Feb 14, 2026

Drawing 50 units from the wrong concentration vial could mean injecting double your intended dose. Or half. That single math error, made with a perfectly good syringe and perfectly good tirzepatide, sends more researchers back to square one than almost any other mistake in peptide protocols. The difference between 2.5 mg and 10 mg at 50 units on your syringe comes down to one number printed on your vial label. Miss it, and everything downstream goes wrong.
The confusion is understandable. Insulin syringes measure in units. Tirzepatide vials list concentrations in mg/mL. Your prescriber writes doses in milligrams. Three different measurement systems converging on one tiny syringe, and you are expected to translate between them without error. Every single time. For researchers working with compounded tirzepatide, this math becomes even more critical because vial concentrations vary widely between pharmacies.
Here is what 50 units actually delivers at each common concentration, how to verify your math before every injection, and the conversion framework that eliminates guesswork permanently. Whether you are working with tirzepatide dosing in units for the first time or switching between concentrations, this guide covers every scenario you will encounter.
SeekPeptides built this resource because dosing accuracy is not optional. It is the foundation of every successful protocol.
The quick answer: 50 units of tirzepatide in milligrams
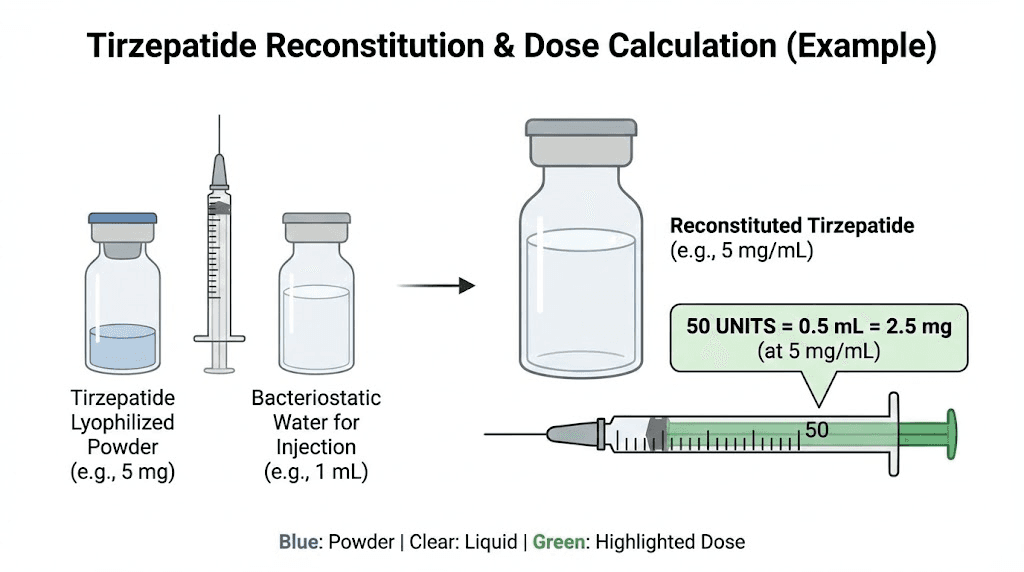
Fifty units on an insulin syringe equals 0.5 mL of liquid. Always. Regardless of what is dissolved in that liquid. That part never changes.
What changes is how many milligrams of tirzepatide live inside that 0.5 mL. The concentration of your vial determines everything.
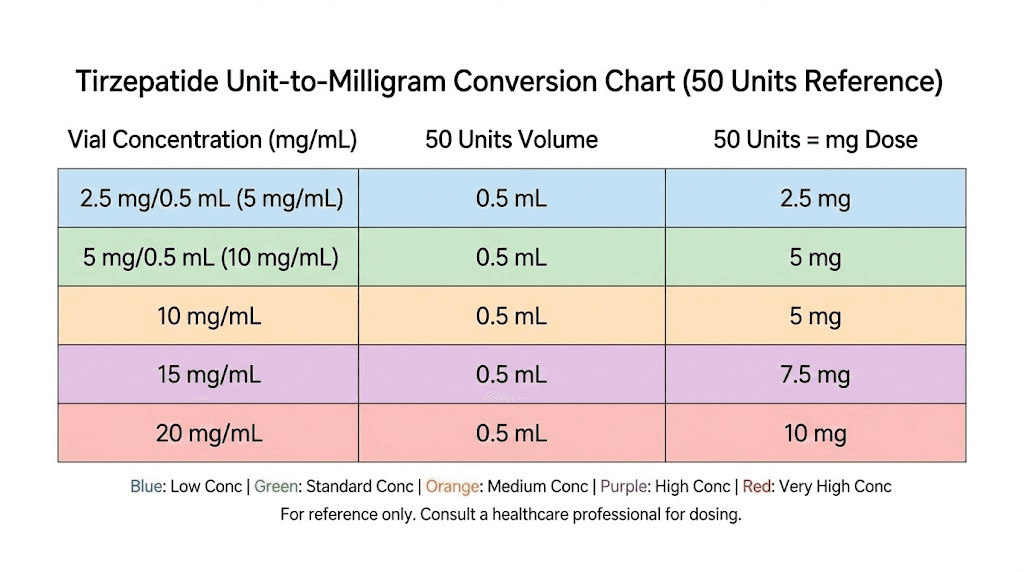
Here is the breakdown for every common tirzepatide concentration you will encounter:
Vial concentration | 50 units (0.5 mL) delivers | Common source |
|---|---|---|
5 mg/mL | 2.5 mg | Some compounding pharmacies, lower-dose vials |
10 mg/mL | 5.0 mg | Most common compounded concentration |
15 mg/mL | 7.5 mg | Higher-concentration compounded vials |
20 mg/mL | 10.0 mg | High-concentration compounded vials |
30 mg/mL | 15.0 mg | Ultra-concentrated compounded vials |
40 mg/mL | 20.0 mg | Maximum concentration compounded vials |
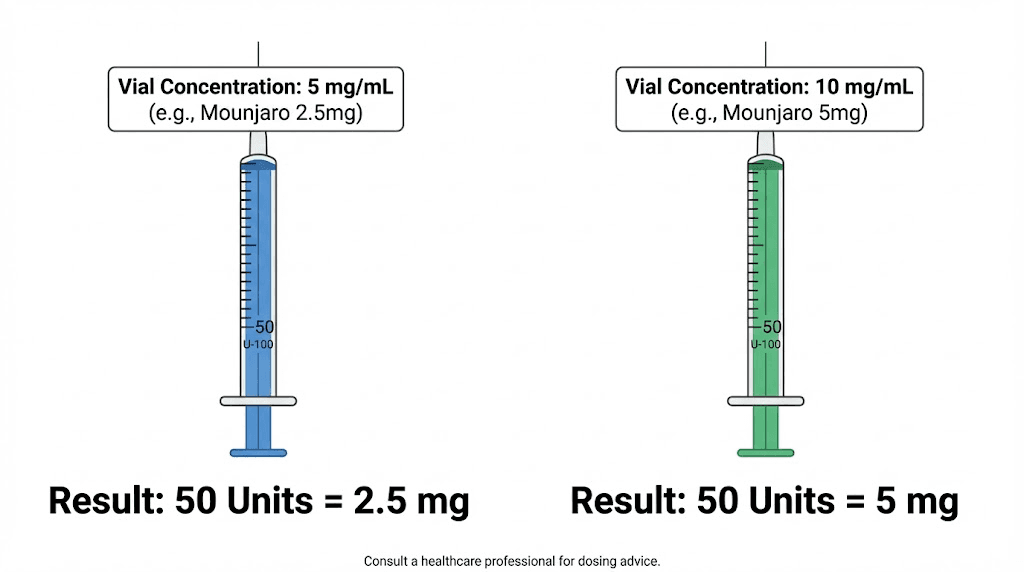
Read that table carefully. At 5 mg/mL, 50 units gives you a gentle 2.5 mg starting dose. At 20 mg/mL, those same 50 units deliver 10 mg, which is a full therapeutic dose reserved for advanced titration phases. Same syringe mark. Wildly different outcomes.
If you are working with standard 2.5 mg tirzepatide doses, 50 units only gives you that amount at 5 mg/mL concentration. At 10 mg/mL, you would need just 25 units for 2.5 mg.
Why the answer depends entirely on your vial concentration
Units on an insulin syringe measure volume. Not drug content. Not potency. Volume.
One hundred units equals 1 mL. Fifty units equals 0.5 mL. Twenty-five units equals 0.25 mL. This ratio never changes regardless of what liquid fills the syringe. Water, saline, tirzepatide at any concentration, it does not matter. The syringe measures how much liquid you draw, nothing more.
Concentration tells you how much active tirzepatide the pharmacy dissolved into each milliliter. A 10 mg/mL vial contains 10 milligrams of tirzepatide in every single milliliter of solution. A 5 mg/mL vial contains half that amount in the same volume of liquid. The tirzepatide molecules are more diluted, spread across more solvent.
This distinction matters enormously for tirzepatide dosage calculations.
Think of it like coffee. A shot of espresso and a full mug of drip coffee might both contain 100 mg of caffeine. But the espresso concentrates that caffeine into 30 mL while the drip coffee spreads it across 350 mL. Drawing 50 mL from the espresso gives you far more caffeine than drawing 50 mL from the drip coffee.
Tirzepatide works the same way.
Your pharmacy chooses the concentration when they compound the vial. Some use 5 mg/mL. Others prefer 10 mg/mL. Higher volume clinics sometimes use 20 mg/mL or even 40 mg/mL to minimize injection volume and maximize doses per vial. Each choice is legitimate. Each changes what 50 units delivers.
The concentration is always printed on your vial
Every compounding pharmacy labels the vial with the concentration. Look for the mg/mL number. It might read "Tirzepatide 10 mg/mL" or "Tirzepatide 5 mg/mL" or any other value. This single number determines your entire dosing math.
If you cannot find it, do not inject. Contact your pharmacy.
For researchers working with reconstituted tirzepatide from lyophilized powder, you determine the concentration yourself based on how much bacteriostatic water you add. A 10 mg vial reconstituted with 1 mL of bacteriostatic water creates 10 mg/mL. The same vial reconstituted with 2 mL creates 5 mg/mL. Your choice, your math, your responsibility.
The universal conversion formula
One formula handles every concentration, every dose, every syringe. Learn it once and you never need a chart again.
To find milligrams from units:
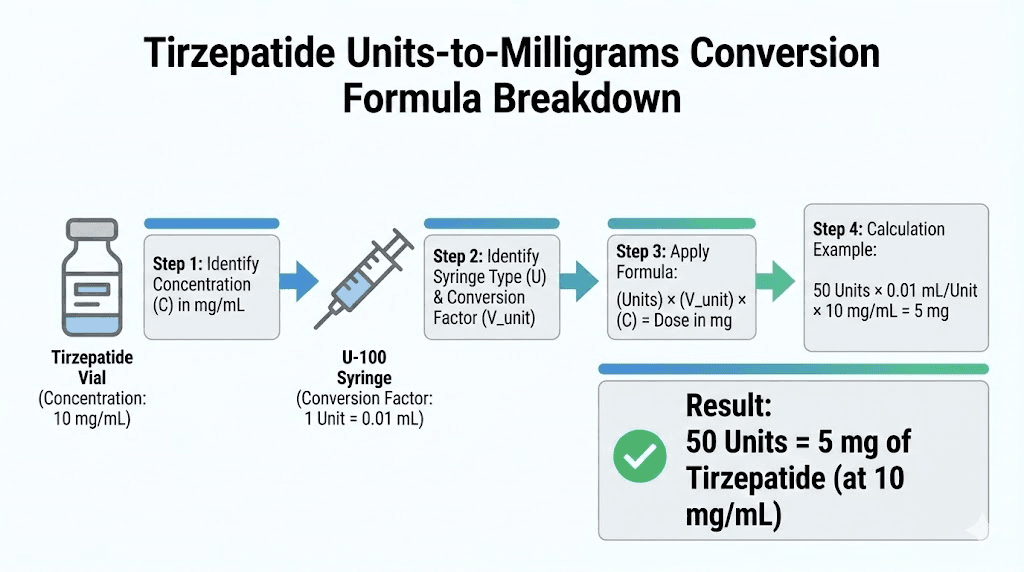
mg = (units / 100) x concentration in mg/mL
For 50 units at 10 mg/mL:
mg = (50 / 100) x 10 = 0.5 x 10 = 5.0 mg
For 50 units at 5 mg/mL:
mg = (50 / 100) x 5 = 0.5 x 5 = 2.5 mg
For 50 units at 20 mg/mL:
mg = (50 / 100) x 20 = 0.5 x 20 = 10.0 mg
Simple. The formula works because 100 units always equals 1 mL on a standard U-100 insulin syringe. Dividing by 100 converts units to milliliters. Multiplying by concentration converts milliliters to milligrams.
To find units from milligrams (the reverse):
units = (desired mg / concentration in mg/mL) x 100
Want 5 mg from a 10 mg/mL vial?
units = (5 / 10) x 100 = 0.5 x 100 = 50 units
Want 2.5 mg from a 10 mg/mL vial?
units = (2.5 / 10) x 100 = 0.25 x 100 = 25 units
Want 7.5 mg from a 10 mg/mL vial?
units = (7.5 / 10) x 100 = 0.75 x 100 = 75 units
These formulas replace memorization with understanding. Once you grasp that units measure volume and concentration determines potency, the math becomes intuitive. For a quick check, you can always use the SeekPeptides peptide calculator to verify your numbers before drawing.
Practice problems to build confidence
Before your next injection, try these. Calculate first, then check against the answers below.
Problem 1: You have a 20 mg/mL vial and need 7.5 mg. How many units?
Problem 2: You drew 30 units from a 10 mg/mL vial. How many mg did you draw?
Problem 3: Your pharmacy switched you from 5 mg/mL to 10 mg/mL. You were drawing 50 units. What should you draw now for the same dose?
Problem 4: You need 12.5 mg from a 25 mg/mL vial. How many units?
Answers:
Problem 1: (7.5 / 20) x 100 = 37.5 units
Problem 2: (30 / 100) x 10 = 3.0 mg
Problem 3: You were getting (50 / 100) x 5 = 2.5 mg. At 10 mg/mL: (2.5 / 10) x 100 = 25 units. Draw half as much.
Problem 4: (12.5 / 25) x 100 = 50 units
Complete conversion charts for every common concentration
While the formula handles any scenario, reference charts speed up daily protocol execution. Print these out, tape them to your refrigerator door, or save them on your phone. Having a visual reference for tirzepatide dosing prevents the most common measurement errors.
5 mg/mL conversion chart
This concentration is common in lower-dose compounded vials and some research-grade preparations. Each unit delivers relatively less tirzepatide, making it easier to measure small doses with precision.
Units drawn | mL volume | mg of tirzepatide |
|---|---|---|
10 units | 0.10 mL | 0.5 mg |
15 units | 0.15 mL | 0.75 mg |
20 units | 0.20 mL | 1.0 mg |
25 units | 0.25 mL | 1.25 mg |
30 units | 0.30 mL | 1.5 mg |
40 units | 0.40 mL | 2.0 mg |
50 units | 0.50 mL | 2.5 mg |
60 units | 0.60 mL | 3.0 mg |
75 units | 0.75 mL | 3.75 mg |
100 units | 1.00 mL | 5.0 mg |
At this concentration, microdosing tirzepatide becomes straightforward. Even 10 units delivers a measurable 0.5 mg, and the larger injection volumes make small adjustments easier to see on the syringe.
10 mg/mL conversion chart
The most widely used concentration for compounded tirzepatide. Most pharmacies default to this because it balances precision with reasonable injection volumes. If your vial does not specify otherwise, 10 mg/mL is the most likely concentration.
Units drawn | mL volume | mg of tirzepatide |
|---|---|---|
5 units | 0.05 mL | 0.5 mg |
10 units | 0.10 mL | 1.0 mg |
15 units | 0.15 mL | 1.5 mg |
20 units | 0.20 mL | 2.0 mg |
25 units | 0.25 mL | 2.5 mg |
30 units | 0.30 mL | 3.0 mg |
40 units | 0.40 mL | 4.0 mg |
50 units | 0.50 mL | 5.0 mg |
60 units | 0.60 mL | 6.0 mg |
75 units | 0.75 mL | 7.5 mg |
100 units | 1.00 mL | 10.0 mg |
At 10 mg/mL, 50 units delivers exactly 5.0 mg. This is the second tirzepatide dosing tier in standard titration protocols, typically reached after four weeks at 2.5 mg. The math works out cleanly, which is one reason pharmacies prefer this concentration.
20 mg/mL conversion chart
Higher concentration vials reduce injection volume, which many researchers prefer for comfort. However, precision becomes more critical because small measurement errors translate to larger dose differences.
Units drawn | mL volume | mg of tirzepatide |
|---|---|---|
5 units | 0.05 mL | 1.0 mg |
10 units | 0.10 mL | 2.0 mg |
12.5 units | 0.125 mL | 2.5 mg |
15 units | 0.15 mL | 3.0 mg |
20 units | 0.20 mL | 4.0 mg |
25 units | 0.25 mL | 5.0 mg |
37.5 units | 0.375 mL | 7.5 mg |
50 units | 0.50 mL | 10.0 mg |
62.5 units | 0.625 mL | 12.5 mg |
75 units | 0.75 mL | 15.0 mg |
Notice the precision challenge. At 20 mg/mL, the difference between 12.5 units and 25 units is the difference between 2.5 mg and 5.0 mg. That is a full dose tier in just 12.5 units of syringe movement. Researchers using this concentration should strongly consider using a 0.3 mL insulin syringe (30 units max) for low doses, where each tick mark represents a smaller volume and allows finer control.
30 mg/mL and 40 mg/mL conversion charts
These ultra-concentrated formulations exist primarily for researchers on higher maintenance doses who want minimal injection volume. They are less common but worth understanding if your pharmacy supplies them.
30 mg/mL:
Units drawn | mL volume | mg of tirzepatide |
|---|---|---|
8.3 units | 0.083 mL | 2.5 mg |
16.7 units | 0.167 mL | 5.0 mg |
25 units | 0.25 mL | 7.5 mg |
33.3 units | 0.333 mL | 10.0 mg |
50 units | 0.50 mL | 15.0 mg |
40 mg/mL:
Units drawn | mL volume | mg of tirzepatide |
|---|---|---|
6.25 units | 0.0625 mL | 2.5 mg |
12.5 units | 0.125 mL | 5.0 mg |
18.75 units | 0.1875 mL | 7.5 mg |
25 units | 0.25 mL | 10.0 mg |
50 units | 0.50 mL | 20.0 mg |
At 40 mg/mL, 50 units delivers a massive 20.0 mg. This is well beyond standard dosing protocols. These concentrations demand extreme care. A two-unit error at 40 mg/mL changes your dose by 0.8 mg. At 5 mg/mL, that same two-unit error changes your dose by only 0.1 mg. Higher concentration means higher consequences for measurement mistakes.
Understanding insulin syringes and how they measure tirzepatide
The confusion between units and milligrams traces back to how insulin syringes were designed. They were never meant for peptide dosing. They were built for insulin, where "units" refers to biological activity rather than volume. But because insulin syringes are widely available, affordable, and graduated for precise small-volume measurement, they became the standard tool for GLP-1 injections including tirzepatide.
Here is what you need to know about the three common syringe sizes.
U-100 insulin syringe sizes
All standard insulin syringes in the United States are U-100, meaning 100 units equals 1 mL. Within that standard, three sizes exist:
Syringe size | Maximum volume | Each tick mark | Best for |
|---|---|---|---|
0.3 mL (30 units) | 0.30 mL | 0.5 units (half-unit markings) | Microdosing, low-dose titration, high-concentration vials |
0.5 mL (50 units) | 0.50 mL | 1 unit | Standard dosing at most concentrations |
1.0 mL (100 units) | 1.00 mL | 1 or 2 units | Higher doses, lower concentrations |
For drawing exactly 50 units, any syringe that holds at least 50 units works. But the 0.5 mL syringe draws up to exactly 50 units at full capacity, which means you cannot draw more than intended. This built-in safety margin makes it the preferred choice when 50 units is your target.
Researchers on tirzepatide weight loss dosing protocols often start with a 0.5 mL syringe and transition to a 1.0 mL syringe as their dose increases beyond 50 units during titration.
Reading the syringe correctly
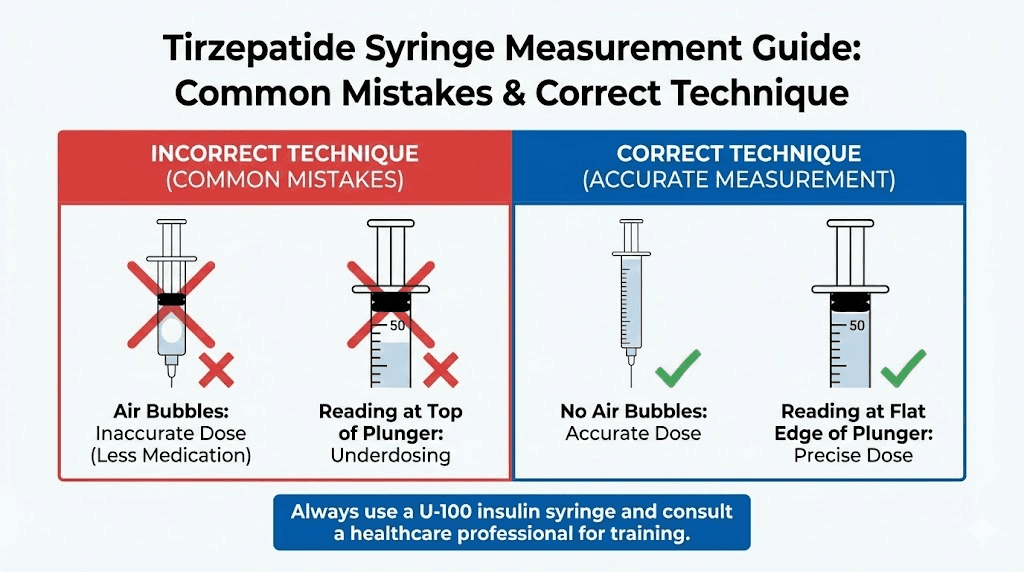
Hold the syringe at eye level with the needle pointing up. The bottom of the curved liquid surface (the meniscus) should align exactly with the 50-unit line. Not the top of the curve. The bottom.
Reading from an angle introduces parallax error. Looking up at the syringe makes 48 units look like 50. Looking down makes 52 units look like 50. Eye level, every time.
Air bubbles also cause errors. A bubble sitting below the liquid line displaces volume, meaning you have drawn less tirzepatide than the syringe shows. Tap the syringe with the needle pointing up to float bubbles to the top, then push the plunger gently to expel them before reading your volume.
These details matter more than most researchers realize. For precise unit measurements, even a 2-3 unit error can shift your actual dose meaningfully at higher concentrations.
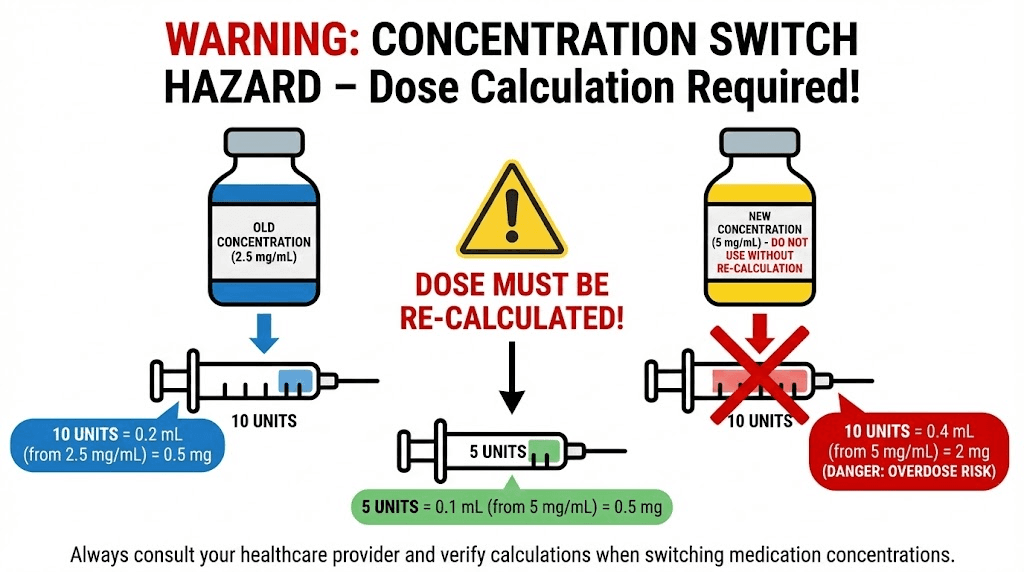
What happens when your pharmacy changes your concentration
This is where dosing errors happen most frequently. Your pharmacy refills your prescription with a different concentration than your previous vial. Maybe they switched suppliers. Maybe they optimized their formulation. Maybe they ran out of your usual concentration.
If you were drawing 50 units from a 10 mg/mL vial (getting 5.0 mg) and your new vial reads 20 mg/mL, drawing the same 50 units now gives you 10.0 mg. Double your dose. Without any warning from your syringe, which still reads 50 units, same as always.
This scenario is not hypothetical. It happens regularly with compounded tirzepatide, especially when pharmacies experience supply chain changes or when patients transfer between providers. The researchers who avoid this problem share one habit: they check the concentration label on every new vial and recalculate before the first injection.
Concentration change safety protocol
Follow this checklist every time you open a new vial:
Step 1: Read the concentration on the new vial label. Write it down.
Step 2: Compare it to your previous vial concentration. Are they the same?
Step 3: If different, recalculate your units using the formula: units = (desired mg / new concentration) x 100
Step 4: Verify with a second calculation method. Use the peptide calculator or run the math manually.
Step 5: Write your new unit amount on the vial with a marker.
Five steps. Under a minute. And it prevents the single most dangerous dosing error in compounded tirzepatide protocols.
Common concentration switches and their impact
Old concentration | New concentration | Old units for 5 mg | New units for 5 mg | If you draw old units |
|---|---|---|---|---|
5 mg/mL | 10 mg/mL | 100 units | 50 units | You get 10 mg (double dose) |
10 mg/mL | 20 mg/mL | 50 units | 25 units | You get 10 mg (double dose) |
10 mg/mL | 5 mg/mL | 50 units | 100 units | You get 2.5 mg (half dose) |
20 mg/mL | 10 mg/mL | 25 units | 50 units | You get 5 mg (half dose, but at correct amount in this case) |
Double dose means significantly amplified side effects. Nausea, vomiting, and gastrointestinal distress increase dramatically with tirzepatide dose jumps. Researchers who accidentally double their dose often experience what feels like severe food poisoning for 48-72 hours. Understanding tirzepatide side effects at various dose levels helps you recognize if something went wrong with your calculation.
Reconstituted tirzepatide: calculating your own concentration
Researchers working with lyophilized (freeze-dried) tirzepatide powder determine their own concentration during reconstitution. This gives you control over the final concentration but adds a layer of responsibility. Your math during reconstitution determines what every unit on your syringe delivers for the entire life of that vial.
The reconstitution math
concentration (mg/mL) = peptide amount (mg) / water volume (mL)
For a 10 mg vial:
Bacteriostatic water added | Resulting concentration | 50 units delivers |
|---|---|---|
1.0 mL | 10 mg/mL | 5.0 mg |
2.0 mL | 5 mg/mL | 2.5 mg |
4.0 mL | 2.5 mg/mL | 1.25 mg |
For a 30 mg vial:
Bacteriostatic water added | Resulting concentration | 50 units delivers |
|---|---|---|
1.0 mL | 30 mg/mL | 15.0 mg |
1.5 mL | 20 mg/mL | 10.0 mg |
3.0 mL | 10 mg/mL | 5.0 mg |
6.0 mL | 5 mg/mL | 2.5 mg |
For a 60 mg vial:
Bacteriostatic water added | Resulting concentration | 50 units delivers |
|---|---|---|
2.0 mL | 30 mg/mL | 15.0 mg |
3.0 mL | 20 mg/mL | 10.0 mg |
6.0 mL | 10 mg/mL | 5.0 mg |
12.0 mL | 5 mg/mL | 2.5 mg |
Most researchers find the sweet spot between precision and convenience at 10 mg/mL. It makes the mental math clean, produces reasonable injection volumes, and aligns with how most compound dosing charts are written.
Choosing your water volume strategically
Your water volume choice should match your dosing phase. Here is the logic.
If you are in early titration at 2.5 mg per week, using 2.0 mL of water with a 10 mg vial gives you 5 mg/mL. At that concentration, 2.5 mg requires 50 units, which is easy to measure accurately. The vial provides 4 doses (10 mg total / 2.5 mg per dose).
If you are at 5 mg per week, 1.0 mL of water with the same 10 mg vial gives you 10 mg/mL. Now 5 mg requires 50 units. Clean math. The vial provides 2 doses.
The principle: choose your water volume so that your weekly dose falls on a round number of units. This reduces measurement error and simplifies your protocol. The peptide reconstitution calculator handles this optimization automatically.
How much bacteriostatic water to use
For detailed guidance on mixing bacteriostatic water with peptides, including step-by-step reconstitution instructions and common mistakes to avoid, check our dedicated guide. The reconstitution process itself is straightforward, but small errors compound over the life of the vial.
The bacteriostatic water preserves the reconstituted solution thanks to the 0.9% benzyl alcohol it contains. This antimicrobial agent allows multi-dose vials to remain safe for repeated needle punctures over their refrigerated shelf life, typically 28-30 days.
Tirzepatide dosing tiers and where 50 units fits in standard protocols
Understanding where 50 units falls within the standard tirzepatide titration schedule helps contextualize your dosing. Tirzepatide follows a step-up approach, starting low and increasing every four weeks based on tolerance and response.
Standard titration schedule
Phase | Weekly dose | Duration | Units at 10 mg/mL | Units at 5 mg/mL | Units at 20 mg/mL |
|---|---|---|---|---|---|
Starting dose | 2.5 mg | Weeks 1-4 | 25 units | 50 units | 12.5 units |
Dose tier 2 | 5.0 mg | Weeks 5-8 | 50 units | 100 units | 25 units |
Dose tier 3 | 7.5 mg | Weeks 9-12 | 75 units | N/A (exceeds syringe) | 37.5 units |
Dose tier 4 | 10.0 mg | Weeks 13-16 | 100 units | N/A | 50 units |
Dose tier 5 | 12.5 mg | Weeks 17-20 | N/A (exceeds 1 mL) | N/A | 62.5 units |
Maximum dose | 15.0 mg | Week 21+ | N/A | N/A | 75 units |
Look at that table carefully. At 10 mg/mL, 50 units corresponds to the 5.0 mg dose tier. At 5 mg/mL, 50 units is the 2.5 mg starting dose. At 20 mg/mL, 50 units is the 10.0 mg dose tier. Same syringe reading. Three entirely different points in the treatment timeline.
This is precisely why concentration awareness matters so much. A researcher who switches from a 5 mg/mL vial to a 10 mg/mL vial and keeps drawing 50 units has just jumped from the starting dose to the second tier without any gradual titration. That unexpected jump often triggers significant gastrointestinal side effects that could have been avoided entirely.
When to stay at 50 units versus increasing
The decision to increase your dose depends on several factors beyond just schedule. If you are experiencing steady weight loss, improved appetite regulation, and tolerable side effects at your current dose, there may be no reason to increase regardless of what the standard titration chart suggests.
Many researchers find their optimal response at 5 mg per week and never need to titrate higher. Others require 10 mg or 15 mg to achieve similar effects. Individual variation in tirzepatide response time and receptor sensitivity means the right dose is the lowest effective dose, not necessarily the highest available dose.
For a thorough look at dose optimization, our guide on why tirzepatide might not be working covers the factors that influence response beyond simple dose adjustments.
Common mistakes when measuring 50 units of tirzepatide
Even experienced researchers make measurement errors. The mistakes below account for the majority of dosing problems reported in peptide research communities.
Mistake 1: not checking vial concentration
This has been emphasized throughout this guide because it is the number one source of dosing errors. Period. Every new vial gets checked. Every refill gets verified. No exceptions. If you have been drawing 50 units and getting 5.0 mg, a pharmacy switch to 20 mg/mL means those same 50 units now deliver 10.0 mg.
Mistake 2: confusing U-100 and U-40 syringes
While U-100 syringes are standard in the United States, U-40 syringes exist for certain veterinary insulin formulations. If you accidentally use a U-40 syringe to draw "50 units," you will actually draw 1.25 mL instead of 0.50 mL. At 10 mg/mL, that means 12.5 mg instead of 5.0 mg. Always verify your syringe markings read U-100.
Mistake 3: air bubbles displacing volume
A visible air bubble in your syringe means you have drawn less liquid than the syringe indicates. If you see the plunger at the 50-unit mark but there is a 5-unit air bubble trapped in the barrel, you only have 45 units of actual tirzepatide solution. At 10 mg/mL, that is 4.5 mg instead of 5.0 mg. Over weeks, these small shortfalls add up.
The fix is simple. Draw slightly past your target, tap the syringe with the needle pointing up to float bubbles to the top, push the plunger to expel the air and excess liquid until you reach exactly 50 units of bubble-free solution.
Mistake 4: reading at an angle
Parallax error. It sounds technical, but it just means reading your syringe from the wrong angle. Always hold the syringe at eye level. The flat bottom of the meniscus should align with the 50-unit line. Not the curved top. Not from above or below. Straight on.
Mistake 5: using the wrong syringe size
A 1.0 mL syringe has wider spacing between unit marks than a 0.3 mL syringe. The wider spacing on a 1.0 mL syringe might seem easier to read, but the thicker barrel means small volume differences are harder to distinguish visually. For 50 units, a 0.5 mL syringe offers the best combination of capacity and precision.
Mistake 6: not accounting for dead space
Every syringe has dead space, the small volume between the bottom of the plunger and the needle hub that holds liquid but does not get injected. In most insulin syringes, this dead space is minimal (0.5-2 units). But with expensive peptides like tirzepatide, even small amounts matter over the life of a vial. Low dead space syringes exist specifically to minimize this waste. If you are calculating peptide costs per injection, dead space factors into your actual cost per dose.
50 units compared to other common tirzepatide measurements
Context helps. Where does 50 units sit relative to other measurements you encounter in tirzepatide protocols? Here is a comprehensive reference connecting units, milligrams, and milliliters across the full dosing range.
At 10 mg/mL (most common compounded concentration)
Dose in mg | Units on syringe | Volume in mL | Protocol phase |
|---|---|---|---|
0.5 mg | 5 units | 0.05 mL | Ultra-low microdose |
1.0 mg | 10 units | 0.10 mL | Low microdose |
2.5 mg | 25 units | 0.25 mL | Standard starting dose |
5.0 mg | 50 units | 0.50 mL | Second dose tier |
7.5 mg | 75 units | 0.75 mL | Third dose tier |
10.0 mg | 100 units | 1.00 mL | Fourth dose tier |
For researchers tracking their protocol, understanding how many mg is 20 units of tirzepatide and how many mg is 40 units provides useful comparison points. At 10 mg/mL, 20 units equals 2.0 mg and 40 units equals 4.0 mg, placing 50 units squarely between the second and third unit reference points in everyday dosing conversations.
Semaglutide comparison for context
Many researchers transition between tirzepatide and semaglutide, or use both sequentially. The unit-to-mg math works identically for both peptides because units always measure volume, not drug content. The difference is in the dosing ranges.
Semaglutide therapeutic doses range from 0.25 mg to 2.4 mg weekly. Tirzepatide ranges from 2.5 mg to 15 mg weekly. If you have been switching between these medications, remember that 50 units from a tirzepatide vial delivers a completely different milligram amount than 50 units from a semaglutide vial, even if both vials happen to share the same concentration.
Understanding how many mg is 50 units of semaglutide provides a useful comparison if you work with both peptides. The conversion formula is identical. The clinical implications of the resulting dose differ completely.
Verifying your dose: the two-calculation rule
Never inject based on a single calculation. Professional pharmacists use double-check systems for a reason. Adopt the same discipline.
Method 1: Formula calculation
mg = (units / 100) x concentration
For 50 units at 10 mg/mL: (50 / 100) x 10 = 5.0 mg
Method 2: Proportional reasoning
100 units = 1 mL = 10 mg (at 10 mg/mL)
50 units = half of 100 = half of 10 mg = 5.0 mg
Both methods should produce the same answer. If they do not, something is wrong. Recheck your concentration, recalculate, and do not inject until the numbers agree.
Method 3: Calculator verification
Use the SeekPeptides peptide calculator as a third independent check. Enter your concentration and desired dose. The calculator returns the exact units to draw. Compare against your manual calculations.
Three methods. One answer. If all three agree, inject with confidence. If any disagree, stop and figure out where the error lives.
This level of verification might seem excessive for a routine injection. It is not. Dosing errors with tirzepatide carry real consequences, from amplified side effects to wasted peptide to stalled progress. The extra 30 seconds of verification costs nothing and protects everything.
Storing your vial after drawing 50 units
After drawing your dose, proper storage of the remaining solution ensures it stays potent for your next injection. Tirzepatide is a delicate peptide molecule that degrades with heat, light, agitation, and contamination.
Refrigeration requirements
Store your vial at 36-46 degrees Fahrenheit (2-8 degrees Celsius). This means the middle shelf of your refrigerator. Not the door, where temperature fluctuates every time you open it. Not the back, where freezing can occur. Not the top shelf near the light.
For researchers wanting specifics on tirzepatide refrigeration requirements, temperature consistency matters more than hitting an exact number within that range. A stable 40 degrees Fahrenheit is better than cycling between 34 and 46 degrees.
Multi-dose vial management
Every time you puncture the rubber stopper with a needle, you introduce a potential contamination pathway. Bacteriostatic water provides antimicrobial protection, but it is not unlimited. Most guidelines recommend using multi-dose vials within 28-30 days of the first puncture.
Track this. Write the date of first use on the vial with a permanent marker. When 28 days pass, assess remaining contents against tirzepatide expiration guidelines. If your solution appears cloudy, discolored, or contains visible particles, discard it regardless of the date.
Between uses, wipe the vial stopper with an alcohol swab before inserting the needle. Every time. This simple step reduces contamination risk substantially.
Travel considerations
Taking your tirzepatide outside the refrigerator starts a clock. At room temperature (up to 86 degrees Fahrenheit), compounded tirzepatide remains stable for limited periods. Most pharmacies recommend no more than a few hours unrefrigerated for compounded formulations, though manufacturer-branded products (Mounjaro, Zepbound) allow up to 21 days at room temperature.
For travel, use an insulated cooling case with gel packs. Avoid direct ice contact, which can freeze the solution. Our guide on how long compounded tirzepatide can be out of the fridge covers travel protocols in detail.
How 50 units fits into popular tirzepatide protocols
Different goals call for different approaches. Here is how 50 units maps to specific protocol strategies.
Protocol 1: standard weight loss titration (10 mg/mL vial)
Goal: Gradual dose escalation following the standard tirzepatide titration schedule.
Where 50 units fits: This is your 5.0 mg dose, typically reached at week 5. You spend weeks 1-4 at 25 units (2.5 mg), then move to 50 units for weeks 5-8 if side effects are manageable.
Expected response: Most researchers report noticeable appetite suppression at 5.0 mg. Weight loss often accelerates during this phase compared to the 2.5 mg starting dose. Research from SURMOUNT trials showed significant weight loss results beginning to differentiate from lower doses at the 5.0 mg tier.
Next step: After 4 weeks at 50 units, assess progress. If weight loss has plateaued or appetite suppression weakened, increase to 75 units (7.5 mg). If 50 units still produces steady results, there is no reason to increase.
Protocol 2: conservative microdosing approach (5 mg/mL vial)
Goal: Minimize side effects with a gradual introduction.
Where 50 units fits: At 5 mg/mL, 50 units delivers 2.5 mg, which is the standard starting dose. This protocol uses a lower concentration vial specifically so that the starting dose requires a larger, easier-to-measure volume.
Advantage: Drawing 50 units is more precise than drawing 25 units. The larger volume reduces relative measurement error. For researchers sensitive to tirzepatide side effects, starting with this concentration allows even sub-2.5 mg dosing by drawing fewer than 50 units.
Protocol 3: maintenance dosing (20 mg/mL vial)
Goal: Sustain results at an established dose with minimal injection volume.
Where 50 units fits: At 20 mg/mL, 50 units delivers 10.0 mg. This is an advanced dose tier for researchers who have already titrated through lower doses and found their maintenance level at 10 mg per week.
Advantage: Only 0.5 mL injected per week. Smaller injection volumes mean less subcutaneous fluid, reduced injection site reactions, and faster absorption. Researchers on maintenance doses often prefer higher concentrations for exactly this reason.
Tirzepatide versus semaglutide: does the conversion math differ?
No. The math is identical. Units always measure volume on a U-100 insulin syringe, and the conversion formula works the same regardless of which peptide fills the syringe.
The difference is clinical, not mathematical. Tirzepatide and semaglutide are different molecules with different dosing ranges, different receptor targets, and different side effect profiles. The semaglutide versus tirzepatide comparison covers these clinical differences thoroughly.
But if you need to know how many mg is 50 units for either peptide, the formula is the same:
mg = (50 / 100) x concentration in mg/mL
The answer changes only if the concentration changes. A 10 mg/mL semaglutide vial and a 10 mg/mL tirzepatide vial both deliver exactly 5.0 mg at 50 units. What those 5.0 mg do inside your body is where the comparison becomes relevant.
For researchers tracking side effect differences between the two peptides, dose equivalence is not straightforward. Five milligrams of tirzepatide is not equivalent to 5 milligrams of semaglutide in terms of clinical effect. Tirzepatide operates as a dual GIP/GLP-1 receptor agonist, while semaglutide targets only GLP-1. This dual mechanism means tirzepatide often produces stronger appetite suppression and greater weight loss results at comparable milligram doses.
How to handle fractional units
Not every calculation produces a clean round number. At 20 mg/mL, a 2.5 mg dose requires 12.5 units. At 30 mg/mL, a 5 mg dose requires 16.7 units. These fractional amounts create practical challenges with standard syringes.
Option 1: use half-unit syringes
The 0.3 mL (30-unit) insulin syringe typically includes half-unit markings. This lets you measure 12.5 units precisely, which is impossible on a standard 1-unit-increment syringe. If your protocol frequently requires fractional units, investing in half-unit syringes eliminates guesswork.
Option 2: adjust your reconstitution
If you are reconstituting your own vials, choose a water volume that produces round-number unit measurements at your target dose. Want 2.5 mg to equal exactly 50 units? Use enough water to create a 5 mg/mL concentration. Want 5 mg to equal exactly 50 units? Create a 10 mg/mL concentration.
This is one of the key advantages of self-reconstitution. The reconstitution calculator can help you find the water volume that produces the cleanest math for your specific dose.
Option 3: round to the nearest measurable unit
If your target is 16.7 units and your syringe measures in whole units, drawing 17 units gives you slightly more than intended. At 30 mg/mL, the difference between 16 units (4.8 mg) and 17 units (5.1 mg) is 0.3 mg. For most protocols, this variation falls within acceptable tolerance. But recognize that you are consistently running slightly above or below target, and track accordingly.
The relationship between concentration, units, and injection comfort
Volume affects more than just math. It affects the physical experience of injection.
At 5 mg/mL, a 10 mg dose requires 100 units (1.0 mL). That is a full syringe of subcutaneous fluid. Some researchers report discomfort, stinging, or visible welts at injection sites when injecting larger volumes. Higher concentrations reduce this problem.
At 20 mg/mL, that same 10 mg dose requires only 25 units (0.25 mL). A quarter of the volume. Less fluid means less tissue distension, less pressure, and faster absorption. Injection sites recover faster, and rotation between sites becomes easier because each injection creates less local impact.
For researchers injecting 50 units specifically, the volume is always 0.5 mL regardless of concentration. This is a moderate injection volume that most people tolerate well. It falls in the comfortable middle ground, enough liquid to distribute the peptide effectively but not so much that it causes significant site reactions.
Proper injection site selection and rotation further improve comfort. The abdomen (at least 2 inches from the navel), outer thigh, and upper arm are standard rotation sites for subcutaneous GLP-1 receptor agonist injections.
Tracking your doses: building a simple log
Accurate dosing means nothing without accurate tracking. A simple dose log prevents the two most common protocol problems: forgetting whether you injected this week and losing track of your titration schedule.
Your log should capture:
Date of each injection
Vial concentration (especially important if it changes between refills)
Units drawn
Calculated mg (verify every time)
Injection site (for rotation tracking)
Side effects noted (type, severity, duration)
Weight (if tracking for weight management)
A simple spreadsheet works. So does a notes app. So does a paper notebook. The format matters less than the consistency. Recording every injection creates a clear history that helps you and your healthcare provider make informed titration decisions.
SeekPeptides members access protocol tracking tools that streamline this process, combining dose logging with progress visualization and titration reminders.
When to adjust from 50 units
Fifty units is not a permanent destination for most researchers. It is a point on a continuum. Knowing when to adjust, up or down, optimizes your outcomes.
Signs you might need more than 50 units
Appetite suppression wearing off before your next weekly dose. Weight loss stalling for 3 or more consecutive weeks despite consistent protocol adherence. Blood glucose levels no longer improving. These signals suggest your current dose may no longer be sufficient.
Before increasing, verify that the issue is actually dose-related. Poor diet alignment, inadequate protein intake, stress, sleep disruption, and medication interactions can all mimic dose insufficiency. Increasing your dose when the real problem is sleep deprivation wastes peptide and amplifies side effects without addressing the root cause.
If dose increase is warranted, standard titration moves from 50 units (at 10 mg/mL = 5.0 mg) to 75 units (7.5 mg). This step-up should happen after at least four weeks at the current dose. Rushing titration increases the risk of severe gastrointestinal side effects including nausea, vomiting, and constipation.
Signs you might need less than 50 units
Persistent nausea lasting more than 3-4 days after injection. Significant fatigue or energy crashes. Rapid weight loss exceeding 1-2% of body weight per week. These suggest your current dose may be too aggressive.
Reducing from 50 units to 40 units (4.0 mg at 10 mg/mL) or even 35 units (3.5 mg) can dramatically improve tolerability while maintaining meaningful therapeutic effect. The research consistently shows that tirzepatide appetite suppression works at lower doses than many researchers expect.
Some researchers find that microdosing approaches produce better outcomes than aggressive titration. The best dose is always the lowest effective dose.
Special considerations for Mounjaro and Zepbound prefilled pens
If you use brand-name tirzepatide (Mounjaro for diabetes, Zepbound for weight management), the conversion math above does not apply in the same way. Prefilled pens deliver a fixed dose with each injection. The pen mechanism measures the dose internally. You do not draw from a vial with a syringe.
Mounjaro and Zepbound pens come in fixed strengths: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg. Each pen delivers its labeled dose. No unit-to-mg conversion needed. No concentration math required.
The 50-unit question is relevant exclusively for researchers using compounded tirzepatide from multi-dose vials with insulin syringes. If you are using compounded tirzepatide from pharmacies like Empower or other compounding sources, the conversion charts in this guide apply directly.
Frequently asked questions
Is 50 units of tirzepatide the same as 50 units of insulin?
In terms of volume, yes. Both equal 0.5 mL on a U-100 syringe. In terms of what is inside that volume, no. Insulin at 50 units delivers 50 international units of insulin. Tirzepatide at 50 units delivers a milligram amount determined by the vial concentration. The syringe measures volume identically. The medications are completely different.
Can I use a tuberculin syringe instead of an insulin syringe for 50 units?
Tuberculin syringes measure in milliliters, not units. To draw the equivalent of 50 units, you would draw 0.50 mL on a tuberculin syringe. The result is identical. Some researchers prefer tuberculin syringes because the milliliter markings align more naturally with concentration math. Both syringe types work as long as you convert correctly.
What if I accidentally drew 60 units instead of 50?
At 10 mg/mL, 60 units delivers 6.0 mg instead of 5.0 mg. That is 1.0 mg more than intended. For most researchers, a single 1 mg overshoot will not cause serious problems, though you may notice increased side effects like nausea or decreased appetite. Do not try to "make up" for the overshoot by reducing your next dose. Simply return to your normal 50 units the following week.
How do I know if my syringe is U-100?
Check the syringe packaging and the barrel itself. U-100 syringes are clearly labeled "U-100" and show 100 units per 1 mL. In the United States, virtually all commercially available insulin syringes are U-100. If you purchased from a standard pharmacy, you almost certainly have U-100 syringes.
Does the needle gauge affect how many mg I draw?
No. Needle gauge (thickness) affects injection comfort, not volume measurement. A 30-gauge needle draws the same volume at 50 units as a 27-gauge needle. Thinner needles (higher gauge numbers) are more comfortable but draw liquid more slowly. For viscous tirzepatide formulations, a slightly thicker needle (27-29 gauge) may draw more smoothly.
Should I account for the liquid left in the needle hub?
Standard insulin syringes have minimal dead space (0.5-2 units). This means a tiny amount of liquid remains in the needle hub after injection. For routine dosing, this loss is negligible. For expensive medications where every microgram counts, low dead space syringes recover most of this wasted volume. Over a full vial, dead space losses can add up to 1-2% of total volume.
Can I split a 50-unit dose across two injection sites?
Technically yes, but there is rarely a reason to do so. Splitting a dose requires two needle punctures, increasing contamination risk and injection site reactions. The 0.5 mL volume of a 50-unit injection is well within the comfortable range for a single subcutaneous injection. The only scenario where splitting might help is if a researcher experiences persistent large welts at injection sites, suggesting their tissue does not tolerate the full volume well.
My pharmacy told me to draw 50 units but did not specify the concentration. What do I do?
Call them back. A dosing instruction without concentration specification is incomplete. You need both pieces of information: how many units to draw AND what concentration your vial contains. Do not assume. Do not guess. Call and confirm before injecting.
External resources
For researchers serious about mastering their tirzepatide protocols, SeekPeptides provides comprehensive dosing guides, protocol tracking tools, and a community of experienced researchers who navigate these exact questions daily. Accurate dosing is the foundation of every successful protocol, and having the right resources makes the difference between guessing and knowing.
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay accurate, your concentrations stay verified, and your protocols stay precise.