Mar 20, 2026

Some people lose 20% of their body weight on GLP-1 medications and look incredible. Others lose the same amount and look deflated. Flat. Weak. The scale tells the same story for both groups, but the mirror tells a completely different one, and the difference almost always comes down to what happened to their muscle.
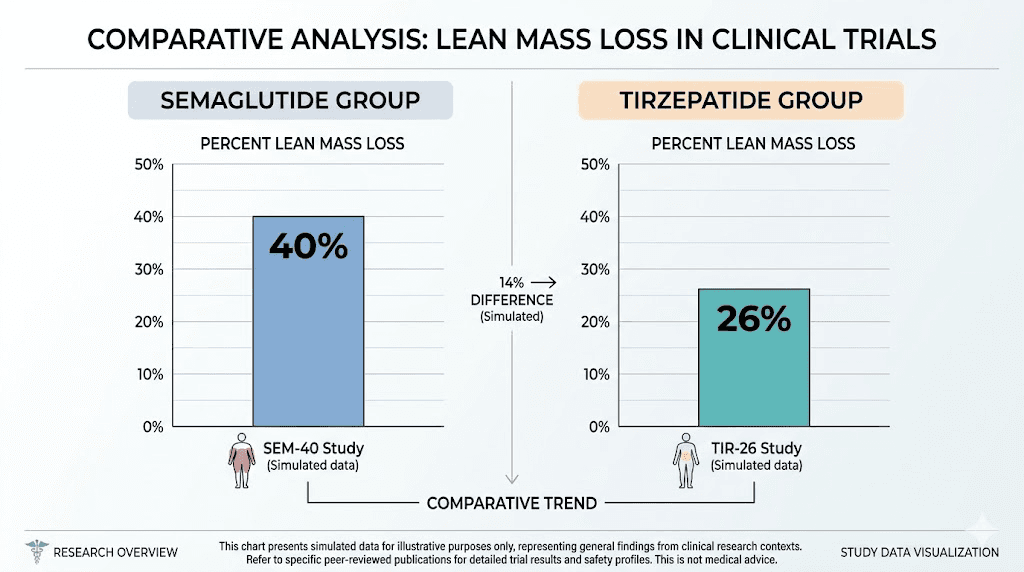
Here is the uncomfortable truth about semaglutide, tirzepatide, and every other GLP-1 receptor agonist on the market. They do not discriminate between fat and muscle when they trigger weight loss. Clinical trial data from the STEP-1 study showed that up to 40% of the weight participants lost on semaglutide came from lean body mass. Not fat. Muscle. The SURMOUNT-1 trial data for tirzepatide was more favorable at roughly 25%, but that still means a person losing 50 pounds could lose 12 or more pounds of pure muscle tissue. That is not a cosmetic problem. That is a metabolic disaster waiting to happen.
Creatine monohydrate, the most studied sports supplement in history, may be the single most effective tool for preventing this outcome. And the best part? There is no documented drug interaction between creatine and GLP-1 medications. They work through completely separate metabolic pathways. Combining them is not just safe for most people. It is strategic.
This guide covers everything researchers and users need to know about pairing creatine with GLP-1 medications, from the science behind muscle loss to specific dosing protocols, timing strategies, kidney function considerations, and the exact steps to preserve lean mass while maximizing fat loss. Whether you are on compounded semaglutide, brand-name tirzepatide, or considering retatrutide, the principles here apply across the board.
Why GLP-1 medications cause muscle loss
Understanding the problem is the first step toward solving it. GLP-1 receptor agonists trigger weight loss primarily through appetite suppression and delayed gastric emptying. People eat less. Sometimes dramatically less. And when caloric intake drops significantly, the body does not just burn fat for energy. It breaks down muscle protein too.
This is not a flaw in the medication. It is basic physiology. Every form of significant weight loss, whether from surgery, caloric restriction, or medication, carries some degree of lean mass loss. The body treats muscle as an expendable energy reserve when calories become scarce.
But GLP-1 medications create a unique problem. The appetite suppression they produce is so powerful that many users struggle to eat enough protein, and protein is the raw material the body needs to maintain muscle tissue. A person who was eating 2,200 calories daily might suddenly struggle to consume 1,200. If their protein intake drops from 120 grams to 50 grams, their muscles are being starved of essential amino acids regardless of what else they do.
The clinical data on lean mass loss
Numbers tell the real story. In the STEP-1 trial, 95 semaglutide-treated participants underwent body composition analysis using DXA scans. The results showed an average loss of 6.9 kilograms of lean soft tissue alongside 10.4 kilograms of fat mass. That means approximately 40% of total weight loss came from lean tissue rather than fat.
The SURMOUNT-1 trial painted a slightly better picture for tirzepatide. Among 124 participants with DXA data, participants lost 5.6 kilograms of lean soft tissue compared to 15.9 kilograms of fat mass. That translates to roughly 26% of weight loss coming from lean mass. Better than semaglutide, but still significant.
What does this look like in practice? A person who loses 60 pounds on semaglutide might lose 24 pounds of muscle. On tirzepatide, that number drops to around 15 pounds. Either way, the loss is substantial enough to reduce metabolic rate, decrease strength, impair functional capacity, and increase the risk of weight regain once the medication is discontinued.
The differences between semaglutide and tirzepatide side effects extend beyond nausea and GI symptoms. Muscle preservation might be one of the most underappreciated factors when choosing between these medications.
Why this matters beyond aesthetics
Muscle is not just about looking good. It is the largest metabolic organ in the body. Every pound of muscle burns approximately 6-7 calories per day at rest, while fat burns only 2. Losing 20 pounds of muscle means your resting metabolic rate drops by 120-140 calories daily. Over a year, that metabolic disadvantage adds up to roughly 15 pounds of potential weight regain.
This explains why so many GLP-1 users experience weight loss plateaus. Their bodies have adapted to the lower caloric intake by shedding metabolically expensive muscle tissue. The same mechanism explains why some people stop losing weight on semaglutide even though their appetite remains suppressed.
Muscle loss also affects bone density, insulin sensitivity, and functional independence as people age. For users over 40, the consequences of unchecked lean mass loss during GLP-1 therapy extend far beyond the scale. This is where creatine enters the conversation.
What creatine actually does in the body
Creatine is not a steroid. It is not a stimulant. It is not even remotely dangerous for healthy individuals. Creatine is a naturally occurring compound found in red meat and fish, and the human body produces about 1-2 grams of it daily through the liver, kidneys, and pancreas.
When you supplement with creatine monohydrate, you are increasing the amount of phosphocreatine stored in your muscles. Phosphocreatine serves as a rapid energy reserve. It regenerates adenosine triphosphate (ATP), the molecule your muscles use for immediate energy during high-intensity activities like lifting weights, sprinting, or any explosive movement.
More phosphocreatine means more ATP regeneration. More ATP means more capacity to train hard. And harder training is the single most powerful stimulus for telling your body to keep its muscle tissue.
Creatine and cellular hydration
Creatine also draws water into muscle cells. This intracellular hydration is not the same as bloating or water retention under the skin. The water goes inside the muscle cell itself, creating what researchers call a more anabolic cellular environment.
Think of it this way. A well-hydrated muscle cell functions better. It synthesizes protein more efficiently. It resists breakdown more effectively. And it signals to the body that this tissue is active, important, and worth preserving, even during a caloric deficit.
This cellular hydration effect matters enormously for GLP-1 users taking supplements because their bodies are already in a catabolic state from reduced caloric intake. Anything that tips the balance toward muscle preservation is valuable. Creatine does exactly that.
The research on creatine during caloric restriction
Multiple studies have examined creatine supplementation during periods of energy restriction, and the findings are consistent. A 2021 review published in Nutrients concluded that creatine supplementation during weight loss enhances lean mass retention and improves muscular strength.
Several trials in calorie-restricted settings show that creatine supplementation helps preserve up to 60% more lean mass compared to non-supplemented controls. When combined with resistance training, individuals maintaining creatine supplementation retained 95% of their muscle mass during caloric restriction, compared to 85% in the control group.
Those numbers matter. The difference between retaining 95% and 85% of your muscle during a 50-pound weight loss could mean the difference between looking toned and athletic versus looking thin but soft. It also means the difference between maintaining your metabolic rate and watching it plummet.
Safety of combining creatine with GLP-1 medications
This is the question most people ask first. And the answer is straightforward. There is no documented pharmacological interaction between creatine and any GLP-1 receptor agonist, including semaglutide, tirzepatide, retatrutide, or liraglutide.
The reason is simple. These substances work through completely different mechanisms and metabolic pathways. GLP-1 medications act on incretin receptors in the gut, brain, and pancreas. Creatine is stored in skeletal muscle and used for phosphagen energy production. They do not compete for absorption, metabolism, or excretion.
That said, there are practical considerations that deserve attention. Not dangerous interactions. Practical ones.
The kidney function question
This is where most confusion arises. Creatine supplementation can modestly increase serum creatinine levels in blood work. Creatinine is a waste product of creatine metabolism, and approximately 1-2% of the creatine stored in your muscles converts non-enzymatically to creatinine each day. Higher creatine stores mean slightly higher creatinine levels.
Here is the critical distinction. Elevated creatinine from creatine supplementation does not indicate kidney damage. It simply reflects higher creatine turnover. This is important because standard kidney function tests (eGFR calculated from creatinine) can be falsely low in creatine users, potentially triggering unnecessary alarm.
The solution is straightforward. If you are taking creatine and your doctor orders kidney function tests, request a cystatin C-based eGFR or enzymatic creatinine assay. These methods are not affected by creatine supplementation and provide accurate kidney function assessment. The KDIGO (Kidney Disease: Improving Global Outcomes) guidelines support this approach.
For reference, the following thresholds warrant medical attention regardless of creatine use:
eGFR below 45 mL/min/1.73m2: co-management with nephrologist advised
eGFR below 30 mL/min/1.73m2: nephrology referral recommended
Pre-existing kidney disease: physician consultation required before starting creatine
Decades of research on creatine supplementation in healthy adults have consistently shown no negative impact on renal function. But the keyword there is healthy. If you have pre-existing kidney conditions, talk to your doctor before adding creatine to your protocol.
Hydration considerations
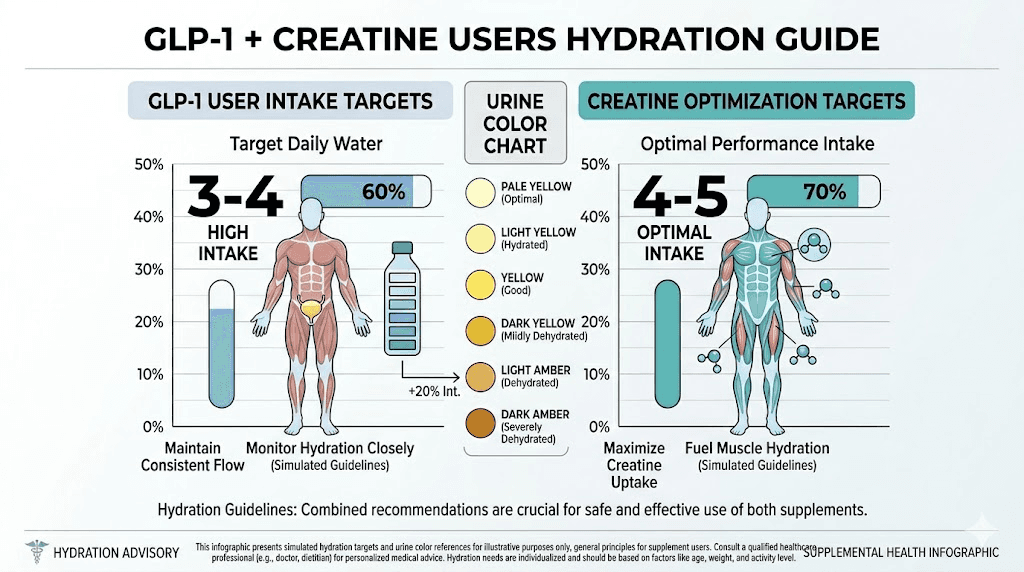
Both creatine and GLP-1 medications increase the importance of adequate hydration, but for different reasons.
Creatine pulls water into muscle cells. This means your overall fluid requirements increase. GLP-1 medications, particularly tirzepatide and semaglutide, can cause gastrointestinal side effects like nausea, vomiting, and diarrhea, all of which increase fluid losses. The combination means dehydration risk is real if you are not deliberately drinking enough water.
Target a minimum of 3-4 liters of water daily when combining creatine with GLP-1 therapy. Use urine color as your guide. Pale yellow means adequately hydrated. Dark yellow or amber means you need to drink more. This simple monitoring strategy prevents the most common practical issue with this combination.
Dizziness on semaglutide is often a hydration problem rather than a medication problem. Adding creatine without increasing water intake can make this worse.
The scale weight paradox
Creatine causes intracellular water retention in muscle tissue. For most people, this means an initial weight gain of 2-4 pounds when starting supplementation. This water weight is not fat. It is not subcutaneous bloating. It is water inside your muscle cells, which is actually a good thing.
But for someone tracking progress on tirzepatide or semaglutide by watching the scale, this initial weight increase can be psychologically challenging. You might see the scale go up 2-3 pounds in the first week of creatine supplementation, even though you are actually losing fat.
The solution? Track body composition, not just body weight. Waist measurements, progress photos, how your clothes fit, and if available, body fat percentage measurements through DXA or bioimpedance scales. These metrics tell the real story of what is happening to your body, and they will show that creatine is helping you lose fat while keeping muscle.
This is particularly relevant for people wondering why they are gaining weight on tirzepatide. If you recently started creatine, the scale increase is almost certainly water in your muscles, not fat gain.
How to dose creatine while on GLP-1 medications
Creatine dosing is simple. That is one of its biggest advantages. Unlike peptides that require precise dosage calculations and reconstitution protocols, creatine comes as a powder you mix into water or a shake.
The maintenance protocol (recommended for most people)
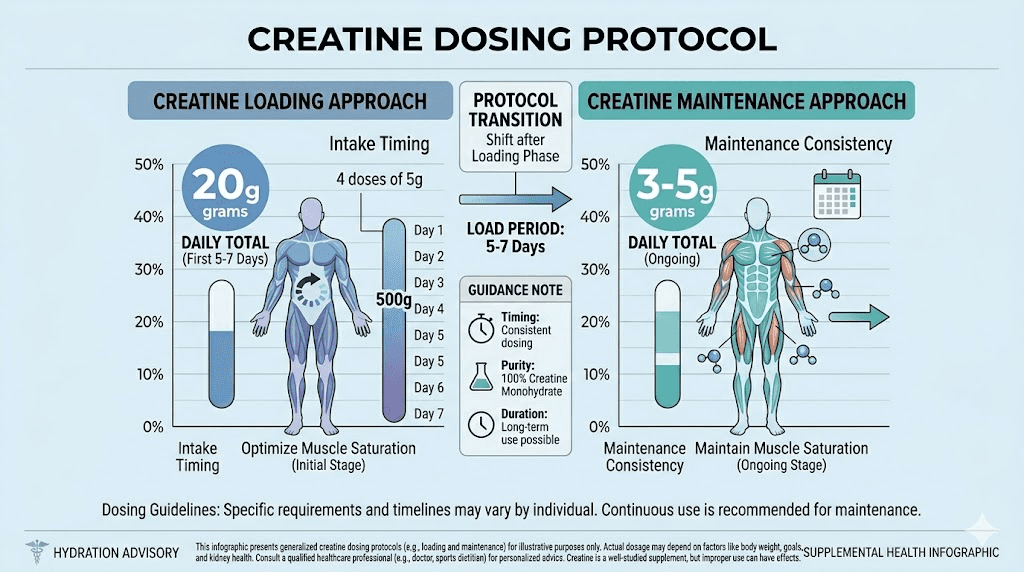
Take 3-5 grams of creatine monohydrate daily. Every day. Including rest days. Including days when you do not train. Consistency matters more than timing.
For most GLP-1 users, 5 grams daily is the ideal target. This accounts for slightly higher turnover rates during caloric restriction and ensures muscle saturation is maintained even when overall food intake is reduced.
Mix it into water, a protein shake, or any beverage. Creatine monohydrate dissolves reasonably well in room temperature liquid and has virtually no taste. Taking it with a meal or a small amount of carbohydrate enhances uptake into muscle cells, though this is an optimization rather than a requirement.
At 5 grams per day without a loading phase, your muscles will reach full creatine saturation in approximately 3-4 weeks. This is perfectly fine. There is no rush.
The loading protocol (optional, faster saturation)
Some people prefer to reach full muscle saturation faster. The loading protocol involves taking 20 grams of creatine daily, split into four 5-gram doses spread throughout the day, for 5-7 days. After the loading phase, drop to the standard 5-gram maintenance dose.
Loading saturates your muscles in about a week instead of three to four weeks. The end result is identical. The only advantage is reaching peak creatine stores sooner.
However, for GLP-1 users, loading carries a practical downside. Taking 20 grams of anything when your appetite is suppressed and your stomach is sensitive can cause GI discomfort. If you are already dealing with tirzepatide bloating or semaglutide burping, adding a loading protocol on top of that is asking for trouble.
The recommendation for most GLP-1 users is to skip the loading phase entirely. Start with 5 grams daily and let saturation build gradually. Your stomach will thank you.
Timing strategies
Research on creatine timing is mixed, but the consensus leans slightly toward post-workout consumption being marginally superior to pre-workout. A study comparing pre-workout versus post-workout creatine found slightly greater improvements in fat-free mass when creatine was taken after training.
That said, the timing difference is small. The most important factor is consistency. Taking 5 grams at the same time every day, whether that is morning, post-workout, or with dinner, is far more important than optimizing the exact minute you consume it.
A practical approach for GLP-1 users:
Training days: Mix 5g creatine into your post-workout protein shake
Rest days: Take 5g with your largest meal of the day (when your stomach is most likely to tolerate it)
Which form of creatine to use
Creatine monohydrate. Full stop.
The supplement industry has created dozens of creatine variations: creatine hydrochloride, creatine ethyl ester, buffered creatine, creatine magnesium chelate, and more. None of them have been shown to be superior to basic creatine monohydrate in any well-designed study. Many are significantly more expensive for no additional benefit.
Creatine monohydrate has over 500 published studies supporting its safety and effectiveness. It is also the cheapest form available. Look for products labeled as Creapure (a high-purity German-manufactured creatine monohydrate) if you want the highest quality, though any reputable brand of creatine monohydrate will work.
When to start creatine relative to your GLP-1 medication
Timing the introduction of creatine relative to your GLP-1 start date matters more than most people realize. Clinical guidance suggests allowing 8-12 weeks of GLP-1 dose titration and gastrointestinal adaptation before adding creatine supplementation.
Here is why. The first weeks on semaglutide or tirzepatide are often the roughest for GI side effects. Nausea, reduced appetite, occasional vomiting, and changes in bowel habits are common during dose escalation. Adding another supplement during this adjustment period complicates things unnecessarily.
If you experience GI symptoms, you want to know whether they are from the GLP-1 medication or from the creatine. Starting both simultaneously makes it impossible to identify the cause. And since GLP-1 side effects typically diminish after the first 4-8 weeks and stabilize during dose titration, waiting makes the process much smoother.
A practical timeline
Weeks 1-4: Start your GLP-1 medication at the prescribed starting dose. Focus on adjusting your diet, managing initial side effects, and establishing your eating patterns. Prioritize protein intake.
Weeks 5-8: Your body has adapted to the medication. GI side effects have largely subsided or become manageable. Begin resistance training if you have not already. This is the foundation that makes creatine supplementation worthwhile.
Weeks 9-12: You are on a stable GLP-1 dose, training regularly, and eating adequate protein. Now introduce creatine at 5 grams daily. Monitor for any GI changes (rare, but possible).
Week 13 onward: Full protocol is in place. GLP-1 medication for appetite control and metabolic benefits. Creatine for muscle preservation. Resistance training for the stimulus. Protein for the building blocks.
This phased approach reduces the risk of GI complications and gives you clear data on how each component affects your body. If something goes wrong, you know exactly what to adjust.
People who have been on GLP-1 medications for months already can start creatine immediately. The 8-12 week recommendation applies to new GLP-1 users who are still in the titration phase.
The complete muscle preservation protocol for GLP-1 users
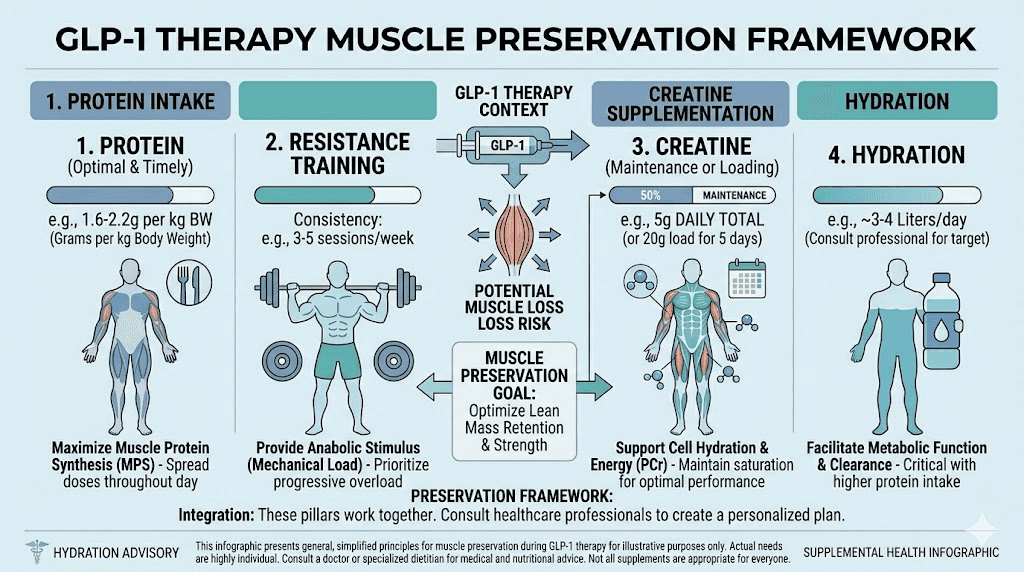
Creatine alone will not save your muscle. It is one piece of a four-part strategy that, when combined, can reduce lean mass loss from 40% down to 10-15% of total weight lost. That is a dramatic improvement. Here is the full protocol.
Pillar 1: Protein intake (the non-negotiable foundation)
No amount of creatine, training, or supplementation will preserve muscle if protein intake is too low. Protein provides the amino acids your body needs to repair, maintain, and build muscle tissue. During caloric restriction, the body increases protein oxidation for energy, making adequate intake even more critical.
Target 1.2-1.6 grams of protein per kilogram of body weight daily. For a 180-pound (82 kg) person, that means 98-131 grams of protein every day. For a 220-pound (100 kg) person, that means 120-160 grams daily.
This is challenging on GLP-1 medications because appetite is suppressed. Here are practical strategies:
Front-load protein at your first meal when appetite is strongest
Use protein shakes to supplement when solid food is unappealing
Choose protein-dense foods: Greek yogurt, eggs, chicken breast, fish, cottage cheese
Track protein intake for the first few weeks until you develop reliable habits
Consider collagen protein as an additional supplement (it counts toward total protein)
If you are struggling to hit protein targets, that problem needs solving before worrying about creatine timing or training optimization. Protein is the foundation everything else builds on.
Check our guides on foods to eat while on semaglutide and what to eat on tirzepatide for meal ideas that prioritize protein within reduced appetites.
Pillar 2: Resistance training (the essential stimulus)
Creatine without resistance training is like fuel without an engine. It helps, but nowhere near its full potential.
Resistance training sends a powerful signal to your body: this muscle is being used, do not break it down for energy. During caloric restriction, this signal becomes even more important. Without it, the body has no reason to prioritize muscle preservation over using muscle protein for energy.
The minimum effective dose for muscle preservation during GLP-1 therapy is 2-3 full-body resistance training sessions per week. These do not need to be two-hour bodybuilding workouts. They need to be structured, progressive, and focused on compound movements that engage multiple muscle groups simultaneously.
Essential compound movements:
Squats or leg press (lower body push)
Deadlifts or hip hinges (posterior chain)
Bench press or push-ups (upper body push)
Rows or pull-ups (upper body pull)
Overhead press (shoulders)
Training structure:
3 sets of 8-12 repetitions per exercise
Rest 2-3 minutes between sets
Progressive overload: gradually increase weight, reps, or sets over time
Total session time: 30-45 minutes
Progressive overload is the key principle. Your body only preserves muscle it believes it needs. If you are lifting the same weight for the same reps week after week, the stimulus is not strong enough to counteract the catabolic effects of caloric restriction.
Peptides for muscle growth can complement this approach, but resistance training is the fundamental requirement that no supplement can replace.
Pillar 3: Creatine supplementation (the amplifier)
With protein and training already in place, creatine amplifies their effects. It increases phosphocreatine stores, allowing you to train harder and recover faster. It hydrates muscle cells, creating a more anabolic environment. And it directly supports the metabolic processes involved in muscle protein synthesis.
The protocol is simple:
5 grams of creatine monohydrate daily
Every day, including rest days
Mixed into water, a shake, or any beverage
Taken with food when possible for optimal absorption
No cycling needed. No loading needed. No fancy timing needed. Just 5 grams, every day, consistently.
Pillar 4: Adequate hydration
Water ties everything together. Proper hydration supports creatine uptake into muscles, helps manage GLP-1 side effects like constipation, aids protein metabolism, and supports overall cellular function.
Minimum targets:
3-4 liters of water daily
Additional 500ml for every 30 minutes of exercise
Monitor urine color (pale yellow = adequate)
Increase intake if experiencing GLP-1-related GI side effects
Many of the common fatigue complaints on semaglutide and tiredness on tirzepatide improve dramatically with better hydration. Adding creatine makes hydration even more important.
Creatine and specific GLP-1 medications
While the general principles apply across all GLP-1 medications, there are nuances worth understanding for each specific compound.
Creatine and semaglutide
Semaglutide (branded as Ozempic and Wegovy) has the highest documented rate of lean mass loss among commonly prescribed GLP-1 medications, with the STEP-1 trial showing approximately 40% of weight loss coming from lean tissue. This makes creatine supplementation particularly valuable for semaglutide users.
Semaglutide users should be especially vigilant about protein intake and resistance training because the appetite suppression can be profound. Some people on higher doses report struggling to eat more than 800-1,000 calories daily, which makes it nearly impossible to consume adequate protein through food alone. Protein shakes become essential rather than optional in these cases.
If you are four weeks into semaglutide with no weight loss, the issue is unlikely to be muscle. But if you are losing weight rapidly without resistance training, you are almost certainly losing significant muscle mass alongside the fat.
Users on semaglutide with B12, semaglutide with glycine, or semaglutide with methylcobalamin can safely add creatine to their existing supplement stack. There are no interactions between these compounds.
For those on semaglutide with L-carnitine, the combination with creatine is actually complementary. L-carnitine supports fat oxidation while creatine supports muscle preservation. Together with adequate protein and training, this stack addresses both sides of the body composition equation.
Creatine and tirzepatide
Tirzepatide (branded as Mounjaro and Zepbound) is a dual GLP-1/GIP receptor agonist that shows somewhat better lean mass preservation than semaglutide alone, with the SURMOUNT-1 trial documenting approximately 25-26% lean mass loss. The GIP receptor activation may provide some additional muscle-protective effects, though the exact mechanism is still being studied.
Despite the better baseline, creatine supplementation remains strongly recommended for tirzepatide users. A 25% lean mass loss ratio still means significant muscle loss during substantial weight loss. And the potential to reduce that further with creatine, protein, and training is well worth the effort.
Tirzepatide users should pay particular attention to the bloating and GI side effects during dose titration. If GI symptoms are severe, delay creatine introduction until symptoms stabilize. There is no urgency. Starting creatine at week 10 instead of week 1 will not significantly affect long-term muscle preservation outcomes.
Those taking tirzepatide with B12, tirzepatide with glycine and B12, or tirzepatide with niacinamide can add creatine without concern. These supplements work through independent pathways and do not interact.
The tirzepatide-levocarnitine blend is particularly interesting when combined with creatine. Levocarnitine (L-carnitine) shuttles fatty acids into mitochondria for energy production, while creatine preserves the muscle cells that contain those mitochondria. The synergy is logical even if no specific study has tested this exact combination.
Creatine and retatrutide
Retatrutide is the newest triple agonist (GLP-1/GIP/glucagon) with the most aggressive weight loss profile. Early trial data showed weight loss of 24% or more of body weight, making muscle preservation even more critical for retatrutide users.
The glucagon receptor activation in retatrutide increases energy expenditure but may also increase protein catabolism. This means retatrutide users may experience higher rates of lean mass loss compared to single or dual agonists, though comprehensive body composition data from large trials is still emerging.
Creatine is arguably most important for retatrutide users given the magnitude of weight loss involved. The protocol remains the same: 5 grams daily, combined with resistance training and adequate protein. But the urgency is higher because more weight lost means more muscle at risk.
Compare the options in our comprehensive semaglutide versus tirzepatide versus retatrutide comparison.
Common mistakes when combining creatine and GLP-1 medications
Knowing what to do is only half the battle. Knowing what not to do prevents the most common pitfalls.
Mistake 1: Prioritizing creatine over protein
Creatine without adequate protein is like putting premium fuel in a car with a flat tire. It helps, but the fundamental problem remains unsolved. Too many people buy creatine powder and think the muscle preservation problem is handled, while eating 50 grams of protein daily.
Fix this first. Hit your protein target of 1.2-1.6 g/kg body weight every single day. Then add creatine. The order matters.
Mistake 2: Skipping resistance training
Creatine and protein without training stimulus will preserve some muscle, but nowhere near what the full protocol achieves. Your body needs a reason to keep muscle tissue. Loading and contracting that muscle under resistance provides that reason. Without it, even perfect nutrition and supplementation cannot fully prevent lean mass loss.
If you are not training, start. If you do not know how, hire a trainer for 3-5 sessions to learn the basic compound movements. This single investment pays dividends for the entire duration of your GLP-1 therapy.
Users who are trying to lose weight on semaglutide without exercise need to understand that while fat loss will still occur, muscle loss will be significantly higher without resistance training, regardless of creatine intake.
Mistake 3: Panicking about scale weight
The initial 2-4 pound weight gain from creatine water retention causes more unnecessary medication adjustments than almost any other factor. People see the scale go up, assume the GLP-1 medication stopped working, and request dose increases or medication switches.
Creatine weight gain is water inside muscle cells. It is beneficial. It is temporary in the sense that it stabilizes after the first week. And it does not reflect fat gain. Track measurements and body composition, not just the number on the scale.
This is a common reason people think tirzepatide is not working anymore or wonder why they are not losing weight on tirzepatide. In many cases, their medication is working perfectly. The scale is just being obscured by creatine water retention in muscles.
Mistake 4: Loading during GI-heavy periods
The 20-gram loading protocol during the first weeks of GLP-1 dose titration is a recipe for misery. Your gut is already adapting to a powerful medication that slows gastric emptying and changes bowel habits. Dumping 20 grams of additional powder into that environment four times a day will likely worsen nausea, bloating, and digestive discomfort.
Skip the loading phase if you are in the first 8 weeks of GLP-1 therapy or currently titrating to a higher dose. The 3-4 week gradual saturation from a standard 5-gram daily dose is perfectly adequate and far more tolerable.
Mistake 5: Neglecting hydration
Creatine pulls water into muscles. GLP-1 medications can cause fluid loss through GI side effects. The combination creates a hydration demand that many people underestimate. Dehydration impairs creatine uptake, reduces exercise performance, worsens GLP-1 headaches, and can confuse kidney function markers.
Three to four liters of water daily is the minimum. More if you exercise intensely or live in a hot climate. This is not optional when combining creatine with GLP-1 medications.
Body composition tracking during GLP-1 therapy with creatine
If you cannot measure it, you cannot manage it. And when combining GLP-1 medications with creatine, traditional weight tracking becomes misleading. You need better metrics.
Methods ranked by accuracy
DXA scan (gold standard): Dual-energy X-ray absorptiometry provides the most accurate breakdown of fat mass, lean mass, and bone mineral density. Getting a baseline scan before starting GLP-1 therapy and follow-up scans every 3-6 months gives you precise data on exactly how much fat versus muscle you are losing. Most imaging centers offer DXA scans for $50-150 without a prescription.
Bioimpedance scales: Consumer-grade smart scales that estimate body fat percentage using electrical impedance. Less accurate than DXA, especially during periods of hydration changes (which creatine creates), but useful for tracking trends over weeks and months. The individual readings may be off by 3-5%, but the direction of change is generally reliable.
Tape measurements: Waist circumference, hip circumference, arm circumference, and thigh circumference provide simple but valuable data. If your waist is shrinking while your arms and thighs are maintaining size, you are losing fat and keeping muscle. This requires only a fabric tape measure and 2 minutes.
Progress photos: Taken under consistent lighting, at the same time of day, wearing the same clothing. Photos capture changes that the scale misses entirely. A person can weigh the same but look dramatically different if they have lost fat and maintained muscle.
Strength metrics: Track your performance in the gym. If your squat, bench press, and deadlift numbers are maintaining or increasing, your muscle is being preserved regardless of what the scale says. Strength loss during GLP-1 therapy is an early warning sign of excessive lean mass loss.
How creatine affects each measurement
Understanding how creatine influences different metrics prevents misinterpretation:
Scale weight: Will increase 2-4 pounds initially, then stabilize. Masks true fat loss in the short term.
DXA lean mass: Will appear slightly higher due to intracellular water. This is accurate in that the muscle cells are genuinely more hydrated and functional.
Bioimpedance: May show artificially higher muscle mass readings due to increased water content affecting electrical conductivity. Trends are still useful.
Tape measurements: Minimally affected. Muscles may appear slightly fuller due to hydration, which is aesthetically positive.
Strength: Should improve or maintain. Creatine directly enhances strength performance, making this the most reliable metric.
Other supplements that work alongside creatine for GLP-1 users
Creatine is the cornerstone, but it works best as part of a comprehensive supplement strategy for GLP-1 users. Here are the evidence-based additions worth considering.
HMB (beta-hydroxy beta-methylbutyrate)
HMB is a metabolite of the amino acid leucine that has anti-catabolic properties. While creatine primarily works by enhancing training performance and cellular hydration, HMB directly inhibits muscle protein breakdown through the ubiquitin-proteasome pathway.
Standard dosing is 1.5-3 grams daily, split into 2-3 doses. Research shows HMB is most effective during caloric restriction, which is exactly the state GLP-1 users are in. Combining creatine and HMB addresses muscle preservation from two different angles: creatine enhances the anabolic stimulus, and HMB reduces the catabolic response.
Vitamin D
A 2023 retrospective analysis of over 461,000 GLP-1 users found that 7.5% developed vitamin D deficiency within six months. Vitamin D is essential for muscle function, calcium absorption, and bone health. Deficiency impairs muscle protein synthesis and increases the risk of sarcopenia.
Test your vitamin D levels before starting GLP-1 therapy and supplement to maintain levels between 40-60 ng/mL. Standard supplementation is 2,000-5,000 IU of vitamin D3 daily, ideally taken with a fat-containing meal for absorption.
Omega-3 fatty acids
Omega-3s (EPA and DHA) have mild anti-catabolic properties and reduce exercise-induced inflammation, potentially speeding recovery between training sessions. For GLP-1 users who are training regularly and eating in a caloric deficit, the anti-inflammatory benefits support consistent training frequency.
Standard dosing is 2-3 grams of combined EPA/DHA daily. Fish oil capsules or liquid form both work. Some users prefer algal omega-3 sources for sustainability reasons.
Electrolytes
Between creatine pulling water into muscles, GLP-1 medications causing GI-related fluid losses, and increased water intake diluting electrolytes, many users benefit from deliberate electrolyte supplementation. Sodium, potassium, and magnesium are the three most important.
Low magnesium in particular can cause muscle cramps, fatigue, and poor sleep, all of which impair training performance and recovery. A magnesium glycinate supplement (200-400mg before bed) addresses this common deficiency while improving sleep quality.
These supplements complement the full protocol described in our supplements to take with tirzepatide guide and our detailed GLP-1 supplement guide.
Creatine and specific populations on GLP-1 therapy
Not everyone on GLP-1 medications is a 35-year-old gym regular. Different populations have different considerations when adding creatine.
Users over 50
Older adults on GLP-1 medications face an amplified muscle loss risk. Age-related muscle decline (sarcopenia) was already occurring before the medication. Adding GLP-1-induced caloric restriction on top of age-related muscle loss creates a compounding effect that can significantly impair functional capacity.
Creatine is particularly well-studied in older adults. A meta-analysis of creatine supplementation in adults over 50 found significant improvements in lean mass, upper body strength, and lower body strength compared to placebo. The standard 5 grams daily dose applies regardless of age.
For this population, resistance training is especially critical. The combination of creatine plus resistance training in older GLP-1 users may be the most impactful intervention available for maintaining independence and functional capacity during weight loss.
Users with type 2 diabetes
Many GLP-1 users have type 2 diabetes, and creatine supplementation has shown interesting effects on glucose metabolism. Some studies suggest creatine may improve GLUT-4 translocation (the process by which glucose enters muscle cells), potentially offering a small additional benefit for blood sugar control.
There is no interaction between creatine and diabetes medications commonly paired with GLP-1 agonists, including metformin combined with semaglutide or metformin with tirzepatide. Creatine does not affect blood sugar in a clinically significant way, though it may provide marginal benefits alongside standard diabetic care.
Women on GLP-1 therapy
Women often express concern about creatine causing a bulky appearance or excessive weight gain. Neither happens. Creatine does not increase testosterone or cause masculine physical changes. The 2-4 pound water retention is intramuscular and typically makes muscles look slightly more defined, not bulky.
Women actually stand to benefit more from creatine during GLP-1 therapy because they typically have less muscle mass to begin with, making every pound of preserved muscle proportionally more important for metabolic rate and functional strength.
Women on GLP-1 medications who are concerned about semaglutide affecting their period or tirzepatide affecting their period should note that creatine has no documented effects on menstrual cycles or hormonal balance.
Users combining GLP-1 with other medications
For those on combination protocols like phentermine and semaglutide or phentermine and tirzepatide, creatine remains safe to add. Phentermine is a stimulant that does not interact with creatine metabolism.
Users on berberine with tirzepatide or berberine with semaglutide can also safely add creatine. Berberine affects glucose metabolism and AMPK activation, which operates independently of creatine phosphagen system.
The long game: creatine during and after GLP-1 therapy
Muscle preservation during GLP-1 therapy is not just about looking good during weight loss. It is about setting up long-term success after the medication is discontinued or reduced.
Why muscle matters for weight maintenance
The biggest predictor of successful weight maintenance after GLP-1 therapy is metabolic rate, and metabolic rate is primarily determined by lean body mass. People who preserve their muscle during weight loss have a higher resting energy expenditure, meaning they can eat more calories without regaining weight.
Consider two people who both lose 60 pounds on semaglutide:
Person A (no creatine, no training): Loses 24 pounds of muscle (40% lean loss). Metabolic rate drops by approximately 168 calories/day. After stopping semaglutide, they regain weight at a daily surplus equivalent to one banana.
Person B (creatine + training + protein): Loses 9 pounds of muscle (15% lean loss). Metabolic rate drops by approximately 63 calories/day. After stopping semaglutide, they have a much larger caloric buffer before weight regain begins.
That 105-calorie daily difference adds up to roughly 11 pounds of potential weight difference over a year. Muscle preservation is not vanity. It is the foundation of sustainable weight loss.
This is directly relevant to people experiencing semaglutide withdrawal symptoms or transitioning off GLP-1 medications. The more muscle you preserve during treatment, the smoother the transition to maintenance will be.
Continuing creatine after GLP-1 discontinuation
There is no reason to stop creatine when you stop GLP-1 medication. Creatine provides ongoing benefits for training performance, muscle maintenance, and even cognitive function regardless of whether you are taking a GLP-1 agonist.
In fact, the transition period after stopping GLP-1 therapy is when creatine is most important. Appetite returns. Caloric intake increases. The body is primed for weight regain. Having preserved muscle mass (and the metabolic rate it supports) provides a critical buffer during this vulnerable period.
Continue with 5 grams daily indefinitely. Creatine has been studied for long-term use (5+ years) with no adverse effects in healthy adults. The cost is minimal (approximately $10-15 per month for quality creatine monohydrate), making it one of the most cost-effective supplements available.
Creatine during GLP-1 dose reduction
Many people transition from full therapeutic doses to maintenance or microdosing protocols rather than discontinuing entirely. During dose reduction, appetite gradually returns while the metabolic benefits of the medication decrease. This is another period where muscle preservation matters enormously.
Keep creatine, protein, and training consistent during dose reductions. The goal is to transition from medication-supported weight maintenance to lifestyle-supported weight maintenance without losing the lean mass you fought to preserve.
Weaning off tirzepatide successfully requires maintaining the habits and supplements that preserved muscle during active treatment. Creatine is one of the easiest to maintain because it costs little, has no side effects, and requires no medical supervision.
Creatine, GLP-1, and exercise performance
One of the underappreciated benefits of creatine for GLP-1 users is its direct effect on training quality. And training quality directly determines muscle preservation outcomes.
How caloric restriction impairs training
When you eat in a significant caloric deficit (which GLP-1 medications reliably create), your body has less available energy for exercise. Training sessions feel harder. Recovery takes longer. Strength declines. Motivation drops. This creates a vicious cycle where the people who need training most are least able to train effectively.
Creatine directly counteracts this. By maintaining phosphocreatine stores in muscles, creatine ensures that your muscles have adequate energy for high-intensity contractions even when overall caloric intake is low. Users consistently report being able to maintain their pre-GLP-1 training intensity despite eating significantly fewer calories.
This matters because training intensity is the primary driver of muscle preservation stimulus. A set of squats at 80% of your max tells your body to keep its muscle. A set of squats at 50% of your max sends a weaker signal. Creatine helps you stay closer to 80% even when your diet is at 50% of its previous level.
Expected performance changes
Within 3-4 weeks of starting creatine (once muscle saturation is achieved), most people notice:
1-2 extra reps per set on compound exercises
Faster recovery between sets (reduced rest time needed)
Maintenance of training weights that were previously declining during caloric restriction
Improved workout energy and reduced perception of effort
Better muscle pumps during training (due to increased intracellular hydration)
These improvements are modest individually but compound dramatically over weeks and months of consistent training. The person who can do 10 reps instead of 8, recover in 2 minutes instead of 3, and maintain their working weights rather than watching them decline will preserve significantly more muscle over a 6-12 month GLP-1 treatment course.
For people wondering whether semaglutide gives you energy or tirzepatide gives you energy, the answer is generally no. But creatine provides the energy your muscles need for training even when your overall energy levels are lower from reduced caloric intake.
Frequently asked questions
Can you take creatine with semaglutide?
Yes. There is no documented drug interaction between creatine and semaglutide. They work through completely different metabolic pathways. Creatine is stored in skeletal muscle for energy production, while semaglutide acts on GLP-1 receptors in the gut and brain. Most healthcare providers consider this combination safe for individuals with normal kidney function. Check our full GLP-1 supplement guide for additional recommendations.
Can you take creatine with tirzepatide?
Yes. Creatine and tirzepatide do not interact pharmacologically. The FDA prescribing information for tirzepatide does not list creatine as a contraindicated supplement. Consider waiting 8-12 weeks after starting tirzepatide before adding creatine to avoid compounding GI side effects during dose titration. See our tirzepatide supplement guide for the complete stack recommendation.
Will creatine make me gain weight on GLP-1 medications?
Creatine causes an initial 2-4 pound increase in scale weight due to intracellular water retention in muscles. This is not fat gain. It is water inside muscle cells, which is beneficial for muscle preservation. After the first week, weight stabilizes and the ongoing fat loss from your GLP-1 medication will be clearly visible in body composition measurements, even if the scale moves slower than expected.
Does creatine affect kidney function tests while on GLP-1?
Creatine can modestly increase serum creatinine levels, which may cause standard eGFR calculations to appear lower than actual kidney function. This does not indicate kidney damage. If you are supplementing with creatine and need kidney function testing, request a cystatin C-based eGFR or enzymatic creatinine assay for accurate results. Decades of research confirm that creatine does not impair kidney function in healthy adults.
How much creatine should I take with GLP-1 medications?
Take 5 grams of creatine monohydrate daily. No loading phase is necessary, especially if you are experiencing GI side effects from your GLP-1 medication. Full muscle saturation occurs within 3-4 weeks at this dose. Take it with food when possible, and mixing it into a protein shake is an efficient way to combine two muscle-preservation strategies into one habit.
Should I stop creatine if I stop my GLP-1 medication?
No. Continue creatine indefinitely. The transition period after stopping GLP-1 therapy is actually when creatine and resistance training are most important for preventing weight regain. The muscle you preserved during treatment supports your metabolic rate and makes weight maintenance easier. Creatine is safe for long-term use and costs approximately $10-15 per month.
Does creatine help with GLP-1 fatigue?
Fatigue during GLP-1 therapy has multiple causes, including caloric restriction, dehydration, and nutrient deficiencies. Creatine does not directly address most of these causes. However, by maintaining phosphocreatine stores in muscles, creatine does support physical energy during training, which can reduce the perception of overall fatigue. Proper hydration (3-4 liters daily) and adequate protein intake typically have a larger impact on GLP-1-related fatigue than creatine alone.
Can creatine prevent the skinny-fat look from GLP-1 weight loss?
When combined with resistance training and adequate protein, creatine is one of the most effective tools for preventing the deflated, skinny-fat appearance that occurs when muscle is lost alongside fat. The SURMOUNT-1 trial data suggests that maintaining lean mass through targeted interventions can shift the composition of weight loss from 40% lean tissue to as low as 10-15% lean tissue, resulting in a more toned, athletic appearance at the same final weight.
External resources
Nutrition support during GLP-1 receptor agonist therapy: systematic review (PubMed)
Preservation of lean soft tissue during GLP-1-induced weight loss: case series (PubMed Central)
SURMOUNT-1: tirzepatide for the treatment of obesity (New England Journal of Medicine)
Body composition changes during tirzepatide treatment in SURMOUNT-1 (Diabetes, Obesity and Metabolism)
Timing, optimal dose, and intake duration of dietary supplements in sports nutrition (PMC)
For researchers serious about optimizing their protocols during GLP-1 therapy, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your muscles stay preserved, your creatine stay saturated, and your GLP-1 results stay permanent.