Mar 18, 2026

Tired of conflicting advice about fiber and GLP-1 medications? You are not alone. Every forum, every blog, every well-meaning friend has a different opinion on which fiber supplement works best with semaglutide or tirzepatide. Some say psyllium. Others swear by inulin. A few insist you do not need supplements at all.
Here is the problem with that advice. It is generic.
GLP-1 receptor agonists change the way your digestive system operates. They slow gastric emptying, alter gut motility, and shift the bacterial landscape of your intestines. The fiber that worked perfectly before you started your semaglutide protocol might now cause painful bloating, excessive gas, or make your constipation even worse. What your body needs from fiber has fundamentally changed, and most guides fail to account for this reality.
This guide does not deal in generalities. It examines every major fiber supplement through the specific lens of GLP-1 pharmacology, gut motility changes, and the real-world experiences of thousands of researchers navigating these exact challenges. You will find specific dosages, timing protocols, head-to-head comparisons, and troubleshooting strategies that account for the unique digestive environment GLP-1 medications create. Whether you are dealing with stubborn constipation, trying to protect your gut microbiome, or simply looking to hit your daily fiber targets while eating less food, the right supplement choice can make or break your experience on these medications.
SeekPeptides members consistently report that getting fiber supplementation right is one of the most impactful changes they make during their GLP-1 protocols. And the data backs them up.
Why fiber matters more on GLP-1 medications
Most people think of fiber as a simple digestive aid. Eat more fiber, stay regular. But when you introduce a GLP-1 receptor agonist into the equation, fiber becomes something far more strategic.
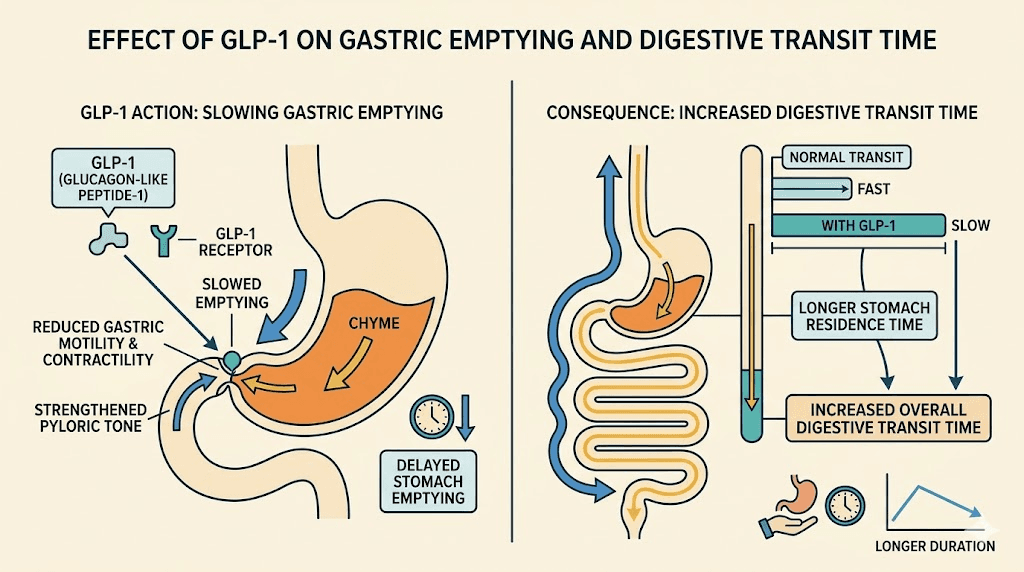
GLP-1 medications like semaglutide and tirzepatide work by mimicking the incretin hormone GLP-1, which signals your brain to reduce appetite and tells your stomach to slow down. That delayed gastric emptying is part of why these medications work so well for weight loss. Food stays in your stomach longer. You feel full faster. You eat less.
But slower digestion creates a cascading effect through your entire gastrointestinal tract.
When your stomach empties more slowly, everything downstream slows too. Transit time through the small intestine extends. Colonic motility decreases. Water absorption from stool increases because content sits in the colon longer. The result? Constipation affects between 15% and 25% of people taking GLP-1 medications, according to clinical trial data. Some studies put the number closer to 40% when you include mild cases that people do not always report to their healthcare providers.
This is where fiber becomes critical. But not just any fiber. The type, amount, timing, and form all matter in ways they simply did not before you started your GLP-1 protocol.
The three roles fiber plays during GLP-1 therapy
Fiber does not just prevent constipation. On GLP-1 medications, it serves three distinct functions that directly impact your results.
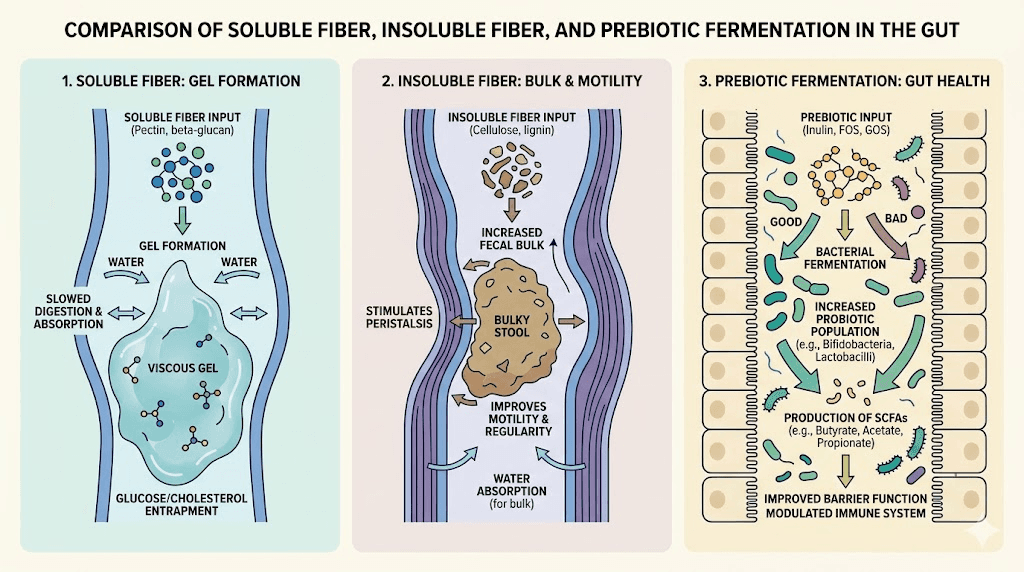
Role 1: Mechanical bulk and motility. Insoluble fiber adds physical bulk to stool and stimulates the stretch receptors in your colon wall. These receptors trigger peristaltic contractions, the wave-like muscle movements that push content through your intestines. When GLP-1 medications slow those natural contractions, insoluble fiber helps compensate by providing the mechanical stimulus your colon needs to keep moving. Without adequate bulk, stool can sit in the colon for days, leading to the hard, dry, difficult-to-pass bowel movements that many semaglutide users report.
Role 2: Gel formation and water retention. Soluble fiber dissolves in water and forms a viscous gel in your digestive tract. This gel performs multiple functions simultaneously. It softens stool by holding water in the intestinal lumen, preventing the excessive drying that happens when transit time slows. It also modulates the rate of nutrient absorption, which can help stabilize blood sugar levels already being managed by your GLP-1 medication. And it provides a physical matrix that helps food and waste move more smoothly through a slower-moving system.
Role 3: Prebiotic fermentation and microbiome support. Certain fibers serve as food for beneficial gut bacteria. When these bacteria ferment fiber, they produce short-chain fatty acids like butyrate, propionate, and acetate. These compounds do far more than support digestive comfort. They strengthen the intestinal barrier, reduce inflammation, and, perhaps most relevant for GLP-1 users, they actually stimulate natural GLP-1 secretion from L-cells in the gut. Research published in the Journal of Nutrition found that pectin-containing soluble fiber improved postprandial glycemic control likely through increased endogenous GLP-1 release. So the right fiber can actually complement your medication rather than just manage its side effects.
Why your pre-medication fiber routine probably will not work anymore
If you were eating a high-fiber diet or taking fiber supplements before starting semaglutide or tirzepatide, you might assume you can continue exactly as before. This assumption leads to problems for two reasons.
First, you are almost certainly eating less food. That means less dietary fiber from whole food sources, even if you are making excellent food choices. A person eating 2,200 calories might easily hit 30 grams of fiber from meals alone. Drop to 1,400 calories, which is common on GLP-1 medications, and hitting that same target becomes nearly impossible without supplementation.
Second, the delayed gastric emptying changes how fiber behaves in your system. Highly fermentable fibers like inulin and fructooligosaccharides can cause significantly more gas and bloating when transit time is already extended. What previously caused mild fullness might now trigger uncomfortable bloating, excessive burping, or even nausea on top of the side effects your medication already produces.
Understanding fiber types: what actually matters for GLP-1 users
Not all fiber is created equal. This is true in general nutrition, but it becomes critically important when your digestive system is operating under the influence of GLP-1 receptor agonists. Understanding the differences between fiber types will save you weeks of uncomfortable trial and error.
Soluble fiber: the gel formers
Soluble fiber dissolves in water. When it hits liquid in your digestive tract, it forms a gel-like substance that moves through your system with relative smoothness. This category includes psyllium husk, beta-glucan from oats, pectin from fruits, and guar gum.
For GLP-1 users, soluble fiber offers several specific advantages. The gel it forms softens stool without adding excessive bulk, which matters when your system is already processing food more slowly. It holds water in the intestinal lumen, counteracting the increased water absorption that comes with extended transit time. And certain soluble fibers, particularly psyllium, have been shown to normalize stool consistency in both directions, helping with constipation AND diarrhea depending on what your body needs.
The downside? Some soluble fibers are highly fermentable, meaning gut bacteria break them down rapidly and produce significant gas in the process. On a GLP-1 medication that already slows gas transit, this can create serious bloating and discomfort.
Insoluble fiber: the bulk builders
Insoluble fiber does not dissolve in water. Think wheat bran, cellulose, lignin, and the tough outer layers of vegetables and grains. It passes through your digestive system largely intact, adding physical bulk to stool and stimulating peristalsis through mechanical contact with intestinal walls.
For GLP-1 users dealing with constipation, insoluble fiber can be a double-edged sword. On one hand, the mechanical stimulation it provides is exactly what a sluggish colon needs. On the other hand, adding too much bulk to a system that is already moving slowly can make things worse, not better. Think of it like adding more cars to an already congested highway. More volume does not help if the throughput is the bottleneck.
The key with insoluble fiber on GLP-1 medications is moderation and hydration. Small amounts combined with adequate water can be very effective. Large amounts without sufficient fluid will almost certainly make constipation worse.
Prebiotic fiber: the microbiome feeders
Prebiotic fibers are a specific subset of fibers, usually soluble and fermentable, that selectively feed beneficial gut bacteria. Inulin, fructooligosaccharides (FOS), galactooligosaccharides (GOS), and resistant starch all fall into this category.
The relationship between prebiotic fiber and GLP-1 therapy is complex and genuinely fascinating. Research shows that GLP-1 agonists themselves alter the gut microbiome, increasing populations of Bacteroidetes and Prevotella, bacteria that excel at fermenting dietary fibers. Adding prebiotic fiber can support this shift, potentially amplifying the metabolic benefits of your medication. A randomized, double-blind, placebo-controlled crossover trial found that prebiotics increased postprandial GLP-2 and improved glucose regulation in patients with type 2 diabetes.
But timing matters enormously. Introducing prebiotic fiber too early in your GLP-1 protocol, before your body has adjusted to the medication, can intensify gastrointestinal side effects significantly. Most practitioners recommend waiting at least 4 to 8 weeks after starting your semaglutide or tirzepatide before introducing prebiotic supplements.
The best fiber supplements for GLP-1 users, ranked
After reviewing the clinical evidence, analyzing community experiences, and examining how each fiber type interacts with GLP-1 pharmacology, here are the top fiber supplements ranked by their overall suitability for people on these medications.
1. Psyllium husk: the gold standard
Psyllium husk earns the top spot for good reason. It is the most studied fiber supplement in the context of gastrointestinal management, and its properties align almost perfectly with what GLP-1 users need.
Psyllium is a soluble, gel-forming fiber derived from the seed husks of Plantago ovata. Unlike many soluble fibers, it is only partially fermented by gut bacteria. This is crucial. It means you get the stool-softening and water-holding benefits of a soluble fiber without the excessive gas production that fully fermentable fibers cause. The American College of Gastroenterology specifically recommends psyllium for managing IBS symptoms, and it remains the only isolated fiber supplement to earn that distinction.
For GLP-1 users, psyllium works in both directions. Constipated? The gel absorbs water and softens stool. Experiencing the loose stools that some people get, particularly with retatrutide? Psyllium absorbs excess water and adds form to stool. This bidirectional action makes it uniquely versatile.
Recommended starting dose: 3.4 grams (approximately one tablespoon or one standard dose of Metamucil) once daily.
Target dose: 5 to 10 grams daily, split into two doses.
Timing: Take at least 30 minutes before meals or 2 hours after. For people on oral semaglutide, maintain the standard 30-minute fasting window before taking any fiber supplement.
Onset of benefit: Most users notice improvement within 2 to 3 days of consistent use.
Forms available: Whole husks, powder (Metamucil, generic psyllium), capsules. Whole husks are least processed and typically cause fewer additives-related issues. Powder mixes more easily into water or protein shakes. Capsules are convenient but require more pills to reach therapeutic doses.
Watch out for: Always take with at least 8 ounces of water. Psyllium without adequate fluid can form a dense mass that worsens constipation or, in rare cases, causes esophageal obstruction. On GLP-1 medications where you might already struggle with reduced fluid intake, this is especially important to remember.
2. Methylcellulose: the gentle alternative
Methylcellulose is a synthetic, non-fermentable, soluble fiber. It is the primary ingredient in Citrucel. And for GLP-1 users who cannot tolerate psyllium or who experience significant gas and bloating, it is an excellent option.
The defining characteristic of methylcellulose is what it does not do. It does not ferment. At all. Gut bacteria cannot break it down, which means zero gas production, zero bloating, and zero of the cramping that fermentable fibers can cause. For someone already managing acid reflux or sulfur burps from their GLP-1 medication, this non-fermentable property is not just convenient. It is essential.
Methylcellulose works by absorbing water and forming a smooth gel that eases stool passage. It is gentler than psyllium, which makes it a good starting point for people who are sensitive to fiber supplements in general.
Recommended starting dose: 2 grams daily (one standard Citrucel dose).
Target dose: 4 to 6 grams daily, split into two or three doses.
Timing: Can be taken with or between meals. Space at least 1 hour from medications.
Onset of benefit: 1 to 3 days for most users.
Drawback: Methylcellulose provides no prebiotic benefit. It passes through your system without feeding beneficial bacteria. If microbiome support is a priority, you may need to combine it with a small amount of prebiotic fiber once your system stabilizes.
3. Acacia fiber (gum arabic): the low-fermentation prebiotic
Acacia fiber occupies a unique middle ground that makes it particularly interesting for GLP-1 users. It is a soluble fiber that also functions as a prebiotic, but unlike inulin or FOS, it ferments very slowly. This slow fermentation means it feeds beneficial gut bacteria without producing the rapid gas buildup that faster-fermenting prebiotics cause.
Research shows acacia fiber increases populations of Bifidobacteria and Lactobacilli, both associated with improved digestive health and reduced inflammation. For GLP-1 users who want microbiome support without the gastrointestinal drama, acacia fiber is worth serious consideration. It blends easily into water without thickening significantly, has almost no taste, and is generally well tolerated even by people with sensitive digestive systems.
Recommended starting dose: 5 grams daily.
Target dose: 10 to 15 grams daily, increased gradually over 2 to 3 weeks.
Timing: Can be mixed into any liquid and taken at any time. Works well in morning breakfast smoothies or post-dinner beverages.
Onset of benefit: Prebiotic effects develop over 2 to 4 weeks. Stool improvement may take 5 to 7 days.
Best for: GLP-1 users who want prebiotic benefits without the bloating risk of inulin. People who have been on their medication for 4 or more weeks and have stable gastrointestinal function. Those taking other supplements alongside their GLP-1 and want to minimize interactions.
4. Partially hydrolyzed guar gum (PHGG): the clinical performer
PHGG is a soluble fiber that has been extensively studied in clinical settings for managing both constipation and diarrhea. It is derived from guar gum but processed to remove the excessive thickening properties that make regular guar gum impractical as a daily supplement.
What makes PHGG stand out is its clinical evidence base. Studies have shown it to be effective for functional constipation, IBS, and post-surgical digestive recovery. It ferments slowly and produces significant amounts of butyrate, a short-chain fatty acid that plays a crucial role in maintaining colonic health and reducing intestinal inflammation.
For GLP-1 users, PHGG offers a combination of gentle stool regulation and meaningful prebiotic activity. It dissolves completely in water without changing the taste or texture significantly, making it one of the easiest fiber supplements to incorporate into a daily routine. The brand Sunfiber is the most widely available PHGG product.
Recommended starting dose: 3 grams daily.
Target dose: 5 to 7 grams daily.
Timing: Flexible. Can be added to any food or drink without altering consistency.
Onset of benefit: Stool improvement within 3 to 5 days. Full prebiotic benefits develop over 2 to 4 weeks.
5. Calcium polycarbophil: the controlled releaser
Calcium polycarbophil (sold as FiberCon) is a synthetic fiber that absorbs water in a controlled, predictable manner. Like methylcellulose, it is non-fermentable, meaning no gas or bloating. Unlike methylcellulose, it is available primarily in tablet form, which some users find more convenient than mixing powders.
Its controlled water absorption means it adapts to intestinal conditions. In a dry environment (constipation), it absorbs water and softens stool. In a wet environment (diarrhea), it absorbs excess liquid. This adaptability makes it useful for GLP-1 users who experience alternating symptoms, which is more common than most guides acknowledge. Some weeks you might deal with constipation from slowed motility. Other weeks, particularly after dose increases, you might experience loose stools. Calcium polycarbophil handles both.
Recommended starting dose: 1 gram daily (two tablets).
Target dose: 2 to 4 grams daily, split into two to four doses.
Maximum dose: 4 grams daily.
Timing: Take with at least 8 ounces of water. Space away from other medications by at least 1 hour.
6. Glucomannan: the appetite synergist
Glucomannan is a soluble fiber derived from the konjac root. It has the highest water-holding capacity of any dietary fiber, expanding up to 50 times its dry weight when exposed to liquid. This extreme expansion is both its superpower and its risk.
For GLP-1 users, glucomannan can complement the appetite-suppressing effects of medications like semaglutide and tirzepatide by creating additional stomach volume. Some users report that taking glucomannan before meals enhances the fullness signal their GLP-1 medication already provides.
However, caution is warranted. On a medication that already slows gastric emptying, adding a fiber that expands dramatically in the stomach can cause significant discomfort, nausea, or even exacerbate bloating symptoms. Start with very small doses and increase slowly. Never take glucomannan tablets, which can swell in the esophagus. Always use the powder form mixed into liquid.
Recommended starting dose: 500 mg (0.5 grams) once daily, mixed in a full glass of water.
Target dose: 1 to 3 grams daily, split into two or three doses before meals.
Critical safety note: Always take with at least 12 ounces of water. Never take in capsule form if you have any swallowing difficulties.
7. Inulin and FOS: the powerful prebiotics (use with caution)
Inulin and fructooligosaccharides are the most researched prebiotic fibers. They powerfully stimulate growth of Bifidobacteria and have demonstrated benefits for insulin sensitivity, mineral absorption, and immune function. The Pendulum GLP-1 Probiotic and similar products often include these prebiotic fibers as part of their formulations.
The problem for GLP-1 users is fermentation speed. Inulin and FOS ferment rapidly, producing significant volumes of hydrogen and carbon dioxide gas. In a digestive system with normal motility, this gas passes relatively quickly. In a system slowed by GLP-1 medication, that gas gets trapped, leading to distension, cramping, and pain. Many users who try inulin supplements early in their GLP-1 protocols report it as one of the most uncomfortable supplement experiences they have had.
That said, inulin has a role for established GLP-1 users. If you have been on your medication for 3 or more months, your gastrointestinal system has largely adapted, and you tolerate other fiber supplements well, introducing a small amount of inulin can provide meaningful microbiome support. The key is patience and very gradual introduction.
Recommended starting dose: 2 grams daily, only after at least 8 weeks on your GLP-1 medication.
Target dose: 5 to 10 grams daily, increased by 1 to 2 grams per week.
Best timing: With a meal, never on an empty stomach.
Head-to-head comparison: choosing the right fiber for your situation
Numbers tell the story better than paragraphs sometimes. This table compares every major fiber supplement across the factors that matter most for GLP-1 users.
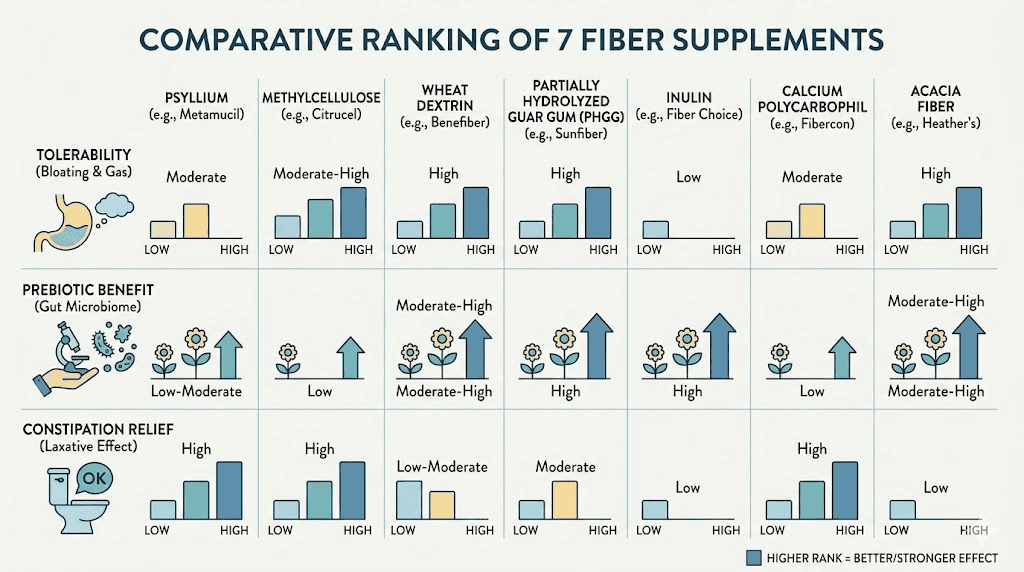
Fiber Supplement | Solubility | Fermentability | Prebiotic | Gas/Bloating Risk | Constipation Relief | Best For |
|---|---|---|---|---|---|---|
Psyllium husk | Soluble | Low | Minimal | Low | Excellent | Most GLP-1 users |
Methylcellulose | Soluble | None | None | Very low | Good | Sensitive stomachs |
Acacia fiber | Soluble | Low-moderate | Yes | Low | Moderate | Microbiome support |
PHGG (Sunfiber) | Soluble | Low-moderate | Yes | Low | Good | IBS overlap |
Calcium polycarbophil | Synthetic | None | None | Very low | Good | Alternating symptoms |
Glucomannan | Soluble | Moderate | Yes | Moderate | Good | Extra satiety |
Inulin/FOS | Soluble | High | Strong | High | Moderate | Established users only |
Wheat bran | Insoluble | Low | Minimal | Low | Moderate | Mild constipation |
Resistant starch | Insoluble | Moderate | Yes | Moderate | Low | Blood sugar management |
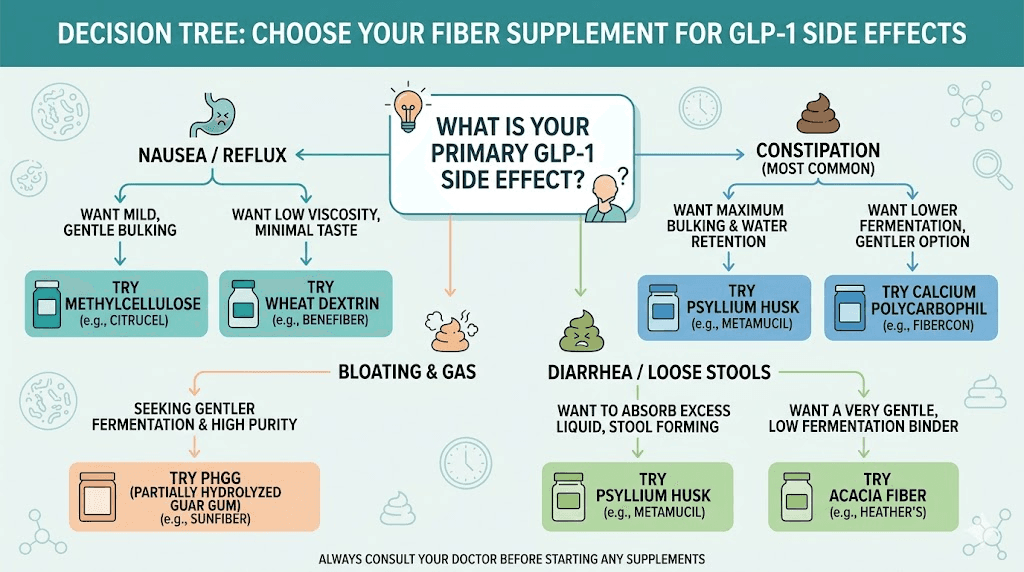
If your primary issue is constipation
Start with psyllium husk. It is the single most effective fiber supplement for managing constipation on GLP-1 medications. Begin with one dose daily and increase to two doses after a week if needed. If psyllium causes any discomfort, switch to methylcellulose. If neither provides adequate relief after 2 weeks of consistent use at full dose, consider adding a magnesium supplement alongside your fiber rather than increasing fiber further.
The combination of psyllium and magnesium citrate addresses constipation from two different mechanisms: psyllium adds bulk and holds water in the stool, while magnesium draws additional water into the intestine through osmosis. Together, they are more effective than either alone.
If your primary issue is bloating and gas
Choose methylcellulose or calcium polycarbophil. Both are non-fermentable, meaning they will not add to the gas production your GLP-1 medication may already be causing. Avoid inulin, FOS, and high doses of acacia fiber until your bloating is under control.
Many GLP-1 users find that bloating improves significantly after the first 4 to 6 weeks on their medication. Once your system stabilizes, you can gradually introduce a low-fermentation prebiotic like acacia fiber if you want microbiome support.
If you want microbiome support
Acacia fiber or PHGG are your best options. Both provide meaningful prebiotic benefits with manageable fermentation. Start with acacia fiber at 5 grams daily and increase gradually. If you are also taking a probiotic supplement, the combination of probiotic bacteria and prebiotic fiber creates what researchers call a synbiotic effect, where each enhances the other.
For maximum microbiome impact, consider a two-phase approach. Phase one (weeks 1 through 4): establish baseline digestive stability with psyllium or methylcellulose. Phase two (weeks 5 and beyond): introduce acacia fiber or PHGG while maintaining your baseline fiber supplement.
If you want appetite support
Glucomannan provides the most appetite-related benefit due to its extreme water-holding capacity. However, use it cautiously on GLP-1 medications. The combination of medication-induced delayed gastric emptying and glucomannan expansion can cause significant nausea if doses are too high.
A safer approach is to use psyllium before meals. It provides moderate stomach volume without the extreme expansion of glucomannan, and it comes with the additional benefit of constipation management. SeekPeptides members frequently report that timing psyllium 20 to 30 minutes before their largest meal helps them feel satisfied with smaller portions.
Dosing protocols: how to introduce fiber on GLP-1 medications
The single biggest mistake GLP-1 users make with fiber supplements is starting too aggressively. Your digestive system is already adapting to a powerful medication. Adding a significant dose of fiber on top of that adaptation process is a recipe for discomfort.
The low-and-slow introduction protocol
This protocol works for any fiber supplement and accounts for the reduced motility that GLP-1 medications cause.
Week 1: Start at 25% of the target dose, once daily. For psyllium, this means approximately 1.5 grams (half a standard dose). Take it at the same time each day, with a full glass of water.
Week 2: If week 1 was tolerated well, increase to 50% of the target dose. For psyllium, this means one full standard dose (3.4 grams) once daily.
Week 3: Increase to 75% of the target dose, or split into two daily doses at 50% each. For psyllium, this means approximately 5 grams split between morning and evening.
Week 4: Reach your full target dose. For psyllium, this is 5 to 10 grams daily in two divided doses.
If at any point you experience significant bloating, gas, or worsening constipation, drop back to the previous week dose and stay there for an additional week before trying to increase again. There is no rush. Consistency at a tolerable dose beats intermittent use at a high dose every time.
Timing fiber around GLP-1 injections
Injection day and the day after tend to be when GLP-1 side effects peak. Many users find that semaglutide and tirzepatide produce the most gastrointestinal effects in the 24 to 48 hours following injection.
Consider reducing your fiber dose by 50% on injection day and the day after, particularly during the first 4 to 8 weeks of treatment or after dose increases. This gives your system room to manage the medication effects without the added demand of processing a full fiber dose.
As your body adapts and side effects diminish, you can maintain your full fiber dose through injection days. Most users reach this point by their second or third month on a stable dose.
Timing fiber around meals
When you take fiber relative to meals matters more on GLP-1 medications than it does normally.
Before meals (20 to 30 minutes): This timing maximizes satiety. The fiber begins absorbing water and expanding before food arrives, enhancing the fullness signal your medication already provides. This approach works best with psyllium or glucomannan. Pairing with nutrient-dense foods ensures you get maximum nutritional value from smaller meals.
With meals: This timing works well for prebiotic fibers like acacia or PHGG. Taking them with food slows their fermentation rate, reducing gas production. It also ensures the fiber mixes with food content, creating a more homogeneous bolus that moves through the digestive tract more smoothly.
Between meals (2 or more hours after eating): This timing is best for addressing constipation specifically. Taking fiber between meals with a large glass of water provides maximum hydration to the fiber without competition from food for water absorption. This approach is particularly effective for people whose constipation has not responded adequately to fiber taken with meals.
Before bed: Taking a dose of psyllium or methylcellulose before bed with 8 to 12 ounces of water can help promote a morning bowel movement. The fiber has all night to absorb water and move through the colon. Many tirzepatide users find this timing particularly effective.
Hydration requirements: the non-negotiable factor
Fiber without adequate water makes constipation worse. This is true for everyone, but it is especially critical for GLP-1 users for three reasons.
First, GLP-1 medications reduce appetite for both food and fluids. Many users report simply forgetting to drink water because they do not feel thirsty. Second, reduced food intake means less water from food sources (fruits, vegetables, soups). Third, the delayed gastric emptying gives the colon more time to absorb water from stool, making adequate hydration even more important.
The minimum recommendation: drink at least 8 ounces of water with every fiber supplement dose. The optimal recommendation: increase total daily water intake by 16 to 24 ounces above your baseline when supplementing with fiber. Track your water intake if necessary. Several SeekPeptides community members report that setting hourly water reminders on their phones made a bigger difference in their GLP-1 experience than any single supplement change.
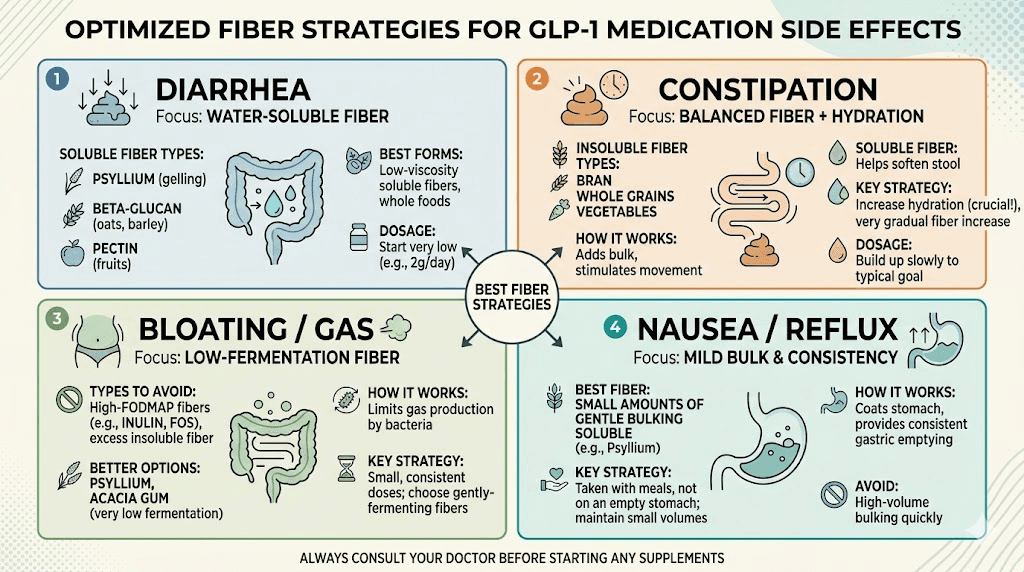
Fiber and common GLP-1 side effects: targeted strategies
Different side effects call for different fiber strategies. What works for constipation may worsen bloating. What helps with diarrhea could slow an already sluggish system. Here is how to match your fiber approach to your specific symptoms.
Managing constipation with fiber
Constipation is the most common reason GLP-1 users turn to fiber supplements. An effective approach combines the right fiber type with proper hydration and timing.
First-line approach: Psyllium husk, 3.4 to 6.8 grams daily in two divided doses, with 8 ounces of water per dose. Take the first dose 30 minutes before breakfast and the second dose before bed.
If psyllium alone is insufficient after 2 weeks: Add magnesium citrate at 200 to 400 mg daily. The combination of bulk-forming fiber and osmotic magnesium addresses constipation from two complementary angles.
If psyllium causes bloating: Switch to methylcellulose at 4 to 6 grams daily. Add gentle physical activity like walking after meals, which stimulates colonic motility independently of fiber.
If constipation is severe: This is beyond what fiber supplements alone can address. Consult your healthcare provider about adding an osmotic laxative like polyethylene glycol (MiraLAX) temporarily while your body adjusts to the medication. Continue fiber supplementation alongside any medical intervention, as fiber provides long-term regulation while laxatives address acute symptoms.
Managing diarrhea with fiber
While constipation gets more attention, diarrhea affects a meaningful percentage of GLP-1 users, particularly during dose titration or when transitioning to newer GLP-1 receptor agonists.
For diarrhea management, psyllium is again the first choice. Its bidirectional action means it absorbs excess water from loose stool, adding form and bulk. Take 3.4 grams with meals (not before meals, as pre-meal timing could worsen loose stools by adding volume to the stomach).
Calcium polycarbophil is an alternative that works through a similar water-absorption mechanism. Its tablet form makes it easy to carry and take with meals when away from home.
Avoid inulin, FOS, and high doses of prebiotic fibers during diarrhea episodes. The rapid fermentation and gas production can exacerbate symptoms and cause additional cramping.
Managing bloating with fiber
If bloating is your primary concern, fiber selection becomes even more critical. The wrong fiber will make bloating dramatically worse.
Safe choices: Methylcellulose (zero fermentation, zero gas), calcium polycarbophil (zero fermentation), psyllium (very low fermentation).
Avoid: Inulin, FOS, GOS, resistant starch, and high-dose acacia fiber until bloating resolves.
Timing tip: Take fiber between meals rather than with meals. This avoids adding bulk to a stomach that is already emptying slowly, which is a primary contributor to the bloating sensation GLP-1 users experience.
Many users find that digestive enzymes taken with meals help reduce bloating independently of fiber choices. The combination of non-fermentable fiber between meals and digestive enzymes with meals can significantly improve comfort.
Managing nausea with fiber
Nausea is the most common GLP-1 side effect overall, and fiber supplements can either help or hurt depending on how they are used.
Fiber can help nausea by stabilizing blood sugar fluctuations that contribute to that queasy feeling. Soluble fiber slows glucose absorption, preventing the rapid swings that can trigger nausea in GLP-1 users, especially between meals.
Fiber can worsen nausea if it adds too much volume to an already slow-emptying stomach. A stomach that cannot move its contents efficiently does not need more bulk.
The solution: use a low-volume, high-impact fiber. PHGG or acacia fiber in small doses (3 to 5 grams) mixed into liquid can provide benefits without significant stomach volume. Avoid psyllium husks or glucomannan on days when nausea is prominent, as their volume-expanding properties can intensify that feeling.
If nausea is a persistent issue, explore comprehensive nausea management strategies alongside your fiber protocol. Anti-nausea foods can also help bridge the gap on difficult days.
Fiber supplements and medication interactions
Fiber supplements can interact with medications, including GLP-1 agonists themselves. Understanding these interactions prevents reduced medication efficacy and unwanted effects.
Fiber and oral semaglutide (Rybelsus)
If you take oral semaglutide, fiber timing becomes critically important. Oral semaglutide must be taken on an empty stomach with no more than 4 ounces of plain water, followed by a 30-minute fasting window. Taking fiber supplements within this window can significantly reduce semaglutide absorption.
Wait at least 30 minutes after taking oral semaglutide before consuming any fiber supplement. Better yet, wait until after your first meal. This ensures the semaglutide has been absorbed before fiber enters the stomach and potentially interferes with the absorption enhancer (SNAC) that oral semaglutide relies on.
Fiber and injectable GLP-1 medications
For injectable semaglutide, tirzepatide, and retatrutide, there is no direct absorption interaction with fiber supplements since the medication enters through subcutaneous injection, bypassing the digestive system entirely. You can take fiber supplements at any time relative to your injection.
However, be mindful that injection days often bring increased gastrointestinal sensitivity. Reducing fiber dose on injection day, as discussed in the timing section, can prevent compounding side effects.
Fiber and other medications
Fiber supplements can reduce the absorption of certain medications taken orally. This is particularly relevant for GLP-1 users who may also be taking:
Thyroid medications (levothyroxine): Take thyroid medication at least 4 hours before or after fiber supplements. Psyllium and other gel-forming fibers can trap thyroid hormone in the gel matrix, significantly reducing absorption.
Metformin: While metformin and fiber can generally be taken together, spacing them by 1 to 2 hours may reduce the gastrointestinal side effects of both. Many GLP-1 users who are transitioning from or combining with metformin find that separating these from fiber supplements improves overall digestive comfort.
Vitamins and minerals: Fiber can reduce absorption of iron, zinc, and calcium when taken simultaneously. If you are taking supplements with your GLP-1 medication, space them at least 2 hours from fiber doses. This is especially important given the reduced caloric intake on GLP-1 medications, which already puts nutritional adequacy at risk.
Blood sugar medications: Soluble fiber can enhance the blood sugar-lowering effect of diabetes medications. If you are taking berberine or other glucose-management supplements alongside your GLP-1 medication, monitor blood sugar carefully when introducing fiber supplements, as the combined effect could cause hypoglycemia.
Building your personalized fiber protocol
No single fiber supplement works optimally for every GLP-1 user. Your ideal protocol depends on your specific symptoms, how long you have been on your medication, your current dose, and your individual digestive response. Here is a framework for building a protocol that works for you.
Phase 1: Foundation (weeks 1 through 4 on GLP-1 medication)
During the initial adjustment period, keep fiber supplementation simple and conservative.
Primary fiber: Psyllium husk OR methylcellulose (choose based on tolerance). Start at minimum dose.
Target intake: 15 to 20 grams total fiber daily (from food and supplements combined).
Focus: Establishing digestive regularity. Preventing severe constipation without adding gastrointestinal stress.
Avoid: Prebiotic fibers, high doses, multiple fiber sources. Your system is adjusting to the medication. Do not overwhelm it.
During this phase, track your bowel movements, any bloating or gas, and hydration. This data will guide your protocol refinements in later phases. Many SeekPeptides members use simple tracking spreadsheets to identify patterns.
Phase 2: Optimization (weeks 5 through 12)
Once your body has adapted to the GLP-1 medication and you have established a baseline fiber routine, you can begin optimizing.
Primary fiber: Continue your foundation fiber at full dose.
Addition: Introduce a prebiotic fiber (acacia or PHGG) at minimum dose. Increase gradually over 2 to 3 weeks.
Target intake: 20 to 30 grams total fiber daily.
Focus: Microbiome support, enhanced digestive function, addressing any remaining symptoms.
This is also the phase where you fine-tune timing. Experiment with before-meal versus between-meal dosing to find what works best for your symptom profile. Keep track of which timing pattern produces the best results.
Phase 3: Maintenance (week 13 and beyond)
By this point, your digestive system has largely adapted to both the medication and fiber supplementation. Your protocol should be well-established and producing consistent results.
Primary fiber: Your chosen foundation fiber at a stable dose.
Prebiotic: Acacia, PHGG, or low-dose inulin at a stable dose.
Target intake: 25 to 35 grams total fiber daily (approaching general population recommendations).
Focus: Long-term health, metabolic optimization, comfortable maintenance.
Adjustments in this phase are typically minor. If you experience dose increases in your GLP-1 medication, temporarily reduce fiber intake by 25 to 50% for 1 to 2 weeks while your system adapts, then return to your maintenance protocol.
The combination approach: building a fiber stack
Many experienced GLP-1 users find that combining two complementary fibers produces better results than relying on a single source. Here are the most effective combinations based on community feedback and clinical logic.
Combination 1: Psyllium plus acacia fiber. The most popular combination among long-term GLP-1 users. Psyllium handles constipation management and stool regulation. Acacia provides prebiotic support with minimal gas. Take psyllium morning and evening. Take acacia with lunch or mixed into an afternoon beverage.
Combination 2: Methylcellulose plus PHGG. Ideal for sensitive digestive systems. Methylcellulose provides zero-gas constipation relief. PHGG adds gentle prebiotic support. Both dissolve easily in water with minimal taste or texture changes.
Combination 3: Psyllium plus glucomannan. For users who want both digestive regulation and appetite support. Take psyllium in the morning and before bed for constipation management. Take a low dose of glucomannan 20 to 30 minutes before your largest meal for satiety enhancement. Be cautious with this combination and ensure adequate hydration, as both fibers are significant water absorbers.
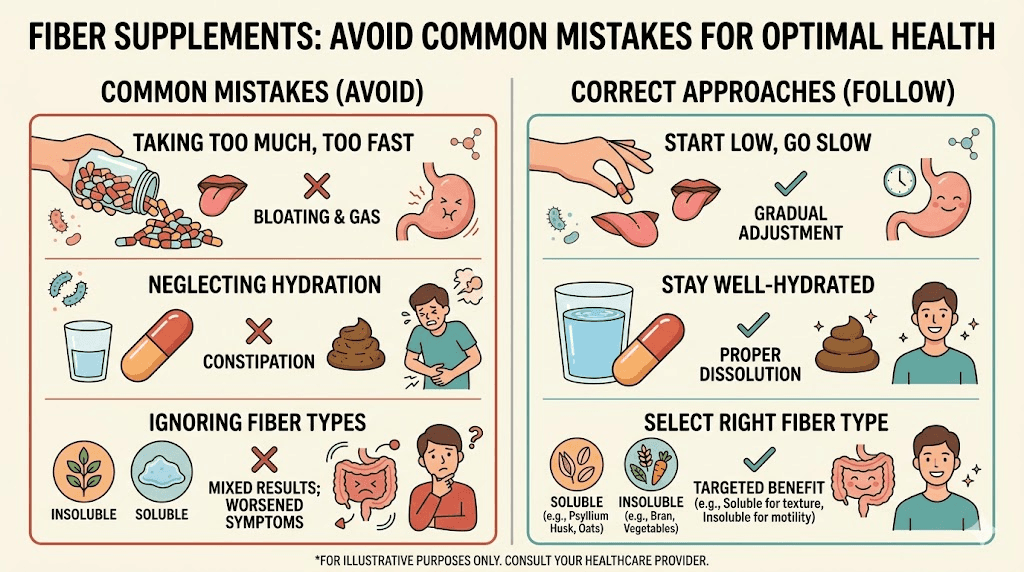
Common mistakes GLP-1 users make with fiber supplements
After analyzing thousands of community discussions, clinical reports, and user experiences, these are the most frequent and impactful mistakes.
Mistake 1: Starting too much, too fast
The most common error by a wide margin. A person starts their GLP-1 medication, experiences constipation within the first week, panics, and immediately begins taking full doses of a fiber supplement. The result is usually worse bloating, more discomfort, and the mistaken conclusion that fiber supplements do not work for them.
The fix: Follow the low-and-slow protocol. Start at 25% of the target dose and increase weekly. Patience is not optional here.
Mistake 2: Insufficient water intake
Taking fiber without adequate water is like adding cement without mixing it. The fiber sits in your digestive tract, absorbing whatever moisture is available, potentially creating a dense, hard mass that worsens constipation significantly. This is especially problematic on GLP-1 medications where fluid intake tends to decrease naturally.
The fix: Drink at least 8 ounces of water with every fiber dose. Add 16 to 24 ounces to your daily total when supplementing with fiber. Set reminders if necessary.
Mistake 3: Choosing high-fermentation fibers first
Inulin and FOS supplements are heavily marketed as gut health solutions. They are also the worst first choice for GLP-1 users. Their rapid fermentation in a slow-moving digestive system produces significant gas, bloating, and discomfort that can persist for days.
The fix: Start with low-fermentation options (psyllium, methylcellulose, calcium polycarbophil). Only introduce prebiotic fibers after your system has stabilized on both your medication and a baseline fiber supplement.
Mistake 4: Ignoring fiber-medication timing
Taking fiber supplements at the same time as other oral medications can significantly reduce medication absorption. This is particularly dangerous with thyroid medications and blood sugar management drugs, where consistent dosing is critical.
The fix: Space fiber supplements at least 2 hours from other medications. For thyroid medications, maintain a 4-hour gap.
Mistake 5: Relying solely on fiber for severe constipation
Fiber is a regulatory tool, not a rescue intervention. If you have gone 4 or more days without a bowel movement, fiber alone is unlikely to resolve the situation. Adding fiber to an already impacted system can actually worsen discomfort.
The fix: For acute constipation, use an osmotic laxative (MiraLAX) or magnesium citrate to address the immediate problem. Then establish a preventive fiber routine to avoid recurrence. Consult your healthcare provider if severe constipation persists.
Mistake 6: Stopping fiber during side effect flares
When GLP-1 side effects intensify, especially after dose increases, many users stop all supplements including fiber. This often leads to a cycle where constipation worsens during the very period when their body is already under stress from the higher dose.
The fix: Reduce fiber dose by 50% during side effect flares rather than stopping completely. Maintain at least a minimum amount to prevent constipation from compounding other symptoms.
Special considerations for different GLP-1 medications
While the general principles of fiber supplementation apply across all GLP-1 receptor agonists, there are nuances worth noting for specific medications.
Fiber considerations for semaglutide (Ozempic, Wegovy)
Semaglutide is the most widely prescribed GLP-1 receptor agonist, and its side effect profile is well documented. Constipation occurs in approximately 15% to 20% of users at maintenance doses. Nausea is more common than constipation, especially during dose escalation.
For semaglutide users, psyllium is typically the best first-line fiber choice. Its low fermentation reduces the risk of adding nausea-triggering gas to an already sensitive stomach. Starting at the lowest dose on the day of injection and the day after helps manage the peak side effect window.
Semaglutide users who experience the sulfur burp phenomenon should be especially cautious with fermentable fibers, as these can exacerbate the issue.
Fiber considerations for tirzepatide (Mounjaro, Zepbound)
Tirzepatide is a dual GIP/GLP-1 receptor agonist with a slightly different side effect profile than pure GLP-1 agonists. Constipation rates are comparable to semaglutide, but tirzepatide users often report more intense initial gastrointestinal symptoms that tend to resolve more quickly as the medication takes effect.
The dual receptor action means tirzepatide affects gastric emptying and intestinal motility through two pathways simultaneously. Some users find that they need slightly higher fiber doses than semaglutide users to achieve the same constipation relief, particularly at higher tirzepatide doses.
The phased introduction protocol is especially important with tirzepatide. Give your body time to adjust to the dual receptor activation before adding significant fiber supplementation.
Fiber considerations for retatrutide
Retatrutide is a triple agonist (GLP-1/GIP/glucagon receptor) with a more complex gastrointestinal impact than either semaglutide or tirzepatide alone. Early clinical data suggests higher rates of gastrointestinal side effects overall, with both constipation and diarrhea being common, sometimes alternating in the same user.
For retatrutide users, the bidirectional action of psyllium becomes particularly valuable. A fiber that can address both constipation and diarrhea without needing to switch products is exactly what the variable gastrointestinal picture of retatrutide demands.
Start very conservatively with fiber on retatrutide. The triple agonist mechanism creates more gastrointestinal variability, making it harder to predict how your system will respond to added fiber.
Fiber considerations for oral semaglutide
As discussed in the medication interactions section, oral semaglutide has specific timing requirements that affect fiber supplementation. The 30-minute fasting window after oral semaglutide must be respected absolutely. Fiber taken during this window will almost certainly reduce semaglutide absorption.
The most practical approach for oral semaglutide users: take semaglutide first thing in the morning, wait 30 minutes, eat breakfast, then take your first fiber dose mid-morning. Take the second dose in the evening before bed. This timing ensures no interference with medication absorption while still providing adequate fiber throughout the day.
Whole food fiber sources that complement supplements on GLP-1 medications
Supplements are important, but they work best alongside whole food fiber sources. The challenge on GLP-1 medications is getting enough fiber from food when your total caloric intake has dropped significantly.
These foods deliver the most fiber per calorie, making them ideal for GLP-1 users eating smaller portions.
Chia seeds: 10 grams of fiber per ounce (about 2 tablespoons). Mix into protein shakes, yogurt, or water. They form a gel similar to psyllium, making them a natural stool softener. Start with 1 tablespoon and increase gradually.
Flaxseeds (ground): 8 grams of fiber per ounce. Also provide omega-3 fatty acids, which may help with the inflammation some GLP-1 users experience. Must be ground to access the fiber. Whole flaxseeds pass through undigested.
Raspberries: 8 grams of fiber per cup. One of the highest-fiber fruits available. Their natural sweetness can help satisfy sugar cravings that some users experience.
Avocado: 10 grams of fiber per whole avocado. Also provides healthy fats and potassium. The creamy texture is often well tolerated even when appetite is reduced. Pairs well with other GLP-1 friendly foods.
Lentils: 15.6 grams of fiber per cup (cooked). Extremely nutrient-dense, providing both fiber and protein. However, they are moderately fermentable, so introduce them gradually if you are prone to bloating.
Artichoke hearts: 7 grams of fiber per half cup. Rich in inulin (a prebiotic), so introduce them after the initial medication adjustment period.
Black beans: 15 grams of fiber per cup (cooked). High fiber and protein density. Pre-soaking and thorough cooking reduces their fermentability and gas-producing potential.
A practical daily food-fiber strategy might include chia seeds in a morning smoothie, half an avocado at lunch, and a serving of lentils or beans at dinner. Combined with a psyllium supplement, this approach can easily reach 25 to 30 grams of total daily fiber even on a reduced-calorie diet.
When fiber supplements are not enough: escalation strategies
Sometimes fiber supplements alone do not fully resolve digestive issues on GLP-1 medications. Recognizing when to escalate and what options exist can prevent unnecessary suffering.
Signs that you need more than fiber
If you have been taking an appropriate fiber supplement at full dose with adequate hydration for 2 or more weeks and you are still experiencing fewer than 3 bowel movements per week, straining with most bowel movements, hard or lumpy stool consistently, or abdominal pain associated with constipation, fiber alone is not going to solve the problem. You need additional interventions.
Complementary strategies
Magnesium supplementation is the most common and effective complement to fiber. Magnesium citrate at 200 to 400 mg daily draws water into the intestine through osmosis, providing a different mechanism of action than fiber. Together, bulk-forming fiber and osmotic magnesium address constipation more comprehensively than either alone.
Probiotic supplements can help normalize gut motility and reduce gas production. Look for strains specifically studied for constipation, such as Bifidobacterium lactis and Lactobacillus reuteri. The Pendulum GLP-1 Probiotic was specifically formulated for GLP-1 users and includes strains that support metabolic health alongside digestive function.
Digestive enzymes can help break down food more efficiently in a system where transit time is extended. This can reduce bloating and gas independent of fiber supplementation.
Regular physical activity stimulates colonic motility through direct mechanical action and sympathetic nervous system activation. Even 20 to 30 minutes of walking after meals can significantly improve digestive function on GLP-1 medications.
Adequate fat intake: Fat stimulates bile release, which has a natural laxative effect. Some GLP-1 users, particularly those focused on high-protein, low-fat diets, inadvertently reduce fat intake to levels that contribute to constipation. Including healthy fats at each meal can complement fiber supplementation.
When to talk to your healthcare provider
Contact your prescribing physician or healthcare provider if constipation persists despite fiber supplementation and complementary strategies for more than 3 weeks, if you experience severe abdominal pain, if you notice blood in your stool, if you develop symptoms of bowel obstruction (vomiting, inability to pass gas, severe abdominal distension), or if constipation is significantly impacting your quality of life or making you consider discontinuing your GLP-1 medication.
Your provider may adjust your GLP-1 dose, prescribe a motility agent, or recommend temporary use of stimulant laxatives under medical supervision.
Frequently asked questions about fiber and GLP-1 medications
Can I take fiber supplements at the same time as my GLP-1 injection?
Yes, for injectable GLP-1 medications like semaglutide and tirzepatide, there is no absorption interaction between fiber supplements and the injection itself. However, consider reducing your fiber dose by 50% on injection day and the day after if you experience heightened gastrointestinal sensitivity during that window.
Will fiber supplements reduce the effectiveness of my GLP-1 medication?
For injectable GLP-1 medications, no. Fiber supplements do not affect the absorption or efficacy of subcutaneously injected semaglutide, tirzepatide, or retatrutide. For oral semaglutide, taking fiber within the 30-minute fasting window can reduce absorption. Always wait at least 30 minutes after oral semaglutide before taking fiber supplements.
How much fiber should I take daily on GLP-1 medications?
The general recommendation is 25 to 35 grams of total daily fiber from all sources (food and supplements combined). Most GLP-1 users need 5 to 15 grams from supplements to bridge the gap left by reduced food intake. Start at the low end and increase gradually based on tolerance and results.
Should I take soluble or insoluble fiber on semaglutide?
For most semaglutide users, soluble fiber (specifically psyllium) is the better starting choice. It forms a gel that softens stool without adding excessive bulk to an already slow-moving system. Insoluble fiber can be added in small amounts once your digestive system has stabilized. A ratio of approximately 70% soluble to 30% insoluble fiber works well for most people on GLP-1 medications.
Can fiber help with GLP-1 weight loss plateaus?
Indirectly, yes. Adequate fiber supports healthy gut bacteria that influence metabolism, helps stabilize blood sugar to prevent energy crashes and cravings, and promotes regular elimination that can mask true weight loss on the scale. While fiber is not a direct weight loss supplement, it supports the physiological environment that allows your GLP-1 medication to work optimally. Users who track their weight loss progress often find that resolving constipation with proper fiber supplementation reveals weight loss that was previously hidden by retained stool.
Is it safe to take fiber long-term on GLP-1 medications?
Yes. Fiber supplementation is one of the safest long-term supplement strategies available. Unlike stimulant laxatives, fiber supplements do not cause dependency or reduce natural bowel function over time. In fact, consistent fiber supplementation may actually improve natural digestive function by supporting the gut microbiome and maintaining healthy bowel habits. The long-term use of GLP-1 medications makes consistent fiber supplementation not just safe but advisable.
What is the best time of day to take fiber supplements on GLP-1 medications?
There is no single best time. It depends on your goals. For constipation prevention, before bed with a large glass of water allows overnight processing. For appetite support, 20 to 30 minutes before your largest meal. For general maintenance, split doses morning and evening provide consistent fiber throughout the day. The most important factor is consistency, taking your fiber at the same times each day.
Can I take too much fiber on GLP-1 medications?
Yes. Exceeding 35 to 40 grams of total daily fiber, especially without proportionally increasing water intake, can cause bloating, gas, cramping, and paradoxically worsen constipation. On GLP-1 medications where transit time is already extended, the ceiling for comfortable fiber intake may be lower than for the general population. Pay attention to your body signals and scale back if discomfort increases with higher doses.
Should I stop fiber supplements when I stop my GLP-1 medication?
When discontinuing GLP-1 medication, your gastric emptying rate and intestinal motility will gradually return to baseline. You may find that you need less supplemental fiber as your digestive system normalizes. However, many people benefit from continued fiber supplementation regardless of GLP-1 use, as most adults do not meet the recommended 25 to 35 grams of daily fiber from food alone. Rather than stopping abruptly, gradually reduce your supplement dose over 2 to 4 weeks after discontinuing your GLP-1 medication and adjust based on how your digestion responds. For guidance on the transition, explore what happens when you stop taking GLP-1 medications.
External resources
PubMed - National Library of Medicine database for fiber and GLP-1 research studies
American College of Gastroenterology - High fiber diet guidelines and recommendations
National Institute of Diabetes and Digestive and Kidney Diseases - Constipation management overview
Dietary Guidelines for Americans - Daily fiber intake recommendations
Choosing the right fiber supplement for your GLP-1 protocol is not about finding the one perfect product. It is about understanding how different fibers interact with your specific medication, your individual digestive response, and your particular symptoms. Start simple. Start slow. Track your results. Adjust based on data, not guesswork.
SeekPeptides members gain access to detailed supplement protocols, dosage calculators, and community insights from thousands of researchers who have navigated these exact challenges. The fiber strategy that transforms your GLP-1 experience might be simpler than you think, but it requires the right information and a systematic approach to get there.
In case I don't see ya, good afternoon, good evening, and good night.