Feb 24, 2026

Three approved sites. One weekly injection. And a decision most people overthink for twenty minutes before they finally commit and push the needle in. Choosing where to inject tirzepatide sounds simple until you are standing there, syringe in hand, wondering if the abdomen really is better than the thigh, whether the upper arm actually works for solo injections, and if that spot you used last Tuesday has healed enough for another round.
The reality is more nuanced than most guides admit. Each tirzepatide injection site comes with its own absorption characteristics, comfort levels, and practical considerations that change depending on your body composition, your tolerance for mild discomfort, and whether you have someone nearby to help. The stomach injection is the most popular choice for a reason, but it is not the only option and it is not always the best one for every person.
This guide breaks down every approved injection site for tirzepatide, explains exactly how to use each one, covers rotation strategies that prevent complications, and addresses the real questions people have after their first few weeks on this GLP-1/GIP receptor agonist. Whether you are brand new to tirzepatide or months into your protocol and looking for ways to improve your injection experience, the information here comes from clinical guidelines, published research, and the practical knowledge that SeekPeptides members rely on daily.
The three FDA-approved tirzepatide injection sites
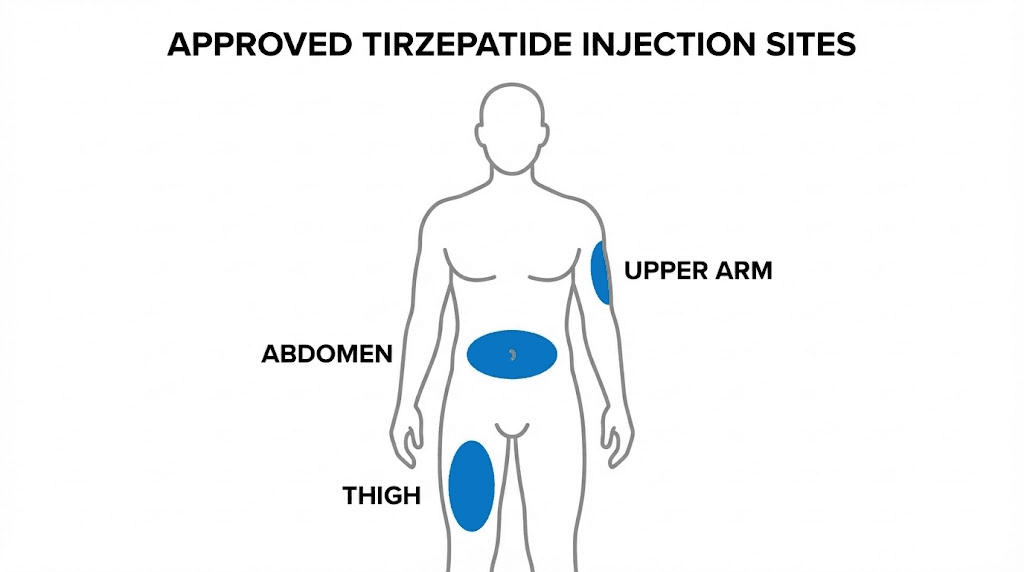
Tirzepatide, sold under the brand names Mounjaro and Zepbound, is administered as a subcutaneous injection. That means the medication goes into the fatty tissue just beneath the skin, not into muscle. The FDA prescribing information identifies three approved injection locations.
The abdomen.
The front of the thigh.
The back of the upper arm.
These are not suggestions or recommendations. They are the specific anatomical areas studied in clinical trials and confirmed to deliver consistent, reliable absorption. Injecting anywhere else, like the buttocks, the calf, or the lower back, falls outside the studied parameters and could affect how the medication enters your bloodstream.
A Phase 1 pharmacokinetic study conducted by Eli Lilly (NCT04050670) specifically examined tirzepatide absorption across all three sites in participants with varying body sizes. The study measured area under the concentration curve (AUC) and maximum concentration (Cmax) at each location. The conclusion was clear. There were no clinically meaningful differences in tirzepatide exposure between the abdomen, thigh, or upper arm. The medication works the same regardless of which approved site you choose.
That said, "works the same" does not mean "feels the same" or "is equally convenient." Each site has distinct practical advantages and drawbacks that matter in everyday use.
Abdomen injection site: the most popular choice
Most people who use tirzepatide inject in the abdomen. There are good reasons for this. The stomach area offers the largest surface area of any approved injection site, which means more room for rotation and less chance of hitting the same spot twice. The subcutaneous fat layer tends to be thickest here, making it easier to get a clean injection into fatty tissue without accidentally going too deep into muscle.
Exact location for abdominal injections
The injection zone for the abdomen is the area below the ribs and above the hip bones, excluding a two-inch radius around the navel. Think of it as a wide belt across your midsection, but with a circle cut out around the belly button.
Stay at least two inches away from the navel in any direction. The tissue immediately surrounding the belly button is thinner and contains more blood vessels, which increases the risk of bruising and discomfort. You can inject on either side of the abdomen, and most people find the area two to four inches to the left or right of the navel at or below navel height is the sweet spot for comfort.
Why the abdomen works so well
Several factors make the abdomen the preferred site for tirzepatide injections. The subcutaneous fat layer here is typically generous, even in leaner individuals. You can see exactly what you are doing without mirrors or contortion. Both hands are free, which gives you full control over the pinch-and-inject technique. And the large surface area means you can divide the entire zone into a grid of eight to twelve distinct spots for systematic rotation.
Absorption from the abdomen tends to be consistent and predictable. While the pharmacokinetic study confirmed equivalent bioavailability across all sites, research on similar subcutaneous medications shows that abdominal fat provides excellent blood flow to the injection area, which supports reliable uptake of the medication into the bloodstream.
Tips for comfortable abdominal injections
Comfort varies from person to person, but several techniques consistently help. Let the medication reach room temperature before injecting, especially if you are using refrigerated compounded tirzepatide. Cold medication stings more going in. Pull the syringe out of the fridge 15 to 30 minutes beforehand.
Pinch a fold of skin between your thumb and forefinger. This lifts the fatty tissue away from the underlying muscle and creates a clear target zone. Insert the needle at a 90-degree angle if using a standard length needle (typically 29-31 gauge, half-inch to five-eighths inch). If you are very lean and using a longer needle, a 45-degree angle may be more appropriate to avoid reaching muscle tissue.
Inject slowly. Pushing the plunger too fast can cause a burning sensation. Take five to ten seconds to deliver the full dose. After injecting, hold the needle in place for about ten seconds before withdrawing, then release the skin pinch. Apply gentle pressure with a cotton ball or gauze for 30 seconds. Do not rub the site, as rubbing can increase bruising and spread the medication in unintended ways.
Front of thigh injection site: a solid alternative
The front of the thigh is the second most commonly used injection site for tirzepatide. It offers its own set of advantages, particularly for people who experience sensitivity or reactions in the abdominal area.
Exact location for thigh injections
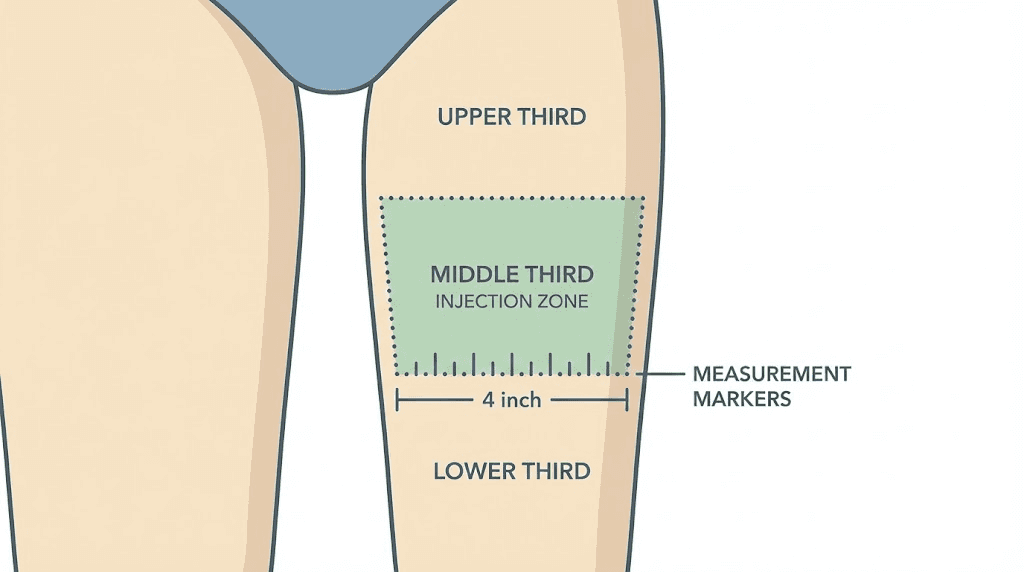
The approved injection area covers the front and outer portion of the thigh, roughly in the middle third between the knee and the hip. Imagine your thigh divided into three equal horizontal sections. The injection zone is the middle section. Stay away from the inner thigh, which has more nerve endings and blood vessels closer to the surface. Avoid the area within two inches of the knee and two inches of the groin.
The outer thigh, specifically the vastus lateralis muscle area overlaid with subcutaneous fat, provides a comfortable injection target for most people. You can inject while sitting down, which some people find more relaxing than standing.
Advantages of thigh injections
The thigh offers several distinct benefits. Access is easy. You do not need to lift your shirt or adjust clothing as much. Both thighs give you significant surface area for rotation when combined, essentially doubling your available injection real estate compared to a single site. The subcutaneous tissue on the front of the thigh is generally thick enough for reliable injection depth even in people with less body fat overall.
Some people report less sensitivity in the thigh compared to the abdomen. Pain perception is individual, but the front of the thigh has somewhat fewer nerve endings per square centimeter than the periumbilical area of the abdomen. If your stomach injections consistently cause discomfort or injection site reactions, switching to the thigh for a few weeks can give your abdominal tissue time to recover while maintaining your dosing schedule.
Tips for comfortable thigh injections
Sit down with your leg relaxed and slightly bent. Tension in the quadriceps muscle makes the tissue firmer and the injection more uncomfortable. Let your leg go completely limp before pinching the skin and inserting the needle.
The same general technique applies. Room temperature medication. Gentle skin pinch. 90-degree angle for standard needles. Slow, steady injection. Hold for ten seconds. Gentle pressure, no rubbing. However, one thigh-specific tip matters. If you are injecting into the outer thigh while sitting, the skin may be stretched tighter than when standing. Some people find it more comfortable to stand with their weight on the opposite leg, allowing the injection-side thigh to relax completely.
Upper arm injection site: when you need a third option
The back of the upper arm is the third approved injection site for tirzepatide. It is the least commonly used of the three, primarily because self-injection in this location is difficult for most people. But it remains a valuable option in certain situations.
Exact location for upper arm injections
The injection zone is the fleshy back portion of the upper arm, roughly halfway between the shoulder and the elbow. The target area is the triceps region where subcutaneous fat naturally accumulates. Avoid the front of the arm (biceps area), the deltoid, and any area close to the elbow joint.
When the upper arm makes sense
The upper arm becomes relevant in several scenarios. If both the abdomen and thigh are experiencing significant reactions and need time to heal, the arm provides a necessary alternative to maintain your dosing schedule. Some people with very little abdominal or thigh fat find the upper arm has a more accessible subcutaneous layer. And if you have a partner, family member, or healthcare provider administering the injection for you, the upper arm is often their preferred site because of the angle and visibility it provides to the person giving the shot.
The self-injection challenge
Here is the honest truth about the upper arm. Most people cannot comfortably inject themselves there with proper technique. The injection requires reaching behind your non-dominant arm with your dominant hand, maintaining a steady grip on the syringe, and inserting the needle at the correct angle, all while keeping the skin pinched. That is a lot of coordination in an awkward position.
If you insist on self-injecting in the upper arm, some practical approaches can help. Use your opposite hand to pinch the back of the arm, then twist your injection hand around to insert the needle. Or use a countertop or table edge to press the back of your arm against, creating the same tissue compression that a manual pinch achieves. Neither method is ideal, and both increase the risk of injecting at the wrong angle or depth.
For most people using tirzepatide at home, the upper arm is best reserved as a backup option when someone else can administer the injection or when both primary sites need a rest.
Why injection site rotation matters
Rotating your injection sites is not optional. It is a critical part of safe, effective tirzepatide use that directly impacts both your comfort and your results.
Lipodystrophy: the main risk of poor rotation
Injecting repeatedly into the same spot causes a condition called lipodystrophy. This manifests in two ways. Lipohypertrophy is the accumulation of abnormal fatty tissue at the injection site, creating hard lumps or nodules under the skin. Lipoatrophy is the opposite, a loss of subcutaneous fat that creates visible depressions or dents. Both forms of lipodystrophy are problematic.
The hard lumps from lipohypertrophy do more than look and feel unpleasant. They alter medication absorption. Research on insulin injection sites, which share the same subcutaneous delivery mechanism as GLP-1 medications, shows that injecting into lipohypertrophic tissue can reduce medication absorption by up to 25%. That means a full dose of tirzepatide injected into damaged tissue may only deliver 75% of the expected medication to your bloodstream. The result is inconsistent effects, unpredictable appetite suppression, and frustration over why the medication seems to work some weeks and not others.
Injection site reactions and recovery time
Even without lipodystrophy, repeated injection in the same spot causes cumulative tissue irritation. Injection site reactions to tirzepatide, which include redness, swelling, itching, and tenderness, are reported by up to 10% of clinical trial participants. These reactions are usually mild and resolve within a few days. But if you keep injecting into the same irritated area, mild reactions can compound into persistent inflammation, increased sensitivity, and longer healing times.
Each specific injection spot needs approximately four to eight weeks of rest before being used again. Not days. Weeks. This is why having access to multiple sites and a systematic rotation plan is so important.
How to create an effective rotation system
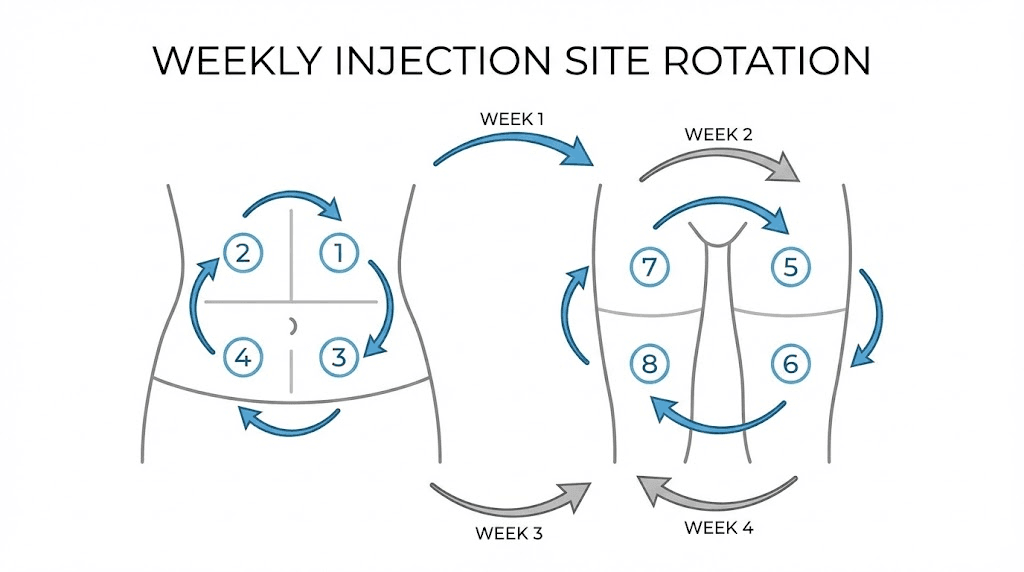
The simplest approach is a grid system for each site. Divide your abdomen into eight zones, four on each side of the navel, arranged in a rough grid pattern. Divide each thigh into four zones, two on the front and two on the outer side. If you use the upper arm, add two zones per arm. This gives you up to twenty distinct injection spots.
With weekly injections of tirzepatide, twenty spots means each individual spot gets roughly five months of rest between uses. That is more than enough time for complete tissue recovery.
A simpler approach works too. Alternate sides each week, left abdomen, then right thigh, then left thigh, then right abdomen, creating a four-week cycle that gives each general area a full month between injections. Within each area, shift the exact spot by at least one inch from the previous injection in that zone.
Track your injections. Write it down. Use a note on your phone, a simple chart on the fridge, or a dedicated tracking tool. Memory alone is unreliable, especially over months of weekly injections. After twelve weeks, you will not remember exactly where you injected on week three.
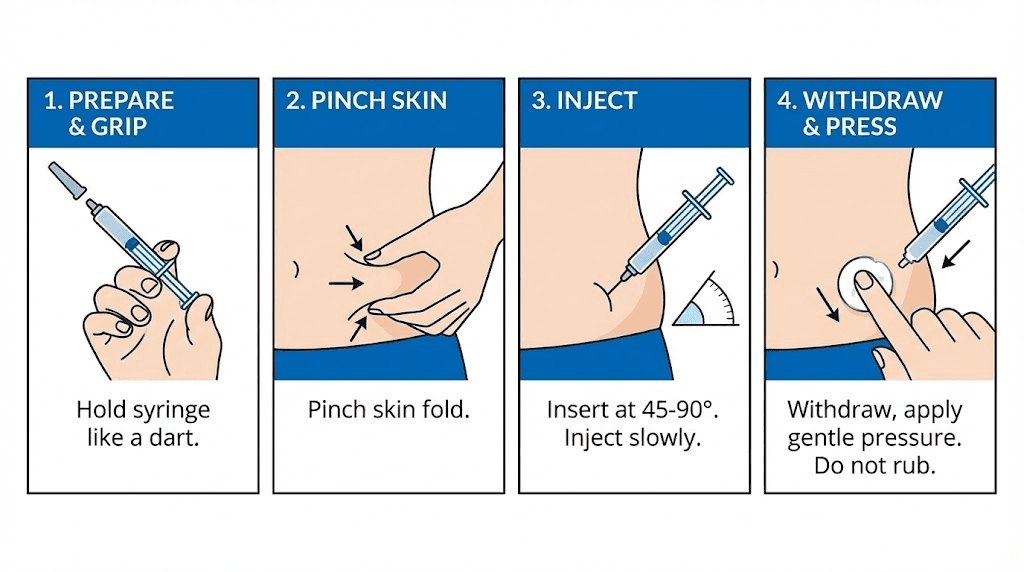
Injection technique step by step
Getting the site right is only half the equation. Proper injection technique determines whether the experience is smooth and painless or uncomfortable and problematic. Here is the complete process, step by step.
Preparation
Wash your hands thoroughly with soap and water. This is not optional and not just for appearance. The most common cause of injection site infection is bacteria transferred from unwashed hands. Gather your supplies before starting, your syringe with the correct dose drawn up, an alcohol swab, a cotton ball or small gauze pad, and a sharps container for disposal.
If using compounded tirzepatide from a vial, make sure you have followed the correct reconstitution protocol and that the solution is clear, colorless, and free of particles. If anything looks cloudy or discolored, do not use it.
Choosing and cleaning the site
Select your injection site based on your rotation schedule. Inspect the area. The skin should be healthy, intact, and free of any of the following.
Bruises from previous injections
Redness or ongoing irritation
Scars or stretch marks
Hard lumps from lipodystrophy
Moles, birthmarks, or skin lesions
Tattoos (the ink can make it harder to see reactions)
Clean the injection site with an alcohol swab using a circular motion from the center outward. Let the alcohol dry completely before injecting. This takes about 30 seconds. Injecting through wet alcohol stings and can push bacteria into the injection track. Patience here prevents problems.
The injection process
Pinch a fold of skin at the chosen site using your non-dominant hand. The fold should be about one to two inches wide. This lifts the subcutaneous fat away from muscle tissue and provides a clear target.
Hold the syringe in your dominant hand like a pencil or dart, with your index finger near the plunger and the barrel resting against your other fingers. Position the needle at a 90-degree angle to the skin surface. For most people using standard subcutaneous needles, perpendicular entry is correct.
Insert the needle with a quick, firm motion. Slow insertion hurts more than fast insertion. Think of it like removing a bandage. Quick is better. Push the needle all the way in until the hub touches the skin or the needle is fully inserted.
Release the skin pinch. Now depress the plunger slowly and steadily. Rushing the injection can cause a burning sensation as the medication disperses too quickly into the tissue. Take five to ten seconds for the full dose. Some people count slowly to ten as they push the plunger.
Once the plunger is fully depressed, hold the needle in place for ten seconds. This allows the medication to disperse and prevents it from tracking back up through the needle path when you withdraw. After ten seconds, pull the needle straight out at the same angle it went in.
After the injection
Apply gentle pressure to the injection site with a cotton ball or gauze for about 30 seconds. Do not massage or rub the area. Rubbing disperses the medication unpredictably, increases bruising, and can worsen injection site reactions.
Dispose of the used syringe immediately in a sharps container. Never recap needles, as this is one of the most common causes of accidental needlestick injuries. If you do not have a designated sharps container, a thick-walled plastic container like a laundry detergent jug works as a temporary solution.
Note the injection date and location in your tracking system. Some people take a quick phone photo of the injection site with a small dot from a washable marker to track exact positioning within a zone.
Does the injection site affect how well tirzepatide works?
This is one of the most common questions people ask, and the research is reassuring. The answer is no, with important caveats.
What the pharmacokinetic data shows
Eli Lilly's injection site study measured how much tirzepatide reached the bloodstream (total exposure, or AUC) and the peak concentration (Cmax) after a 5mg subcutaneous injection in the abdomen, thigh, and upper arm. The results showed no clinically relevant differences between any of the three sites. Peak blood concentration occurred between 8 and 72 hours after injection regardless of location, and the total amount of medication absorbed was equivalent across all three sites.
This makes sense given the pharmacology of tirzepatide. It is a once-weekly medication with a long half-life of approximately five days. Minor differences in initial absorption rate are smoothed out over the weekly dosing cycle. Unlike rapid-acting insulin, where absorption speed directly affects glucose control within minutes, tirzepatide builds to steady-state levels over several weeks of consistent dosing.
The caveat: damaged tissue changes everything
While the injection site itself does not matter for absorption, the condition of the tissue absolutely does. Injecting into healthy subcutaneous fat produces consistent, predictable absorption. Injecting into lipohypertrophic tissue, scar tissue, or acutely inflamed tissue produces unpredictable, potentially reduced absorption.
This is why rotation is so critical. The site itself is interchangeable. The tissue health at that site is not.
Body composition considerations
Your body composition can influence which sites work best for you practically, even if absorption remains equivalent. People with higher body fat percentages generally have more subcutaneous tissue at all three sites, making all locations comfortable and easy. People with lower body fat may find certain sites have insufficient subcutaneous tissue for a comfortable injection. In these cases, prioritizing the site with the most subcutaneous fat, often the abdomen, even in lean individuals, produces the most comfortable experience.
The Lilly study specifically enrolled participants across a range of body mass indices to confirm that absorption remained equivalent regardless of body size. Whether you have a BMI of 22 or 40, the three approved sites deliver the medication equally.
Abdomen vs thigh vs upper arm: how to choose
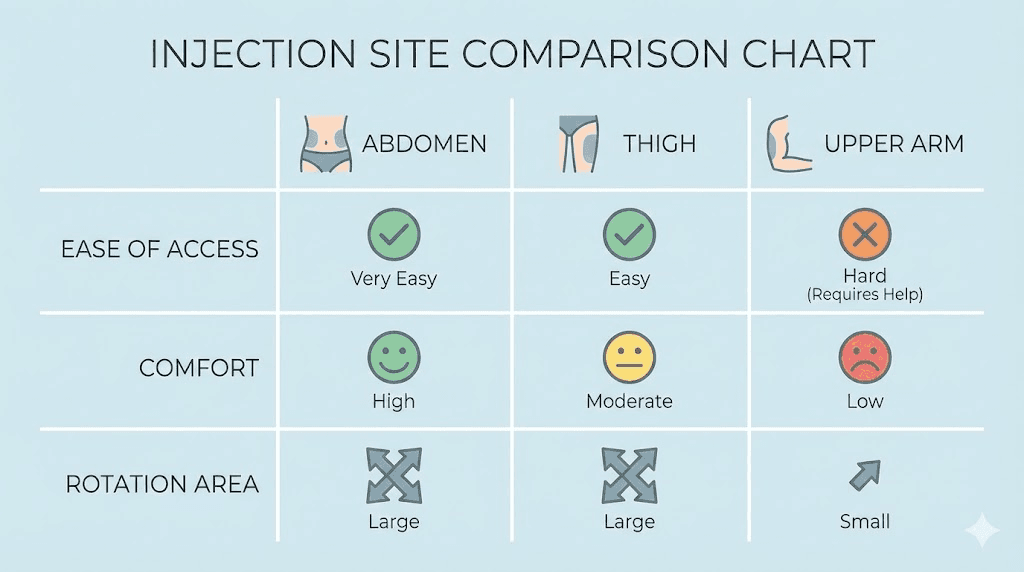
With equivalent efficacy across all sites, the choice comes down to practical factors. Here is a direct comparison to help you decide.
Factor | Abdomen | Thigh | Upper arm |
|---|---|---|---|
Self-injection ease | Excellent | Good | Difficult |
Rotation area | Large | Moderate (x2 legs) | Small |
Fat layer thickness | Usually thickest | Variable | Variable |
Visibility during injection | Excellent | Good | Poor (behind arm) |
Pain sensitivity | Moderate | Lower | Variable |
Needs assistance | No | No | Usually yes |
Clothing access | Requires lifting shirt | Requires shorts/pants adjustment | Requires short sleeve |
For most people, the optimal approach is to use the abdomen as the primary site and the thighs as the secondary rotation sites. This gives you three large areas (abdomen, right thigh, left thigh) that you can cycle through on a three-week rotation, with the upper arm held in reserve for situations where the other sites need additional rest.
Choosing based on body type
If you carry more weight in your midsection, the abdomen offers the thickest subcutaneous layer and the most comfortable experience. If you are lean through the trunk but have more tissue in your legs, the thighs may be more comfortable. If you are lean everywhere, focus on the abdomen and supplement with thigh injections, using careful pinch technique to ensure you stay in the subcutaneous layer.
Choosing based on reaction history
If you consistently experience redness and itching at one particular site, your body may be more reactive to injections in that area. This is not unusual. Some people develop mild localized allergic responses to the needle puncture or the medication vehicle at specific anatomical locations but not others. Try switching to a different site for several weeks to see if the reactions resolve.
Common injection site problems and solutions
Even with perfect technique, injection site issues occasionally arise. Knowing how to handle them prevents minor annoyances from becoming real problems.
Bruising
Small bruises after injection are common and not concerning. They happen when the needle nicks a small capillary under the skin. The blood leaks into surrounding tissue and creates a visible discoloration that typically resolves within a week or two.
To minimize bruising, let the alcohol dry completely before injecting. Apply gentle pressure, not rubbing, after withdrawing the needle. Avoid areas where you can see blood vessels through the skin. If you take blood thinners, supplements like fish oil or vitamin E, or high-dose aspirin, you may bruise more easily. Discuss this with your healthcare provider if bruising is persistent.
Lumps and nodules
Small, firm lumps at the injection site usually fall into one of two categories. Temporary lumps that appear immediately after injection and resolve within hours to days are typically caused by the medication pooling in the subcutaneous tissue before absorption. These are normal and harmless.
Persistent lumps that remain for weeks or grow larger may indicate early lipohypertrophy. This is a signal that you need to improve your rotation protocol. Stop injecting in that area immediately and give it at least eight weeks of complete rest. The lumps should gradually soften and shrink. If they do not resolve within three months, mention them to your healthcare provider.
Redness and itching
Mild redness and itching at the injection site are among the most commonly reported side effects of tirzepatide. Up to 10% of clinical trial participants experienced these reactions. They typically appear within hours of the injection and resolve within one to three days.
For mild reactions, a cold compress applied for 10 to 15 minutes can reduce inflammation and itching. Over-the-counter hydrocortisone cream (1%) applied to the area can help with persistent itching. An oral antihistamine like cetirizine or loratadine, taken 30 to 60 minutes before injection, can prevent or reduce reactions for people who consistently experience them.
If redness expands beyond two inches from the injection site, becomes hot to the touch, or is accompanied by fever, these are signs of a possible infection that requires medical attention. Do not attempt to treat these symptoms at home.
Pain during injection
Some degree of sensation during injection is normal. Sharp, significant pain is not. Common causes of excessive pain include cold medication, which causes the tissue to contract and increases nerve sensitivity. Injecting into muscle rather than subcutaneous fat, which happens when the needle is too long or the injection angle is wrong for your body composition. Reusing needles, which become dull after a single use. And injecting into tissue that is already inflamed from a recent injection.
Solutions are straightforward. Warm the medication to room temperature. Use a proper pinch technique to ensure subcutaneous placement. Never reuse needles. And track your rotation carefully to avoid revisiting recently used spots.
Medication leaking after injection
If you notice a small drop of liquid on your skin after withdrawing the needle, a tiny amount of medication has tracked back out through the needle path. This is called leakback and it is usually insignificant, amounting to less than 0.1ml of your dose.
To prevent leakback, keep the needle in place for a full ten seconds after completing the injection before withdrawing. Apply gentle pressure immediately after pulling the needle out. If leakback is a consistent problem, discuss with your healthcare provider whether a slightly longer or thicker gauge needle might help.
Special considerations for compounded tirzepatide
A growing number of people use compounded tirzepatide rather than the brand-name prefilled pens. The injection site guidelines remain the same, but several practical differences affect the injection experience.
Needle selection
Brand-name Mounjaro and Zepbound come in prefilled single-dose pens with pre-attached needles designed specifically for subcutaneous injection. With compounded tirzepatide, you select your own syringes and needles. The standard recommendation is a 29 to 31 gauge needle, half-inch to five-eighths inch in length, attached to a 1ml insulin syringe.
Thinner gauge numbers (higher numbers like 31) mean thinner needles that cause less pain but may be harder to push through thicker skin. Thicker gauge numbers (lower numbers like 27) are easier to handle but slightly more painful on insertion. Most SeekPeptides members find 30-gauge, half-inch needles to be the ideal balance of comfort and practicality.
Volume differences
Brand-name pens deliver a fixed dose in a fixed volume that is optimized for subcutaneous comfort. Compounded tirzepatide concentrations vary by pharmacy, and the volume you inject may be larger than the brand-name equivalent. Larger volumes take longer to inject, require more space in the subcutaneous tissue, and may produce a more noticeable lump immediately after injection.
If you are injecting volumes larger than 0.5ml, consider injecting more slowly to allow the tissue to accommodate the fluid. Some people split larger volumes into two separate injections at different sites within the same session to reduce localized tissue pressure.
Storage considerations that affect injection comfort
Compounded tirzepatide typically requires refrigeration, and cold medication causes significantly more injection site discomfort than room-temperature medication. Always remove your vial from the fridge 15 to 30 minutes before your scheduled injection time. You can also warm the filled syringe by holding it in your closed fist for two to three minutes. Do not use hot water, a microwave, or any external heat source, as these can degrade the medication.
Understanding proper tirzepatide storage is essential for both medication efficacy and injection comfort. Refer to our complete storage guide for detailed temperature and stability information.
Injection site concerns by body area
Different areas of the body present different challenges. Here is a deeper look at site-specific concerns that the general guides do not usually cover.
Abdominal concerns
After significant weight loss: People who have lost substantial weight on tirzepatide may notice changes in their abdominal tissue over time. As subcutaneous fat decreases, the tissue becomes thinner and the margin between subcutaneous and intramuscular injection narrows. If you started your protocol at a higher weight and have lost significant fat from your midsection, reassess your technique periodically. You may need to switch from a 90-degree to a 45-degree angle, use a shorter needle, or transition to the thigh as your primary site.
After abdominal surgery: If you have had any abdominal surgery, including C-section, appendectomy, hernia repair, or abdominoplasty, scar tissue in the area can interfere with injection comfort and absorption. Inject at least two inches away from any surgical scars, and be alert for signs that the tissue is not absorbing normally, such as persistent lumps or reduced medication effects when using areas near scar tissue.
Thigh concerns
Muscle injections: People with well-developed quadriceps or very low body fat on the thighs face a higher risk of accidentally injecting into muscle rather than subcutaneous tissue. Intramuscular injection of tirzepatide is not dangerous, but it can cause more pain, faster absorption, and potentially more intense side effects including increased muscle soreness. If you suspect your thigh injections are hitting muscle, switch to a 45-degree angle and ensure you are pinching a generous fold of skin.
Exercise timing: Injecting into the thigh before intense leg exercise can increase blood flow to the area and may speed absorption, potentially intensifying side effects. While the overall weekly exposure remains the same, the peak concentration may arrive faster. If you exercise regularly, time your thigh injections for rest days or inject in a different site on leg training days.
Upper arm concerns
Insufficient fat: The back of the upper arm has highly variable subcutaneous fat depth. Some people have ample tissue here, while others have almost none. If you can clearly see muscle definition in the triceps area, there may not be enough subcutaneous tissue for a comfortable, effective injection. Try pinching the skin before deciding. If you cannot pinch at least half an inch of tissue, choose a different site.
Angle difficulty: The awkward angle required for self-injection in the upper arm increases the risk of injecting too shallow (intradermal, which causes a painful wheal) or too deep (intramuscular). If you must self-inject here, consider using an injection aid device that holds the syringe at the correct angle while you operate the plunger with your free hand.
How tirzepatide injection sites compare to other GLP-1 medications
If you are switching to tirzepatide from semaglutide or another GLP-1 medication, you may be wondering whether the injection site approach changes. The short answer is that the approved sites are the same across all subcutaneous GLP-1 receptor agonists, but there are some practical differences worth noting.
Semaglutide and tirzepatide share the same three approved injection sites: abdomen, thigh, and upper arm. The best injection site for semaglutide follows the same principles outlined here. Liraglutide (Saxenda/Victoza), which is a daily injection rather than weekly, also uses these same sites but requires more frequent rotation due to daily use.
One difference between tirzepatide and semaglutide worth noting involves injection site reactions. Clinical trial data shows that tirzepatide produces injection site reactions in approximately 3-7% of patients, while semaglutide rates are generally lower at 1-2%. If you experienced minimal injection site issues on semaglutide, you may notice slightly more local reactivity with tirzepatide. Diligent rotation becomes even more important.
For those transitioning between medications, our semaglutide to tirzepatide conversion chart provides detailed dosage equivalency information, and the switching dosage chart covers the reverse transition.
Timing your injection for best results
While injection site selection does not affect absorption, the timing of your injection can influence your overall experience.
Consistency matters most
Choose a day and general time of day that you can maintain consistently each week. Tirzepatide has a five-day half-life, and consistent weekly dosing produces the most stable blood levels. If you inject every Tuesday morning, stick with Tuesday mornings. The best time to take your GLP-1 shot is ultimately the time you can do it reliably every week.
Managing side effects through timing
Many people experience nausea or decreased appetite in the first 24 to 48 hours after injection, with effects tapering as the week progresses. Some strategies involve timing injections to align these peak effect periods with your schedule.
Injecting on Friday evening means peak appetite suppression occurs over the weekend, when social eating and dining out are more common. Injecting on Sunday evening means the strongest effects carry you through the workweek, when structured eating is typically easier. Injecting in the evening can help you sleep through the initial nausea window, while injecting in the morning lets you monitor for any unexpected reactions during waking hours.
There is no universally correct time. Experiment and find what works for your lifestyle.
Can you change your injection day?
Yes, but do it gradually. If you need to shift your injection day, Eli Lilly recommends that the interval between any two doses should be at least 72 hours (3 days). So if you normally inject on Tuesday and want to move to Friday, you would inject on your regular Tuesday, then wait until at least Friday of the same week for your next dose, then continue on Fridays going forward. Do not inject more frequently than the minimum interval to compensate for the shift.
Injection supplies and preparation
Having the right supplies prepared before each injection makes the process smoother and safer.
For brand-name prefilled pens
If you are using Mounjaro or Zepbound prefilled pens, your supplies are straightforward. The pen itself, an alcohol swab, a cotton ball or gauze, and a sharps container. The pens come with the needle pre-attached under a cap. Check the expiration date on the pen before each use. Inspect the solution through the viewing window. It should be clear and colorless.
For compounded tirzepatide from a vial
Compounded tirzepatide requires more preparation. You will need the medication vial, a drawing needle (18-21 gauge for easier drawing), your injection needle and syringe (29-31 gauge), alcohol swabs for both the vial top and the injection site, cotton balls or gauze, and a sharps container.
Draw the correct dose using the tirzepatide dosage calculator to convert your prescribed milligram dose into the correct volume based on your vial concentration. Double-check the math before every injection. Dosing errors with compounded medications are more common than with prefilled pens because the calculation step introduces human error. SeekPeptides provides tools and resources to help members verify their calculations and maintain accurate dosing protocols.
After drawing the dose with the larger drawing needle, switch to your injection needle. This is important. Drawing through a rubber vial stopper dulls the needle tip, making injection more painful. Fresh injection needles for each injection are non-negotiable.
Injection site hygiene and infection prevention
Subcutaneous injections are generally very safe from an infection standpoint, but proper hygiene eliminates the small risk that exists.
Hand washing
Wash your hands with soap and water for at least 20 seconds before handling any injection supplies. If soap and water are not available, use an alcohol-based hand sanitizer with at least 60% alcohol content. Dry your hands completely before touching the syringe.
Skin preparation
Clean the injection site with a 70% isopropyl alcohol swab. Wipe in a circular motion starting at the center and moving outward to push bacteria away from the injection point. Wait for the alcohol to evaporate completely, approximately 30 seconds. Blowing on the site to speed drying is counterproductive, as your breath introduces bacteria.
Do not re-touch the cleaned area before injecting. If you accidentally touch it, clean it again with a fresh alcohol swab.
Signs of infection
Monitor your injection site for 48 to 72 hours after each injection. Normal post-injection effects include mild redness, slight tenderness, and a small lump. These should improve day by day. Seek medical attention if you notice spreading redness (especially with red streaks), increasing warmth at the site, pus or drainage, fever or chills, or increasing pain rather than decreasing pain over time. Injection site infections are rare but require prompt antibiotic treatment when they occur.
Travel and injection site considerations
Maintaining your tirzepatide schedule while traveling adds logistical challenges to injection site management.
When traveling with injectable medications, keep your medication in a temperature-controlled bag. TSA and most international airport security allow injectable medications with proper documentation. Carry a copy of your prescription and a letter from your healthcare provider if traveling internationally.
Hotel rooms and airplane lavatories are not ideal injection environments, but they work. The key is maintaining your hygiene protocol. Bring individually wrapped alcohol swabs, not a bottle of rubbing alcohol that could spill. Carry a portable sharps container. And stick to your rotation schedule even when your routine is disrupted.
Some people find it easier to inject in the thigh while traveling because it requires less space and less clothing removal than abdominal injections. This can be done discreetly in a bathroom stall or airplane lavatory by simply pulling up a shorts or pant leg.
Needle phobia and injection anxiety
Fear of needles is extremely common, affecting an estimated 20-30% of adults to some degree. If needle anxiety is making your tirzepatide injections stressful, several approaches can help.
Ice the injection site for 30 to 60 seconds before injecting. This numbs the skin and significantly reduces the sensation of needle insertion. The cold also constricts blood vessels, potentially reducing bruising.
Use distraction techniques. Listen to music, watch a video on your phone, or have a conversation with someone while injecting. Looking away from the injection site as the needle goes in can reduce anxiety significantly.
Practice deep breathing. Take three slow, deep breaths before injecting. Exhale slowly as you insert the needle. The exhalation activates your parasympathetic nervous system, reducing the stress response.
Consider an auto-injector device if manual syringe injection is too anxiety-provoking. Some people find that not being able to see the needle makes the process easier. Brand-name Mounjaro and Zepbound pens function this way. For compounded tirzepatide, aftermarket auto-injector devices are available that hold a standard syringe and deliver the injection with a button press.
The peptide injection pen guide covers auto-injector options in detail for those who prefer pen-style delivery.
Frequently asked questions
Can I inject tirzepatide in my buttocks?
No. The buttocks are not an FDA-approved injection site for tirzepatide. Only the abdomen, front of thigh, and back of upper arm have been studied for proper absorption. Injecting in unapproved sites may result in inconsistent medication delivery, altered absorption rates, or increased risk of complications.
Is it better to inject tirzepatide in the stomach or thigh?
Neither is objectively better. Pharmacokinetic studies confirm equal absorption from both sites. Choose based on comfort, convenience, and your rotation schedule. Most people start with the abdomen and add the thigh to their rotation over time. The best site is the one you can inject confidently and consistently each week.
How far apart should injection sites be?
At minimum, inject at least one inch (2.5 centimeters) away from your previous injection site within the same general area. Ideally, give each specific spot four to eight weeks of rest before using it again. A systematic rotation grid helps ensure adequate spacing and rest periods between injections.
What happens if I accidentally inject into muscle?
Intramuscular injection of tirzepatide is not dangerous, but it may cause more pain at the injection site, faster absorption, and potentially more pronounced initial side effects like nausea. The overall weekly efficacy remains the same because the total amount of medication absorbed does not change significantly. If it happens occasionally, there is no need to re-dose. Adjust your technique, angle, or pinch method for next time.
Should I alternate sides each week?
Yes, alternating sides is a simple and effective rotation strategy. If you inject in the left abdomen this week, inject in the right abdomen or right thigh next week. This natural alternation gives each side a minimum of two weeks rest between injections within the same general area.
Can I inject through clothing?
No. Never inject through clothing. The fabric can push bacteria into the injection site, the needle can carry fabric fibers into the subcutaneous tissue, and you cannot properly clean the skin or verify the injection site condition through clothing. Always inject on clean, dry, exposed skin.
What if I see blood when I withdraw the needle?
A small amount of bleeding after withdrawal is normal and simply means the needle nicked a small blood vessel. Apply gentle pressure with a cotton ball until the bleeding stops, usually within one to two minutes. The blood is from the surface tissue, not from a dangerous depth. Your medication was still delivered correctly.
Does the time of day I inject matter?
Not for medication effectiveness. Tirzepatide works the same whether injected morning, afternoon, or evening. However, the timing can affect how you experience side effects. Some people prefer evening injections so they sleep through the initial nausea window. Others prefer morning injections so they can monitor for unexpected reactions while awake.
External resources
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact questions. Members access detailed tirzepatide protocols, injection dosage charts, and expert guidance that takes the guesswork out of every aspect of peptide research.
In case I do not see you, good afternoon, good evening, and good night. May your injection sites stay healthy, your rotation stay consistent, and your results stay on track.