Mar 31, 2026

You started semaglutide. The scale is finally moving. The appetite suppression feels like a superpower you never knew existed. But then you catch yourself in the mirror. Something looks different. Not just smaller. Weaker. The arms that used to fill out your sleeves look deflated. The shoulders that carried grocery bags without a second thought feel less capable. And that nagging voice in the back of your head asks the question nobody wants to hear: how much of what you are losing is actually fat?
It is a legitimate concern. A study published in Obesity found that up to 39% of weight lost on semaglutide came from lean body mass. Not fat. Muscle. The very tissue that keeps your metabolism humming, protects your joints, helps you climb stairs at 70, and determines whether weight loss transforms your health or just makes you a smaller, weaker version of yourself.
This is where creatine enters the conversation.
Creatine monohydrate is the single most studied supplement in sports nutrition history. Hundreds of clinical trials. Decades of safety data. And a growing body of evidence suggesting it may be one of the most effective tools for preserving muscle mass during caloric restriction, which is exactly what semaglutide creates. The combination of semaglutide protocols and strategic creatine supplementation represents something researchers and clinicians are increasingly paying attention to: a way to keep the weight loss benefits of GLP-1 therapy while protecting the lean tissue your body desperately needs to hold onto.
This guide covers everything about combining creatine and semaglutide. Whether they interact. Whether they are safe together.
How creatine actually works in the context of reduced caloric intake. What the research says about muscle preservation during GLP-1 therapy. Specific protocols for timing, dosing, and pairing creatine with resistance training while on semaglutide. And the practical troubleshooting details that most guides skip entirely. If you are on semaglutide and worried about losing muscle along with fat, you are in the right place. SeekPeptides members have been navigating this exact challenge, and the evidence points to creatine as one of the smartest additions to a GLP-1 weight loss protocol.
Why semaglutide causes muscle loss in the first place
Before discussing creatine as a solution, you need to understand the problem. Semaglutide does not target muscle directly. It does not break down protein fibers. It does not interfere with muscle protein synthesis in any direct pharmacological way. But it creates conditions that make muscle loss almost inevitable for anyone who does not take deliberate steps to prevent it.
The primary mechanism is simple. Semaglutide suppresses appetite dramatically. People eat significantly less. In clinical trials, participants on 2.4mg semaglutide reduced their caloric intake by 30-40% compared to baseline. That kind of caloric deficit drives weight loss, but your body does not exclusively burn fat stores for energy. It also breaks down muscle tissue, especially when protein intake drops alongside overall calories.
Three mechanisms drive semaglutide-related muscle loss:
Reduced caloric intake. When you eat 30-40% fewer calories, your body enters a sustained catabolic state. Without adequate protein and resistance stimulus, muscle becomes expendable fuel. The body prioritizes organ function and basic metabolic needs over maintaining skeletal muscle it perceives as unnecessary for survival.
Reduced protein consumption. Most people on semaglutide do not just eat less food. They eat less of everything, including protein. When you can barely finish half a chicken breast, hitting your daily protein target becomes genuinely difficult. And protein intake on semaglutide is arguably the single most important dietary factor for muscle preservation.
Reduced physical activity in some users. Semaglutide fatigue is real, particularly during the dose titration phase. Some users report decreased energy and motivation for exercise, especially in the first 4-8 weeks. Less resistance training means less stimulus for muscle maintenance. And without that stimulus, the body has even less reason to preserve muscle tissue during weight loss.
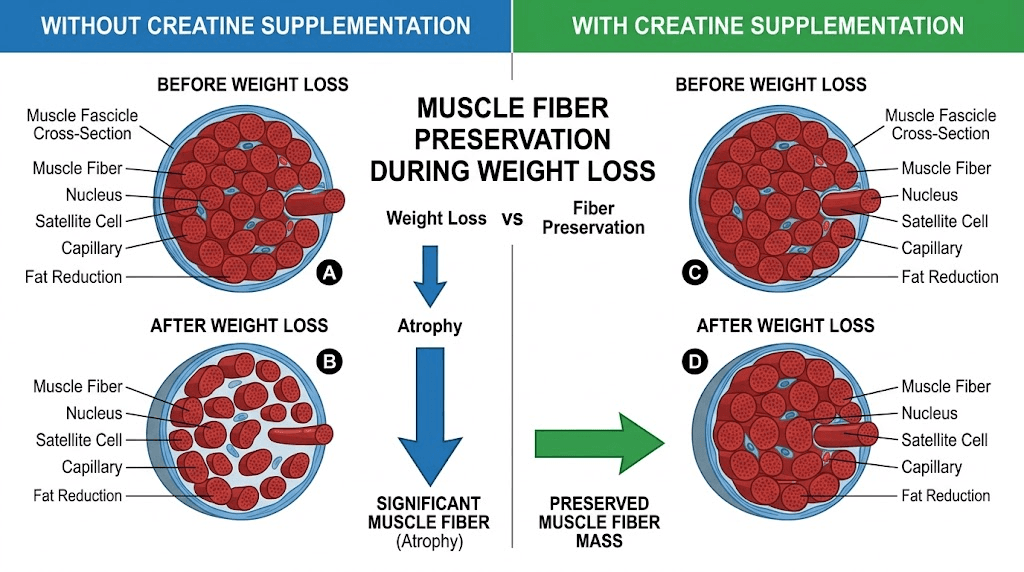
The 39% lean mass loss figure is an average from clinical trials where participants were not given specific exercise or supplementation protocols. It represents what happens when semaglutide drives weight loss in the absence of deliberate muscle preservation strategies. Not a worst-case scenario. A default outcome. That distinction matters because it means the muscle loss is preventable. You just need the right tools. Creatine is one of them.
What creatine actually does in your body
Creatine is not a steroid. It is not a stimulant. It is not a drug. It is an amino acid derivative that your body produces naturally, primarily in the liver, kidneys, and pancreas. You also consume it through dietary sources like red meat and fish. Your body stores approximately 120-140 grams of creatine at any time, with about 95% residing in skeletal muscle as phosphocreatine.
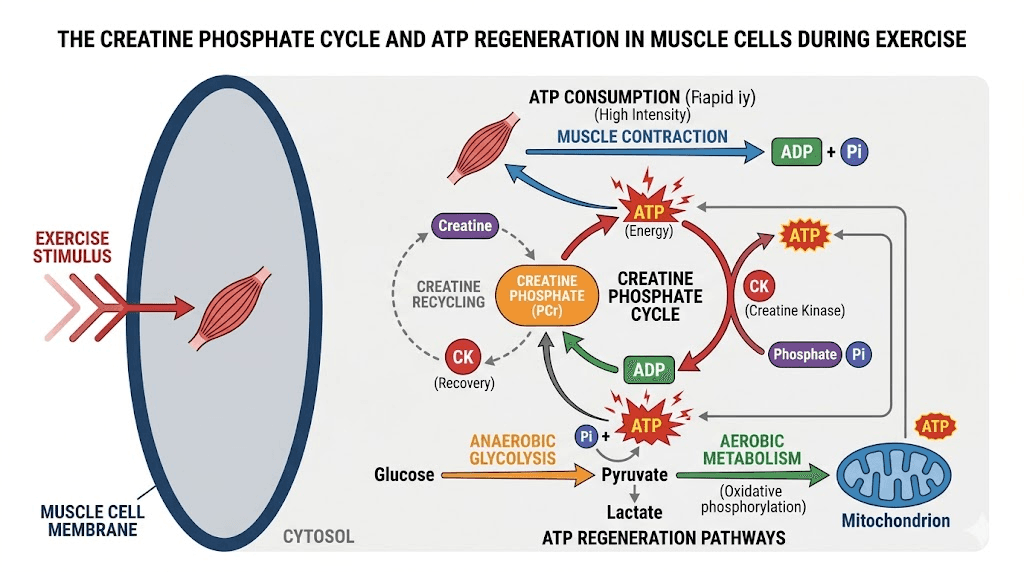
The primary function of creatine relates to energy production. During high-intensity exercise, your muscles use adenosine triphosphate (ATP) as immediate fuel. ATP gets broken down to adenosine diphosphate (ADP), releasing energy in the process. Phosphocreatine donates its phosphate group to ADP, regenerating ATP so your muscles can keep working. More stored creatine means faster ATP regeneration. Faster ATP regeneration means more work capacity during resistance training.
But creatine does more than just fuel workouts. Research has identified several mechanisms relevant to muscle preservation:
Increased intracellular water retention. Creatine draws water into muscle cells, creating a more anabolic cellular environment. This cell volumization signals the cell to increase protein synthesis and decrease protein breakdown. Think of it as the muscle cell sensing that it is well-hydrated and well-resourced, so it shifts toward building rather than breaking down.
Enhanced satellite cell activity. Satellite cells are muscle stem cells that repair and grow muscle tissue. Creatine supplementation has been shown to increase the number and activity of satellite cells, particularly when combined with resistance training. More active satellite cells mean better muscle repair and maintenance capacity.
Reduced myostatin expression. Myostatin is a protein that limits muscle growth. Some research suggests creatine supplementation may reduce myostatin levels, potentially removing one of the brakes on muscle maintenance. This mechanism is less well-established than the others, but the preliminary data is promising.
Improved training performance. By increasing phosphocreatine stores, creatine allows you to perform more reps, lift heavier weights, and recover faster between sets. Better training stimulus means stronger signals for muscle preservation. When your muscles are regularly challenged with adequate resistance, your body fights harder to maintain them, even during a caloric deficit.
For someone on semaglutide who is eating 30-40% fewer calories than before, every single one of these mechanisms matters. The improved training capacity means you can still challenge your muscles despite lower energy availability. The cell volumization promotes an anabolic state that directly opposes the catabolic environment created by caloric restriction. And the satellite cell activation supports muscle repair even when nutritional resources are limited.
Is it safe to take creatine with semaglutide?
Yes. There is no documented pharmacological interaction between creatine monohydrate and semaglutide. Zero. They work through completely different mechanisms in completely different systems.
Semaglutide is a GLP-1 receptor agonist that primarily acts on receptors in the brain (appetite regulation), pancreas (insulin secretion), and gastrointestinal tract (gastric emptying). Creatine is an amino acid derivative that is stored in skeletal muscle and used for energy metabolism. Their metabolic pathways do not cross. Their mechanisms do not interfere with each other. No clinical evidence suggests any negative interaction between the two.
The MHRA and FDA have not flagged any contraindication between creatine and semaglutide or any other GLP-1 receptor agonist. Drug interaction databases show no known interactions. And the millions of people who take creatine daily while using various medications provide a robust real-world safety signal.
That said, there are practical considerations that matter:
Kidney function monitoring
This is the most common concern and the most misunderstood. Creatine supplementation increases serum creatinine levels. Creatinine is a waste product of creatine metabolism, and it is the standard biomarker used to estimate kidney function (eGFR). When you take creatine, your creatinine goes up, not because your kidneys are struggling, but because there is simply more creatine being metabolized.
A systematic review and meta-analysis found that creatine supplementation was associated with a small but statistically significant increase in serum creatinine of approximately 0.07 micromol/L. However, actual kidney function measured by glomerular filtration rate (GFR) showed no statistically significant differences between creatine users and controls. The kidneys are fine. The blood test just looks different.
Why does this matter for semaglutide users? Because your doctor may order blood work to monitor kidney function while you are on semaglutide, particularly if you have diabetes or other risk factors. If you are taking creatine and your creatinine comes back elevated, you or your doctor might panic. You should not. But you should tell your healthcare provider that you take creatine so they can interpret the results correctly. Better yet, ask for a cystatin C test instead of creatinine-based eGFR if you want an accurate picture of kidney function while supplementing with creatine.
Semaglutide itself has shown kidney-related considerations in some populations. The FLOW trial demonstrated a 24% reduction in kidney disease progression in patients with type 2 diabetes and chronic kidney disease taking semaglutide. However, rare cases of acute kidney injury have been reported, primarily linked to severe dehydration from GI side effects. Creatine does not add to this risk, but adequate hydration becomes even more important when combining both.
Gastrointestinal tolerance
Semaglutide already causes GI side effects in many users. Nausea, bloating, constipation, and dizziness are all common, particularly during dose escalation. Adding creatine to an already sensitive stomach requires some thought.
Creatine monohydrate at standard doses (3-5 grams daily) rarely causes GI issues in healthy individuals. But people with reduced gastric motility from semaglutide may notice mild bloating or stomach discomfort if they take a large dose on an empty stomach. The solution is straightforward: take creatine with food, use a micronized form for better dissolution, and avoid loading protocols (more on this below).
Hydration requirements
Both semaglutide and creatine increase your need for adequate hydration, though for different reasons. Semaglutide reduces appetite, which means you drink less passively (much of our daily water intake comes from food). The GI side effects, particularly if you experience acid reflux or nausea, can further reduce fluid intake. Creatine draws water into muscle cells, which is part of how it works, but it means the rest of your body needs adequate water to compensate.
The practical implication: aim for a minimum of 3 liters of water daily when combining semaglutide and creatine. More if you exercise regularly or live in a hot climate. Dehydration is the one genuinely avoidable risk factor here, and it is entirely within your control.
The muscle preservation evidence: what research actually shows
No published clinical trial has specifically studied creatine supplementation in a semaglutide-treated population. That is worth stating clearly upfront. The direct combination has not been investigated in a randomized controlled trial. However, the individual evidence for each compound is so robust, and the mechanisms so complementary, that the case for combining them is strong.
Here is what we know from the available research:
Creatine during caloric restriction
Multiple studies have examined creatine supplementation during energy-restricted diets. The consistent finding is that creatine, when combined with resistance training, helps preserve significantly more lean mass compared to resistance training alone during caloric restriction.
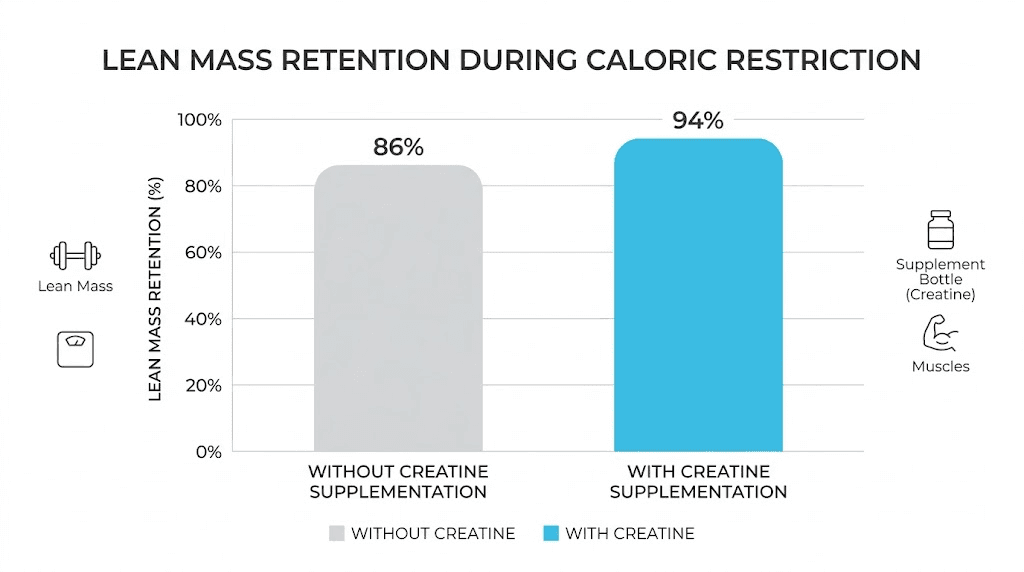
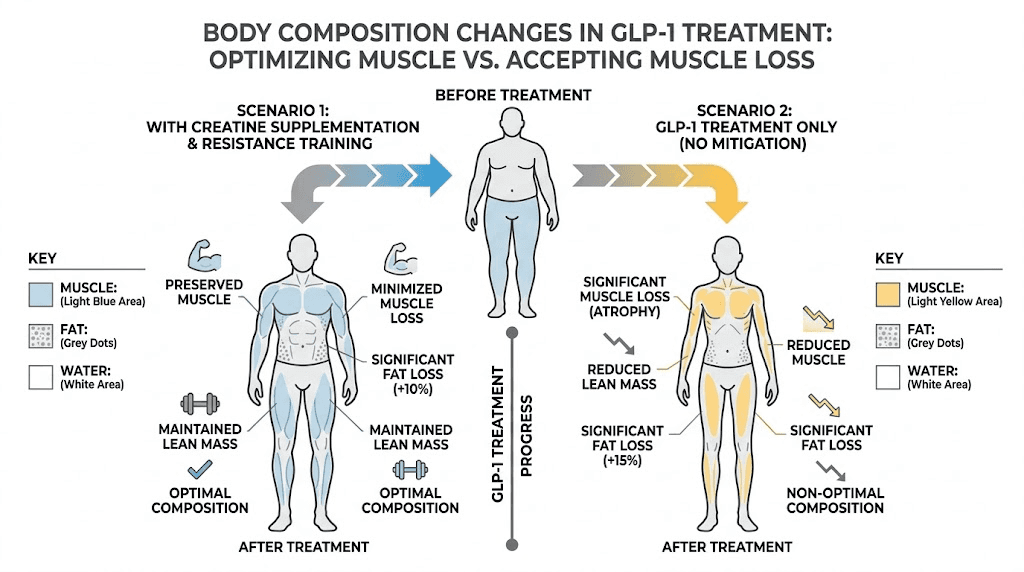
Research shows that individuals combining creatine supplementation with resistance training during weight loss maintained 95% of their muscle mass, compared to 85% in the control group. That 10% difference sounds small until you realize it translates to preserving an extra 1-2 kg of lean tissue over a typical weight loss period. For someone losing 15-20 kg on semaglutide, that could mean the difference between losing 6 kg of muscle and losing 2-3 kg.
Another analysis found that creatine supplementation can blunt lean mass decline by up to 60% compared to non-supplemented controls in hypocaloric states. The mechanism appears to involve both the direct cellular effects of creatine (cell volumization, satellite cell activation) and the indirect benefit of being able to train harder and maintain better workout quality despite eating less.
Creatine in older adults
Much of the creatine research relevant to semaglutide users comes from studies in older adults, a population that shares key similarities with GLP-1 users: they are prone to muscle loss, often have reduced protein intake, and benefit enormously from resistance training but may struggle with training intensity. Meta-analyses in adults aged 50-80 show significant gains in lean body mass when creatine is combined with resistance training compared to placebo and resistance training only. The creatine group increased lean body mass by an average of 1.32 kg compared to placebo. These were not young athletes with optimized nutrition. These were regular older adults dealing with real-world constraints on their diet and training, much like someone on semaglutide.
The narrative review on supplements during GLP-1 therapy
A narrative review published in a peer-reviewed journal specifically examined dietary supplement considerations during GLP-1 receptor agonist treatment. The review concluded that while creatine supplementation has not been studied directly in a GLP-1RA population, the existing evidence supports daily creatine supplementation with resistance training as part of a comprehensive GLP-1RA care plan. The rationale is straightforward: the mechanisms by which creatine preserves muscle are not dependent on the method of caloric restriction. Whether you eat less because of willpower, a structured diet, or a GLP-1 agonist suppressing your appetite, the muscle preservation mechanisms of creatine remain the same.
If you are also considering creatine with tirzepatide or creatine with other GLP-1 medications, the same principles apply. The choice of GLP-1 agonist does not change the fundamental relationship between creatine, resistance training, and muscle preservation.
Creatine dosing protocol while on semaglutide
The dosing protocol for creatine while on semaglutide is simpler than most supplements. But there are specific modifications worth making to accommodate the GI sensitivity and reduced appetite that semaglutide creates.
Standard maintenance dose
Take 3-5 grams of creatine monohydrate daily. Every day. Not just on training days. Creatine works through saturation, meaning your muscles need to be consistently loaded with phosphocreatine to get the benefits. Missing days reduces muscle creatine stores and diminishes the protective effect.
For most people on semaglutide, 5 grams daily is the target. If you weigh under 70 kg (154 lbs), 3 grams may be sufficient. If you weigh over 90 kg (198 lbs), some research suggests up to 10 grams daily may be beneficial, though splitting this into two 5-gram doses is easier on the stomach.
Skip the loading phase
Traditional creatine protocols often recommend a loading phase of 20 grams daily (split into 4 doses of 5 grams) for 5-7 days. Do not do this while on semaglutide. The loading phase is designed to saturate muscle creatine stores quickly, but it comes with a significantly higher risk of GI distress. Bloating, stomach cramping, and diarrhea are common during loading, and these are the last things you need on top of semaglutide side effects.
Instead, simply take 5 grams daily and let your stores saturate naturally. It takes about 3-4 weeks instead of 5-7 days. The end result is the same. Full muscle creatine saturation. The only difference is the timeline, and patience is a small price to pay for avoiding unnecessary GI misery.
Timing considerations
The research on creatine timing is mixed, and the differences are small regardless. But for semaglutide users, practical timing matters more than theoretical optimization:
Best option: take creatine with a meal. Specifically, with a meal that contains protein and carbohydrates. The insulin spike from carbohydrates may slightly enhance creatine uptake into muscle cells, but more importantly, taking it with food reduces the chance of stomach upset. If you are only eating one or two real meals on semaglutide, take your creatine with the largest one.
Post-workout is slightly better than pre-workout. Some research suggests marginally better muscle uptake when creatine is consumed after exercise rather than before. The difference is small enough that consistency matters more than timing. If you can remember to take it after training, do that. If you can only remember to take it with breakfast, that works too.
Avoid taking creatine on an empty stomach. This applies to everyone, but especially to semaglutide users whose gastric motility is already altered. An empty stomach combined with semaglutide-slowed digestion can lead to creatine sitting in your stomach longer than usual, potentially causing discomfort.
Form matters
Use creatine monohydrate. Not creatine hydrochloride. Not buffered creatine. Not creatine ethyl ester. Creatine monohydrate is the most researched, most effective, and least expensive form available. Every credible study on creatine and muscle preservation used creatine monohydrate.
Within the monohydrate category, choose a micronized version. Micronized creatine has smaller particle sizes, dissolves better in water, and is easier on the stomach. This matters when your GI system is already dealing with semaglutide-induced changes to gastric emptying and motility.
Building a complete muscle preservation protocol on semaglutide
Creatine alone will not save your muscle mass on semaglutide. It is one piece of a multi-faceted approach. The complete protocol involves protein, resistance training, and creatine working together. Remove any one element and the others become significantly less effective.
Protein targets
Aim for 1.6-2.2 grams of protein per kilogram of body weight daily. This is higher than general population recommendations because you are in a caloric deficit. Your body needs more protein when losing weight to prevent muscle breakdown, not less. The protein requirements on semaglutide are non-negotiable if you care about body composition.
Hitting these targets while eating 30-40% fewer calories is genuinely challenging. Practical strategies include prioritizing protein at every eating opportunity, using protein shakes when solid food feels impossible, choosing protein-dense foods like Greek yogurt, eggs, and lean meat, and considering protein shakes designed for GLP-1 users.
Resistance training
You need to lift weights. Or perform bodyweight exercises that challenge your muscles sufficiently. Cardio alone will not preserve muscle mass. Walking will not preserve muscle mass. You need progressive overload, meaning your muscles must be challenged to lift heavier loads or perform more reps over time.
The minimum effective dose for muscle preservation during weight loss is 2-3 sessions per week targeting all major muscle groups. Each session should include compound movements (squats, deadlifts, presses, rows) performed for 3-4 sets of 6-12 repetitions. If you are new to resistance training, start with bodyweight exercises or light weights and progress gradually.
Creatine specifically enhances your capacity to maintain training intensity during caloric restriction. Without creatine, many semaglutide users find their workouts suffer as their caloric intake drops. Weights feel heavier. Recovery takes longer. Motivation declines. Creatine helps buffer these effects by ensuring your muscles have adequate phosphocreatine for high-intensity efforts.
For those wondering about building muscle while on GLP-1 medications, the answer is yes, it is possible, but it requires deliberate effort. Creatine makes that effort more productive.
The synergy protocol
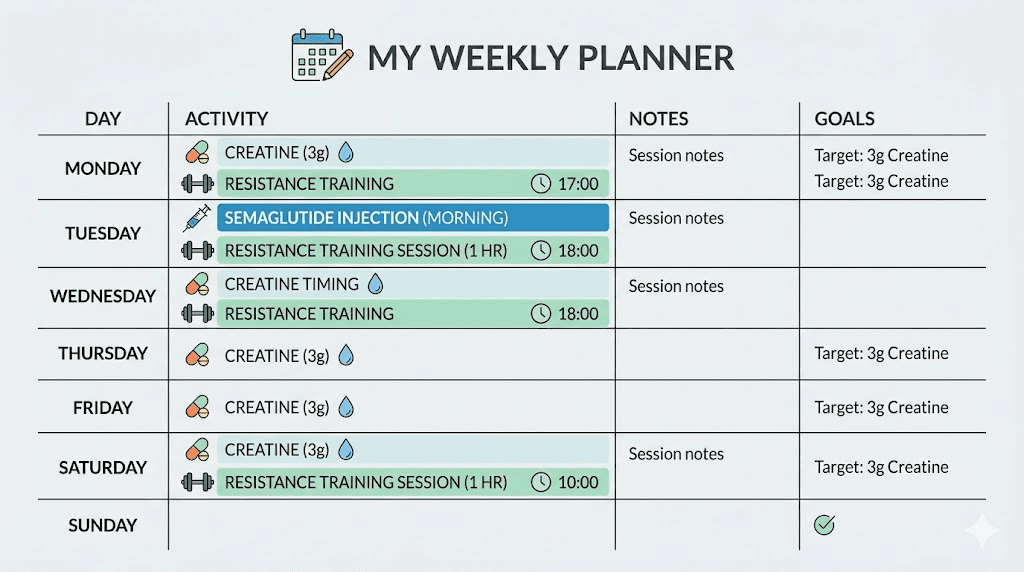
Here is what a complete weekly protocol looks like when combining semaglutide, creatine, and resistance training:
Daily:
5 grams creatine monohydrate with your largest meal
1.6-2.2 grams protein per kg bodyweight, distributed across meals
Minimum 3 liters water
Semaglutide injection on your regular schedule
3-4 times per week:
30-45 minutes resistance training
Focus on compound movements
Track weights and reps to ensure progressive overload
Take creatine within 2 hours post-workout on training days
Weekly check-ins:
Track body weight and waist circumference (not just scale weight)
Note training performance (are weights going up or maintaining?)
Assess energy levels and energy on semaglutide
Evaluate GI tolerance of creatine
Creatine and semaglutide side effects: what to watch for
Most people tolerate the combination well. But understanding potential issues helps you troubleshoot quickly if something feels off.
Weight gain on the scale
This is the most common source of confusion. Creatine causes water retention in muscle cells. This is a feature, not a bug. It is part of how creatine protects muscle. But it means the scale may go up by 1-3 kg (2-6 lbs) in the first few weeks of supplementation, even while you are losing fat.
This is not fat gain. It is not semaglutide stopping to work. It is intracellular water being stored in muscle tissue, which is exactly where you want it. If you are tracking your semaglutide results by scale weight alone, starting creatine will temporarily skew those numbers. Track waist circumference and how your clothes fit alongside scale weight for a more accurate picture.
Some users get frustrated and stop creatine because the scale stalls or increases. This is a mistake. The water retention is a sign creatine is working, and the muscle preservation benefits are worth far more than a temporary number on the scale.
GI overlap
If you are in the early weeks of semaglutide dose titration and experiencing significant nausea or bloating, consider starting creatine after your GI symptoms stabilize. There is no rush. Starting creatine at the same time as semaglutide means you cannot tell which supplement is causing any given GI symptom. Wait until your body adjusts to semaglutide (usually 2-4 weeks at a stable dose), then introduce creatine.
If you are already on a stable semaglutide dose with manageable GI symptoms, creatine is usually well-tolerated. Start with 3 grams daily for the first week, then increase to 5 grams if no issues arise.
Dehydration signs
Watch for headaches, dark urine, dizziness, and dry mouth. These can result from inadequate water intake, and both semaglutide and creatine increase your hydration needs. If you experience lightheadedness on semaglutide, adding creatine without increasing water intake could make it worse. Simple fix: drink more water.
Blood work considerations
As mentioned earlier, creatine will elevate serum creatinine levels. If your doctor orders blood work while you are on semaglutide, tell them you are taking creatine. This prevents unnecessary concern over a false positive for kidney impairment. If you want to get an accurate kidney function assessment, stop creatine for 3-5 days before the blood draw, or ask for a cystatin C test, which is not affected by creatine supplementation.
Understanding how semaglutide affects blood work results is important regardless of whether you take creatine. GLP-1 medications can influence several markers, and knowing what to expect helps you interpret results accurately.
Common mistakes when combining creatine and semaglutide
After reviewing hundreds of forum posts, community discussions, and clinical observations, these are the most frequent errors people make when trying to preserve muscle on semaglutide with creatine:
Mistake 1: taking creatine without resistance training
Creatine is not a magic muscle preservation pill. Without resistance training, creatine provides some cellular-level benefits (cell volumization, hydration), but the majority of its muscle-preserving effects depend on being combined with exercise that challenges your muscles. Taking 5 grams of creatine daily while sitting on the couch is dramatically less effective than taking 5 grams while training 3-4 times per week.
Mistake 2: not eating enough protein
Creatine supports muscle preservation. Protein builds and repairs muscle. If your protein intake is 60 grams daily because semaglutide killed your appetite, creatine cannot compensate for that deficiency. You need both. The best foods to eat on semaglutide are protein-rich options that pack maximum nutrition into smaller portions.
Mistake 3: stopping creatine because of scale weight
Already covered, but worth repeating. The 1-3 kg of water weight creatine adds is not the enemy. It is a sign the supplement is working. If your semaglutide weight loss stalls temporarily after starting creatine, trust the process. Measure your waist. Check how your clothes fit. The fat loss is still happening underneath the water retention.
Mistake 4: loading creatine during semaglutide titration
The loading phase (20g daily for a week) is unnecessary for everyone, but it is especially problematic for semaglutide users. Your stomach is already adjusting to a medication that slows gastric emptying. Dumping 20 grams of creatine into that environment is asking for trouble. Just take 5 grams daily and be patient.
Mistake 5: relying on creatine alone without addressing the bigger picture
Creatine is one tool. A powerful tool, but one tool. If you are not also addressing caloric intake on semaglutide, protein consumption, resistance training, sleep quality, and stress management, creatine alone will not prevent significant muscle loss. Think of muscle preservation as a comprehensive strategy, not a single supplement solution.
Creatine timing around your semaglutide injection
Some users wonder whether they should adjust their creatine intake around their weekly semaglutide injection. This is a reasonable question since semaglutide side effects tend to peak in the 24-48 hours following injection.
The short answer: you do not need to change your creatine routine around injection day.
The longer answer: if you reliably experience significant nausea or stomach upset in the day or two after your semaglutide injection, you might find it more comfortable to take creatine with a bland meal during those days rather than with a larger meal. Some users find that mixing creatine into a smoothie or protein shake on injection day is easier on the stomach than taking it with solid food.
What you should not do is skip creatine entirely for 2-3 days around injection day. Consistency matters for maintaining muscle creatine saturation. Missing one day occasionally is not a problem. Missing 2-3 days every week will reduce your muscle creatine stores and diminish the supplement benefit.
If your semaglutide injection schedule conflicts with your creatine routine, the timing of your semaglutide shot can be adjusted in consultation with your healthcare provider to find a schedule that works for both.
Comparing creatine to other muscle preservation supplements on semaglutide
Creatine is not the only supplement that may help preserve muscle during GLP-1 therapy. Here is how it compares to other commonly discussed options:
Supplement | Evidence strength | Muscle preservation | Ease of use | Cost | GI tolerance |
|---|---|---|---|---|---|
Creatine monohydrate | Very strong | High | Very easy | Low | Good |
Whey protein | Very strong | High | Easy | Moderate | Variable |
HMB | Moderate | Moderate | Easy | Moderate | Good |
Essential amino acids | Moderate | Moderate | Easy | Moderate | Good |
L-carnitine | Weak-moderate | Low-moderate | Easy | Moderate | Good |
Vitamin D | Moderate (if deficient) | Low-moderate | Very easy | Low | Good |
Creatine and whey protein sit at the top of this list for good reason. They have the strongest evidence bases, the most practical benefits, and the best cost-to-benefit ratios. If you can only add two supplements to your GLP-1 protocol, make them creatine and a quality protein powder.
HMB (beta-hydroxy-beta-methylbutyrate) deserves mention because it specifically targets muscle protein breakdown. A metabolite of leucine, HMB may reduce muscle catabolism during caloric restriction. Some practitioners recommend stacking creatine and HMB for maximum muscle preservation. The evidence for this combination is promising but not as robust as creatine alone.
L-carnitine with semaglutide is another popular combination, though its primary mechanism relates to fat oxidation rather than direct muscle preservation. It may complement creatine, but should not replace it if muscle preservation is the priority.
Special considerations for different populations
Women on semaglutide
Women benefit from creatine supplementation just as much as men, but many women avoid creatine because of concerns about looking "bulky" or gaining water weight. The reality: creatine does not make women bulky. It helps preserve the lean tissue that keeps metabolism high and supports bone density, both of which are especially important during significant weight loss.
Women also tend to have lower baseline creatine stores than men, which means they may benefit disproportionately from supplementation. A 3-gram daily dose is typically sufficient for women under 70 kg. If you are concerned about semaglutide and menstrual effects, creatine does not interact with hormonal regulation in any meaningful way.
Older adults on semaglutide
Older adults face an elevated risk of sarcopenia (age-related muscle loss) that compounds with semaglutide-induced lean mass reduction. For adults over 50, creatine supplementation combined with resistance training is arguably even more important than for younger users. The meta-analyses in this age group show clear benefits for lean mass preservation and functional strength.
If you are an older adult on semaglutide, your protein target should be at the higher end of the range (2.0-2.2 grams per kg body weight), and creatine should be considered a baseline supplement, not an optional add-on. Your semaglutide dosage may also need more careful titration to balance weight loss with muscle preservation.
People with existing kidney concerns
If you have diagnosed kidney disease (stage 3 or higher), discuss creatine supplementation with your nephrologist before starting. While meta-analyses show no adverse renal effects in healthy individuals, the data in people with established kidney disease is limited. Semaglutide itself may have kidney-protective effects (as shown in the FLOW trial), but the combination with creatine in this population has not been studied.
If you have mild kidney impairment (stage 1-2) with stable function, creatine at standard doses is generally considered safe. But monitoring is appropriate, and your healthcare team should know about all supplements you are taking.
Real-world protocols: putting it all together
Protocol 1: beginner (just starting semaglutide)
Weeks 1-4 (semaglutide 0.25mg): Focus on adjusting to semaglutide. No creatine yet. Establish your first-week semaglutide routine, get GI side effects under control, and start a resistance training habit with 2 sessions per week.
Weeks 5-8 (semaglutide 0.5mg): Introduce creatine at 3 grams daily with your largest meal. Continue resistance training, increasing to 3 sessions per week. Focus on hitting protein targets of 1.6 grams per kg bodyweight.
Weeks 9+ (semaglutide 1.0mg+): Increase creatine to 5 grams daily if tolerated. Maintain 3-4 resistance training sessions weekly. Increase protein target to 2.0 grams per kg bodyweight. Track body composition, not just scale weight.
Protocol 2: experienced (already on stable semaglutide dose)
If you are already on a stable semaglutide dose and want to add creatine:
Week 1: Start with 3 grams creatine monohydrate daily, taken with your post-workout meal (or largest meal on non-training days).
Week 2: Increase to 5 grams daily if GI tolerance is good.
Week 3+: Maintain 5 grams daily. Full muscle creatine saturation will be reached by weeks 3-4. You should notice improved training performance, particularly on compound lifts, and better recovery between sessions.
Ongoing: Continue indefinitely. Creatine does not need to be cycled. The benefits accumulate and maintain as long as supplementation continues. If you stop, muscle creatine stores deplete over 4-6 weeks and the benefits gradually diminish.
Protocol 3: transitioning between GLP-1 medications
If you are switching from tirzepatide to semaglutide or switching from semaglutide to tirzepatide, maintain your creatine supplementation through the transition. Do not stop creatine just because you are changing medications. Muscle preservation is important regardless of which GLP-1 agonist you use.
During the transition period, you may experience renewed GI symptoms as your body adjusts to the new medication. If this happens, temporarily reduce creatine to 3 grams daily until symptoms stabilize, then return to 5 grams.
Frequently asked questions
Will creatine make me gain weight on semaglutide?
Creatine causes 1-3 kg of intracellular water retention in muscle tissue. This shows up on the scale but is not fat gain. Your fat loss from semaglutide continues unchanged. Track waist circumference alongside scale weight for a more accurate picture of your progress.
Can creatine cause kidney damage when combined with semaglutide?
No documented evidence shows kidney damage from creatine in healthy individuals, and there is no known interaction between creatine and semaglutide that would increase kidney risk. However, stay adequately hydrated and inform your healthcare provider about creatine supplementation before blood work.
Should I take creatine on days I do not exercise?
Yes. Creatine works through muscle saturation, which requires daily consistent intake regardless of training schedule. Take 5 grams daily, every day, with food.
Does creatine interact with semaglutide in any way?
No pharmacological interaction exists between creatine monohydrate and semaglutide. They work through completely different mechanisms and metabolic pathways. They are safe to take together.
How long does it take for creatine to work on semaglutide?
Without a loading phase, muscle creatine stores reach full saturation in approximately 3-4 weeks of daily 5-gram dosing. You may notice improved training performance within 1-2 weeks. The muscle preservation benefits accumulate over time and are most apparent after 8-12 weeks of consistent use combined with resistance training.
What is the best form of creatine for semaglutide users?
Micronized creatine monohydrate. It dissolves better, is easier on the stomach, and has the strongest evidence base. Avoid creatine hydrochloride, buffered creatine, or liquid creatine, as none have superior evidence and some may cause more GI issues.
Can I mix creatine in my protein shake?
Absolutely. Mixing creatine into a protein shake is one of the easiest ways to get both supplements in a single serving. The protein and carbohydrates in the shake may actually enhance creatine uptake. This is an especially good strategy for semaglutide users who struggle with appetite and want to maximize nutrition in fewer eating opportunities.
Should I stop creatine before blood work?
If your blood work includes a creatinine-based kidney function test, you have two options: stop creatine 3-5 days before the draw for an accurate creatinine reading, or continue creatine and ask your doctor to use a cystatin C test for kidney function assessment instead.
Is 3 grams of creatine enough, or do I need 5 grams?
Three grams daily will eventually saturate muscle creatine stores, but it takes longer and may not maintain full saturation in larger individuals. Five grams is the standard research dose used in most clinical trials. For most semaglutide users, 5 grams daily is the recommended target unless GI issues require starting lower.
Can creatine help with semaglutide fatigue?
Creatine may indirectly help with semaglutide-related fatigue by improving exercise performance and recovery. Creatine also plays a role in brain energy metabolism, and some research suggests it may support cognitive function. However, it is not a direct treatment for fatigue. If fatigue is a major issue, address hydration, nutrition, sleep, and semaglutide management strategies first.
What about creatine and semaglutide for body recomposition?
Body recomposition, losing fat while gaining muscle simultaneously, is the holy grail of fitness. It is difficult under normal circumstances and even more challenging during the significant caloric deficit semaglutide creates. But it is not impossible, especially for certain populations.
Beginners to resistance training may achieve modest body recomposition on semaglutide with creatine. The combination of a new training stimulus, adequate protein, and creatine supplementation can support muscle growth even in a caloric deficit for people whose muscles have not been exposed to regular resistance training before.
For experienced lifters, true recomposition on semaglutide is unlikely. The caloric deficit is simply too large. But what creatine and resistance training can achieve is something almost as good: maximum fat loss with minimal muscle loss. The end result looks similar to recomposition in the mirror because you lose fat without losing the muscle definition underneath.
If your goal is body recomposition rather than just weight loss, your semaglutide diet plan needs to prioritize protein above all else, and your training needs to include progressive overload. Creatine supports both sides of this equation by preserving existing muscle while allowing you to train hard enough to stimulate new growth (or at minimum, maintain what you have).
Tracking your semaglutide before and after results with photos and measurements, not just scale weight, will give you the best picture of whether your protocol is working for body composition rather than just total weight loss.
The bigger picture: semaglutide is not just about weight loss
Here is something that gets lost in the conversation about semaglutide and muscle loss. The goal of semaglutide therapy is not just to weigh less. It is to be healthier. And health is not determined by the number on the scale. It is determined by body composition, metabolic function, physical capability, and long-term sustainability.
Losing 20 kg of pure fat while maintaining all your muscle mass produces a dramatically different health outcome than losing 15 kg of fat and 5 kg of muscle. The first scenario gives you a faster metabolism, stronger bones, better functional capacity, and a much lower risk of weight regain. The second scenario gives you a slower metabolism, reduced bone density, less physical capability, and a higher risk of regaining everything you lost.
Creatine is a 15-cent-per-day supplement that can meaningfully shift your outcome toward the first scenario. Combined with adequate protein, consistent resistance training, and the right nutritional choices on semaglutide, it represents one of the highest-value additions to a GLP-1 weight loss protocol.
If you are on semaglutide and you are not taking creatine, the question is not whether you should start. The question is why you have not started yet.
For researchers and users serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides covering everything from semaglutide dosing and supplement stacking to week-by-week result tracking and long-term weight maintenance strategies. SeekPeptides members access detailed protocols, dosing calculators, and expert guidance designed specifically for people navigating GLP-1 therapy.
External resources
Dietary supplement considerations during GLP-1 receptor agonist treatment: a narrative review (PMC)
Effect of creatine supplementation on kidney function: systematic review and meta-analysis (PMC)
A short review of the most common safety concerns regarding creatine ingestion (PMC)
Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes (NEJM)
In case I do not see you, good afternoon, good evening, and good night. May your creatine stay saturated, your muscles stay intact, and your semaglutide results stay transformative.