Feb 27, 2026

Before you inject another dose, stop and read this. The needle went deeper than expected. Maybe the plunger felt different. Maybe the injection hurt more than usual. And now a question is circling in your mind: did that semaglutide go into muscle instead of fat?
You are not alone. Thousands of people self-administering compounded semaglutide or brand-name formulations wonder this exact thing every single week. The worry is understandable. Semaglutide is designed for subcutaneous injection, meaning it belongs in the fatty layer just beneath the skin. Not the muscle. When it ends up somewhere it was not designed to go, questions multiply fast.
Here is the reassuring part. An accidental intramuscular injection of semaglutide is unlikely to cause serious harm. The medication will still be absorbed. Your body will still process it. But the absorption rate changes, the side effect profile may shift, and the experience at the injection site itself can be noticeably different. This guide covers everything you need to know about what happens when semaglutide enters muscle tissue, what symptoms to watch for, exactly what steps to take right now, and how to prevent it from happening again. Whether you are on your first week of semaglutide or months into your protocol, proper injection technique matters more than most people realize.
What happens when semaglutide goes into muscle instead of fat
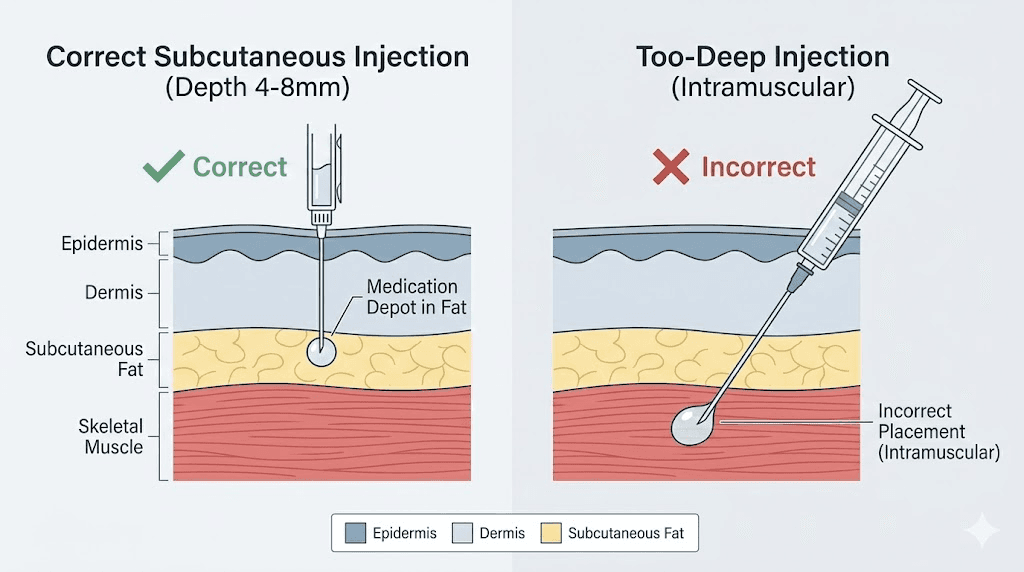
Understanding the difference between subcutaneous and intramuscular injection starts with blood supply. Muscle tissue contains far more blood vessels than the subcutaneous fat layer sitting just beneath your skin. That difference in vascularity changes everything about how a medication gets absorbed.
Semaglutide was specifically engineered for slow, gradual absorption through fatty tissue. The dosing protocols and pharmacokinetics are built around this assumption. When the medication enters subcutaneous fat, it creates a small depot. Think of it as a reservoir. The drug molecules slowly diffuse from that reservoir into surrounding capillaries over hours and days, creating the steady, predictable blood levels that make semaglutide effective for weight loss and blood sugar management.
Muscle tissue changes this equation.
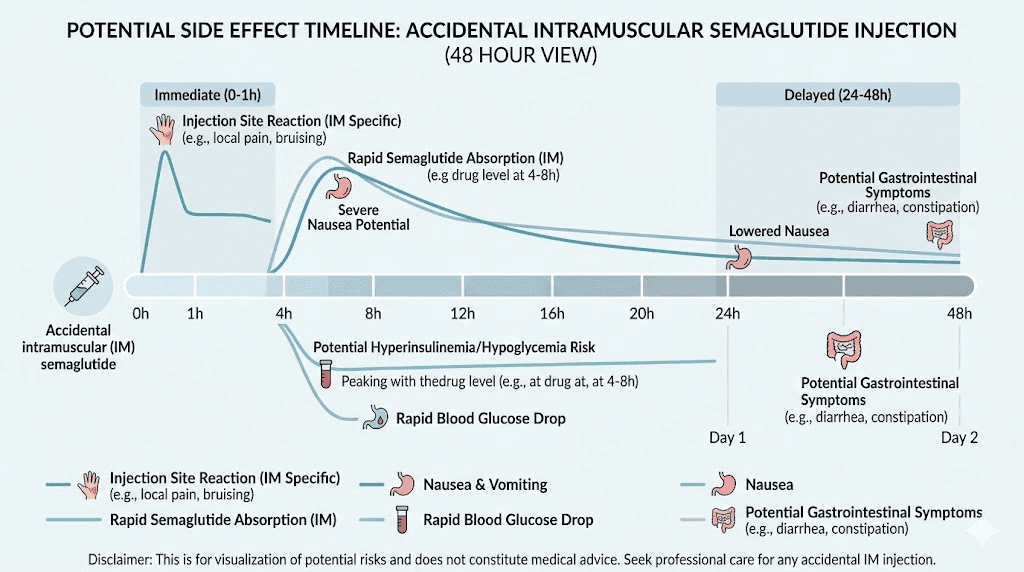
When semaglutide enters muscle, the richer blood supply means faster absorption. Instead of a slow, controlled release over days, the medication enters the bloodstream more rapidly. Peak blood levels may arrive sooner than intended. The duration of action may shorten. And the predictable pharmacokinetic profile that your prescriber relied on when setting your dose gets disrupted.
Does this mean disaster? No. The semaglutide molecule itself does not change. It is the same medication whether it sits in fat or muscle. The GLP-1 receptors it binds to do not care where the injection happened. But the speed and intensity of its effects can shift, and that is where the practical differences show up in how you feel over the next few days.
The absorption rate difference explained
Studies on subcutaneous versus intramuscular injection of various medications consistently show that intramuscular delivery produces faster peak plasma concentrations. For a medication like semaglutide that is meant to maintain steady levels across an entire week, this faster absorption can create a spike-and-drop pattern rather than the smooth curve your body expects.
The subcutaneous fat layer acts like a sponge. It absorbs the medication and releases it slowly. Fat tissue has relatively poor blood circulation compared to muscle, which is exactly what makes it ideal for weekly injectable medications. The timeline for semaglutide to work depends heavily on this steady absorption pattern.
Muscle tissue, by contrast, is dense with capillaries. Blood flow through active muscle can be 20 to 40 times higher than through resting subcutaneous tissue. This means a dose of semaglutide injected intramuscularly could reach peak concentrations in the bloodstream significantly faster than the same dose injected subcutaneously.
The practical result? You might feel the effects of semaglutide more intensely in the first 24 to 48 hours after an accidental muscle injection. Appetite suppression may kick in faster and feel stronger than usual. But the flip side is equally important. Those effects may also wear off sooner than expected, potentially leaving you with less coverage toward the end of your dosing week.
Does it affect how well semaglutide works
For a single accidental intramuscular injection, the overall impact on your treatment goals is minimal. Your body still receives the full dose. The medication still activates GLP-1 receptors. Appetite suppression still occurs. Blood sugar regulation still happens.
The concern is not about effectiveness disappearing entirely. It is about the distribution of that effectiveness over time. Instead of a steady 7-day coverage, you might get 4 to 5 days of stronger effect followed by 2 to 3 days of diminished effect. For most people, this single-instance disruption is clinically insignificant. Your next properly administered subcutaneous injection will return things to normal.
However, repeated intramuscular injections over multiple weeks could theoretically affect overall treatment outcomes. Inconsistent blood levels mean inconsistent appetite suppression, inconsistent blood sugar control, and potentially slower weight loss progress. This is why correcting your technique matters, not because one mistake will ruin everything, but because consistent subcutaneous delivery produces the best long-term results.
Immediate side effects to watch for
After accidentally injecting semaglutide into muscle, certain side effects may appear more quickly or with greater intensity than usual. Not everyone experiences them. Some people notice no difference at all. But knowing what to watch for eliminates the guesswork and the anxiety that comes with it.
Injection site reactions
The most immediate and noticeable difference is at the injection site itself. Muscle tissue contains more nerve endings than subcutaneous fat. Significantly more. This means an intramuscular injection typically hurts more than a properly placed subcutaneous one.
Pain. That is often the first sign something went deeper than intended.
The discomfort from an intramuscular injection tends to be deeper and more aching compared to the mild sting of a subcutaneous injection. You might feel a dull throb at the site for several hours or even a day or two. This is normal. The muscle fibers were disrupted by the needle, and your body responds with localized inflammation.
Bruising is another common sign. When the needle passes through the subcutaneous layer and into muscle, it has more tissue to traverse and more blood vessels to potentially nick along the way. You might notice a bruise developing at the injection site within a few hours. Most injection-site bruises are small, less than an inch across, and resolve within 7 to 14 days without any treatment.
A small lump or nodule at the injection site can also occur. This happens because the medication, originally intended to create a depot in loose fatty tissue, instead sits in denser muscle fibers that do not disperse it as easily. These lumps typically resolve on their own as the medication absorbs, usually within a few days.
Gastrointestinal symptoms
Nausea is the most commonly reported side effect of semaglutide regardless of injection technique. But after an intramuscular injection, it can arrive faster and hit harder. The reason is straightforward. Faster absorption means more semaglutide reaching GLP-1 receptors in a shorter time window, and those receptors in the brain and gut respond accordingly.
If you are already prone to semaglutide-related bloating or nausea, an accidental muscle injection may amplify these symptoms temporarily. Some people report more intense nausea in the first 12 to 24 hours after an intramuscular dose compared to their usual subcutaneous injections.
Other gastrointestinal effects to monitor include vomiting, diarrhea, abdominal pain, and constipation. These effects are dose-dependent, meaning the faster the medication hits your system, the more pronounced they may be during the initial absorption phase. For most people, these amplified GI effects settle down within 24 to 48 hours as blood levels of semaglutide stabilize.
Fatigue and dizziness
Fatigue and dizziness sometimes accompany the faster onset of semaglutide effects. When the medication reaches higher peak concentrations more quickly, some people experience a more pronounced sense of tiredness or lightheadedness. This usually resolves within the first day or two.
Staying hydrated helps. Eating small, manageable meals helps more. The combination of faster appetite suppression and potential nausea can lead some people to eat and drink less than they should in the hours after an intramuscular injection. Dehydration and insufficient calorie intake amplify fatigue and dizziness regardless of injection technique.
When symptoms are NOT related to the injection route
Here is something worth understanding. Many of the side effects people attribute to an accidental muscle injection are actually normal side effects of semaglutide at any injection site. Nausea, reduced appetite, and burping occur commonly with subcutaneous injections too, especially during the first few weeks of treatment or after a dose increase.
If you recently started semaglutide or just moved to a higher dose, the symptoms you are experiencing may be entirely normal and unrelated to injection depth. The anxiety of thinking you injected incorrectly can make you hyperaware of every sensation, turning ordinary side effects into apparent emergencies. Take a breath. Monitor. And use the checklist in the next section to guide your response.
What to do right now: step-by-step response guide
You think you injected semaglutide into muscle. Maybe you know for certain. Either way, here is exactly what to do.
Step 1: do not panic
This is genuinely the most important step. An accidental intramuscular injection of semaglutide is not a medical emergency. The medication is not toxic to muscle tissue. It will not cause permanent damage. It will still work. Your body will process it.
Step 2: do not inject another dose
The medication is in your body. Whether it entered fat or muscle, you received your full dose. Taking a second injection because you think the first one "did not count" would give you a double dose. That creates a genuine overdose risk with significantly amplified side effects. Dosing accuracy matters, and doubling up is far more dangerous than an intramuscular injection.
Step 3: note the injection details
Write down what happened. The injection site. The time. The dose. How deep the needle went. Whether you pinched the skin. What the injection felt like. This information is useful if you need to discuss the incident with your healthcare provider, and it helps you identify what went wrong so you can correct your injection technique next time.
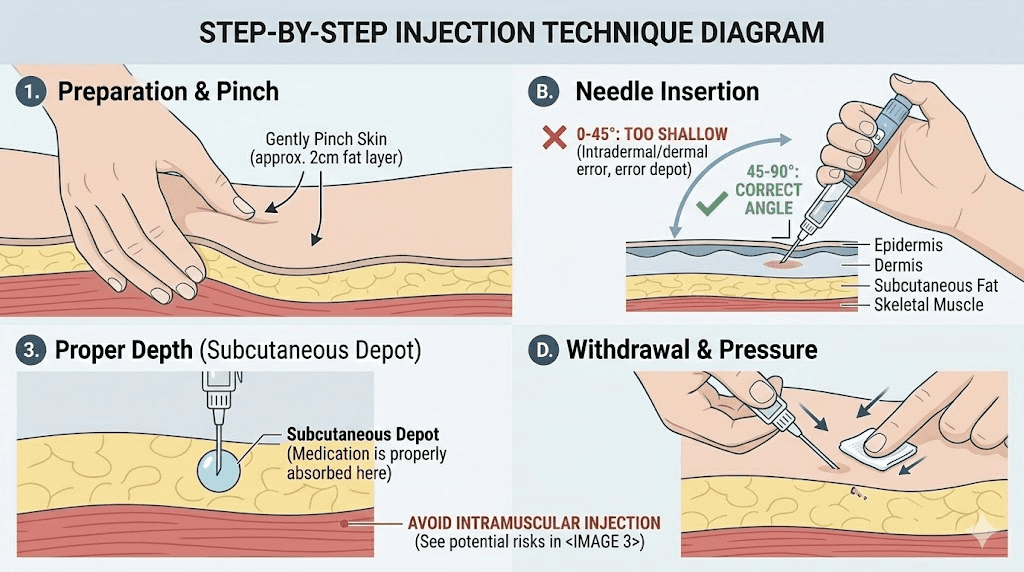
Step 4: apply gentle pressure
If the injection site is painful or you see early signs of bruising, apply gentle pressure with a clean gauze pad for 10 to 20 seconds. Do not rub the area. Rubbing can spread blood under the skin and worsen bruising. A cold compress applied for 10 to 15 minutes can help reduce inflammation and discomfort.
Step 5: monitor for 24 to 48 hours
Watch for the side effects described above. Most will be mild and self-limiting. Keep track of any nausea, injection site pain, fatigue, or gastrointestinal changes. Stay hydrated. Eat small, bland meals if nausea occurs. Follow the recommended food guidelines for semaglutide to minimize GI discomfort.
Step 6: continue your regular dosing schedule
Take your next dose at the normally scheduled time. Use the proper subcutaneous technique covered later in this guide. One accidental intramuscular injection does not require any changes to your dosing schedule, frequency, or amount.
Step 7: contact your healthcare provider if needed
Most people will not need medical attention after an accidental muscle injection. But contact your provider if you experience severe or persistent pain at the injection site lasting more than 48 hours, signs of infection such as increasing redness, warmth, swelling, or pus, severe nausea or vomiting that prevents you from keeping fluids down, or any symptoms that feel significantly different from your normal semaglutide experience.
Why semaglutide is designed for subcutaneous injection
The FDA approved semaglutide exclusively for subcutaneous administration. This is not an arbitrary decision. The entire clinical development program, every pharmacokinetic study, every efficacy trial, every safety assessment, was conducted using subcutaneous injection. The dosing recommendations that your prescriber follows assume subcutaneous delivery.
The pharmacokinetic rationale
Semaglutide has a half-life of approximately 7 days, which is what allows for once-weekly dosing. This long half-life depends partly on the slow absorption from subcutaneous tissue. The fatty tissue creates a drug depot that releases semaglutide gradually, maintaining therapeutic blood levels throughout the entire week.
When you look at a semaglutide dosage chart, the recommended doses were calibrated specifically for subcutaneous absorption kinetics. The dosing in units reflects how much medication needs to enter subcutaneous tissue to produce the desired steady-state blood levels across seven days.
Intramuscular injection was not studied in clinical trials. The FDA labeling explicitly states that semaglutide should not be administered intramuscularly or intravenously. This does not mean intramuscular injection is acutely dangerous. It means the safety and efficacy of that route have not been formally evaluated, so no clinical data exists to guide intramuscular dosing.
The practical design features
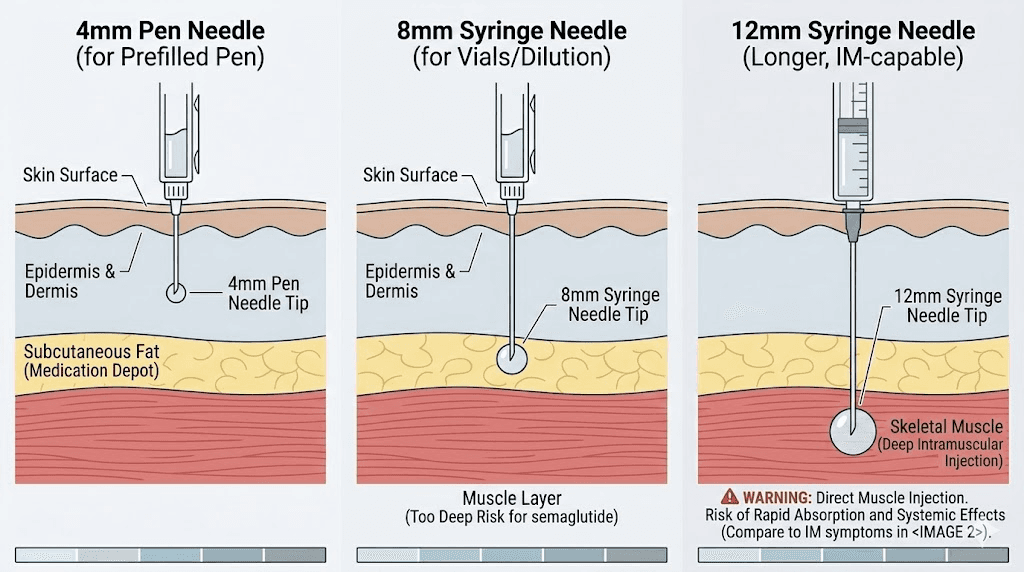
Everything about semaglutide delivery systems is designed for subcutaneous injection. Pre-filled pens like Ozempic and Wegovy use short 4mm needles, specifically chosen to reach the subcutaneous fat layer without penetrating into muscle. The needle gauge is fine enough to minimize discomfort in the relatively nerve-sparse fatty tissue. Even the volume of the injection, typically small, is optimized for subcutaneous depot formation.
For people using compounded semaglutide with insulin syringes, needle length becomes a more important consideration. Insulin syringes typically come with needles ranging from 6mm to 12.7mm. The longer the needle, the higher the risk of reaching muscle tissue, especially in areas with thinner subcutaneous fat layers. Understanding reconstitution and proper injection tools is part of safe semaglutide use.
The anatomy of a proper injection site
Knowing where to inject is half the battle. Knowing what lies beneath the skin at each injection site is the other half. Your skin has three main layers that matter for injection technique, and understanding them turns injection from guesswork into precision.
Skin, fat, and muscle: the three layers
The outermost layer is the epidermis and dermis, collectively known as the skin. This layer is thin, typically 1 to 3 millimeters. Your needle passes through this quickly.
Beneath the skin lies the subcutaneous fat layer. This is where semaglutide belongs. The thickness of this layer varies dramatically depending on the injection site, your body composition, your sex, and your overall body fat percentage. In the abdomen, the average subcutaneous fat thickness is about 14 millimeters. In the thigh, it averages about 10 millimeters. Women generally have thicker subcutaneous fat layers than men, with an average difference of roughly 5 millimeters.
Below the fat sits muscle. Once the needle passes through the subcutaneous layer, it enters muscle tissue. This is the layer you want to avoid with semaglutide.
The three approved injection sites
Three areas of the body provide the best combination of adequate subcutaneous fat, accessibility for self-injection, and consistent absorption. Choosing the right site and understanding its anatomy prevents most accidental intramuscular injections before they happen.
The abdomen. This is the most commonly recommended injection site for semaglutide. The abdomen typically has the thickest subcutaneous fat layer of any approved injection site, with average depths of 12 to 20 millimeters depending on body composition. Inject at least 2 inches away from the navel. Avoid the area directly around the belly button, where the fat layer thins and the abdominal fascia sits closer to the surface.
The front or outer thigh. The thigh injection site offers good subcutaneous access for most people, though the fat layer here is typically thinner than the abdomen. The front and outer portions of the mid-thigh provide the best fat-to-muscle ratio. Avoid the inner thigh, where major blood vessels run closer to the surface.
The back of the upper arm. This site is better suited for injections administered by someone else, as self-injection in the upper arm requires awkward positioning. The subcutaneous layer here is moderate in thickness and varies significantly between individuals.
How body composition affects injection depth
Body composition is the single biggest factor determining whether a given needle length will reach muscle. A person with 35 percent body fat has substantially more subcutaneous padding than someone at 15 percent body fat. The BMI considerations for GLP-1 medications extend beyond eligibility and into practical injection technique.
Research on subcutaneous tissue thickness shows that differences of 10 kg/m-squared in BMI account for approximately 4 millimeters of variation in subcutaneous fat depth. For someone with a lower BMI or less body fat, even a standard-length needle can reach muscle in certain injection sites.
This is particularly relevant for people who have been on semaglutide for several months and have experienced significant weight loss. As you lose body fat, your subcutaneous layer gets thinner. An injection technique that worked perfectly at the beginning of your treatment may start reaching muscle tissue as your body composition changes. Reassessing your technique periodically is not overcautious. It is smart.
How to tell if you injected into muscle
Sometimes you know immediately. Other times, the signs show up hours later. And sometimes, you genuinely cannot tell. Here are the most reliable indicators that semaglutide ended up in muscle rather than fat.
During the injection
Increased resistance. Muscle tissue is denser than subcutaneous fat. If the plunger felt harder to push than usual, or if the needle seemed to meet more resistance as it entered the tissue, you may have reached muscle.
Sharper, deeper pain. Subcutaneous injections in fatty tissue typically produce a mild sting or sometimes no pain at all. Hitting muscle feels different. The pain is deeper, more of an ache than a sting, and it often continues after the needle is removed.
A sensation of hitting something firm. Fat tissue feels soft and gives way easily. Muscle feels firmer and more structured. If you felt the needle encounter something tighter than expected, it likely passed through the fat layer.
After the injection
More soreness than usual. A properly placed subcutaneous injection should leave minimal soreness. If the injection site aches like you received a vaccination (which is an intramuscular injection by design), that is a strong indicator the semaglutide went into muscle.
Bruising. While bruising can occur with subcutaneous injections too, deeper bruising, the kind that feels tender to pressure and takes longer to appear, often suggests muscle penetration.
Faster onset of effects. If your appetite suppression kicks in faster than usual or your side effects seem more intense in the first 12 to 24 hours, faster absorption from muscle tissue may be the explanation.
Earlier wearing off. If you notice your appetite returning or effects plateauing sooner than usual before your next dose, the faster absorption may have shortened the effective duration.
When you genuinely cannot tell
Sometimes the injection felt normal, there is no unusual pain, and no obvious signs point one way or the other. If this is the case, the most likely scenario is that you injected correctly into subcutaneous tissue. The fact that you are questioning it suggests awareness, not necessarily error. Continue your normal schedule and focus on proper technique for future injections.
How to prevent accidental muscle injections
Prevention is straightforward once you understand the mechanics. Every accidental muscle injection results from one or more of a small number of fixable factors: wrong needle length, wrong injection angle, wrong injection site, or failure to create adequate separation between fat and muscle.
Choose the right needle length
Needle length is your first line of defense against accidental muscle injection.
For pre-filled pens like Ozempic, the standard NovoFine Plus pen needles are 4mm at 32 gauge. At this length, the needle physically cannot reach muscle tissue in most people when inserted perpendicularly into an area with adequate subcutaneous fat. This is by design.
For syringe injections with compounded semaglutide, needle selection requires more thought. Insulin syringes commonly come with 6mm, 8mm, or 12.7mm (half-inch) needles. For subcutaneous injection, 6mm to 8mm needles are generally appropriate for most people. Longer needles, particularly 12.7mm, significantly increase the risk of reaching muscle, especially in leaner individuals or at injection sites with thinner fat layers.
If you have lost significant weight during your semaglutide treatment or carry less body fat than average, consider switching to shorter needles. A 6mm needle with proper technique keeps most people safely in the subcutaneous zone. Your semaglutide dosage calculator helps determine exact volumes, and your needle selection should match your current body composition, not where you started.
Master the skin pinch technique
Pinching the skin at your injection site creates a fold of subcutaneous tissue that lifts the fat layer away from the underlying muscle. This simple technique can effectively double the distance between your needle tip and the muscle layer.
Here is how to do it correctly. Using your non-dominant hand, grasp a fold of skin and fat between your thumb and index finger. Lift gently but firmly. You want to create a raised fold of tissue, not squeeze so hard that the fat compresses. The fold should feel soft and pliable, not tight.
With the skin pinched, insert the needle into the raised fold at a 90-degree angle. The pinch ensures the needle enters fat tissue that has been lifted well away from the muscle beneath. Once the injection is complete and you have held the needle in place for the recommended time, release the skin pinch before or after removing the needle.
The skin pinch is especially important for people with lower body fat percentages, those using needles longer than 6mm, and anyone injecting in the thigh or upper arm where subcutaneous fat tends to be thinner than in the abdomen.
Use the correct injection angle
Injection angle works together with needle length to determine how deep the needle penetrates.
A 90-degree angle, straight into the skin, is appropriate when you can grasp at least 2 inches of tissue in your skin pinch. This perpendicular approach works well with short needles (4mm to 6mm) in areas with adequate fat.
A 45-degree angle reduces effective penetration depth and is recommended when you can only grasp about 1 inch of tissue, when using longer needles, or when injecting in sites with thinner subcutaneous fat. Tilting the needle reduces the vertical depth it reaches by roughly 30 percent compared to a straight 90-degree insertion.
For lean individuals or anyone concerned about muscle penetration, the 45-degree angle combined with a skin pinch provides the maximum margin of safety. This combination is particularly useful at various GLP-1 injection sites where fat thickness varies.
Rotate injection sites systematically
Injecting in the same spot repeatedly causes several problems. The subcutaneous tissue can develop localized changes that alter absorption. Scar tissue may form, creating harder areas where it is more difficult to distinguish fat from muscle. And repeated trauma to the same area increases inflammation and discomfort.
Establish a rotation pattern. Many people find it helpful to divide their abdomen into quadrants and rotate through them weekly. Others alternate between abdomen and thigh. Whatever system you choose, the key is consistency. Always move to a different spot within your chosen area, maintaining at least 1 to 2 inches of separation from your previous injection site.
Abdominal injection techniques and rotation strategies apply equally to semaglutide and other subcutaneous GLP-1 medications.
Complete injection technique: step by step
Getting your injection technique right eliminates nearly all risk of accidental muscle injection. This section walks through the complete process, from preparation through post-injection care. Whether you use a pre-filled pen or a syringe, the fundamentals remain the same.
Before the injection
Let the medication reach room temperature. Cold semaglutide can cause stinging, tissue irritation, and increased discomfort that makes it harder to distinguish between normal injection sensation and accidental muscle penetration. Remove the pen or vial from the refrigerator 15 to 30 minutes before your injection. Understanding proper semaglutide storage is essential. Never freeze semaglutide, and keep it within the recommended temperature range.
Wash your hands thoroughly with soap and water.
Clean the injection site with an alcohol swab. Let the alcohol dry completely before injecting. Injecting through wet alcohol increases stinging.
If using a vial, reconstitute properly according to the concentration specified. Use the correct amount of bacteriostatic water for your vial size. Check the mixing chart to confirm your ratios.
During the injection
Choose your injection site. The abdomen, at least 2 inches from the navel, is preferred for most people. Check that the area is free from bruises, scars, lumps, or skin abnormalities.
Pinch the skin if your needle is longer than 4mm or if you have less subcutaneous fat in the chosen area.
Insert the needle smoothly at the appropriate angle. A 90-degree angle for most people with adequate fat. A 45-degree angle for leaner individuals or when using longer needles. Do not jab or push aggressively. Smooth, steady pressure gets the needle through the skin with less tissue trauma.
Inject the medication slowly. Rushing the injection increases pressure at the needle tip and can push the medication deeper than intended. A slow, steady push on the plunger gives the medication time to disperse into the subcutaneous tissue.
Hold the needle in place. For pen injections, hold for at least 6 seconds (Ozempic) or until you hear or feel the second click (Wegovy). For syringe injections, hold for 5 to 10 seconds after depressing the plunger completely. This ensures the full dose is delivered and prevents medication from leaking back out through the needle track.
Remove the needle at the same angle you inserted it. Do not twist or angle the needle during removal.
After the injection
Apply gentle pressure to the site with clean gauze or your finger for 10 to 20 seconds. Do not rub. Rubbing spreads blood under the skin and can worsen bruising.
Dispose of the needle safely. Never recap a used needle. Use a sharps container.
Note the injection site in a log or on your body map so you remember to rotate to a different spot next time.
Special considerations for lean individuals
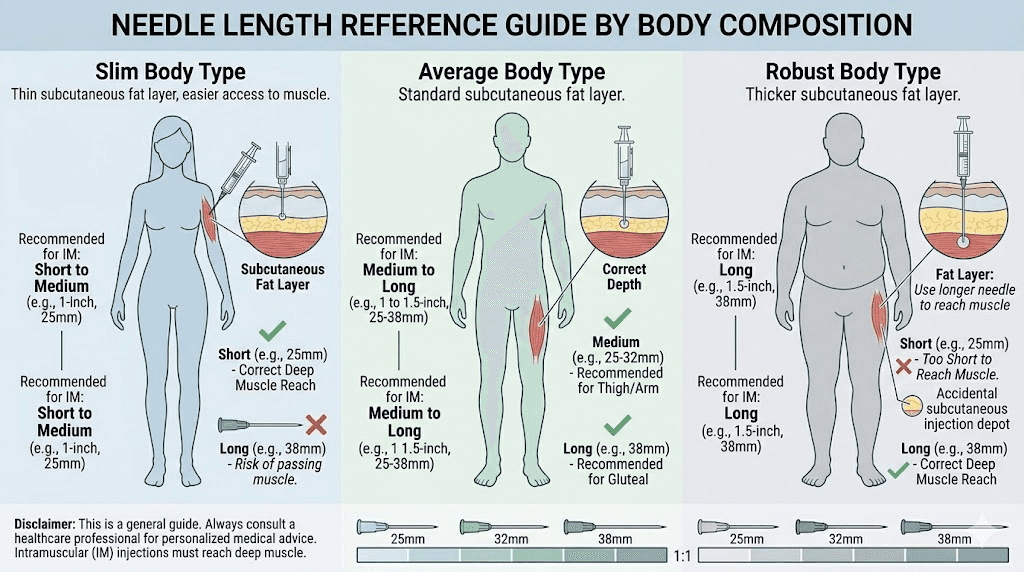
If you have lower body fat, the risk of accidental muscle injection increases significantly. This section is particularly important for men with athletic builds, people who have lost substantial weight on their semaglutide program, and anyone with a BMI under 25 who is using semaglutide for blood sugar management rather than weight loss.
Why lean individuals face higher risk
The math is simple. Thinner subcutaneous fat layer plus same needle length equals higher probability of reaching muscle. A person with 8 millimeters of subcutaneous fat in their thigh is one needle length away from muscle. Someone with 20 millimeters of fat has much more margin for error.
Men are generally at higher risk than women because they carry less subcutaneous fat and more lean mass at equivalent body weights. The average subcutaneous fat thickness difference between men and women is approximately 5 millimeters, which is significant when you are working with 4mm to 8mm needles.
Technique modifications for lean body types
Always use the shortest effective needle. For pen injections, the standard 4mm NovoFine needles are almost always sufficient. For syringe injections, opt for 6mm needles rather than 8mm or longer.
Always pinch the skin. For lean individuals, the skin pinch is not optional. It is essential. Grasp a generous fold of tissue at your injection site before inserting the needle. This lift provides critical separation between the needle tip and the muscle layer.
Prefer the abdomen. Even in lean individuals, the abdomen typically retains more subcutaneous fat than the thigh or arm. If your body fat is low enough that thigh injections feel like they are hitting muscle, switch to abdominal injections exclusively.
Consider a 45-degree angle. Reducing the injection angle from 90 degrees to 45 degrees effectively shortens the penetration depth. For a 6mm needle, a 45-degree angle reduces the effective depth to roughly 4mm. Combined with a skin pinch, this provides excellent subcutaneous access even in very lean individuals.
These same principles apply to other injectable peptides as well. People using tirzepatide, retatrutide, or other peptide injections face the same anatomical considerations.
Common injection mistakes beyond hitting muscle
Accidental muscle injection is just one of several technique errors that can affect your semaglutide experience. Understanding the full range of common mistakes helps you refine your approach and get the most from each dose.
Injecting too shallow (intradermal injection)
The opposite problem of going too deep is not going deep enough. An intradermal injection places the medication in the skin itself, between the epidermis and the subcutaneous fat layer. This happens when the needle barely breaks the surface, often because of excessive fear of going too deep.
Signs of intradermal injection include a visible blister or raised welt at the injection site, significant stinging or burning during injection, poor absorption leading to reduced effectiveness, and visible leaking of medication from the injection site. If this happens consistently, you may find yourself not losing weight on semaglutide despite proper dosing.
Not rotating injection sites
Repeated injections in the same location can cause lipohypertrophy, a condition where fatty tissue thickens and hardens at the injection site. These thickened areas absorb medication unpredictably, leading to inconsistent blood levels and suboptimal results. Always rotate your injection sites.
Injecting into scar tissue or abnormal skin
Scars, stretch marks, and areas of skin with tattoos or visible abnormalities should be avoided. These areas may have altered tissue composition that affects absorption. They can also be more painful and more prone to injection site reactions.
Injecting cold medication
Injecting semaglutide straight from the refrigerator causes increased stinging, more tissue irritation, and greater likelihood of an exaggerated pain response that makes it difficult to assess whether you reached the correct tissue depth. Always let your medication warm to room temperature first. Just make sure not to leave it out too long.
Using a needle more than once
Reusing needles increases infection risk, but it also affects injection comfort and accuracy. Used needles become dull, develop microscopic barbs on the tip, and require more force to penetrate tissue. That extra force can push the needle deeper than intended, increasing the risk of muscle penetration. Fresh needles are sharper, smoother, and more predictable.
Rushing the injection
Speed creates problems at every stage. Rushing the insertion increases pain and reduces control over depth. Rushing the medication delivery increases pressure at the depot site. And pulling the needle out too quickly after injection can cause medication to leak back through the needle track, reducing the effective dose. Take your time. A calm, controlled injection takes 30 seconds. That half-minute investment prevents a week of uncertainty.
The role of injection technique in semaglutide effectiveness
Many people focus exclusively on dose amount when thinking about semaglutide effectiveness. They track their units and milligrams precisely. They follow the dosage charts meticulously. And yet, inconsistent injection technique can undermine all that precision.
Injection technique determines absorption consistency. Absorption consistency determines blood level stability. Blood level stability determines how effectively semaglutide suppresses appetite, controls blood sugar, and drives weight loss throughout the entire dosing period. The chain is direct and unforgiving.
Consistency matters more than perfection
One accidental muscle injection will not derail your progress. But chronically inconsistent technique can create a pattern of variable absorption that mimics dose inadequacy or treatment resistance. If you find yourself wondering why semaglutide is not working, injection technique deserves a hard look before assuming the medication has stopped being effective.
Think about it this way. If half your injections go into fat and half go into muscle, you are essentially taking two different medications. The subcutaneous doses give you steady, week-long coverage. The intramuscular doses give you faster but shorter-acting peaks. Your body never settles into a consistent response pattern, and your results suffer accordingly.
Technique and the dose escalation process
The standard semaglutide titration schedule starts at a low dose and increases every four weeks. This gradual escalation allows your body to adjust to the medication and helps identify the dose that balances effectiveness with tolerable side effects. But the titration assumes consistent subcutaneous absorption at each dose level.
If your injection technique varies, you might experience side effects at a lower dose that are actually caused by accidental intramuscular injection rather than the dose itself being too high. This could lead to unnecessary concern about dose tolerance or premature decisions about dose adjustments.
Conversely, inconsistent subcutaneous delivery might make a dose seem less effective than it actually is, potentially leading to premature dose increases. Nailing your technique first, then assessing dose adequacy, is the logical approach. The timing of your injection matters too, but technique matters more.
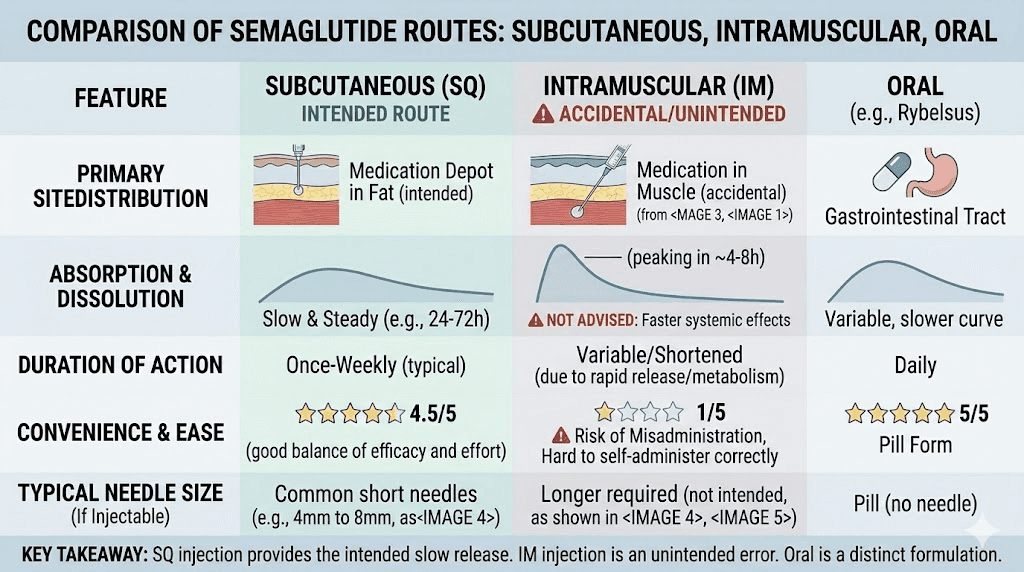
Comparing injection routes: subcutaneous, intramuscular, and other options
Semaglutide is available in multiple formulations, each designed for a specific delivery route. Understanding how these routes differ helps contextualize why subcutaneous injection is the standard for the injectable form and what alternatives exist for people who struggle with injections.
Subcutaneous injection (standard)
This is the gold standard for injectable semaglutide. Brands like Ozempic and Wegovy, plus compounded formulations, are all designed for this route. Benefits include slow, controlled absorption, predictable pharmacokinetics, once-weekly dosing, and minimal injection site discomfort with proper technique.
Intramuscular injection (accidental)
Not an approved route. Faster absorption, higher peak concentrations, potentially shorter duration of action. The medication still works, but the pharmacokinetic profile differs from what was studied in clinical trials. The only reason semaglutide ends up in muscle is technique error.
Oral semaglutide
For people who want to avoid injections entirely, oral semaglutide options exist. Rybelsus is the FDA-approved oral formulation, taken daily rather than weekly. The oral route has different bioavailability and requires specific dosing instructions, including taking the tablet on an empty stomach with a small amount of water and waiting 30 minutes before eating or drinking anything else.
Sublingual semaglutide formulations have also emerged as compounded alternatives, dissolving under the tongue for direct absorption through the oral mucosa. The comparison between injectable and oral peptides involves trade-offs in convenience, absorption, and dosing flexibility.
Why injection remains preferred despite the learning curve
Subcutaneous injection provides the most reliable, consistent drug delivery of any semaglutide formulation. The once-weekly dosing is more convenient than daily oral formulations. And the bioavailability, the percentage of the dose that actually reaches your bloodstream, is significantly higher with injection than with oral administration.
The injection learning curve is real but short. Most people develop confident, consistent technique within 3 to 4 injections. The initial anxiety about self-injection fades quickly, especially once you experience how minor the physical sensation actually is with proper technique. Your first week on semaglutide may feel uncertain, but by week four, injection becomes routine.
Understanding semaglutide formulations and injection considerations
Not all semaglutide products are identical in terms of injection technique requirements. The formulation you use, whether it is a brand-name pen, compounded vial, or specialty blend, affects your injection approach and your risk of accidental muscle injection.
Pre-filled pen devices (Ozempic, Wegovy)
Pre-filled pens are designed to minimize injection errors. The built-in 4mm pen needles are specifically sized for subcutaneous delivery across all body types. The pen mechanism controls injection speed and volume. And the device itself limits how much control, or lack of control, the user has over depth and angle.
The risk of accidental muscle injection with a pre-filled pen is very low. The 4mm needle simply does not reach muscle tissue in the vast majority of anatomical scenarios. Even in very lean individuals, the combination of skin thickness and subcutaneous fat typically exceeds 4mm at approved injection sites.
Compounded semaglutide vials
Compounded semaglutide requires users to reconstitute the medication and draw it into syringes themselves. This introduces several additional variables. Needle length depends on the syringe used. Injection depth depends on the user. And proper mixing ratios determine concentration accuracy.
If you use compounded semaglutide, paying extra attention to needle selection and injection technique is critical. The 5mg dosage chart and 10mg dosage chart provide volume guidance, but proper delivery technique is equally important.
Semaglutide combination blends
Some compounded formulations combine semaglutide with other ingredients like vitamin B12, glycine, methylcobalamin, or L-carnitine. These blended formulations follow the same injection technique principles as standard semaglutide. The addition of other compounds does not change the subcutaneous targeting or the risks associated with accidental muscle injection.
The injection volume may differ with combination products, which can affect the feel of the injection and the size of the subcutaneous depot. Follow the specific reconstitution and dosing instructions for your particular formulation.
Accidental muscle injection versus other semaglutide concerns
It helps to put accidental muscle injection in perspective by comparing it to other common semaglutide concerns. Many of the things people worry most about are significantly less consequential than they believe.
Accidental muscle injection versus missed dose
A missed dose is actually more disruptive to your treatment than an accidental muscle injection. With a muscle injection, you still received your full dose, just through a different tissue route. With a missed dose, you received nothing. Your blood levels drop, appetite suppression fades, and you lose an entire week of treatment effect.
If you are deciding between potentially imperfect injection technique and skipping a dose, always inject. A less-than-ideal injection beats no injection every time.
Accidental muscle injection versus expired semaglutide
Using expired semaglutide or semaglutide that has been improperly stored is a larger concern than injection route. Degraded semaglutide may have reduced potency, meaning you could be getting less medication than your dose specifies regardless of how perfectly you inject it. Proper shelf life awareness and storage practices affect treatment efficacy more than the occasional injection depth error.
Accidental muscle injection versus wrong dose
Drawing up the wrong volume of compounded semaglutide, resulting in too much or too little medication, has a more direct impact on treatment outcomes than injection route. Ensuring accurate dosing with the correct unit-to-milligram conversion is fundamentally more important than whether the correctly measured dose enters fat or muscle.
Accidental muscle injection versus stopping treatment
Some people become so anxious about injection technique that they consider stopping semaglutide altogether. Stopping semaglutide comes with its own set of consequences, including appetite rebound and potential weight regain. An imperfect injection that still delivers the medication is overwhelmingly preferable to abandoning treatment because of injection anxiety.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers comprehensive injection guides, dosing calculators, and expert resources that remove the guesswork from self-administration.
How other GLP-1 medications compare for injection technique
Semaglutide is not the only GLP-1 receptor agonist that requires subcutaneous injection. Understanding how related medications handle the same injection technique challenges provides useful context and shows that these considerations are universal across the class.
Tirzepatide injection technique
Tirzepatide follows the same subcutaneous injection principles as semaglutide. The injection sites are identical: abdomen, thigh, and upper arm. The needle recommendations are similar. And the risk of accidental muscle injection carries the same consequences, faster absorption and potentially amplified side effects.
People who have experienced injection site reactions with tirzepatide report similar patterns to semaglutide. Redness, itching, and localized swelling can occur with either medication, and these reactions are more common when the injection reaches muscle tissue or when technique is inconsistent.
Retatrutide injection technique
The triple agonist retatrutide is also administered subcutaneously. The injection site selection and technique principles mirror those for semaglutide and tirzepatide. As this newer medication gains wider use, proper injection technique remains equally critical for optimal absorption and efficacy.
The universal principle
Every subcutaneous injectable medication, whether it is a peptide injection, insulin, or a GLP-1 receptor agonist, relies on the same anatomical targeting. The fat layer is the destination. The muscle is the boundary. And technique is the bridge between good intentions and good outcomes.
Understanding proper injection methods for one medication transfers directly to others. If you master semaglutide injection technique, you already know how to properly inject tirzepatide, retatrutide, or any other subcutaneous medication. The injection pen systems and reconstitution processes may vary, but the fundamental technique stays the same.
Building long-term injection confidence
Injection anxiety is real. It affects people at every stage of treatment, from those preparing for their very first dose to experienced users who suddenly wonder if they have been doing it wrong all along. Building confidence requires knowledge, practice, and a realistic perspective on the risks involved.
The learning curve is shorter than you think
Most people find that injection anxiety peaks before the first injection and drops sharply after it. By the third or fourth injection, the process feels familiar. By the eighth or tenth, it becomes automatic. The physical sensation of a properly administered subcutaneous injection is genuinely minimal, often less than a mosquito bite.
If you are still building confidence with your technique, consider watching your injection area rather than looking away. Seeing the needle enter the skin, watching the plunger depress, and observing the medication delivery gives your brain the visual feedback it needs to build a reliable technique pattern.
Practice with saline
Some healthcare providers recommend practicing injection technique with sterile saline before injecting your first dose of semaglutide. This allows you to experience the physical sensation of subcutaneous injection, practice the skin pinch, and get comfortable with needle insertion depth without the pressure of "wasting" medication. Check with your provider about whether a practice session makes sense for your situation.
When to seek hands-on instruction
If you continue to struggle with injection technique or repeatedly suspect you are hitting muscle, ask your healthcare provider or a nurse for a supervised injection session. Having someone watch your technique and provide real-time corrections is far more effective than reading guides or watching videos. Many pharmacies also offer injection training for patients using self-administered medications.
SeekPeptides members get access to comprehensive injection technique guides, including visual step-by-step walkthroughs and troubleshooting resources designed specifically for peptide self-administration.
Traveling with semaglutide: injection challenges on the go
Injection technique challenges multiply when you are away from the comfort of your bathroom at home. Traveling with semaglutide introduces variables like unfamiliar environments, limited privacy, temperature control concerns, and the general stress of being out of your routine.
When injecting in unfamiliar settings, the risk of accidental muscle injection can increase simply because you are less relaxed. Tension in your body, including at the injection site, can make the subcutaneous tissue feel firmer and more muscle-like. Take an extra moment to relax the injection area. Consciously let the muscles underneath go slack before pinching the skin and inserting the needle.
Proper storage during travel matters too. Travel storage guidelines for injectable medications help ensure your semaglutide maintains potency throughout your trip. A degraded medication combined with imperfect travel injection technique compounds the problem.
The connection between injection technique and side effects
Many people who report troublesome semaglutide side effects never consider that their injection technique might be a contributing factor. The relationship between how you inject and what you experience afterward is more direct than most users realize.
Side effects that may be technique-related
If your bloating or nausea seems to vary significantly from week to week despite being on the same dose, inconsistent injection technique is a plausible explanation. Weeks where the injection lands properly in subcutaneous tissue produce one absorption pattern. Weeks where it hits muscle produce another. The resulting blood level fluctuations manifest as variable side effects.
Similarly, if you experience occasional bouts of more intense fatigue or headaches on some weeks but not others, the explanation might be absorption variation from inconsistent injection depth rather than some mysterious metabolic change.
Side effects unrelated to injection technique
Not everything is about technique. Many semaglutide side effects, including insomnia, menstrual changes, changes in sex drive, and hair thinning, are systemic effects that occur regardless of how perfectly you inject. These are related to the medication mechanism itself, not the delivery route.
The key is distinguishing between effects that vary with your injection technique and effects that remain consistent regardless. Variable effects point to technique. Consistent effects point to the medication itself.
What your healthcare provider needs to know
If you accidentally inject semaglutide into muscle, you should know what information your healthcare provider will find most useful if you choose to report the incident.
Tell them the exact injection site. Tell them the needle length and gauge you used. Describe whether you pinched the skin and what angle you inserted the needle at. Report any unusual pain during or after the injection, any changes in side effects compared to your previous injections, and how long any injection site symptoms lasted.
This information helps your provider assess whether your technique needs correction and whether any dose adjustments are warranted. It also helps them distinguish between a one-time accident and a pattern of incorrect technique that might be affecting your treatment outcomes.
Most providers will reassure you that a single accidental intramuscular injection is not harmful. They may review your injection technique with you or suggest a supervised injection at your next appointment. Some may recommend switching to a shorter needle or adjusting your injection site selection.
Diet and lifestyle factors that support optimal semaglutide absorption
While injection technique is the primary determinant of absorption, certain dietary and lifestyle factors can influence how well semaglutide works in your body, regardless of whether the occasional injection lands in fat or muscle.
Eating the right foods on semaglutide supports the medication effectiveness and helps manage side effects. Following a structured semaglutide diet plan that emphasizes lean protein, fiber-rich vegetables, and adequate hydration creates the metabolic environment where semaglutide works best.
Knowing which foods to avoid on semaglutide is equally important. High-fat and greasy meals can amplify GI side effects, which may already be heightened after an accidental muscle injection. A comprehensive food list for semaglutide users takes the guesswork out of meal planning during treatment.
Some people also pair semaglutide with supplements like berberine to support metabolic outcomes. Others use semaglutide with niacinamide combinations. These complementary approaches can enhance results regardless of occasional technique variations.
Weight loss on semaglutide happens even without exercise, but combining the medication with physical activity produces better outcomes. The caveat for our topic: exercise increases blood flow to muscles. If you work out the muscles near your injection site shortly after injecting, and the injection happened to land in muscle, the increased blood flow could further accelerate absorption. Avoid intense exercise at the injection site area for at least a few hours after your weekly dose.
When to seek emergency medical attention
An accidental intramuscular semaglutide injection is almost never a medical emergency. But certain symptoms, whether related to the injection route or not, warrant immediate medical attention.
Seek emergency care if you experience signs of a severe allergic reaction including swelling of the face, lips, tongue, or throat, difficulty breathing, or widespread hives. These reactions are extremely rare with semaglutide but can occur with any injectable medication regardless of injection depth.
Contact your provider urgently if you experience severe, unrelenting abdominal pain, especially if accompanied by nausea and vomiting. While GI side effects are common with semaglutide, severe abdominal pain could indicate pancreatitis, a rare but serious side effect that requires medical evaluation.
Signs of infection at the injection site, including increasing redness, warmth, swelling, pus, or red streaking radiating from the injection site, also warrant prompt medical attention. Infections are more common with poor injection technique, reused needles, or inadequate site cleaning, and can occur whether the injection entered fat or muscle.
Hypoglycemia, dangerously low blood sugar, is a concern primarily for people taking semaglutide alongside other diabetes medications like insulin or sulfonylureas. The faster absorption from an intramuscular injection could theoretically increase the risk of blood sugar dropping too low. Monitor blood sugar more frequently than usual for 24 to 48 hours after a suspected intramuscular injection if you take additional diabetes medications.
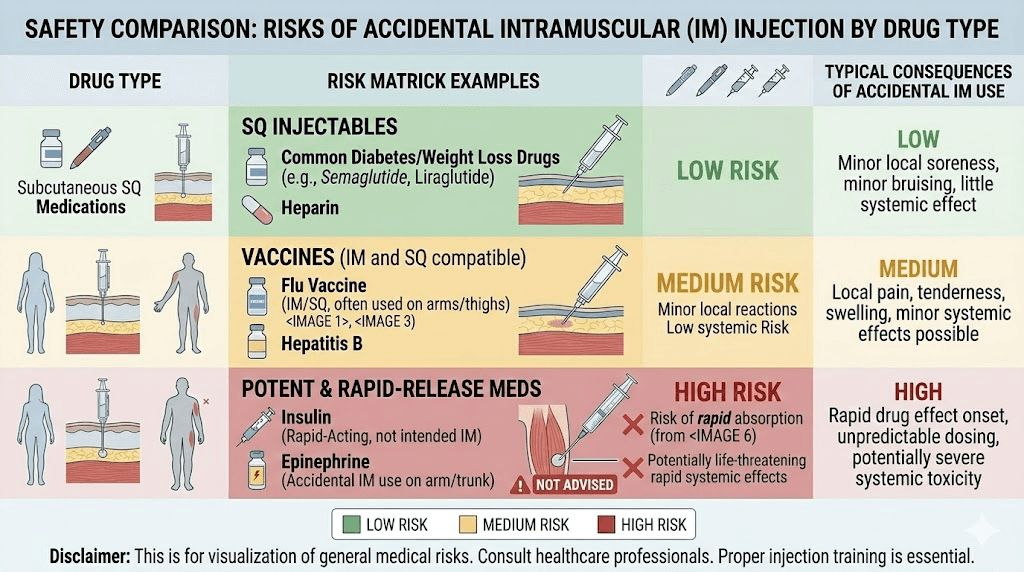
Comparing semaglutide to other medications commonly injected incorrectly
Semaglutide is not unique in being accidentally injected into the wrong tissue layer. The same mistake happens with insulin, heparin, and various other self-administered injectable medications. Looking at how these situations compare provides helpful perspective.
Insulin injected intramuscularly absorbs 50 percent faster than subcutaneous insulin, which can cause significant hypoglycemia. This is a well-documented clinical problem because the consequences of faster insulin absorption are more immediately dangerous than faster semaglutide absorption. Semaglutide, by contrast, does not carry the same acute hypoglycemia risk when injected too deeply, unless combined with other blood sugar-lowering medications.
The clinical experience with accidental intramuscular insulin injection provides indirect evidence about what happens when peptide medications enter muscle. The fundamental pharmacokinetic principle is consistent: muscle injection means faster absorption, higher peak levels, and shorter duration. The severity of the consequences depends on the specific medication and its therapeutic window.
For semaglutide, that therapeutic window is relatively wide. The difference between slightly higher and slightly lower blood levels of semaglutide produces noticeable but not dangerous effects. This is why accidental muscle injection, while not ideal, is not the crisis that some online forums make it out to be.
Long-term injection technique tips from experienced users
People who have been self-injecting semaglutide or similar medications for months or years develop practical insights that supplement the clinical guidelines. These tips come from real-world experience.
Find your golden zone. Most experienced users identify one or two areas on their body where injections consistently feel right, absorb well, and produce minimal discomfort. For many, it is the lower abdomen, 2 to 4 inches below the navel and slightly to either side. This area typically has reliable subcutaneous depth even as body composition changes.
Inject at the same time each week. Consistency in timing helps you build a routine that reduces the chance of rushing or being distracted during the injection. Many people choose a quiet time on the same day each week. The best time of day is whenever you can give the process your full, unhurried attention.
Stand or sit in the same position. Body position affects how your tissue layers distribute. If you inject while lying down one week and standing the next, the subcutaneous fat layer at your injection site may shift position relative to the underlying muscle. Consistency in posture promotes consistency in injection depth.
Feel before you inject. Before cleaning the site and pinching the skin, palpate the area with your fingers. Feel for the softness of subcutaneous fat versus the firmness of underlying muscle. If the area feels too firm or you can easily feel muscle fibers, move to a spot with more padding.
Trust the process. After dozens of successful injections, the occasional questionable one is statistically inevitable. Do not let one uncertain injection spiral into weeks of second-guessing. Your technique is probably fine. The fact that you are thinking about it means you care enough to do it right.
Semaglutide injection and weight loss progress
The reason most people are injecting semaglutide in the first place is weight loss. And injection technique, while important, is just one piece of a much larger puzzle.
Your weight loss trajectory on semaglutide depends on dose, diet, activity level, metabolic factors, sleep quality, stress management, and medication adherence, in addition to injection technique. An occasional accidental muscle injection will not measurably slow your first month results or long-term progress.
What might slow progress is the anxiety loop that follows a suspected bad injection. Worrying about technique, obsessively analyzing every sensation, skipping doses out of fear, these behavioral responses to injection anxiety cause more harm than the accidental muscle injection itself.
Focus on what you can control. Get properly set up with semaglutide. Follow a supportive eating plan. Use the dosage calculator to confirm your units are correct. Keep your medication properly stored. And inject with the best technique you can manage, knowing that perfection is not required for excellent results.
SeekPeptides provides its members with evidence-based protocols, personalized guidance, and a community of thousands who have navigated these exact injection concerns on their way to successful outcomes.
Other semaglutide accidents and how to handle them
Since we are talking about injection mistakes, it is worth addressing other common semaglutide accidents that generate questions and anxiety.
Accidentally took expired semaglutide
If you accidentally used expired semaglutide, the medication is unlikely to be harmful, but it may have reduced potency. Expired semaglutide may not suppress appetite or control blood sugar as effectively as fresh medication. The risk is not danger but diminished effectiveness. Replace expired medication and continue your regular schedule.
Semaglutide left out of the fridge
Temperature excursions happen. If your semaglutide was left out overnight or exposed to warmth, the impact depends on the duration and temperature. Most semaglutide formulations tolerate room temperature for limited periods, but prolonged heat exposure degrades the peptide. Check your specific product labeling for temperature tolerance guidelines, and understand expiration rules for opened products.
Unusual semaglutide appearance
If your semaglutide looks different than expected, whether the color has changed or you are wondering why your semaglutide is red, do not inject it until you have verified the cause. Discoloration can indicate degradation, contamination, or simply a different formulation than you are used to. When in doubt, contact your pharmacy.
Frequently asked questions
Is accidentally injecting semaglutide into muscle dangerous?
No. While semaglutide is designed for subcutaneous injection, an accidental intramuscular injection is not dangerous. The medication will still be absorbed and will still work. The main differences are faster absorption, potentially more intense temporary side effects, and increased pain at the injection site. Continue your regular dosing schedule and focus on correcting your injection technique for future doses.
Should I take another dose if I injected semaglutide into muscle?
Absolutely not. You received your full dose of semaglutide regardless of which tissue layer it entered. Taking a second dose creates an overdose scenario with significantly amplified side effects including severe nausea and GI distress. Continue with your next scheduled dose at the normal time.
How do I know if I injected semaglutide into muscle or fat?
Signs of intramuscular injection include deeper, aching pain at the injection site, more soreness than usual lasting hours to days, bruising, faster onset of appetite suppression, and more intense initial side effects. Subcutaneous injections typically cause minimal pain, little to no bruising, and gradual onset of effects.
What needle length prevents accidental muscle injection?
For pen injections, the standard 4mm pen needles are safe for virtually all body types. For syringe injections with compounded semaglutide, 6mm needles are recommended for most people. Needles longer than 8mm increase the risk of reaching muscle, especially in leaner individuals and at injection sites with thinner subcutaneous fat.
Can accidental intramuscular injection affect my weight loss results?
A single accidental intramuscular injection will not meaningfully affect your overall weight loss trajectory. However, consistently hitting muscle due to poor technique could lead to irregular absorption patterns and suboptimal results over time. Correcting your technique ensures the most reliable outcomes.
Is it normal for semaglutide injections to hurt?
Mild stinging during injection is normal. Significant pain suggests the needle may be reaching muscle tissue or hitting a nerve. Letting the medication reach room temperature before injecting, using fresh needles, cleaning the site and letting alcohol dry completely, and using proper pinch technique all reduce injection discomfort significantly.
Does the injection site affect how well semaglutide works?
Absorption rates can vary slightly between injection sites. The abdomen generally provides the most consistent and reliable absorption for GLP-1 injections. The thigh and upper arm are acceptable alternatives. Rotating between sites prevents tissue changes that can alter absorption over time.
What should I do if I get a lump after injecting semaglutide?
Small lumps at the injection site are common and usually resolve within a few days as the medication absorbs. They can occur with both subcutaneous and intramuscular injections. If a lump persists beyond a week, grows in size, becomes increasingly painful, or shows signs of infection, contact your healthcare provider. Review the injection site reaction guide for detailed management advice.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based injection guides, dosing calculators, personalized protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your injections stay subcutaneous, your technique stay consistent, and your results stay on track.