Mar 22, 2026

You are losing muscle. Right now. On semaglutide. And the culprit is not the medication itself. It is the number of calories you are eating, or more precisely, the number you are not eating. Research shows that approximately 40% of the weight lost on semaglutide comes from lean mass, including muscle. That number should stop you cold. Because muscle is metabolically active tissue. It burns calories at rest. It keeps your metabolism humming along even when you are sleeping. And when it disappears, your metabolism slows, your results stall, and the weight comes back faster than it left.
The appetite suppression from semaglutide is powerful. So powerful that many people simply stop eating enough. They celebrate the lower number on the scale without realizing their body is cannibalizing its own muscle tissue to make up for the caloric shortfall. This is not a minor concern. It is the single biggest nutritional mistake people make on semaglutide, and fixing it requires understanding exactly how many calories your body needs, not just to lose weight, but to lose the right kind of weight.
This guide breaks down the precise calorie targets for semaglutide users based on body weight, activity level, dose phase, and individual goals.
You will learn how to calculate your personal calorie floor, how to structure your macronutrients to preserve muscle, and how to adjust your intake as the medication suppresses your appetite. Every recommendation here comes from clinical research and evidence-based nutrition science. SeekPeptides built this guide because getting calories wrong on semaglutide does not just slow your progress. It undermines the entire point of taking the medication in the first place.
How semaglutide changes your hunger and calorie intake
Understanding how semaglutide suppresses appetite is essential before setting calorie targets. The medication works by mimicking GLP-1, a hormone your gut naturally produces after eating. But semaglutide activates GLP-1 receptors in the brain far more intensely than natural GLP-1 ever could, fundamentally changing how hungry you feel, how quickly you feel full, and how often you think about food.
Clinical research tells the story in numbers.
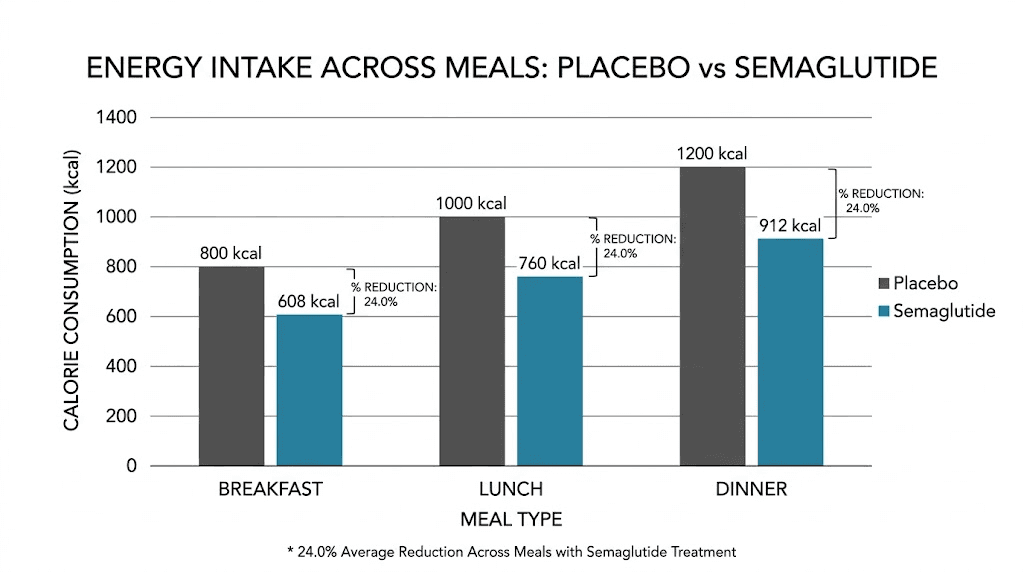
In a controlled study measuring ad libitum eating (meaning participants could eat as much as they wanted), semaglutide reduced total energy intake by 24% across all meals throughout the day. That is roughly 500 to 700 fewer calories consumed without anyone counting, restricting, or trying. The reduction happened automatically because participants simply wanted less food. They felt satisfied sooner. They stopped thinking about their next meal. The STEP 1 trial, published in the New England Journal of Medicine, showed that this sustained caloric reduction led to an average weight loss of 14.9% of body weight over 68 weeks. Compare that to just 2.4% with placebo. Among semaglutide users, 86.4% achieved at least 5% weight loss, 69.1% achieved 10% or more, and a remarkable 50.5% lost 15% or more of their starting weight.
But here is the problem nobody talks about.
A 24% reduction in energy intake sounds great on paper. But if you were already eating 1,800 calories before starting semaglutide, a 24% reduction puts you at roughly 1,370 calories per day. For many people, particularly men or those with higher body weights, that number falls dangerously close to or below the minimum threshold for adequate nutrition. And the appetite suppression does not discriminate between helpful calorie reduction and harmful calorie restriction. Your brain simply tells you that you are not hungry, regardless of whether your muscles, organs, and bones are getting what they need.
This is why passive calorie reduction, just eating however much you feel like, is not a safe strategy on semaglutide. You need intentional calorie targets. The medication handles the appetite side of the equation brilliantly. Your job is to make sure the calories you do eat are sufficient, strategic, and protective of your lean mass. If you have noticed fatigue on semaglutide, hair thinning, or feeling cold all the time, inadequate calorie intake is likely the reason.
Why eating too little is just as dangerous as eating too much
Most people start semaglutide with one goal. Lose weight. And the medication delivers on that promise aggressively. But weight loss without nutritional guardrails creates a cascade of problems that can take months or even years to reverse.
Muscle loss tops the list.
A 2024 analysis of semaglutide outcomes found that participants lost an average of 15.3 kg total, of which 5.3 kg was lean mass. That ratio, roughly 35-40% of total weight lost coming from muscle, significantly exceeds what happens with diet and exercise alone, where lean mass typically accounts for only 15-20% of weight lost. The difference comes down to calorie and protein adequacy. When you eat enough protein within a sufficient calorie framework, your body preferentially burns fat. When calories drop too low, your body turns to muscle as fuel because it is metabolically expensive tissue that the body will sacrifice to conserve energy during perceived starvation.
The consequences extend beyond aesthetics. Losing muscle means your metabolism slows. Every pound of muscle burns roughly 6-7 calories per day at rest, compared to about 2 calories per pound of fat. Lose 10 pounds of muscle and your resting metabolic rate drops by 60-70 calories daily. Over a year, that metabolic slowdown adds up to roughly 7 pounds of weight regain, even if you eat the same amount. This is exactly why so many people experience weight loss stalls on semaglutide and eventual weight regain after stopping.
Hair loss is another red flag. Telogen effluvium, the medical term for stress-related hair shedding, typically appears 2-3 months after the body enters a prolonged caloric deficit. The mechanism is straightforward. Hair follicles are metabolically active but not essential for survival. When your body senses inadequate nutrition, it diverts resources away from hair growth toward critical organs. Many semaglutide users blame the medication for their hair loss, but the real culprit is almost always insufficient calorie and protein intake.
Then there is the hormonal disruption. Chronic undereating on semaglutide can affect menstrual cycles, estrogen levels, thyroid function, and cortisol production. Your body interprets severe calorie restriction as a threat. It downregulates reproductive hormones, slows thyroid output, and ramps up stress hormones. All of this happens silently. You might notice sleep problems, dizziness, or worsening fatigue long before bloodwork reveals the damage.
The minimum calorie thresholds exist for a reason. Most nutrition experts and clinical guidelines set the floor at 1,200 calories daily for women and 1,500 calories daily for men. Dropping below these numbers without direct medical supervision puts you at risk for nutrient deficiencies, immune suppression, bone density loss, and metabolic adaptation that makes future weight loss harder. The American Diabetes Association explicitly warns that very low-calorie diets, defined as fewer than 800 calories daily, should only be undertaken under strict medical oversight with supplementation and monitoring.
Calculating your personal calorie target
Generic calorie recommendations are a starting point. But your body is not generic. The number of calories you should eat on semaglutide depends on your current weight, height, age, sex, activity level, and how much lean mass you want to preserve. Calculating your personal target involves three steps.
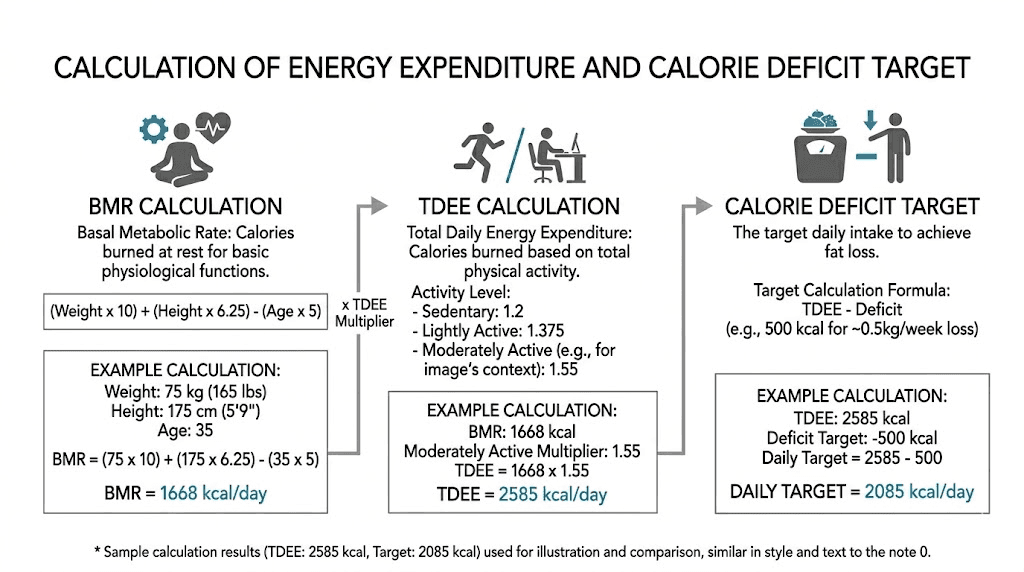
Step 1: find your basal metabolic rate
Your basal metabolic rate (BMR) represents the number of calories your body burns at complete rest, just to keep your organs functioning, your heart beating, and your cells alive. This is your absolute floor for calorie intake, though in practice you should eat above it.
The Mifflin-St Jeor equation is the most widely validated formula for estimating BMR. Use the semaglutide dosage calculator on SeekPeptides for dosing specifics, but for calories, here is how to calculate your BMR:
For women: BMR = (10 x weight in kg) + (6.25 x height in cm) - (5 x age) - 161
For men: BMR = (10 x weight in kg) + (6.25 x height in cm) - (5 x age) + 5
As a quick example, a 40-year-old woman who weighs 85 kg (187 lbs) and stands 165 cm (5 foot 5) tall would calculate: (10 x 85) + (6.25 x 165) - (5 x 40) - 161 = 850 + 1,031 - 200 - 161 = 1,520 calories. That is what her body needs just to exist. Before walking, working, exercising, or even digesting food.
Step 2: calculate your total daily energy expenditure
Your total daily energy expenditure (TDEE) takes your BMR and multiplies it by an activity factor that accounts for how much you move throughout the day. This gives you the total number of calories you burn in a typical 24-hour period.
Activity multipliers:
Sedentary (desk job, little exercise): BMR x 1.2
Lightly active (light exercise 1-3 days per week): BMR x 1.375
Moderately active (moderate exercise 3-5 days per week): BMR x 1.55
Very active (hard exercise 6-7 days per week): BMR x 1.725
Using our example, the 40-year-old woman with a BMR of 1,520 who exercises moderately would have a TDEE of 1,520 x 1.55 = 2,356 calories per day. That number represents what she burns. Not what she should eat. The eating number comes next.
Step 3: apply the right calorie deficit
For steady, sustainable weight loss that preserves muscle, research supports a moderate deficit of 500 to 750 calories below your TDEE. This produces weight loss of approximately 1 to 2 pounds per week, which is the range associated with the best ratio of fat loss to muscle preservation.
Our example woman would target: 2,356 - 500 = 1,856 calories for conservative loss, or 2,356 - 750 = 1,606 calories for more aggressive loss.
Both numbers stay well above the 1,200-calorie minimum floor. Both provide enough energy for her body to function properly while still losing weight. And here is the crucial detail: semaglutide is already doing much of the heavy lifting by naturally reducing her appetite by roughly 24%. She does not need to stack a severe calorie cut on top of the medication-driven appetite reduction. A moderate, intentional deficit combined with semaglutide produces better long-term results than an extreme deficit that sacrifices muscle.
If your calculated target falls below 1,200 (women) or 1,500 (men), use those minimums as your floor. Do not go lower without medical supervision. If you are working with compounded semaglutide and experiencing strong appetite suppression, you may need to eat deliberately above your hunger signals to meet these minimums. Check your semaglutide dose chart and consider whether your dose needs adjustment if appetite suppression makes eating nearly impossible.
Calorie recommendations by body weight
Not everyone wants to calculate formulas. Here is a quick reference table based on common starting weights, assuming moderate activity and a 500-calorie deficit. These numbers provide a safe, effective starting point for most semaglutide users.
Starting weight | Estimated TDEE | Target calories (500 deficit) | Minimum floor |
|---|---|---|---|
150 lbs (68 kg) female | 1,850 | 1,350 | 1,200 |
180 lbs (82 kg) female | 2,100 | 1,600 | 1,200 |
200 lbs (91 kg) female | 2,250 | 1,750 | 1,200 |
220 lbs (100 kg) female | 2,400 | 1,900 | 1,200 |
180 lbs (82 kg) male | 2,300 | 1,800 | 1,500 |
200 lbs (91 kg) male | 2,500 | 2,000 | 1,500 |
230 lbs (104 kg) male | 2,700 | 2,200 | 1,500 |
260 lbs (118 kg) male | 2,900 | 2,400 | 1,500 |
These numbers assume a moderately active lifestyle. If you are sedentary, subtract 200-300 calories from the TDEE estimate. If you are very active or doing resistance training (which you absolutely should be on semaglutide), add 100-200 calories. The key principle is simple. Never eat below the minimum floor regardless of how little appetite you have.
Notice how the lighter starting weights leave less room for calorie restriction. A 150-pound woman on semaglutide has a calculated target of only 1,350 calories, barely above the 1,200 minimum. For people in this situation, the calorie deficit needs to be smaller, around 300-400 calories, with a greater emphasis on exercise to create the remaining deficit through activity rather than food restriction. If you are trying to lose weight on semaglutide without exercise, understand that your calorie target must be handled even more carefully to avoid muscle loss.
People starting at higher weights have more room to work with. A 260-pound man can maintain a 500-calorie deficit while still eating 2,400 calories, enough to support substantial protein intake, diverse nutrition, and adequate energy for daily life. This is one reason semaglutide tends to produce the most dramatic early results in people with higher starting weights. They can sustain a meaningful deficit without approaching dangerous calorie minimums.
The protein equation that protects your muscle
Calories matter. But within those calories, protein is the single most important macronutrient for semaglutide users. Without adequate protein, even a perfectly calculated calorie target will not prevent muscle loss.
Here is the science.
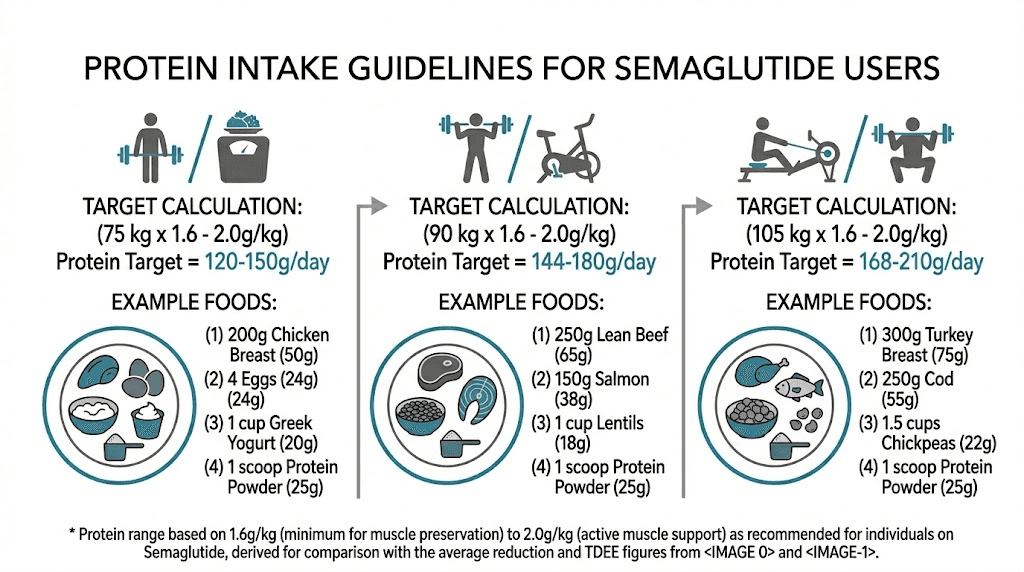
A study presented at the Endocrine Society annual meeting examined 130 participants on semaglutide, comparing outcomes between a high-protein group (1.6 grams per kilogram of body weight daily, roughly 30% of total calories) and a standard-protein group (0.8 g/kg, roughly 15% of total calories). The high-protein group lost more total weight and lost significantly less lean mass. The difference was not subtle. Being older, female, or eating less protein were all independently linked to greater muscle loss in the semaglutide group.
The research is clear on targets.
For semaglutide users actively losing weight, aim for 1.2 to 1.6 grams of protein per kilogram of body weight daily. This translates to approximately 20-30% of your total calories coming from protein. Here is what that looks like at different body weights:
Body weight | Minimum protein (1.2 g/kg) | Optimal protein (1.6 g/kg) |
|---|---|---|
150 lbs (68 kg) | 82 g/day | 109 g/day |
180 lbs (82 kg) | 98 g/day | 131 g/day |
200 lbs (91 kg) | 109 g/day | 146 g/day |
230 lbs (104 kg) | 125 g/day | 166 g/day |
260 lbs (118 kg) | 142 g/day | 189 g/day |
For someone eating 1,600 calories daily, hitting 130 grams of protein means 520 of those calories (130 x 4 calories per gram) come from protein. That is about 33% of total intake. This is why protein must be the foundation of every meal and snack on semaglutide. You simply do not have caloric room for empty carbohydrates or low-nutrient foods when protein requirements are this high relative to total intake.
The best protein sources for semaglutide users are ones that pack maximum protein into minimum calories. Chicken breast delivers 31 grams of protein per 165 calories. Greek yogurt provides 15-20 grams per 100-150 calories. Egg whites give 11 grams per 52 calories. Protein shakes designed for GLP-1 users can deliver 25-40 grams per serving and are particularly useful when appetite suppression makes solid food unappealing. Cottage cheese, lean fish, turkey breast, and tofu all fall into the high-protein, moderate-calorie category that semaglutide users should prioritize.
If you are experiencing strong appetite suppression from your current semaglutide dose, consider frontloading protein at your first meal of the day. Research shows that semaglutide appetite suppression tends to intensify as the day progresses. Eating a protein-rich breakfast or early lunch gives you the best chance of hitting your targets before the medication makes eating feel impossible. High-protein breakfast ideas for GLP-1 users and GLP-1 recipes for weight loss can help you plan meals that maximize protein within your calorie budget.
Combining semaglutide with creatine supplementation also shows promise for muscle preservation. Creatine supports muscle protein synthesis and helps maintain strength during caloric restriction. It is one of the few supplements with strong evidence for GLP-1 users.
Your complete macronutrient breakdown
Protein is the priority. But the remaining calories need to come from somewhere, and how you divide them between carbohydrates and fats affects your energy levels, digestive comfort, and overall health on semaglutide.
Here is the evidence-based breakdown for semaglutide users:
Protein: 25-30% of total calories
This is non-negotiable. At 1,600 calories, this means 100-120 grams of protein daily. At 2,000 calories, aim for 125-150 grams. The higher end of this range is better for anyone doing resistance training, anyone over 50, or anyone who has already lost significant weight.
Carbohydrates: 40-45% of total calories
Despite what low-carb advocates claim, carbohydrates are not the enemy on semaglutide. They fuel your workouts, support brain function, and provide fiber that helps manage the constipation that commonly accompanies semaglutide. The key is choosing complex carbohydrates: vegetables, whole grains, legumes, and fruits. These digest slowly, provide sustained energy, and contain micronutrients your body needs. Aim for 25-38 grams of fiber daily from whole food sources, or supplement with a high-quality fiber supplement if you are not reaching that target through food alone.
Fat: 25-30% of total calories
Healthy fats support hormone production, nutrient absorption, and satiety. At 1,600 calories, this means roughly 44-53 grams of fat daily. Focus on sources like avocado, olive oil, nuts, seeds, and fatty fish. These provide omega-3 fatty acids and fat-soluble vitamins that support overall health during weight loss. Avoid excessive saturated fat and fried foods, which can worsen the bloating and acid reflux that some semaglutide users experience.
Here is what the breakdown looks like at common calorie levels:
Daily calories | Protein (g) | Carbs (g) | Fat (g) |
|---|---|---|---|
1,200 | 90-100 | 120-135 | 33-40 |
1,400 | 105-115 | 140-158 | 39-47 |
1,600 | 120-130 | 160-180 | 44-53 |
1,800 | 135-150 | 180-203 | 50-60 |
2,000 | 150-165 | 200-225 | 56-67 |
2,200 | 165-180 | 220-248 | 61-73 |
Notice that even at 1,200 calories, the protein target stays high at 90-100 grams. This is deliberate. When total calories are low, protein must represent a larger percentage of intake to protect lean mass. This is exactly why eating the right foods on semaglutide matters so much more than it does for someone eating 2,500 or 3,000 calories daily. Every calorie has to earn its place.
Semaglutide formulations with B12 can help address the vitamin deficiencies that become more likely at lower calorie intakes. B12 supports energy production and nerve function, both of which suffer when nutrition is inadequate. Some compounded versions also include glycine or L-carnitine, which may support fat metabolism and muscle preservation during weight loss.
Calorie targets by semaglutide dose phase
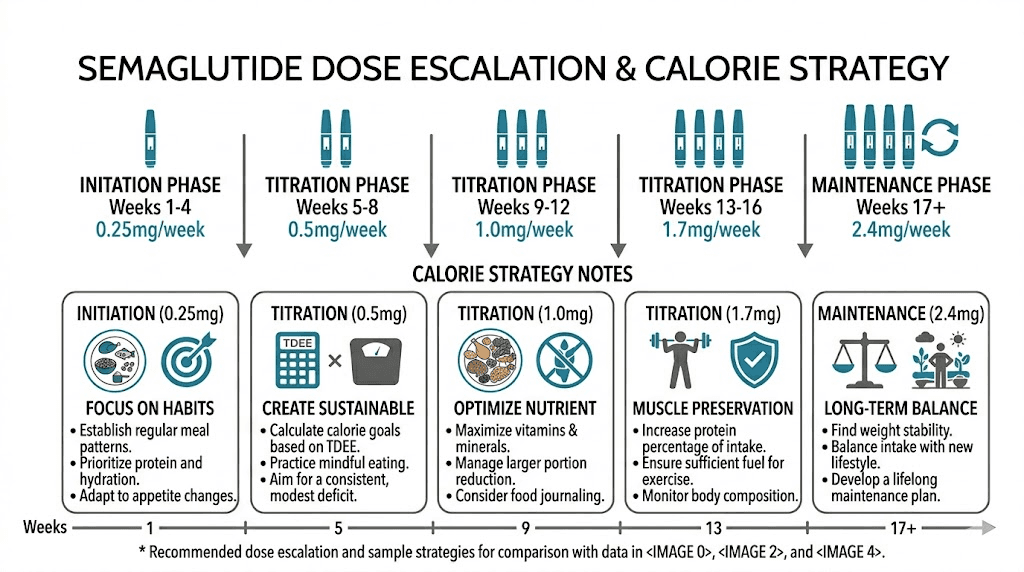
Your calorie needs are not static on semaglutide. They change as the medication dose increases, as your body weight decreases, and as your appetite suppression intensifies. Here is how to adjust your calorie strategy across the typical dose escalation timeline.
Starting dose phase (0.25 mg, weeks 1-4)
Appetite suppression at 0.25 mg is mild for most people. Many users report barely noticing a difference during their first week on semaglutide. This is your window to establish good eating habits before the medication ramps up.
Calorie strategy: Eat at your full calculated target (TDEE minus 500). Do not restrict further. Use this time to practice hitting your protein targets, eating nutrient-dense foods, and establishing a meal schedule that works for your lifestyle. The medication is doing very little appetite work at this stage, so your calorie counting skills will matter more now than at any other point.
Escalation phase (0.5 mg to 1.0 mg, weeks 5-16)
This is where the appetite suppression becomes real. Most users report significant hunger reduction at 0.5 mg, with further suppression at 1.0 mg. Some people find eating to be genuinely difficult. The food aversion that accompanies this phase can make previously enjoyable meals seem repulsive.
Calorie strategy: Your target stays the same, but you may need to eat more deliberately. If you are struggling to hit your calorie floor, try liquid calories like protein shakes, smoothies, or soups that go down easier than solid food. Eat at scheduled times even if you are not hungry. Smaller, more frequent meals (4-5 per day) often work better than trying to hit calories in 2-3 large meals. Pay close attention to when side effects peak and schedule your biggest meal during your window of least appetite suppression, which for most people is morning or early afternoon.
Therapeutic dose phase (1.7 mg to 2.4 mg, weeks 17+)
At full therapeutic doses, appetite suppression is at maximum. This is also when results accelerate and the risk of undereating becomes highest. Many people at this dose report eating fewer than 1,000 calories daily without realizing it.
Calorie strategy: Active calorie monitoring becomes essential. Track everything. If your intake consistently falls below 1,200 (women) or 1,500 (men) despite your best efforts, talk to your provider about whether the dose is appropriate. Some people do better at a slightly lower dose that allows adequate nutrition while still providing meaningful weight loss. The goal is not maximum appetite suppression. The goal is maximum fat loss with minimum muscle loss, and that requires eating enough to fuel the process.
If you are on a 5mg/ml concentration of compounded semaglutide, fine-tuning your dose in small increments is easier and can help you find the sweet spot between appetite control and nutritional adequacy. The injection technique and timing of your dose can also influence how manageable your appetite suppression feels throughout the week.
Maintenance phase
Once you reach your goal weight, calorie strategy shifts from deficit to maintenance. Your new TDEE will be lower than when you started because you weigh less, and potentially because you have lost some metabolic rate along the way. Recalculate using your current weight and activity level. Most people in maintenance need to eat at or slightly above their new TDEE to prevent further weight loss while deciding how long to continue semaglutide. Understanding the GLP-1 maintenance dose concept is important for this transition.
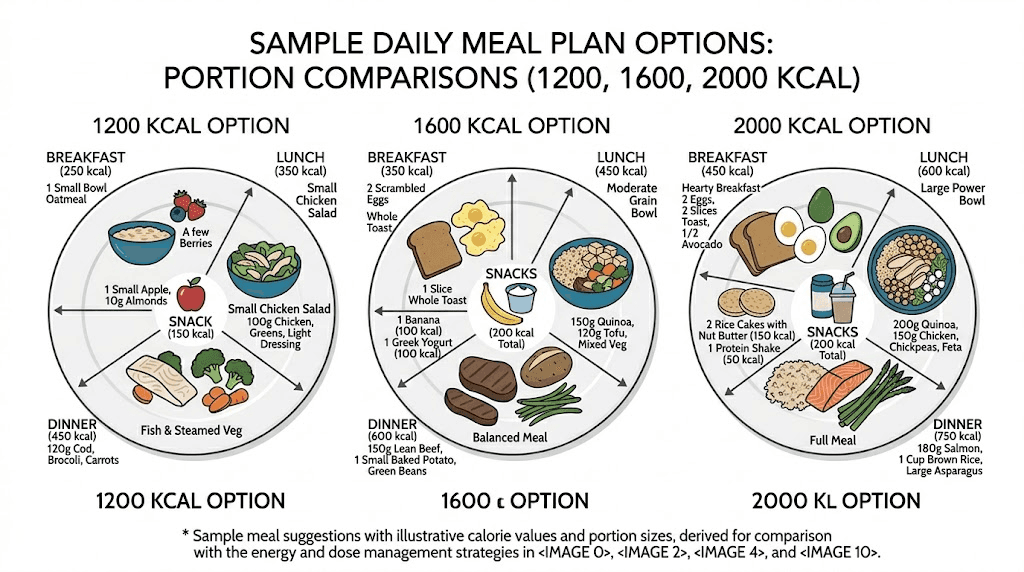
Sample daily meal plans at different calorie levels
Theory is helpful. But seeing exactly what a day of eating looks like at different calorie targets makes the whole thing practical. Here are sample meal plans optimized for semaglutide users, with protein prioritized at every meal.
1,200-calorie plan (minimum for women)
Breakfast (350 calories, 35g protein): 3 egg whites scrambled with 1 whole egg, 1/2 cup black beans, 1/4 avocado, salsa. This front-loads protein when appetite is typically strongest in the morning.
Lunch (400 calories, 40g protein): 5 oz grilled chicken breast over mixed greens with cherry tomatoes, cucumber, 1 tablespoon olive oil dressing, and 1/2 cup quinoa.
Snack (150 calories, 25g protein): 1 cup plain Greek yogurt with a small handful of berries. Greek yogurt is one of the most efficient protein-per-calorie foods available.
Dinner (300 calories, 30g protein): 5 oz baked cod with roasted broccoli and cauliflower, seasoned with lemon and garlic. White fish is extremely low in calories while delivering substantial protein.
Daily totals: 1,200 calories, 130g protein (43%), 95g carbs (32%), 33g fat (25%)
At 1,200 calories, every meal does double duty. There is zero room for calorie-dense, low-nutrient foods. If you find this restrictive, it is because 1,200 calories is restrictive, and it is the absolute minimum. If your TDEE calculation allows for more, eat more. For a complete food list for semaglutide users, focus on the foods that pack the most nutrition into the fewest calories.
1,600-calorie plan (common target for women)
Breakfast (400 calories, 35g protein): Protein smoothie with 1 scoop whey protein, 1 cup unsweetened almond milk, 1 banana, 1 tablespoon peanut butter, handful of spinach.
Lunch (450 calories, 40g protein): Turkey and vegetable stir-fry with 6 oz ground turkey, mixed bell peppers, zucchini, snap peas, soy sauce, over 3/4 cup brown rice.
Snack (200 calories, 20g protein): 1/2 cup cottage cheese with sliced peaches and a sprinkle of cinnamon.
Dinner (400 calories, 35g protein): 5 oz salmon fillet with roasted sweet potato (1/2 medium) and steamed asparagus with lemon.
Evening snack (150 calories, 15g protein): Protein bar or 2 hard-boiled eggs with salt and pepper.
Daily totals: 1,600 calories, 145g protein (36%), 155g carbs (39%), 44g fat (25%)
This plan gives more flexibility. The addition of an evening snack means you do not need to cram all your nutrition into three meals. The protein stays high throughout the day, ensuring your muscles receive a steady supply of amino acids. If certain foods trigger GI discomfort, the foods to avoid on semaglutide guide can help you identify and eliminate problem items.
2,000-calorie plan (common target for men)
Breakfast (500 calories, 40g protein): 3-egg omelet with turkey sausage, bell peppers, onions, and 1/4 cup shredded cheese. 1 slice whole grain toast with 1/2 tablespoon butter.
Lunch (550 calories, 45g protein): Large chicken and black bean bowl with 6 oz chicken breast, 1/2 cup black beans, brown rice, salsa, 1/4 avocado, and mixed greens.
Snack (200 calories, 25g protein): Protein shake with water or almond milk.
Dinner (500 calories, 40g protein): 6 oz lean steak with roasted vegetables (broccoli, brussels sprouts, carrots) and 1 medium baked potato with a tablespoon of plain Greek yogurt.
Evening snack (250 calories, 15g protein): 1/4 cup mixed nuts and 1 string cheese.
Daily totals: 2,000 calories, 165g protein (33%), 190g carbs (38%), 64g fat (29%)
At 2,000 calories, meal variety expands significantly. You can include healthy fats, whole grains, and a wider range of vegetables without sacrificing protein targets. This calorie level also supports an active lifestyle that includes resistance training, which is one of the most effective strategies for preserving muscle during semaglutide weight loss. For more meal planning ideas, the complete semaglutide diet plan and GLP-1 dinner ideas guides provide extensive options.
What happens when you eat too few calories on semaglutide
The warning signs of undereating are predictable. They follow a pattern. And they escalate if you ignore them.
Week 1-2 below minimum: Increased fatigue and reduced energy. You might chalk this up to the medication, but if you were eating adequately before and the only change is reduced calorie intake, food is the likely culprit. Semaglutide fatigue is common, but it should improve as your body adapts, not get worse over time.
Week 2-4: Difficulty concentrating. Mood changes including irritability, anxiety, or feelings of depression. Cold intolerance, particularly in your hands and feet. Your body is beginning to downregulate non-essential processes to conserve energy.
Month 2-3: Hair shedding begins. This is telogen effluvium, and it often takes people by surprise because there is a delay between the caloric insult and the visible hair loss. By the time you notice hair on your pillow or in the shower drain, the damage was done weeks ago. GLP-1 hair loss is almost always nutritional in origin and resolves when adequate calories and protein are restored, but regrowth takes 3-9 months.
Month 3-6: Metabolic adaptation sets in. Your body has learned to function on fewer calories by slowing your resting metabolic rate. This is the plateau that causes so much frustration. People think the medication stopped working. In reality, their body adapted to chronic undereating by becoming more efficient, burning fewer calories at rest, and holding onto fat stores more aggressively. Breaking through a semaglutide plateau often requires eating more, not less, to convince your body it is safe to release stored energy.
Beyond 6 months of chronic undereating: Menstrual irregularities or loss. Brittle nails and dry skin. Sleep disruption. Weakened immune function. Slow wound healing. Bone density concerns. These are serious complications that require medical attention and nutritional rehabilitation.
If you are losing more than 2 pounds per week consistently, that is a signal you may be in too severe a deficit. Sustainable fat loss happens at 1-2 pounds per week. Anything faster than that almost certainly includes muscle loss. Checking your progress with body composition tools rather than just a scale can help you distinguish between fat loss and muscle loss.
How to track calories when your appetite disappears
Tracking calories on semaglutide presents a unique challenge. When your appetite vanishes, you do not naturally think about food, which means you do not naturally track it either. By the time you realize you have only eaten 800 calories today, it is 8 PM and the thought of food makes you queasy.
Here are practical strategies that work.
Set meal alarms, not hunger cues. Your hunger signals are unreliable on semaglutide. Set phone alarms at your planned meal times and eat regardless of whether you feel hungry. Treat meals like medication. You do not skip your semaglutide dose because you do not feel like taking it. Do not skip meals because you do not feel like eating.
Front-load your calories. Most semaglutide users find that appetite is strongest in the morning and diminishes throughout the day. Eat your largest, most protein-rich meal first. If you can get 40-50% of your daily calories in by lunchtime, the pressure to eat large portions later is reduced.
Use calorie-dense, nutrient-dense foods. When volume is the problem (you simply cannot eat enough food), switch to calorie-dense options. A tablespoon of olive oil adds 120 calories. A quarter cup of nuts adds 200 calories. Avocado, nut butters, cheese, and dried fruit all pack significant calories into small volumes. These are not junk foods. They are nutrient-dense tools for meeting your calorie targets when appetite is suppressed.
Drink your calories strategically. Protein smoothies and shakes are invaluable for semaglutide users who cannot stomach solid food. A smoothie with protein powder, banana, peanut butter, milk, and spinach can deliver 500+ calories and 40+ grams of protein in a form that goes down much easier than a plate of chicken and vegetables. Choosing the right protein shake for GLP-1 protocols can make the difference between meeting your targets and falling short.
Track before you eat, not after. Plan your meals the night before or first thing in the morning. Log them in a tracking app before you eat them. This way you know whether your planned intake meets your targets before the day starts, and you can make adjustments proactively rather than discovering at bedtime that you are 500 calories short.
Use the injection timing to your advantage. Many people find that appetite suppression is strongest in the 2-3 days immediately following their semaglutide injection and loosens slightly before the next dose. If you take your shot on a particular day, plan your heaviest eating days for days 5-7 of your injection cycle when appetite may be slightly more permissive. Understanding the best time to take semaglutide and its relationship to your eating schedule helps you work with the medication rather than against it.
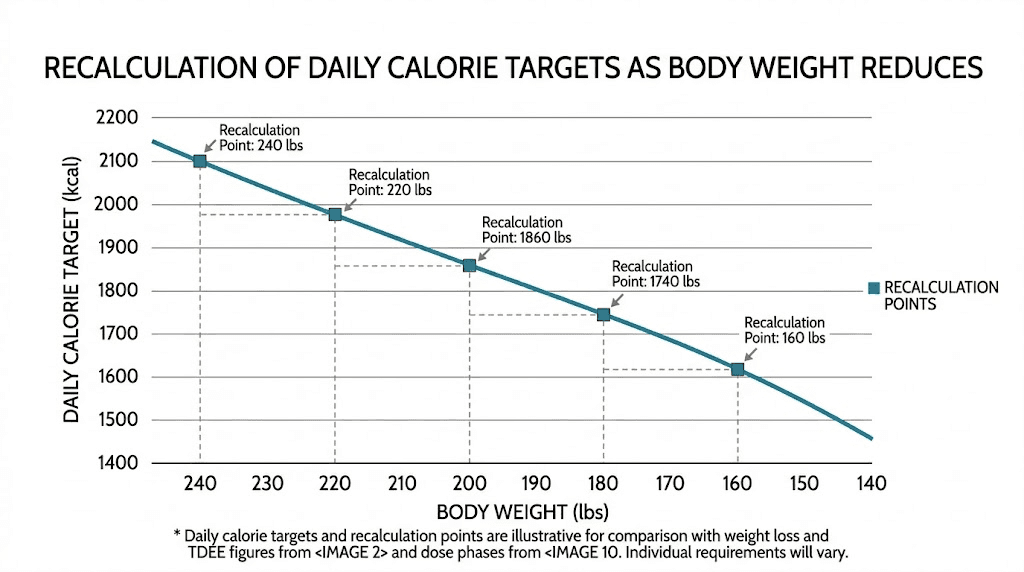
Adjusting your calories as you lose weight
Your calorie target is not a set-it-and-forget-it number. As you lose weight, your body requires fewer calories to function. A person who weighed 230 pounds six months ago and now weighs 195 pounds has a meaningfully different metabolic rate. Continuing to eat the same number of calories that produced weight loss at 230 pounds will eventually stop producing results at 195 pounds.
Recalculate your TDEE every 15-20 pounds of weight loss, or roughly every 2-3 months. Use your new weight in the BMR formula, then apply the same activity multiplier and deficit calculation. The new number will be lower, which means your calorie target drops. But, and this is critical, it should never drop below the minimum floor of 1,200 (women) or 1,500 (men).
If recalculation puts your target below those minimums, you have two options. First, increase your activity level. Adding 30 minutes of walking, resistance training, or any physical activity increases your TDEE and allows a higher calorie target while maintaining the same deficit. Second, accept a slower rate of loss. At lower body weights, a 300-calorie deficit instead of 500 is both safer and more sustainable. The math changes as you get smaller, and forcing an aggressive deficit at a lower weight is a recipe for muscle loss and metabolic adaptation.
If you find yourself stuck with no weight loss after several weeks despite consistent calorie tracking, the issue may be metabolic adaptation from previously eating too little. Counterintuitively, a GLP-1 reset period where you eat at maintenance calories for 1-2 weeks can restart weight loss by signaling to your body that the famine is over and it is safe to release stored fat again.
Common calorie mistakes on semaglutide
After analyzing hundreds of semaglutide nutrition discussions and clinical outcomes, certain patterns emerge. These are the mistakes that undermine results most frequently.
Mistake 1: Celebrating low calorie days. Eating 700 calories and feeling proud about it is the most dangerous mindset on semaglutide. Low calorie days are not victories. They are threats to your lean mass, your metabolism, and your long-term results. Every day below your calorie floor is a day your body breaks down muscle for fuel.
Mistake 2: Ignoring protein while counting calories. A 1,500-calorie day of pasta, bread, and fruit juice looks identical on the scale to a 1,500-calorie day of chicken, vegetables, and Greek yogurt. But the nutritional outcomes are completely different. The first option provides almost no protein, meaning your body will break down muscle to get the amino acids it needs. The second option preserves muscle while burning fat. Building the right diet on semaglutide means tracking protein alongside total calories.
Mistake 3: Not accounting for the medication appetite reduction. Many people calculate their calorie deficit and then add semaglutide appetite suppression on top. The medication is already creating a 24% reduction in energy intake. Stacking a 750-calorie intentional deficit on top of that can push total intake dangerously low. Your calculated deficit should be your total deficit, not your intentional deficit on top of the medication effect.
Mistake 4: Skipping meals entirely. Some semaglutide users go entire days eating one small meal. This is not intermittent fasting. This is undereating. Your muscles need a steady supply of amino acids throughout the day to maintain themselves. Extended periods without protein intake accelerate muscle breakdown. Even if you are not hungry, eating something protein-rich every 4-5 hours protects your lean mass.
Mistake 5: Comparing your calorie intake to other semaglutide users. A 250-pound man and a 140-pound woman have vastly different calorie needs. Online forums are full of people sharing their calorie counts without context, and following someone else calorie plan that was not designed for your body is a recipe for either overeating or undereating. Calculate your own targets using the formulas above.
Mistake 6: Ignoring hydration. Semaglutide slows gastric emptying, which can reduce your thirst cues just like it reduces your hunger cues. Dehydration amplifies constipation, dizziness, headaches, and fatigue. Women should aim for approximately 91 ounces (2.7 liters) of total water daily. Men should target 125 ounces (3.7 liters). These targets come from the National Academies of Sciences and include water from food sources, but most semaglutide users need to actively drink more water than they think.
Mistake 7: Dropping calories too fast. Research supports a step-down approach where you reduce calories by 200-300 per week rather than making dramatic cuts. If you were eating 2,200 calories before semaglutide and want to target 1,600, reduce to 2,000 for a week, then 1,800, then 1,600. This gradual approach reduces side effects, improves adherence, and gives your body time to adapt without triggering aggressive metabolic compensation. If you are just starting semaglutide, the comprehensive tips guide covers this transition in detail.
When to increase your calories
Sometimes the right move is eating more, not less. Here are the clear signals that your calorie intake needs to go up.
Persistent fatigue that does not improve. Early semaglutide fatigue is normal. Fatigue that persists beyond the first 4-6 weeks, or fatigue that gets worse over time, usually means you are not eating enough. Before blaming the medication, try increasing calories by 200-300 per day for two weeks and see if energy improves. Understanding semaglutide energy effects helps you distinguish between medication-related and nutrition-related fatigue.
Hair shedding. If you notice increased hair loss 2-3 months into your semaglutide protocol, increase calories and protein immediately. The hair loss reflects nutritional inadequacy that happened weeks ago. Correcting it now will stop further shedding and allow regrowth over the next 3-9 months.
Weight loss exceeding 2 pounds per week consistently. Occasional weeks with higher loss are normal, especially early on or after dose increases. But sustained loss of more than 2 pounds weekly over a month or more indicates an excessive deficit that is almost certainly including muscle tissue. Increasing calories by 200-300 per day should slow loss to the 1-2 pound weekly range that optimizes the fat-to-muscle loss ratio.
Strength decline in the gym. If you are doing resistance training (and you should be), pay attention to your strength numbers. A modest decline is expected during calorie restriction. A significant or rapid decline in strength means your muscles are not getting enough fuel. Increase calories, particularly around workouts, and make sure pre and post-workout nutrition includes adequate protein and carbohydrates.
Menstrual irregularity. For women, changes to your cycle on semaglutide can indicate insufficient calorie intake affecting hormone production. This is your body telling you that it does not have enough energy to support reproductive function. It is a serious warning sign. Increase calories and consult your healthcare provider. Learn more about how semaglutide affects your period and when changes warrant medical attention.
Cold intolerance. Feeling unusually cold, especially in your extremities, is a classic sign of metabolic downregulation from insufficient calories. Your body reduces heat production to conserve energy. If you notice feeling cold on semaglutide, inadequate calorie intake is the most common explanation. Increasing food intake by 200-300 calories daily often resolves this within a week.
Special considerations for different populations
Not all semaglutide users have the same calorie needs. Several populations require specific adjustments to the general guidelines above.
Adults over 50
Muscle preservation becomes even more critical with age. After 50, the body naturally loses muscle mass at a rate of 1-2% per year (sarcopenia), and adding semaglutide-driven calorie restriction on top of age-related muscle loss can be devastating. Older adults should aim for the higher end of the protein range (1.4-1.6 g/kg) and should never target calories below 1,400 (women) or 1,600 (men) without medical oversight. Resistance training is not optional for this group. It is essential.
People doing resistance training
If you are strength training 3-5 times per week (which you should be on semaglutide), your calorie needs are higher than the sedentary calculations suggest. Use the "moderately active" or "very active" multiplier when calculating your TDEE, and add 100-200 calories on training days, primarily from carbohydrates and protein. Your pre-workout meal should include 20-30 grams of protein and 30-50 grams of complex carbohydrates, consumed 60-90 minutes before training. Your post-workout meal should include 25-40 grams of protein within 2 hours of finishing. The creatine and GLP-1 guide covers supplementation strategies that support muscle retention during training and calorie restriction.
People switching from tirzepatide
If you are switching from tirzepatide to semaglutide, be aware that the appetite suppression profiles differ between the two medications. Tirzepatide activates both GLP-1 and GIP receptors, producing somewhat different hunger patterns. Your calorie needs may shift during the transition. Monitor your intake carefully for the first 4-6 weeks after switching and recalculate as needed.
People taking semaglutide with other compounds
Compounded formulations that include B12, glycine, L-carnitine, or niacinamide do not change your calorie requirements, but they may influence how you feel on restricted calories. B12 and L-carnitine support energy production. Glycine supports sleep and recovery. These compounds do not replace adequate calorie intake, but they can make restricted eating more tolerable.
If you are combining semaglutide with phentermine, berberine, or metformin, these additional medications can further affect appetite and blood sugar, making calorie monitoring even more important. The stacking of appetite-suppressing compounds increases the risk of inadvertent undereating.
The role of exercise in your calorie equation
Exercise changes the math. And it changes it in your favor.
A person who eats 1,600 calories and does no exercise has a smaller calorie deficit than a person who eats 1,800 calories and burns 400 through exercise. But the second person is eating more food, getting more protein, getting more micronutrients, and preserving more muscle. The exercise creates calorie expenditure that allows higher food intake while maintaining the same net deficit. This is why every clinical guideline for semaglutide recommends combining the medication with physical activity.
Resistance training deserves special emphasis. While cardio burns calories during the activity, resistance training builds and maintains the muscle tissue that keeps your metabolism elevated 24 hours a day. A person who loses 50 pounds with semaglutide plus resistance training will have a dramatically different body composition, metabolic rate, and long-term outcome than someone who loses 50 pounds with semaglutide alone.
If you are not currently exercising, start simple. Walking 30 minutes daily and doing 2-3 strength training sessions per week is enough to meaningfully shift your calorie equation and protect your muscle mass. The semaglutide without exercise guide explains what you are leaving on the table by skipping physical activity, and the difference in outcomes is substantial.
On training days, consider adding 150-300 calories above your usual target, primarily from protein and complex carbohydrates. This fuels the workout, supports recovery, and ensures your muscles have the raw materials they need to maintain themselves. On rest days, return to your standard calorie target. This cycling approach, sometimes called calorie cycling, optimizes both fat loss and muscle preservation across the week.
Hydration and micronutrients: the overlooked pieces
Calories and macronutrients get the attention. But on semaglutide, hydration and micronutrients matter just as much because reduced food intake means reduced nutrient intake across the board.
Water intake targets. The National Academies recommend approximately 91 ounces (2.7 liters) of total water daily for women and 125 ounces (3.7 liters) for men. These numbers include water from food, but semaglutide users who eat less food get less water from dietary sources. Aim to drink at least 64-80 ounces of plain water daily, more if you exercise or live in a warm climate. Adequate hydration reduces GLP-1 constipation, supports kidney function, and helps your body metabolize fat efficiently.
Key micronutrients to monitor. When you eat fewer calories, you get fewer vitamins and minerals by default. The micronutrients most at risk during semaglutide weight loss include:
Iron: Reduced meat intake can lead to deficiency, causing fatigue and weakness
Calcium and Vitamin D: Critical for bone health, especially during rapid weight loss
B vitamins: B12 in particular supports energy and nerve function. Compounded semaglutide with methylcobalamin addresses this directly
Magnesium: Supports muscle function, sleep, and hundreds of enzymatic reactions
Zinc: Important for immune function and hair health
Omega-3 fatty acids: Anti-inflammatory and protective against the metabolic stress of calorie restriction
A high-quality multivitamin, combined with adequate protein and diverse vegetable intake, helps fill the micronutrient gaps that inevitably open during calorie restriction. For a complete supplementation strategy, see the supplements guide for GLP-1 users and the GLP-1 vitamin guide. A quality probiotic also supports the gut health changes that accompany both semaglutide use and dietary shifts.
Frequently asked questions
Is 1,000 calories a day enough on semaglutide?
No. For the vast majority of adults, 1,000 calories daily is too low, even with semaglutide appetite suppression. This level falls below established minimums (1,200 for women, 1,500 for men) and dramatically increases the risk of muscle loss, nutrient deficiency, and metabolic slowdown. If your appetite is so suppressed that you cannot eat above 1,000 calories, discuss a dose reduction with your provider. The semaglutide dosage guide covers how dose adjustments work.
Will eating too few calories on semaglutide cause hair loss?
Yes. Telogen effluvium, the stress-related hair shedding that many semaglutide users experience, is primarily caused by rapid weight loss and inadequate calorie or protein intake. The shedding typically begins 2-3 months after the nutritional deficit starts. Maintaining adequate calories (above the minimum floor) and protein (1.2-1.6 g/kg body weight) is the most effective prevention strategy. Our complete GLP-1 hair loss guide covers this in depth.
Should I eat the same calories every day on semaglutide?
Not necessarily. Calorie cycling, where you eat slightly more on active days and slightly less on rest days, can optimize both performance and fat loss. A common approach is to eat at your full target on training days and reduce by 200-300 calories on sedentary days. The weekly average matters more than any single day, so if you have a lower-calorie day due to strong appetite suppression, compensate with slightly higher intake the following day.
Do I need to count calories on semaglutide or can I just eat intuitively?
Intuitive eating is unreliable on semaglutide because the medication fundamentally alters your hunger and satiety signals. Most people who eat intuitively on semaglutide undereat significantly. Tracking calories, at least for the first 3-4 months, ensures you are meeting your minimums. After that, many people develop enough awareness of portion sizes and protein content to track less formally. But periodic check-ins with actual calorie counting help prevent gradual drift toward inadequate intake.
How do I know if I am eating enough protein on semaglutide?
Track your protein intake for a typical week. If you consistently hit 1.2-1.6 grams per kilogram of body weight daily, you are in the protective range. Signs that protein is too low include progressive weakness, slower recovery from exercise, increased hunger between meals, and visible muscle loss. Using a peptide calculator for dosing and a food tracking app for nutrition helps keep both sides of the equation accurate.
Can I do a very low calorie diet on semaglutide for faster results?
Very low calorie diets (below 800 calories daily) should only be done under direct medical supervision with appropriate supplementation and monitoring. Combining semaglutide with a VLCD dramatically increases the risk of serious muscle loss, nutritional deficiency, and metabolic damage. The research consistently shows that moderate calorie restriction (500-750 below TDEE) produces better long-term outcomes than extreme restriction, because it preserves the metabolic rate and lean mass that determine whether you keep the weight off.
My semaglutide appetite suppression varies week to week. How should I handle calories?
This is normal. Appetite suppression is typically strongest 1-3 days after injection and weakens before the next dose. Focus on your weekly calorie average rather than stressing about daily variation. On days with strong suppression, prioritize protein-rich foods and calorie-dense options that are easier to consume. On days with more appetite, eat fuller meals that include vegetables, whole grains, and variety. The weekly pattern of how semaglutide makes you feel becomes predictable over time, and you can plan your meal prep accordingly.
Should I change my calorie intake if I experience GI side effects?
GI side effects like bloating, constipation, sulfur burps, and nausea do not change your calorie target, but they may change how you eat. Smaller, more frequent meals reduce GI distress. Avoiding high-fat and fried foods helps. Staying upright after eating and eating slowly also reduces symptoms. The calorie goal stays the same, but the delivery method adapts to what your GI system tolerates.
For researchers serious about optimizing their semaglutide results through proper nutrition, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized protocol tools, and a community of thousands who have navigated these exact nutritional challenges.
External resources
Once-Weekly Semaglutide for Weight Management: A Clinical Review (PMC)
STEP 1 Trial: Once-Weekly Semaglutide in Adults with Overweight or Obesity (NEJM)
Effect of Semaglutide 2.4mg on Energy Intake, Appetite, and Gastric Emptying (PMC)
Higher Protein Intake May Protect Against Muscle Loss on Anti-Obesity Drugs (Endocrine Society)
In case I do not see you, good afternoon, good evening, and good night. May your calories stay sufficient, your protein stay high, and your muscle stay right where it belongs.