Feb 12, 2026
What if the problem with your semaglutide results is not the peptide at all, but how you prepared it?
That question haunts researchers who spend money on quality semaglutide, only to watch their results fall flat. The vial sits in the fridge. The dose gets drawn. The injection happens on schedule. But the outcomes never match the clinical data. And the culprit, more often than anyone wants to admit, is a reconstitution error made in the very first five minutes of handling the peptide.
Reconstituting a 5mg semaglutide vial is not complicated. But it is precise. One wrong move, whether it is squirting water directly onto the lyophilized powder, shaking the vial to speed up dissolution, or choosing the wrong diluent, can degrade the peptide before you ever draw your first dose. The difference between a vial that delivers consistent results for weeks and one that loses potency on day three often comes down to technique. Simple technique. Technique that takes less than ten minutes to learn and less than five minutes to execute.
This guide covers every step of the reconstitution process for a 5mg semaglutide vial, from selecting your supplies to calculating exact doses, storing the solution properly, and avoiding the mistakes that waste both peptide and money. Whether you are handling your first vial or your fiftieth, the semaglutide reconstitution chart for 5mg tables and protocols here will serve as your definitive reference. And if math is not your strong suit, the peptide reconstitution calculator at SeekPeptides can handle the numbers for you.
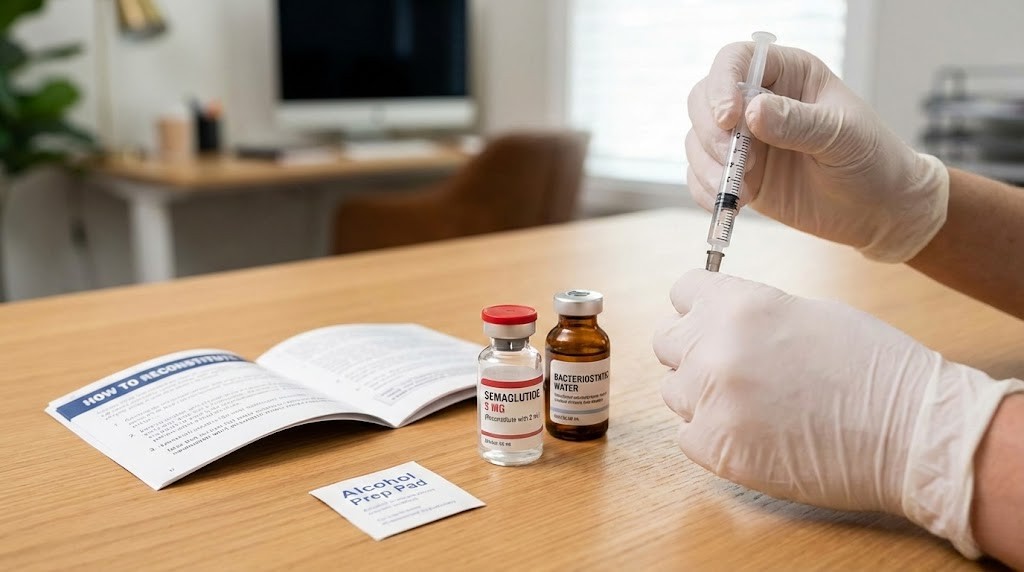
What you need before you start
Preparation matters more than most people think. A sterile workspace and the right supplies turn reconstitution from a stressful guessing game into a straightforward five-minute process. Skip a single item on this list and you risk contamination, inaccurate dosing, or peptide degradation before you even begin.
Here is what you need:
One 5mg semaglutide vial (lyophilized powder, sealed with a flip-off cap)
Bacteriostatic water (containing 0.9% benzyl alcohol as a preservative)
Alcohol swabs (70% isopropyl alcohol, individually wrapped)
A sterile syringe (3ml syringe with a needle for drawing water and injecting into the vial)
Insulin syringes (for drawing and administering individual doses, typically 0.5ml or 1ml with 29-31 gauge needles)
A clean, flat surface (wiped down with alcohol)
Sharps disposal container
The choice of diluent deserves special attention, and we will cover that in detail below. For now, understand that bacteriostatic water for peptides is the standard for multi-dose vials because the benzyl alcohol preservative prevents bacterial growth between uses. If you use sterile water instead, you lose that protection entirely.
Your workspace should be clean and well-lit. Wash your hands thoroughly. Lay out all supplies before you begin. Rushing through reconstitution leads to the kinds of common peptide mistakes beginners make, and those mistakes cost real money. A single contaminated vial means throwing away weeks of supply. A single math error means inconsistent dosing for the entire duration of the vial.
Understanding semaglutide as a peptide
Semaglutide is not just another weight loss compound. It is a 31-amino-acid GLP-1 receptor agonist with a molecular weight of 4,113.58 g/mol and the chemical formula C187H291N45O59. That molecular complexity is exactly why reconstitution technique matters so much. Large peptide molecules are fragile. Physical stress, temperature extremes, and contamination can all break the bonds that make semaglutide effective.
The peptide shares 94% structural homology with native human GLP-1, the hormone your body naturally produces to regulate blood sugar and appetite. But researchers modified three key positions to dramatically extend its half-life. An aminoisobutyric acid (Aib) substitution at position 8 resists degradation by the DPP-4 enzyme. An arginine substitution at position 34 prevents binding in the wrong location. And a C18 fatty diacid chain attached at position 26 allows the peptide to bind to albumin in the bloodstream, which slows its clearance and gives it a half-life of approximately seven days.
Those modifications are why semaglutide works as a once-weekly injection rather than requiring multiple daily doses. But they also create specific handling requirements. The fatty acid side chain makes the molecule sensitive to mechanical stress, which is why you never shake the vial. The isoelectric point of 5.4 means the peptide is most stable at a pH between 7.4 and 7.8, which aligns perfectly with the pH of bacteriostatic water. Understanding how peptides work at this molecular level helps explain why every step of the reconstitution process exists.
In its lyophilized form, semaglutide appears as a white to off-white powder or cake inside the vial. This freeze-dried format preserves the peptide structure during storage, keeping the molecule intact until you are ready to use it. The lyophilized vs liquid peptides comparison makes the advantage clear: lyophilized peptides maintain potency far longer than pre-mixed solutions. That is why reconstitution is a step you perform yourself rather than buying pre-mixed vials.
When stored properly in lyophilized form, semaglutide remains stable for two to three years. Once reconstituted, that stability window shrinks to 28 days under refrigeration. The clock starts the moment water touches the powder. Understanding what are peptides and how they degrade helps you appreciate why proper technique preserves every microgram of active compound in your vial.
Choosing the right diluent for semaglutide
Not all water is the same. This single decision, which diluent you add to your 5mg semaglutide vial, determines whether you get 28 days of consistent dosing or a single contaminated use. The guide on water to mix with peptides covers this in depth, but here is what you need to know specifically for semaglutide.
Bacteriostatic water (recommended)
Bacteriostatic water contains 0.9% benzyl alcohol. That small percentage of preservative prevents bacterial growth inside the vial after you puncture the rubber stopper. Since a 5mg semaglutide vial lasts multiple weeks at most doses, you will draw from it many times. Each needle puncture introduces a small contamination risk. The benzyl alcohol neutralizes that risk.
This is the standard choice for multi-dose peptide vials. It has a pH near 7.0, which falls within the stability range for semaglutide. It is widely available, inexpensive, and comes in sterile vials ready for use. For a deeper understanding of why this diluent dominates peptide protocols, read the full breakdown on how much bacteriostatic water to add to peptides.
Sterile water (single-use only)
Sterile water contains no preservative. Zero. Once you open it and puncture your peptide vial, bacterial contamination becomes a real possibility with every subsequent draw. If you must use sterile water, you should draw the entire vial contents into individual syringes immediately and store them separately. This is impractical for most people.
Some researchers choose sterile water because of sensitivity to benzyl alcohol. That is a valid reason. But it changes the entire workflow. You cannot simply pull a dose from the fridge each week. You need to pre-load every syringe on day one.
Normal saline (0.9% sodium chloride)
Normal saline is occasionally used for peptide reconstitution, but it offers no preservative benefit and can slightly alter the peptide environment compared to bacteriostatic water. For semaglutide specifically, bacteriostatic water remains the preferred choice among researchers who want maximum stability and convenience.
The bottom line is simple. Use bacteriostatic water. The complete guide on how much bacteriostatic water to mix with 5mg semaglutide walks through exact volumes, and the how to mix peptides with bac water article covers technique for any peptide you handle.
How much water to add to a 5mg semaglutide vial
This is where most confusion begins. The amount of bacteriostatic water you add determines the concentration of your reconstituted solution, which directly affects how many units you draw per dose. Get this wrong and every single injection will be inaccurate. Get it right and dosing becomes effortless math.
There is no single correct amount. Different volumes create different concentrations. The right choice depends on your dosing needs, syringe precision, and personal preference. Here are the three most common options:
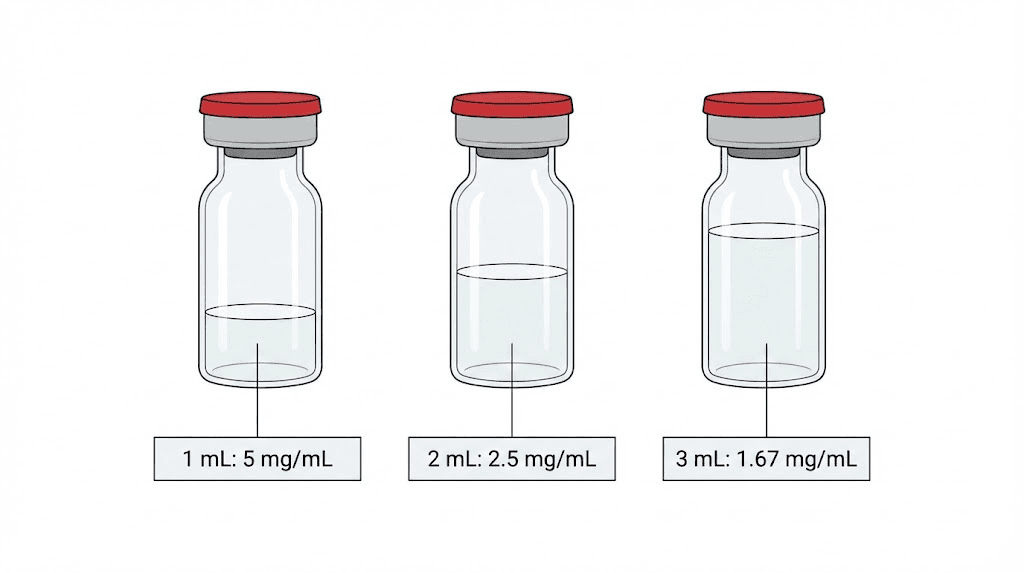
Option 1: 2ml of bacteriostatic water (most popular)
Adding 2ml to a 5mg vial produces a concentration of 2.5mg/ml. This is the most widely used ratio because it creates manageable volumes for common dose ranges. At 2.5mg/ml, a 0.25mg dose requires drawing just 0.1ml (10 units on an insulin syringe). A 0.5mg dose is 0.2ml (20 units). The math stays clean and the volumes are easy to measure accurately.
The semaglutide 5mg/2ml dosage chart provides a complete reference for this concentration, and the semaglutide dosage calculator can verify your math instantly.
Option 2: 1ml of bacteriostatic water (higher concentration)
Adding 1ml produces a concentration of 5mg/ml. This doubles the potency per unit of volume, which means smaller injection volumes. At 5mg/ml, a 0.25mg dose requires only 0.05ml (5 units). That is extremely precise and requires a high-quality insulin syringe to measure accurately. This option works best for people who prefer minimal injection volume or who are dosing at the lower end of the titration schedule.
The semaglutide 5mg/ml dosage chart maps every common dose at this concentration. But be warned: at higher concentrations, small measuring errors produce larger dosing mistakes. A single unit off on your syringe at 5mg/ml equals 0.05mg. At 2.5mg/ml, that same one-unit error equals only 0.025mg.
Option 3: 3ml of bacteriostatic water (lower concentration)
Adding 3ml produces a concentration of approximately 1.67mg/ml. This creates larger injection volumes, which some people find easier to measure precisely. At 1.67mg/ml, a 0.25mg dose requires about 0.15ml (15 units). The tradeoff is that higher doses require substantial volumes, and a full 2.4mg maintenance dose would require nearly 1.44ml, which exceeds the capacity of a standard 1ml insulin syringe.
For most researchers, the 2ml option hits the sweet spot between measurement precision and practical injection volumes. The semaglutide reconstitution chart covers all three concentrations in detail.
Here is a quick reference:
Water added | Concentration | 0.25mg dose | 0.5mg dose | 1.0mg dose | 2.4mg dose |
|---|---|---|---|---|---|
1ml | 5mg/ml | 5 units | 10 units | 20 units | 48 units |
2ml | 2.5mg/ml | 10 units | 20 units | 40 units | 96 units |
3ml | 1.67mg/ml | 15 units | 30 units | 60 units | 144 units |
The peptide calculator handles these conversions automatically if you prefer not to do the math manually. Understanding how to calculate peptide dosages is valuable regardless, because it helps you verify your numbers and catch errors before they become problems.
Step-by-step reconstitution process
You have your supplies. You have chosen your water volume. Now it is time to actually reconstitute the vial. This process takes about five minutes when done correctly. Do not rush it.
Step 1: Clean everything
Wipe down your work surface with an alcohol swab. Wash your hands with soap and water, then dry them completely. Open a fresh alcohol swab and clean the rubber stopper on both your semaglutide vial and your bacteriostatic water vial. Let the alcohol evaporate for about 10 seconds before proceeding. Do not blow on it. Do not wipe it dry. Just wait.
This step seems basic. It is. But skipping it is one of the fastest ways to contaminate a vial that needs to last 28 days. The peptide safety and risks guide explains why sterility protocols exist and what happens when they are ignored.
Step 2: Draw the bacteriostatic water
Attach a needle to your 3ml syringe if it is not already attached. Pull back the plunger to your desired volume, filling the syringe with air. For the standard 2ml reconstitution, pull back to the 2ml mark. Insert the needle through the center of the bacteriostatic water rubber stopper and push the air in. This equalizes pressure inside the vial and makes drawing water easier. Then invert the vial and slowly pull back the plunger to draw your desired volume of water.
Check for air bubbles. Tap the syringe gently to move any bubbles to the top, then push them back into the vial. Draw a tiny bit more water to replace what you expelled with the bubbles. Precision matters here. If you planned 2ml, draw 2ml. Not 1.8ml. Not 2.3ml. Exactly 2ml.
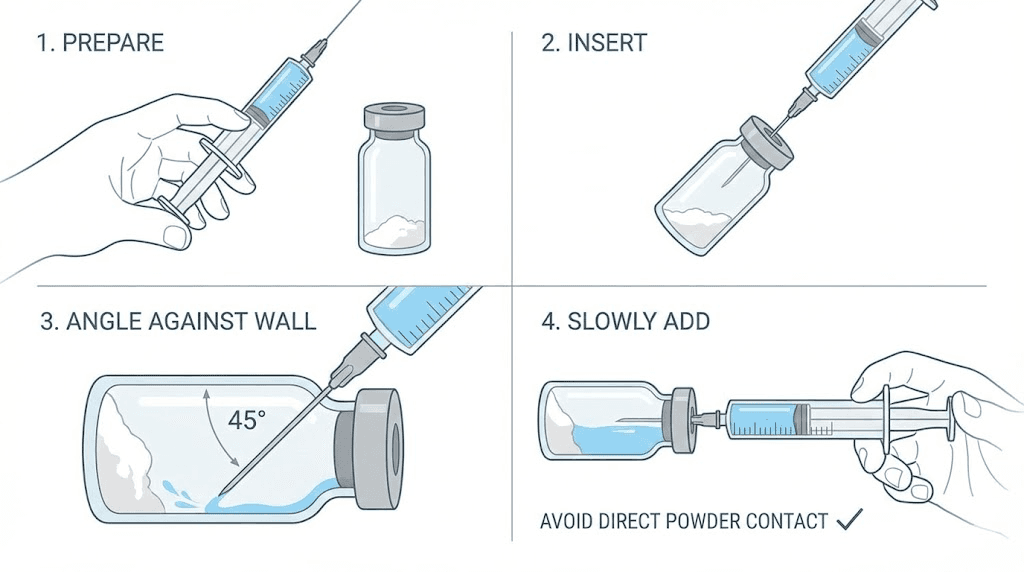
Step 3: Inject the water into the semaglutide vial
This is the most critical step, and it is where most people make their biggest mistake.
Insert the needle through the rubber stopper of the semaglutide vial. Angle the needle so it points toward the inner wall of the vial, not straight down at the powder. Now, slowly depress the plunger. Let the water trickle down the glass wall. It should slide gently toward the powder at the bottom.
Never aim the stream directly at the lyophilized cake. The force of water hitting the powder creates foaming, which introduces air into the solution and can denature the peptide through mechanical stress. The guide on how to reconstitute peptides emphasizes this point because it applies to every peptide you will ever handle, not just semaglutide.
Go slow. This is not a race. Take 30 to 60 seconds to inject the full volume of water. The slower you go, the less turbulence you create, and the more intact your peptide molecules remain.
Step 4: Swirl gently (never shake)
Once all the water is in the vial, remove the syringe and set it aside for disposal. Now, gently tilt the vial on its side and roll it between your palms. You can also swirl it in small, slow circles. The goal is to help the water reach all the lyophilized powder without creating violent agitation.
Do not shake the vial. Do not flick it. Do not invert it rapidly. Shaking creates shear forces that break peptide bonds and denature the molecule. A denatured peptide is a useless peptide. You would never know by looking at it, because the solution might still appear clear, but the biological activity would be degraded.
Semaglutide typically dissolves within one to three minutes of gentle swirling. If some powder remains stuck to the wall, set the vial upright in the refrigerator and check back in 15 to 30 minutes. Often the remaining particles dissolve on their own as the temperature equalizes. Patience preserves potency.
Step 5: Inspect the solution
A properly reconstituted semaglutide solution should be completely clear and colorless. No particles. No cloudiness. No foam that does not dissipate within a few minutes. Hold the vial up to a light source and look carefully.
If you see floating particles, the vial may be contaminated. If the solution is cloudy or discolored, the peptide may have degraded. If there is persistent foam that does not resolve after five minutes, you likely shook the vial too aggressively. In any of these cases, the safest course is to discard the vial and start fresh. Recognizing these signs early prevents wasted doses, and the section below on identifying degraded semaglutide covers this in more detail.
Step 6: Label and refrigerate
Write the date of reconstitution on the vial or on a small piece of tape affixed to it. This starts your 28-day clock. Place the vial upright in the refrigerator at 2-8 degrees Celsius (35.6 to 46.4 degrees Fahrenheit). Do not place it in the freezer. Do not leave it on the counter.
The peptide storage guide and how to store peptides after reconstitution provide comprehensive storage protocols for all peptides, including specific temperature ranges and light exposure guidelines that keep your semaglutide potent through the last dose.
Concentration reference table and dose calculations
Numbers matter in peptide work. A miscalculated dose is a wasted dose, or worse, an unintended dose that produces side effects without therapeutic benefit. This section provides every reference table you need to dose accurately from a reconstituted 5mg semaglutide vial.
At 2.5mg/ml (2ml water added to 5mg vial)
This is the most commonly used concentration. It produces clean, easy-to-calculate volumes for standard insulin syringes that mark in units where 100 units equals 1ml.
Desired dose | Volume to draw | Insulin syringe units |
|---|---|---|
0.25mg | 0.1ml | 10 units |
0.5mg | 0.2ml | 20 units |
0.75mg | 0.3ml | 30 units |
1.0mg | 0.4ml | 40 units |
1.25mg | 0.5ml | 50 units |
1.5mg | 0.6ml | 60 units |
1.7mg | 0.68ml | 68 units |
2.0mg | 0.8ml | 80 units |
2.4mg | 0.96ml | 96 units |
The formula is straightforward: divide your desired dose in milligrams by the concentration in mg/ml, then multiply by 100 to convert to insulin syringe units. So for a 1.0mg dose at 2.5mg/ml, you calculate 1.0 divided by 2.5, which equals 0.4ml, which equals 40 units. The semaglutide dosage chart in units and the semaglutide dosage chart in ml both provide this information in different formats depending on your preference.
At 5mg/ml (1ml water added to 5mg vial)
Higher concentration means smaller volumes. Precision becomes more critical here.
Desired dose | Volume to draw | Insulin syringe units |
|---|---|---|
0.25mg | 0.05ml | 5 units |
0.5mg | 0.1ml | 10 units |
0.75mg | 0.15ml | 15 units |
1.0mg | 0.2ml | 20 units |
1.25mg | 0.25ml | 25 units |
1.5mg | 0.3ml | 30 units |
1.7mg | 0.34ml | 34 units |
2.0mg | 0.4ml | 40 units |
2.4mg | 0.48ml | 48 units |
Notice how 5 units at this concentration delivers 0.25mg. On many insulin syringes, 5 units is the smallest clearly marked increment. That is manageable but leaves no room for error. If you find yourself frequently dosing at the lower end, the 2ml dilution might be more practical. The semaglutide 5mg vial dosage chart covers both concentrations in a single reference.
At 1.67mg/ml (3ml water added to 5mg vial)
Desired dose | Volume to draw | Insulin syringe units |
|---|---|---|
0.25mg | 0.15ml | 15 units |
0.5mg | 0.3ml | 30 units |
1.0mg | 0.6ml | 60 units |
1.7mg | 1.02ml | 102 units |
2.4mg | 1.44ml | 144 units |
At this concentration, the lower doses become very easy to measure precisely. But notice the problem at higher doses: 1.7mg requires more than 1ml, and 2.4mg requires 1.44ml. A standard 1ml insulin syringe cannot hold that volume. You would need a larger syringe, which typically has less precise markings. This is why the 3ml dilution works best for people who plan to stay at lower doses throughout their protocol.
If any of these calculations feel overwhelming, the semaglutide dosage in units conversion chart and the semaglutide syringe dosage chart lay out every common scenario in visual formats that eliminate guesswork. You can also verify any calculation using the semaglutide dosage calculator.
How to draw your dose from a reconstituted vial
Reconstitution is only half the equation. Drawing an accurate dose from the vial matters just as much. Sloppy technique here means inaccurate dosing for the entire life of the vial.
Choosing the right syringe
Use an insulin syringe. Period. These syringes are marked in units (where 100 units equals 1ml), which aligns perfectly with the concentration math above. They come with fine-gauge needles (29 to 31 gauge) that minimize injection discomfort and vial stopper damage.
For doses at the 2.5mg/ml concentration, a 1ml (100-unit) insulin syringe works for all doses up to 2.4mg. For the 5mg/ml concentration, a 0.5ml (50-unit) syringe provides finer markings that make small doses easier to measure. The semaglutide syringe conversion chart matches syringe types to concentration levels so you can choose the most precise option for your dose range.
The drawing process
Remove the reconstituted semaglutide vial from the refrigerator. Let it warm to room temperature for two to three minutes. Cold solutions are slightly more viscous, which can make drawing slower and less accurate.
Swab the rubber stopper with an alcohol wipe. This applies every single time you access the vial, not just the first time. Pull back the plunger of your insulin syringe to the volume you need, filling it with air equal to your dose volume. Insert the needle through the stopper and push the air in. This replaces the liquid you are about to remove, preventing a vacuum that makes future draws difficult.
Invert the vial. Pull back the plunger slowly and steadily until you reach your target volume. Check for air bubbles. If you see any, tap the syringe barrel gently with your fingernail until the bubbles rise to the top, then push them back into the vial. Draw again to reach your target volume.
Air bubbles in a subcutaneous injection are not dangerous in the way they would be intravenously. But they displace liquid, which means your dose volume is inaccurate. A 10-unit draw with a 2-unit air bubble is really an 8-unit dose. Over weeks of dosing, those small errors compound. The peptide injections guide covers syringe technique in much greater detail, and the peptide dosing guide explains why precision at each draw matters for your results.
Understanding units vs. milligrams
This is where confusion runs rampant. Units on an insulin syringe do not correspond to any universal measurement of semaglutide. They are simply volume markings.
On a standard U-100 insulin syringe, 100 units equals 1ml. That is all a unit means in this context. The actual milligram dose depends entirely on your reconstitution concentration. At 2.5mg/ml, 10 units equals 0.25mg. At 5mg/ml, 10 units equals 0.5mg. Same number of units, completely different dose.
This is why articles like how many mg is 40 units of semaglutide and how many mg is 50 units of semaglutide and 20 units of semaglutide in mg exist. The answer always depends on concentration. If you do not know your concentration, you do not know your dose. The semaglutide dosing chart in units provides the translation across all common concentrations.
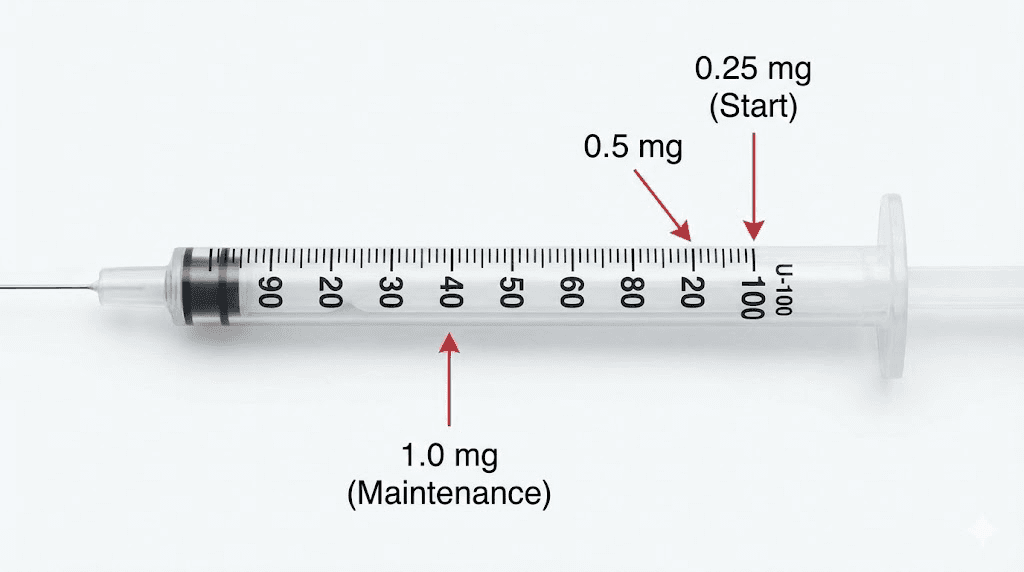
Titration schedule for 5mg semaglutide
You do not start semaglutide at the full dose. Nobody does. The titration protocol exists because GLP-1 receptor agonists cause gastrointestinal side effects, primarily nausea, that are dose-dependent. Starting low and escalating gradually gives the body time to adapt, reducing the severity and duration of these effects.
Here is the standard titration schedule used in clinical research:
Phase | Weeks | Weekly dose | Units at 2.5mg/ml | Units at 5mg/ml |
|---|---|---|---|---|
Phase 1 | 1-4 | 0.25mg | 10 units | 5 units |
Phase 2 | 5-8 | 0.5mg | 20 units | 10 units |
Phase 3 | 9-12 | 1.0mg | 40 units | 20 units |
Phase 4 | 13-16 | 1.7mg | 68 units | 34 units |
Maintenance | 17+ | 2.4mg | 96 units | 48 units |
Each phase lasts four weeks. Some researchers extend a phase if they are still experiencing significant side effects at the current dose. There is no rush to reach maintenance. The semaglutide 5mg dosage chart outlines this schedule with additional detail, and understanding how fast semaglutide works helps set realistic expectations for each phase.
A few important notes about titration. First, the 0.25mg starting dose is not a therapeutic dose. It is purely for acclimatization. Meaningful GLP-1 receptor activation for appetite suppression typically begins around 0.5mg to 1.0mg, though individual responses vary. If you are wondering how long semaglutide takes to work or specifically how long semaglutide takes to suppress appetite, the answer usually falls between weeks 4 and 8, depending on individual sensitivity and titration speed.
Second, not everyone needs to reach 2.4mg. Some researchers achieve their desired outcomes at 1.0mg or 1.7mg and stay there. The compounded semaglutide dose chart and the compounded semaglutide guide discuss how individual responses inform dosing decisions. If you plateau at a certain dose, you can escalate further. If side effects become unmanageable, you can step back to the previous dose and try escalating again after another four weeks.
Third, consistency matters more than speed. Taking your dose on the same day each week, at approximately the same time, produces more stable blood levels than erratic scheduling. Semaglutide has a half-life of approximately seven days, which means weekly dosing maintains relatively steady concentrations. The how long to stay on semaglutide article covers long-term usage considerations including what happens when you stop.
How long does a 5mg vial last
A single 5mg vial holds a finite amount of peptide. How long it lasts depends entirely on your weekly dose. This matters for planning purchases, managing refrigerator storage, and ensuring you do not run out mid-titration.
Weekly dose | Doses per vial | Duration (weeks) | Duration (months) |
|---|---|---|---|
0.25mg | 20 | 20 | ~5 months |
0.5mg | 10 | 10 | ~2.5 months |
1.0mg | 5 | 5 | ~1.25 months |
1.7mg | ~2.9 | ~3 | ~3 weeks |
2.4mg | ~2.08 | ~2 | ~2 weeks |
At the starting dose of 0.25mg per week, a single 5mg vial lasts 20 weeks, which is nearly five months. That is an extraordinary amount of time from one vial. But remember the 28-day stability rule: once reconstituted, the solution should be used within 28 days. At 0.25mg per week, you would only use 1mg in 28 days, meaning 4mg would go to waste if you reconstituted the entire vial at once.
This is an important planning consideration. If you are in the early titration phases, you might consider whether a smaller reconstitution volume makes sense, or whether purchasing smaller vials is more cost-effective. The peptide cost calculator can help you compare options. The article on how long compounded semaglutide lasts in the fridge discusses stability timelines in detail, and the question of does compounded semaglutide need to be refrigerated has a definitive answer: yes, always.
At the maintenance dose of 2.4mg per week, a 5mg vial lasts roughly two weeks. You get two doses plus a small remainder. At this stage, many researchers also look at semaglutide reconstitution chart for 10mg vials because the 10mg option lasts longer at higher doses and reduces reconstitution frequency. The semaglutide 10mg dosage chart and how much bacteriostatic water for 10mg semaglutide cover the larger vial size.
Storage after reconstitution
You have reconstituted your 5mg semaglutide vial. The solution is clear. The date is written on the label. Now what?
Storage is not optional. It is as critical as the reconstitution itself. A perfectly prepared vial stored improperly will degrade faster than a poorly reconstituted vial stored correctly. Temperature is the single most important factor.
Temperature requirements
Reconstituted semaglutide must be stored at 2-8 degrees Celsius. That is 35.6 to 46.4 degrees Fahrenheit. This is standard refrigerator temperature. Place the vial upright in the main body of the refrigerator, not in the door where temperature fluctuates every time you open it. Not in the back where it might freeze if your refrigerator runs cold.
At temperatures above 25 degrees Celsius (77 degrees Fahrenheit), the peptide degrades measurably. Brief excursions, like the few minutes it takes to draw a dose, are not a problem. But leaving the vial on a countertop for hours will cost you potency. The article on how long peptides last at room temperature quantifies this degradation rate, and the answer is sobering for anyone who has been careless with storage.
Light exposure
Light accelerates peptide degradation. Ultraviolet light is the worst offender, but even normal indoor lighting contributes to breakdown over time. Keep the vial in its box if it came with one, or store it in a dark area of the refrigerator. Some researchers wrap vials in aluminum foil for additional protection. This is not strictly necessary for a 28-day window under refrigeration, but it does not hurt.
Freezing
Do not freeze reconstituted semaglutide. Ever. Ice crystal formation physically damages the peptide structure, creating aggregation and reducing biological activity. This damage is irreversible. Even if the solution thaws and appears clear, the peptide has been compromised.
Lyophilized (unreconstituted) semaglutide powder can be stored frozen or at room temperature. The freeze-drying process already removed the water, so ice crystals cannot form. But once water is added, freezing becomes destructive. The how long peptides last in powder form article explains why lyophilized peptides are so much more resilient than reconstituted ones.
The 28-day rule
Use your reconstituted semaglutide within 28 days. This is not an arbitrary number. It reflects the combined stability data for the peptide itself and the preservative activity of the benzyl alcohol in bacteriostatic water. After 28 days, both potency and sterility become questionable. The question of can you use expired semaglutide comes up often, and while the peptide does not become dangerous, it does become progressively less effective. The broader topic of do peptides expire applies the same principles across all peptide types.
If you will not use the entire vial within 28 days, consider reconstituting with less water to create a higher concentration, allowing smaller volumes per dose and potentially fewer unused portions. Or use the how long reconstituted peptides last in fridge guide and the how long peptides last in the fridge reference to plan your usage schedule before you reconstitute.
Common reconstitution mistakes and how to avoid them
Mistakes happen. The question is whether you catch them before they cost you an entire vial of semaglutide, or after. This section covers the most frequent errors researchers make and how to prevent each one.
Mistake 1: Squirting water directly onto the powder
This is the most common reconstitution error by far. The natural instinct is to aim the stream of water at the lyophilized cake sitting at the bottom of the vial. It seems logical. You want the water to dissolve the powder, so you aim at the powder. But the force of the water stream hitting the delicate freeze-dried structure creates foaming, introduces air into the solution, and generates mechanical stress that can denature the peptide.
The fix: always aim the needle at the glass wall of the vial and let the water trickle down slowly. The water will reach the powder on its own. Patience here preserves potency. The general how to reconstitute peptides guide hammers this point because it is the single most impactful technique improvement a beginner can make.
Mistake 2: Shaking the vial
You see a clump of undissolved powder. Your instinct says shake it. Do not.
Shaking creates shear forces, rapid mechanical stress that breaks peptide bonds. Semaglutide, with its fatty acid chain at position 26, is particularly susceptible to mechanical denaturation. The solution might look fine after shaking. It might even be clear. But the biological activity of the molecule has been compromised in ways you cannot see.
Swirl gently instead. If powder remains after gentle swirling, wait. Set the vial in the fridge and check back in 30 minutes. Time dissolves what force destroys.
Mistake 3: Using sterile water for a multi-dose vial
Sterile water has no preservative. Every time you insert a needle through the rubber stopper to draw a dose, you risk introducing bacteria into a solution that has no defense against them. Over days and weeks of repeated access, the contamination risk grows.
If you use sterile water, you should draw all doses into individual syringes immediately after reconstitution and store them separately. For most people, this is impractical and increases the risk of dosing errors. Just use bacteriostatic water. The comparison at bacteriostatic water for peptides explains the differences and why the choice matters for multi-use vials.
Mistake 4: Not cleaning vial stoppers
Every vial stopper gets swabbed with alcohol. Every time. No exceptions. This applies to the bacteriostatic water vial, the semaglutide vial before reconstitution, and the semaglutide vial before every subsequent dose draw. Rubber stoppers are not sterile surfaces. They collect dust, microorganisms, and contaminants from the environment.
Mistake 5: Math errors in concentration calculations
The most dangerous mistake is also the most preventable. Confusing units with milligrams, using the wrong concentration for your calculations, or drawing 20 units when you meant 2 units, these errors produce either underdosing or overdosing. Both waste your peptide and compromise your results.
Always double-check your math. Write down your concentration and tape it to the vial. Use the peptide reconstitution calculator to verify calculations. Reference the semaglutide mixing chart for 5mg before every draw if needed. There is no shame in checking twice. There is plenty of frustration in getting it wrong.
Mistake 6: Poor storage after reconstitution
Leaving the vial out on the counter. Storing it in the freezer. Placing it in the refrigerator door where temperature fluctuates. Exposing it to direct sunlight. Any of these can degrade your peptide within days rather than weeks. Follow the storage guidelines above without exception.
Mistake 7: Injecting air bubbles
Small air bubbles in a subcutaneous injection are not medically dangerous. But they displace liquid volume, which means your actual peptide dose is less than what you intended to draw. Over multiple doses, this creates inconsistency in your protocol. Take the extra 30 seconds to tap out air bubbles before injecting.
For a comprehensive list of errors that extends beyond reconstitution to all aspects of peptide handling, the common peptide mistakes beginners make article covers over a dozen pitfalls that catch even experienced researchers off guard.
Signs your reconstituted semaglutide has gone bad
Peptide degradation is not always obvious. But there are visible and practical indicators that your reconstituted semaglutide is no longer viable. Knowing these signs prevents you from wasting weeks on a peptide that has lost its potency.
Visual indicators
A properly reconstituted and stored semaglutide solution should remain clear and colorless throughout its 28-day life. If you notice any of the following, the peptide may be compromised:
Cloudiness or haziness. A solution that was once crystal clear but has turned cloudy indicates protein aggregation. The peptide molecules are clumping together, which means they are no longer in their active form. This can result from temperature excursions, contamination, or simple degradation over time.
Visible particles. Floating specks, fibers, or crystals in the solution suggest contamination or precipitation. Do not use a vial with visible particulate matter.
Discoloration. Any yellow, brown, or pink tint indicates chemical degradation. Fresh reconstituted semaglutide is colorless. Any color change means something has gone wrong.
Persistent foam. Small bubbles from drawing doses are normal and resolve quickly. A layer of foam that persists for more than a few minutes suggests protein denaturation, usually from shaking or temperature damage.
Practical indicators
Sometimes the solution looks fine but the peptide is not working. This is harder to detect because it requires noticing the absence of expected effects rather than the presence of visible problems.
If you have been at a dose that previously produced noticeable appetite suppression and that effect suddenly disappears, potency loss is a possible explanation. If your progress has stalled despite consistent dosing, the peptide may have degraded. The article on why not losing weight on semaglutide discusses multiple factors that affect results, including peptide quality. Semaglutide fatigue and other side effects that suddenly disappear at a dose that previously caused them can also signal potency loss.
When to discard
Discard the vial if you observe any visual abnormality. Discard it after 28 days regardless of how it looks. Discard it if you suspect it was left at room temperature for more than a few hours or if it was accidentally frozen. When in doubt, throw it out. The cost of a new vial is always less than the cost of weeks wasted on degraded peptide.
Reconstituting 5mg semaglutide vs 10mg vials
Once you move past the early titration phases and begin using higher doses, you may consider switching from 5mg to 10mg vials. The reconstitution process is identical, but the math and practical considerations change in important ways.
Key differences
A 10mg vial contains twice the peptide mass. If you add the same 2ml of bacteriostatic water, you get a concentration of 5mg/ml instead of 2.5mg/ml. If you add 4ml to maintain the 2.5mg/ml concentration, you have twice the total volume to work through.
At higher maintenance doses like 2.4mg per week, a 10mg vial lasts roughly four weeks, which aligns neatly with the 28-day stability window. A 5mg vial at that dose lasts only about two weeks, meaning you must reconstitute a new vial mid-month. For convenience and consistency, the 10mg vial makes more practical sense at maintenance doses. The semaglutide mixing chart for 10mg and the semaglutide mixing chart provide side-by-side comparisons.
When to use 5mg vs 10mg
The 5mg vial is ideal during the early titration phases (0.25mg to 1.0mg per week) because you use less peptide per week and do not need a large supply. It is also suitable for researchers who want to test semaglutide before committing to a larger purchase.
The 10mg vial makes sense once you have titrated to 1.7mg or higher and plan to stay at that dose or move to 2.4mg. The larger vial reduces the frequency of reconstitution, which means fewer opportunities for contamination and less time spent on preparation.
The reconstitution technique, however, does not change at all. Same water-down-the-wall method. Same gentle swirling. Same storage requirements. The only difference is the concentration you calculate and the volumes you draw. For anyone considering the switch, the semaglutide reconstitution chart for 10mg covers every detail of the larger vial size.
Safety considerations
Reconstituting and handling peptides at home carries inherent responsibilities. While semaglutide itself has a well-documented safety profile from extensive clinical research, the process of reconstitution, storage, and self-administration introduces variables that clinical settings control but home users must manage themselves.
Sterility is non-negotiable
Every needle is single-use. Every stopper gets swabbed. Every surface gets cleaned. Reusing needles introduces both contamination risk and increased discomfort due to dulled needle tips. The small cost of a new insulin syringe for each dose is negligible compared to the risk of a contaminated vial.
The peptide safety and risks article covers the full spectrum of safety considerations, from sterile technique to recognizing adverse reactions. If you are new to self-injection, the peptide injections guide provides step-by-step instruction on proper subcutaneous injection technique, and the article on where to inject GLP-1 identifies the preferred injection sites.
Know your source
The quality of your semaglutide matters as much as your reconstitution technique. Understanding the difference between research vs pharmaceutical peptides helps you evaluate what you are working with. Third-party testing certificates, proper lyophilization, and sealed vials under vacuum are all quality indicators worth verifying before you ever begin reconstitution. The peptide vial research article explains what to look for when evaluating vial quality.
Diet and lifestyle context
Semaglutide does not work in isolation. The peptide suppresses appetite and modulates glucose metabolism, but outcomes depend heavily on the broader context of diet and activity. The semaglutide diet plan covers nutritional strategies that complement GLP-1 agonist use. The question of can you drink on semaglutide comes up frequently, and the answer involves both safety and efficacy considerations that merit careful thought.
Understanding potential side effects
GLP-1 receptor agonists affect appetite, gastric motility, and blood sugar regulation. Nausea is the most common side effect, particularly during dose escalation. This is precisely why the titration schedule exists. Other reported effects include constipation, diarrhea, headache, and fatigue. The semaglutide fatigue article addresses one of the more frustrating side effects in detail. Some users have also reported hair thinning, which the GLP-1 hair loss guide examines thoroughly.
If you decide to discontinue semaglutide, doing so abruptly rather than tapering can produce rebound effects. The article on semaglutide withdrawal symptoms explains what to expect and how to manage the transition.
Comparing semaglutide with alternatives
Semaglutide is not the only GLP-1 agonist available. Tirzepatide, which acts on both GLP-1 and GIP receptors, is an increasingly popular alternative. The comparison between semaglutide vs tirzepatide is one of the most researched topics among peptide researchers. If you are considering switching, the switching from semaglutide to tirzepatide guide and the semaglutide to tirzepatide conversion chart provide the dosing equivalencies you need. The reverse scenario, switching from tirzepatide to semaglutide, is covered as well.
For those exploring the broader landscape of weight management peptides, the articles on peptides for weight loss, best peptide for fat loss, and peptides for fat loss provide comprehensive comparisons across multiple peptide options. The best peptide for visceral fat loss narrows the focus to the specific fat depot that most affects metabolic health.
Advanced considerations for experienced researchers
Once you have the basics mastered, there are several more nuanced aspects of semaglutide reconstitution and usage worth understanding.
Compounded formulations
Compounded semaglutide comes from compounding pharmacies and may include additional ingredients like vitamin B12 or glycine. The reconstitution process for compounded formulations follows the same general principles, but the specific instructions from the compounding pharmacy should always take priority. The compounded semaglutide guide provides a thorough overview of what makes these formulations different.
Semaglutide combined with B12 has become particularly popular because B12 may help offset some of the fatigue that GLP-1 agonists can cause. The semaglutide with B12 article and the semaglutide with B12 dosage chart cover dosing specifics for these combination formulations. Similarly, semaglutide with glycine represents another combination that researchers are exploring.
Different pharmacies may also provide different dosing charts specific to their formulations. The Strive pharmacy semaglutide dosage chart, the iVIM semaglutide dosing chart, the Empower pharmacy semaglutide guide, and the Direct Meds semaglutide guide all reflect the specific concentrations and instructions those providers use.
Oral semaglutide and alternative delivery methods
Injectable semaglutide is not the only delivery option. Oral formulations have become available, though they involve different pharmacokinetics and dosing protocols. The oral semaglutide drops guide covers how these formulations work and how their dosing compares to injectable versions. The broader comparison of injectable vs oral peptides examines the bioavailability differences that make injection the preferred route for most peptide researchers. There are even GLP-1 patch delivery systems in development, which the Onmorlo GLP-1 patches article explores.
Stacking and combination protocols
Some researchers combine semaglutide with other peptides as part of broader protocols. The peptide stacks guide and the peptide stack calculator help with planning these combination approaches. The best peptide stack for weight loss article specifically addresses weight management combinations.
Whether combining semaglutide with BPC-157 for gut support, TB-500 for tissue repair, or other peptides, each compound still needs to be reconstituted separately. Never mix different peptides in the same vial unless the specific combination has been validated. The peptide cycle planning resource helps organize multi-peptide protocols.
Understanding the relationship between semaglutide and GLP-1
A common question among newcomers is whether semaglutide and GLP-1 are the same thing. They are not. The article is GLP-1 the same as Ozempic clarifies this distinction. GLP-1 is the natural hormone. Semaglutide is a modified analog designed to last much longer in the body. Ozempic is a brand name for a specific pharmaceutical semaglutide product. The Ozempic alternatives article covers other options for those researching the broader GLP-1 agonist category.
For researchers who want a deeper understanding of the molecular science behind peptides like semaglutide, the peptide formula guide breaks down the chemistry that makes these molecules work.
SeekPeptides members access comprehensive protocol guides, dosing calculators, and a community of experienced researchers who have navigated these exact reconstitution and dosing decisions. Whether you are handling your first vial or optimizing an established protocol, the evidence-based resources at SeekPeptides cover every step of the process.
Practical tips for consistent reconstitution
Beyond the core steps, a few practical habits make the entire process smoother and more reliable over time.
Always use the same water volume. Switching between 1ml and 2ml dilutions between vials creates confusion and increases the risk of dosing errors. Pick one concentration and stick with it. Your muscle memory with the syringe will become a second layer of error-catching.
Reconstitute at the same time and place. Routine breeds precision. When you always reconstitute at the same countertop, with the same supplies laid out in the same order, you are less likely to skip a step or make a mistake.
Keep a dose log. Write down the date, time, and number of units drawn for each dose. This catches errors in real time and gives you a reference if you question whether you took your dose that week.
Dispose of sharps properly. Every used needle goes into a sharps container. Not the trash. Not the recycling. A proper sharps container. When it is full, dispose of it according to your local guidelines.
The broader article on getting started with peptides covers these foundational habits in the context of peptide research generally. The peptide dosage chart serves as a universal reference that applies the same calculation principles to any peptide you handle. For those who want a free tool that handles all the math, the free peptide reconstitution calculator and the peptide calculator for weight loss are both available through SeekPeptides.
Reconstitution for other peptides
The technique you learn with semaglutide transfers directly to other peptides. If you also work with tirzepatide, the how to reconstitute tirzepatide guide and the tirzepatide reconstitution chart follow the same fundamental principles. The tirzepatide reconstitution chart PDF provides a printable version you can keep near your workspace. For BPC-157, the BPC-157 dosage calculator handles the math. For TB-500, the TB-500 dosage calculator does the same.
The water-down-the-wall technique, the gentle swirl, the 28-day storage window, the temperature requirements, all of these principles apply to virtually every lyophilized peptide. Master them once with semaglutide and you are prepared for any peptide you encounter. The complete list of injectable peptides shows just how broad the applications are, and the nasal spray peptides article covers non-injectable delivery methods for those exploring alternatives.
Frequently asked questions
Can I use regular tap water or distilled water to reconstitute semaglutide?
No. Tap water contains microorganisms, minerals, and chlorine that will contaminate and degrade the peptide. Distilled water, while free of minerals, is not sterile and contains no preservative for multi-dose use. Always use bacteriostatic water for peptides or, in specific circumstances, sterile water for single-use applications. The guide on water to mix with peptides explains why diluent choice matters so much.
What happens if I accidentally shake the vial instead of swirling it?
A single brief shake is unlikely to destroy the entire vial. But vigorous or prolonged shaking can denature the peptide through mechanical stress. If you accidentally shook it once, let the solution settle, check for persistent foam or cloudiness, and proceed with caution. If you shook it hard or repeatedly, the potency may be compromised. Consider starting a new vial if you notice diminished effects. The how to reconstitute peptides guide provides additional context on why gentle handling matters.
Can I travel with reconstituted semaglutide?
Yes, but temperature control is essential. Use an insulated cooler bag with ice packs to maintain 2-8 degrees Celsius during transit. Do not put the vial directly against ice, which could freeze it. The peptide storage guide has specific recommendations for travel scenarios. Keep your reconstituted solution out of direct sunlight and avoid leaving it in hot vehicles.
How do I know if my semaglutide vial is still good after 25 days?
Visually inspect the solution. If it remains clear, colorless, and free of particles, it is likely still viable. However, potency does decline gradually over time. If you are within the 28-day window and the solution looks normal, proceed with your dose. After 28 days, discard regardless of appearance. The article on how long compounded semaglutide lasts in the fridge provides more detail on stability timelines.
Is the reconstitution process different for compounded semaglutide?
The fundamental technique is identical. Water down the wall, gentle swirl, refrigerate. However, compounded formulations may come pre-reconstituted or may include additional ingredients that alter the concentration or storage requirements. Always follow the specific instructions from your compounding pharmacy first. The compounded semaglutide guide covers the nuances of these formulations in depth.
What should I do if the powder does not dissolve completely?
Give it time. Place the vial upright in the refrigerator and check back in 30 minutes. Most undissolved particles will dissolve on their own as the temperature stabilizes and the water slowly saturates the remaining powder. If particles persist after an hour, try another round of very gentle swirling. If they still will not dissolve, the lyophilized powder may have been compromised before reconstitution, and you should consider discarding the vial.
Can I draw from the same vial with different syringe sizes?
Yes, as long as you are using the same concentration calculation for all draws. The syringe size does not affect the peptide. Just ensure you are reading the volume markings correctly on whichever syringe you use. The semaglutide syringe dosage chart shows how different syringe sizes correspond to the same dose.
Do I need to warm the vial before drawing each dose?
Letting the vial sit at room temperature for two to three minutes before drawing can make the process slightly easier because cold solutions are more viscous. But it is not strictly necessary. The brief time it takes to swab the stopper and prepare your syringe is usually sufficient. Do not leave the vial out for extended periods, and always return it to the refrigerator immediately after drawing your dose.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your reconstitutions stay sterile, your concentrations stay accurate, and your results stay consistent.