Mar 15, 2026

Tired of that burning sensation creeping up your chest every time you take your semaglutide injection? You are not alone. Thousands of researchers and patients report the same frustrating experience, that persistent heartburn that makes you question whether the weight loss benefits are worth the discomfort.
The good news is that semaglutide-related acid reflux is both common and manageable, and most people find relief without stopping their protocol entirely.
Here is the reality that most guides gloss over. Acid reflux on semaglutide is not random. It follows predictable patterns. It responds to specific interventions. And it almost always improves with time and the right adjustments. The key is understanding exactly why your body reacts this way, what triggers make it worse, and which management strategies actually work based on clinical evidence rather than guesswork.
This guide covers every aspect of semaglutide and gastrointestinal symptoms, from the molecular mechanisms driving your reflux to the exact dietary changes, medication options, and lifestyle modifications that bring real relief. Whether you are just starting your first week on semaglutide or dealing with persistent symptoms months into treatment, you will find actionable protocols you can implement today. SeekPeptides has compiled research from clinical trials, gastroenterology literature, and thousands of real-world patient experiences to create the most comprehensive resource available on this topic.
How semaglutide causes acid reflux at the cellular level
Understanding why semaglutide triggers acid reflux requires looking at what the peptide actually does inside your digestive system. Semaglutide is a GLP-1 receptor agonist that mimics a natural hormone your body produces after eating. This hormone tells your brain you are full, reduces appetite, and, critically for this discussion, slows the rate at which your stomach empties its contents into the small intestine.
That delayed gastric emptying is the primary culprit.
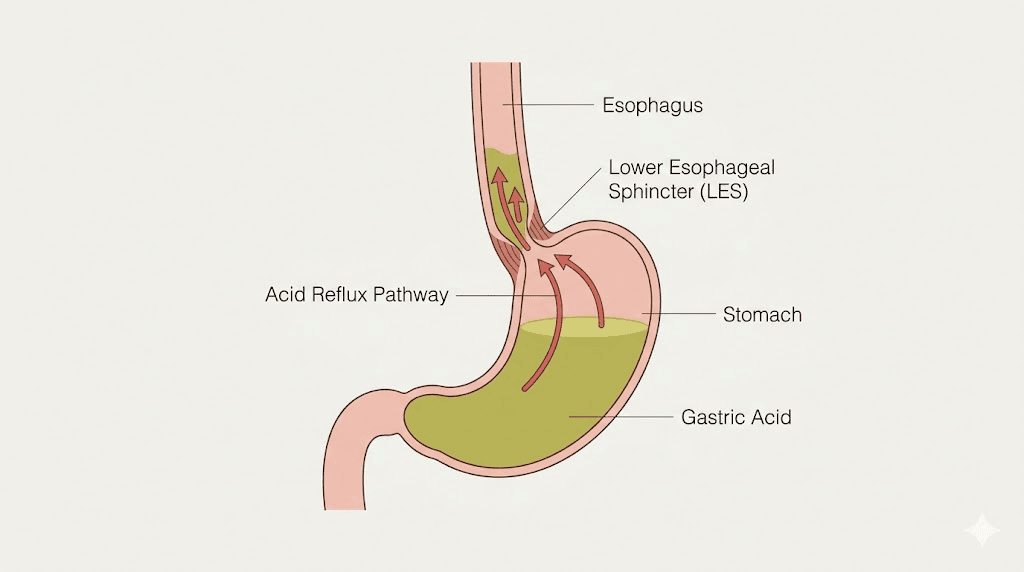
When food sits in your stomach longer than normal, several things happen simultaneously. Intragastric pressure increases as the stomach walls stretch to accommodate food that would normally have moved downstream. Gastric acid production continues on its normal schedule, but now that acid has nowhere productive to go. The combination of increased pressure and excess acid creates the perfect conditions for retrograde flow, meaning stomach contents push back up through the lower esophageal sphincter and into the esophagus.
The lower esophageal sphincter is a ring of muscle that acts as a one-way valve between your esophagus and stomach. Under normal conditions, it stays closed except when you swallow. But increased intragastric pressure can overwhelm this valve, forcing it open and allowing acidic stomach contents to splash upward. Some research suggests that GLP-1 receptor activation may also directly relax the lower esophageal sphincter, making it even more susceptible to opening when it should stay shut.
There is another mechanism at play that many guides miss entirely. Semaglutide-induced nausea, which affects up to 44% of people taking the higher doses, can trigger retching and vomiting. These forceful contractions repeatedly compromise the lower esophageal sphincter integrity, creating a cycle where nausea leads to reflux, reflux causes more irritation, and that irritation worsens nausea. Breaking this cycle early is critical for long-term comfort.
The gastric emptying timeline
Normal gastric emptying takes approximately 4 to 5 hours for a standard meal. Semaglutide can extend this to 8 hours or longer, depending on the dose and individual response. During those extra hours, your stomach is essentially working overtime, churning acid against food that is not moving. The dose you are taking matters significantly here, as higher doses produce more dramatic slowing of gastric emptying and correspondingly more reflux risk.
Research shows the delay is most pronounced during the first 1 to 2 hours after a meal, which is why many people notice their worst reflux symptoms shortly after eating rather than on an empty stomach. This timing pattern is important because it tells you exactly when your management strategies need to be most aggressive.
Why some people get reflux and others do not
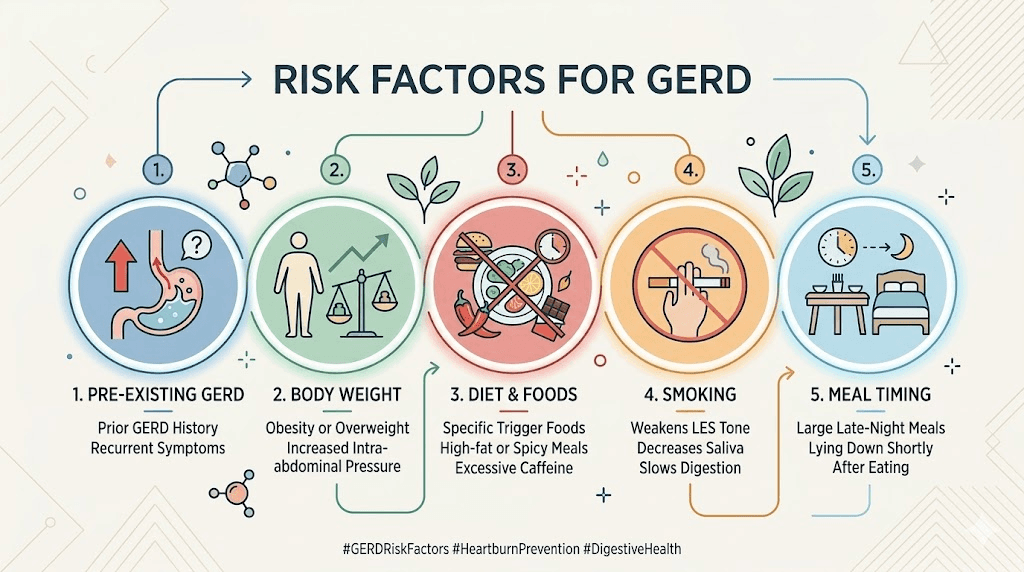
Not everyone on semaglutide experiences acid reflux, and understanding the risk factors helps predict who is most vulnerable. Pre-existing conditions play a major role. If you had occasional heartburn before starting semaglutide, you are significantly more likely to experience worsened symptoms. A history of GERD, hiatal hernia, or esophagitis amplifies the risk considerably.
Body composition matters too. Higher body weight is independently associated with increased reflux risk because abdominal fat places additional pressure on the stomach. Paradoxically, this means the very people who benefit most from semaglutide weight loss are also most likely to experience reflux, at least initially. As weight decreases, reflux often improves naturally, creating a situation where symptoms get worse before they get better.
Other risk factors include smoking, alcohol consumption, eating large meals, lying down shortly after eating, and consuming trigger foods like chocolate, caffeine, citrus, and high-fat dishes. These are all modifiable, which means you have significant control over your reflux outcomes regardless of how semaglutide affects your physiology.
How common is acid reflux on semaglutide
Clinical trial data provides a clear picture. In the STEP trials that led to Wegovy approval, approximately 5% of participants reported GERD or acid reflux symptoms, compared to 3% in the placebo group. That 2% difference might sound small, but it represents a meaningful increase in risk that becomes more significant when you factor in the broader category of gastrointestinal side effects.
The full gastrointestinal picture is more telling. Up to 36.4% of semaglutide users report some form of GI symptoms, compared to 15.3% on placebo. While not all of these are reflux specifically, many overlap. Nausea (reported by up to 44% on higher doses), bloating, burping, and constipation all contribute to increased reflux risk through different mechanisms.
Real-world numbers are likely higher than clinical trial data suggests. Clinical trials use strict protocols, monitor patients closely, and exclude people with severe pre-existing GERD. In everyday practice, where people eat irregular meals, forget dietary guidelines, and may not titrate doses as carefully, reflux rates of 10 to 15% are commonly reported by prescribers.
When symptoms typically appear
Most people notice reflux symptoms during two specific windows. The first is during the initial titration phase, when the body is adjusting to a new medication that fundamentally changes how the digestive system operates. This typically means the first 4 to 8 weeks of treatment, with symptoms peaking around weeks 2 to 4.
The second window occurs after dose increases. Standard semaglutide protocols increase the dose every 4 weeks. Each escalation brings a temporary resurgence of GI symptoms as the body adjusts to the stronger gastric emptying delay. For many people, reflux symptoms that had resolved at one dose level return briefly when moving to the next.
The encouraging news: most people experience significant improvement over time. Studies show that GI symptoms, including reflux, attenuate substantially after completing the dose titration period. Many users report that symptoms that felt unbearable at week 2 were barely noticeable by month 3. Patience and proper management during the adjustment period make all the difference.
Recognizing semaglutide acid reflux symptoms
Acid reflux from semaglutide presents differently than typical heartburn for many people. Knowing what to look for helps you catch it early and respond appropriately before it becomes severe.
Classic symptoms
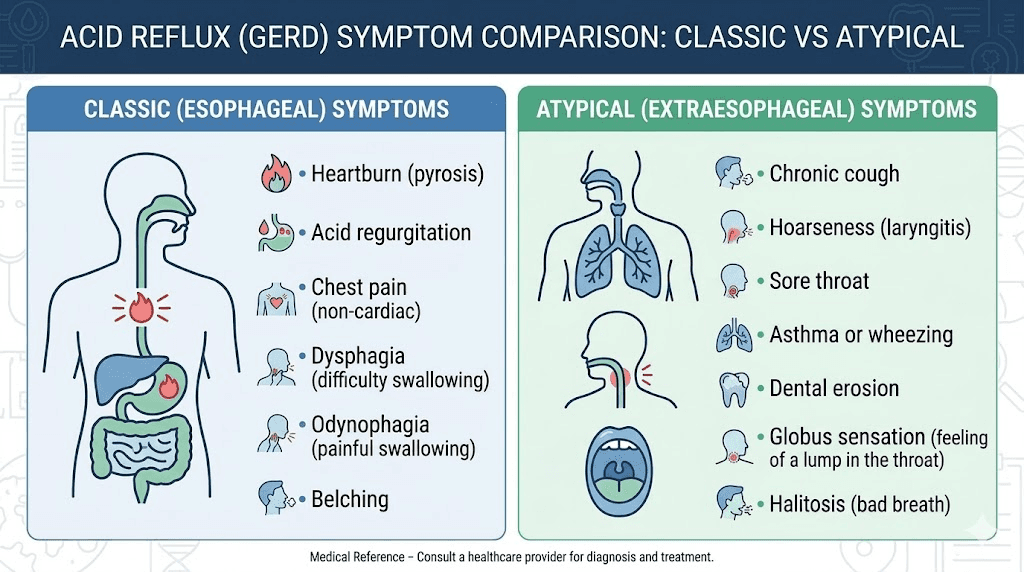
The most recognizable symptom is a burning sensation in the chest that rises from the upper abdomen toward the throat. This burning typically worsens after meals, when lying down, or when bending over. It may come with a sour or bitter taste in the mouth as stomach acid reaches the back of the throat. Regurgitation, where you actually feel food or liquid coming back up, is another common presentation.
Excessive burping is particularly common with semaglutide-related reflux and often precedes the burning sensation. Many people report that belching provides temporary relief, only for the discomfort to return minutes later. This pattern is characteristic of increased intragastric pressure from delayed emptying.
Atypical symptoms people miss
Some semaglutide users experience what gastroenterologists call "silent reflux" or laryngopharyngeal reflux. This presents without the classic heartburn but causes persistent throat clearing, a chronic cough that worsens after eating, hoarseness, a feeling of a lump in the throat, or worsening asthma symptoms. These atypical presentations are easy to attribute to other causes, which delays treatment.
Night symptoms deserve special attention. If you wake up coughing, with a sour taste, or with unexplained throat soreness, reflux during sleep is likely responsible. Nighttime reflux is more damaging to the esophagus because gravity is no longer helping keep acid in the stomach, and the protective swallowing reflex is reduced during sleep.
When reflux becomes concerning
Most semaglutide-related reflux is uncomfortable but not dangerous. However, certain symptoms require immediate medical attention. Difficulty swallowing or painful swallowing could indicate esophageal inflammation or stricture formation. Vomiting blood, even small amounts that look like coffee grounds, suggests mucosal damage. Black, tarry stools indicate bleeding somewhere in the upper GI tract. Severe, persistent abdominal pain radiating to the back could signal pancreatitis, a rare but serious semaglutide side effect.
Chest pain that feels different from your usual heartburn, or pain accompanied by shortness of breath, sweating, or jaw pain, requires emergency evaluation. These symptoms can mimic cardiac events, and it is always better to rule out serious causes than to assume it is "just heartburn."
The complete management protocol for semaglutide acid reflux
Managing reflux while continuing semaglutide requires a layered approach. Start with the least invasive strategies and escalate only as needed. Most people find relief with dietary and lifestyle changes alone, but knowing the full range of options ensures you are prepared for any severity level.
Tier 1: dietary modifications that work immediately
Dietary changes provide the fastest relief because they directly address the mechanism causing your reflux. The foods you avoid matter more than any other single intervention.
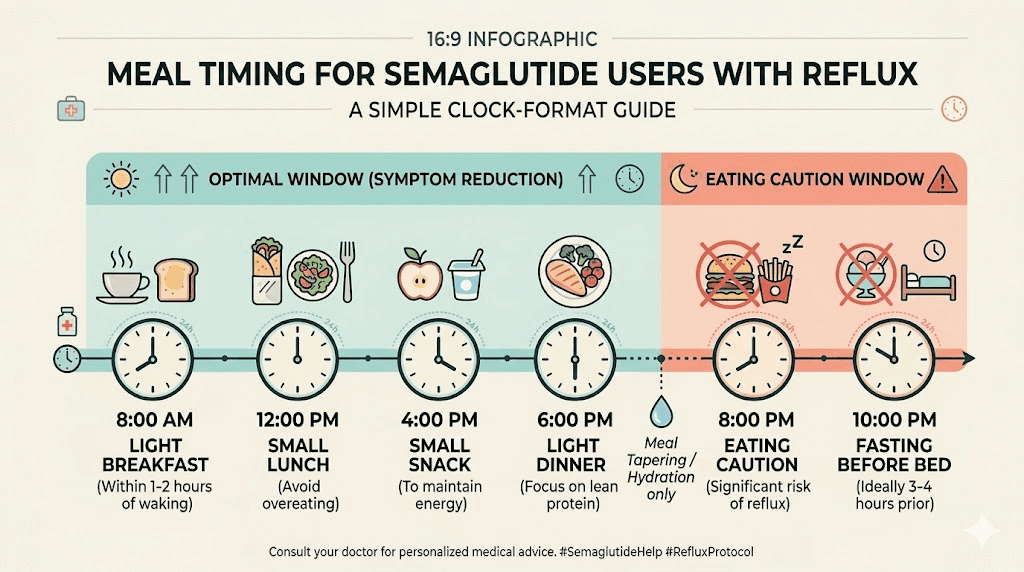
Meal size is everything. The single most effective change is reducing meal portions. Semaglutide already suppresses appetite, so your body is already signaling that it wants less food. Listen to it. Eating until you are 60 to 70% full, rather than your pre-semaglutide "full," dramatically reduces intragastric pressure. Aim for 4 to 6 smaller meals rather than 2 to 3 large ones.
Specific trigger foods to eliminate or reduce include chocolate, coffee, caffeinated tea, carbonated beverages, alcohol (especially red wine and beer), citrus fruits and juices, tomato-based products, spicy foods, peppermint, onions, garlic, and high-fat meals. You do not need to eliminate everything at once. Start by removing the most common offenders, chocolate, coffee, and alcohol, then systematically reintroduce them one at a time to identify your personal triggers.
The best foods for semaglutide users dealing with reflux include lean proteins (chicken, fish, turkey), non-citrus fruits (bananas, melons, apples), vegetables (except tomatoes and onions), whole grains (oatmeal, brown rice), and low-fat dairy. These foods are less likely to trigger reflux while providing the nutrition your body needs during weight loss.
Eating speed matters more than most people realize. Chewing thoroughly and eating slowly, taking at least 20 to 30 minutes per meal, gives your stomach time to signal fullness before you overeat. Fast eating consistently correlates with worse reflux outcomes because you consume more food before satiety signals reach your brain.
The complete semaglutide diet plan should incorporate these reflux-friendly principles from day one. Planning meals in advance prevents the impulse eating of trigger foods that worsens symptoms.
Tier 2: lifestyle modifications that reduce reflux by 40 to 60%
Beyond diet, specific behavioral changes significantly reduce reflux frequency and severity.
Timing your meals relative to lying down. This is non-negotiable. Do not eat anything for at least 2 to 3 hours before lying down, and ideally 4 hours before bed. Gravity is your best friend when it comes to keeping acid in your stomach. Eating late and then going to sleep is the single most common mistake that turns manageable reflux into severe nighttime symptoms.
Elevate the head of your bed. Place 6 to 8 inch blocks under the headboard legs, or use a wedge pillow designed for GERD. Simply propping up extra pillows does not work because it creates a bend at the waist that actually increases abdominal pressure. The entire upper body needs to be elevated at a gentle angle so gravity continuously pulls stomach acid downward.
Clothing choices. Tight belts, waistbands, and compression garments increase abdominal pressure and push stomach contents upward. Wearing loose-fitting clothing around the midsection, especially after meals, provides measurable relief.
Post-meal activity. A gentle 10 to 15 minute walk after eating helps stimulate gastric motility without the jarring movements that worsen reflux. Avoid intense exercise, bending over, or heavy lifting for at least 1 to 2 hours after meals. Activities that increase abdominal pressure, like crunches, deadlifts, or heavy squats, are best done on a relatively empty stomach.
Stress management deserves mention here because stress directly increases stomach acid production and heightens esophageal sensitivity. Chronic stress makes the same amount of reflux feel significantly worse. Deep breathing exercises, meditation, or even just conscious relaxation after meals can reduce symptom perception meaningfully.
Understanding how semaglutide affects your overall wellbeing helps you contextualize reflux symptoms within the broader picture of temporary side effects that improve over time.
Tier 3: over-the-counter medications
When lifestyle modifications are not enough, several OTC options provide effective relief.
Antacids (calcium carbonate, magnesium hydroxide). Products like Tums, Rolaids, and Maalox neutralize existing stomach acid on contact. They work within minutes but only last 1 to 3 hours. Best used as needed for occasional breakthrough symptoms. Taking one 30 minutes before a meal can prevent reflux in predictable trigger situations.
H2-receptor antagonists (famotidine, cimetidine). Famotidine (Pepcid) reduces acid production for 8 to 12 hours per dose. It is more effective than antacids for preventing reflux rather than just treating it. A dose of 20mg taken 30 to 60 minutes before meals provides consistent protection. Many semaglutide users find that taking famotidine before dinner, their most problematic meal, eliminates evening and nighttime symptoms entirely.
Proton pump inhibitors (omeprazole, esomeprazole, lansoprazole). OTC PPIs are the strongest acid-reducing medications available without a prescription. Omeprazole 20mg taken once daily in the morning, 30 minutes before breakfast, reduces acid production by up to 70% within 5 days. For semaglutide-related reflux that does not respond to H2 blockers, an 8-week course of a PPI is the standard recommendation.
The American College of Physicians recommends using PPIs at the lowest effective dose for the shortest duration necessary. Many semaglutide users need PPIs only during dose titration phases, then successfully step down to H2 blockers or lifestyle management alone once their body adjusts.
Tier 4: prescription interventions
If OTC medications provide insufficient relief, prescription-strength options are available. Higher-dose PPIs (omeprazole 40mg, esomeprazole 40mg) taken once or twice daily can suppress acid production by up to 90%. Potassium-competitive acid blockers like vonoprazan represent a newer class that works faster and more completely than traditional PPIs.
Some gastroenterologists recommend combining a PPI with an H2 blocker, using the PPI in the morning and an H2 blocker at bedtime to provide 24-hour coverage. This combination approach targets both daytime and nighttime reflux through complementary mechanisms.
Prokinetic agents like metoclopramide can help by speeding up gastric emptying, directly counteracting the semaglutide-induced delay. However, these medications have their own side effects and are typically reserved for cases where other approaches fail.
The dose-response relationship: how your semaglutide dose affects reflux
Not all semaglutide doses produce equal reflux risk. Understanding this relationship helps you optimize your treatment.
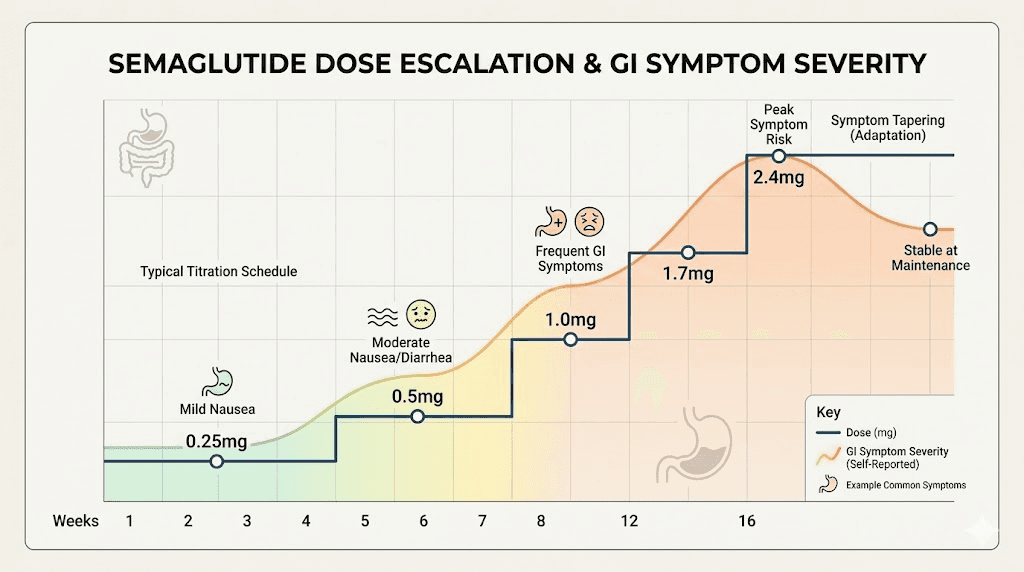
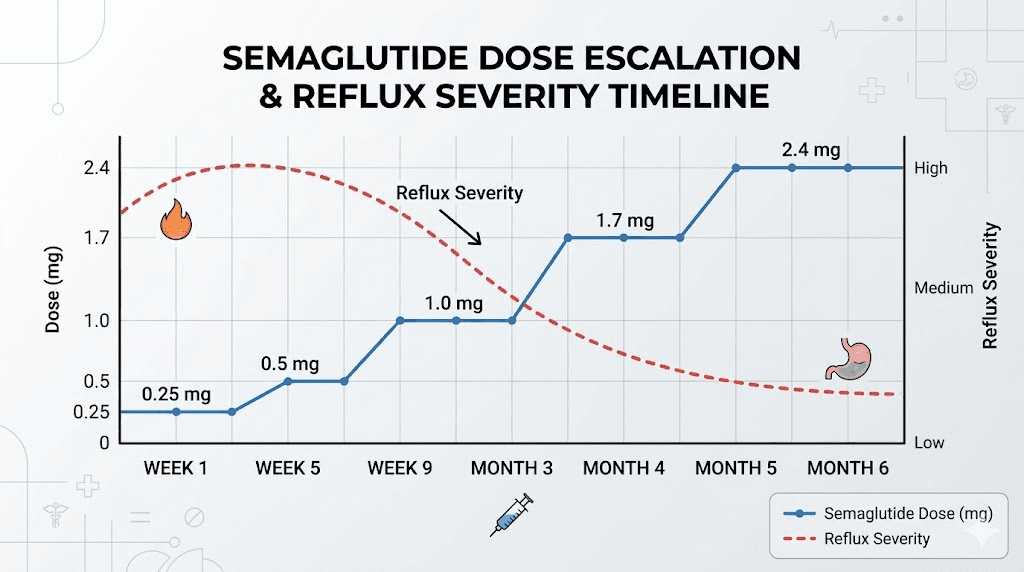
Clinical data shows a clear dose-dependent pattern. At the starting dose of 0.25mg, GI side effects including reflux are relatively uncommon because the gastric emptying delay is modest. At 0.5mg, symptoms begin appearing in susceptible individuals. By the time patients reach the maintenance dose of 2.4mg for weight management, GI symptoms are at their peak frequency.
This dose-response pattern has practical implications. If reflux becomes severe after a dose increase, staying at the previous dose for an additional 2 to 4 weeks allows your body more time to adjust. The standard titration schedule of 4 weeks per dose level is a minimum, not a mandate. Your prescriber can extend the titration period at any level if side effects warrant it.
Some researchers and clinicians advocate for splitting the semaglutide dose across two injections per week instead of one. The theory is that smaller, more frequent doses produce a smoother pharmacokinetic profile with less dramatic peaks in GLP-1 activity, potentially reducing the intensity of gastric emptying delay and associated reflux. While not officially recommended in prescribing information, anecdotal reports from clinicians suggest this approach helps some patients with dose-limiting GI side effects.
The amount of semaglutide you are taking matters, but so does the concentration of your reconstituted solution. Using the semaglutide dosage calculator ensures you are injecting the correct amount and not accidentally overdosing, which would amplify all side effects including reflux.
Injection timing and reflux: does when you inject matter
The timing of your weekly semaglutide injection can influence reflux patterns, though the evidence is largely observational rather than from controlled trials.
Semaglutide has a half-life of approximately one week, meaning blood levels remain relatively stable between injections. However, peak plasma concentrations occur 1 to 3 days after injection, and some users report that GI symptoms, including reflux, are most pronounced during this peak window. By days 5 to 7, as levels begin to decline slightly, symptoms often improve.
The best time of day to take semaglutide for reflux management depends on your schedule. Many clinicians suggest injecting in the evening or before bed, so that the initial absorption phase (when mild nausea and GI effects are most likely) occurs during sleep. Others recommend morning injections so that peak effects align with daytime hours when you are upright and active, which naturally reduces reflux through gravity.
There is no universally "right" answer here. Experiment with different injection days and times over several weeks to identify your personal optimal schedule. Track your symptoms in a journal noting injection time, meal times, symptom onset, and severity. Patterns usually emerge within 2 to 3 injection cycles.
The injection site does not directly affect reflux, but subcutaneous injections in the abdomen versus the thigh can produce slightly different absorption rates, which might indirectly influence the timing of GI effects.
Semaglutide acid reflux versus pre-existing GERD: critical differences
If you had GERD before starting semaglutide, your management approach needs adjustment. Pre-existing GERD combined with semaglutide creates a compounding effect that requires more aggressive intervention than either condition alone.
People with established GERD typically already have a compromised lower esophageal sphincter, often from chronic acid exposure or a hiatal hernia. Adding semaglutide-induced gastric emptying delay to an already weakened sphincter creates significantly higher reflux risk. Clinical experience suggests these patients should start preventive acid-suppressing medication (usually a PPI) at the same time they begin semaglutide, rather than waiting for symptoms to develop.
If you are currently managing GERD with medication, do not reduce or stop your acid-suppressing regimen when starting semaglutide. Many patients mistakenly assume that since semaglutide reduces appetite and food intake, their reflux will improve. In reality, the delayed gastric emptying typically worsens reflux regardless of how much food is in the stomach.
For patients with Barrett esophagus or a history of esophageal strictures, close monitoring during semaglutide treatment is essential. These conditions indicate prior severe acid damage, and any worsening of reflux could accelerate disease progression. Regular endoscopic surveillance should continue on schedule, with earlier evaluation if symptoms change.
Diet protocols specifically designed for semaglutide users with reflux
Generic GERD diet advice does not account for the unique challenges semaglutide creates. Here are specific protocols designed for this combination.
Protocol 1: the reflux-friendly semaglutide meal plan
Goal: Minimize reflux while maintaining adequate nutrition during semaglutide-assisted weight loss.
Breakfast (7:00 to 8:00 AM): Oatmeal with banana slices and a small amount of almond butter, or scrambled eggs with whole grain toast. Avoid coffee on an empty stomach. If you need caffeine, have it with food and limit to one cup. The complete food list for semaglutide users provides additional breakfast options.
Mid-morning snack (10:00 AM): Small portion of Greek yogurt with melon, or a handful of almonds. Keep it under 200 calories.
Lunch (12:00 to 1:00 PM): Grilled chicken or fish with steamed vegetables and brown rice. Avoid tomato-based sauces, heavy dressings, and fried preparations. Eat slowly, taking at least 20 minutes.
Afternoon snack (3:00 PM): Apple slices with a small amount of peanut butter, or a protein shake made with non-citrus fruit. GLP-1 friendly protein shakes are formulated to be easy on the stomach.
Dinner (6:00 to 7:00 PM, at least 3 hours before bed): Baked salmon or lean turkey with roasted root vegetables. Keep fat content moderate. This is typically the meal where reflux is worst, so keep portions smallest here.
Critical rule: Nothing after 7:00 PM except water (room temperature, not cold or hot). No bedtime snacks. No late-night eating. This single rule eliminates nighttime reflux for most semaglutide users.
Protocol 2: the elimination and reintroduction approach
Goal: Identify your personal trigger foods systematically.
Phase 1 (Weeks 1 to 2): Eliminate all common triggers simultaneously. No coffee, chocolate, alcohol, citrus, tomatoes, spicy food, peppermint, carbonated drinks, or high-fat meals. Eat only bland, reflux-safe foods. This establishes a baseline of minimal symptoms.
Phase 2 (Weeks 3 to 6): Reintroduce one trigger food every 3 to 4 days. Keep a detailed symptom journal. Rate reflux severity on a 1 to 10 scale for 72 hours after each reintroduction. Foods that increase your score by 3 or more points are confirmed personal triggers. Foods that produce no change are safe to include in your regular diet.
Phase 3 (Ongoing): Build your personalized diet around confirmed safe foods while permanently avoiding identified triggers. Most people find they have 3 to 5 major triggers rather than needing to avoid everything.
Hydration strategies for reflux management
How you drink matters as much as what you eat. Large volumes of liquid during meals dilute digestive enzymes and increase stomach volume, both of which worsen reflux. Sip small amounts during meals and do most of your hydrating between meals.
Water temperature makes a difference. Room temperature or slightly warm water is less likely to trigger reflux than ice-cold water, which can cause stomach contractions. Herbal teas like chamomile and ginger are generally well-tolerated and may actually soothe the esophageal lining.
Avoid carbonated beverages entirely during active reflux episodes. The gas they produce increases intragastric pressure and directly promotes belching and reflux. If you drink alcohol at all, understanding alcohol interactions with semaglutide is essential, as alcohol both worsens reflux and interacts with the medication in ways that amplify GI side effects.
Comparing reflux risk across GLP-1 medications
If reflux becomes unmanageable on semaglutide, understanding how it compares to alternatives helps inform discussions with your prescriber about switching options.
Tirzepatide is the most common alternative considered. As a dual GIP/GLP-1 receptor agonist, tirzepatide also delays gastric emptying and carries similar reflux risk. Clinical trial data suggests comparable GI side effect profiles, though some patients who cannot tolerate one medication do better on the other due to individual receptor sensitivity differences. If tirzepatide interests you, discuss transitioning options with your provider. The conversion chart between the two medications helps ensure appropriate dosing during switches.
Retatrutide, a newer triple receptor agonist, shows similar GI side effect patterns in clinical trials. The addition of a glucagon receptor component may theoretically affect reflux differently, but comparative data is still limited.
Oral semaglutide (Rybelsus) presents a unique consideration. It requires administration on an empty stomach with a small amount of water, followed by a 30-minute fasting period. Some patients report that the oral formulation causes less reflux than injectable semaglutide, while others find the required empty-stomach dosing triggers more morning nausea and reflux. The oral semaglutide guide covers these distinctions in detail.
The sublingual semaglutide formulation offers yet another delivery method that may affect GI tolerance differently, though evidence remains primarily anecdotal at this stage.
Medication | Reflux Risk | Gastric Emptying Delay | Notes |
|---|---|---|---|
Semaglutide (injectable) | Moderate (5–10%) | Significant | Most studied, predictable response |
Semaglutide (oral) | Moderate (5–10%) | Significant | Empty stomach requirement may worsen morning reflux |
Tirzepatide | Moderate (5–10%) | Significant | Dual receptor, similar GI profile |
Retatrutide | Moderate (data limited) | Significant | Triple receptor, emerging data |
Liraglutide | Lower | Moderate | Shorter half-life, less potent but fewer GI effects |
Natural and complementary approaches to semaglutide reflux
Several natural approaches show promise for managing reflux alongside conventional treatments. These are not replacements for medical management but can provide additional relief.
Ginger
Ginger has well-documented prokinetic effects, meaning it can speed gastric emptying. This directly counteracts the delayed emptying caused by semaglutide. Fresh ginger tea (1 to 2 inches of grated ginger steeped in hot water for 10 minutes) taken 20 to 30 minutes before meals may reduce reflux episodes. Avoid ginger ale, as the carbonation negates the benefit. Research suggests 1 to 1.5 grams of ginger daily is effective for nausea and may improve gastric motility.
Probiotics
Gut microbiome changes during semaglutide treatment may influence GI symptoms including reflux. The best probiotics for semaglutide users include strains like Lactobacillus rhamnosus and Bifidobacterium lactis that support digestive function without increasing gas production (which would worsen reflux).
Slippery elm and marshmallow root
These mucilaginous herbs create a protective coating on the esophageal lining when taken before meals. They do not reduce acid production but can reduce the damage and discomfort caused by reflux episodes. Available as teas, lozenges, or capsules. No known interactions with semaglutide.
Aloe vera juice
Decolorized, purified aloe vera juice (1 to 2 ounces before meals) has shown modest benefit for reflux symptoms in small studies. Avoid products containing aloe latex, which can worsen GI symptoms. Look for inner leaf gel preparations specifically.
Melatonin
Perhaps surprisingly, melatonin plays a role in gastric acid regulation. Research suggests that 3 to 6mg of melatonin at bedtime may reduce nighttime reflux by strengthening the lower esophageal sphincter and reducing acid secretion. This approach also helps with semaglutide-related sleep disturbances, addressing two problems simultaneously.
Breathing exercises
Diaphragmatic breathing exercises strengthen the crural diaphragm, which forms part of the lower esophageal sphincter complex. Studies show that 30 minutes of daily diaphragmatic breathing practice for 4 weeks can reduce reflux episodes by up to 50% in some patients. The technique involves breathing deeply into the belly rather than the chest, with slow, controlled exhalations.
Week-by-week management guide for new semaglutide users
This protocol assumes you are starting semaglutide for the first time and want to minimize reflux from day one.
Before starting (preparation week)
Begin dietary modifications before your first injection. Eliminate major trigger foods, establish smaller meal portions, and set up your sleep environment with bed elevation. Stock up on antacids and consider starting famotidine 20mg daily if you have any history of heartburn. This proactive approach prevents reflux from ever getting established.
Review the first week on semaglutide guide so you know what to expect across all side effects, not just reflux.
Weeks 1 to 4 (0.25mg dose)
Most people tolerate this starting dose well. Reflux is uncommon but can occur, especially in those with risk factors. Continue dietary precautions. Take antacids as needed. If reflux occurs more than twice per week, start famotidine 20mg before your most problematic meal. Track symptoms daily to establish your personal baseline.
Weeks 5 to 8 (0.5mg dose)
First dose increase brings the first significant risk of GI symptoms. Expect 1 to 2 weeks of adjustment. Reflux symptoms that appear here typically peak around days 3 to 7 of the new dose and improve by week 2. Be strict with meal timing and portion control during this adjustment. Consider prophylactic famotidine if symptoms appeared at the lower dose.
Weeks 9 to 12 (1.0mg dose)
This is where many people first experience significant reflux. The gastric emptying delay at 1.0mg is substantially greater than at 0.5mg. If reflux is occurring more than 3 times per week despite lifestyle measures and H2 blockers, transition to a PPI. Verify your dosing is accurate to ensure you are not accidentally exceeding the intended amount.
Weeks 13 to 16 (1.7mg dose)
For weight management protocols, this higher dose further intensifies gastric emptying delay. However, your body has been adjusting for three months, and many people find that reflux actually improves at this stage compared to the initial weeks at 1.0mg. The body adapts. Continue current management strategies and adjust as symptoms dictate.
Weeks 17 to 20 (2.4mg maintenance dose)
The maintenance dose produces maximum therapeutic effect and maximum gastric emptying delay. If you have reached this dose without significant reflux, you are unlikely to develop it now. If reflux has been managed with medication, attempt a gradual step-down after 4 to 6 weeks at maintenance. Many patients can transition from PPIs to H2 blockers, or from H2 blockers to occasional antacids, as their body fully acclimates.
Months 3 to 6 and beyond
Long-term semaglutide users generally report that GI symptoms, including reflux, stabilize or resolve entirely. The body adapts to the altered gastric emptying rate. Weight loss itself reduces abdominal pressure, further improving reflux. The week-by-week results timeline shows that most side effects follow a predictable arc of worsening, plateau, and improvement.
SeekPeptides members access detailed week-by-week protocol tracking tools that help monitor symptoms alongside weight loss progress, making it easier to identify patterns and optimize management.
Semaglutide acid reflux and sleep: managing nighttime symptoms
Nighttime reflux is the most disruptive form and the most damaging to esophageal tissue. When you sleep, you lose the protective effects of gravity and the frequent swallowing that clears acid during waking hours. Acid contact time with the esophageal lining increases dramatically, raising the risk of esophagitis, stricture formation, and potentially Barrett esophagus with chronic exposure.
The nighttime reflux protocol
Stop all food and drinks (except small sips of water) at least 3 to 4 hours before bedtime. If your last meal is dinner at 6:00 PM and you go to bed at 10:00 PM, that gives your stomach 4 hours to process food before you lie down. With semaglutide-delayed gastric emptying, this window may need to be even longer, up to 5 hours for some people.
Elevate the head of your bed 6 to 8 inches using bed risers or a foam wedge that runs the full length of your torso. The angle should feel gentle enough to sleep comfortably but steep enough that you feel gravity pulling you slightly toward the foot of the bed.
Sleep on your left side when possible. The anatomy of the stomach means that left-side sleeping positions the esophageal junction above the level of gastric acid, while right-side sleeping does the opposite and can worsen reflux significantly. This is one of the most evidence-based and underutilized sleep position recommendations in GERD management.
Take your H2 blocker or PPI strategically. Famotidine before dinner provides coverage through the night. If using a PPI, the morning dose provides all-day coverage, but adding an evening H2 blocker specifically for nighttime protection is a well-established combination strategy.
Avoid alcohol in the evening.
Beyond its direct irritant effects on the esophageal lining, alcohol relaxes the lower esophageal sphincter and impairs the protective clearing reflexes during sleep. Even moderate amounts significantly worsen nighttime reflux.
If you experience semaglutide-related fatigue, you might be tempted to nap after meals. Resist this urge. Post-meal napping is a major reflux trigger because it combines food in the stomach with a recumbent position during peak acid production.
When acid reflux means you should reconsider semaglutide
For most people, semaglutide acid reflux is manageable and temporary. But there are situations where the reflux risk outweighs the benefits of continued treatment.
You should discuss alternatives with your prescriber if:
Severe reflux persists despite maximum medical therapy (twice-daily PPI plus lifestyle modifications) for more than 8 weeks. Reflux is causing documented esophagitis on endoscopy that is not improving. You develop difficulty swallowing that worsens over time. Reflux requires such aggressive medication management that the polypharmacy burden becomes problematic. Quality of life is severely impacted despite all interventions.
The decision to continue or stop semaglutide when reflux is severe should be made collaboratively between you and your healthcare provider, weighing the metabolic benefits of continued semaglutide therapy against the risks of ongoing acid exposure. Do not discontinue semaglutide abruptly without medical guidance, as this can trigger withdrawal effects and rapid weight regain.
Alternatives might include switching to a different GLP-1 medication (some patients tolerate one better than another despite similar mechanisms), reducing the maintenance dose to a level that produces fewer GI effects while still providing benefit, or transitioning to tirzepatide or another agent in the class.
Semaglutide acid reflux and compounded formulations
Many semaglutide users obtain their medication through compounding pharmacies rather than brand-name products. This introduces additional considerations for reflux management.
Compounded semaglutide may include additional ingredients like vitamin B12, glycine, or L-carnitine. Some of these additives are specifically included to reduce GI side effects. B12 supplementation addresses the nutrient depletion that can occur with reduced food intake and altered absorption. Glycine may have a gastroprotective effect. Niacinamide-containing formulations offer additional metabolic support.
The concentration and vehicle of compounded products can vary between pharmacies. Higher concentrations mean smaller injection volumes, which some patients report produces fewer injection-site and systemic GI reactions. If you are using compounded semaglutide, verify the concentration and reconstitution details to ensure accurate dosing.
Storage matters too. Improperly stored semaglutide may degrade, altering its pharmacokinetic profile in ways that could affect GI tolerability. Follow proper refrigeration guidelines and check that your medication has not been exposed to extreme temperatures. If your semaglutide gets warm, it may not work as expected.
Supplements that help and hurt semaglutide acid reflux
Several common supplements interact with reflux in ways that semaglutide users should know about.
Supplements that may help
Magnesium glycinate: Supports digestive function and may reduce acid production. The glycinate form is the least likely to cause GI upset. 200 to 400mg daily.
Zinc carnosine: Specifically shown to protect the stomach lining and promote healing of mucosal damage. 75mg twice daily on an empty stomach. Particularly useful if reflux has already caused some esophageal irritation.
DGL (deglycyrrhizinated licorice): Chewable tablets taken before meals increase mucus production that protects the stomach and esophageal lining. 400mg before meals, up to three times daily.
Digestive enzymes: Taking a broad-spectrum digestive enzyme supplement with meals may help reduce the time food spends in the stomach by assisting breakdown, partially counteracting the delayed emptying effect.
Supplements that may worsen reflux
Iron supplements: Highly irritating to the stomach lining and the esophagus. If you need iron, take it with food, avoid the ferrous sulfate form (switch to iron bisglycinate), and separate from any acid-reducing medications by at least 2 hours.
NSAIDs and aspirin: While not supplements technically, many people take daily aspirin or use ibuprofen regularly. These damage the stomach lining and dramatically worsen reflux. Use acetaminophen instead when possible.
Vitamin C (ascorbic acid): High-dose vitamin C is acidic and can directly irritate the esophagus and stomach. If supplementing, use the buffered form (calcium ascorbate or sodium ascorbate).
Fish oil: Large doses of omega-3 fatty acids can trigger reflux in some people because fat delays gastric emptying even further. If taking fish oil, use enteric-coated capsules that dissolve in the small intestine rather than the stomach.
Exercise and semaglutide acid reflux
Physical activity is essential during semaglutide treatment for maintaining muscle mass and enhancing weight loss. But certain exercises can make reflux significantly worse while others actually help.
Exercises that worsen reflux
High-impact activities (running, jumping, burpees) jostle stomach contents and can force acid upward. Core-intensive exercises (crunches, sit-ups, planks) increase abdominal pressure directly. Heavy weightlifting, especially exercises that involve a Valsalva maneuver (holding breath against a closed glottis), dramatically spikes intra-abdominal pressure. Inverted positions (yoga headstands, decline bench) literally pour stomach acid toward the esophagus.
Exercises that improve reflux
Walking is the gold standard. A 15 to 30 minute walk after meals aids gastric motility without the jarring of higher-impact activities. Swimming (with proper breathing technique) is excellent. Cycling at moderate intensity works well. Light resistance training with controlled breathing is generally safe. Yoga (upright poses, avoid inversions) combines physical activity with stress-reducing breathing that benefits reflux.
Timing exercise around meals
Wait at least 1 to 2 hours after eating before any moderate or intense exercise. A gentle walk immediately after eating is the exception. The worst combination is a large meal followed by intense core work within 30 minutes, which practically guarantees a reflux episode on semaglutide.
The semaglutide weight loss without exercise guide covers strategies for those whose reflux is severe enough to limit physical activity temporarily.
The connection between semaglutide, acid reflux, and other GI symptoms
Acid reflux rarely occurs in isolation on semaglutide. Understanding how it connects to other GI symptoms helps you address the root causes rather than treating each symptom separately.
Reflux and nausea
These two symptoms feed each other in a vicious cycle. Nausea causes retching that weakens the lower esophageal sphincter. Reflux causes esophageal irritation that triggers more nausea. Breaking this cycle requires addressing both symptoms simultaneously. Anti-nausea strategies (ginger, smaller meals, staying hydrated) indirectly reduce reflux, while anti-reflux measures (acid suppression, elevation) reduce the nausea caused by acid irritation. Understanding how semaglutide makes you feel overall helps differentiate between normal adjustment and symptoms needing intervention.
Reflux and bloating
Semaglutide bloating and reflux share the same root cause: delayed gastric emptying leading to increased stomach volume and pressure. Addressing one typically improves the other. Gas-producing foods (beans, cruciferous vegetables, carbonated drinks) worsen both conditions simultaneously.
Reflux and constipation
Semaglutide constipation creates back-pressure throughout the GI tract. When the colon is full and distended, it takes up more space in the abdominal cavity, pushing against the stomach and increasing reflux risk. Maintaining regular bowel movements through adequate fiber, hydration, and gentle movement helps reflux management indirectly.
Reflux and sulfur burps
Sulfur burps on GLP-1 medications often accompany reflux and share similar triggers. The combination of delayed emptying and fermentation of food in the stomach produces hydrogen sulfide gas, which creates both the characteristic egg-like smell and the belching that brings acid up with it.
Long-term considerations for semaglutide users with acid reflux
If you plan to use semaglutide long-term, understanding the chronic reflux implications helps you make informed decisions about monitoring and management.
PPI safety for long-term use
Extended PPI use (longer than 8 weeks at full dose) carries potential risks including magnesium depletion, B12 deficiency, slightly increased fracture risk, and possible kidney effects. If you need ongoing PPI therapy, work with your prescriber to find the lowest effective dose. Consider periodic attempts to step down to H2 blockers or lifestyle management alone. Get baseline and periodic monitoring of magnesium and B12 levels.
B12 supplementation may be particularly important if you are combining long-term semaglutide use with PPI therapy, as both can reduce B12 absorption through different mechanisms.
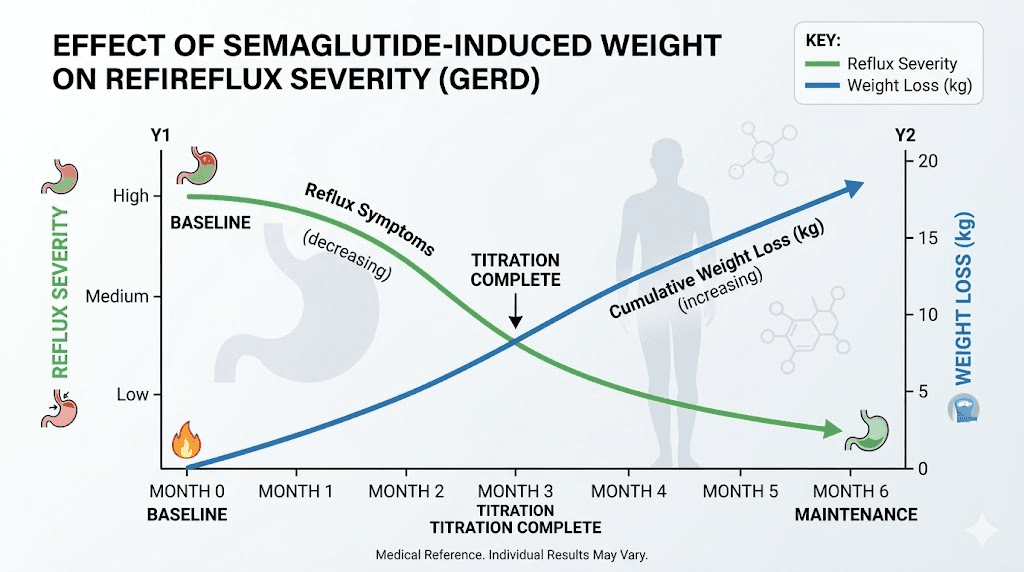
Weight loss and reflux improvement
Here is the encouraging long-term picture. As semaglutide produces weight loss, reflux typically improves progressively. Every 10% reduction in body weight significantly decreases GERD symptoms and may even eliminate the need for acid-suppressing medication. The early results might not show this improvement yet, but by months 3 to 6, the weight loss benefit to reflux becomes apparent.
This creates a situation where semaglutide initially worsens reflux through delayed emptying but ultimately improves it through weight loss. The management challenge is getting through the early phase with minimal discomfort while the weight loss catches up to provide its own protective effect.
Esophageal monitoring
If you have persistent reflux symptoms for more than 3 months despite adequate treatment, or if you have alarm symptoms (difficulty swallowing, pain with swallowing, unintentional weight loss beyond therapeutic effects, anemia), endoscopic evaluation is appropriate. This is not to alarm you but to ensure that chronic acid exposure has not caused changes to the esophageal lining that need specific monitoring or treatment.
For researchers serious about optimizing their GLP-1 protocols while managing side effects effectively, SeekPeptides provides comprehensive management guides, symptom tracking tools, and access to a community of experienced users who have navigated these exact challenges.
Frequently asked questions
Does semaglutide cause acid reflux in everyone?
No. Clinical trials show that approximately 5% of semaglutide users develop GERD symptoms, compared to 3% on placebo. Real-world rates may be higher at 10 to 15%, but the majority of users do not experience significant reflux. Individual responses vary widely based on pre-existing conditions, dose, diet, and lifestyle factors.
Will my acid reflux go away once I stop semaglutide?
In most cases, yes. Semaglutide-induced reflux is caused by delayed gastric emptying, which returns to normal after discontinuation. Most people see reflux resolve within 2 to 4 weeks of stopping the medication. However, if semaglutide unmasked a pre-existing GERD tendency, some degree of reflux may persist.
Can I take omeprazole with semaglutide?
Yes. There are no known drug interactions between semaglutide and proton pump inhibitors including omeprazole, esomeprazole, or lansoprazole. Many clinicians actively recommend PPI therapy for semaglutide users with significant reflux symptoms. Take the PPI 30 minutes before your first meal of the day for maximum effectiveness.
Is acid reflux worse with injectable or oral semaglutide?
Neither form is consistently worse. Injectable and oral semaglutide produce similar systemic GLP-1 effects once absorbed. However, oral semaglutide must be taken on an empty stomach, which some people find triggers morning nausea and reflux. Injectable users can time their dose more flexibly around meals.
Should I stop semaglutide if I get severe heartburn?
Do not stop semaglutide without discussing with your prescriber. Severe heartburn is manageable with appropriate medical therapy in the vast majority of cases. Stopping abruptly can trigger withdrawal effects and rapid weight regain. Instead, speak with your provider about dose adjustment, medication for reflux, or alternative approaches. Only stop if symptoms persist despite maximum therapy or if you develop alarm symptoms like difficulty swallowing or vomiting blood.
Does the brand of semaglutide matter for acid reflux?
Brand-name Ozempic and Wegovy use the same semaglutide molecule and produce identical effects including reflux risk. Compounded semaglutide contains the same active ingredient but may include additional compounds that could slightly alter the GI experience. Some patients report better tolerance with certain compounding pharmacy formulations, though this has not been systematically studied.
Can I take Tums while on semaglutide?
Yes. Over-the-counter antacids like Tums (calcium carbonate) are safe to use with semaglutide. They work by neutralizing existing stomach acid and provide quick relief for occasional breakthrough symptoms. They do not interfere with semaglutide absorption or effectiveness.
How long does semaglutide acid reflux last?
For most people, the worst reflux symptoms occur during the first 4 to 8 weeks of treatment or after dose increases, then gradually improve. By months 3 to 6, most users report significant improvement or complete resolution. The side effect timeline follows a predictable pattern for the majority of patients.
External resources
National Institute of Diabetes and Digestive and Kidney Diseases - Acid Reflux (GER and GERD)
American College of Gastroenterology - Acid Reflux Guidelines
PMC - Severe Reflux Oesophagitis Caused by GLP-1 Receptor Agonist
For researchers serious about managing every aspect of their peptide protocols, SeekPeptides offers evidence-based guides, comprehensive side effect management protocols, and a community of thousands who have navigated these exact situations successfully.
In case I do not see you, good afternoon, good evening, and good night. May your stomach stay calm, your esophagus stay clear, and your protocols stay effective.