Feb 4, 2026

Most people start tirzepatide wrong. They jump straight to the standard 2.5 mg weekly dose, experience a wave of nausea that lasts for days, and either white-knuckle through it or quit entirely. Neither outcome is ideal. Neither is necessary.
There is a better way.
Microdosing tirzepatide means beginning at doses well below the FDA-approved starting point, sometimes as low as 0.25 mg, and titrating upward gradually over weeks or months. The concept borrows from a simple principle that experienced researchers already understand: the body adapts better to incremental changes than sudden ones. And when it comes to a dual GIP/GLP-1 receptor agonist as powerful as tirzepatide, giving your gastrointestinal system time to adjust can mean the difference between sticking with your protocol and abandoning it after week two.
This guide covers everything you need to build a microdosing tirzepatide chart that actually works. You will find week-by-week schedules, unit-to-milligram conversions for compounded formulations, strategies for splitting doses between men and women, and the clinical data behind why lower starting doses may reduce side effects without sacrificing long-term results. Whether you are new to GLP-1 peptides for weight loss or switching from semaglutide to tirzepatide, the dosing charts and protocols below will give you a clear path forward.
SeekPeptides members have been tracking microdosing protocols since compounded tirzepatide first gained traction, and the patterns that emerge from real-world use tell a more nuanced story than any single clinical trial can capture.
What microdosing tirzepatide actually means
The term gets thrown around loosely. Some people use it to describe any dose below the standard titration schedule. Others apply it specifically to sub-milligram doses that require compounded formulations. The distinction matters because your approach to microdosing will determine what form of tirzepatide you need, how you measure it, and what results you can realistically expect.
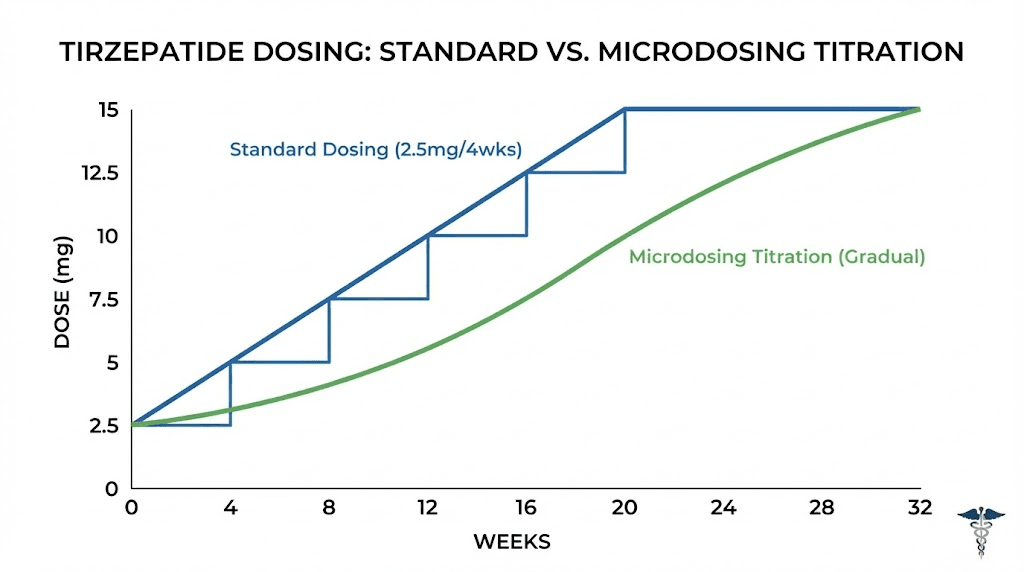
Standard tirzepatide dosing follows a clear FDA-approved path. You start at 2.5 mg once weekly for four weeks. Then you increase to 5 mg weekly for at least four more weeks. From there, your provider may increase the dose in 2.5 mg increments every four weeks until reaching a maintenance dose between 5 mg and 15 mg weekly. The tirzepatide dosing guide covers this standard escalation in full detail.
Microdosing sits below that floor.
True microdosing protocols begin at 0.125 mg to 0.5 mg weekly, doses that are one-fifth to one-twentieth of the standard starting point. At these levels, tirzepatide still activates both GLP-1 and GIP receptors, but the activation is gentler, more gradual, and far less likely to trigger the gastrointestinal side effects that make the first few weeks of standard dosing so difficult for many people.
A modified microdosing approach uses doses between 0.5 mg and 2.0 mg weekly. This range sits between true microdosing and the standard protocol. It is where most people who describe themselves as microdosing tirzepatide actually land. The goal is not to stay at sub-therapeutic doses forever but to build tolerance slowly enough that your body can adapt without the nausea, vomiting, and bloating that characterize rapid titration.
Why people choose to microdose tirzepatide
The reasons break down into three categories. Understanding which category applies to you will shape the protocol you follow.
Reducing gastrointestinal side effects
This is the primary driver. In the SURMOUNT-1 clinical trial, gastrointestinal adverse events were the most commonly reported side effects across all dose groups. Nausea affected a significant percentage of participants, and it was most pronounced during the dose-escalation period. The standard protocol already accounts for this by starting at 2.5 mg and increasing every four weeks, but for some people, even 2.5 mg hits too hard.
Tirzepatide slows gastric emptying. That is part of how it works. Food sits in your stomach longer, which promotes satiety and reduces calorie intake. But when this mechanism kicks in too aggressively, the result is persistent nausea, bloating, and sometimes vomiting. These symptoms are not dangerous, but they are deeply unpleasant, and they cause a meaningful percentage of people to discontinue treatment entirely.
In the SURMOUNT-1 trial, treatment discontinuation rates due to adverse events were 4.3% for the 5 mg group, 7.1% for the 10 mg group, and 6.2% for the 15 mg group. Those numbers might seem small, but they represent real people who gave up on a medication that could have helped them because the side effects were too much to tolerate. Microdosing attempts to solve that problem by giving the GI system more time to adapt.
The role of peptides in gut health is well documented. Tirzepatide interacts with gut receptors that influence motility, secretion, and inflammation. Starting at lower doses allows these systems to recalibrate gradually rather than being overwhelmed.
Sensitivity to medications
Some people are simply more sensitive to pharmaceutical interventions. They require lower doses of everything, from caffeine to cold medicine to peptides. For these individuals, jumping straight to 2.5 mg of tirzepatide can feel like jumping into the deep end of a pool when they have never been swimming. A microdosing chart gives them a shallow entry point.
Women tend to require lower starting doses than men, a pattern documented by Dr. Craig Koniver, who has suggested that women may do well starting at approximately 60% of the lowest standard dose (around 1.5 mg weekly) while men may tolerate starting at approximately 72% (around 1.8 mg weekly). This gender-based variation in response is consistent with how many peptides affect women differently than men.
Weight maintenance after initial loss
The third category involves people who have already lost significant weight on standard doses and want to step down to a maintenance protocol. The SURMOUNT-4 trial demonstrated that when participants switched from tirzepatide to placebo, they regained approximately 14% of their body weight over 52 weeks. Those who continued on tirzepatide experienced additional weight loss instead.
This creates a dilemma. Staying on high doses indefinitely works for weight maintenance but comes with ongoing side effects and cost. Stopping entirely leads to weight regain. Microdosing offers a potential middle ground, using lower doses to maintain some level of receptor activation, appetite regulation, and metabolic benefit without the full side effect burden of higher doses.
The data on this approach is limited. No randomized clinical trial has specifically studied microdose maintenance protocols for tirzepatide. But the theoretical framework makes sense, and anecdotal reports from communities tracking these protocols show promising patterns. The relationship between peptides and fat loss often involves finding the minimum effective dose that produces results while keeping side effects manageable.
The complete microdosing tirzepatide chart
What follows is a comprehensive week-by-week microdosing chart. This is not medical advice. This is a reference framework based on protocols reported by clinicians, compounding pharmacies, and real-world users. Your healthcare provider should guide your specific dosing decisions.
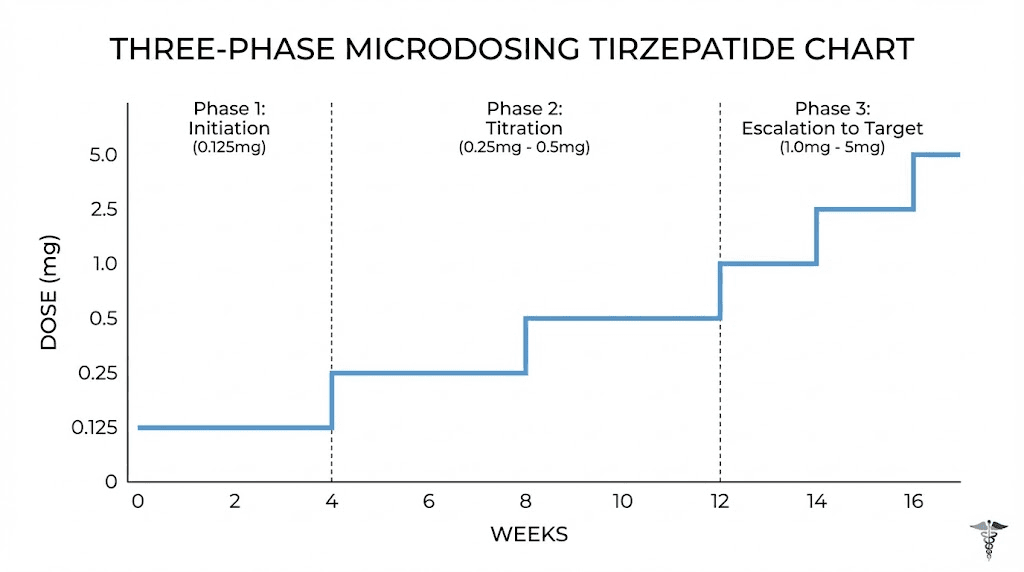
Phase 1: Ultra-low introduction (weeks 1 through 4)
The goal of phase one is simple. Introduce tirzepatide to your system at a dose low enough that your GI tract barely notices. You are not trying to lose weight yet. You are not trying to suppress appetite. You are laying groundwork.
Week | Dose (mg) | Frequency | Weekly total | Goal |
|---|---|---|---|---|
1 | 0.125 | Once weekly | 0.125 mg | Receptor priming |
2 | 0.25 | Once weekly | 0.25 mg | Tolerance building |
3 | 0.375 | Once weekly | 0.375 mg | Gradual adaptation |
4 | 0.5 | Once weekly | 0.5 mg | Baseline establishment |
At these doses, most people experience zero side effects. Some report a very mild reduction in appetite, particularly in the 24 to 48 hours after injection. Others feel nothing at all. Both responses are normal.
The key is patience. Do not rush through this phase because you feel fine. The point is to let your GLP-1 and GIP receptors begin responding to exogenous stimulation at a pace that does not overwhelm them. Think of it like stretching before exercise. The peptide dosing guide explains why gradual titration matters for all peptide protocols, not just tirzepatide.
Phase 2: Building therapeutic range (weeks 5 through 10)
Now you begin to approach doses where tirzepatide starts producing noticeable effects. Appetite reduction becomes more apparent. Some people notice changes in food preferences, particularly a decreased desire for high-calorie foods. Energy levels may shift. This is where the medication begins to do its work.
Week | Dose (mg) | Frequency | Weekly total | Goal |
|---|---|---|---|---|
5 | 0.75 | Once weekly | 0.75 mg | Early appetite modulation |
6 | 1.0 | Once weekly | 1.0 mg | Metabolic activation |
7-8 | 1.5 | Once weekly | 1.5 mg | Sustained appetite control |
9-10 | 2.0 | Once weekly | 2.0 mg | Pre-standard stabilization |
During this phase, you might experience the first hints of GI side effects. Mild nausea is common, usually appearing within 12 to 24 hours of injection and resolving within a day or two. If nausea becomes persistent or severe at any dose, the protocol is straightforward: hold at your current dose for an additional week or two before increasing. There is no penalty for going slow. The only mistake is pushing through side effects that make you want to quit.
Many people who microdose tirzepatide report that phase two is where they start seeing measurable weight loss, even at doses well below the standard starting point. The best peptides for weight loss work through multiple mechanisms simultaneously, and tirzepatide activates both GIP and GLP-1 pathways, meaning even modest receptor activation can produce metabolic benefits.
You can use the semaglutide dosage calculator as a reference point for understanding how GLP-1 dosing works in general, though tirzepatide has its own unique pharmacokinetic profile due to its dual receptor mechanism.
Phase 3: Standard therapeutic entry (weeks 11 through 16)
By week 11, you have given your body ten weeks of gradual adaptation. Your GLP-1 and GIP receptors have been activated at progressively higher levels. Your GI system has adjusted to the slowed gastric emptying that tirzepatide causes. You are ready to enter the standard dosing range.
Week | Dose (mg) | Frequency | Weekly total | Goal |
|---|---|---|---|---|
11-12 | 2.5 | Once weekly | 2.5 mg | Standard starting dose |
13-16 | 5.0 | Once weekly | 5.0 mg | First therapeutic plateau |
For many microdosers, 2.5 mg feels remarkably manageable when reached through gradual titration rather than as a starting point. The nausea that might have been debilitating at week one is now mild or absent at week eleven. The appetite suppression that might have felt overwhelming is now a controlled, comfortable reduction in hunger.
This is the payoff. The extra weeks invested in microdosing translate into a smoother experience at therapeutic doses, better adherence to the protocol long-term, and potentially better outcomes. The full tirzepatide dosing guide covers what happens beyond week 16 as you continue titrating toward your maintenance dose.
Microdosing charts for men versus women
Body composition, hormone levels, and metabolic rate all influence how tirzepatide behaves in your system. The same dose does not produce identical effects in a 240-pound man and a 150-pound woman. Acknowledging this reality makes microdosing protocols more effective.
Microdosing chart for women
Women generally respond to lower doses of tirzepatide. This is consistent with how peptides work in women over 40 and aligns with clinical observations about gender-based differences in GLP-1 sensitivity.
Week | Dose (mg) | Notes |
|---|---|---|
1-2 | 0.125 | Assess baseline tolerance |
3-4 | 0.25 | Monitor for any GI symptoms |
5-6 | 0.5 | First appetite changes expected |
7-8 | 1.0 | Noticeable hunger reduction |
9-10 | 1.5 | Approach standard entry point |
11-14 | 2.5 | Standard starting dose reached |
15+ | 3.5-5.0 | Titrate based on response |
Women may find that they achieve satisfactory appetite control and weight loss at doses that would be considered sub-therapeutic for men. A woman maintaining at 5 mg weekly may experience the same relative benefit as a man at 7.5 mg or 10 mg. This is not a rule, but a pattern worth discussing with your healthcare provider. The safest peptides for women all share this principle: start lower, titrate slower, and let the response guide the protocol.
Hormonal fluctuations during the menstrual cycle can also affect tirzepatide tolerance. Some women report increased nausea during the luteal phase (the two weeks before menstruation). If you notice this pattern, consider timing your dose increases for the follicular phase when GI tolerance tends to be higher. Women navigating menopause-related weight challenges may find microdosing particularly useful, as hormonal changes during perimenopause and menopause can increase sensitivity to GLP-1 medications.
Microdosing chart for men
Men typically tolerate slightly higher starting doses and faster titration. But "slightly" is the operative word. The difference is not dramatic enough to justify skipping the gradual approach entirely.
Week | Dose (mg) | Notes |
|---|---|---|
1-2 | 0.25 | Assess baseline tolerance |
3-4 | 0.5 | Monitor GI response |
5-6 | 1.0 | First metabolic effects |
7-8 | 1.5-1.8 | Building toward therapeutic range |
9-10 | 2.5 | Standard starting dose reached |
11-14 | 5.0 | First therapeutic plateau |
15+ | 7.5-10.0 | Titrate based on response |
Men carrying significant visceral fat may respond especially well to tirzepatide because the GIP receptor activation specifically targets fat metabolism in ways that peptides for visceral fat loss exploit. The dual mechanism of tirzepatide means it attacks both the appetite side (through GLP-1) and the metabolic side (through GIP) simultaneously, making it particularly effective for the kind of stubborn abdominal fat that many men struggle with.
Men interested in combining weight loss with muscle preservation should also explore how peptides support both weight loss and muscle gain.
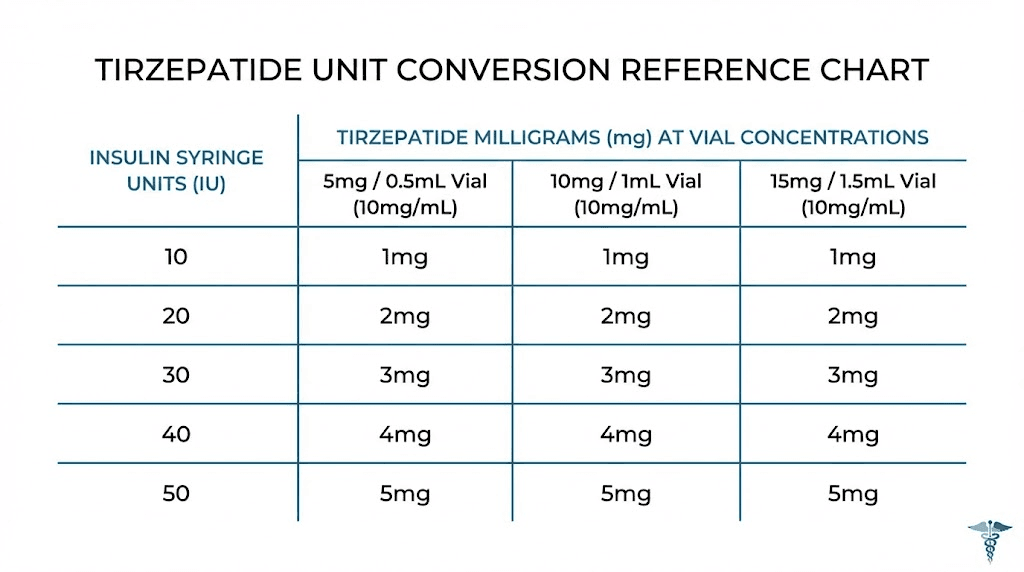
Understanding tirzepatide units and milligram conversions
This is where confusion multiplies. If you are using brand-name Zepbound or Mounjaro pens, dosing is simple because each pen delivers a fixed amount. But microdosing requires compounded tirzepatide, which comes in vials at various concentrations, measured in milligrams per milliliter. Converting between milligrams, milliliters, and insulin syringe units is essential.
The basics of unit conversion
An insulin syringe measures volume in "units" where 100 units equals 1 milliliter. This is a volume measurement, not a potency measurement. The amount of tirzepatide in those units depends entirely on the concentration of the solution.
Here is the critical relationship:
Dose (mg) = Volume (mL) x Concentration (mg/mL)
Or in syringe units:
Units to draw = (Desired dose in mg / Concentration in mg/mL) x 100
Common compounded tirzepatide concentrations
Concentration | 0.25 mg dose | 0.5 mg dose | 1.0 mg dose | 2.5 mg dose | 5.0 mg dose |
|---|---|---|---|---|---|
2.5 mg/mL | 10 units | 20 units | 40 units | 100 units | 200 units (2 draws) |
5 mg/mL | 5 units | 10 units | 20 units | 50 units | 100 units |
10 mg/mL | 2.5 units | 5 units | 10 units | 25 units | 50 units |
20 mg/mL | 1.25 units | 2.5 units | 5 units | 12.5 units | 25 units |
100 mg/mL | 0.25 units | 0.5 units | 1 unit | 2.5 units | 5 units |
This table is your cheat sheet. Find your vial concentration in the left column, then read across to find how many units to draw for your target dose. The peptide calculator can help you verify these numbers for your specific situation.
Notice how the same dose requires vastly different volumes depending on concentration. Drawing 0.25 mg from a 2.5 mg/mL vial means pulling 10 units. Drawing the same 0.25 mg from a 100 mg/mL vial means pulling a fraction of one unit, which is nearly impossible to measure accurately with a standard insulin syringe. This is why concentration matters enormously for microdosing. Higher concentration vials are designed for standard and higher doses. Lower concentration vials work better for microdosing because they allow for more precise measurement at small doses.
Understanding how to calculate peptide dosages is a foundational skill that applies to every reconstituted peptide, not just tirzepatide. The math is identical whether you are working with tirzepatide, BPC-157, or any other injectable peptide.
Choosing the right syringe for microdosing
Standard insulin syringes come in three sizes: 30-unit (0.3 mL), 50-unit (0.5 mL), and 100-unit (1.0 mL). For microdosing, the 30-unit syringe is almost always your best option because it has finer graduation marks that allow more precise dosing.
A 30-unit syringe typically has half-unit markings, meaning you can measure doses as small as 0.5 units. With a 5 mg/mL concentration, that translates to a minimum measurable dose of 0.025 mg, more than precise enough for any microdosing protocol. The fundamentals of peptide injection cover syringe selection, technique, and site rotation in greater detail.
How tirzepatide works at microdose levels
Understanding the mechanism helps explain why microdosing can produce benefits even at sub-therapeutic doses. Tirzepatide is not a simple on-off switch. It is a dual agonist that activates two distinct receptor systems, each with their own dose-response curves.
The dual receptor mechanism
Tirzepatide is the first approved dual GIP/GLP-1 receptor agonist. It activates both glucose-dependent insulinotropic polypeptide (GIP) receptors and glucagon-like peptide-1 (GLP-1) receptors. These two receptor systems overlap in some functions and diverge in others.
GLP-1 receptor activation produces several effects that researchers have studied extensively. It slows gastric emptying, which is the primary mechanism behind appetite suppression and also the primary cause of GI side effects. It enhances insulin secretion in response to glucose. It suppresses glucagon release, reducing the liver glucose output. And it acts on brain regions involved in satiety, particularly the hypothalamus and brainstem. The broader category of weight loss peptides leverages these same GLP-1 pathways.
GIP receptor activation adds a complementary layer. It improves beta-cell function in the pancreas. It influences fat metabolism directly, promoting more efficient energy storage and utilization. And research published in JCI Insight reveals something fascinating: tirzepatide shows an "imbalanced" affinity, engaging GIP receptors more strongly than GLP-1 receptors while producing biased signaling at the GLP-1 receptor that favors cAMP generation over beta-arrestin recruitment.
What does that mean in practical terms? It means tirzepatide activates GLP-1 receptors differently than pure GLP-1 agonists like semaglutide. The signaling profile may contribute to the superior weight loss outcomes tirzepatide produces in head-to-head comparisons and potentially explains why some people tolerate tirzepatide better than semaglutide despite its greater overall potency.
What happens at very low doses
At microdose levels (0.125 to 0.5 mg weekly), receptor activation is partial. Critics argue that ultra-low doses do not activate GLP-1 and GIP receptors enough to produce predictable metabolic changes. They are probably right in a strict pharmacological sense. These doses are sub-therapeutic, meaning they fall below the level that clinical trials have demonstrated to produce statistically significant weight loss.
But "sub-therapeutic" does not mean "zero effect." Receptor activation exists on a continuum, not as a binary threshold. Even at low doses, some degree of receptor engagement occurs. The GI effects are attenuated, which is exactly why people microdose, but metabolic effects are also attenuated. You trade side effects for slower, more gradual results.
The real value of microdosing is in the transition. You are not staying at 0.25 mg forever. You are using those early weeks to prepare your system for standard therapeutic doses. Think of it as the warm-up before the main event. The warm-up itself does not win the race, but it prevents injury and allows you to perform better when it counts.
Understanding how peptides work at the molecular level helps contextualize why gradual dose escalation produces different outcomes than immediate full-dose administration. Receptor desensitization, downregulation, and adaptation all play roles that are dose-dependent and time-dependent.
Clinical evidence: what the trials actually show
Honesty matters here. No randomized controlled trial has studied microdosing tirzepatide specifically. The protocols described in this article are based on clinician experience, compounding pharmacy guidelines, and community-reported outcomes. What the clinical trials do show is how tirzepatide performs at standard and higher doses, which gives us a framework for understanding what lower doses might achieve.
SURMOUNT-1 results by dose
The landmark SURMOUNT-1 trial enrolled 2,539 adults with obesity or overweight (BMI of 30 or higher, or 27 or higher with at least one weight-related complication). Participants were randomized to receive weekly injections of tirzepatide at 5 mg, 10 mg, or 15 mg, or placebo, for 72 weeks.
The results were striking.
Dose group | Average weight loss | Average pounds lost | Achieved 5% loss | Achieved 20% loss |
|---|---|---|---|---|
Placebo | 2.4% | 5 lbs (2 kg) | 35% | 3% |
5 mg weekly | 16.0% | 35 lbs (16 kg) | 85% | 32% |
10 mg weekly | 21.4% | 49 lbs (22 kg) | 89% | 50% |
15 mg weekly | 22.5% | 52 lbs (24 kg) | 91% | 57% |
Several things stand out. First, even the lowest dose (5 mg) produced an average weight loss of 16%, or about 35 pounds. That number exceeds what most older anti-obesity medications achieved at any dose. Second, there is a dose-response relationship, but it flattens at higher doses. The jump from 5 mg to 10 mg produced an additional 5.4% weight loss. The jump from 10 mg to 15 mg produced only an additional 1.1%. Third, 85% of people on just 5 mg achieved at least 5% weight loss, demonstrating that even the lowest studied dose produces clinically meaningful results for the vast majority of users.
What does this mean for microdosing? It suggests that the dose-response curve for tirzepatide is steep at the lower end. You get a lot of benefit from the first few milligrams. Each additional milligram produces diminishing returns. This is encouraging for anyone considering a lower-dose approach, because it implies that you do not need maximum doses to achieve meaningful outcomes. Exploring the full landscape of peptide stacks for weight loss reveals similar dose-response patterns across multiple compounds.
SURMOUNT-4: maintenance and weight regain
The SURMOUNT-4 trial addressed a critical question: what happens when you stop tirzepatide? After an initial treatment period, participants were randomized to either continue tirzepatide or switch to placebo.
Those who switched to placebo regained approximately 14% of their body weight over 52 weeks. Those who continued tirzepatide maintained their weight loss and experienced additional reduction. This finding underscores why maintenance dosing matters and why microdosing might serve as a viable long-term strategy for people who have achieved their weight loss goals but want to prevent regain without the side effects and costs of high-dose therapy.
The research on maintaining muscle during peptide-assisted weight loss is equally relevant to the maintenance discussion, because preserving lean mass is critical for preventing metabolic slowdown during and after weight loss.
Compounded tirzepatide: what you need to know
Brand-name tirzepatide comes in pre-filled single-use pens (Zepbound and Mounjaro) at fixed doses: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg. These pens are designed for one injection and cannot be used for microdosing because there is no way to deliver a fraction of the pen contents accurately.
Microdosing requires compounded tirzepatide. This is a formulation prepared by a compounding pharmacy that comes in a multi-use vial with a specified concentration, allowing you to draw precisely the amount you need using an insulin syringe.
Regulatory landscape
The regulatory situation for compounded tirzepatide has shifted significantly. In March 2025, the FDA ended enforcement discretion for compounded tirzepatide after determining that no drug shortage exists. This means compounding pharmacies face restrictions on producing tirzepatide copies in most cases. However, compounding remains available in certain circumstances, particularly when a licensed prescriber determines a clinically significant difference for a specific patient.
This regulatory change has practical implications for microdosing. If compounded tirzepatide becomes less accessible, microdosing with brand-name pens is essentially impossible at sub-2.5 mg doses. Eli Lilly has also warned that using brand-name pens for multiple draws (to extract smaller doses) poses contamination risks because the pens lack preservatives and are approved for single use only.
The broader peptide regulation landscape is evolving rapidly. Staying informed about legal access to compounded peptides is essential for anyone following a microdosing protocol.
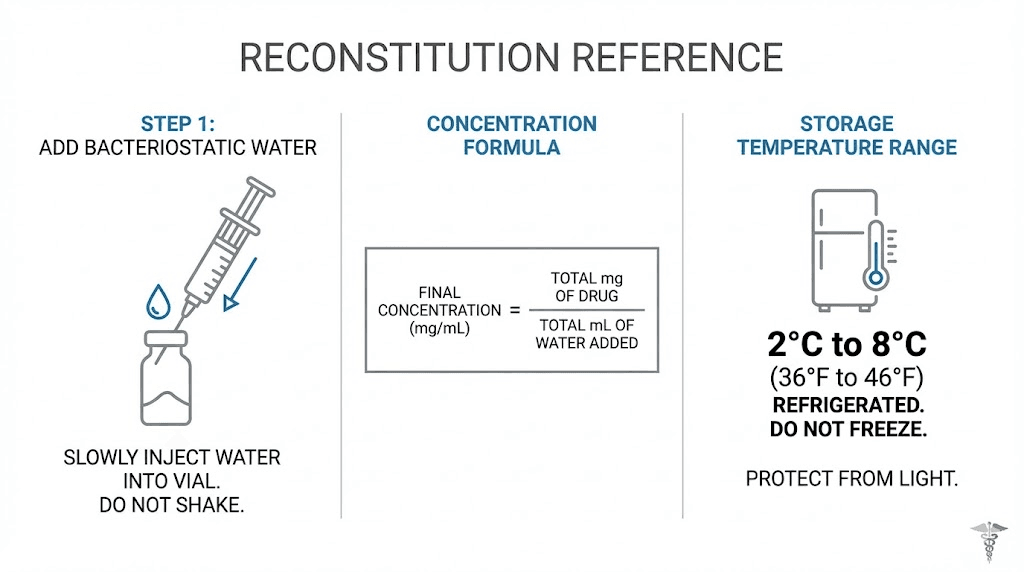
Reconstitution and storage
If you are working with compounded tirzepatide in a lyophilized (freeze-dried) form, you will need to reconstitute it before use. This process involves adding a specific volume of bacteriostatic water to the vial to achieve your target concentration.
The math is straightforward:
Concentration (mg/mL) = Total peptide in vial (mg) / Volume of water added (mL)
For microdosing, you want a lower concentration to make small doses easier to measure. If your vial contains 10 mg of tirzepatide and you add 4 mL of bacteriostatic water, you get a concentration of 2.5 mg/mL. At this concentration, 0.25 mg requires drawing 10 units on your insulin syringe, an amount that is easy to measure accurately.
Storage requirements are standard for reconstituted peptides: refrigerate at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius), never freeze, and protect from direct light. The peptide storage guide covers everything you need to know about maintaining potency after reconstitution. For specific reconstitution techniques, the peptide reconstitution guide walks through the process step by step.
Understanding bacteriostatic water quality and its role in preserving reconstituted peptides is crucial. Unlike sterile water, bacteriostatic water contains a small amount of benzyl alcohol that inhibits bacterial growth, allowing multi-use vials to remain safe for several weeks after reconstitution. The peptide reconstitution calculator can help you determine the exact amount of water to add for your desired concentration.
Injection technique for microdosing
Proper injection technique matters more at lower doses because small measurement errors represent a larger percentage of the total dose. Drawing 0.25 mg instead of 0.5 mg is a 50% error. Drawing 4.75 mg instead of 5.0 mg is a 5% error. Precision increases in importance as doses decrease.
Preparing the injection
Clean the vial stopper with an alcohol swab. Draw air into the syringe equal to the volume you plan to extract. Insert the needle through the stopper and inject the air. This equalizes pressure and makes drawing the liquid easier. Invert the vial, position the needle tip below the liquid surface, and slowly pull back the plunger to your target volume.
Check for air bubbles. Flick the syringe gently to move any bubbles to the top, then push the plunger slightly to expel them. Air bubbles in a subcutaneous injection are not dangerous, but they reduce the accuracy of your dose by displacing liquid volume. The peptide injections guide covers technique in comprehensive detail.
Injection sites and rotation
Subcutaneous injection sites include the abdomen (avoiding a two-inch radius around the navel), the front of the thighs, and the back of the upper arms. Rotate injection sites with each dose to prevent lipodystrophy, a condition where subcutaneous fat at the injection site changes texture due to repeated injections in the same location.
Insert the needle at a 45 to 90 degree angle depending on your body composition. Leaner individuals may need the 45 degree angle to ensure the needle reaches subcutaneous tissue without penetrating muscle. Inject slowly, hold for 5 to 10 seconds after the plunger is fully depressed, then withdraw. Understanding the differences between injectable and oral peptide delivery helps explain why subcutaneous injection remains the gold standard for tirzepatide administration.
Timing your weekly injection
Tirzepatide is administered once weekly. Choose a consistent day and time. Many people prefer injecting in the evening before bed so that any initial nausea occurs during sleep. Others prefer morning injections so the appetite-suppressing effects align with daytime eating patterns.
There is no clinical data suggesting one timing strategy is superior. Consistency matters more than timing. Pick a schedule that you can maintain reliably week after week. If you miss a dose, take it as soon as you remember as long as your next scheduled dose is at least three days away. If it is less than three days, skip the missed dose and resume your regular schedule.
Managing side effects during microdose titration
The whole point of microdosing is to minimize side effects. But some people experience them even at low doses, and knowing how to respond keeps your protocol on track.
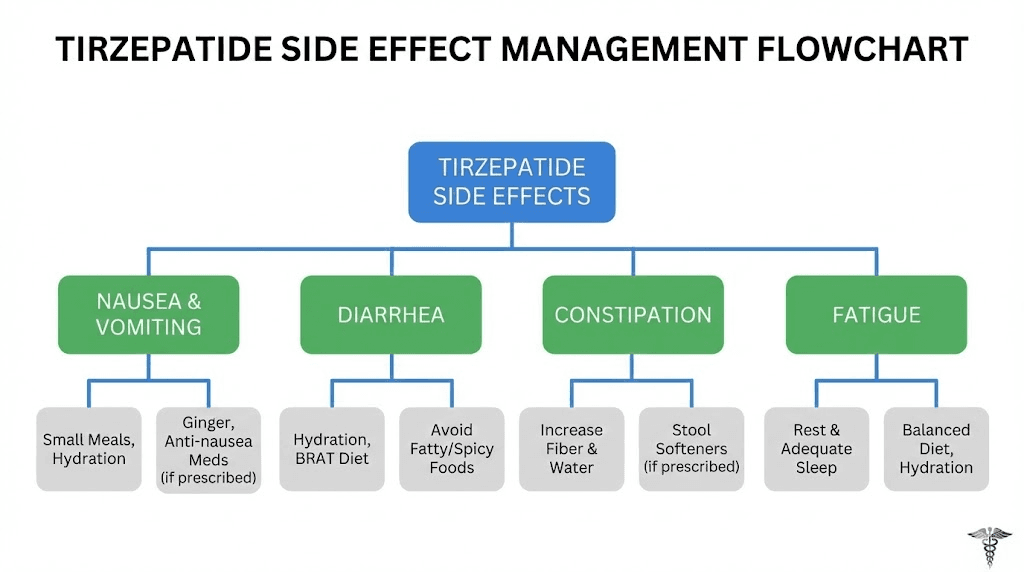
Nausea
The most common side effect at any dose. During microdosing, nausea tends to be milder and shorter-lived than during standard titration. If it occurs, these strategies help:
Eat smaller, more frequent meals instead of large ones
Avoid high-fat and greasy foods, which slow gastric emptying further
Stay hydrated, dehydration worsens nausea significantly
Ginger tea or ginger supplements have modest anti-nausea effects
Consider timing your injection before bed so nausea peaks during sleep
If nausea persists for more than three days after injection, or if it worsens with each dose, hold at your current dose for an additional one to two weeks before attempting an increase. Persistent nausea is your body telling you the dose is too much, too fast. The peptide safety guide covers when side effects warrant medical attention versus when they resolve with patience.
Constipation
Slowed gastric emptying can slow the entire digestive tract. Constipation affects a meaningful percentage of tirzepatide users at all doses. Preventive measures include increasing fiber intake gradually (not suddenly, which makes bloating worse), drinking at least 64 ounces of water daily, maintaining physical activity, and considering a magnesium supplement if dietary measures are insufficient.
Fatigue
Some people experience fatigue during the first few weeks of tirzepatide use, regardless of dose. This typically resolves as the body adapts. Reduced caloric intake can contribute, especially if the appetite suppression leads to unintentionally skipping meals. Ensuring adequate protein intake (at least 0.7 to 1.0 grams per pound of lean body mass) helps maintain energy levels. The best peptides for energy article explores how to address fatigue that persists beyond the adaptation period.
Injection site reactions
Redness, mild swelling, or itching at the injection site. These are generally benign and resolve within hours. If reactions persist or worsen, discuss with your healthcare provider. Switching injection sites with each dose minimizes this issue.
When to stop or seek medical attention
Microdosing does not eliminate all risk. Stop tirzepatide and contact your healthcare provider immediately if you experience severe abdominal pain that does not resolve (possible pancreatitis), vision changes, rapid heartbeat, signs of allergic reaction (rash, difficulty breathing, facial swelling), or symptoms of thyroid issues (lump or swelling in the neck, difficulty swallowing, persistent hoarseness). These are rare but serious. The common peptide mistakes guide includes a section on recognizing when side effects cross the line from expected to concerning.
Split-dose microdosing: an alternative approach
Instead of one weekly injection at a very low dose, some protocols divide the weekly amount into two or three smaller injections given on different days. The logic is that more frequent, smaller doses create a more stable blood level of tirzepatide throughout the week, potentially reducing side effects further while maintaining more consistent receptor activation.
How split dosing works
Weekly target | Split into 2 doses | Split into 3 doses | Schedule |
|---|---|---|---|
0.5 mg/week | 0.25 mg twice weekly | ~0.17 mg three times weekly | Mon/Thu or Mon/Wed/Fri |
1.0 mg/week | 0.5 mg twice weekly | ~0.33 mg three times weekly | Mon/Thu or Mon/Wed/Fri |
2.0 mg/week | 1.0 mg twice weekly | ~0.67 mg three times weekly | Mon/Thu or Mon/Wed/Fri |
2.5 mg/week | 1.25 mg twice weekly | ~0.83 mg three times weekly | Mon/Thu or Mon/Wed/Fri |
Split dosing requires more injections per week, which some people find inconvenient. But for those who experience a pronounced "surge and crash" pattern with weekly dosing, where side effects peak in the first 24 to 48 hours and appetite suppression wanes by day five or six, splitting the dose can smooth out the experience considerably.
The concept parallels how some peptide cycling protocols distribute doses across a week to maintain more consistent blood levels. The peptide stack calculator can help you plan multi-dose schedules.
Every-three-day dosing
Another variation uses an every-three-day schedule instead of weekly. For example, instead of 1.0 mg once weekly, you take approximately 0.43 mg every three days. This approach has been reported by some clinicians working with sensitive patients, though it requires careful tracking to avoid dosing errors.
One real-world example: a 54-year-old woman lost 38 pounds over 10 months using a microdosed tirzepatide protocol that started at 0.25 mg every four days and gradually worked up to 3 mg. Her results demonstrate that non-standard dosing schedules can produce meaningful outcomes, though they require commitment and consistency.
Microdosing tirzepatide for weight maintenance
After achieving your weight loss goal, the question becomes: what now? The data is clear that stopping tirzepatide entirely leads to significant weight regain. But maintaining high therapeutic doses indefinitely means ongoing costs and side effects.
The maintenance microdosing protocol
The idea is straightforward. After reaching your target weight on a standard dose, gradually titrate down to the lowest dose that maintains your results. This might be 2.5 mg weekly for some people. Others might find that 1.0 mg or even 0.5 mg provides enough appetite regulation and metabolic support to prevent regain.
Phase | Duration | Approach | Goal |
|---|---|---|---|
Active loss | Until target weight | Standard doses (5-15 mg) | Achieve weight loss goal |
Stabilization | 8-12 weeks | Hold at effective dose | Let body adjust to new weight |
Step-down | 12-24 weeks | Reduce by 1.25-2.5 mg every 4-6 weeks | Find minimum effective dose |
Maintenance | Ongoing | Lowest effective dose | Prevent regain |
The step-down phase is critical. Dropping from 15 mg to nothing is a recipe for rapid regain. Tapering gradually allows your body appetite regulation systems to partially readjust. Some people find a stable maintenance dose. Others discover that they cannot reduce below a certain threshold without weight creeping back.
Monitoring is essential during maintenance. Weigh yourself weekly at the same time under the same conditions. If weight increases by more than 3 to 5 pounds over two consecutive weeks, it may indicate that your maintenance dose is too low. Slight adjustments up, even by 0.5 mg per week, can recapture the effect. The peptide cycling guide discusses how to structure long-term protocols with built-in monitoring and adjustment points.
SeekPeptides members tracking maintenance protocols report that the minimum effective dose varies widely between individuals. Some maintain full results at 2.5 mg weekly. Others need 5 mg. A smaller number find they can maintain at sub-milligram doses when combined with consistent exercise and dietary habits. There is no universal maintenance dose, only your maintenance dose, discovered through careful, supervised titration.
Microdosing versus standard dosing: a direct comparison
Neither approach is objectively better. Each has trade-offs that matter differently depending on your priorities, health status, and goals.
Factor | Microdosing | Standard dosing |
|---|---|---|
Time to therapeutic dose | 10-16 weeks | 4-8 weeks |
GI side effects | Significantly reduced | Common during escalation |
Speed of weight loss | Slower initially | Faster initially |
Treatment adherence | Higher (fewer dropouts) | Lower (side effects cause quits) |
Requires compounded form | Yes (usually) | No (brand pens available) |
Clinical evidence | Limited (no RCTs) | Extensive (SURMOUNT trials) |
Cost | Variable (compounded pricing) | Brand-name pricing |
Provider support | Fewer experienced providers | Standard medical guidance |
The adherence factor deserves emphasis. The best protocol is the one you actually follow. A theoretically optimal dose means nothing if side effects cause you to skip weeks or stop entirely. If microdosing keeps you on track for 12 months while standard dosing would have caused you to quit at month two, the microdosing approach wins decisively in total outcomes.
This principle applies across all peptide dosing strategies. The optimal dose balances efficacy against tolerability against sustainability. Missing any one of those three factors undermines the other two.
Combining microdosed tirzepatide with lifestyle changes
Tirzepatide is not a standalone solution at any dose. But it is especially important to pair microdosing with lifestyle modifications, because the lower receptor activation at sub-therapeutic doses means you are relying more on behavioral changes to drive results during the early weeks.
Nutrition strategies
Tirzepatide reduces appetite, which means you will naturally eat less. But eating less of a poor diet is still a poor diet. The quality of what you eat matters as much as the quantity, especially at lower doses where appetite suppression is subtle rather than dramatic.
Prioritize protein. Aim for 0.7 to 1.0 grams per pound of lean body mass daily. Protein preserves muscle during weight loss, supports satiety between meals, and provides the amino acid building blocks that your body needs for repair and maintenance. The connection between peptides and muscle growth is well established, and adequate protein intake maximizes the muscle-sparing effects of any weight loss protocol.
Reduce ultra-processed foods. They trigger the reward pathways in your brain that GLP-1 medications help modulate. Eating fewer processed foods and more whole foods amplifies the appetite-regulating effects of tirzepatide, even at microdose levels.
Stay hydrated. Tirzepatide slows gastric emptying, and dehydration compounds the constipation and nausea that can result. Aim for at least half your body weight in ounces of water daily (a 200-pound person should drink at least 100 ounces).
Exercise considerations
Resistance training is non-negotiable during peptide-assisted weight loss. Without it, a significant portion of weight lost will come from muscle, not just fat. This reduces your metabolic rate and makes weight regain more likely.
Start with two to three resistance training sessions per week. Compound movements (squats, deadlifts, presses, rows) provide the most muscle-stimulating bang for your time investment. Add moderate cardiovascular exercise (walking, cycling, swimming) for heart health and calorie expenditure, but do not rely on cardio alone. The role of peptides in athletic performance extends beyond weight loss to include recovery, endurance, and muscle development.
Be aware that reduced caloric intake during the early weeks of microdosing may affect exercise performance. You might feel less energetic during workouts. This is normal and usually improves as your body adapts to its new eating patterns. Do not abandon exercise because it feels harder initially. Maintaining it is what protects your muscle mass and metabolic rate.
Sleep and stress management
Cortisol, the stress hormone, directly opposes many of the metabolic benefits tirzepatide provides. Chronic stress increases appetite, promotes fat storage (particularly visceral fat), and disrupts insulin sensitivity. Managing stress through consistent sleep (7 to 9 hours nightly), regular physical activity, and stress-reduction practices amplifies the effects of any tirzepatide protocol, micro or standard.
Poor sleep also increases ghrelin, the hunger hormone, and decreases leptin, the satiety hormone. These hormonal shifts can overpower the appetite-suppressing effects of low-dose tirzepatide. Getting your sleep right is not optional, it is a foundational requirement for the protocol to work as intended. Peptides for anxiety and stress may provide complementary support for people struggling with the cortisol side of the equation.
Common mistakes in tirzepatide microdosing
Mistakes happen. Some cost money. Others cost time. A few cost results. Here are the most frequent ones and how to avoid them.
Mistake 1: staying at microdoses too long
Microdosing is a bridge, not a destination. The goal is to reach therapeutic doses with fewer side effects, not to remain at 0.25 mg indefinitely. Some people get comfortable at low doses because side effects are minimal and there is a slight appetite reduction, so they stay there for months. The problem is that sub-therapeutic doses do not produce the metabolic changes needed for meaningful weight loss. If you have been at a microdose for more than eight weeks without increasing, reassess your protocol with your provider.
Mistake 2: wrong vial concentration for the dose
Using a 100 mg/mL vial to measure a 0.25 mg dose requires drawing 0.25 units, a nearly impossible amount to measure accurately with any insulin syringe. Always match your vial concentration to your dosing needs. For microdosing, concentrations of 2.5 to 5 mg/mL are ideal because they allow small doses to be measured in volumes that are practical and precise. The bacteriostatic water dilution guide explains how to achieve your target concentration during reconstitution.
Mistake 3: skipping meals entirely
Tirzepatide reduces appetite. That is the point. But some people, especially during the transition from microdose to standard dose, find that they have virtually no desire to eat. Going extended periods without eating is counterproductive. Your body needs adequate protein, vitamins, and minerals to function properly during weight loss. Aim for at least three small meals per day, even if appetite is minimal. A protein shake counts.
Mistake 4: not tracking progress
Without data, you are guessing. Track your weight weekly, note side effects and their severity, record your doses and any adjustments, and monitor energy levels, mood, and sleep quality. This information helps you and your provider make informed dosing decisions. It also helps identify patterns that might not be obvious otherwise. SeekPeptides provides tracking tools that members use to monitor their peptide protocols over time.
Mistake 5: contamination from multi-use brand pens
Attempting to microdose using brand-name Zepbound or Mounjaro pens by withdrawing small amounts across multiple sessions creates contamination risk. These pens contain no preservatives and are designed for single use. Compounded vials with bacteriostatic water are the appropriate format for multi-draw microdosing. The peptide shelf life guide explains how preservatives in bacteriostatic water protect against bacterial contamination in multi-use vials.
Tirzepatide microdosing and other peptide stacks
Some researchers explore combining microdosed tirzepatide with other peptides. The rationale is that lower tirzepatide doses leave more room for complementary compounds without overwhelming the system. While stacking introduces complexity, understanding the possibilities helps inform decisions.
Tirzepatide and BPC-157
BPC-157 is a gastric pentadecapeptide that demonstrates gut-protective and healing properties in research. Some people stack it with tirzepatide to counteract the GI side effects. The theory is that BPC-157's gastric protective mechanisms may reduce the nausea and GI distress that tirzepatide causes. This combination is not clinically studied, but the mechanistic logic is sound. The BPC-157 dosing guide covers standard protocols for this healing peptide.
Tirzepatide and cagrilintide
Cagrilintide paired with tirzepatide represents a combination that targets different pathways. Cagrilintide is a long-acting amylin analog that promotes satiety through distinct mechanisms from GLP-1 or GIP agonism. Adding a microdose of cagrilintide to a microdose of tirzepatide could theoretically produce additive appetite suppression through multi-pathway activation. The cagrilintide weight loss profile provides context on this emerging compound.
Tirzepatide and growth hormone peptides
Weight loss protocols that include muscle-preserving peptides address one of the main concerns about rapid weight loss: muscle wasting. Compounds like CJC-1295 and ipamorelin stimulate growth hormone release, which supports muscle maintenance and fat metabolism. Pairing these with microdosed tirzepatide creates a protocol that addresses weight loss, muscle preservation, and recovery simultaneously.
The peptide stack calculator helps researchers plan multi-compound protocols, and the guide to stacking multiple peptides explains the principles behind combining compounds safely.
How long before microdosed tirzepatide works
Expectations need calibrating. If you define "works" as significant weight loss, microdosing takes longer to produce visible results than standard dosing. The timeline depends on how quickly you titrate and what dose you ultimately reach.
Timeline of effects by phase
Weeks 1 through 4 (ultra-low doses, 0.125 to 0.5 mg): Most people feel nothing or very subtle appetite changes. Weight may fluctuate within normal range. This phase is about tolerance building, not results.
Weeks 5 through 10 (building doses, 0.75 to 2.0 mg): Appetite suppression becomes noticeable. Some people start losing 1 to 2 pounds per week. Food cravings, especially for high-sugar and high-fat foods, may decrease. Energy levels might shift as the body adjusts to reduced caloric intake.
Weeks 11 through 16 (standard therapeutic doses, 2.5 to 5.0 mg): Weight loss accelerates to rates consistent with clinical trial data. At 5 mg weekly, the SURMOUNT-1 trial showed average weight loss of 16% over 72 weeks. Most of that loss occurs during the first 40 weeks, with the rate being highest between weeks 8 and 24 of therapeutic dosing.
Weeks 17 and beyond (optimization phase): If weight loss plateaus and you have not reached your goal, further dose increases (up to 15 mg weekly) may be appropriate. The guide to peptide timelines provides realistic expectations for multiple compounds.
Patience is not just a virtue here. It is a strategy. People who rush through titration and experience severe side effects are more likely to abandon their protocol entirely. People who titrate slowly are more likely to reach and maintain therapeutic doses for the duration needed to achieve meaningful results. Over a 12-month horizon, the slower starter who maintains consistency almost always outperforms the fast starter who quits at month two.
The science of GIP and GLP-1 receptor sensitivity at low doses
To understand why microdosing works for some people and not others, you need to understand receptor sensitivity. Every person has a different baseline sensitivity to GIP and GLP-1 receptor activation. This is not a theory. It is documented in the pharmacology literature and explains why the same dose produces wildly different experiences in different people.
Receptor density and individual variation
GLP-1 receptors are distributed throughout the body. They are found in the pancreas (where they regulate insulin secretion), the stomach (where they slow gastric emptying), the brain (where they influence appetite and satiety), and the cardiovascular system (where they affect heart rate and blood pressure). GIP receptors are concentrated in the pancreas, adipose tissue, bone, and the central nervous system.
The density of these receptors varies between individuals. Some people have higher receptor density in their gut, making them more sensitive to the GI effects of tirzepatide. Others have higher density in the brain appetite centers, making them more sensitive to the appetite-suppressing effects. This variation explains why one person at 2.5 mg experiences debilitating nausea while another at the same dose barely notices a change in appetite. The peptide mechanism guide explains receptor dynamics in broader context.
Genetic factors contribute to this variation. Polymorphisms in the GLP1R gene affect receptor function and have been associated with differences in glucose metabolism, body weight, and response to GLP-1 medications. While genetic testing for GLP-1 receptor sensitivity is not yet standard clinical practice, the research points toward a future where dosing protocols could be personalized based on genetic profiles.
Receptor desensitization and tachyphylaxis
When receptors are exposed to an agonist continuously, they can become less responsive over time. This process, called desensitization or tachyphylaxis, is one reason why some people experience a "plateau" in tirzepatide effectiveness at a given dose. The receptors literally become less sensitive to the same level of stimulation.
Microdosing may actually help manage this process. By starting at very low levels of receptor activation and increasing gradually, you allow the receptors to adapt without the dramatic desensitization that can occur with sudden, high-level activation. Think of it like gradually increasing the volume on speakers versus turning them to maximum immediately. The gradual approach preserves sensitivity.
This concept is relevant for anyone considering peptide cycling strategies, because cycling between active use and rest periods can restore receptor sensitivity for multiple peptide types. The guide to cycling different peptides discusses how different compounds affect receptor sensitivity over time.
The pharmacokinetics of low-dose tirzepatide
Tirzepatide has a half-life of approximately five days, which supports once-weekly dosing. At standard doses, steady-state blood levels are reached after approximately four to five weeks of consistent weekly administration. At microdoses, the same pharmacokinetic principles apply, but peak blood levels are proportionally lower.
This means that at 0.25 mg weekly, the steady-state blood level of tirzepatide is approximately one-tenth of what it would be at 2.5 mg weekly. Whether this level is sufficient to produce meaningful metabolic effects depends on individual receptor sensitivity. For highly sensitive individuals, even one-tenth of the therapeutic concentration may produce noticeable appetite modulation. For less sensitive individuals, this level may produce no detectable effect at all.
The five-day half-life also explains why split dosing (dividing the weekly amount into two or three administrations) can smooth out the experience. Instead of a single peak followed by a gradual decline, multiple smaller peaks create a more stable blood concentration throughout the week. The comprehensive peptide dosing guide covers pharmacokinetic principles that apply across all injectable peptides.
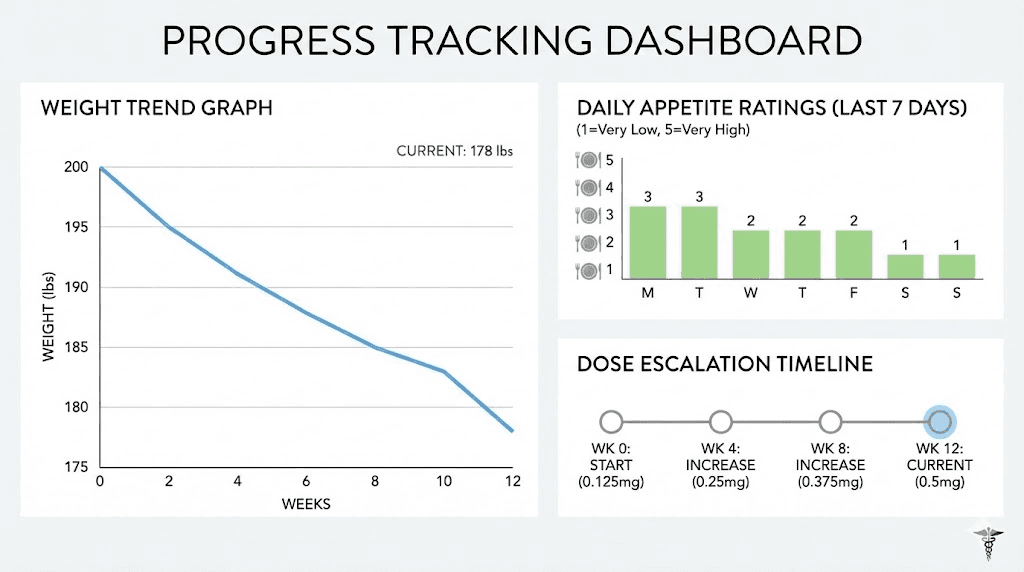
Tracking your microdosing progress effectively
Data drives decisions. Without systematic tracking, microdosing becomes guesswork. With proper monitoring, you can identify the exact dose where your body begins responding, spot side effects before they become problematic, and adjust your protocol based on evidence rather than intuition.
What to track daily
Keep a daily log that includes the following data points. It does not need to be elaborate. A simple spreadsheet or notebook entry works fine.
Appetite level: Rate on a 1 to 10 scale before each meal. This helps identify when tirzepatide begins affecting your hunger signals. A consistent drop from 7-8 to 4-5 before lunch, for example, indicates that appetite suppression is engaging.
GI symptoms: Record nausea, bloating, constipation, or diarrhea with severity (mild, moderate, severe) and duration. This data tells you whether to hold, increase, or adjust your dose at each titration point.
Energy levels: Note your subjective energy on the same 1 to 10 scale. Significant drops in energy may indicate insufficient caloric intake, dehydration, or a need to slow your titration schedule.
Food intake: You do not need to count every calorie, but recording general meal content and portion sizes helps correlate appetite changes with actual eating behavior. Sometimes people feel less hungry but eat the same amount out of habit, which undermines the protocol.
What to track weekly
Body weight: Weigh yourself at the same time, on the same day, wearing the same amount of clothing (ideally right after waking, after using the bathroom, before eating). Weekly weight fluctuates, so focus on the four-week average trend rather than any single reading.
Body measurements: Waist circumference, hip circumference, and if possible, a body composition measurement (using calipers, a smart scale, or DEXA scan). Weight alone does not tell the full story because you might lose fat while maintaining or gaining muscle, resulting in minimal scale movement despite significant body composition improvement. The peptides for belly fat article discusses why waist circumference often changes before the scale does.
Dose and timing: Record exactly what you injected, when, and at what injection site. This creates an audit trail that your healthcare provider can review during consultations.
What to track monthly
Progress photos: Take consistent photos under the same lighting, at the same angle, in the same clothing. Visual changes often appear before scale changes, especially in the first few months.
Blood work: If your provider recommends it, monthly or quarterly blood panels can track metabolic markers including fasting glucose, HbA1c, insulin levels, lipid profiles, and liver function. These objective markers confirm whether the protocol is producing metabolic benefits beyond weight loss. The peptide testing labs guide covers what to test and when.
SeekPeptides members use integrated tracking tools designed specifically for peptide protocol monitoring. These tools aggregate daily logs, weekly measurements, and dose history into a single dashboard that makes patterns visible at a glance. Having your data organized this way transforms the conversation with your healthcare provider from vague reports of how you feel into concrete, data-driven discussions about protocol optimization.
Tirzepatide microdosing for specific populations
Different populations face unique challenges with tirzepatide. Microdosing protocols can be adapted to address these specific needs.
People with type 2 diabetes
Tirzepatide was originally developed and approved for type 2 diabetes management (as Mounjaro) before receiving approval for weight management (as Zepbound). For people with type 2 diabetes, microdosing requires additional monitoring because even low doses can affect blood glucose levels.
The dual GIP/GLP-1 mechanism enhances insulin secretion in a glucose-dependent manner. This means it primarily boosts insulin when blood sugar is elevated, reducing the risk of hypoglycemia compared to some other diabetes medications. However, if you are also taking sulfonylureas or insulin, adding even a microdose of tirzepatide could push blood glucose too low. Close coordination with your endocrinologist or diabetes care provider is essential.
Blood glucose monitoring should increase in frequency during the microdosing titration phase. Check fasting glucose daily and postprandial glucose at least once daily until you establish how your body responds at each dose level. Understanding how pancreatic peptide hormones regulate blood sugar provides useful background for anyone managing diabetes with peptide-based therapies.
People with previous GI conditions
Individuals with a history of gastroparesis, irritable bowel syndrome, inflammatory bowel disease, or chronic nausea are among the strongest candidates for microdosing. Their GI systems are already compromised, making them more susceptible to the gastric-slowing effects of tirzepatide.
For these individuals, the ultra-low introduction phase (weeks 1 through 4 at 0.125 to 0.5 mg) may need to be extended to 6 or even 8 weeks. Each dose increase should be smaller, perhaps 0.125 mg instead of 0.25 mg. And the threshold for holding at a dose should be lower, meaning you stay at a dose longer at the first sign of GI distress rather than pushing through. Research into peptides that support gut health can identify complementary compounds that may ease the transition.
People over 60
Older adults metabolize medications differently due to changes in liver function, kidney function, body composition, and receptor sensitivity that accompany aging. They are also at greater risk of muscle loss during weight loss, which has more severe consequences for mobility, bone health, and independence than it does for younger populations.
Microdosing is particularly appropriate for older adults because it allows for slow, careful dose escalation that minimizes the risk of dehydration (from nausea and reduced fluid intake), excessive muscle catabolism (from rapid caloric deficit), and medication interactions (which become more common with polypharmacy in older populations). The longevity peptides guide covers compounds specifically relevant to aging populations.
Protein intake becomes even more critical for older adults on tirzepatide. Aim for at least 1.0 to 1.2 grams per pound of lean body mass daily, the higher end of the general recommendation. And prioritize resistance training, even if it means lighter weights and simpler movements. Maintaining muscle mass in older adults on GLP-1 medications is not just about aesthetics. It is about preserving functional independence. The safest peptides for muscle growth includes options that older adults may find appropriate under medical supervision.
Athletes and fitness-focused individuals
Some athletes use microdosed tirzepatide specifically to reduce body fat while preserving muscle mass and performance. The logic is that full therapeutic doses cause appetite suppression so dramatic that maintaining the caloric intake needed for training becomes nearly impossible. A microdose, by contrast, provides a modest metabolic nudge without obliterating appetite.
This approach has gained traction in fitness communities, particularly among people looking to get lean for competition or aesthetic goals without the muscle-wasting effect that aggressive caloric deficits produce. Typical athletic microdosing protocols stay in the 0.5 to 2.0 mg range and may be cycled (used for 8 to 12 weeks during a cutting phase, then discontinued during maintenance or building phases).
The athletic performance peptide guide covers how various compounds intersect with training goals. For athletes concerned about body composition specifically, the fat-burning peptides for men and weight loss peptides for women articles provide gender-specific context. Do note that drug testing implications apply for competitive athletes, and tirzepatide may be prohibited by certain sporting organizations.
What happens if microdosing does not work for you
Not everyone responds to microdosing. Some people titrate slowly, tolerate the low doses well, but never experience meaningful appetite suppression or weight loss until they reach standard therapeutic doses anyway. Others find that the slow approach simply tests their patience beyond what they can sustain.
Signs that microdosing may not be your best approach
If you have been at a dose for four or more weeks with zero noticeable changes in appetite, energy, or food behavior, and you have experienced no GI side effects whatsoever, you may be someone whose receptor sensitivity requires higher doses to engage. In this case, a faster titration to the standard 2.5 mg starting dose may be more appropriate.
If you are losing patience with the gradual approach and find yourself skipping doses or losing motivation, the psychological cost of microdosing may outweigh the physiological benefit. Adherence is everything. A protocol that keeps you engaged and consistent will always outperform one that is theoretically better but practically abandoned.
Alternative approaches
Standard titration with GI support: Start at the standard 2.5 mg and use anti-nausea strategies (ginger, small meals, hydration, timing injections at bedtime) to manage side effects rather than avoiding them through lower doses.
Switching to semaglutide: Some people who do not tolerate tirzepatide well (even at microdoses) do better on semaglutide. The GLP-1-only mechanism produces a different side effect profile, and the semaglutide versus tirzepatide comparison can help you evaluate which might suit your physiology better.
Non-GLP-1 alternatives: For people who cannot tolerate GLP-1 medications at any dose, other weight loss peptides work through different mechanisms. Compounds like AOD-9604 (a modified growth hormone fragment) and 5-amino-1MQ target fat metabolism without the GI effects that GLP-1 agonists produce. The alternatives to GLP-1 medications article provides a comprehensive overview of other options.
Combination strategies: Some providers combine a lower dose of tirzepatide with other compounds to achieve the desired metabolic effect without the side effects of high-dose monotherapy. The weight loss peptide stack guide explores these multi-compound approaches in detail.
Cost considerations for microdosing protocols
Cost is a practical factor that affects whether microdosing is feasible for your situation. The economics differ significantly between brand-name and compounded formulations.
Brand-name versus compounded pricing
Brand-name Zepbound and Mounjaro carry substantial retail prices. Because these pens deliver fixed doses, using them for microdosing wastes medication (if you use a single pen across multiple weeks, you risk contamination, and the remaining medication goes to waste). This makes brand-name pens economically impractical for microdosing.
Compounded tirzepatide has historically been less expensive per milligram. However, the regulatory landscape shift in 2025 has affected availability and pricing. The peptide cost calculator can help you compare the per-dose costs of different formulations and concentrations.
Cost per effective dose
Microdosing uses less medication per week during the titration phase, which means lower weekly costs during that period. However, the total treatment duration may be longer (because you spend additional weeks at sub-therapeutic doses), which partially offsets the per-week savings.
Consider the total cost over a 6 to 12 month period rather than the weekly cost alone. A 16-week microdosing protocol followed by standard dosing may cost roughly the same total amount as jumping straight to standard dosing for the same period, because the lower initial weekly costs are balanced by the additional weeks of treatment. The financial analysis parallels what researchers encounter with any peptide cost assessment, where the total protocol cost matters more than the per-unit price.
The hidden cost of quitting
The most expensive outcome is starting tirzepatide at a standard dose, experiencing intolerable side effects, and quitting after two to four weeks. You have spent the cost of one or two pens with nothing to show for it. Microdosing may have a slower start, but if it keeps you adherent for 12 months instead of quitting at month one, the return on investment is dramatically higher.
Frequently asked questions
Can I microdose tirzepatide with brand-name pens?
Not safely. Brand-name Zepbound and Mounjaro pens are single-use devices without preservatives. Drawing partial doses from these pens creates contamination risk and makes accurate measurement difficult. Microdosing requires compounded formulations in multi-use vials with bacteriostatic water that allows precise measurement of small doses.
Is microdosing tirzepatide FDA approved?
No. The FDA has approved tirzepatide (as Zepbound for weight management and Mounjaro for type 2 diabetes) at standard doses starting at 2.5 mg weekly. Microdosing is an off-label practice that has not been evaluated in randomized clinical trials. The peptide legality guide covers the regulatory framework for peptide use in detail.
How much weight can I lose with microdosed tirzepatide?
It depends entirely on how long you stay at microdoses versus how quickly you reach standard therapeutic levels. The SURMOUNT-1 trial showed 16% average weight loss at 5 mg weekly over 72 weeks. If you spend 10 weeks microdosing before reaching 2.5 to 5 mg, your results over 72 total weeks may be modestly lower due to the delayed therapeutic onset, but adherence benefits may compensate. Understanding fat-burning peptide mechanisms provides context for realistic expectations.
Can I combine microdosed tirzepatide with semaglutide?
This is not recommended. Both tirzepatide and semaglutide activate GLP-1 receptors. Combining them doubles the GLP-1 stimulation without the benefit of the unique GIP activation advantage tirzepatide provides. The semaglutide vs tirzepatide comparison explains why choosing one over the other makes more sense than stacking both.
What concentration should I ask for when ordering compounded tirzepatide?
For microdosing, a concentration of 2.5 to 5 mg/mL works best. This range allows you to measure doses as small as 0.125 mg using standard insulin syringes with reasonable accuracy. Higher concentrations (10+ mg/mL) are better suited for standard and higher doses. Use the reconstitution calculator to determine the right dilution for your specific vial.
Should I microdose if I have never used GLP-1 medications before?
Microdosing is most commonly used by people who are sensitive to medications, have a history of GI issues, or had previous difficulty tolerating GLP-1 agonists. If you have no such history, the standard starting dose of 2.5 mg weekly may be perfectly appropriate. Discuss your options with a healthcare provider who can assess your individual risk factors. The getting started with peptides guide provides a framework for new users.
How do I know when to stop microdosing and move to standard doses?
When you can tolerate your current dose for two weeks with minimal or no GI side effects, you are ready to increase. The microdosing phase ends when you reach 2.5 mg weekly (the standard starting dose). From there, follow the standard titration schedule with increases of 2.5 mg every four weeks as tolerated, up to a maximum of 15 mg weekly.
Is microdosing tirzepatide safe?
The safety profile of tirzepatide at standard doses is well established through the SURMOUNT and SURPASS clinical trial programs. Microdosing uses lower doses, which in principle carries a lower risk of dose-dependent side effects. However, the lack of clinical trial data specifically on microdosing means the safety profile at ultra-low doses has not been formally characterized. Working with a qualified healthcare provider is essential for monitoring and adjusting your protocol safely.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access personalized protocol builders, dosing calculators, and expert-reviewed guides that account for individual factors most resources overlook.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay precise, your tolerance stay strong, and your progress stay consistent.