Feb 8, 2026

Tired of stepping on the scale and seeing the same number? You are not alone. You started tirzepatide expecting steady drops every week, and for a while it delivered. Then it stopped. Or maybe it never really started the way you expected. Either way, you are frustrated, confused, and wondering whether this medication is even working anymore.
Here is the thing most guides will not tell you. Tirzepatide works for the vast majority of people. In the SURMOUNT-1 clinical trial, over 96% of participants on the highest dose achieved clinically meaningful weight loss of 5% or more. That means roughly 9 out of 10 people respond. But responding and losing weight consistently are two very different things. Plateaus happen. Stalls happen. And sometimes the problem is not the medication at all.
This guide breaks down every reason your weight loss might have stalled on tirzepatide. Not vague advice. Not generic tips. Specific, research-backed causes with equally specific solutions. We will cover metabolic adaptation, dosing issues, dietary mistakes, muscle loss, hormonal interference, and the dozen other factors that determine whether tirzepatide delivers transformative results or frustrating stagnation. SeekPeptides has compiled this from clinical data, real-world experiences, and the latest research so you can identify exactly what is going wrong and fix it.
Understanding how tirzepatide causes weight loss in the first place
Before you can troubleshoot a stall, you need to understand what tirzepatide actually does. It is not a simple appetite suppressant. Tirzepatide is a dual GIP and GLP-1 receptor agonist, which means it activates two different hormone pathways simultaneously. This dual mechanism is why it outperforms semaglutide and other single-agonist medications in head-to-head trials.
The GLP-1 component slows gastric emptying, meaning food stays in your stomach longer. You feel full faster and stay full longer. It also acts on appetite centers in the brain, reducing hunger signals at their source. The GIP component adds something unique. It improves how your body processes fat, enhances insulin sensitivity, and appears to increase fat oxidation, meaning your body gets better at burning stored fat for fuel.
Research published in Cell Metabolism found that tirzepatide did not prevent the metabolic slowdown that normally accompanies weight loss, but it significantly increased fat oxidation. Your body burns more fat relative to other fuel sources while on the medication. This is important because it means the weight you lose is disproportionately fat rather than muscle.
In the SURMOUNT-1 trial, participants achieved average weight loss of 16%, 21.4%, and 22.5% on the 5mg, 10mg, and 15mg doses respectively. The body composition data showed approximately 75% of weight lost was fat mass and 25% was lean mass. These numbers matter because they set realistic expectations for what tirzepatide can and cannot do.
Why this matters for your plateau
If you understand the mechanisms, you can identify which one is failing. Is your appetite suppression wearing off? That points to a dosing issue. Is your weight stable but body composition improving? That is not actually a stall. Is your metabolic rate crashing? That points to muscle loss. Each problem has a different solution, and throwing generic advice at a specific problem wastes time.
Reason 1: You have not reached your optimal dose yet
This is the single most common reason for disappointing early results. Tirzepatide uses a mandatory titration schedule. You start at 2.5mg for four weeks. This is not a therapeutic dose. It exists solely to let your body adjust to the medication and minimize gastrointestinal side effects.
Many people see little to no weight loss at 2.5mg. Some see none at 5mg either. That is completely normal.
The titration schedule looks like this: 2.5mg for weeks 1 through 4, then 5mg for weeks 5 through 8, then 7.5mg for weeks 9 through 12, then 10mg for weeks 13 through 16, and potentially 12.5mg and 15mg after that. Each step takes a minimum of four weeks. Reaching the maximum 15mg dose takes at least 20 weeks. That is nearly five months before you are even at the highest dose.
If you are only six or eight weeks in and frustrated, the honest answer might simply be patience. The SURMOUNT-1 data showed that 90% of participants who had less than 5% weight loss by week 12 still achieved clinically meaningful results by week 72. Late responders are real. They are common. And they still get excellent outcomes.
What to do about it
Track your starting date and current dose. If you are below 10mg, you likely have not reached your optimal therapeutic range yet. Discuss your titration timeline with your healthcare provider. Do not rush the escalation. Faster titration means worse side effects, not faster results. But also do not stay at a sub-therapeutic dose longer than necessary. The research on how long tirzepatide takes to work consistently shows that meaningful results often require 12 to 16 weeks at therapeutic doses.
Reason 2: Metabolic adaptation is slowing your progress
Your body does not want to lose weight. From an evolutionary perspective, fat storage kept your ancestors alive during famine. When you start losing weight, your body fights back. This is called metabolic adaptation, and it happens to everyone regardless of the method they use to lose weight.
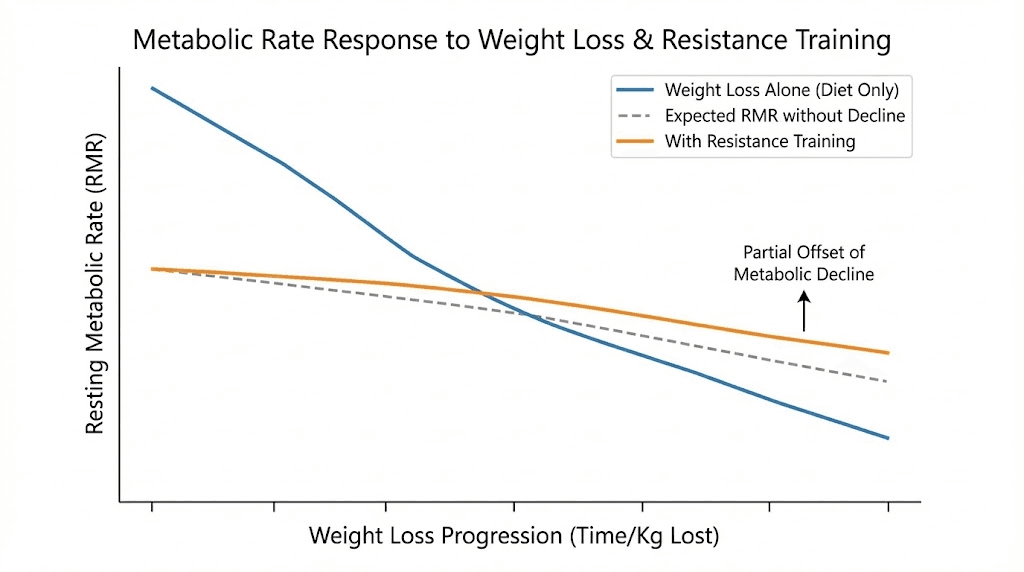
Here is what happens at the cellular level. As you lose weight, your resting metabolic rate decreases. You burn fewer calories at rest because you are carrying less mass. Your hunger hormones shift. Ghrelin, the hunger hormone, increases. Leptin, the satiety hormone, decreases. Your body becomes more efficient at extracting energy from food and more reluctant to burn stored fat.
The interesting finding from tirzepatide research is that the medication does not prevent this metabolic adaptation. A study in Cell Metabolism confirmed that the reduction in sleeping metabolic rate and 24-hour energy expenditure was comparable between tirzepatide and placebo groups after adjusting for changes in body weight. The medication does not stop your metabolism from slowing down.
What it does do is increase fat oxidation and suppress appetite despite the hormonal shifts working against you. But there is a limit. At some point, your reduced caloric needs catch up to your reduced intake, and weight loss stalls.
The math behind your stall
Consider this example. A 220-pound person might burn roughly 2,200 calories at rest. After losing 30 pounds, their resting metabolic rate might drop to 1,900 calories. If their food intake on tirzepatide stabilized around 1,800 calories early in treatment, the initial deficit was 400 calories per day, which is enough for roughly a pound of fat loss per week. After the 30-pound loss, that deficit shrinks to just 100 calories, which is barely noticeable on the scale and easily wiped out by normal daily variation in water weight.
What to do about it
You cannot prevent metabolic adaptation entirely, but you can manage it. Resistance training preserves muscle mass, which keeps your metabolic rate higher. Adequate protein intake protects lean tissue. Strategic caloric adjustments, not extreme restriction, maintain a meaningful deficit. And sometimes you need to accept that the rate of loss will naturally slow as you get lighter. A half-pound per week at 180 pounds is physiologically different from two pounds per week at 250 pounds, even though both represent progress.
Reason 3: You are losing muscle, and it is killing your metabolism
This might be the most underappreciated reason for tirzepatide plateaus. It deserves its own section because it connects to almost every other problem on this list.
The SURMOUNT-1 body composition analysis found that approximately 25% of weight lost on tirzepatide comes from lean mass. That includes muscle. For someone who loses 50 pounds, that means roughly 12 to 13 pounds of muscle gone. Muscle is metabolically active tissue. Every pound of muscle burns approximately 6 to 7 calories per day at rest. Losing 12 pounds of muscle costs you about 72 to 84 calories per day in resting metabolism.
That number might sound small, but it compounds. Combine it with the general metabolic slowdown from losing weight, and your daily energy expenditure can drop by 200 to 400 calories compared to where it was when you started treatment. That is the difference between losing a pound a week and staying flat.
Some research suggests the lean mass loss percentage may be even higher, with up to 39% of weight lost on GLP-1 and GIP/GLP-1 medications coming from lean mass in certain populations. The people most at risk are those who drastically cut calories, skip protein, and do no resistance exercise.
Signs you are losing too much muscle
Increased fatigue beyond what tirzepatide normally causes. Feeling weak during daily activities. Saggy skin that seems disproportionate to the weight you have lost. The scale dropping but your body looking soft rather than toned. Feeling cold more easily. Slower recovery from minor illnesses or injuries.
What to do about it
Resistance training two to three times per week. This is not optional if you want to keep losing weight. You do not need a gym membership or fancy equipment. Bodyweight exercises, resistance bands, or basic free weights work. The goal is to signal to your body that muscle is essential and should not be broken down for energy.
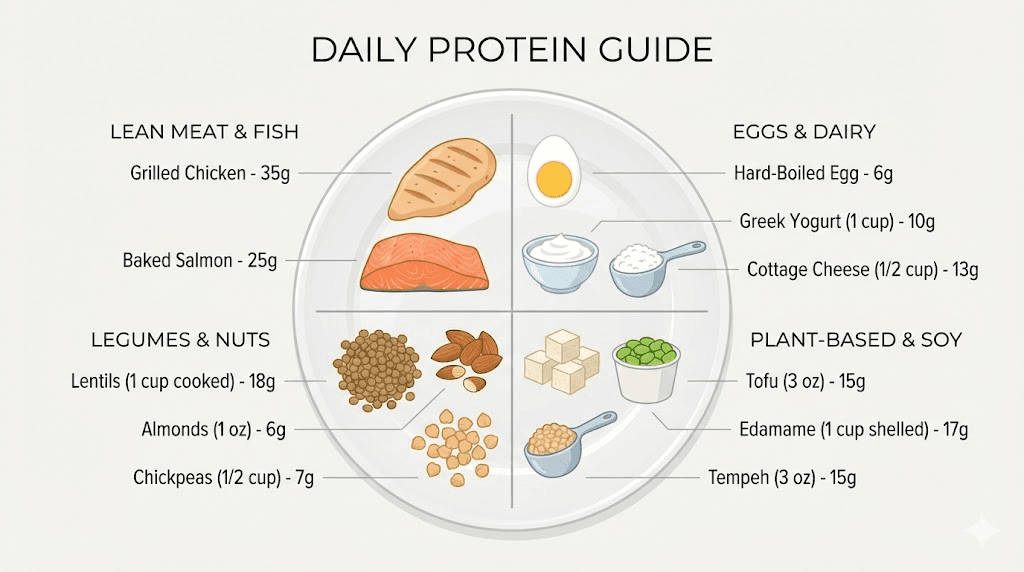
Protein intake of 1.2 to 1.6 grams per kilogram of ideal body weight daily. For a person with an ideal body weight of 160 pounds (72.5 kilograms), that means 87 to 116 grams of protein per day. Some experts recommend even higher at 1.6 to 2.2 grams per kilogram. Prioritize protein at every meal, aiming for 25 to 35 grams per sitting.
This can be challenging on tirzepatide because the appetite suppression makes eating difficult. But skipping meals or eating only small amounts of low-protein foods is a recipe for muscle loss and metabolic slowdown. Protein shakes, Greek yogurt, eggs, and lean meats should become staples. Check out how peptides support weight loss for women specifically, since muscle preservation strategies differ slightly by sex.
Reason 4: Your protein intake is too low
This deserves its own section because it is both incredibly common and incredibly fixable.
Low protein is one of the biggest underlying causes of slow progress on tirzepatide. Here is why. When you eat less food overall, which tirzepatide virtually guarantees, and the food you do eat is carbohydrate-heavy or fat-heavy with minimal protein, your body starts pulling amino acids from muscle tissue to meet its needs. Muscle breaks down. Metabolism drops. Weight loss stalls.
The standard dietary recommendation of 0.8 grams of protein per kilogram is woefully inadequate during active weight loss. That recommendation was designed for healthy adults maintaining their weight, not for people in a significant caloric deficit trying to preserve lean mass.
How much protein you actually need
Research-backed targets for people losing weight on GLP-1 medications:
Minimum effective dose: 1.2 grams per kilogram of ideal body weight per day. Optimal range: 1.2 to 1.6 grams per kilogram per day. High-performance range: 1.6 to 2.2 grams per kilogram per day. Some obesity medicine physicians simplify this to a minimum of 100 grams of protein daily regardless of body weight.
For practical purposes: aim for 25 to 35 grams of protein per meal across three meals, plus a protein-rich snack if possible. That gets most people to 80 to 120 grams per day.
The appetite suppression problem
Here is the catch. Tirzepatide suppresses your appetite so effectively that many people struggle to eat enough of anything, let alone enough protein. You feel full after a few bites. The thought of eating more feels impossible. And when you do eat, reaching for simple carbohydrates feels easier than cooking a protein-rich meal.
Solutions: protein shakes and smoothies are your best friend because liquids bypass some of the fullness signals. Greek yogurt packs 15 to 20 grams in a small serving. Cottage cheese, eggs, and jerky are dense protein sources in small volumes. Collagen peptides in coffee or tea add 10 to 15 grams without changing the taste significantly. Prioritize protein first at each meal, before eating anything else. And understand the connection between B12 supplementation and GLP-1 medications, since B12 deficiency can worsen fatigue and reduce your ability to exercise.
Reason 5: You are eating more than you think
Nobody wants to hear this one. But it matters.
Tirzepatide reduces appetite dramatically, but it does not eliminate the ability to eat. And as your body adapts to the medication, especially at a given dose, the appetite suppression can gradually weaken. Many people unconsciously increase their intake over time without realizing it.
Research on caloric tracking consistently shows that people underestimate their intake by 20 to 50%. Even registered dietitians underestimate by 10 to 20%. This is not about willpower or honesty. It is about the human brain being genuinely terrible at estimating portion sizes and caloric density.
Liquid calories are the biggest blind spot. A daily latte with whole milk adds 200 to 300 calories. A glass of juice is 150 to 200. Cooking oils add 120 calories per tablespoon. Salad dressings, sauces, nuts, and cheese are all calorie-dense foods that add up invisibly.
What to do about it
Track your food intake for one to two weeks. Not forever. Just long enough to see the truth. Use an app. Weigh portions when possible. Do not change your eating habits during this tracking period because the goal is to see what you actually eat, not what you think you eat.
Most people who do this discover one of two things. Either they are eating more calories than they thought, or they are eating far less protein than they need. Both problems have straightforward solutions. Adjust portions down or protein up based on what the data shows. This single step has restarted weight loss for thousands of people on GLP-1 medications.
Reason 6: You are not exercising, or you are exercising wrong
Exercise alone is a poor weight loss strategy. The research is clear on that. But exercise combined with tirzepatide is a game-changer. A Lilly-sponsored study found that people who combined tirzepatide with intensive lifestyle intervention, including regular exercise, lost an additional 21.1% of their body weight on top of what the medication alone achieved. By week 84, total mean weight loss reached 26.6% from study entry.
The problem is that many people on tirzepatide either do not exercise at all or focus exclusively on cardio. Neither approach is optimal.
Why cardio alone is not enough
Steady-state cardio, like walking on a treadmill for 45 minutes, burns calories during the activity but does little for your resting metabolic rate. It can even make metabolic adaptation worse in some cases because the body becomes more efficient at the activity over time, burning fewer calories for the same work. And excessive cardio without adequate protein and strength training can accelerate muscle loss.
Why strength training is essential
Strength training sends a powerful signal to your body: keep this muscle. Even in a caloric deficit, regular resistance exercise dramatically reduces the amount of lean mass lost. It also increases resting metabolic rate both acutely, through post-exercise oxygen consumption, and chronically, through increased muscle mass.
You do not need to become a powerlifter. Two to three sessions per week targeting major muscle groups is sufficient. Squats, deadlifts, presses, rows, and lunges form a complete program. Even bodyweight versions of these movements provide significant benefit. The goal is progressive overload, gradually increasing the challenge over time.
The ideal exercise approach
Strength training two to three times weekly for muscle preservation. Moderate cardio, walking is excellent, three to five times weekly for additional calorie burn. High-intensity interval training one to two times weekly if tolerated. Daily step count target of 7,000 to 10,000 steps. This combination maximizes fat loss while protecting the muscle that keeps your metabolism humming. Understanding the role of peptides in weight loss and muscle gain provides additional context for why preserving lean tissue matters so much during GLP-1 therapy.
Reason 7: Medical conditions are interfering
Sometimes the problem is not the medication or your lifestyle. It is another medical condition working against you.
Hypothyroidism
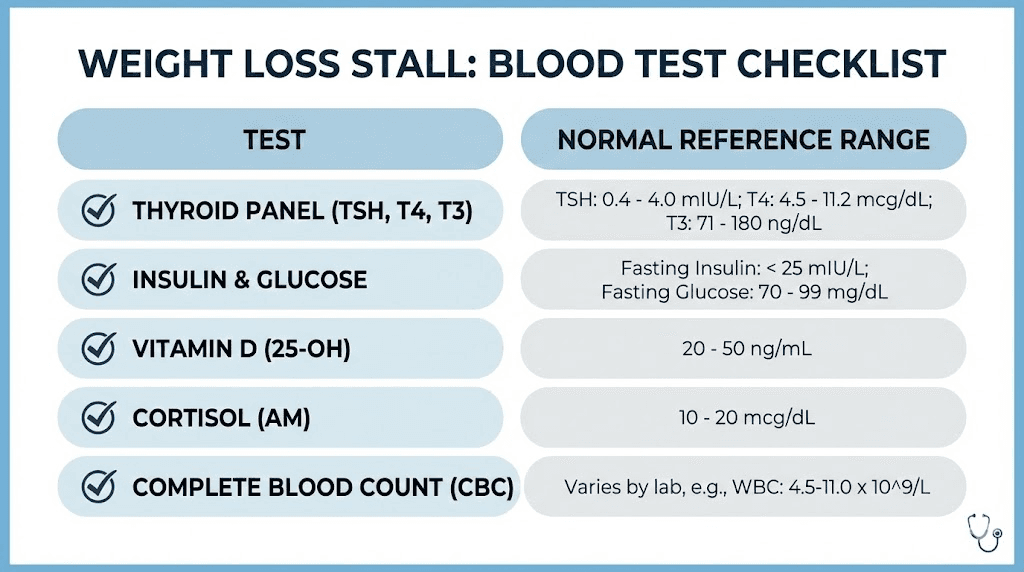
An underactive thyroid slows metabolism significantly. Even mild hypothyroidism, sometimes called subclinical hypothyroidism, can reduce resting metabolic rate by 5 to 15%. If you have not had your thyroid checked recently, this is worth investigating. TSH, free T3, and free T4 blood tests are the standard panel. Thyroid antibodies should be tested if autoimmune thyroiditis is suspected.
Polycystic ovary syndrome (PCOS)
PCOS affects up to 12% of women of reproductive age and creates significant insulin resistance that can blunt tirzepatide's effectiveness. Women with PCOS often respond differently to weight loss medications and may need higher doses, different dietary strategies specifically focused on insulin management, or additional medications.
Insulin resistance and type 2 diabetes
Severe insulin resistance can slow weight loss even on tirzepatide. The medication helps with insulin sensitivity, but if your baseline resistance is extreme, progress may be slower than clinical trial averages. Monitoring fasting insulin, HbA1c, and fasting glucose provides insight. The connection between peptides and hormone balance is relevant here because hormonal dysfunction rarely involves just one system.
Cushing syndrome and elevated cortisol
Chronically elevated cortisol promotes fat storage, especially visceral fat. True Cushing syndrome is rare, but subclinical cortisol elevation from chronic stress is extremely common. A 24-hour urinary free cortisol test or late-night salivary cortisol test can help identify this issue.
Medications that cause weight gain
Several common medications promote weight gain and can directly oppose tirzepatide. These include certain antidepressants like mirtazapine and paroxetine, antipsychotics like olanzapine and quetiapine, beta-blockers, corticosteroids, some anticonvulsants like valproate, and insulin. If you take any of these and your weight loss has stalled, discuss alternatives with your prescribing provider.
What to do about it
Get comprehensive bloodwork. At minimum: complete metabolic panel, thyroid panel (TSH, free T3, free T4), fasting insulin, HbA1c, cortisol, and a lipid panel. For women, add testosterone, DHEA-S, and sex hormone binding globulin. This baseline helps identify hidden factors that no amount of dietary modification will overcome.
Reason 8: Stress and cortisol are sabotaging you
Stress does not just make you feel bad. It fundamentally changes how your body processes and stores fat.
When you are stressed, your adrenal glands release cortisol. In short bursts, this is fine. It is your fight-or-flight system doing its job. But chronic stress means chronically elevated cortisol, and that creates a cascade of weight-loss-killing effects.
Cortisol increases appetite and specifically increases cravings for calorie-dense comfort foods, exactly the foods that pack on visceral fat. It promotes fat storage in the abdominal area. It increases insulin resistance. It breaks down muscle tissue, worsening the metabolic slowdown we discussed earlier. It disrupts sleep, which creates its own separate set of weight loss problems.
Tirzepatide does not directly address cortisol. It targets incretin receptors rather than the hypothalamic-pituitary-adrenal axis. While substantial weight loss may indirectly improve cortisol metabolism through reduced adiposity, the medication cannot override the effects of chronic psychological stress.
What to do about it
Identify your major stressors. You do not need to eliminate all stress, but you need to manage the chronic, grinding variety.
Evidence-based stress reduction techniques include regular physical activity (which you should already be doing for muscle preservation), adequate sleep (see next section), mindfulness or meditation practices even for just 10 minutes daily, limiting news and social media consumption, setting boundaries around work hours, and addressing relationship or financial stressors directly rather than avoiding them.
Sometimes fixing sleep and managing stress can restart weight loss without changing food or exercise habits at all.
Reason 9: Poor sleep is undermining everything
Sleep deprivation is one of the most potent disruptors of weight loss. And most people do not realize they are sleep-deprived because they have normalized functioning on too little rest.
Research consistently shows that inadequate sleep, defined as less than seven hours per night, affects weight loss through multiple mechanisms. It increases ghrelin (hunger hormone) by 15 to 28%. It decreases leptin (satiety hormone) by a similar amount. It increases cortisol, compounding the stress effects discussed above. It impairs insulin sensitivity, sometimes by as much as 30% after just four nights of poor sleep. It reduces motivation to exercise. It increases cravings for high-calorie, high-carbohydrate foods. And it shifts body composition changes toward muscle loss rather than fat loss.
One study found that sleep-restricted dieters lost 55% less fat and 60% more lean mass compared to well-rested dieters eating the same number of calories. The same caloric deficit produced dramatically different body composition outcomes based solely on sleep.
What to do about it
Aim for seven to nine hours of actual sleep, not just time in bed. Maintain a consistent sleep schedule, even on weekends. Keep your bedroom cool, 65 to 68 degrees Fahrenheit is optimal. Eliminate screens for at least 30 minutes before bed. Limit caffeine after noon. Address sleep apnea if present, which is common in people with obesity and can dramatically improve with weight loss. If you suspect sleep quality issues, consider tracking your sleep with a wearable device or requesting a sleep study.
Reason 10: You are actually a non-responder (rare but real)
Let us address the elephant in the room. Not everyone responds to tirzepatide.
In the SURMOUNT-1 trial, approximately 9% of participants on the highest 15mg dose did not achieve clinically meaningful weight loss of 5% or more. That is roughly 1 in 11 people. If you have been at a therapeutic dose, typically 10mg or 15mg, for 12 to 16 weeks with minimal response, you may fall into this category.
Non-response is a real phenomenon, not a personal failing. It likely reflects individual differences in receptor sensitivity, gut microbiome composition, genetics, and the complex interplay of hormonal systems that regulate body weight.
How to know if you are a true non-responder versus just stalled
Timing matters. If you have been on 15mg for at least 12 weeks and have lost less than 5% of your starting body weight despite good dietary compliance and regular exercise, that suggests non-response rather than a simple plateau. If you lost weight initially and then stalled, that is more likely a plateau caused by one of the other reasons in this article.
Also consider: are you taking the medication correctly? Subcutaneous injection once weekly, same day each week, properly stored and not expired. Storage matters because degraded medication will not work properly. If you are using compounded tirzepatide, confirm the source is reputable and the product has been tested. Check our guide on Peptide Sciences tirzepatide for quality considerations.
What to do about it
Discuss with your healthcare provider. Options may include switching to a different medication such as retatrutide or semaglutide, adding a complementary medication, investigating underlying conditions more thoroughly, or considering whether the non-response is actually a medication quality issue. True pharmaceutical non-response is rare enough that it is worth ruling out everything else first.
Reason 11: Your expectations do not match reality
Sometimes the "stall" is actually normal, expected weight loss that does not match unrealistic expectations.
What the clinical trials actually show
Average weight loss on tirzepatide 15mg over 72 weeks was 22.5% of starting body weight. For a 250-pound person, that is about 56 pounds. That sounds impressive, and it is. But notice the timeframe: 72 weeks. That is nearly a year and a half. The average rate works out to less than a pound per week.
Early in treatment, weight comes off faster. Two to three pounds per week is common in the first few months, especially at higher starting weights. But as you lose weight, the rate naturally slows. A half-pound per week in months 6 through 12 is completely normal and still represents significant progress over time.
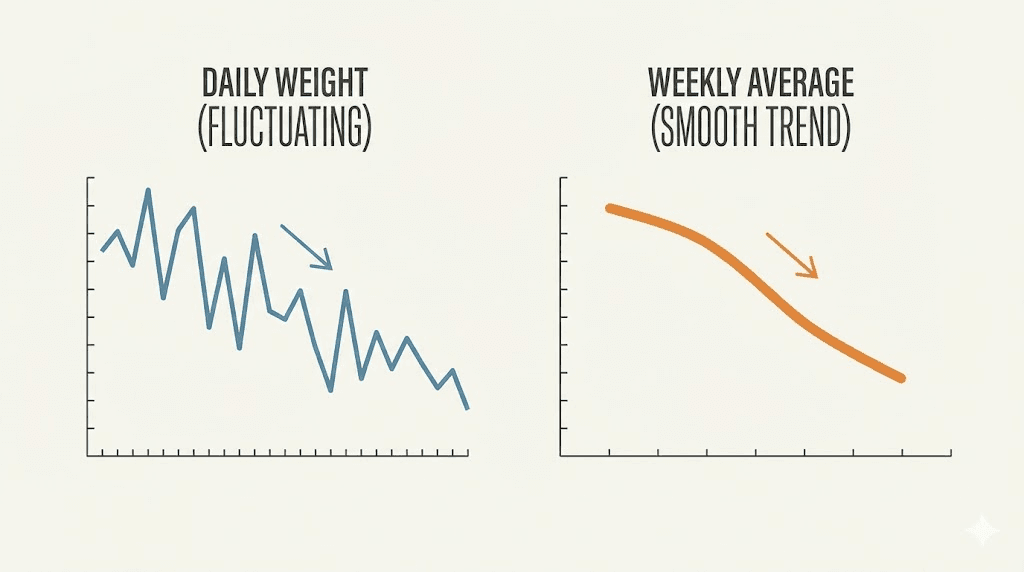
The scale is a liar
Day-to-day weight fluctuations of 2 to 5 pounds are normal and reflect changes in water retention, glycogen stores, food volume in the gut, sodium intake, and hormonal cycles. You can gain 3 pounds overnight from a high-sodium meal without gaining any fat whatsoever.
If you weigh yourself daily and react to every fluctuation, you will go insane. Weigh yourself weekly at most, same day, same time, first thing in the morning after using the bathroom, wearing similar clothing. Better yet, track a four-week rolling average rather than individual data points. The trend matters. Individual weigh-ins do not.
Body recomposition is real
If you are strength training (as recommended above), you may be building muscle while losing fat simultaneously. Muscle is denser than fat, so your scale weight may stay flat while your body is actually transforming. Take measurements: waist, hips, chest, thighs, and arms. Take progress photos monthly. How your clothes fit is a more reliable indicator than the scale. Real tirzepatide before and after results show that visual changes often outpace scale changes, especially when people are exercising.
Reason 12: You have been on the same dose too long
This is related to reason 1 but applies to people who initially responded well and then stalled.
Some people find an effective dose, lose weight steadily for several months, and then plateau. In these cases, the plateau may indicate that your current dose is no longer creating sufficient appetite suppression or metabolic effects at your new, lower body weight.
Think about it this way. The dose that created a significant caloric deficit at 250 pounds may not create the same deficit at 200 pounds. Your caloric needs are lower. Your body has partially adapted to the medication. And the appetite suppression that felt overwhelming at first may have gradually weakened.
What to do about it
If you are not already at the maximum dose of 15mg, discuss dose escalation with your healthcare provider. The standard titration allows increases at four-week intervals. If you plateaued at 5mg, moving to 7.5mg often restarts progress. If you plateaued at 10mg, 12.5mg or 15mg may be your optimal dose.
If you are already at 15mg and have stalled, the options are more limited. Your provider may discuss medication combinations, switching to a different agent, or focusing intensively on the lifestyle factors that amplify tirzepatide's effects. Understanding the complete dosing protocol helps you have a more informed conversation with your provider.
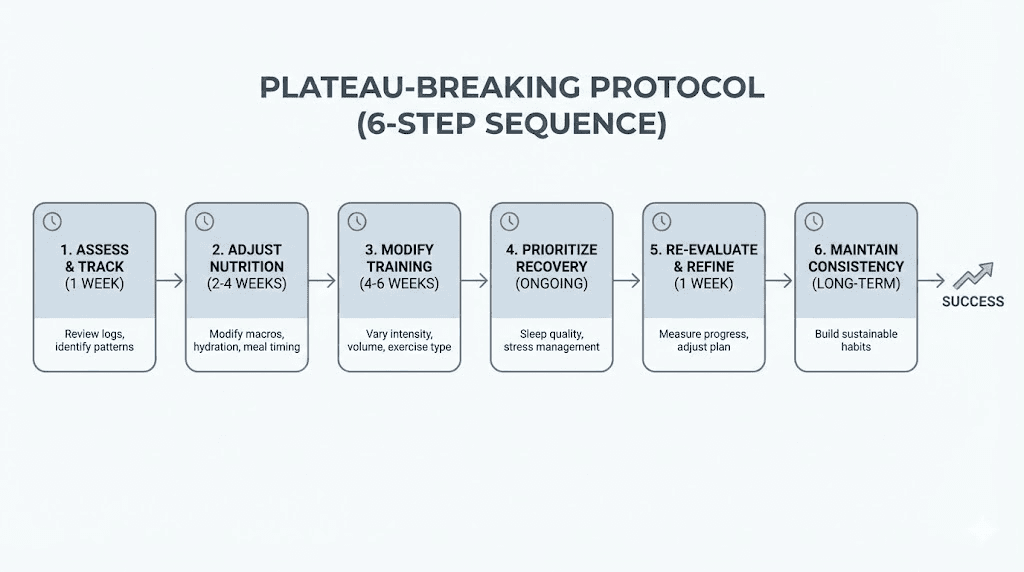
Breaking through your plateau: the complete action plan
Now that you understand the reasons, here is a step-by-step protocol for restarting weight loss. Do not try to implement everything simultaneously. Work through these in order, spending one to two weeks on each step before adding the next.
Step 1: Audit your basics (week 1-2)
Track your food intake for 7 to 14 days. Calculate your average daily protein intake. Confirm your current tirzepatide dose and duration at that dose. Weigh yourself at the same time each day for one week to establish a true baseline. Check your sleep duration and quality. Assess your current exercise habits honestly.
Step 2: Fix protein first (week 2-3)
If your protein is below 1.2 grams per kilogram of ideal body weight, fix this immediately. This single change restarts weight loss for many people. Protein shakes, Greek yogurt, cottage cheese, and eggs are the easiest high-protein foods to eat when appetite is suppressed. Aim for protein at every meal and snack. The supplementation guide for tirzepatide with B12 explains additional nutritional considerations during GLP-1 therapy.
Step 3: Add or upgrade exercise (week 3-4)
If you are not exercising, start with two strength training sessions per week and daily walking. If you are only doing cardio, add resistance training. If you are already strength training, increase the intensity through progressive overload, more weight, more reps, or more challenging movements. The goal is to preserve and ideally build muscle while creating additional caloric expenditure.
Step 4: Optimize sleep and stress (week 4-5)
Aim for seven to nine hours nightly. Implement one stress management technique consistently. These changes compound over time and their effects on weight loss are significant even though they do not involve food or exercise directly.
Step 5: Consult your provider (week 5-6)
If steps 1 through 4 have not restarted progress, it is time for a medical evaluation. Request comprehensive bloodwork including thyroid, insulin, cortisol, and metabolic panels. Discuss dose adjustment if applicable. Review any other medications that might be contributing. Consider whether a specialist referral to an obesity medicine physician or endocrinologist would be appropriate.
Step 6: Reassess and adjust (ongoing)
Weight loss is not linear. There will be weeks of rapid progress and weeks of nothing. The key is the trend over months, not weeks. If you have implemented all of the above and given each step adequate time, you should see the scale start moving again within four to eight weeks. If not, your provider can explore additional options including medication changes or combinations.
The role of compounded tirzepatide in weight loss stalls
If you are using compounded tirzepatide rather than brand-name Mounjaro or Zepbound, medication quality becomes an important variable.
Compounded medications are not subject to the same manufacturing standards as FDA-approved products. The actual concentration of tirzepatide in a compounded vial may vary from what the label states. Storage conditions during shipping may have degraded the peptide. And some compounding pharmacies produce higher-quality products than others.
Signs of a medication quality issue
You experienced initial appetite suppression that disappeared even at higher doses. The medication looks cloudy, discolored, or has particles floating in it. You have no gastrointestinal side effects at any dose, which paradoxically suggests the medication may not be active since some degree of GI effects is expected. Your injection sites show no reaction whatsoever.
What to do about it
Source your compounded tirzepatide from reputable pharmacies that provide certificates of analysis. Proper storage is essential, as tirzepatide degrades when left at room temperature for extended periods. If you suspect a quality issue, switching to a different compounding pharmacy or to brand-name product can help determine whether the medication or other factors are causing your stall. Understanding proper peptide storage after reconstitution is critical for maintaining potency.
Alcohol and tirzepatide: the hidden progress killer
Alcohol deserves special attention because it sabotages weight loss through multiple pathways simultaneously.
First, alcohol contains 7 calories per gram, nearly as calorie-dense as fat at 9 calories per gram. A single glass of wine is 125 to 150 calories. A craft beer can be 200 to 300. A cocktail with mixers can exceed 400. These calories provide zero protein, zero essential nutrients, and are not registered by your hunger signals, meaning they add to rather than replace food calories.
Second, alcohol directly impairs fat oxidation. Your body prioritizes metabolizing alcohol over everything else, including fat. As long as alcohol is in your system, fat burning essentially stops. For a single drink, this might last a few hours. For a heavy drinking session, fat metabolism can be suppressed for 24 hours or more.
Third, alcohol weakens inhibition and increases appetite. The carefully planned high-protein meal turns into pizza and wings. The plan to stop at one glass becomes three. And the morning after often involves high-calorie comfort foods to manage the hangover.
Fourth, alcohol disrupts sleep quality. Even moderate consumption reduces deep sleep and REM sleep, compounding the sleep-related weight loss problems discussed earlier.
What to do about it
Reducing or eliminating alcohol is one of the highest-impact changes you can make during a tirzepatide plateau. If complete abstinence is not realistic, limit consumption to one to two drinks per week maximum. Choose lower-calorie options. Never drink on an empty stomach. And account for alcohol calories in your overall intake.
Water retention masking fat loss
Here is a scenario that drives people crazy. You are doing everything right. Your diet is on point, you are exercising, your sleep is good. But the scale will not budge. And then one morning you wake up three pounds lighter for no apparent reason.
Water retention is the most common explanation for short-term weight stalls that resolve spontaneously. Your body holds water for dozens of reasons: high sodium intake, hormonal fluctuations (especially around menstruation), increased cortisol, new exercise routines that cause inflammation, certain medications, carbohydrate intake fluctuations, and even weather changes.
The phenomenon called the "whoosh effect" is real. Fat cells do not disappear instantly when you burn fat. They initially fill with water, maintaining their size temporarily. Then, seemingly randomly, the water releases and the scale drops dramatically overnight. This is why the trend matters more than any individual weigh-in.
What to do about it
Stay adequately hydrated. Counterintuitively, drinking more water helps reduce water retention because it signals to your body that fluid is plentiful and there is no need to hold onto it. Monitor sodium intake without obsessing over it. Be aware of your menstrual cycle if applicable, as water retention of 2 to 8 pounds is normal in the luteal phase. And stop weighing yourself daily if the fluctuations are causing you psychological distress. Weekly or biweekly weigh-ins plus waist measurements give you accurate progress data without the daily emotional roller coaster.
The psychological side of weight loss stalls
We cannot talk about weight loss plateaus without addressing the mental component. A stall is not just a number problem. It is an emotional experience that can undermine your entire approach.
The frustration spiral
Weight stall leads to frustration. Frustration leads to stress. Stress elevates cortisol. Cortisol promotes fat storage and muscle breakdown. Which causes more weight stalling. Which causes more frustration. This is not metaphorical. It is a documented physiological cycle that makes stalls self-perpetuating.
The comparison trap
Social media is full of dramatic transformation stories. Someone lost 80 pounds in six months on tirzepatide. Someone else dropped four dress sizes in three months. These stories are real, but they represent the most dramatic end of the bell curve. Comparing your week 20 results to someone else's highlight reel is a guaranteed recipe for disappointment. The men's tirzepatide results page and the general before and after guide show the realistic range of outcomes.
The all-or-nothing mindset
Many people respond to a stall by either giving up entirely or going to extremes, slashing calories to 800 per day, exercising for two hours daily, or adding supplements and shortcuts that have no evidence behind them. Both responses make the problem worse. Giving up means losing whatever progress you have made. Extremes cause muscle loss, metabolic crashes, and burnout.
What to do about it
Reframe the stall as normal rather than failure. Every single person who has lost significant weight has experienced plateaus. It is part of the process, not evidence that the process is broken. Focus on non-scale victories: energy levels, sleep quality, how clothes fit, strength in the gym, blood work improvements, reduced joint pain. These changes are happening even when the scale is not moving. And consider talking to a therapist or counselor if the emotional toll of the weight loss journey is affecting your quality of life.
Tirzepatide and GLP-1 tolerance: does it wear off?
A common fear is that tirzepatide loses effectiveness over time due to tolerance. Let us look at what the evidence actually says.
Long-term data from SURMOUNT-4 examined what happens when people continue tirzepatide beyond the initial weight loss phase. At 88 weeks, 89.5% of participants receiving tirzepatide maintained at least 80% of the weight loss achieved during the lead-in period. This is strong evidence against the idea that the medication simply stops working.
What does happen is that weight loss transitions from rapid loss to maintenance. This is expected. Once you reach a new equilibrium between your reduced caloric intake and your reduced caloric expenditure, weight stabilizes. This is not tolerance. It is physics. You have reached a new set point where energy in equals energy out.
True pharmacological tolerance, where the same dose produces progressively less receptor activation, has not been demonstrated with tirzepatide in clinical trials. The appetite suppression may feel less dramatic over time because you have adapted psychologically to feeling less hungry. But the physiological effects on gastric emptying, insulin sensitivity, and fat oxidation persist.
When people stop tirzepatide
The SURMOUNT-4 trial also showed what happens when tirzepatide is discontinued. Participants who switched to placebo after the initial weight loss period regained a significant portion of lost weight. This confirms that the medication is still actively working, since stopping it leads to weight regain. If it had truly stopped working, there would be no difference between staying on it and stopping. The semaglutide withdrawal experience is similar and provides useful context for understanding GLP-1 medication discontinuation.
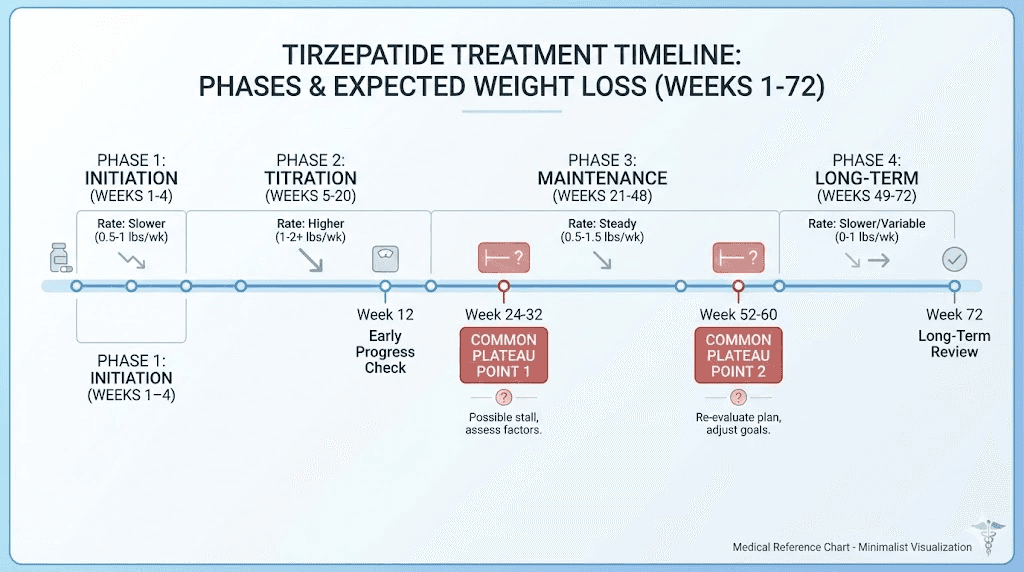
Specific troubleshooting by timeframe
Where you are in your tirzepatide journey determines the most likely cause of your stall. Here is a targeted troubleshooting guide based on timing.
Stall in weeks 1 through 8 (early treatment)
Most likely cause: sub-therapeutic dose. You are still at 2.5mg or 5mg, which are titration doses, not fully therapeutic doses. Action: be patient. Continue titrating up on schedule. Focus on building good habits around protein, exercise, and sleep while the medication ramps up.
Stall in weeks 8 through 16 (mid-treatment)
Most likely causes: dose still needs to increase, protein intake is too low, or you are not exercising. Action: audit protein intake, add strength training if not already doing it, discuss dose escalation with your provider. Check how your experience compares to normal appetite suppression timelines.
Stall in weeks 16 through 36 (established treatment)
Most likely causes: metabolic adaptation, muscle loss, lifestyle factors (sleep, stress, alcohol), or underlying medical conditions. Action: implement the full action plan above. Get bloodwork done. Consider whether you need a higher dose or have reached a natural plateau that will resolve with time.
Stall beyond week 36 (late treatment)
Most likely cause: you have reached or are approaching your body's new equilibrium. Weight loss naturally slows as you get lighter. At this point, you may have lost 15 to 20% of your starting weight, which is an exceptional outcome even though it does not feel like it. Action: focus on body composition rather than scale weight. Intensify strength training. Consider that maintenance, not further loss, may be the appropriate goal. Discuss expectations with your provider.
What the late responder data tells us
Perhaps the most reassuring finding from the SURMOUNT-1 post-hoc analysis is the late responder data.
Participants who had less than 5% weight loss by week 12 were classified as late responders. The analysis found that 90% of these late responders ultimately achieved clinically meaningful weight loss by week 72. The average time for late responders to reach 5% weight loss was approximately 25 weeks.
This means that even if you are 12 weeks in with disappointing results, the odds are overwhelmingly in your favor. Nine out of ten people in your exact situation went on to achieve meaningful results. They just needed more time.
The late responder data also showed that while late responders achieved somewhat less total weight loss than early responders, the clinical significance was still substantial. These were not people losing a trivial amount of weight. They were achieving outcomes that meaningfully improved their health markers, mobility, and quality of life.
Tracking progress beyond the scale
If you take one thing from this entire article, let it be this: the scale is the least reliable measure of progress during tirzepatide treatment.
Here is what you should track instead:
Waist circumference. This correlates more strongly with metabolic health improvements than body weight. Measure at the navel, same spot every time, first thing in the morning. A decrease in waist circumference while weight is stable means you are losing visceral fat and gaining lean tissue. That is a win.
How clothes fit. Your jeans do not lie. If they are getting looser but the scale is flat, your body is changing in exactly the right direction.
Energy levels. Are you sleeping better? Moving more easily? Getting through the day without afternoon crashes? These reflect genuine health improvements that the scale cannot capture.
Bloodwork. HbA1c, fasting glucose, lipid panel, inflammatory markers, and liver enzymes should all improve with effective tirzepatide treatment. These improvements often precede visible weight loss and represent the most important health outcomes.
Strength and fitness. If you can walk farther, lift more, or climb stairs more easily, your body is changing regardless of what the number says.
Progress photos. Take front, side, and back photos monthly in the same clothing and lighting. Visual changes are often dramatic even when the scale appears stalled.
When to consider switching medications
If you have genuinely tried everything in this article, given each intervention adequate time (at least 12 to 16 weeks at maximum dose with optimized lifestyle factors), and still are not seeing results, it may be time to discuss alternatives.
Options include switching to semaglutide, as different GLP-1 medications can produce different responses in different people. Switching from tirzepatide to semaglutide is well-documented and some people respond better to one than the other. Retatrutide, a triple agonist targeting GIP, GLP-1, and glucagon receptors, is showing even more impressive weight loss results in clinical trials and may become available in the near future. Your provider might also consider combination approaches using multiple mechanisms of action.
The key point: not responding to tirzepatide does not mean you are destined to remain at your current weight. It means this particular tool is not the right fit, and there are other tools available.
Frequently asked questions
How long should I wait before worrying about a tirzepatide plateau?
At minimum, give yourself 12 to 16 weeks at a therapeutic dose, typically 10mg or higher, before concluding that tirzepatide is not working. Weight loss in the first 4 to 8 weeks on lower titration doses is often minimal and this is expected. The SURMOUNT-1 trial data shows that late responders can take up to 25 weeks to achieve clinically meaningful results, so patience is critical. Check the complete tirzepatide timeline for week-by-week expectations.
Can I take supplements to break through my tirzepatide plateau?
No supplement can replace the fundamentals of adequate protein, resistance training, sufficient sleep, and stress management. However, certain supplements may help support your overall health during weight loss. B12 supplementation is commonly recommended with GLP-1 medications since absorption may be affected. A basic multivitamin covers potential gaps from reduced food intake. Protein powder counts as a supplement and is genuinely useful for meeting protein targets. Be skeptical of any product claiming to "boost" tirzepatide effectiveness.
Is it normal to not lose weight the first month on tirzepatide?
Yes, completely normal. The first four weeks at 2.5mg are a titration phase, not a treatment phase. Many people see zero weight loss at this dose. Some even gain a small amount due to water retention. This is not an indication that the medication will not work. The real results typically begin appearing at 5mg to 7.5mg and accelerate at 10mg and above. The complete dose chart outlines what to expect at each level.
Should I eat less to lose weight faster on tirzepatide?
Not necessarily, and severe restriction can backfire. Eating too little, especially too little protein, accelerates muscle loss, which slows metabolism and makes plateaus worse. The goal is a moderate caloric deficit with high protein, not starvation. Most successful tirzepatide users eat between 1,200 and 1,800 calories daily depending on their size, with at least 80 to 100 grams of protein. Extreme calorie restriction below 1,000 calories daily is counterproductive and can be dangerous.
Does tirzepatide stop working after a while?
No. Clinical data from long-term trials shows that tirzepatide continues to be effective for weight maintenance well beyond the initial loss period. What changes is the rate of loss: rapid in the first several months, then gradually slowing as you approach a new equilibrium. This slowing is physics, not tolerance. The medication is still reducing appetite, improving insulin sensitivity, and increasing fat oxidation. Stopping the medication typically leads to weight regain, confirming it remains active. Read about appetite suppression timelines for more detail.
Can I combine tirzepatide with other weight loss medications?
Some providers do prescribe combination approaches, but this should only be done under close medical supervision. Common combinations include tirzepatide with metformin for insulin resistance, or with phentermine for additional appetite suppression during plateaus. Never add medications on your own. The interactions with tirzepatide combinations require medical oversight to manage safely.
How much weight should I realistically expect to lose on tirzepatide?
Clinical trial averages show 16% to 22.5% of starting body weight over 72 weeks, depending on dose. For a 250-pound person, that is 40 to 56 pounds. For a 200-pound person, 32 to 45 pounds. Individual results vary significantly based on starting weight, dose, lifestyle factors, and genetics. Some people exceed trial averages. Others fall below. Real before and after results provide a realistic range of outcomes.
External resources
SURMOUNT-1 Trial Full Results, New England Journal of Medicine
Body Composition Changes During Tirzepatide Weight Reduction, PMC
For researchers serious about optimizing their weight loss protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized protocol builders, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed dosing protocols, dosage calculators, and expert guidance tailored to your specific situation.
In case I do not see you, good afternoon, good evening, and good night. May your scale keep trending downward, your protein stay high, and your patience stay stronger than any plateau.