid checked recently, ask your doctor to include it in your next blood work.
9. Sleep quality is undermining your efforts
Poor sleep has a devastating effect on weight loss that most people underestimate. Research consistently shows that sleeping fewer than 6 hours per night increases ghrelin (the hunger hormone), decreases leptin (the satiety hormone), raises cortisol (which promotes fat storage), and reduces insulin sensitivity. If you are sleeping poorly, your body is biochemically primed to hold onto weight, regardless of what medication you are taking.
Some people experience disrupted sleep in the first few weeks of semaglutide, particularly if gastrointestinal side effects like nausea are present. If this applies to you, addressing the nausea (eating smaller meals, avoiding fatty foods, taking the injection before bed) can improve sleep quality and potentially accelerate weight loss.
10. Compounded semaglutide may differ from brand-name versions
If you are using compounded semaglutide rather than brand-name Wegovy or Ozempic, this could be a factor. The FDA has warned that some compounding pharmacies use semaglutide salts (like semaglutide acetate or semaglutide sodium) rather than the semaglutide base found in FDA-approved products. These salt forms have not been tested in clinical trials for safety or effectiveness, and their bioavailability may differ from the original formulation.
Compounded products can also vary in formulation, dosage accuracy, and quality from one batch to another. If you are on compounded semaglutide and seeing no response at all, even subtle appetite changes, it may be worth discussing the product source with your prescriber. Understanding proper storage of compounded semaglutide is also critical, as improper storage can degrade the active ingredient and reduce effectiveness.
What you should be tracking instead of weight
The scale is the least useful measurement tool during the first month of semaglutide therapy. Seriously. If you are going to track anything during weeks 1 through 8, focus on these metrics instead. They will give you a much clearer picture of whether the medication is working.
Appetite changes
Are you thinking about food less often? Do meals satisfy you sooner? Is the space between meals more comfortable? Even subtle shifts in appetite indicate that semaglutide is activating the right pathways. Rate your hunger before each meal on a scale of 1 to 10, and track whether those numbers trend downward over the first month. A change from averaging 8/10 to 6/10 is significant, even if the scale has not moved.
Portion sizes
Are you leaving food on your plate more often? Finishing meals sooner? Ordering less when eating out? Reduced portion sizes are one of the earliest visible signs that semaglutide is working, and they often appear before any weight change. Even a 10% to 15% reduction in portion sizes, if sustained, will translate to weight loss over the coming weeks.
Cravings and food noise
"Food noise" is the term that has emerged for the constant mental chatter about food: what to eat next, what snacks are available, what sounds good right now. Many semaglutide users report a significant reduction in food noise as one of the earliest effects. If your mind is quieter about food than it was a month ago, the medication is doing its job.
Blood sugar stability
If you have a glucose monitor or notice changes in energy levels throughout the day, pay attention. More stable energy, fewer afternoon crashes, and reduced sugar cravings are all signs that semaglutide is improving your metabolic function. These changes precede weight loss and predict better outcomes at higher doses.
Waist measurements
The tape measure catches changes that the scale misses. Measure your waist at the belly button level, your hips at the widest point, and your thighs at mid-thigh. Do this once a week at the same time (morning, after using the bathroom, before eating). Even half an inch of change over four weeks indicates progress, and body composition changes, especially reductions in visceral fat, can happen without the scale moving.
The realistic semaglutide weight loss timeline
Knowing what to expect and when to expect it can prevent the frustration that leads many people to quit prematurely. Here is what the clinical data and real-world experience suggest for a typical semaglutide journey.
Weeks 1 through 4 (0.25 mg)
Expected weight loss: 0 to 4 pounds. Many people lose nothing. Some gain a pound or two from water retention. Appetite changes may be subtle or absent. Gastrointestinal side effects (nausea, constipation) are common as your body adjusts. This phase is about tolerance, not results.
Weeks 5 through 8 (0.5 mg)
Expected weight loss: 2 to 6 pounds total from baseline. Appetite suppression becomes more noticeable at this dose. You may start eating smaller portions without effort. Some people experience their first real weight loss during this phase, though it remains modest. Semaglutide fatigue may occur as your body adjusts to reduced calorie intake.
Weeks 9 through 12 (1.0 mg)
Expected weight loss: 5 to 12 pounds total from baseline. This is typically when weight loss becomes visible and consistent. Appetite suppression is more pronounced. Food choices often shift naturally toward lighter, more nutritious options. Appetite suppression becomes a reliable feature rather than an occasional effect.
Weeks 13 through 16 (1.7 mg)
Expected weight loss: 8 to 18 pounds total from baseline. Weight loss accelerates as you approach the therapeutic dose. Most people are now losing 1 to 2 pounds per week consistently. The trajectory is clear and encouraging.
Weeks 17 through 28 (2.4 mg maintenance)
Expected weight loss: 12 to 30 pounds total from baseline. This is the steepest part of the weight loss curve. At the full dose, appetite suppression is at its maximum, metabolic effects are fully engaged, and the combination of reduced intake and improved metabolic function drives consistent, significant weight loss.
Weeks 28 through 68 (2.4 mg continued)
Expected weight loss: 20 to 50+ pounds total from baseline (10% to 17% of starting body weight). Weight loss continues but the rate gradually slows. The body reaches a new equilibrium. In the STEP 1 trial, weight loss reached its nadir around week 60 before stabilizing.
The critical takeaway: you are currently in the earliest, flattest part of this curve. The steep descent has not begun.
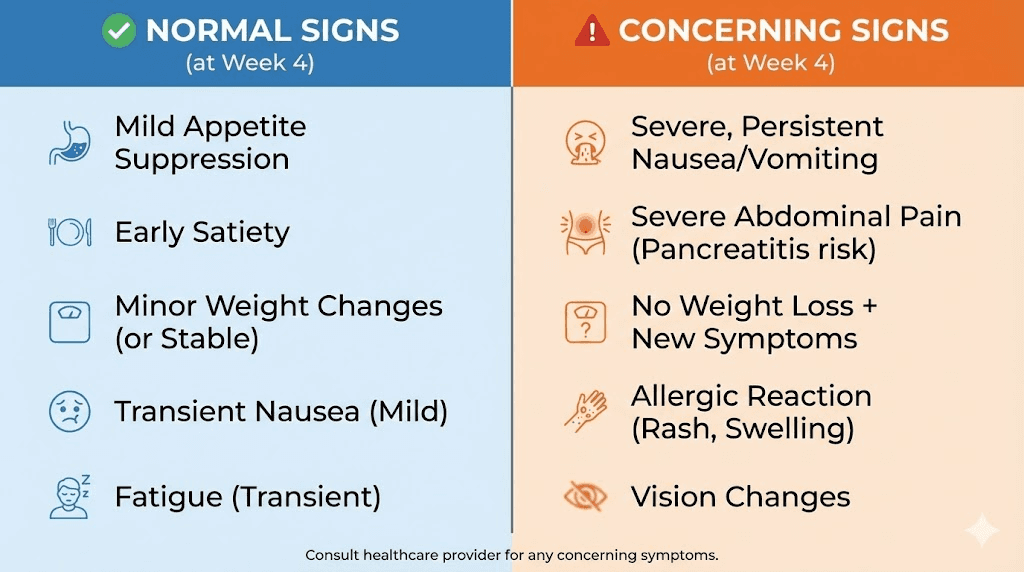
When no weight loss at 4 weeks is actually a concern
While the default answer is "it is too early to worry," there are specific situations where no weight loss at four weeks warrants a conversation with your prescriber.
You feel zero appetite change
If you feel absolutely no difference in hunger, satiety, or food interest after four full weeks, this is worth mentioning. Most people notice at least subtle appetite changes on 0.25 mg, even if those changes are not enough to drive weight loss yet. Complete absence of any effect could indicate an absorption issue, particularly if you are using a compounded product.
You are gaining weight
A small amount of weight gain (1 to 3 pounds) from water retention is normal and temporary. But if you have gained more than 5 pounds while taking semaglutide, something else is happening. It could be a medication interaction, an underlying endocrine issue, or a behavioral pattern that needs addressing. Do not ignore a significant upward trend.
You are experiencing severe side effects with no benefits
If you have been dealing with significant nausea, vomiting, or diarrhea for four weeks without any appetite suppression or weight change, the risk-benefit balance needs reassessing. Side effects without benefits suggest the medication may not be right for you, or the product may have quality issues.
You have had trouble with injections
Inconsistent dosing is a common reason for poor early results. If you have missed doses, varied the injection day significantly, or had trouble with the injection technique, the medication may not be reaching steady state on schedule. Semaglutide should be injected on the same day each week, and consistency matters enormously during the dose-escalation phase.
Understanding proper injection technique and finding the right reconstitution method can make a significant difference in outcomes if you are using a compounded vial product.
What to do right now to set up month 2 for success
Instead of panicking about the scale, use these remaining days before your dose increases to optimize everything else. Think of month 1 as preparation for the real weight loss phase. Here is your action plan.
Dial in your nutrition foundations
You do not need a perfect diet, but you do need some structure. Focus on protein first, aiming for at least 0.7 grams per pound of body weight daily. Protein preserves muscle during weight loss, increases satiety, and has the highest thermic effect of any macronutrient (meaning your body burns more calories digesting it). Good sources include chicken, fish, eggs, Greek yogurt, and legumes. A solid semaglutide-friendly eating plan emphasizes protein at every meal.
Reduce ultra-processed foods gradually. These items are engineered to override satiety signals, which directly works against what semaglutide is trying to do. You do not need to eliminate them entirely, but shifting your ratio toward whole foods amplifies the medication effectiveness significantly.
Hydration matters more than most people think. Dehydration can trigger hunger signals that feel identical to real hunger. Aim for at least 64 ounces of water daily, and increase that amount if you are exercising or experiencing semaglutide-related constipation.
Start or refine an exercise routine
Exercise during semaglutide therapy serves multiple purposes beyond burning calories. It preserves muscle mass (critical since weight loss medications can cause some lean mass loss), improves insulin sensitivity, boosts mood, and accelerates metabolic adaptations. But the type of exercise matters.
Resistance training 3 to 4 times per week is the single most important exercise you can do while on semaglutide. Studies show that patients who combined semaglutide with resistance training preserved significantly more muscle mass than those who did not exercise, with some even gaining muscle while losing fat. Start with basic movements: squats, lunges, push-ups, rows, and planks. You do not need a gym. You need consistency.
Add moderate cardio 2 to 3 times per week. Walking 30 to 45 minutes daily is sufficient. Intense cardio is not necessary and can actually increase hunger, which works against the medication. Keep it moderate and sustainable.
Optimize your sleep
Aim for 7 to 9 hours of quality sleep per night. If nausea is disrupting your sleep, try taking your injection on a day when you can afford a slightly rough next day. Some people find that injecting before bed reduces daytime nausea. Others prefer morning injections so the nausea peaks during the day when they are active and distracted. Experiment during this first month to find your optimal injection timing.
Start a tracking system
Create a simple weekly log that tracks weight, waist measurement, appetite rating (1-10 before meals), sleep hours and quality, exercise performed, and how you feel overall. This data will be invaluable at your next appointment, giving your prescriber concrete information to guide dose adjustments. It also provides objective evidence of progress when the scale is not cooperating.
Lifestyle changes that amplify semaglutide results
The STEP trials that produced those impressive 15% weight loss numbers did not just test semaglutide. They tested semaglutide plus lifestyle intervention. Participants received dietary counseling, exercise guidance, and behavioral support alongside the medication. The drug alone, without lifestyle modification, produces smaller results. Here is how to create your own lifestyle intervention.
The protein leverage hypothesis
Research from the University of Sydney has shown that humans eat until they consume a threshold amount of protein, regardless of how many total calories they take in. This means that if your diet is low in protein, you will naturally eat more of everything to hit that protein target. By front-loading protein in your meals, you hit the target faster and consume fewer total calories. This works synergistically with semaglutide appetite suppression.
Practical application: start each meal with your protein source. Eat the chicken before the rice. Have the eggs before the toast. This simple sequencing trick has been shown to reduce total meal intake by 10% to 20% in studies, even without semaglutide.
Meal timing and frequency
As semaglutide begins suppressing appetite (which will intensify with dose increases), many people naturally shift toward fewer, larger meals rather than multiple small snacks. This pattern, sometimes called time-restricted eating, aligns well with the medication mechanism. Instead of fighting to maintain three meals and two snacks, let your appetite guide your eating frequency.
Some people on semaglutide find that they naturally gravitate toward two substantial meals per day with no snacking. Others maintain three smaller meals. There is no right answer. The key is to eat when genuinely hungry and stop when satisfied, rather than following a rigid schedule that may conflict with the appetite signals the medication is sending.
Stress management
Chronic stress elevates cortisol, which promotes visceral fat storage and increases cravings for high-calorie, high-sugar foods. If your stress levels are high, cortisol is actively working against semaglutide. Basic stress reduction techniques like 10 minutes of daily meditation, regular walks in nature, deep breathing exercises, or even simply reducing screen time before bed can lower cortisol levels enough to make a measurable difference in weight loss outcomes.
Alcohol reduction
Understanding whether you can drink on semaglutide is important for several reasons. Alcohol adds empty calories, impairs judgment around food choices, disrupts sleep, and can worsen gastrointestinal side effects. Many semaglutide users report decreased interest in alcohol naturally, which is likely a GLP-1 mediated effect on reward pathways. If you can reduce or eliminate alcohol during the dose escalation phase, you remove a significant barrier to weight loss.
Comparing your experience to realistic expectations
Social media has badly distorted expectations for semaglutide weight loss. Let us correct the record with actual data.
What Instagram and TikTok show versus reality
The dramatic transformation posts you see online represent the best-case outcomes, often after 6 to 12 months on the medication. Nobody posts "I lost 0 pounds in my first month on semaglutide" even though that is a perfectly normal and common experience. The selection bias is extreme. You are comparing your week 4 results to someone else curated week 40 results, and that comparison is both unfair and misleading.
Reddit experiences
Forum discussions on Reddit paint a more honest picture. Users commonly report 8% to 18% body weight reduction within 6 to 12 months, often surpassing prior diet or medication efforts. But they also report frustrating early weeks, plateaus lasting 2 to 3 weeks at various points, and non-linear progress. A common pattern described online is losing nothing for weeks, then suddenly dropping 3 to 4 pounds over a few days, then plateauing again. Weight loss on semaglutide is rarely a smooth, steady decline.
The 13.6% who are true non-responders
In the STEP 1 trial, 86.4% of participants on semaglutide lost at least 5% of their body weight. That means 13.6% did not, even after 68 weeks at the full dose. These are true non-responders, and they exist. But they were identified after more than a year of treatment at the maximum dose, not after four weeks at the starting dose. You cannot know at week 4 whether you are in the 86% who respond or the 14% who do not. It is simply too early.
If you are concerned about being a non-responder, the honest answer is that you need to wait. Stay on the medication, follow the dose escalation schedule, implement the lifestyle changes described above, and reassess at the 3 to 6 month mark. That is when the data becomes meaningful.
The compounded semaglutide factor
If you are using compounded semaglutide rather than brand-name Wegovy or Ozempic, there are specific considerations that could affect your early results.
Salt form versus base form
FDA-approved semaglutide products (Wegovy and Ozempic) use semaglutide base as the active ingredient. Some compounding pharmacies use semaglutide salts, such as semaglutide acetate or semaglutide sodium. These are chemically different from the base form and have not been tested in clinical trials. Their absorption, distribution, and effectiveness may differ. The FDA has specifically warned about this distinction.
Dosage accuracy
Compounded products can vary in potency from one batch to another. If your compounded vial contains less semaglutide than labeled, or if the semaglutide has degraded due to improper manufacturing or poor storage, you may be getting less medication than you think. Proper reconstitution technique is essential when working with compounded vials, and understanding how much bacteriostatic water to mix with your vial directly affects the accuracy of each dose.
Storage and handling
Compounded semaglutide requires proper refrigeration. If the product was exposed to high temperatures during shipping, left out of the fridge for extended periods, or stored improperly at any point in the supply chain, the active ingredient may have degraded. Make sure you understand compounded semaglutide storage requirements and follow them precisely.
What to do if you suspect product quality issues
If you have been on compounded semaglutide for 4 weeks with absolutely no effects, not even subtle appetite changes, nausea, or any other sign that the medication is active in your system, consider discussing with your prescriber. Options include trying a different compounding pharmacy, switching to brand-name Wegovy or Ozempic if insurance covers it, or having your current product tested. The Empower Pharmacy semaglutide guide can help you understand what to look for in a reputable compounder.
Semaglutide versus tirzepatide: does the choice matter for early results?
Some people who see no results on semaglutide wonder whether tirzepatide (Mounjaro/Zepbound) would work better. It is a fair question, though the answer at week 4 is the same: it is too early to know.
Tirzepatide works on two receptors (GLP-1 and GIP) rather than just GLP-1 alone, and clinical trials suggest it may produce slightly greater average weight loss than semaglutide. The SURMOUNT-1 trial showed average weight loss of 20.9% at the highest dose over 72 weeks, compared to semaglutide average of 14.9% at the highest dose over 68 weeks. But tirzepatide also follows a dose escalation schedule and starts at a sub-therapeutic dose, meaning the first four weeks are similarly uneventful for many people.
The semaglutide versus tirzepatide comparison is complex and depends on individual factors including insurance coverage, side effect tolerance, cost, and metabolic profile. Switching medications after only four weeks on a starting dose is almost never recommended. Give semaglutide a proper trial at therapeutic doses before considering alternatives.
If you are curious about the dosage differences between the two medications, or wondering about switching between them, those resources can help you understand the landscape without making premature decisions.
Supplements and additions that might help
While no supplement replaces proper dose escalation and lifestyle changes, certain additions can support your early semaglutide journey.
Vitamin B12
There is growing interest in combining semaglutide with B12. GLP-1 receptor agonists can sometimes reduce B12 absorption by slowing gastric emptying, and B12 deficiency can cause fatigue, weakness, and even weight gain. Some compounding pharmacies offer semaglutide pre-mixed with B12 for this reason. If you are experiencing significant fatigue on semaglutide, a B12 supplement is a reasonable addition to discuss with your prescriber.
Glycine
The combination of semaglutide with glycine has emerged as a topic of interest in the weight loss community. Glycine is an amino acid that may help reduce some of the gastrointestinal side effects of semaglutide while supporting metabolic health. Some users report better tolerance and fewer stomach issues when taking glycine alongside their GLP-1 medication.
Fiber supplementation
If reduced food intake is causing constipation, a fiber supplement can help. Psyllium husk is gentle and effective. Start with a small amount (one teaspoon daily) and increase gradually, drinking plenty of water. Constipation can cause several pounds of water retention and stool weight that masks fat loss on the scale.
Electrolytes
Eating less means consuming fewer electrolytes. Low sodium, potassium, or magnesium can cause water retention, fatigue, muscle cramps, and headaches. An electrolyte supplement or adding a pinch of salt to water can help, particularly during the first few months when your eating patterns are shifting most dramatically.
The mental game: managing expectations and frustration
The emotional aspect of seeing no weight loss after starting a medication you were excited about cannot be understated. Here is how to manage the psychology of this phase.
Reframe the timeline
You did not gain your excess weight in four weeks. You will not lose it in four weeks. Weight loss medication is a long-term intervention, not an instant fix. The people who achieve the best outcomes on semaglutide are those who commit to at least 6 to 12 months of treatment, implement lifestyle changes alongside the medication, and resist the urge to quit when progress is slow in the early weeks.
Stop weighing yourself daily
Daily weigh-ins during the first month of semaglutide are an exercise in frustration. Water weight fluctuates by 2 to 5 pounds day to day based on sodium intake, hydration, menstrual cycle, bowel movements, and exercise. Weighing yourself daily shows you noise, not signal. Switch to weekly weigh-ins under consistent conditions (same day, same time, same clothing, after using the bathroom, before eating), or better yet, weigh monthly during the dose escalation phase and focus on the non-scale metrics described earlier.
Avoid comparison traps
Everyone responds to semaglutide differently. Your genetics, metabolism, starting weight, diet, exercise habits, stress levels, sleep quality, and countless other factors influence your unique response curve. Comparing your week 4 results to anyone else, whether online or in your personal life, provides zero useful information. Your only valid comparison is you at week 4 versus you at week 20.
Talk to your prescriber, not the internet
If you are genuinely concerned, call your doctor or weight loss clinic. They can review your specific situation, check for underlying issues, and provide reassurance based on their experience with hundreds of patients. Internet forums and social media, while occasionally helpful, are not substitutes for personalized medical guidance.
Week-by-week action plan for your first 8 weeks
Here is a concrete plan to maximize your outcomes during the dose escalation phase. Follow this, and by the time you reach 1.0 mg, your body will be optimally positioned for the accelerated weight loss phase.
Week 1 (0.25 mg, dose 1)
Take your first injection. Note any side effects. Start a food journal (even a simple one in your phone notes). Weigh yourself once on the morning after your injection to establish a baseline. Focus on learning your injection technique and establishing which day of the week works best for your injection schedule.
Week 2 (0.25 mg, dose 2)
Maintain injection consistency (same day, same time). Begin focusing on protein intake, aiming for 25 to 30 grams of protein at each meal. Start drinking more water if you are not already at 64 ounces daily. Do not weigh yourself this week. Notice any changes in appetite, even subtle ones.
Week 3 (0.25 mg, dose 3)
Begin or continue an exercise routine. Three resistance training sessions and two 30-minute walks per week is an excellent baseline. Take your waist measurement for the first time. Continue the food journal. If experiencing nausea, try smaller, more frequent meals.
Week 4 (0.25 mg, dose 4)
Weigh yourself under consistent conditions. Take waist measurement. Compare appetite levels to week 1. If you have noticed any appetite changes, you are on track. If you have noticed zero changes, make a note to discuss with your prescriber at your next appointment. This is where you are right now, and if you are reading this article, you are doing exactly the right thing: seeking information rather than quitting.
Week 5 (0.5 mg, dose 1 at new dose)
The dose doubles. This is where many people feel the first real appetite suppression. Continue protein focus. Continue exercise. Manage any new side effects from the dose increase (nausea is common when stepping up). The semaglutide dosing chart can help you track where you are in the escalation schedule.
Week 6 (0.5 mg, dose 2)
Appetite changes should be more noticeable now. Portions may naturally decrease. Food noise may quiet. Continue the same routine. If nausea is severe, discuss a slower escalation with your prescriber.
Week 7 (0.5 mg, dose 3)
Weigh yourself (weekly check-in). Take waist measurement. Compare all metrics to week 4. Most people will see some movement by now, whether on the scale, the tape measure, or in their appetite patterns. If everything is still completely flat, book an appointment with your prescriber.
Week 8 (0.5 mg, dose 4)
The second escalation approaches. Review your food journal. How have your portions changed? How has your hunger changed? Take stock of non-scale victories. Prepare for the next dose increase to 1.0 mg, which is when weight loss typically accelerates meaningfully for most people.
When to talk to your doctor: the 8-week checkpoint
If you have completed 8 full weeks of semaglutide (4 weeks at 0.25 mg and 4 weeks at 0.5 mg) with absolutely zero weight loss and zero appetite changes, it is time for a medical conversation. This is different from the 4-week mark, where patience is almost always the right answer.
Questions to ask your prescriber
Come prepared with your tracking data. Specific questions to raise include: Should we check thyroid function? Am I on any medications that might be interfering? Is the compounded product I am using a reputable source? Should we consider a faster dose escalation? Are there other factors we should investigate? Would you recommend any blood work to rule out metabolic issues?
Potential adjustments your doctor might suggest
Based on your 8-week data, your prescriber might recommend accelerated dose escalation if you are tolerating the current dose well with no side effects, a switch from compounded to brand-name semaglutide, adding or adjusting thyroid medication, reviewing and potentially changing other medications that may interfere, or referral to a registered dietitian for nutrition optimization.
What your doctor should NOT suggest at this point
Any prescriber who tells you to give up on semaglutide after only 4 to 8 weeks, unless you are experiencing dangerous side effects, does not understand the medication timeline. The evidence is clear: semaglutide requires months at therapeutic doses to demonstrate its full potential. Finding a prescriber who understands this timeline is important for your success.
Long-term success strategies beyond the first month
As you move past the frustrating early weeks, these strategies will help you build momentum and maximize your eventual results.
Build habits during dose escalation that stick during weight loss
The dose escalation period is actually a gift in disguise. Use it to build the nutrition, exercise, and sleep habits that will amplify semaglutide once you reach the therapeutic dose. People who establish these habits before the rapid weight loss phase begins consistently achieve better outcomes than those who rely solely on the medication and scramble to add lifestyle changes later.
Plan for the long game
Research from the STEP 5 trial, which followed participants for two years, shows that semaglutide duration matters. Continued treatment maintains weight loss. Stopping treatment leads to weight regain in most people. Think of semaglutide not as a short-term fix but as a long-term metabolic tool. This mindset shift reduces the pressure to see immediate results and allows you to focus on sustainable lifestyle changes that complement the medication.
Address the root causes alongside the medication
Semaglutide addresses the biological drivers of overeating, specifically hunger hormones and brain appetite regulation. But it does not address emotional eating, stress eating, or food addiction directly. If these are significant factors in your weight, consider adding behavioral support (therapy, counseling, or a support group) alongside the medication. The combination of pharmaceutical appetite suppression and behavioral change tools is more powerful than either alone.
For researchers looking to optimize their approach, SeekPeptides offers comprehensive resources on peptide-based weight loss strategies, including detailed protocol guides, community support from experienced users, and evidence-based information that goes beyond what most online sources provide.
Understanding semaglutide withdrawal and dose changes
Some people, frustrated by lack of early results, consider stopping semaglutide or skipping doses. This is almost always counterproductive.
What happens when you skip or stop
Skipping a dose disrupts the steady-state concentration you have been building for four weeks. It essentially resets the clock, meaning your body needs another 4 to 5 weeks to rebuild consistent drug levels. If you skip a dose, take it as soon as you remember (as long as your next scheduled dose is at least 2 days away). If it is closer than that, skip the missed dose and take the next one on schedule.
Stopping entirely leads to semaglutide withdrawal effects including the return of appetite, potential weight regain, and a rebound in food cravings. If you do decide to stop, do so in consultation with your prescriber rather than abruptly.
Dose acceleration: is faster escalation an option?
Some prescribers will accelerate the dose escalation if patients tolerate the starting dose well and experience no side effects. This is a clinical decision that balances the desire for faster results against the risk of gastrointestinal side effects. If you have had zero nausea on 0.25 mg, your prescriber might consider moving to 0.5 mg after two weeks instead of four. This is not standard protocol but is within clinical discretion. Ask about it if you are tolerating the medication well.
The role of metabolic adaptation
Understanding metabolic adaptation helps explain why early weight loss on semaglutide can be unpredictable.
What metabolic adaptation means
Your body actively resists weight loss. This is not a flaw. It is a survival mechanism refined over millions of years of evolution. When your body senses reduced calorie intake, it responds by lowering your resting metabolic rate, increasing hunger hormones, making you more efficient at extracting calories from food, and reducing unconscious movement (fidgeting, restlessness). This is why diet alone usually fails for long-term weight loss, and it is part of why semaglutide is revolutionary. The medication directly counteracts some of these adaptive responses.
How semaglutide fights adaptation
Unlike calorie restriction alone, semaglutide actively suppresses the hunger hormones that spike during dieting. It maintains the feeling of fullness even as calorie intake decreases. It improves insulin sensitivity, which helps your body access fat stores more efficiently. And it appears to influence the brain set point for body weight, essentially telling your hypothalamus that a lower weight is acceptable. These mechanisms take time to fully engage, which is yet another reason why four weeks is too early to judge.
Frequently asked questions
Is it normal to not lose weight in the first month of semaglutide?
Yes, completely normal. The starting dose of 0.25 mg is sub-therapeutic for weight loss. Clinical trial data shows average first-month weight loss of only 2% of body weight, and many participants lost nothing at all during weeks 1 through 4. Meaningful weight loss typically begins once doses reach 1.0 mg or higher, usually around weeks 9 through 12. For a full semaglutide timeline, the evidence points to patience.
How much weight should I have lost by week 4 on semaglutide?
The clinical average is 0 to 4 pounds at the four-week mark, with 2% of body weight being the typical average. Some people lose more, many lose nothing. This number is a poor predictor of long-term results. People who lost zero pounds in month 1 have gone on to lose 15% or more of their body weight by month 12 in clinical trials.
Should I increase my semaglutide dose faster if I am not losing weight?
Do not adjust your dose without consulting your prescriber. The standard schedule increases from 0.25 mg to 0.5 mg at week 5. Some prescribers may accelerate this if you are tolerating the medication well, but this is a clinical decision that requires medical judgment. The semaglutide dosage chart shows the recommended escalation pathway.
Can I eat normally on semaglutide and still lose weight?
Semaglutide works by reducing appetite, which naturally leads to eating less. If your appetite has not decreased yet (common at the starting dose), you may need to make conscious dietary adjustments. Focusing on protein, reducing ultra-processed foods, and following a structured semaglutide diet plan can bridge the gap until appetite suppression kicks in at higher doses.
Does compounded semaglutide work as well as Wegovy?
Compounded semaglutide has not been tested in clinical trials, so its effectiveness compared to brand-name products is unknown. The FDA has warned about quality variations, particularly regarding salt forms versus base forms. If you are using compounded semaglutide and experiencing zero effects, discuss product quality with your prescriber.
Will semaglutide cause muscle loss?
Studies show that weight loss on semaglutide involves some lean mass loss alongside fat loss, similar to any calorie-restricted weight loss. Participants in 68 to 72 week trials lost 10% or more of their muscle mass in some studies. However, combining semaglutide with resistance training 3 to 5 times per week and adequate protein intake (0.7 to 1.0 g per pound of body weight) significantly reduces muscle loss. Some people even gain muscle while losing fat when they exercise consistently.
When should I be worried about no weight loss on semaglutide?
At 4 weeks, concern is premature. At 8 weeks (after two dose levels), consider discussing with your prescriber if you have had zero appetite changes. At 3 to 6 months on the full 2.4 mg dose, if you have not lost at least 5% of body weight, NICE guidelines recommend reassessing whether the medication is appropriate for you.
Can other medications prevent semaglutide from working?
Several medication classes can slow weight loss, including certain antidepressants (SSRIs like paroxetine, mirtazapine), beta-blockers, corticosteroids, insulin, and some anti-seizure medications. Do not stop any prescribed medication without consulting your doctor, but do inform your prescriber about everything you take so they can account for potential interactions.
External resources
STEP 5 Trial: Two-Year Effects of Semaglutide in Adults with Overweight or Obesity (Nature Medicine)
Once-Weekly Semaglutide for Weight Management: A Clinical Review (PMC)
FDA Concerns with Unapproved GLP-1 Drugs Used for Weight Loss
For researchers serious about optimizing their weight loss protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, personalized dosage calculators, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your patience stay strong, your doses stay consistent, and your results stay worth the wait.