Apr 2, 2026

That burning sensation behind your breastbone after your weekly injection is not in your head. It is real, it is common, and it is one of the most underreported side effects of tirzepatide therapy. While nausea and constipation get most of the attention in clinical discussions, heartburn quietly affects somewhere between 4% and 14% of people taking this medication, and many never mention it to their healthcare provider because they assume it is just part of the process.
It does not have to be.
Heartburn on tirzepatide has specific causes, predictable timing, and proven solutions. The medication slows gastric emptying as part of how it works, which creates conditions that can push stomach acid upward into the esophagus. Understanding exactly why this happens gives you a clear path to managing it, often without changing your dose or stopping the medication entirely. This guide covers everything from the clinical data behind tirzepatide-related heartburn to the dietary adjustments, over-the-counter options, and lifestyle strategies that researchers and clinicians have found most effective. Whether you are dealing with mild occasional burning or persistent acid reflux that is disrupting your daily routine, the answers are here.
Why tirzepatide causes heartburn in the first place
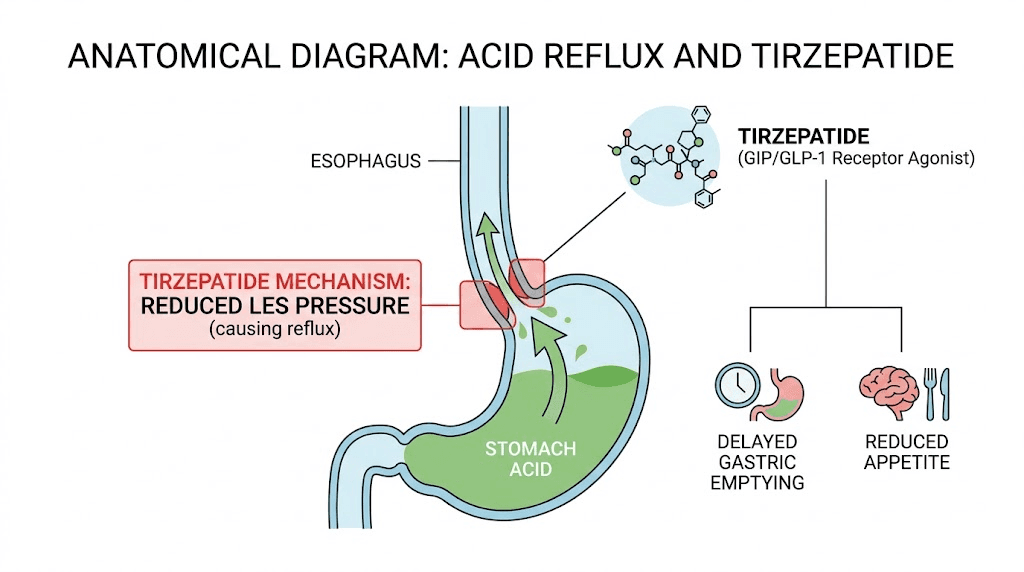
The mechanism is straightforward once you understand what tirzepatide does inside the digestive system. This medication activates both GLP-1 and GIP receptors, which among other effects suppresses appetite and significantly slows the rate at which your stomach empties its contents into the small intestine. That delayed gastric emptying is actually central to how tirzepatide produces weight loss. Food stays in the stomach longer, you feel full for extended periods, and you naturally eat less.
But there is a cost.
When food sits in the stomach for longer than usual, intragastric pressure increases. That pressure pushes upward against the lower esophageal sphincter, the muscular valve that normally keeps stomach acid contained. If that sphincter relaxes even slightly under the additional pressure, acidic stomach contents flow backward into the esophagus. That backward flow is what you feel as heartburn, that characteristic burning sensation behind the sternum that sometimes radiates up toward the throat.
Research published in the American College of Gastroenterology journal confirmed this connection, finding that GLP-1 receptor agonists are associated with increased risk of gastroesophageal reflux in susceptible patients. Importantly, the studies show that tirzepatide does not increase stomach acid production itself. The amount of acid your stomach makes stays roughly the same. The problem is purely mechanical, acid ending up where it should not be because food is not moving through quickly enough.
The dose escalation factor
Heartburn tends to appear or worsen during specific windows of tirzepatide dose escalation. When you move from 2.5mg to 5mg, or from 5mg to 7.5mg, your body adjusts to a stronger effect on gastric emptying. That adjustment period is when reflux symptoms are most likely to surface. According to SURMOUNT trial data, gastrointestinal side effects including heartburn were most pronounced during these dose transition periods and typically improved within 4 to 8 weeks at a stable dose.
This pattern matters because it tells you something important. If heartburn appears right after a dose increase, there is a good chance it will improve on its own as your body adapts. That does not mean you should ignore it, but it does mean the trajectory is often favorable.
Pre-existing conditions that raise your risk
Not everyone on tirzepatide gets heartburn. Several factors increase your likelihood significantly:
History of GERD or acid reflux, even if it was well-controlled before starting tirzepatide
Hiatal hernia, which already weakens the lower esophageal sphincter
Obesity, which increases abdominal pressure (though this improves as you lose weight on the medication)
Smoking, which relaxes the esophageal sphincter
Certain medications like NSAIDs, calcium channel blockers, or bisphosphonates that independently increase reflux risk
Eating large meals or eating close to bedtime
If you had occasional heartburn before starting tirzepatide, the medication can amplify it significantly during the early weeks. Knowing this ahead of time lets you take preventive steps before the first dose.
How common is heartburn on tirzepatide compared to other side effects
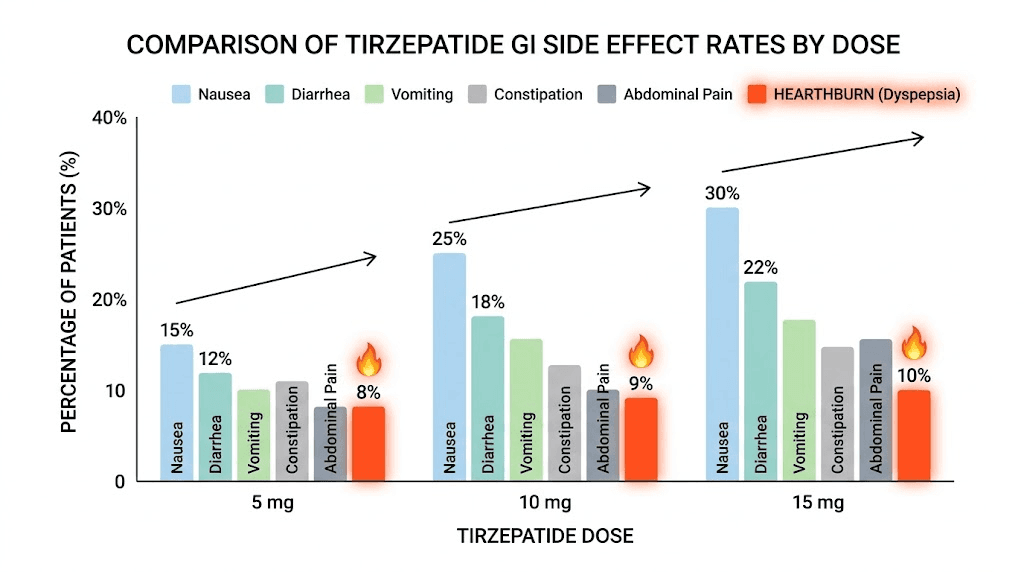
Clinical trial data from the SURMOUNT program gives us concrete numbers. Here is where heartburn and acid reflux fall compared to the other gastrointestinal side effects of tirzepatide:
Side effect | 5mg dose | 10mg dose | 15mg dose |
|---|---|---|---|
Nausea | 24.6% | 33.3% | 31.0% |
18.7% | 21.2% | 23.0% | |
16.8% | 17.1% | 11.7% | |
Vomiting | 8.3% | 10.7% | 12.2% |
Heartburn/GERD | ~4% | ~8-10% | ~10-14% |
~5% | ~7% | ~8% |
The numbers tell an interesting story. Heartburn is less common than nausea or diarrhea but more common than many people expect. It falls in the same range as other underreported side effects like feeling cold, increased thirst, and dry mouth. The 10mg dose appears to be a particular inflection point, with heartburn rates roughly doubling compared to the 5mg dose. At the highest approved dose of 15mg, somewhere around 1 in 7 to 1 in 10 users reports some degree of acid reflux or heartburn.
What the raw numbers do not capture is severity. Most heartburn cases on tirzepatide fall into the mild to moderate range. Severe, persistent GERD that requires medication changes or discontinuation affects approximately 2% or fewer patients across all dose levels. So while heartburn is common enough to warrant attention, it is rarely a deal-breaker for continued therapy.
When heartburn typically starts and how long it lasts
Timing matters. Knowing when to expect heartburn and how long it typically persists helps you plan your management strategy and decide when something might need medical attention.
The typical timeline
Week 1-2 after starting or increasing dose: This is the highest-risk window. Your body is adjusting to the new level of gastric slowing. Many people who will experience heartburn notice it within the first 10 days of a dose change. Some feel it after their very first injection.
Weeks 2-4: Symptoms often peak during this period, especially if you have not yet implemented dietary or lifestyle changes. The appetite suppression is strong during this window, which paradoxically can help, you eat less, which means less food in the stomach to generate acid.
Weeks 4-8: Most people see significant improvement by this point. The gastrointestinal system adapts to the new rate of gastric emptying, and the lower esophageal sphincter adjusts. If you have been following the dietary recommendations in this guide, heartburn often becomes occasional rather than persistent.
Beyond 8 weeks at a stable dose: If heartburn persists unchanged beyond 8 weeks at the same dose, that suggests it may not self-resolve and warrants discussion with your healthcare provider about management strategies or dose adjustment.
The dose escalation reset
Here is what catches many people off guard. You manage heartburn at 5mg, it goes away, and then you move up to 7.5mg and it comes back. Each dose increase can reset the clock on gastrointestinal adaptation. The good news is that each subsequent adjustment period tends to be shorter and less severe than the initial one because your body has already partially adapted to the mechanism of gastric slowing.
Some clinicians recommend extending dose escalation intervals specifically for patients prone to GI side effects. Instead of increasing every 4 weeks as the standard protocol suggests, staying at each dose for 6 to 8 weeks can reduce the severity of heartburn during transitions. This is particularly relevant if you are using a compounded tirzepatide formulation where dose adjustments are more flexible.
Immediate relief strategies that actually work
When heartburn strikes, you want it gone. Fast. Here are the evidence-based options ranked by speed and effectiveness.
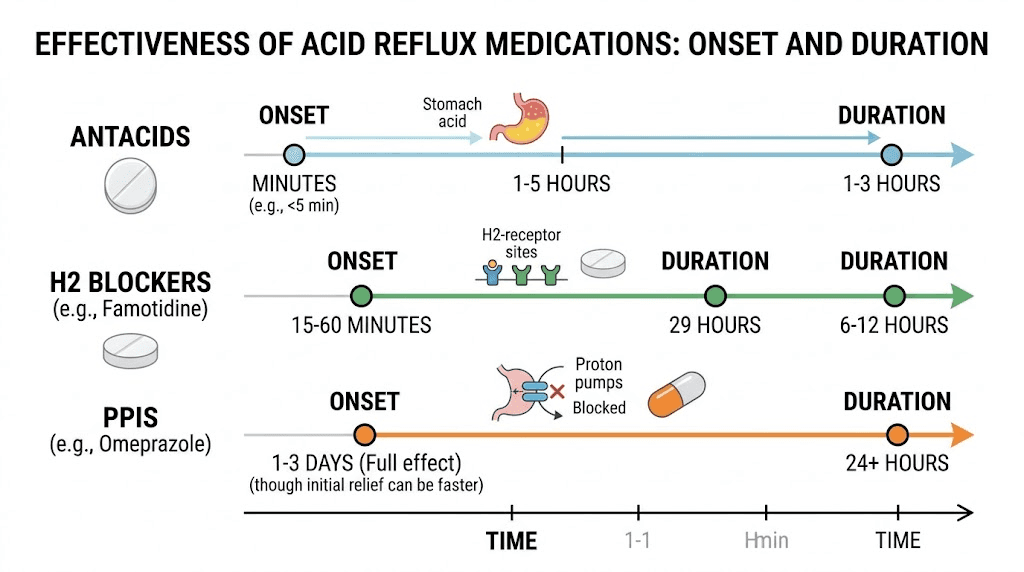
Over-the-counter antacids
Antacids like calcium carbonate (Tums), magnesium hydroxide (Milk of Magnesia), or aluminum hydroxide neutralize stomach acid directly. They work within 5 to 15 minutes. That speed makes them the best option for acute episodes.
The limitation is duration. Most antacids provide 30 to 60 minutes of relief. For occasional heartburn after meals, that is often enough. For persistent reflux, you need something longer-acting.
One important note: calcium-based antacids can contribute to constipation, which is already a common side effect of tirzepatide. If constipation is also an issue for you, magnesium-based antacids are a better choice since magnesium has a mild laxative effect.
H2 receptor blockers
Famotidine (Pepcid) and cimetidine reduce acid production by blocking histamine receptors in the stomach lining. They take 30 to 60 minutes to start working but provide 6 to 12 hours of relief. This makes them ideal for predictable heartburn, like the kind that hits every evening after dinner.
Taking famotidine 30 minutes before your evening meal can preempt heartburn before it starts. Many tirzepatide users find this approach more practical than waiting for symptoms and then treating reactively.
Proton pump inhibitors
PPIs like omeprazole (Prilosec), lansoprazole (Prevacid), and esomeprazole (Nexium) are the most powerful acid-reducing medications available without a prescription. They block the proton pumps in stomach lining cells that produce acid, reducing acid output by up to 90%.
The catch is timing. PPIs take 1 to 4 days to reach full effectiveness. They are not rescue medications for acute heartburn. They are preventive tools for ongoing management. The American College of Gastroenterology recommends PPIs as first-line therapy for moderate to severe reflux symptoms.
If your heartburn is occurring more than twice per week while on tirzepatide, a 2-week course of an OTC PPI is a reasonable starting point. Talk to your healthcare provider if symptoms persist beyond that, as they may want to evaluate for GERD or other complications.
Dietary changes that make the biggest difference
Medication can control symptoms. Diet can prevent them. The combination of both is what most successful tirzepatide users rely on to eliminate heartburn entirely.
Foods that trigger heartburn on tirzepatide
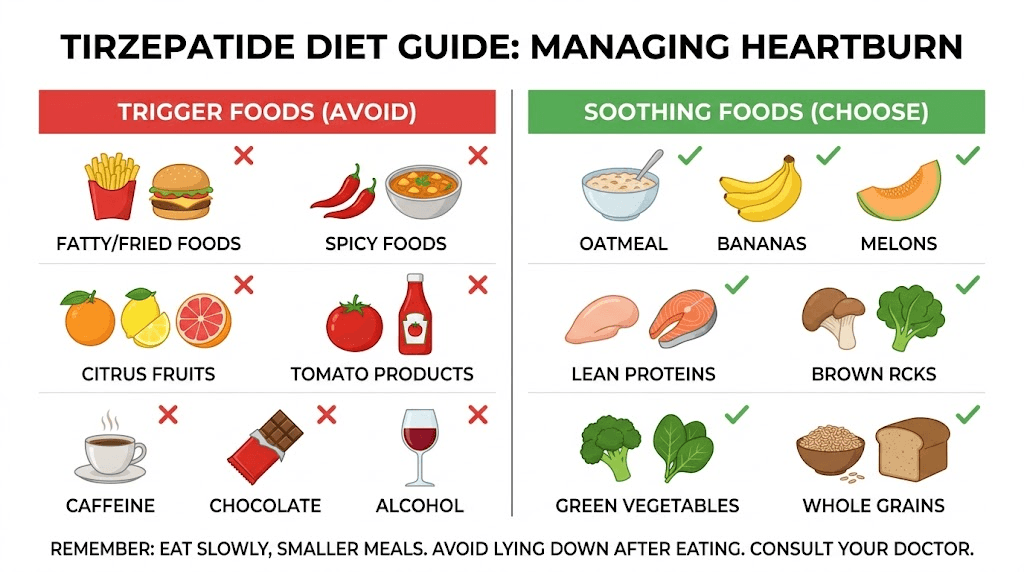
Some foods relax the lower esophageal sphincter, increase acid production, or slow gastric emptying further. When your stomach is already emptying slowly from tirzepatide, these foods compound the problem. The biggest offenders, based on both gastroenterology research and reports from tirzepatide users:
High-fat foods are the single worst trigger. Fat slows gastric emptying independently of tirzepatide, stacking on top of the medication effect. Fried foods, fatty cuts of meat, heavy cream sauces, and butter-heavy dishes should be the first things you reduce. This aligns with the broader food avoidance guidelines for tirzepatide users.
Acidic foods like tomatoes, tomato-based sauces, citrus fruits, and vinegar-based dressings directly irritate an already-inflamed esophageal lining. If you already have heartburn, these make it worse. If you do not have heartburn yet, these can trigger the first episode.
Spicy foods irritate the esophageal and stomach lining, increasing the sensation of burning even if acid levels are normal. Capsaicin in particular can relax the lower esophageal sphincter.
Caffeine and chocolate both relax the lower esophageal sphincter. Coffee is a double problem because it also increases acid secretion. If you are a heavy coffee drinker experiencing heartburn on tirzepatide, reducing intake to one morning cup or switching to a low-acid variety can make a noticeable difference.
Carbonated beverages introduce gas into the stomach, increasing intragastric pressure. This is the same pressure mechanism that tirzepatide itself creates through delayed emptying. The combination can push acid upward more forcefully. If you enjoy sparkling water, try still water for a few weeks and see if symptoms improve.
Alcohol relaxes the esophageal sphincter, increases acid production, and irritates the stomach lining directly. It is a triple threat for heartburn. Our guide on drinking on tirzepatide covers this in detail. If you do choose to drink occasionally, our guide on the best alcohol choices on tirzepatide identifies options that are least likely to trigger reflux. But in the context of heartburn specifically, alcohol reduction is one of the most impactful single changes you can make.
Peppermint is a surprising one. While it helps nausea (which is why many tirzepatide users reach for it), peppermint relaxes the lower esophageal sphincter and can worsen heartburn. If nausea and heartburn coexist, ginger is a safer alternative.
Foods that help reduce heartburn
It is not all about avoidance. Certain foods actively help manage acid reflux while supporting your tirzepatide diet plan:
Lean proteins like chicken breast, fish, turkey, and egg whites are easy to digest and do not trigger reflux. They also support the high-protein intake that is critical for preserving muscle mass during GLP-1 mediated weight loss. Protein shakes can be an especially good option since they are already partially broken down and move through the stomach more easily.
Non-citrus fruits like bananas, melons, apples, and pears are naturally low in acid and unlikely to trigger symptoms. Bananas in particular have a mild antacid effect.
Vegetables are almost universally safe for heartburn sufferers. Green beans, broccoli, asparagus, cauliflower, and leafy greens are excellent choices. Root vegetables like sweet potatoes and carrots also work well. Check our complete guide to eating on tirzepatide for full meal planning ideas.
Whole grains like oatmeal, brown rice, and whole wheat bread absorb stomach acid and are high in fiber, which promotes digestive regularity. Oatmeal specifically is one of the most recommended breakfast options for people managing both tirzepatide therapy and acid reflux. Our GLP-1 breakfast ideas guide has several oatmeal-based options, and our dinner ideas for GLP-1 users features heartburn-friendly evening meals. The complete GLP-1 recipe collection includes dozens of options that work well for acid reflux management.
Ginger has natural anti-inflammatory properties and has been shown in multiple studies to reduce nausea and improve gastric motility. A small amount of fresh ginger in tea or meals can help heartburn without the sphincter-relaxing effects of peppermint.
Meal timing and portion strategies
How you eat matters as much as what you eat. These timing strategies are specifically designed for the delayed gastric emptying that tirzepatide creates:
Eat smaller, more frequent meals. Three large meals create more intragastric pressure than five smaller ones. Since tirzepatide already reduces appetite, most users naturally eat less at each sitting. Lean into that tendency rather than trying to force three full meals. Your tirzepatide meal plan should reflect this smaller-more-frequent approach.
Stop eating at least 3 hours before lying down. This is the single most important timing rule. With tirzepatide slowing gastric emptying, food stays in your stomach longer than it would otherwise. If you eat dinner at 7pm and go to bed at 10pm, your stomach may still contain significant food volume when you lie flat. That horizontal position removes gravity from the equation, making reflux almost inevitable.
Do not eat right after your injection. Some users report that nausea and heartburn are worst on injection day and the day after. If this pattern applies to you, keep meals especially small and bland during that 24 to 48 hour window. The best time to take your tirzepatide shot can be adjusted to minimize overlap with your largest meals.
Eat slowly and chew thoroughly. Rushing through meals introduces more air into the stomach and sends larger food particles into a digestive system that is already working at reduced speed. Taking 20 to 30 minutes per meal significantly reduces post-meal heartburn.
Lifestyle changes beyond diet
Diet gets the most attention, but several non-dietary factors have equal or greater impact on heartburn management while taking tirzepatide.
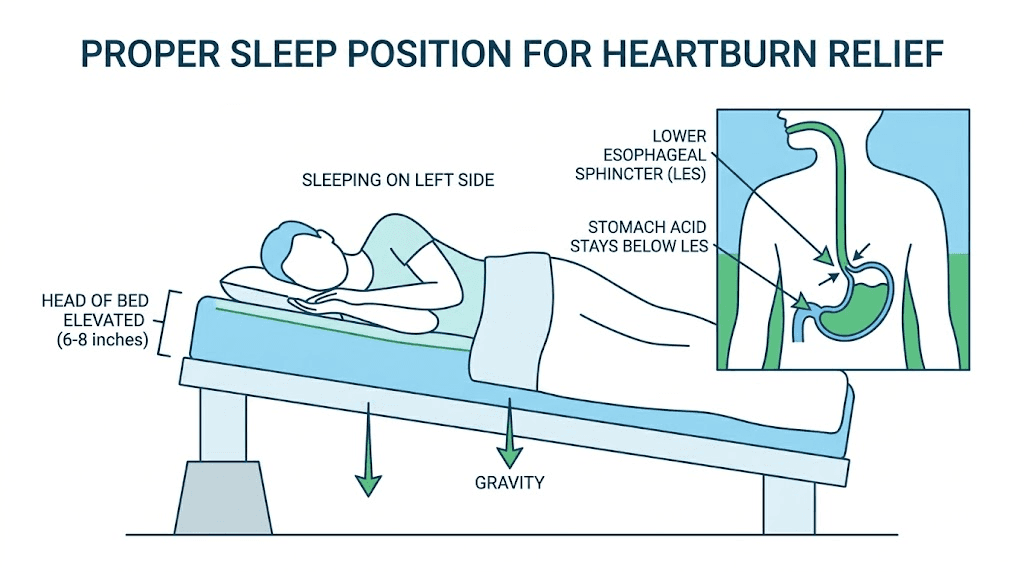
Elevate the head of your bed
This is the most underrated heartburn intervention. Raising the head of your bed by 6 to 8 inches (using bed risers under the headboard legs, not extra pillows) keeps gravity working in your favor while you sleep. Studies consistently show that bed elevation reduces nighttime reflux episodes by 60% to 70%. Extra pillows alone are not as effective because they bend you at the waist rather than elevating the entire upper body, which can actually increase abdominal pressure.
Watch your clothing
Tight waistbands, compression garments, and snug belts increase intra-abdominal pressure. If you are losing weight on tirzepatide (which most users do within the first few weeks), your existing clothes may become loose enough that this stops being a factor. But during the transition period, choose loose-fitting clothing around the midsection.
Do not lie down after eating
Beyond the 3-hour pre-bedtime rule, avoid lying down on the couch after meals. If you need to rest, recline at a 45-degree angle or higher. Better yet, take a gentle 15 to 20 minute walk after eating. Light post-meal movement actually promotes gastric emptying, partially counteracting tirzepatide-induced slowing, and keeps the esophageal sphincter in a favorable position.
Manage stress
Stress increases stomach acid production and sensitizes the esophageal lining to pain. The combination of stress and tirzepatide-induced delayed emptying creates an unfavorable environment for acid reflux. Basic stress management, whether that is meditation, exercise, adequate sleep, or simply reducing unnecessary commitments, has a measurable effect on heartburn frequency. This is particularly relevant because tirzepatide and anxiety can interact in ways that compound stress-related GI symptoms.
Stop smoking
Smoking directly relaxes the lower esophageal sphincter, increases acid production, reduces saliva (which normally neutralizes esophageal acid), and damages the esophageal lining. If you smoke and have heartburn on tirzepatide, quitting may resolve symptoms entirely without any other intervention. No other single change has as dramatic an effect on acid reflux as smoking cessation. The metabolic benefits are compounding, since tirzepatide already boosts metabolism, and quitting smoking further improves cardiovascular and metabolic health.
Optimize your sleep position
Sleeping on your left side reduces reflux episodes compared to sleeping on your right side or your back. The anatomical explanation is that the stomach curves to the left, so lying on the left side keeps the gastroesophageal junction above the level of stomach contents. Combined with bed elevation, left-side sleeping is a powerful nighttime heartburn strategy. This is worth noting if tirzepatide-related insomnia is already disrupting your sleep, as heartburn can make sleep quality even worse.
Supplements and complementary approaches
Several supplements show evidence for heartburn management. Here is what the research supports and what it does not.
What works
Ginger (250-500mg, 2-3 times daily): Multiple clinical studies support ginger for nausea and mild reflux. It accelerates gastric emptying slightly, which directly addresses the mechanism behind tirzepatide-related heartburn. Fresh ginger tea or standardized ginger capsules are both effective forms.
Melatonin (3-6mg at bedtime): An underappreciated option. Research published in BMC Gastroenterology found that melatonin at 3-6mg nightly reduced GERD symptoms comparably to omeprazole in some patients. Melatonin strengthens the lower esophageal sphincter and reduces acid secretion. The sleep benefits are an added bonus, particularly for those experiencing fatigue on tirzepatide.
Probiotics: Emerging evidence suggests certain probiotic strains (particularly Lactobacillus and Bifidobacterium species) improve upper GI symptoms including reflux. While the evidence is not as strong as for PPIs, probiotics carry essentially zero risk and may help with multiple GI symptoms simultaneously, including the bloating that often accompanies heartburn.
Fiber supplements: Adequate fiber intake promotes regular gastric motility and can help food move through the system more efficiently, even with tirzepatide-induced slowing. Psyllium husk is particularly well-studied for upper GI symptom improvement. Start with small doses and increase gradually to avoid gas and bloating.
What does not work (despite popular claims)
Apple cider vinegar: The theory that heartburn is caused by too little acid (and therefore ACV helps) has no scientific support. In people with tirzepatide-induced reflux, the problem is acid in the wrong place, not insufficient acid. ACV can actually irritate an already-inflamed esophagus.
Baking soda (as a long-term strategy): While baking soda does neutralize acid instantly, the high sodium content makes regular use problematic. It can also cause rebound acid production. Occasional use in an emergency is fine, but it should not be your go-to remedy.
Milk: The calcium and protein in milk do briefly buffer stomach acid, but the fat content stimulates more acid production within 30 minutes. The net effect is often worse heartburn than before you drank it.
The supplement stack that works with tirzepatide
For users managing multiple GI symptoms while on tirzepatide, this combination addresses heartburn while supporting overall digestive health. The supplements to take with tirzepatide guide covers the full picture, but for heartburn specifically:
Morning: Probiotic on empty stomach, fiber supplement with breakfast
Before dinner: Ginger capsule 30 minutes before eating
Bedtime: Melatonin 3mg
As needed: Magnesium-based antacid for breakthrough symptoms
This approach targets the problem from multiple angles, improving gastric motility, strengthening the esophageal sphincter, reducing acid exposure, and providing acute relief when needed.
When heartburn on tirzepatide signals something more serious
Most heartburn on tirzepatide is benign and manageable. But certain patterns warrant immediate medical attention.
Red flags you should not ignore
Difficulty swallowing (dysphagia): If food feels like it is getting stuck or you have trouble swallowing liquids, this could indicate esophageal narrowing from chronic acid exposure. Seek medical evaluation promptly.
Vomiting blood or material that looks like coffee grounds: This indicates upper GI bleeding and requires immediate emergency care.
Black, tarry stools: Another sign of GI bleeding further down the digestive tract. Do not wait on this one.
Unintentional weight loss beyond what tirzepatide would explain: If you are losing weight faster than expected (beyond the typical tirzepatide weight loss timeline), particularly with persistent heartburn, there may be an underlying condition that needs investigation.
Chest pain that radiates to the arm, jaw, or back: Heartburn and cardiac events can feel similar. If you have any doubt, call emergency services. It is always better to have heartburn diagnosed as heartburn than to dismiss a cardiac event as reflux.
Persistent symptoms despite 2 weeks of PPI therapy: If omeprazole or similar medications are not controlling your heartburn, your provider may want to perform an endoscopy or pH monitoring to evaluate for complications like Barrett esophagus or esophageal stricture.
Symptoms that wake you from sleep regularly: Nighttime reflux that disrupts sleep despite bed elevation and dietary timing suggests more severe GERD that may require prescription-strength management.
GERD versus occasional heartburn
Occasional heartburn is normal. Everyone gets it from time to time, whether they take tirzepatide or not. GERD is something different, a chronic condition where reflux occurs frequently enough to damage the esophageal lining.
The general clinical threshold is heartburn occurring more than twice per week for several weeks. If your tirzepatide-related heartburn crosses that line and does not respond to the lifestyle and OTC medication strategies outlined above, a gastroenterology evaluation is appropriate. Eli Lilly medical information specifically notes that tirzepatide has not been studied in patients with severe GERD, so close monitoring is warranted in this population.
Should you adjust your tirzepatide dose for heartburn
This is the question everyone wants answered. And the answer depends on severity, timing, and how well other management strategies are working.
When dose adjustment is not necessary
Mild to moderate heartburn that responds to dietary changes, lifestyle modifications, or OTC medications does not require a dose change. The weight loss and metabolic benefits of tirzepatide at your current dose are significant, and reducing the dose to manage a symptom that can be controlled through other means is usually not the best trade-off.
If your heartburn appeared during dose escalation and is gradually improving, stay the course. The adaptation period is temporary. Use the strategies in this guide to manage symptoms while your body adjusts.
When dose adjustment makes sense
Severe heartburn that does not respond to 4 to 6 weeks of aggressive management (dietary changes plus OTC medications) at a particular dose may warrant stepping back. This does not necessarily mean abandoning tirzepatide. Options include:
Returning to the previous dose: If heartburn appeared at 10mg but was absent at 7.5mg, stepping back to 7.5mg for a longer period before attempting escalation again often works. Many users still achieve excellent weight loss at moderate doses. Our tirzepatide dosage calculator can help determine if a lower dose still meets your goals.
Slower titration: Instead of increasing every 4 weeks, extending to 8 or even 12 weeks between dose increases gives the GI system more time to adapt. This is one advantage of using microdosed tirzepatide or split dosing, where smaller amounts are administered more frequently to reduce peak drug concentration.
Dose splitting: Some clinicians have patients split their weekly dose into two smaller injections given 3 to 4 days apart. This produces more stable drug levels with less peak-related GI distress. The microdose tirzepatide schedule guide covers various splitting approaches.
When to consider switching medications
Rarely, some individuals simply cannot tolerate tirzepatide at any effective dose due to persistent heartburn or GERD. In these cases, switching to semaglutide may be an option. Semaglutide and tirzepatide side effect profiles differ in important ways. While semaglutide also causes GI side effects, its single-receptor mechanism (GLP-1 only, versus tirzepatide dual GLP-1/GIP action) produces a different pattern of gastric effects that some people tolerate better.
Our guide on switching from tirzepatide to semaglutide covers the conversion process, expected differences, and what to discuss with your healthcare provider. The semaglutide vs tirzepatide comparison page provides a comprehensive side-by-side analysis, and the conversion chart maps equivalent doses between the two medications. Some users also explore alternating between semaglutide and tirzepatide as a strategy to manage side effects while maintaining efficacy.
Exercise and heartburn on tirzepatide
Physical activity is a critical component of any weight loss protocol, and tirzepatide users who exercise regularly tend to achieve better results than those who rely on the medication alone. But exercise and heartburn have a complicated relationship that requires careful navigation.
Exercises that help heartburn
Low to moderate intensity activities performed in an upright position generally improve gastric motility and reduce reflux. Walking is the gold standard. A 15 to 20 minute walk after meals promotes gastric emptying, keeps the esophageal sphincter in a favorable position through upright posture, and burns additional calories to support your weight loss timeline.
Swimming can be helpful as the horizontal position is offset by the gentle compression of water and the rhythmic breathing patterns. Cycling, yoga (with modifications to avoid inversions and deep forward folds), and light resistance training are all generally well-tolerated.
Strength training deserves special mention. Building and preserving muscle mass during GLP-1 therapy is essential for maintaining metabolic rate and preventing the muscle loss that sometimes accompanies rapid weight loss. Our guide on building muscle while on GLP-1 covers the specifics. For heartburn management, the key is to avoid heavy lifting immediately after meals and to use controlled breathing (exhaling on exertion) rather than holding your breath, which increases intra-abdominal pressure.
Exercises that worsen heartburn
High-intensity exercise within 2 hours of eating is the most common exercise-related heartburn trigger on tirzepatide. Vigorous running, heavy squats and deadlifts, and HIIT workouts all increase intra-abdominal pressure significantly. The jarring motion of running can physically slosh stomach contents upward.
Exercises that involve lying flat or being inverted, like bench press, leg raises, or downward-facing yoga poses, put the esophageal sphincter below stomach level, inviting acid to flow the wrong direction. If these are part of your routine, schedule them for times when your stomach is as empty as possible, ideally first thing in the morning before eating or at least 3 hours after a meal.
The optimal exercise timing on tirzepatide
The best exercise window for heartburn prevention is mid-morning (if you have not eaten since a small breakfast 2 hours prior) or late afternoon (well after lunch). Avoid exercising on injection day and the day after if you are prone to GI symptoms during peak medication levels. The optimal injection timing can be coordinated with your exercise schedule to minimize conflicts.
If you experience heartburn during exercise despite timing it well, consider taking an antacid 30 minutes beforehand or switching to lower-intensity activities until your body adapts to the current dose level. Many users find that combining supplements like creatine with their tirzepatide protocol supports workout performance while managing side effects.
Medications that can worsen heartburn while on tirzepatide
Several common medications independently increase heartburn risk. When combined with tirzepatide-induced delayed gastric emptying, the cumulative effect can be significant. Review this list with your healthcare provider if heartburn is a persistent problem.
NSAIDs (ibuprofen, naproxen, aspirin): These directly irritate the stomach lining and can weaken the esophageal sphincter.
If you need pain relief while on tirzepatide, acetaminophen (Tylenol) is a safer choice for heartburn sufferers. This is particularly relevant if you are managing tirzepatide-related muscle pain or joint pain, as the instinct is often to reach for ibuprofen.
Calcium channel blockers: Used for blood pressure management, these medications (amlodipine, nifedipine) relax smooth muscle throughout the body, including the lower esophageal sphincter. If you take one of these and experience heartburn on tirzepatide, ask your provider about alternative blood pressure medications that do not affect the esophageal sphincter.
Bisphosphonates (alendronate, risedronate): Used for osteoporosis, these medications are known to cause esophageal irritation and must be taken upright with a full glass of water. The delayed gastric emptying from tirzepatide can extend their contact time with the esophageal lining. If you are concerned about bone loss on tirzepatide and taking bisphosphonates, timing becomes especially important.
Iron supplements: These are notorious GI irritants that cause nausea, constipation, and can worsen heartburn. If you need iron supplementation while on tirzepatide, liquid or chelated forms are generally better tolerated than standard ferrous sulfate tablets.
Certain antibiotics (tetracyclines, doxycycline): These can cause direct esophageal irritation, especially if they get stuck in the esophagus. Always take with a full glass of water and remain upright for at least 30 minutes afterward.
Potassium supplements: These can irritate the GI tract, particularly in pill form. Potassium-rich foods are generally better tolerated than supplements for maintaining electrolyte balance.
Heartburn management by tirzepatide dose level
Because heartburn risk and severity vary significantly across dose levels, your management approach should be calibrated to your current dose.
At 2.5mg (starting dose)
Heartburn at this dose is uncommon, affecting fewer than 3% of users. If it occurs, it is usually mild and responds well to basic dietary modifications alone. Most users at this dose do not need any medication for heartburn. This is the introductory period where you are establishing baseline habits that will serve you well at higher doses. Review what to expect after your first tirzepatide dose for the full picture.
At 5mg
Heartburn rates climb to roughly 4-6% at this dose. The increase in gastric slowing compared to 2.5mg is meaningful. Implementing the 3-hour pre-bedtime eating rule and reducing high-fat meals is usually sufficient. Have antacids available but you may not need them. This is also when appetite suppression becomes more noticeable, which naturally leads to smaller meals and potentially less reflux.
At 7.5mg
This is an intermediate dose that many compounded tirzepatide users land on. Heartburn rates reach approximately 6-8%. The microdosing approach can be particularly helpful at this level, where splitting the dose can reduce peak-related GI effects. Adding famotidine before your largest meal is a reasonable preventive measure if dietary changes alone are not controlling symptoms.
At 10mg
The 10mg dose represents a significant inflection point for GI side effects generally, and heartburn specifically. Rates reach 8-10% at this level. Most users who will experience heartburn on tirzepatide encounter it here. The full management protocol described earlier in this guide becomes relevant. PPIs may be needed for the first time during the adjustment to this dose. Consulting the comprehensive dose chart helps you understand what to expect.
At 12.5mg and 15mg
The highest approved doses carry heartburn rates of 10-14%. However, many users who have adapted through the lower doses find that incremental increases at this level produce less severe heartburn than the earlier jumps. The GI system has already partially adapted to delayed gastric emptying. If heartburn has been well-controlled at 10mg with your management protocol, adding a slightly more aggressive version of the same approach (perhaps adding melatonin or switching from H2 blockers to PPIs) often handles the 12.5mg and 15mg transitions.
For users on compounded formulations, the ability to titrate in smaller increments (10mg to 11mg to 12mg rather than jumping straight to 12.5mg) is a significant advantage for heartburn-prone individuals.
Heartburn on tirzepatide versus semaglutide
If you are choosing between these two medications, or considering a switch specifically because of heartburn, the comparison is relevant.
Both semaglutide and tirzepatide slow gastric emptying. Both can cause heartburn. But the mechanisms differ slightly because tirzepatide acts on two receptors (GLP-1 and GIP) while semaglutide acts on one (GLP-1 only). The dual-receptor action of tirzepatide may produce more pronounced gastric effects in some individuals, which could translate to higher heartburn rates.
However, research published in the Annals of Internal Medicine found an important nuance: longer-acting GLP-1 receptor agonists (which includes both tirzepatide and once-weekly semaglutide) were actually associated with lower GERD risk than shorter-acting versions like liraglutide. The sustained, steady receptor activation appears to be better tolerated than the repeated peaks and troughs of shorter-acting agents.
In the head-to-head dosage comparison, tirzepatide generally produces greater weight loss (15-22% vs 12-15% with semaglutide over 72 weeks). That additional efficacy comes with a modestly higher GI side effect profile overall. For most users, the greater weight loss more than justifies the additional GI management required. But for those with severe pre-existing GERD, starting with semaglutide and its slightly gentler GI profile may be the more pragmatic choice.
What your doctor should know about your heartburn
Coming prepared to your medical appointment makes a significant difference in the quality of care you receive. If heartburn is affecting your tirzepatide experience, here is what your provider needs to know and what you should ask.
Information to bring to your appointment
Symptom diary: At minimum, track heartburn frequency (episodes per week), timing (after meals, at night, on injection day), severity (1-10 scale), and what provides relief. Two weeks of data gives your provider enough pattern information to make meaningful recommendations.
Current medications and supplements: Include everything, prescription drugs, OTC medications, vitamins, and herbal supplements. As discussed earlier, several common medications interact with heartburn. Your provider cannot identify medication-related causes without a complete list. This is especially relevant if you are taking supplements alongside tirzepatide or combining it with other medications like metformin or berberine.
Your tirzepatide history: Current dose, when you started, dose escalation timeline, and when heartburn first appeared relative to dose changes. The temporal relationship between dose changes and symptom onset is often the most diagnostically useful piece of information.
Previous GERD history: Any history of acid reflux, hiatal hernia, or esophageal issues before starting tirzepatide. Pre-existing conditions change the management approach significantly.
Questions to ask your provider
Should I slow down my dose escalation? This is the most practical question for most heartburn sufferers. A provider who understands GLP-1 therapy knows that slower titration reduces GI side effects without compromising long-term weight loss outcomes.
Should I switch to a PPI? If OTC H2 blockers are not controlling symptoms, your provider can prescribe higher-strength PPIs or recommend specific OTC PPIs at therapeutic doses.
Do I need an endoscopy? If symptoms are persistent, severe, or accompanied by red flags (difficulty swallowing, unexplained weight loss beyond tirzepatide effects, vomiting), an endoscopic evaluation may be warranted. This is not something to worry about for typical mild heartburn, but it is an important conversation for severe cases.
Is this heartburn or something else? Chest burning has multiple potential causes. Your provider can distinguish tirzepatide-related reflux from cardiac issues, gallbladder problems (which blood work can help evaluate), esophageal spasm, or other conditions that might mimic heartburn.
A complete heartburn management protocol for tirzepatide users
Here is a step-by-step approach that integrates everything in this guide into a practical protocol. SeekPeptides members have access to even more detailed protocol builders, but this framework covers the essentials.
Phase 1: Prevention (start before or with your first dose)
Eliminate known trigger foods: high-fat foods, spicy dishes, citrus, caffeine, carbonation, alcohol
Adopt the 3-hour rule: no eating within 3 hours of lying down
Elevate the head of your bed 6-8 inches
Switch to 5-6 smaller meals instead of 3 large ones
Start a daily probiotic and fiber supplement
Keep ginger capsules and antacids accessible
Phase 2: Early management (if symptoms appear)
Add famotidine (Pepcid) 20mg 30 minutes before your largest meal daily
Use magnesium-based antacids for breakthrough symptoms
Add ginger 250mg before dinner
Review your food diary for patterns (most people have 1-2 specific triggers)
Implement left-side sleeping
Walk 15-20 minutes after meals
Phase 3: Escalation (if symptoms persist beyond 2 weeks)
Switch from H2 blocker to PPI (omeprazole 20mg daily, taken 30 minutes before breakfast)
Continue all Phase 1 and 2 strategies
Add melatonin 3mg at bedtime
Consider whether current dose escalation timing is appropriate
Schedule provider discussion if symptoms are not improving
Phase 4: Reassessment (if symptoms persist beyond 4-6 weeks)
Discuss dose adjustment with provider (slower titration, dose reduction, or split dosing)
Consider gastroenterology referral for endoscopic evaluation
Evaluate for H. pylori infection, which can coexist and complicate reflux management
Discuss prescription-strength PPI if OTC versions are insufficient
This protocol works because it is graduated. You implement the least invasive strategies first and escalate only as needed. Most tirzepatide users with heartburn find relief in Phase 1 or 2. Very few need to reach Phase 4. The key principle is patience combined with systematic intervention. Jumping straight to the most aggressive options (stopping the medication or demanding a dose reduction) before trying basic management strategies means potentially giving up significant health benefits for a problem that had a simple solution.
Document what you try and what works. This record becomes invaluable if you eventually need to discuss your situation with a specialist, and it helps you quickly re-implement effective strategies if heartburn returns during future dose escalations.
Real-world tips from experienced tirzepatide users
Clinical guidelines are essential, but practical wisdom from people who have actually managed heartburn on tirzepatide adds another layer of useful information.
Injection day meals: Many users report that heartburn is worst on injection day and the 24 to 48 hours following. Planning your blandest, smallest meals for this window, and your most flavorful or larger meals for days 4-6 of your weekly cycle, can dramatically reduce episodes. Understanding the best time of day to inject tirzepatide helps you plan around this pattern.
The water strategy: Sipping small amounts of alkaline or room-temperature water throughout the day (rather than drinking large volumes at meals) dilutes stomach acid gently without increasing gastric volume at any single point. Cold water can slow gastric emptying further, so room temperature or warm water is preferred.
Keep electrolytes balanced: Tirzepatide-related GI symptoms can affect mineral absorption. Adequate magnesium in particular helps with both heartburn (magnesium-based antacids) and the body aches and muscle pain that some users experience.
Track your triggers: Heartburn patterns are highly individual. What triggers one person may be perfectly fine for another. A simple food and symptom diary for 2 weeks can reveal your specific triggers, which is far more useful than generic avoidance lists. SeekPeptides members use our tracking tools to identify these patterns quickly.
Do not suffer in silence: Many tirzepatide users do not mention heartburn to their healthcare providers because they assume it is just something they have to tolerate. It is not. Your provider has options, including prescription medications, dose adjustments, and referrals, that can make a significant difference. The weight loss benefits of tirzepatide should not come at the cost of chronic discomfort.
The connection between heartburn and other tirzepatide side effects
Heartburn rarely exists in isolation. Understanding how it connects to other GI symptoms helps you address the root cause rather than chasing individual symptoms.
Heartburn and nausea: These frequently co-occur because they share the same underlying mechanism, delayed gastric emptying. The strategies that help heartburn (smaller meals, avoiding fatty foods, ginger supplementation) also tend to improve nausea. If nausea is your primary concern, our guides on what to expect during early tirzepatide therapy cover management in detail.
Heartburn and bloating: Bloating on tirzepatide results from the same food-sitting-in-stomach-longer phenomenon. Reducing bloating through smaller meals and gentle post-meal movement typically reduces heartburn simultaneously.
Heartburn and constipation: Constipation increases intra-abdominal pressure, which worsens reflux. Treating constipation with fiber, adequate hydration, and magnesium often improves heartburn as a secondary benefit. The GLP-1 constipation relief guide covers this in detail.
Heartburn and burping: Excessive burping is another sign of increased intragastric pressure. If you are burping frequently and experiencing heartburn, it confirms that pressure management (through meal size, timing, and body position) should be your primary focus.
Heartburn and dry mouth: Tirzepatide can reduce saliva production in some users. Saliva is naturally alkaline and helps neutralize any acid that reaches the esophagus. Dry mouth removes that protection layer, making heartburn feel more intense. Staying hydrated and using sugar-free gum to stimulate saliva can address both issues.
Specific considerations for compounded tirzepatide users
If you are using a compounded tirzepatide formulation, there are several unique considerations for heartburn management.
Formulation differences: Compounded tirzepatide may contain different excipients (inactive ingredients) than brand-name Mounjaro or Zepbound. Some excipients can affect GI tolerability. If you switched from brand-name to compounded tirzepatide and heartburn appeared or worsened, the formulation difference could be a factor. The B12 compound formulations and glycine-containing compounds may have different GI profiles than basic tirzepatide.
Dosing flexibility: One advantage of compounded formulations is more granular dose control. Instead of jumping from 5mg to 7.5mg, you can step up in 1mg increments (5mg to 6mg to 7mg to 7.5mg). This gentler titration often prevents the heartburn spikes associated with larger dose jumps. Use the compounded tirzepatide dosage calculator to plan a gradual escalation schedule.
Reconstitution and storage: Improperly reconstituted or stored tirzepatide may have altered bioactivity that could affect GI tolerability. Following proper reconstitution protocols and storage guidelines ensures consistent dosing and predictable side effect profiles. Our guides on tirzepatide refrigeration duration, what happens if tirzepatide gets warm, and shelf life cover all the storage variables that matter. If you are traveling with tirzepatide, temperature management becomes especially important for both potency and tolerability.
Common myths about heartburn on tirzepatide
Misinformation about GLP-1 side effects circulates widely online. These myths can lead to poor decision-making, unnecessary medication changes, or avoidable suffering. Here are the most common ones and the truth behind them.
Myth: Heartburn means tirzepatide is damaging your stomach. Tirzepatide does not damage the stomach lining or increase acid production. The heartburn comes from acid reaching the esophagus through a mechanical process (delayed emptying plus increased pressure), not from any toxic or erosive effect on stomach tissue. The medication is not harming your digestive system. It is temporarily changing how quickly your stomach empties, and in some people that creates conditions for reflux.
Myth: You should take tirzepatide with food to prevent heartburn. Tirzepatide is a subcutaneous injection, not an oral medication. It enters your bloodstream through tissue under the skin, bypassing the digestive system entirely. Whether your stomach is full or empty when you inject has no effect on how the medication is absorbed. However, eating a large meal around the same time as your injection can coincidentally worsen heartburn because the delayed emptying effect begins just as your stomach is full. Small meals on injection day work better, but that is about stomach contents, not medication absorption.
Myth: If you get heartburn on tirzepatide, you will get it on all GLP-1 medications. While all GLP-1 receptor agonists slow gastric emptying to some degree, the effect varies between medications. Tirzepatide activates both GLP-1 and GIP receptors, producing a different gastric profile than single-receptor agents like semaglutide. Some people who cannot tolerate tirzepatide GI effects do fine on semaglutide, and vice versa. The comparative side effect profiles between the two medications show meaningful differences in specific GI symptoms.
Myth: Heartburn on tirzepatide gets worse over time. The opposite is generally true. Most heartburn improves with continued use as the body adapts to delayed gastric emptying. The worst period is typically the first 4 to 8 weeks at any given dose. Long-term users who experienced initial heartburn frequently report that it resolved completely by months 3 to 6. Combined with the anti-reflux benefits of weight loss, the long-term trajectory favors improvement.
Myth: You need to stop tirzepatide at the first sign of heartburn. This is the most harmful myth. Heartburn is a manageable side effect in the vast majority of cases. Stopping an effective weight loss and metabolic health medication for a symptom that responds to dietary changes and OTC medications would mean losing significant health benefits. The decision to stop or switch should only be made in consultation with your healthcare provider, after management strategies have been tried, and only for severe or complicated cases. If tirzepatide stops working for other reasons, that is a different conversation, but heartburn alone is rarely a valid reason for discontinuation.
Myth: Natural remedies are better than medication for tirzepatide heartburn. Some natural approaches (ginger, sleep position, meal timing) genuinely help. But when heartburn is moderate to severe, PPIs and H2 blockers are dramatically more effective than any supplement or home remedy. Suffering unnecessarily because you want to avoid "chemicals" is counterproductive. The best approach combines evidence-based medications with lifestyle modifications, using the least aggressive intervention that controls symptoms adequately.
Long-term outlook for heartburn on tirzepatide
The good news is that for most users, heartburn on tirzepatide is a temporary challenge, not a permanent condition. And unlike some side effects that require ongoing management throughout the entire course of treatment, heartburn tends to follow a clear arc of onset, peak, and resolution that gives you a light at the end of the tunnel.
As your body adapts to the medication over weeks and months, gastrointestinal side effects generally improve. The SURMOUNT trial data showed that the majority of GI adverse events, including heartburn, were mild to moderate in severity and occurred primarily during dose escalation phases. Once participants reached their target dose and maintained it, GI symptoms decreased substantially.
This trajectory is similar to what users experience with other GI side effects. The metabolic improvements and benefits beyond weight loss continue to build over time even as side effects diminish. There is another factor working in your favor. As you lose weight on tirzepatide (and most users experience significant weight loss, as documented in tirzepatide before and after results and male-specific results), abdominal pressure decreases. Less abdominal pressure means less force pushing stomach contents upward through the esophageal sphincter. Many users find that their heartburn actually becomes less problematic than it was before starting tirzepatide, because the weight loss itself resolves one of the major contributing factors to acid reflux. For users concerned about maintaining their results long-term, our guides on maintaining weight loss after tirzepatide and weaning off tirzepatide cover the transition process, including how GI symptoms change when you reduce or discontinue the medication. Some users who eventually stop tirzepatide find their heartburn resolves completely once gastric emptying returns to normal speed, while the weight-related improvements in reflux persist.
If you are considering alternatives to manage weight while reducing GI side effects, the comparison between phentermine and GLP-1 medications is worth reviewing, as phentermine works through an entirely different mechanism that does not affect gastric emptying. Similarly, understanding whether switching between GLP-1 medications might help your specific situation can inform discussions with your provider. For those curious about the newest options, the three-way comparison between semaglutide, tirzepatide, and retatrutide covers how each medication differs in GI side effect profiles.
For researchers serious about optimizing their protocols and managing side effects effectively, SeekPeptides provides comprehensive side effect management guides, dosing protocol builders, and a community of experienced users who have navigated these exact challenges. The evidence-based approach to GI symptom management that SeekPeptides members access goes well beyond what any single article can cover, with personalized recommendations based on your specific symptoms, dose, and medical history.
Frequently asked questions
Can I take Tums while on tirzepatide?
Yes. Calcium carbonate antacids like Tums do not interact with tirzepatide and are safe for occasional heartburn relief. However, be aware that calcium-based antacids can worsen constipation, which is already a common tirzepatide side effect. Magnesium-based antacids are generally a better choice for people on GLP-1 medications.
Is heartburn on tirzepatide permanent?
No. For the vast majority of users, heartburn is temporary and most pronounced during dose escalation periods. It typically improves within 4 to 8 weeks at a stable dose. As you lose weight, reduced abdominal pressure often eliminates the problem entirely.
Does omeprazole interact with tirzepatide?
There are no known clinically significant interactions between omeprazole (or other PPIs) and tirzepatide. However, because tirzepatide slows gastric emptying, the absorption timing of oral medications including PPIs may be affected. Taking your PPI on an empty stomach 30 minutes before breakfast helps ensure consistent absorption regardless of gastric emptying speed.
Should I stop tirzepatide if I get heartburn?
Heartburn alone is not a reason to stop tirzepatide. The condition is manageable in the vast majority of cases through dietary changes, OTC medications, and lifestyle modifications. Only stop or modify tirzepatide under the guidance of your healthcare provider. If heartburn is severe, persistent, and unresponsive to treatment, a dose adjustment or medication switch is more appropriate than discontinuation.
Does the B12 compound version of tirzepatide cause less heartburn?
There is no clinical evidence that tirzepatide compounded with B12 causes more or less heartburn than standard tirzepatide. B12 is generally well-tolerated and does not affect gastric acid production or esophageal sphincter function. Individual experiences may vary based on other excipients in the compound.
Can I take famotidine (Pepcid) every day while on tirzepatide?
Famotidine is considered safe for daily use for up to 2 weeks without medical supervision. For longer-term daily use, consult your healthcare provider. Many tirzepatide users find that daily famotidine during dose escalation periods (4-6 weeks) is sufficient, after which they can transition to as-needed use.
Does heartburn mean tirzepatide is working?
Not directly. Heartburn is a side effect of delayed gastric emptying, which is one mechanism through which tirzepatide works. But heartburn is not required for the medication to be effective. Many people experience full appetite suppression and fat burning without any heartburn at all. The absence of heartburn does not mean the medication is not working.
Is heartburn worse with higher doses of tirzepatide?
Generally, yes. Clinical trial data shows a dose-dependent relationship, with heartburn rates approximately doubling from the 5mg to 10mg dose. However, the relationship is not linear, and many people tolerate higher doses well after adapting. The tirzepatide dose chart includes expected side effect profiles at each level.
Can heartburn on tirzepatide damage my esophagus?
Occasional heartburn is unlikely to cause lasting damage. Chronic, unmanaged GERD (heartburn more than twice per week for several weeks) can lead to esophagitis, Barrett esophagus, or esophageal strictures over time. This is why managing symptoms promptly is important rather than simply tolerating them. If OTC medications and lifestyle changes are not controlling your symptoms, seek medical evaluation.
Does taking tirzepatide with food help or hurt heartburn?
Tirzepatide is injected subcutaneously, not taken orally, so food timing relative to the injection does not directly affect absorption. However, eating a large meal close to injection time can combine food-related gastric distension with the medication onset of delayed emptying, potentially worsening heartburn. Keeping meals small on injection day is a practical approach. See our calorie guide for tirzepatide for meal planning help.
Will losing weight on tirzepatide eventually cure my heartburn?
For many people, yes. Excess abdominal weight is one of the strongest risk factors for GERD. As tirzepatide-driven weight loss reduces abdominal pressure, reflux symptoms often improve substantially. Some users find their heartburn is better at month 6 than it was before starting the medication, because the weight loss benefit outweighs the gastric slowing effect.
Should I change my injection site if I have heartburn?
No. Injection site (abdomen, thigh, or upper arm) does not affect GI side effects. The heartburn is caused by systemic drug effects on gastric emptying, not local tissue effects at the injection site. However, if you experience injection site reactions alongside heartburn, rotating sites as our thigh injection guide recommends is still good practice.
Is it safe to take tirzepatide with acid reflux medication long-term?
PPIs and H2 blockers are generally safe for use alongside tirzepatide. Long-term PPI use (beyond 1 year) has its own set of considerations, including potential effects on calcium absorption, magnesium levels, and vitamin B12 status. Since many tirzepatide users already supplement with B12, discuss any long-term acid suppression therapy with your healthcare provider to ensure nutrient status is monitored.
External resources
American College of Gastroenterology: Acid Reflux Guidelines
NIH National Institute of Diabetes and Digestive and Kidney Diseases: GERD
In case I do not see you, good afternoon, good evening, and good night. May your reflux stay quiet, your meals stay comfortable, and your protocols stay effective.