Feb 12, 2026

Of the 480 adverse event reports the FDA received about compounded tirzepatide through April 2025, a staggering number traced back to one root cause. Dosing errors. Patients measured 5 to 20 times their intended dose because nobody showed them the math. Not because the math is hard. Because nobody showed them.
That ends here.
Calculating your compounded tirzepatide dose requires exactly two numbers and one formula. Your vial concentration in mg/mL. Your target dose in milligrams. And a division problem a fourth grader could solve. But getting it wrong, even slightly, means the difference between effective weight loss and a trip to the emergency room. The FDA documented hospitalizations from dosing miscalculations where healthcare providers themselves got the unit-to-milligram conversion wrong. This is not a beginner mistake. It is a universal vulnerability for anyone working with compounded formulations. SeekPeptides built its peptide dosage calculator specifically to eliminate this problem, and this guide walks you through the complete calculation process so you understand every number before you draw a single unit into a syringe.
This guide covers the universal dosage formula, complete conversion charts for every common concentration, step-by-step real-world examples, the most dangerous calculation mistakes, reconstitution math for lyophilized powder, dose escalation schedules with exact unit counts, and a verification system that catches errors before they reach your body. Whether your vial reads 5 mg/mL or 60 mg/mL, you will know exactly how many units to draw for any milligram dose.
The universal compounded tirzepatide dosage formula
Every compounded tirzepatide calculation uses the same formula. Learn it once. Use it forever. There is no special math for different concentrations, different vial sizes, or different pharmacies. One formula covers everything.
The two-step calculation
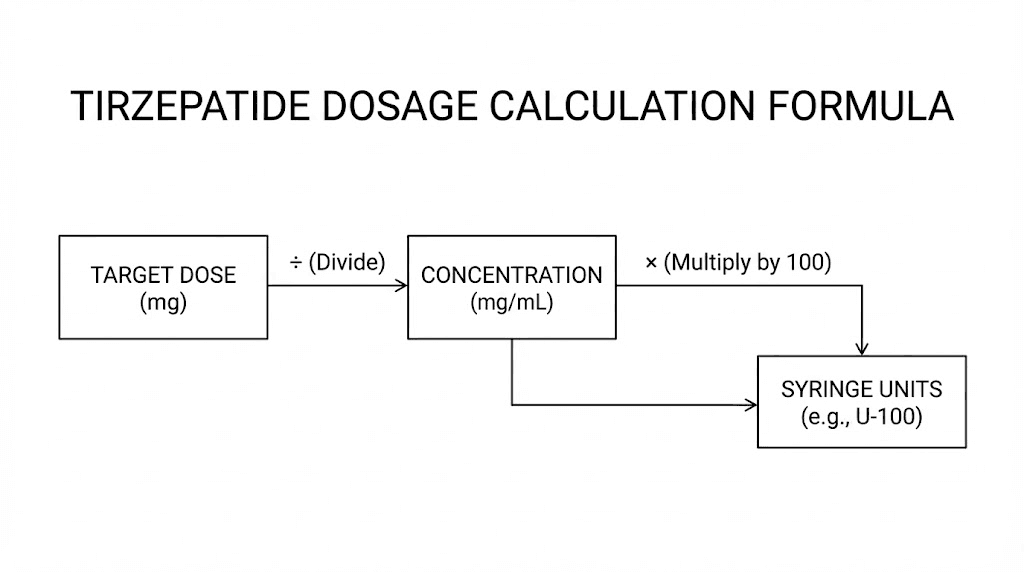
Step 1: Convert your dose to volume
Volume (mL) = Desired dose (mg) / Vial concentration (mg/mL)
Step 2: Convert volume to syringe units
Syringe units = Volume (mL) x 100
That is it. Two operations. Division, then multiplication. The result tells you exactly how many units to draw on a standard U-100 insulin syringe.
Or combine them into a single formula:
Units = (Desired dose in mg / Concentration in mg/mL) x 100
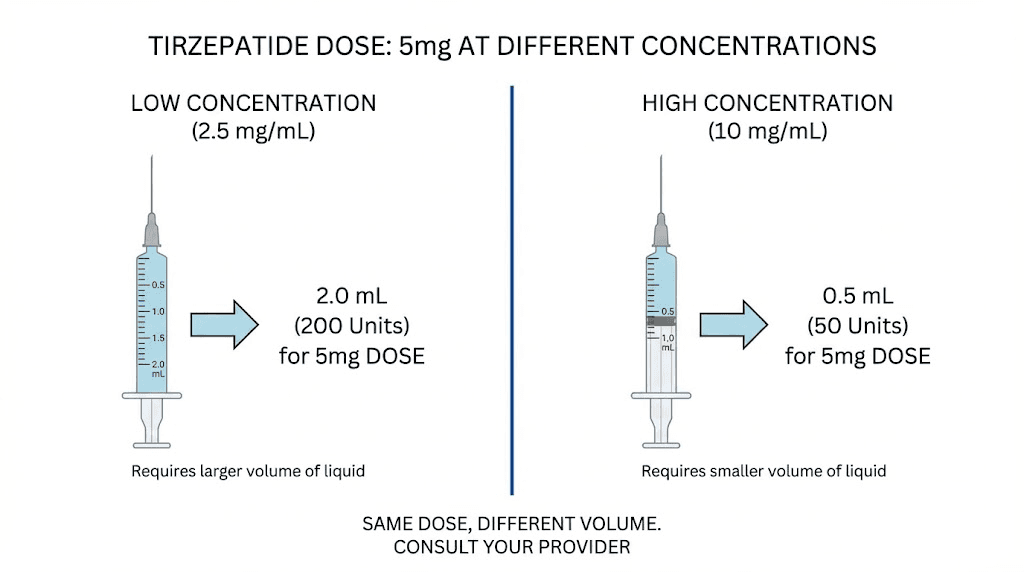
Let us test it. You want 2.5 mg from a 10 mg/mL vial. Units = (2.5 / 10) x 100 = 25 units. Draw to the 25-unit mark on your syringe. Done.
Now the same dose from a 20 mg/mL vial. Units = (2.5 / 20) x 100 = 12.5 units. Same milligrams. Half the volume. Completely different syringe reading. This is why understanding your concentration matters more than memorizing unit counts. For a deeper look at how to calculate peptide dosages across different compounds, our complete calculation guide covers the fundamentals.
Why one formula works for every concentration
The formula works because it accounts for the only variable that changes between vials: concentration. Everything else stays constant. A U-100 syringe always treats 100 units as 1 mL. A milligram is always a milligram. The only question is how many milligrams your pharmacy packed into each milliliter of liquid.
Low concentration (5 mg/mL) means fewer milligrams per milliliter, so you need more volume for the same dose. High concentration (40 mg/mL) means more milligrams per milliliter, so you need less volume. The formula automatically adjusts for both scenarios.
Think of it like coffee. Weak brew requires a bigger cup to get the same caffeine. Strong espresso delivers the same caffeine in a tiny shot. The caffeine amount (milligrams) stays the same. The liquid volume changes based on strength (concentration). Your syringe units are just measuring that liquid volume.
Complete conversion charts by concentration
While the formula handles any calculation, reference charts save time and prevent arithmetic errors during routine dosing. These charts cover every standard dose at the most common compounding pharmacy concentrations. Bookmark these alongside the compound tirzepatide dosage chart for quick reference.
5 mg/mL conversion chart
This lower concentration is common for starting-dose protocols where precision matters most.
Dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
1.25 mg | 0.25 mL | 25 units | Half starting dose |
2.5 mg | 0.50 mL | 50 units | Starting dose |
5.0 mg | 1.00 mL | 100 units | First escalation (full syringe) |
At 5 mg/mL, the 5.0 mg dose fills an entire 1 mL syringe. Doses above 5 mg require either a larger syringe or a higher concentration vial. This is why most pharmacies reserve this concentration for patients on starting doses or microdosing tirzepatide protocols.
10 mg/mL conversion chart
The most widely used concentration from compounding pharmacies. A good balance of precision and practicality.
Dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
1.25 mg | 0.125 mL | 12.5 units | Half starting dose |
2.5 mg | 0.25 mL | 25 units | Starting dose |
5.0 mg | 0.50 mL | 50 units | First escalation |
7.5 mg | 0.75 mL | 75 units | Second escalation |
10.0 mg | 1.00 mL | 100 units | Third escalation (full syringe) |
At 10 mg/mL, every standard dose tier lands on a clean, easy-to-read number of units. The 2.5 mg starting dose requires exactly 25 units, a clearly marked line on any insulin syringe. This is one reason this concentration remains the industry default. For the complete tirzepatide dosage chart in units, our dedicated guide covers all scenarios.
15 mg/mL conversion chart
A middle-ground concentration that some pharmacies use for mid-range dosing.
Dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
2.5 mg | 0.167 mL | 16.7 units | Starting dose |
5.0 mg | 0.333 mL | 33.3 units | First escalation |
7.5 mg | 0.50 mL | 50 units | Second escalation |
10.0 mg | 0.667 mL | 66.7 units | Third escalation |
15.0 mg | 1.00 mL | 100 units | Maximum dose (full syringe) |
Notice the problem. At 15 mg/mL, most standard doses produce fractional unit counts. Drawing exactly 16.7 units on a syringe where each line represents 1 or 2 units introduces measurement error. If your pharmacy provides this concentration, a 0.3 mL syringe with 0.5-unit markings offers better precision for the lower doses.
20 mg/mL conversion chart
Higher concentration for researchers on escalated doses who want smaller injection volumes.
Dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
2.5 mg | 0.125 mL | 12.5 units | Starting dose |
5.0 mg | 0.25 mL | 25 units | First escalation |
7.5 mg | 0.375 mL | 37.5 units | Second escalation |
10.0 mg | 0.50 mL | 50 units | Third escalation |
12.5 mg | 0.625 mL | 62.5 units | Fourth escalation |
15.0 mg | 0.75 mL | 75 units | Maximum dose |
At 20 mg/mL, even the maximum 15 mg dose stays under 100 units. This means every dose tier fits comfortably in a standard 1 mL syringe with room to spare. The tirzepatide dosing for weight loss in units becomes much more manageable at higher concentrations. Many researchers who advance beyond the 5 mg tier request this concentration specifically to keep injection volumes small and comfortable.
30 mg/mL conversion chart
Used by some pharmacies for patients on higher maintenance doses.
Dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
2.5 mg | 0.083 mL | 8.3 units | Starting dose |
5.0 mg | 0.167 mL | 16.7 units | First escalation |
7.5 mg | 0.25 mL | 25 units | Second escalation |
10.0 mg | 0.333 mL | 33.3 units | Third escalation |
15.0 mg | 0.50 mL | 50 units | Maximum dose |
At 30 mg/mL, the maximum 15 mg dose requires only 50 units, half a syringe. Injection comfort is excellent. But precision at starting doses becomes challenging, as 8.3 units is nearly impossible to measure accurately on a standard syringe. This concentration works best for patients already past the 5 mg dose tier. Understanding the relationship between tirzepatide dosage in units and your specific vial concentration prevents these precision problems.
40 mg/mL and 50 mg/mL conversion charts
Some specialty compounders produce ultra-high concentrations for minimal injection volume.
Dose (mg) | 40 mg/mL units | 50 mg/mL units |
|---|---|---|
5.0 mg | 12.5 units | 10 units |
7.5 mg | 18.75 units | 15 units |
10.0 mg | 25 units | 20 units |
12.5 mg | 31.25 units | 25 units |
15.0 mg | 37.5 units | 30 units |
Ultra-high concentrations reduce injection volume dramatically. At 50 mg/mL, the full 15 mg maximum dose requires just 30 units, barely a quarter of a syringe. But starting doses become impractical. Drawing 5 units for a 2.5 mg dose at 50 mg/mL is asking for measurement error. These concentrations are designed for maintenance-phase researchers, not beginners. The tirzepatide dose chart can help you determine which concentration best matches your current protocol stage.
How compounded tirzepatide differs from brand-name dosing
If you have used Mounjaro or Zepbound, the switch to compounded formulations introduces a fundamental change in how dosing works. Understanding this difference prevents the most dangerous category of dosing errors.
Brand-name tirzepatide: no math required
Mounjaro and Zepbound come as pre-filled auto-injector pens. Each pen contains a single, fixed dose. The 2.5 mg pen delivers exactly 2.5 mg. The 5 mg pen delivers exactly 5 mg. You press a button. The full dose goes in. No syringes, no calculations, no concentration to check.
This simplicity is by design. Eli Lilly engineered the delivery system to eliminate dosing errors entirely. You cannot accidentally take double or half your dose with a pen, it delivers the full contents and only the full contents.
Compounded tirzepatide: calculation required every time
Compounded tirzepatide arrives in multi-dose vials. You draw each dose yourself using an insulin syringe. The vial contains enough tirzepatide for multiple injections, and you must calculate the correct volume for your specific dose at your specific concentration.
This means every injection involves a calculation. Every new vial requires checking the concentration. Every pharmacy change might mean a different concentration. The margin for error that brand-name pens eliminate gets reintroduced with compounded vials.
The SURMOUNT-1 clinical trial demonstrated weight loss of up to 22.5% in participants using FDA-approved tirzepatide. Those results came with precisely controlled doses. Reproducing those results with compounded formulations demands the same dosing precision, which starts with accurate calculations. The compound tirzepatide dosing chart provides the week-by-week schedule that mirrors clinical trial protocols.
What the FDA says about compounded dosing risks
The FDA has issued explicit warnings about compounded GLP-1 receptor agonist dosing. Their concerns center on three issues: variable concentrations between pharmacies, unclear dosing instructions provided to patients, and the measurement challenges of using insulin syringes for non-insulin medications.
Through April 2025, the FDA received 480 adverse event reports related to compounded tirzepatide. Multiple reports involved hospitalizations. The agency noted that "many patients mistakenly administered 5 to 20 times their intended dose" because of unit-to-milligram confusion. Healthcare providers themselves made dosing miscalculations when converting between milligrams, milliliters, and units.
This is not fear-mongering. It is documented reality. And it is entirely preventable with the right calculation method. Understanding peptide safety fundamentals is the foundation of responsible research.
The five most dangerous calculation mistakes
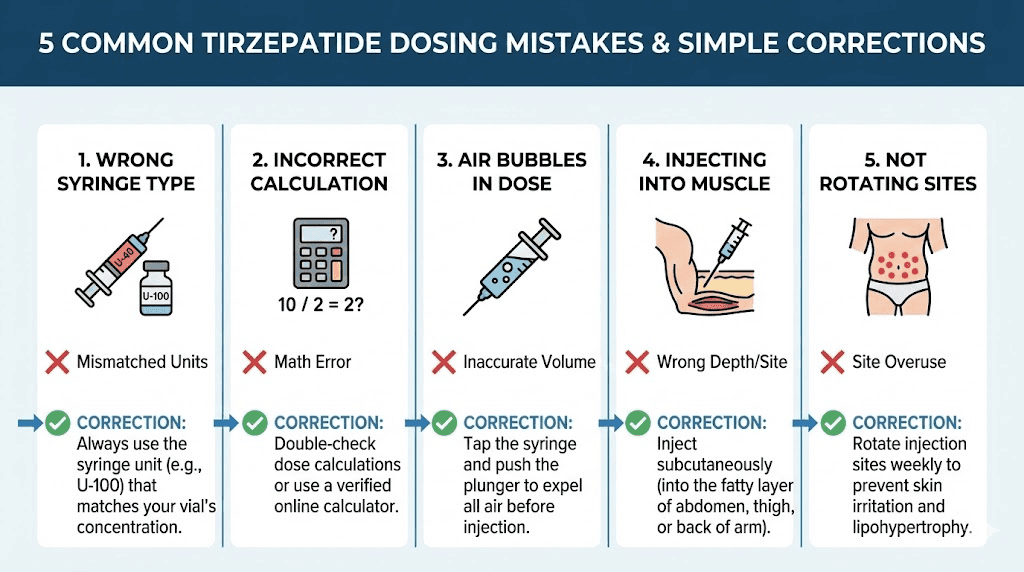
Knowing the formula is necessary. But knowing where people go wrong is equally important. These five mistakes account for the vast majority of compounded tirzepatide dosing errors. Each one is preventable.
Mistake 1: confusing units with milligrams
This is the single most dangerous error. Someone reads "take 2.5 mg" and draws 2.5 units on the syringe. At 10 mg/mL, 2.5 units is only 0.025 mL, delivering 0.25 mg. That is one-tenth of the intended dose.
The reverse is worse. Someone told to "take 25 units" assumes that means 25 mg. At 10 mg/mL, 25 units delivers 2.5 mg. But 25 mg would require 250 units, 2.5 full syringes, and a dangerously high dose that no protocol would prescribe.
Units measure volume. Milligrams measure mass. They are different things measured in different ways.
Mistake 2: not checking concentration on a new vial
You have been drawing 25 units from a 10 mg/mL vial for weeks. Your pharmacy sends a 20 mg/mL vial. You draw 25 units from habit. You just doubled your dose from 2.5 mg to 5 mg without realizing it.
This happens when pharmacies change suppliers, when insurance routes you to a different compounder, or when your provider switches your prescription. Always, every single time, read the mg/mL number on the vial label before calculating. The common peptide mistakes beginners make guide covers this and other critical errors in detail.
Mistake 3: confusing total vial content with concentration
A vial labeled "30 mg / 3 mL" contains 30 mg total in 3 mL of liquid. The concentration is 10 mg/mL. Some people see "30 mg" and use 30 as their concentration number, calculating wildly incorrect unit counts.
Always look for the per-milliliter number. If the label shows only total content and total volume, divide: total mg / total mL = concentration in mg/mL. Your dosage calculator needs the per-milliliter number, not the total.
Mistake 4: using the wrong syringe type
Not all syringes are U-100. A U-40 syringe, designed for U-40 insulin, treats 40 units as 1 mL instead of 100 units as 1 mL. If you use a U-40 syringe and draw to the "25" mark thinking it is 0.25 mL, you actually drew 0.625 mL, 2.5 times more liquid than intended.
Always verify your syringe says "U-100" on the barrel. If there is any doubt, count the total number of unit markings. A U-100 syringe shows 100 units at the 1 mL mark. A U-40 shows 40 units at the 1 mL mark. Proper tools matter as much as proper math in peptide dosing.
Mistake 5: rounding on imprecise syringes
A 1 mL (100-unit) syringe has markings every 2 units. If your calculated dose is 12.5 units, you cannot measure this precisely. You will round to 12 or 14, introducing a 0.5-unit error that translates to real milligrams.
At 20 mg/mL, a 0.5-unit rounding error equals 0.1 mg per injection. Over 4 weeks, that accumulates to 0.4 mg of deviation from your intended protocol. The fix is simple. Use a 0.3 mL or 0.5 mL syringe with 1-unit or 0.5-unit markings when your dose requires fractional units. The smaller syringe gives you the precision that larger syringes cannot. This level of care applies to any peptide injection protocol.
Reconstitution math: when you control the concentration
Some researchers work with lyophilized (freeze-dried) tirzepatide powder rather than pre-mixed liquid vials. In this scenario, you create the concentration yourself by choosing how much bacteriostatic water to add. This gives you control but also adds a critical calculation step before you can use the dosage formula.
The reconstitution formula
Concentration (mg/mL) = Total peptide in vial (mg) / Total bacteriostatic water added (mL)
A 30 mg vial with 3 mL of bacteriostatic water produces 10 mg/mL. The same 30 mg vial with 1.5 mL produces 20 mg/mL. With 6 mL, you get 5 mg/mL. You choose.
Once you know your concentration, the dosage formula works exactly the same way: Units = (dose mg / concentration mg/mL) x 100.
Choosing the right concentration during reconstitution
The ideal concentration depends on your current dose tier and desired precision level. Here is a practical guide.
Your current dose | Recommended concentration | Why |
|---|---|---|
2.5 mg (starting) | 5-10 mg/mL | Larger volume = easier measurement |
5.0 mg | 10 mg/mL | 50 units, clean measurement |
7.5-10 mg | 10-20 mg/mL | Balances precision and volume |
12.5-15 mg | 20-30 mg/mL | Keeps volume under 75 units |
The goal is to land your dose on a unit count that is easy to read on your syringe. Round numbers like 25, 50, and 75 are ideal. Awkward fractions like 16.7 or 33.3 invite measurement error. If possible, choose a concentration that produces clean unit counts for your specific dose.
For a step-by-step walkthrough of the mixing process, see the complete tirzepatide reconstitution guide. The SeekPeptides reconstitution calculator takes your vial size and desired concentration and tells you exactly how much bacteriostatic water to add.
Reconstitution examples with dosage calculations
Example 1: 10 mg vial for starting dose
You have a 10 mg vial. You want 2.5 mg doses. You want each dose to be 25 units for easy measurement.
Work backwards: if 25 units delivers 2.5 mg, then 100 units (1 mL) delivers 10 mg. So you need 10 mg/mL concentration.
Bacteriostatic water needed: 10 mg / 10 mg/mL = 1 mL.
Add 1 mL of bac water. Each 25 units gives you 2.5 mg. The vial contains 4 doses (10 mg total / 2.5 mg per dose).
Example 2: 30 mg vial for escalating doses
You have a 30 mg vial. You are on 5 mg but expect to escalate to 7.5 mg. You want both doses to produce clean unit counts.
At 10 mg/mL: 5 mg = 50 units, 7.5 mg = 75 units. Both clean numbers.
Bacteriostatic water: 30 mg / 10 mg/mL = 3 mL.
Add 3 mL. The vial holds 6 doses at 5 mg or 4 doses at 7.5 mg. For information on how much bacteriostatic water to add to peptides generally, our mixing guide covers proper technique.
Example 3: 60 mg vial for maximum dose
You have a 60 mg vial. You take 15 mg weekly. You want small injection volume.
At 30 mg/mL: 15 mg = 50 units. Clean, comfortable, half a syringe.
Bacteriostatic water: 60 mg / 30 mg/mL = 2 mL.
Add 2 mL. The vial holds 4 weekly doses. Total duration: 4 weeks before needing a new vial. Understanding how long tirzepatide lasts in the fridge becomes critical when each vial covers a month of dosing.
The complete dose escalation schedule with exact unit counts
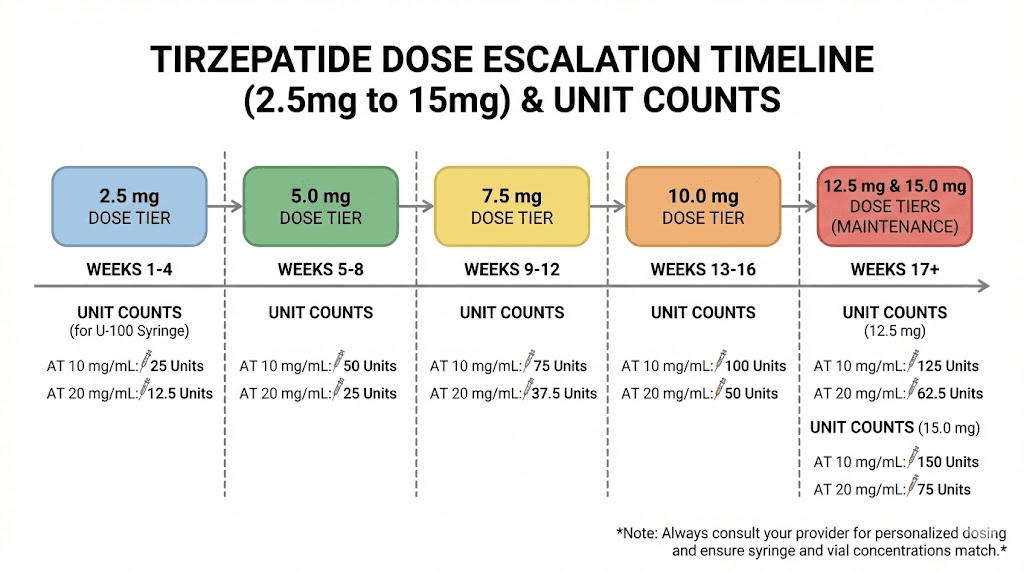
Tirzepatide follows a structured escalation schedule developed through clinical trials. The SURMOUNT program established the protocol: start at 2.5 mg weekly, hold for 4 weeks minimum, then increase by 2.5 mg increments. Here is that schedule with exact unit counts for every common concentration.
Standard escalation at 10 mg/mL
Weeks | Dose | Units | Notes |
|---|---|---|---|
1-4 | 2.5 mg | 25 units | Tolerance assessment |
5-8 | 5.0 mg | 50 units | First therapeutic dose |
9-12 | 7.5 mg | 75 units | Enhanced effect |
13-16 | 10.0 mg | 100 units | Full syringe, consider higher concentration |
17-20 | 12.5 mg | N/A | Exceeds 1 mL syringe, switch to 20 mg/mL |
21+ | 15.0 mg | N/A | Requires higher concentration |
At 10 mg/mL, you hit the syringe limit at 10 mg. Any dose above requires either a second injection, a larger syringe, or, most practically, a switch to a higher concentration. This is the natural point where most researchers transition to 20 mg/mL vials.
Standard escalation at 20 mg/mL
Weeks | Dose | Units | Notes |
|---|---|---|---|
1-4 | 2.5 mg | 12.5 units | Fractional, use precise syringe |
5-8 | 5.0 mg | 25 units | Clean measurement |
9-12 | 7.5 mg | 37.5 units | Fractional, use precise syringe |
13-16 | 10.0 mg | 50 units | Clean measurement |
17-20 | 12.5 mg | 62.5 units | Fractional |
21+ | 15.0 mg | 75 units | Clean, comfortable volume |
At 20 mg/mL, every dose tier fits in a single syringe with room to spare. The trade-off is fractional units at some dose levels (12.5, 37.5, 62.5), which require a 0.3 mL or 0.5 mL syringe with 1-unit markings for accuracy.
The SURMOUNT-1 trial showed weight loss of 15% at 5 mg, 21.4% at 10 mg, and 22.5% at 15 mg over 72 weeks. Reaching those higher doses requires disciplined escalation and accurate dosing at every step. Rushing the escalation or miscalculating doses increases side effect severity without improving outcomes. Understanding how fast tirzepatide works helps set realistic expectations for each escalation phase.
When to hold at a dose tier
Not everyone needs to reach 15 mg. The clinical trials found meaningful weight loss at every dose tier. If you are losing weight consistently at 5 mg with manageable side effects, there may be no reason to escalate further. Higher doses produce more weight loss on average, but they also produce more gastrointestinal side effects.
Hold at your current dose if:
You are losing 1-2 pounds per week consistently
Side effects are mild and manageable
Appetite suppression feels effective
Your provider recommends maintaining the current level
Escalate if:
Weight loss has plateaued for 4+ weeks despite dietary compliance
Appetite suppression has noticeably decreased
Your provider recommends the next tier
You have tolerated the current dose well for the minimum hold period
If you find yourself stalling, our guide on why you are not losing weight on tirzepatide covers every potential factor beyond just dose adjustment.
Verification system: catching errors before they reach your body
Knowing the formula is not enough. You need a system that catches errors before they become injections. This three-step verification process takes less than 60 seconds and has prevented more dosing mistakes than any calculator alone.
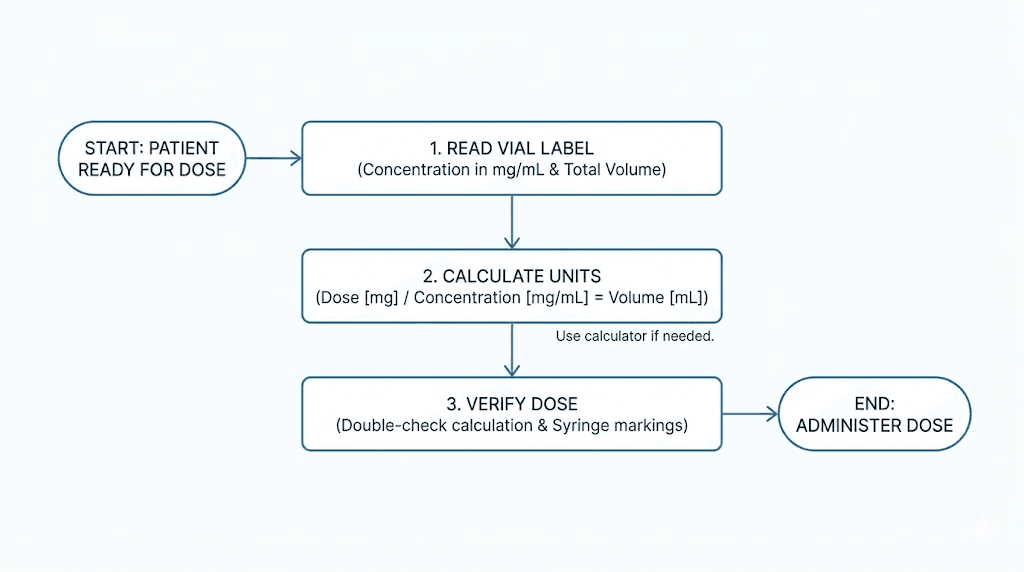
Step 1: the label check
Before any calculation, read your vial label completely. Find three pieces of information:
1. Compound name: Confirm it says tirzepatide (not semaglutide, not something else)
2. Concentration: Find the mg/mL number (this is your calculation input)
3. Expiration date: Confirm the vial is not expired or past its beyond-use date
If any of these are unclear, missing, or surprising, stop. Contact your pharmacy. The FDA has flagged compounded products with labeling errors, including wrong concentrations and misspellings that indicate quality control issues.
Step 2: the double calculation
Calculate your dose using the formula. Then immediately verify by working backwards.
Forward: Units = (dose mg / concentration mg/mL) x 100
Backward: Dose mg = (units / 100) x concentration mg/mL
If the backward calculation matches your intended dose, your math is correct. If it does not match, you made an error somewhere. Find it before proceeding.
Example: You want 5 mg from a 20 mg/mL vial.
Forward: (5 / 20) x 100 = 25 units.
Backward: (25 / 100) x 20 = 5 mg. Confirmed.
This takes 10 seconds. It prevents catastrophic errors. Make it automatic. This same verification approach applies to any peptide dosage calculation.
Step 3: the visual reasonability check
After drawing your dose, look at the syringe. Does the volume look reasonable compared to previous doses?
If you normally draw 25 units and today you calculated 50 units for the same dose, something changed. Maybe the vial concentration is different. Maybe you made a math error. Either way, stop and verify before injecting.
If the syringe looks nearly empty (under 10 units) for what should be a standard dose, question it. If it is nearly full (over 80 units) when it usually is not, question it. Your eyes are a sanity check that catches errors your math missed.
How the SeekPeptides calculator handles these calculations
SeekPeptides designed its calculator tools specifically for compounded peptide dosing. The platform addresses every step in the calculation chain, from reconstitution to final syringe units.
The peptide dosage calculator
Enter your desired dose in milligrams and your vial concentration in mg/mL. The peptide dosage calculator outputs your exact syringe units. No formula memorization needed. No arithmetic errors possible. It handles tirzepatide, semaglutide, retatrutide, and any other injectable compound.
The reconstitution calculator
For lyophilized powder: enter your vial size in milligrams and desired concentration. The reconstitution calculator tells you exactly how much bacteriostatic water to add. Then the dosage calculator converts your resulting concentration to syringe units for any dose.
The cost calculator
Comparing vials at different concentrations? The peptide cost calculator normalizes pricing to cost-per-milligram, the only fair comparison metric. A cheaper vial is not actually cheaper if it contains fewer total milligrams of active compound.
Beyond the calculators, SeekPeptides members access comprehensive protocol guides, detailed dosing guides, storage instructions, and a community of experienced researchers who have navigated every dosing scenario this guide covers.
Switching concentrations safely
Concentration changes are inevitable. Your pharmacy may alter their formulation. You might switch providers. Or you may intentionally move to a higher concentration as your dose increases. Every transition requires fresh calculations.
The golden rule
Always recalculate from milligrams. Never try to convert directly from old units to new units.
Wrong: "I was taking 50 units, my new vial is twice the concentration, so I will take 25 units." This shortcut works mathematically but introduces error if you misremember your old concentration or your new vial is not exactly twice.
Right: "My dose is 5 mg. My new vial is 20 mg/mL. Units = (5/20) x 100 = 25 units." Start from the dose. Always.
This principle applies whether you are changing tirzepatide concentrations or switching between different GLP-1 compounds entirely. The semaglutide to tirzepatide conversion chart covers cross-compound switching in detail.
Concentration switch checklist
Use this every time you start a new vial:
1. Read the new vial label. Write down the concentration.
2. Compare to your previous vial. Same or different?
3. If different, recalculate units from your milligram dose.
4. Verify with the backward calculation.
5. Draw the dose and do the visual reasonability check.
6. Log the new concentration and unit count in your dosing journal.
This process takes one minute. It prevents the most common source of compounded tirzepatide overdoses.
Syringe selection and measurement precision
The syringe you choose directly impacts how accurately you can measure your calculated dose. Not all syringes offer the same precision, and using the wrong one can introduce meaningful errors.
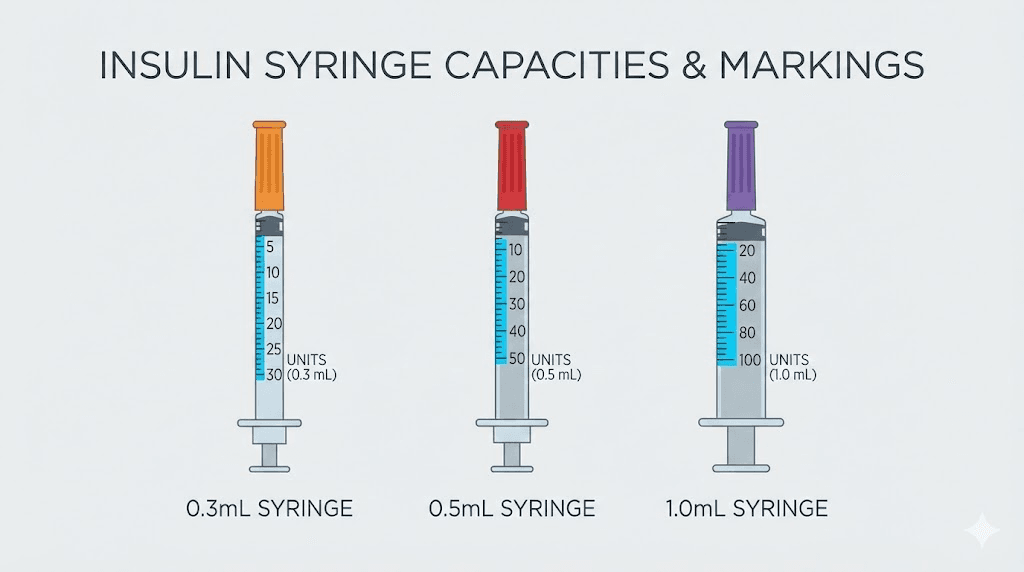
U-100 syringe sizes and their precision
0.3 mL (30 units max): Each line represents 0.5 or 1 unit. Best precision for doses under 30 units. Ideal for starting doses at higher concentrations (20+ mg/mL) and microdosing protocols. This is the most accurate option for small-volume doses.
0.5 mL (50 units max): Each line represents 1 unit. Good precision for most compounded tirzepatide doses. Handles starting through moderate doses comfortably. The sweet spot for researchers using 10-20 mg/mL concentrations.
1.0 mL (100 units max): Each line represents 2 units. Adequate for larger doses (50+ units) but imprecise for small doses. If your calculated dose falls between the 2-unit markings, you cannot measure it accurately on this syringe. Use a smaller syringe instead.
Matching syringe to concentration
Concentration | Starting dose units | Best syringe |
|---|---|---|
5 mg/mL | 50 units | 0.5 mL or 1.0 mL |
10 mg/mL | 25 units | 0.3 mL or 0.5 mL |
20 mg/mL | 12.5 units | 0.3 mL |
30 mg/mL | 8.3 units | 0.3 mL |
40 mg/mL | 6.25 units | 0.3 mL |
The pattern is clear. As concentration increases, starting dose volume decreases, and syringe precision becomes more critical. At 40 mg/mL, the starting 2.5 mg dose requires only 6.25 units. Even on a 0.3 mL syringe with 0.5-unit markings, this is challenging to measure precisely. This is another reason why matching concentration to dose tier matters for getting started with peptides safely.
Reading the meniscus correctly
Liquid in a syringe curves at the surface. This curve is called the meniscus. Always read the dose at the bottom of the meniscus, not the top of the curve. Reading from the top adds 0.5-1 unit of error.
Hold the syringe at eye level. Look straight across. The flat bottom of the liquid surface should align with your target unit marking. This technique sounds basic, but it prevents a consistent source of small errors that compound over weeks of dosing.
Storage factors that affect your calculated dose accuracy
Your dosage calculation assumes full potency. But tirzepatide degrades over time and under improper conditions. A vial that has lost 20% of its potency means your calculated 5 mg dose actually delivers closer to 4 mg of active compound. The math was right. The chemistry changed.
Temperature requirements
Reconstituted tirzepatide must be stored at 36-46 degrees Fahrenheit (2-8 degrees Celsius). Standard refrigerator temperature. Room temperature accelerates degradation. Heat destroys it. Freezing can damage the peptide structure.
If your vial sat on the counter for a few hours, it is likely fine. If it spent a full day or more at room temperature, potency may be compromised. For detailed guidance, see does tirzepatide need to be refrigerated and how long compounded tirzepatide can be out of the fridge.
Beyond-use dating
Most compounding pharmacies assign a 28-42 day beyond-use date for reconstituted tirzepatide. After this date, potency is not guaranteed. Using a vial past its beyond-use date means your dosage calculator gave you a number based on full potency, but the vial may deliver less.
Track your reconstitution dates. Write them on the vial. Plan your vial sizes so you finish each one within the beyond-use window. General peptide storage principles apply universally.
Signs your vial has degraded
Clear liquid does not guarantee potency. But visible changes guarantee problems. Never use tirzepatide that shows cloudiness, floating particles, color change, or unusual thickness. These indicate breakdown products.
If your results have been declining despite consistent dosing and good compliance, degraded peptide is a possible explanation. Consider whether your vial has been stored properly and whether it is within its use window. Understanding whether peptides expire and what happens when they do is essential knowledge.
Comparing tirzepatide dosage calculations to semaglutide
Many researchers transition between tirzepatide and semaglutide or use both sequentially. The dosage calculation formula is identical for both compounds. But the clinical doses are dramatically different because these are different molecules with different potencies.
Same math, different dose ranges
The formula Units = (mg / concentration) x 100 works for both. But tirzepatide doses range from 2.5 to 15 mg weekly, while semaglutide doses range from 0.25 to 2.4 mg weekly. A 10-fold difference in dosing scale.
At 10 mg/mL concentration, the tirzepatide starting dose of 2.5 mg requires 25 units. The semaglutide starting dose of 0.25 mg requires just 2.5 units, an almost immeasurably small volume on most syringes. This is why semaglutide typically comes in much lower concentrations than tirzepatide.
Compound | Starting dose | Maximum dose | Typical concentration |
|---|---|---|---|
Tirzepatide | 2.5 mg | 15 mg | 10-30 mg/mL |
Semaglutide | 0.25 mg | 2.4 mg | 1-5 mg/mL |
Retatrutide | 1.0 mg | 12 mg | 5-20 mg/mL |
If you are switching compounds, do not assume similar unit counts deliver similar effects. The tirzepatide vs semaglutide dosage chart details the equivalency considerations. For the semaglutide 5 mg/mL dosage chart specifically, our dedicated guide covers every semaglutide concentration.
Why you cannot convert tirzepatide units to semaglutide units
Twenty-five units of tirzepatide at 10 mg/mL delivers 2.5 mg of tirzepatide. Twenty-five units of semaglutide at 1 mg/mL delivers 0.25 mg of semaglutide. Same unit count. Same syringe marking. Completely different compounds at completely different doses.
Beyond the volume math, the pharmacological equivalence is complex. In the SURPASS-2 trial, tirzepatide 5 mg outperformed semaglutide 1 mg for weight loss, but these are not "equivalent" doses. They are different drugs with different mechanisms. Tirzepatide is a dual GIP/GLP-1 receptor agonist. Semaglutide targets only GLP-1 receptors. The retatrutide vs semaglutide comparison shows how triple-agonist compounds add even more complexity.
Never convert between compounds using unit-to-unit ratios. Always work with milligram doses prescribed by your provider for each specific compound.
Tracking your doses: the dosing journal approach
A dosing journal does not just help you remember what you took. It creates a verifiable record that catches patterns, identifies errors, and provides data for optimizing your protocol.
What to log for every injection
1. Date and time of injection
2. Vial concentration (mg/mL)
3. Calculated units drawn
4. Milligrams the units represent
5. Injection site (rotate sites systematically)
6. Vial number and reconstitution date
7. Side effects (if any, note severity and duration)
8. Weight (weekly, same day, same conditions)
Why logging prevents errors
When you write down your concentration every week, you will notice immediately if a new vial has a different number. When you log your units, you create a comparison point that flags unusual calculations. When you track side effects alongside doses, you can see whether a dose change caused new symptoms or whether symptoms resolve at the current tier.
This data is also invaluable if you ever need to discuss your protocol with a healthcare provider. Instead of saying "I think I was taking about 7.5 mg," you can show exact records. Precision in documentation mirrors precision in peptide cycle planning.
Special dosing scenarios
Not every situation fits the standard escalation model. Here are calculation approaches for common special scenarios that the basic formula handles once you know how to apply it.
Splitting doses
Some researchers split their weekly dose into two injections (every 3.5 days) to maintain more stable blood levels and reduce side effect peaks. The calculation is identical: just divide your weekly milligram dose by two and calculate units for the half-dose.
Weekly 5 mg split into twice weekly at 10 mg/mL: Each injection = 2.5 mg = 25 units. Simple.
Weekly 10 mg split into twice weekly at 20 mg/mL: Each injection = 5 mg = 25 units. Same syringe reading, different total weekly dose. This is why tracking milligrams, not units, matters for protocol consistency.
Missed dose recovery
If you miss a dose and it has been fewer than 4 days since your scheduled injection, take it immediately. Calculate your normal dose. No changes to the math.
If more than 4 days have passed, skip the missed dose. Take your normal dose at the next scheduled time. Do not double up. Never inject two doses to "catch up." Doubling dramatically increases side effect risk and provides no additional therapeutic benefit. Understanding how long tirzepatide takes to work helps put a single missed dose into perspective, it will not derail your progress.
Sub-therapeutic microdosing
Some researchers start below the 2.5 mg tier to assess tolerance, especially if they are sensitive to fatigue, anxiety, or gastrointestinal effects from new medications.
Common microdoses and their calculations at 10 mg/mL:
1.0 mg = 10 units
1.25 mg = 12.5 units
1.5 mg = 15 units
2.0 mg = 20 units
The microdosing tirzepatide chart covers detailed sub-therapeutic protocols and escalation schedules from micro to standard doses.
Transitioning from brand-name pens to compounded vials
If you previously used Mounjaro or Zepbound pens and are switching to compounded vials, the milligram dose should remain the same. Only the delivery method changes.
Was on Mounjaro 5 mg pen? Calculate 5 mg from your compounded vial. At 10 mg/mL: 50 units. At 20 mg/mL: 25 units.
The key difference is injection technique. Pens are spring-loaded auto-injectors. Vials require manual syringe injection. Our injection technique guide covers proper subcutaneous injection with syringes. For a broader look at compounded formulations, see the compounded tirzepatide guide.
Advanced topics: combining tirzepatide with other compounds
Some researchers combine tirzepatide with complementary compounds. Each compound requires its own separate dosage calculation. Never mix compounds in the same syringe unless specifically formulated together by a compounding pharmacy.
Tirzepatide with B12
Some compounding pharmacies combine tirzepatide with cyanocobalamin (vitamin B12) in the same vial. The concentration listed on the label refers to the tirzepatide component. B12 does not change your tirzepatide dosage calculation, it is along for the ride at whatever volume you draw.
If your vial says "Tirzepatide 10 mg/mL with B12 1 mg/mL" and you draw 25 units for your 2.5 mg tirzepatide dose, you automatically receive 0.25 mg of B12 in the same injection. No additional math needed. See the tirzepatide with B12 guide for detailed protocol information.
Tirzepatide with glycine
Similarly, some formulations include glycine as a stabilizer or buffer. The glycine does not affect your tirzepatide calculation. Use the tirzepatide mg/mL concentration for all dosage math. Our tirzepatide glycine guide explains the rationale behind this combination.
Tirzepatide with niacinamide
Niacinamide is another additive found in some compounded tirzepatide formulations. As with B12 and glycine, it does not change your tirzepatide dosage calculation. Draw your calculated units based on the tirzepatide concentration. The tirzepatide niacinamide guide covers the science behind this formulation approach.
Separate compound stacking
If you use tirzepatide alongside other peptides like BPC-157, TB-500, or other compounds, each one gets its own calculation, its own syringe, and its own injection. Never combine vials. The peptide stack calculator helps manage multi-compound protocols.
What to do if you make a dosing error
Despite every precaution, errors happen. Here is what to do depending on the type and severity of the mistake.
Overdose (took more than intended)
The most common symptoms are gastrointestinal: severe nausea, vomiting, diarrhea, and abdominal pain. These can be intense but are typically self-limiting within 24-48 hours.
Mild overdose (1.5-2x intended dose):
Stay hydrated with electrolyte solutions
Eat small, bland meals
Skip the next scheduled dose
Resume normal dosing at the following scheduled time
Severe overdose (3x+ intended dose):
Monitor for signs of severe dehydration
Watch for hypoglycemia (shakiness, confusion, sweating)
Seek medical attention if symptoms are severe or worsening
Bring your vial to the ER so providers know the exact concentration
The FDA case of a patient hospitalized in the ICU after unsupervised dose escalation underscores the seriousness of significant dosing errors.
Underdose (took less than intended)
Less dangerous but undermines your protocol. If you realize within a few hours, you can administer the remaining units as a separate injection. If you realize the next day, accept the lower dose for that week and resume normally at the next scheduled injection. Do not add extra to compensate.
Preventing future errors
After any dosing error:
1. Document what happened (wrong concentration, wrong unit count, wrong syringe)
2. Identify the root cause
3. Add a check to your verification process that would have caught it
4. Consider switching to a concentration that produces cleaner unit counts
5. Use the SeekPeptides calculator as a verification step going forward
Frequently asked questions
How do I calculate my compounded tirzepatide dose in units?
Use this formula: Units = (desired dose in mg / vial concentration in mg/mL) x 100. For example, 2.5 mg from a 10 mg/mL vial: (2.5 / 10) x 100 = 25 units. The peptide dosage calculator can verify your math instantly.
Why do different compounding pharmacies use different concentrations?
Pharmacies choose concentrations based on common dose ranges and practical considerations. Lower concentrations (5-10 mg/mL) offer better precision for starting doses. Higher concentrations (20-50 mg/mL) reduce injection volume for patients on elevated doses. Some pharmacies offer multiple concentrations and recommend specific ones based on your prescribed dose tier.
Can I use the same syringe for different tirzepatide concentrations?
Yes, U-100 insulin syringes work with any concentration. The syringe measures volume, not concentration. However, the number of units you draw changes based on concentration. Always recalculate when switching vials. A 0.3 mL syringe with 1-unit markings provides the best precision for high-concentration vials.
What if my calculated dose falls between syringe markings?
Switch to a smaller syringe with finer markings. A 0.3 mL syringe has 0.5 or 1-unit markings that let you measure fractional units precisely. If even that is not precise enough, consider adjusting your reconstitution to produce a concentration that gives you clean unit counts for your dose.
Is there a maximum number of units I should draw from one vial?
A standard 1 mL U-100 syringe holds 100 units maximum. If your dose requires more than 100 units, you either need a higher concentration vial or must split the dose between two syringes. Most researchers switch to a higher concentration before reaching this point.
How do I know if my compounding pharmacy changed my concentration?
Check the label on every new vial. The mg/mL number should be clearly printed. If it differs from your previous vial, recalculate your units before injecting. If the label is unclear, contact the pharmacy directly. Never guess at concentration.
Should I use a dosage calculator or do the math myself?
Both. Calculate manually first to understand the math, then verify with a calculator to catch arithmetic errors. This dual approach catches mistakes that either method alone might miss. The goal is confidence in every measurement.
How many doses are in one compounded tirzepatide vial?
Divide the total milligrams in the vial by your weekly milligram dose. A 50 mg vial at 2.5 mg weekly = 20 doses (20 weeks). At 10 mg weekly = 5 doses (5 weeks). Factor in beyond-use dating, as the vial must be used within 28-42 days of reconstitution regardless of remaining content.
External resources
For researchers committed to getting every calculation right from the start, SeekPeptides provides the most comprehensive resource available, with precision calculators, evidence-based protocols, detailed dosing guides, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay precise, your concentrations stay verified, and your protocols stay consistent.