Feb 21, 2026
You are wasting tirzepatide. Maybe not a lot. Maybe just a fraction of each dose. But if the amount of bacteriostatic water in your 10mg vial is wrong, every single injection you draw is either too concentrated to measure accurately or too diluted to last through your protocol. And with tirzepatide costing what it does, even small measurement errors add up fast.
The frustrating part is that most guides skip the details. They tell you to "add bacteriostatic water" without explaining why the amount matters, how it changes your syringe readings, or what happens when you pick the wrong concentration for your dosing schedule. You end up guessing. And guessing with a peptide this powerful is not something anyone should do.
This guide covers everything about mixing bacteriostatic water with a 10mg tirzepatide vial. Not the vague "add some water" advice. The exact amounts, the math behind each concentration option, complete dosing charts for every dose level in units, and a step-by-step reconstitution process that protects the peptide from degradation. Whether you are on a starting dose of 2.5mg or working up to 10mg per week, the amount of water you add to that vial determines how easy or difficult accurate dosing becomes. And accuracy, when it comes to tirzepatide dosing for weight loss, is everything.
The direct answer: how much bacteriostatic water for a 10mg tirzepatide vial
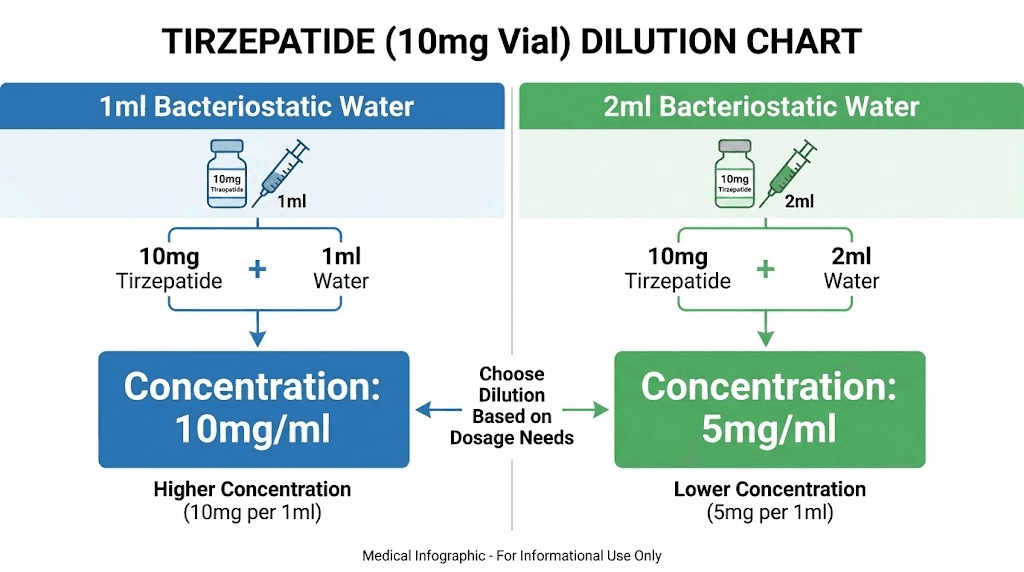
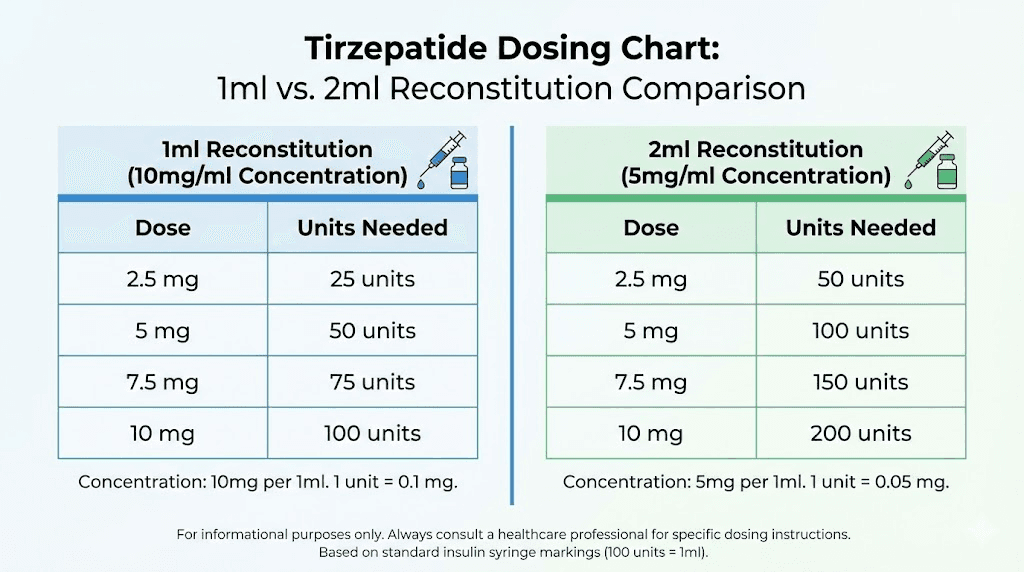
For a 10mg tirzepatide vial, the two most common reconstitution volumes are 1ml and 2ml of bacteriostatic water.
Adding 1ml creates a concentration of 10mg/ml. Adding 2ml creates a concentration of 5mg/ml. Both work. Both are safe. The right choice depends on your dosing protocol and the type of syringe you are using.
Most researchers prefer 2ml of bacteriostatic water for a 10mg vial. This produces a 5mg/ml concentration that is easier to measure accurately on a standard U-100 insulin syringe, especially at lower starting doses like 2.5mg. The 1ml option works well for experienced users who need smaller injection volumes or are on higher doses.
Here is the quick reference:
Bacteriostatic water added | Concentration | 2.5mg dose in units | 5mg dose in units | Best for |
|---|---|---|---|---|
1ml | 10mg/ml | 25 units | 50 units | Higher doses, smaller volumes |
2ml | 5mg/ml | 50 units | 100 units | Starting doses, easier measuring |
That is the short answer. But the amount of water you choose has consequences that ripple through your entire protocol. The sections below explain exactly why concentration matters, how to reconstitute properly, and how to draw accurate doses at every level from 2.5mg through 10mg.
Why the amount of bacteriostatic water changes everything
The amount of bacteriostatic water you add does not change the total amount of tirzepatide in the vial. A 10mg vial contains 10mg regardless of whether you add 1ml, 2ml, or even 3ml of water. What changes is the concentration, and concentration determines how many units you draw on your syringe for each dose.
Think of it like dissolving sugar in water. One teaspoon in a small cup creates very sweet water. The same teaspoon in a large jug creates barely sweet water. Same amount of sugar. Different concentration. Different experience.
How concentration works (the basic math)
The formula is simple:
Concentration = Total peptide (mg) / Total water (ml)
For a 10mg vial:
10mg / 1ml = 10mg/ml
10mg / 2ml = 5mg/ml
10mg / 3ml = 3.33mg/ml
On a U-100 insulin syringe, 100 units equals 1ml. So each unit on the syringe equals 0.01ml. Multiply the concentration by 0.01, and you get the amount of tirzepatide per unit on the syringe. This is the number you need to calculate peptide dosages correctly.
At 10mg/ml: each unit contains 0.1mg (100mcg) of tirzepatide.
At 5mg/ml: each unit contains 0.05mg (50mcg) of tirzepatide.
This matters more than most people realize. At the 10mg/ml concentration, the difference between 25 units and 26 units is 0.1mg, a 4% dosing error on a 2.5mg dose. At the 5mg/ml concentration, the same one-unit difference is only 0.05mg, a 2% error. When you are working with a potent GLP-1 receptor agonist like tirzepatide, those percentage differences in accuracy matter for consistent results. The peptide reconstitution calculator on SeekPeptides can help you verify these numbers before you mix.
Why two people can get different results from the same vial
This is the problem nobody talks about. Two researchers buy the same 10mg tirzepatide vial from the same source. One adds 1ml of bacteriostatic water. The other adds 2ml. Their syringes show different unit counts for identical doses. If either one misreads their dosage chart in units, they end up taking substantially more or less than intended.
Under-dosing means wasted weeks waiting for results that should have arrived sooner. Over-dosing means unnecessary side effects, potentially severe ones like nausea, vomiting, or the kind of gastrointestinal issues that make people quit their protocol entirely. Neither outcome is acceptable when the solution is simply getting the water amount right from the start.
The concentration you choose also affects how long the vial lasts. With 2ml of water, a 10mg vial at 2.5mg per week lasts exactly four weeks, perfectly within the 28-day stability window for reconstituted tirzepatide. But at higher doses like 5mg per week, that same vial lasts only two weeks, meaning nearly half the reconstituted solution never gets used before the 28-day limit if you are only at the start of your protocol. Planning matters.
Option 1: adding 1ml of bacteriostatic water to 10mg tirzepatide
Adding 1ml of bacteriostatic water to your 10mg tirzepatide vial creates a concentration of 10mg/ml. This is the more concentrated option, producing smaller injection volumes for any given dose.
When 1ml makes sense
The 1ml reconstitution works best in specific situations. If you are on a higher dose, say 7.5mg or above, the smaller injection volume means less liquid under the skin. Some people find this more comfortable. Large injection volumes can cause localized reactions, particularly stinging or a raised bump at the injection site.
The 1ml option also makes sense if you have experience with insulin syringes and can confidently read markings at the 25-unit level. A 2.5mg dose at this concentration is exactly 25 units. That is manageable for someone who has been doing subcutaneous injections for a while. But for someone new to peptide injections, the smaller volume means smaller margin for error.
Complete dosing chart at 10mg/ml (1ml of bacteriostatic water)
Desired dose | Volume to draw | Units on insulin syringe | Duration at this dose (10mg vial) |
|---|---|---|---|
1.25mg (microdose) | 0.125ml | 12.5 units | 8 weeks |
2.5mg (starting dose) | 0.25ml | 25 units | 4 weeks |
5mg | 0.50ml | 50 units | 2 weeks |
7.5mg | 0.75ml | 75 units | 1.3 weeks |
10mg | 1.0ml | 100 units | 1 week |
Notice the problem at the 1.25mg microdose level. You need to draw 12.5 units. On most insulin syringes, the markings are at every 2 units (for a 100-unit syringe) or every 1 unit (for a 30-unit syringe). Drawing exactly 12.5 units requires estimating the halfway point between markings. That introduces measurement error. If you are following a microdosing tirzepatide protocol, the 2ml reconstitution gives you much more precise measurements.
Drawbacks of the 1ml approach
Accuracy is the main concern. At 10mg/ml, even a small misread of the syringe changes your dose significantly. Drawing 27 units instead of 25 units means you are taking 2.7mg instead of 2.5mg. Over a full month of weekly injections, that adds up to an extra 0.8mg of tirzepatide you did not intend to take.
The other drawback is vial longevity. At the starting dose of 2.5mg per week, a 10mg vial lasts four weeks. But you only added 1ml of liquid. After four draws of 0.25ml each, you have extracted all 1ml. In practice, some liquid always remains in the vial because the needle and syringe dead space traps a small amount. This means your fourth dose might come up slightly short unless you account for dead-space volume or use a low dead-space syringe.
Option 2: adding 2ml of bacteriostatic water to 10mg tirzepatide
Adding 2ml of bacteriostatic water to a 10mg vial produces a concentration of 5mg/ml. This is the more commonly recommended option, and for good reason.
When 2ml makes sense
Two milliliters is the standard recommendation for most researchers. The 5mg/ml concentration strikes the best balance between accuracy and practicality. Your starting dose of 2.5mg equals 50 units on the syringe, right at the halfway mark. That is easy to read. Easy to draw. Hard to mess up.
This concentration also aligns well with the standard tirzepatide dosing schedule for the early weeks of a protocol. When you are titrating up from 2.5mg to 5mg over the first eight weeks, the 5mg/ml concentration keeps every dose in a comfortable range on the syringe.
If you are newer to peptide reconstitution, the 2ml approach gives you more room for error. A one-unit mistake on the syringe changes your dose by only 0.05mg instead of 0.1mg. That is a meaningful difference in precision, especially when you are still getting used to drawing doses.
Complete dosing chart at 5mg/ml (2ml of bacteriostatic water)
Desired dose | Volume to draw | Units on insulin syringe | Duration at this dose (10mg vial) |
|---|---|---|---|
1.25mg (microdose) | 0.25ml | 25 units | 8 weeks |
2.5mg (starting dose) | 0.50ml | 50 units | 4 weeks |
5mg | 1.0ml | 100 units | 2 weeks |
7.5mg | 1.5ml | 150 units (2 draws) | 1.3 weeks |
10mg | 2.0ml | 200 units (2 draws) | 1 week |
At this concentration, the 7.5mg and 10mg doses require more liquid than a standard 1ml (100-unit) insulin syringe can hold. You would need to draw twice: for example, 75 units plus 75 units for the 7.5mg dose. This is why the 2ml reconstitution works best for the earlier phases of a protocol when doses are lower. For higher doses, the 1ml reconstitution may be more practical.
Why most researchers prefer 2ml
Three reasons keep coming up consistently.
First, accuracy. Fifty units is the center line of a 100-unit syringe. It is the easiest marking to read, and the hardest to get wrong. When your dosage calculations land on clean numbers like 50 or 100 units, you eliminate the guesswork that causes dosing errors.
Second, the four-week alignment. At 2.5mg per week, a 10mg vial with 2ml of water provides exactly four doses. Four weeks. That matches the standard titration period before increasing to 5mg. You use the entire vial, nothing wasted, and then reconstitute a fresh vial for the next dose level.
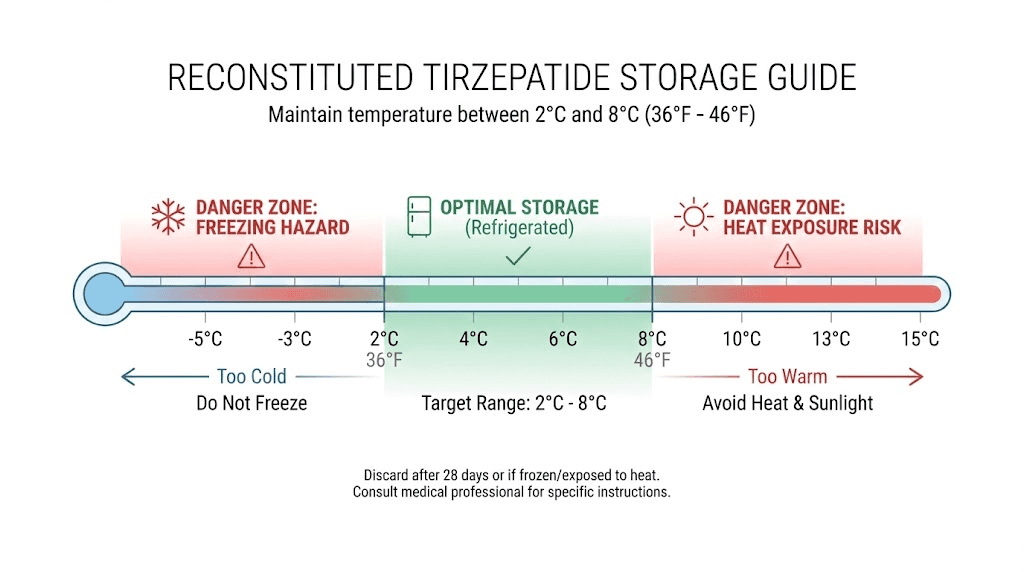
Third, the stability window. Reconstituted tirzepatide remains stable for approximately 28 days when stored properly in the refrigerator. Four weeks of weekly doses at 2.5mg fits perfectly within that window. No scrambling to use up leftover solution before it degrades.
Step-by-step reconstitution guide for 10mg tirzepatide
Reconstitution is not complicated. But it does require following a specific sequence to protect the peptide from damage. Tirzepatide is a delicate molecule. Rough handling, contamination, or improper technique can reduce potency or introduce bacteria into a solution you will be injecting into your body.
What you need before you start
Gather everything first. Do not start the process and then go searching for supplies.
10mg tirzepatide vial (lyophilized powder)
Bacteriostatic water (not sterile water, not saline, not normal water)
Sterile syringe for reconstitution (a 3ml syringe with a needle works well)
Alcohol swabs (70% isopropyl alcohol pads)
U-100 insulin syringes for dosing (29-31 gauge)
Sharps container for disposal
Clean, well-lit workspace
A note on the water: you must use bacteriostatic water, not sterile water for injection. Bacteriostatic water contains 0.9% benzyl alcohol as a preservative, which prevents bacterial growth in a multi-dose vial. Sterile water has no preservative. If you use sterile water, you can only draw from the vial once before contamination becomes a risk. Since a 10mg vial at the starting dose provides four weeks of doses, you need the preservative to keep the solution safe across all four draws. This is explained in more detail in the complete guide to mixing peptides with bacteriostatic water.
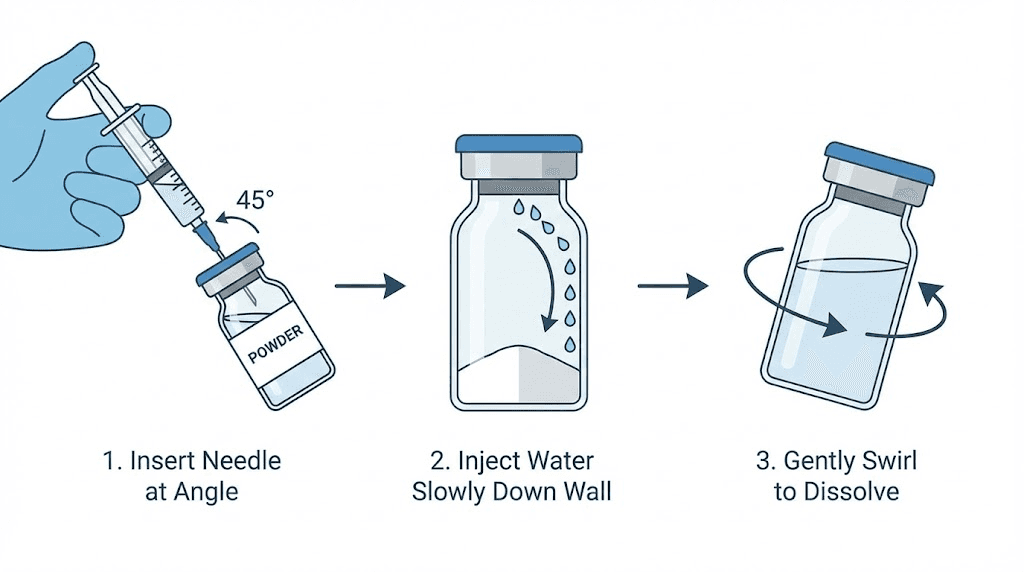
The reconstitution process
Step 1: Wash your hands thoroughly with soap and water. Dry them completely.
Step 2: Clean the rubber stopper on both the tirzepatide vial and the bacteriostatic water vial with alcohol swabs. Let them air dry for 10 to 15 seconds. Do not blow on them.
Step 3: Using the reconstitution syringe, draw your chosen amount of bacteriostatic water. For most people, this is 2ml. For the higher-concentration option, draw 1ml. Verify the amount by holding the syringe at eye level.
Step 4: Insert the needle into the tirzepatide vial through the center of the rubber stopper. Tilt the vial slightly so the needle tip touches the inside wall of the vial, near the glass.
Step 5: Slowly depress the plunger. Let the water trickle down the inside wall of the vial. This is critical. Do not spray the water directly onto the lyophilized powder. Direct force can damage the peptide structure. Let gravity and surface tension do the work. The water should flow down the glass and pool at the bottom around the powder.
Step 6: Remove the syringe. Do not shake the vial. Gently swirl or roll the vial between your palms. Imagine you are trying to warm your hands, not mix a cocktail. The powder should dissolve within 30 to 60 seconds. If small particles remain, set the vial down and wait 2 to 3 minutes. Swirl again gently.
Step 7: Inspect the solution. It should be clear and colorless. If it is cloudy, contains particles that will not dissolve, or looks discolored, do not use it. A properly reconstituted tirzepatide solution looks like plain water.
Step 8: Label the vial with the reconstitution date, the concentration (5mg/ml or 10mg/ml), and the amount of tirzepatide. Store immediately in the refrigerator.
The full reconstitution process with additional visual guidance is covered in the complete tirzepatide reconstitution guide.
What the solution should look like
Clear. Colorless. No particles. No cloudiness.
If you see anything floating in the solution, it means the peptide has not fully dissolved or has degraded. Sometimes a brief waiting period resolves this. But if particles persist after 5 minutes of gentle swirling, the vial may have been damaged by heat exposure, shaking, or age. Do not inject a solution that is not completely clear.
A slight foaming on the surface is normal if you swirled too vigorously. Let the foam settle. It does not indicate a problem with the peptide itself. Just give it a minute and the bubbles will dissipate.
How to draw your dose with an insulin syringe
This is where most mistakes happen. Not during reconstitution, but during the drawing process. Understanding how milliliters translate to syringe units eliminates the confusion.
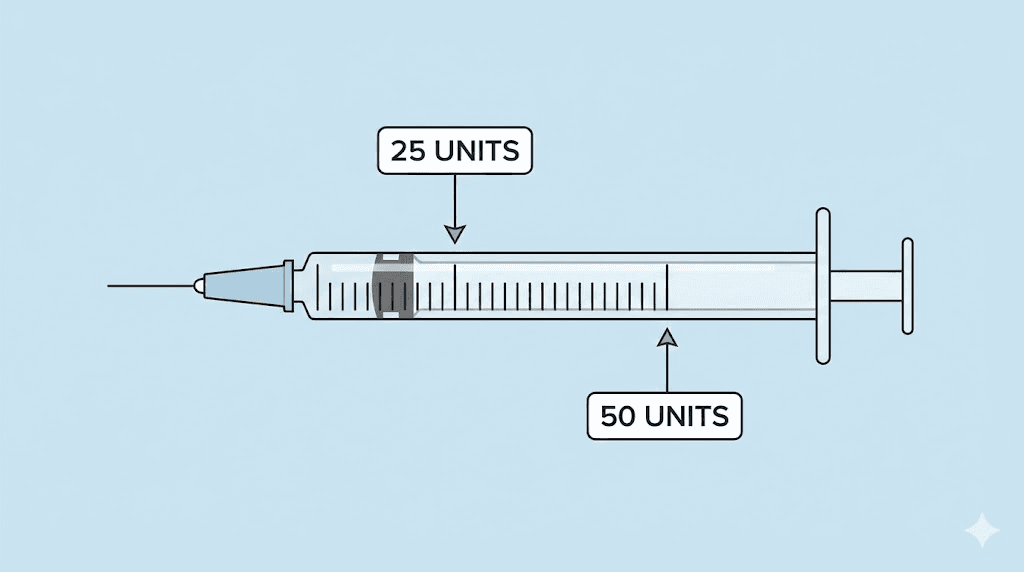
Understanding U-100 insulin syringe markings
A standard U-100 insulin syringe holds 1ml of liquid. It is marked with 100 units. Each unit equals 0.01ml. These syringes come in different sizes: 30-unit (0.3ml), 50-unit (0.5ml), and 100-unit (1.0ml). The markings are designed for insulin, but they work perfectly for measuring reconstituted peptides.
For tirzepatide dosing, 100-unit syringes give you the most flexibility. The syringe markings are spaced farther apart on a 100-unit syringe, making them easier to read. If you are on a very low dose and want maximum precision, a 50-unit or 30-unit syringe provides finer graduations.
The key formula for any concentration:
Units to draw = (Desired dose in mg / Concentration in mg per ml) x 100
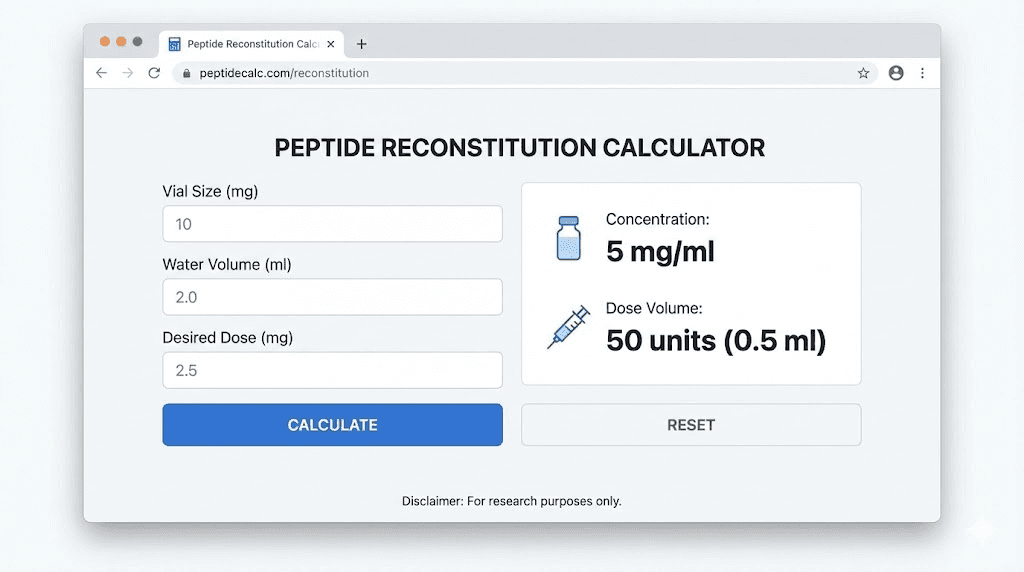
Using the SeekPeptides peptide calculator makes this even simpler. Enter your vial size, water volume, and desired dose, and it calculates the exact number of units.
Drawing a 2.5mg dose
At 5mg/ml (2ml water added): Draw 50 units. This is the halfway mark on a 100-unit syringe.
At 10mg/ml (1ml water added): Draw 25 units. This is the quarter mark on a 100-unit syringe.
The 2.5mg dose is the standard starting dose for tirzepatide. Most protocols maintain this dose for four weeks before increasing. Fifty units is one of the easiest measurements to draw accurately, which is another reason the 2ml reconstitution is preferred for beginners.
Drawing a 5mg dose
At 5mg/ml (2ml water added): Draw 100 units. This is a full syringe.
At 10mg/ml (1ml water added): Draw 50 units. The halfway mark.
The 5mg dose is usually the second step in the standard tirzepatide escalation schedule. At the 5mg/ml concentration, 100 units is straightforward but uses the entire syringe capacity. If you are on this dose and reconstituted with 2ml, you are pulling the full 1ml in a single draw. That works, but leaves no room for error. At the 10mg/ml concentration, the 50-unit draw is cleaner and more comfortable for the 5mg dose.
Drawing a 7.5mg dose
At 5mg/ml (2ml water added): You need 150 units. A single 100-unit syringe cannot hold this. You would draw 100 units in one syringe and 50 units in another, injecting both.
At 10mg/ml (1ml water added): Draw 75 units. Clean single draw.
This is the dose level where the 1ml reconstitution starts to make more practical sense. Drawing 75 units for a 7.5mg dose is simple. Splitting a dose across two syringes introduces extra steps and more opportunities for error. If you know your protocol will reach 7.5mg or higher, consider the 1ml reconstitution from the start.
Drawing a 10mg dose
At 5mg/ml (2ml water added): You need 200 units. That is two full syringes. Workable but cumbersome.
At 10mg/ml (1ml water added): Draw 100 units. One full syringe.
For the 10mg dose level, the 1ml reconstitution clearly wins on convenience. One syringe, one injection, one draw. However, by the time most people reach the 10mg dose, they typically have access to larger vial sizes like 30mg vials, which provide better value and easier dosing at this level.
Seven reconstitution mistakes that ruin tirzepatide
Tirzepatide is a peptide. Peptides are proteins. Proteins are fragile. Certain handling mistakes degrade the molecule, reduce potency, or contaminate the solution. Here are the most common errors and how to avoid them.
Mistake 1: spraying water directly onto the powder
This is the number one reconstitution mistake. When you push bacteriostatic water directly onto the lyophilized powder at high pressure, the force can denature the peptide chains. Always aim the needle at the inside wall of the vial and let the water trickle down. Slow and gentle. The guides on how much bacteriostatic water to add to peptides all emphasize this technique.
Mistake 2: shaking the vial
Never shake a reconstituted peptide vial. Shaking creates foam, introduces air bubbles, and causes physical stress that degrades the peptide through a process called denaturation. The agitation breaks the weak bonds holding the protein in its active shape. Gently swirl or roll instead. If you need a refresher on proper technique, the common peptide mistakes guide covers this and other errors in detail.
Mistake 3: using the wrong type of water
Bacteriostatic water is the only appropriate diluent for multi-dose tirzepatide vials. Using sterile water eliminates the bacterial inhibitor, making the solution unsafe for repeated draws. Using saline can cause precipitation. Using tap water or distilled water from the store introduces contaminants. The bacteriostatic water for peptides guide explains why the specific type of water matters so much.
Mistake 4: not cleaning the vial stoppers
Every time you insert a needle through the rubber stopper, it can push surface bacteria into the solution. Always swab the top with alcohol before each draw. This applies to both the initial reconstitution and every subsequent dose draw. Contamination is cumulative. Miss one cleaning, and you have introduced bacteria that multiply over the next 28 days in a nutrient-rich peptide solution.
Mistake 5: using too much or too little water
Adding more water than intended (say, 3ml instead of 2ml) dilutes the solution beyond your planned concentration. Now your dosing chart is wrong. Every dose you draw is lower than expected. The reverse, adding too little water, creates an overly concentrated solution with the same problem in the opposite direction. Measure carefully. Use a syringe with clear ml markings for the reconstitution step, not an insulin syringe. A 3ml luer-lock syringe is ideal for measuring 1-2ml of water precisely.
Mistake 6: storing at room temperature after reconstitution
Reconstituted tirzepatide must be refrigerated immediately. Leaving it on the counter, even for a few hours, accelerates degradation. The temperature sensitivity of tirzepatide means that prolonged exposure to room temperature reduces potency faster than most people expect. Refrigerate at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit) immediately after mixing.
Mistake 7: reusing needles
Each needle insertion through the rubber stopper dulls the tip and risks introducing contaminants. Use a fresh needle for every draw. This protects both the solution and your injection sites. Dull needles cause more tissue damage and increase the likelihood of bruising or discomfort at the injection site. A new needle every time is the standard for safe peptide research.
Storing your reconstituted tirzepatide
Proper storage after mixing is just as important as the reconstitution itself. The wrong storage conditions can degrade your tirzepatide faster than anything else.
Refrigeration requirements
Store reconstituted tirzepatide in the refrigerator at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit). This temperature range slows chemical degradation and bacterial growth. The back of the refrigerator tends to maintain the most stable temperature. Avoid the door shelves, which experience temperature fluctuations every time the refrigerator opens.
Keep the vial upright and away from light. Light exposure, particularly UV light, can degrade peptides over time. If your refrigerator has a glass door or interior lights, store the vial in a small box or wrap it in foil. The comprehensive peptide storage guide covers optimal storage conditions for all peptide types.
How long reconstituted tirzepatide lasts
The standard recommendation is 28 days after reconstitution. Some sources cite 30 days, but 28 is the more conservative and widely accepted timeframe. After 28 days, the peptide may still contain active tirzepatide, but the concentration could have dropped below the labeled amount, and bacterial contamination risk increases.
This 28-day window is why vial size and reconstitution volume need to be planned together. A 10mg vial at 2.5mg per week gives you exactly four doses over four weeks. Perfect. But a 10mg vial at 5mg per week gives only two doses, meaning you use up the vial in two weeks with potentially half the reconstituted volume unused. If tirzepatide expiration and waste concern you, match your vial size to your weekly dose so each vial gets fully used within the stability window.
What happens if it gets warm
Brief exposure to room temperature, like during a dose draw, is fine. But leaving reconstituted tirzepatide at room temperature for extended periods degrades the peptide. Studies on similar GLP-1 peptides show measurable potency loss after just a few hours above 25 degrees Celsius.
If you accidentally left your vial out overnight, the safest approach is to discard it. The cost of a replacement vial is less than the cost of injecting degraded peptide that does not work or causes unexpected reactions. If you travel with tirzepatide, insulated pouches with ice packs maintain the cold chain. The traveling with peptides guide offers practical tips for maintaining temperature during transport.
How to choose the right concentration for your protocol
The best concentration depends on where you are in your dosing schedule. There is no single right answer that applies to everyone at every phase. Here is how to think through the decision.
Starting dose (2.5mg): which concentration works best
At the 2.5mg starting dose, the 2ml reconstitution (5mg/ml) is almost always the better choice. Drawing 50 units is clean and accurate. The vial lasts exactly four weeks. The math is simple. If you are new to subcutaneous injections and still developing confidence with syringe technique, the larger volume and cleaner measurements reduce anxiety and errors.
This is consistent with the approach recommended for anyone following the standard tirzepatide dosing schedule for weight loss. The initial four weeks at 2.5mg are about building tolerance, not pushing boundaries. Accuracy matters more than convenience at this stage.
Maintenance dose (5 to 15mg): which concentration works best
Once you move past the starting dose, the picture shifts. At 5mg per week with a 5mg/ml concentration, you are drawing 100 units, a full syringe. That works fine. But at 7.5mg, you need 150 units. That means two separate draws and two injections.
For doses of 7.5mg and above, the 1ml reconstitution (10mg/ml) produces cleaner single draws. Seventy-five units for 7.5mg. One hundred units for 10mg. Both are manageable with a single syringe. If your protocol is headed toward these higher doses, switching to the 1ml reconstitution when you move past 5mg simplifies the process. The compound dosing chart for tirzepatide provides detailed unit counts across all vial sizes and concentrations.
Practically, if you are on a dose above 5mg, you may want to consider larger vial sizes. A 20mg vial or a 30mg vial provides better value and more flexibility for higher doses.
Microdosing: which concentration works best
Microdosing tirzepatide at 1mg to 1.25mg per week is growing in popularity for specific protocols. At these tiny doses, precision is everything.
With the 5mg/ml concentration, a 1.25mg dose equals 25 units. Clean.
With the 10mg/ml concentration, a 1.25mg dose equals 12.5 units. Not clean. You are estimating between syringe markings, introducing up to 8% measurement error.
For microdosing, the 2ml reconstitution is clearly superior. Some microdosers even add 3ml of water to create a 3.33mg/ml concentration, making extremely low doses easier to measure. However, more water means a shorter usable window if you are drawing large volumes relative to the total solution. The microdosing tirzepatide chart walks through the math for these specialized protocols.
How a 10mg vial fits the standard tirzepatide dosing schedule
The approved dosing schedule for tirzepatide follows a titration pattern designed to minimize side effects. You start low and increase gradually. Understanding how a single 10mg vial fits into this schedule helps with planning and budgeting.
Phase | Weekly dose | Duration | 10mg vials needed | Notes |
|---|---|---|---|---|
Phase 1 | 2.5mg | 4 weeks | 1 vial | Perfect match, vial lasts exactly 4 weeks |
Phase 2 | 5mg | 4 weeks | 2 vials | Each vial lasts 2 weeks |
Phase 3 | 7.5mg | 4 weeks | 3 vials | Each vial lasts ~1.3 weeks |
Phase 4 | 10mg | 4 weeks | 4 vials | 1 vial per week |
The 10mg vial is ideal for the Phase 1 starting dose. One vial, four weeks, done. As you titrate up through higher doses, the 10mg vial becomes less economical. Two vials for Phase 2 is manageable. Three or four vials for Phase 3 and Phase 4 gets expensive and wasteful since each vial has solution remaining after the last needed draw.
This is why many people start with 10mg vials and transition to 30mg vials once they reach 5mg per week or higher. A 30mg vial with 3ml of water provides a 10mg/ml concentration that delivers clean doses at the 5mg, 7.5mg, 10mg, and even 12.5mg levels.
The SeekPeptides platform provides dosage calculators that map out vial usage across your entire protocol, helping you plan purchases and minimize waste. If you are trying to figure out how many vials you need for a complete 16-week titration, those tools save time and prevent the frustrating discovery that you are one vial short halfway through a dose increase.
Comparing 10mg vials to other tirzepatide vial sizes
The 10mg vial is one of several sizes available for compounded tirzepatide. Knowing how it compares helps you make better purchasing decisions as your protocol evolves.
Vial size | Recommended bac water | Concentration | Weeks at 2.5mg | Weeks at 5mg | Weeks at 10mg |
|---|---|---|---|---|---|
5mg | 1ml | 5mg/ml | 2 | 1 | 0.5 |
10mg | 1-2ml | 5-10mg/ml | 4 | 2 | 1 |
20mg | 2ml | 10mg/ml | 8 | 4 | 2 |
30mg | 3ml | 10mg/ml | 12 | 6 | 3 |
The 5mg vial is less common for tirzepatide but exists. It is typically reconstituted with 1ml of water for a 5mg/ml solution. At the starting dose, it lasts only two weeks, which is less than ideal.
For researchers on lower doses (2.5 to 5mg), the 10mg vial hits the sweet spot. For those on maintenance doses above 5mg, the larger vial sizes provide better value and longer usability. The reconstituting tirzepatide chart covers all vial sizes with detailed mixing and dosing instructions.
Using a reconstitution calculator
Math mistakes account for a significant number of dosing errors. If you are not confident in your calculations, or if you just want a quick double-check, reconstitution calculators eliminate the guesswork.
The free peptide reconstitution calculator on SeekPeptides works like this:
Enter your vial size (10mg)
Enter the amount of bacteriostatic water added (1ml or 2ml)
Enter your desired dose (2.5mg, 5mg, etc.)
The calculator returns the exact number of units to draw on your insulin syringe
This is particularly useful when switching between vial sizes or concentrations. If you move from a 10mg vial with 2ml of water to a 30mg vial with 3ml of water, the units per dose change completely. Running the numbers through a calculator prevents the kind of mistakes that lead to unexplained lack of results or sudden onset of side effects like headaches.
For researchers who use semaglutide alongside or as an alternative to tirzepatide, separate calculators handle the semaglutide reconstitution math since the dosing ranges are different.
Advanced considerations for 10mg tirzepatide reconstitution
Dead space and volume loss
Every syringe has dead space, the small amount of liquid that remains in the needle hub and syringe barrel after the plunger is fully depressed. Standard insulin syringes have approximately 0.01 to 0.05ml of dead space. Over four draws from a 10mg vial, this can mean losing 0.04 to 0.2ml of solution, enough to reduce your final dose by 5 to 10%.
Low dead-space syringes minimize this loss. If you are concerned about getting every last unit out of a vial, they are worth the small extra investment. Alternatively, you can slightly overfill each draw by 1 to 2 units to compensate, though this requires careful tracking to avoid running out before your fourth dose.
Air bubbles and their impact
Small air bubbles in the syringe displace solution and reduce your actual dose. Before injecting, hold the syringe with the needle pointing up, tap the barrel gently to move bubbles to the top, and push the plunger slightly to expel them. This is standard injection technique covered in the GLP-1 injection guide.
Air bubbles are not dangerous for subcutaneous injections. A small bubble injected under the skin will be absorbed harmlessly. The concern is dosing accuracy, not safety. If you draw 50 units but 5 units of that is air, you are only injecting 45 units of solution, which is 10% less tirzepatide than intended.
Combining vial remnants
Some researchers wonder if they can combine leftover solution from two vials into one. This is generally not recommended. Each vial has its own reconstitution date, and combining them creates uncertainty about the total peptide content and the effective expiration date. Additionally, each transfer introduces contamination risk. It is better to plan your reconstitution and dosing to use each vial completely.
Tirzepatide compared to other peptides you might reconstitute
If you are experienced with other peptides, it helps to understand how tirzepatide reconstitution compares. The basic process is the same, but the concentrations and volumes differ.
Semaglutide is the most common comparison. A 5mg semaglutide vial is typically reconstituted with 1 to 2ml of bacteriostatic water, producing concentrations of 5mg/ml or 2.5mg/ml respectively. The dosing ranges for semaglutide (0.25mg to 2.4mg) are much lower than tirzepatide, so the unit counts on the syringe are smaller. The semaglutide versus tirzepatide comparison covers how these two GLP-1 peptides differ in dosing, efficacy, and mechanism.
Retatrutide, the newer triple agonist, also comes in 10mg vials. The reconstitution process for 10mg retatrutide follows the same principles, though the dosing schedule differs. If you are considering switching between peptides, understanding the concentration differences prevents the kind of dosing confusion that happens when people apply one peptide dose chart to a different peptide.
For general reconstitution principles that apply to all peptides, the complete peptide reconstitution guide provides a universal framework.
What to do if something goes wrong
You added the wrong amount of water
If you added too much water, your solution is more dilute than planned. Do not try to remove water from the vial. Instead, recalculate your dosing based on the actual concentration. For example, if you added 3ml instead of 2ml to a 10mg vial, your concentration is 3.33mg/ml instead of 5mg/ml. A 2.5mg dose at this concentration requires 75 units instead of 50. Adjust your dosage chart in units accordingly and move forward.
If you added too little water, the solution is more concentrated. The same principle applies: recalculate and adjust. But be extra careful with your measurements, since the higher concentration means each unit contains more tirzepatide, and errors have a bigger impact.
The powder did not dissolve completely
Give it more time. Some tirzepatide lyophilized powder takes 2 to 5 minutes to fully dissolve, especially if the vial was stored at very cold temperatures. Gentle rolling helps. If particles persist after 10 minutes of patient swirling, the vial may have been compromised. High temperatures during shipping or prolonged storage above recommended conditions can cause irreversible aggregation. In that case, the safest option is to contact your supplier about a replacement.
You dropped the vial
If the vial is intact and the stopper did not dislodge, the solution is probably fine. But check for any cracks in the glass, particularly hairline fractures that might not be immediately visible. Cracked glass can introduce glass particles into the solution. If in doubt, discard it. The cost of a new vial is not worth the risk of injecting glass fragments.
Connecting reconstitution to your broader tirzepatide protocol
Reconstitution is one step in a larger protocol. The bacteriostatic water amount you choose connects to your diet plan, your supplement stack, your injection schedule, and your overall weight loss strategy. Getting the mixing right sets the foundation for everything else.
Timing matters too. Many researchers plan their reconstitution for the same day each week, right before their injection. This minimizes the time the reconstituted solution sits in the refrigerator. Others prefer to reconstitute at the start of a new vial cycle and draw doses throughout the month. Both approaches work, as long as the 28-day window is respected.
If you are experiencing side effects like muscle pain, fatigue, or anxiety, your reconstitution might not be the cause, but verifying your concentration and dose accuracy should be one of the first troubleshooting steps. Sometimes what looks like a side effect from the peptide itself is actually a dosing error from incorrect reconstitution math.
The foods to avoid on tirzepatide, the recommended diet, and the best time to take your injection all interact with how well your protocol works. But none of those factors matter if the foundation, your reconstitution, is wrong.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed tirzepatide dosing guides, personalized calculators, and expert support for every phase of the process.
Frequently asked questions
Can I use sterile water instead of bacteriostatic water for 10mg tirzepatide?
Sterile water for injection works for single-use vials only. Since a 10mg vial provides multiple doses over several weeks, you need bacteriostatic water with its benzyl alcohol preservative to prevent bacterial contamination between draws. Using sterile water in a multi-dose vial creates a serious infection risk.
What happens if I add 3ml of bacteriostatic water to a 10mg vial?
Adding 3ml creates a concentration of approximately 3.33mg/ml. This is a valid option, especially for microdosing protocols where you need very precise measurements of small doses. The trade-off is larger injection volumes at standard doses: a 2.5mg dose requires 75 units, and a 5mg dose requires 150 units (two syringe draws). Verify your math with the reconstitution calculator whenever you use a non-standard water volume.
How do I know if my reconstituted tirzepatide has gone bad?
Look for cloudiness, visible particles, discoloration, or an unusual smell. Properly reconstituted and stored tirzepatide should remain clear and colorless for up to 28 days. If it has been longer than 28 days or if the solution looks different from when you first mixed it, discard it and reconstitute a fresh vial. The tirzepatide expiration guide has more details on shelf life indicators.
Can I freeze reconstituted tirzepatide to make it last longer?
No. Freezing reconstituted peptide solutions can cause ice crystals to form that damage the protein structure. This is different from the lyophilized (freeze-dried) powder, which is stable at frozen temperatures. Once water is added, the rules change. Keep it refrigerated, never frozen. The peptide storage after reconstitution guide explains the science behind this.
Is 10mg/ml concentration too strong for tirzepatide?
Not at all. The 10mg/ml concentration from adding 1ml of water to a 10mg vial is safe and effective. Commercial tirzepatide products (Mounjaro, Zepbound) use even higher concentrations in their pre-filled injection pens. The concentration does not affect the peptide itself, only how much volume you draw for each dose. Higher concentration means smaller volumes, which some people actually prefer.
Do I need different syringes for reconstitution and injection?
Yes. Use a larger gauge syringe (18 to 22 gauge) with a standard luer-lock tip for drawing and injecting the bacteriostatic water during reconstitution. Then use a fine gauge insulin syringe (29 to 31 gauge) for drawing and administering your dose. The larger needle makes reconstitution faster, while the finer needle makes injections less painful.
How does tirzepatide reconstitution compare to semaglutide reconstitution?
The process is identical. The difference is in the dosing. Semaglutide doses range from 0.25mg to 2.4mg, much lower than tirzepatide doses of 2.5mg to 15mg. This means semaglutide vials are typically reconstituted with less water to keep the unit counts manageable. A 10mg semaglutide vial might use 1ml of water for a 10mg/ml concentration, while a 10mg tirzepatide vial often uses 2ml. The tirzepatide versus semaglutide dosage chart lays out the differences clearly.
What if I am switching from a pre-filled pen to a compounded vial?
Pre-filled pens like Mounjaro deliver exact doses automatically. Switching to a compounded vial with manual reconstitution requires you to handle the mixing and measuring yourself. The active ingredient is the same, but the responsibility for accuracy shifts to you. Start with the 2ml reconstitution for its forgiving measurements, and use a compounded tirzepatide dosage calculator until the process becomes second nature. The conversion chart helps translate pen doses to vial doses.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your reconstitution stay precise, your concentrations stay accurate, and your results stay consistent.