Feb 5, 2026

Tired of stepping on the scale every morning and seeing the same number stare back at you? You are not alone. Thousands of people start semaglutide with high hopes, expecting the pounds to melt away like the clinical trial headlines promised. But weeks pass. Sometimes months. And the scale barely moves, or worse, it creeps in the wrong direction. The frustration is real. The confusion is worse. Because everywhere you look online, someone is raving about their incredible transformation, their dramatic before-and-after photos, their seemingly effortless weight loss with peptide-based therapies. So what is wrong with you?
Nothing. Nothing is wrong with you.
The truth is that semaglutide does not work the same way for every person. Clinical trials paint an average picture, but averages hide enormous variation. Some participants in the STEP 1 trial lost over 20% of their body weight. Others lost almost nothing. In fact, roughly 10 to 15% of people on semaglutide qualify as non-responders, meaning they fail to achieve even 5% total body weight loss. And a real-world study found that 54% of 93 enrolled individuals did not hit the 5% weight loss target at all. Those numbers rarely make the headlines. But they matter, because if you are reading this, you are probably living inside that statistic right now, wondering why the medication everyone calls a miracle is not working for you. This guide covers every reason semaglutide might stall, plateau, or fail entirely, along with the specific, evidence-based strategies to break through and finally see results. Whether you need a semaglutide dosage adjustment, a lifestyle change, or an entirely different approach, the answer is here.
How semaglutide actually works for weight loss
Before troubleshooting why semaglutide is not working, you need to understand what it is supposed to do. And more importantly, what it is not supposed to do. Semaglutide is a GLP-1 receptor agonist. That is a technical term for a compound that mimics a natural hormone your gut produces after eating. The hormone, glucagon-like peptide-1, sends signals to your brain that say "you are full, stop eating." Semaglutide amplifies that signal dramatically. But appetite suppression is only part of the story, and understanding the full mechanism explains why so many variables can derail your results.
The appetite suppression pathway
GLP-1 receptors sit in the hypothalamus, the brain region that controls hunger and satiety. Understanding what peptides are used for starts with this receptor-level interaction. When semaglutide binds to these receptors, it reduces appetite at a neurological level. This is not willpower. This is chemistry. Your brain literally receives fewer hunger signals, and the signals it does receive carry less urgency. Most people describe it as food simply becoming less interesting. The constant mental chatter about what to eat next, when to eat next, whether to grab a snack, all of it quiets down. For many people on semaglutide, this is the first time in their lives they have experienced true food neutrality.
But here is the critical detail. Appetite suppression does not guarantee a caloric deficit.
You can eat less frequently and still consume the same number of calories if your food choices are calorie-dense. A person who stops snacking but switches to larger, richer meals may see zero net change in energy intake. The timeline for appetite suppression also varies widely. Some people feel it within days. Others need months at therapeutic doses before the effect fully kicks in. If you are still in the early weeks, patience is not just a virtue. It is a requirement.
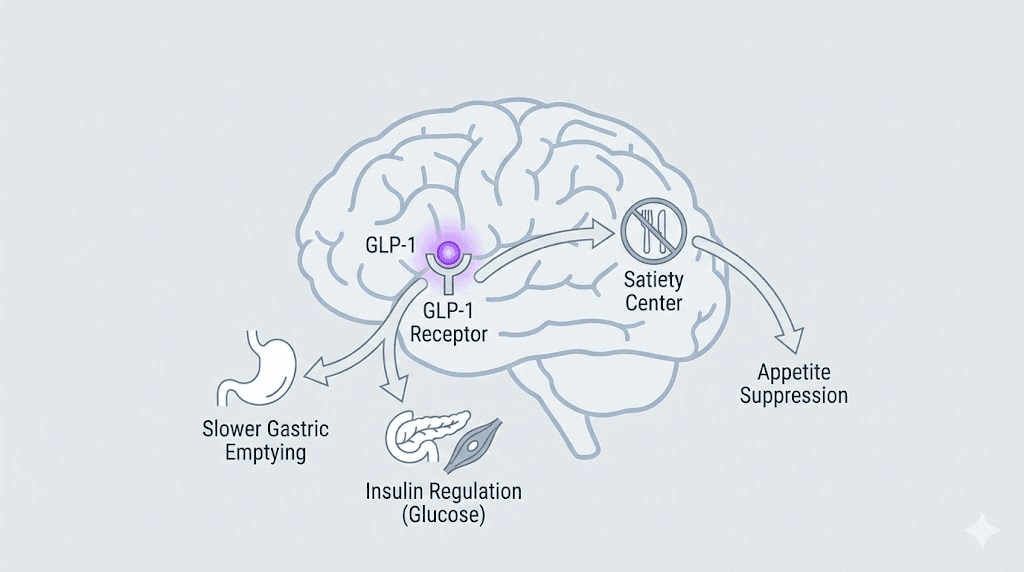
Delayed gastric emptying
Semaglutide slows down how quickly food leaves your stomach. This is called delayed gastric emptying, and it serves a dual purpose. First, it keeps you feeling physically full for longer after eating. Second, it slows the absorption of glucose into your bloodstream, which prevents the insulin spikes that drive fat storage and subsequent hunger. This mechanism is why many semaglutide users report that a small meal keeps them satisfied for hours, sometimes uncomfortably so. It also explains the most common side effects, including nausea, bloating, and occasional vomiting, because food is simply sitting in the stomach longer than the body expects.
Insulin regulation and blood sugar control
Semaglutide was originally developed for type 2 diabetes, and its insulin-regulating properties remain central to how it works. The medication stimulates insulin secretion when blood sugar is elevated and suppresses glucagon, the hormone that tells your liver to release stored glucose. This dual action creates more stable blood sugar throughout the day. Stable blood sugar means fewer cravings. It means less of the crash-and-binge cycle that derails so many weight loss efforts. The GLP-3 peptide research explores how related gut hormones contribute to this metabolic regulation. For people with insulin resistance, this mechanism can be transformative. For those without significant insulin dysfunction, it adds a modest but meaningful layer of metabolic support. You can learn more about how this relates to broader peptide-based hormone balance strategies.
What semaglutide does NOT do
This is where expectations collide with reality, and it is crucial to understand before evaluating your results. The fundamentals of how peptides work apply here. Semaglutide does not significantly increase your metabolic rate. Research shows that resting metabolic rate, adjusted for lean body mass, does not meaningfully differ between semaglutide users and placebo groups. The medication does not burn fat directly. It does not build muscle. It does not override the laws of thermodynamics. It creates conditions, reduced hunger, slower digestion, better blood sugar, that make it easier to maintain a caloric deficit. But the deficit itself still has to happen. And if something is preventing that deficit, semaglutide cannot compensate. That understanding is the foundation for everything that follows.
The most common reasons semaglutide is not working
There is rarely a single reason. More often, it is a combination of factors working against you simultaneously. Some are within your control. Some are not. All of them are fixable, or at minimum, addressable. Let us walk through each one systematically, because finding your specific roadblock is the first step to removing it. The common mistakes beginners make with peptide protocols often mirror the mistakes people make with semaglutide specifically. If you are interested in how different peptides approach weight loss, understanding these barriers will help you evaluate all your options more clearly.
Your dose is still too low
This is the number one reason people think semaglutide has failed them. And it is the easiest to fix.
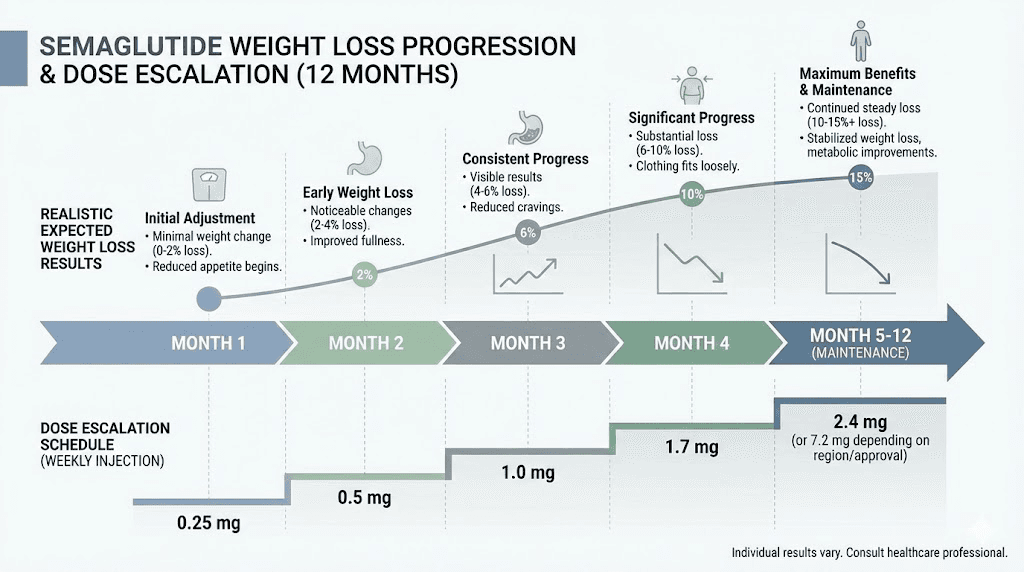
Semaglutide uses a gradual dose escalation schedule. You start at 0.25 mg per week. After four weeks, you move to 0.5 mg. Then 1.0 mg. Then 1.7 mg. Finally, 2.4 mg, which is the maximum dose approved for weight loss. Each step lasts at least four weeks. That means reaching the full therapeutic dose takes a minimum of 16 to 20 weeks, roughly four to five months. During those early months, many people experience only mild appetite suppression. Some notice nothing at all. And the weight loss during dose escalation is often minimal, perhaps 3 to 4% of body weight in the first month at sub-therapeutic doses. The real results typically do not appear until you have been at 1.7 mg or 2.4 mg for several consecutive weeks. If you are currently at 0.5 mg or 1.0 mg and wondering why nothing is happening, this is almost certainly your answer. You have not reached the dose where the medication works at full strength. Use the semaglutide dosage calculator to understand exactly where you are in the titration schedule and what to expect at each level.
You have not given it enough time
Impatience kills more semaglutide protocols than any medical condition.
Clinical trials measured outcomes at 68 weeks, that is over 15 months. The headline number of 14.9% average weight loss from STEP 1 did not happen in a few weeks. It accumulated gradually over more than a year. The first four weeks? Barely noticeable for most participants. The first eight weeks? Maybe 5 to 10 pounds. The dramatic results came later, after months of sustained use at therapeutic doses. Yet many people evaluate semaglutide after just six or eight weeks, often while still at a low dose, and conclude it is not working. That is like judging a marathon at mile two. The reality is that most significant weight loss with semaglutide occurs between months three and twelve. And the STEP 5 trial showed that weight loss continued through week 104, a full two years, with approximately 15% mean weight loss maintained. Your body needs time to adjust, respond, and change. If you have been on semaglutide for less than four months, particularly if you have not yet reached the 2.4 mg dose, it is simply too early to conclude it is not working.
Your calorie intake is still too high
Semaglutide reduces appetite. It does not eliminate it. And reduced appetite does not automatically mean reduced calories.
Consider this scenario. Before semaglutide, you ate 2,800 calories per day. The medication reduces your appetite by roughly 25%, so you naturally drop to around 2,100 calories. But if your maintenance level, the calories your body needs to stay at its current weight, is 2,000 calories, you are only in a 100-calorie daily deficit. At that rate, you would lose about one pound every 35 days. Barely perceptible. Meanwhile, someone else with the same appetite reduction might go from 3,200 calories to 2,400 while having a maintenance level of 2,200.
Their 200-calorie deficit produces faster, more visible results. The medication is working identically in both cases. The difference is the starting caloric picture. And this is where many people get stuck. They assume semaglutide will handle the calorie math automatically, and for some, it does. But for others, especially those who already eat a calorie-dense diet or who respond to the appetite suppression by making higher-calorie food choices during the meals they do eat, manual attention to food intake becomes necessary. Tracking your protocols and intake carefully makes a measurable difference in outcomes.
You are not tracking food intake
This connects directly to the previous point. Without tracking, you are guessing. And humans are spectacularly bad at guessing calories. Even experienced researchers who understand precise dosage calculations for peptides often underestimate their food intake.
Research consistently shows that people underestimate their caloric intake by 30 to 50%. That is not a moral failing. It is a cognitive limitation. Portion sizes are hard to judge. Cooking oils add hidden calories. A handful of nuts here, a splash of cream in coffee there, an extra tablespoon of salad dressing, these add up faster than anyone realizes. On semaglutide, the stakes are higher because the margin for error is thinner. If the medication creates a 300-calorie-per-day appetite reduction but you are unknowingly eating 400 extra calories through untracked additions, you end up in a surplus. Not a deficit. Even temporary tracking, just two to three weeks of honest logging in a food tracking app, can reveal blind spots you never knew existed. The same precision that matters when using a peptide cost calculator applies to tracking your nutritional investment. You do not have to track forever. But doing it once can recalibrate your entire understanding of what and how much you are actually eating.
Physical activity is insufficient
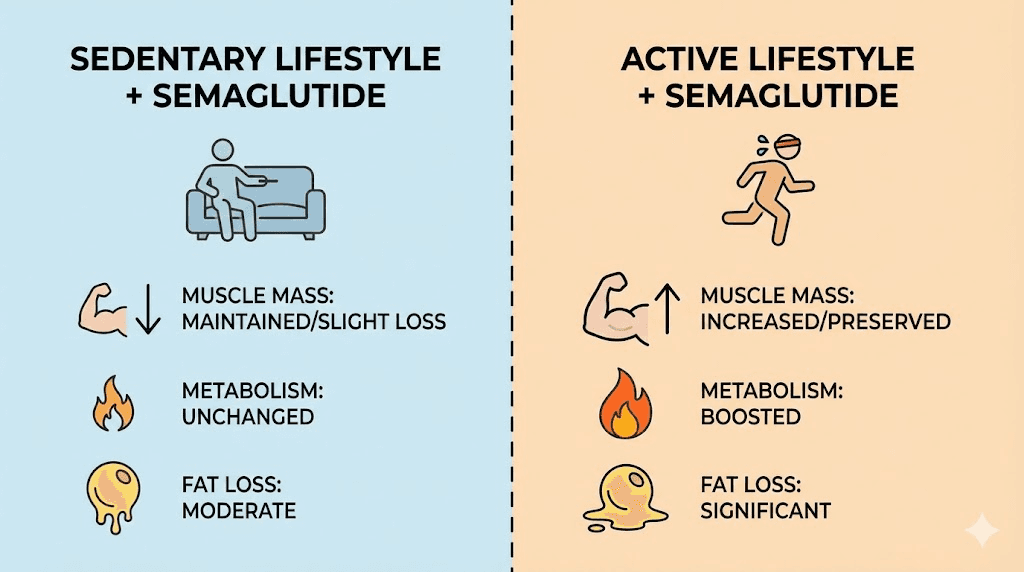
Semaglutide was studied in conjunction with lifestyle interventions, which included increased physical activity. The athletic performance peptide category covers how physical activity integrates with various peptide protocols. The clinical trials did not test semaglutide in a vacuum. They paired it with counseling on diet and exercise. The STEP 3 trial, which combined semaglutide with intensive behavioral therapy including structured exercise, saw even greater weight loss of 16.0% versus 5.7% with placebo.
Exercise contributes to weight loss in two direct ways. It burns additional calories, expanding your deficit. And it builds or preserves muscle mass, which keeps your resting metabolic rate from dropping as you lose weight. Without exercise, weight loss on semaglutide tends to include more lean tissue loss. That means you lose weight on the scale, but your body composition does not improve proportionally. And with less muscle, your metabolism slows, making future weight loss harder. This is why people who combine semaglutide with consistent resistance training see not just better weight loss numbers, but better body composition outcomes. For guidance on exercise approaches that pair well with peptide-based fat loss strategies, structured programs make an enormous difference.
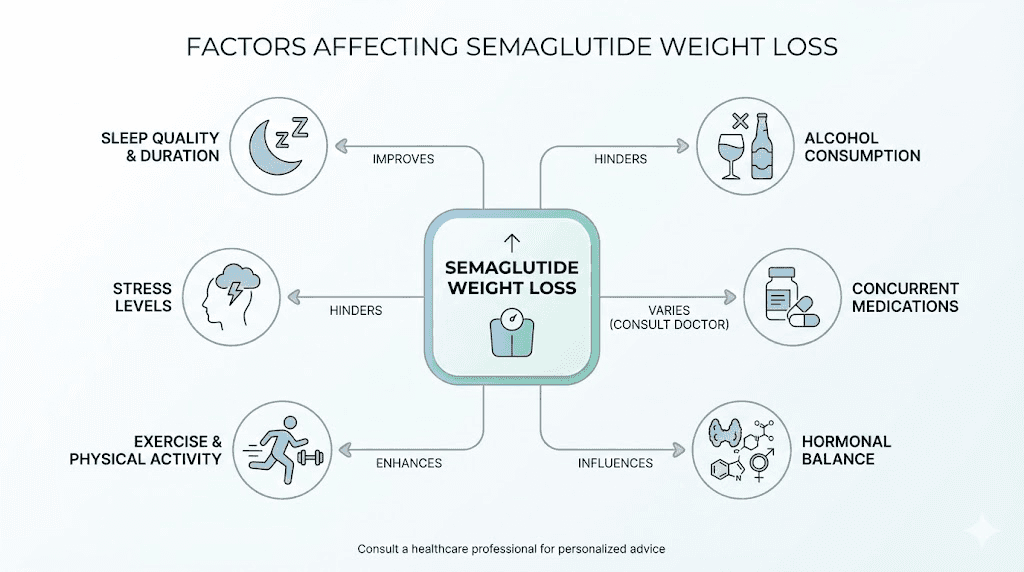
Poor sleep quality is sabotaging your progress
Sleep is the invisible variable most people overlook. And it is devastating to weight loss.
Poor sleep increases ghrelin, the hunger hormone. It decreases leptin, the satiety hormone. It impairs insulin sensitivity, raises cortisol, and shifts food preferences toward high-calorie, high-carbohydrate options. In other words, bad sleep actively fights against everything semaglutide is trying to do. One study found that sleep-deprived individuals consumed an average of 385 additional calories per day compared to well-rested controls. That single variable can erase your entire caloric deficit. If you are sleeping less than seven hours per night, or if your sleep quality is poor due to sleep apnea, stress, screen time, or irregular schedules, this may be the missing piece. Fixing sleep does not require medication or complicated protocols. Consistent bedtimes, dark rooms, limited screen exposure before bed, and addressing sleep apnea if present can transform not just your weight loss, but your entire response to semaglutide. Those researching peptides for energy and focus optimization often find that sleep quality improvements provide more benefit than any compound alone.
Chronic stress and elevated cortisol
Stress does not just make you feel bad. It makes you store fat.
Cortisol, the primary stress hormone, promotes visceral fat accumulation, the dangerous fat stored around your organs and midsection. It increases insulin resistance. It triggers cravings for comfort foods. And it breaks down muscle tissue, which further slows your metabolism. Chronic stress creates a hormonal environment that actively resists weight loss, regardless of what medication you are taking. Semaglutide can reduce appetite, but it cannot override a cortisol-driven metabolic state that prioritizes fat storage. If your life involves sustained high stress, whether from work, relationships, financial pressure, or health anxiety, addressing that stress is not optional. It is a fundamental requirement for the medication to work as intended. Strategies like regular exercise, mindfulness practices, adequate sleep, and boundary-setting around stressors all lower cortisol and create conditions where semaglutide can do its job. Understanding the relationship between peptides and stress-related conditions provides additional context for managing the psychological barriers to weight loss. For those interested in how other compounds address stress-related weight gain, exploring strategies for targeting belly fat may reveal complementary approaches that specifically target visceral fat accumulation driven by cortisol.
Underlying medical conditions
Sometimes the obstacle is medical, not behavioral. Several conditions can significantly slow or prevent weight loss on semaglutide, and they deserve serious investigation if you have addressed all the lifestyle factors above and still see no movement.
Hypothyroidism. An underactive thyroid slows metabolism at a fundamental level. If your thyroid hormone levels are low or poorly managed, even a perfect diet and exercise program will produce suboptimal results. Semaglutide does not treat thyroid dysfunction, and thyroid issues can blunt its effectiveness. The hormone balance guide covers how hormonal dysfunction interacts with peptide-based protocols. Research shows that patients with hypothyroidism who did lose weight on semaglutide saw decreases in TSH levels, suggesting the two conditions interact in complex ways. If you have not had your thyroid checked recently, or if your levothyroxine dose has not been adjusted in a while, this is worth investigating with your healthcare provider.
Polycystic ovary syndrome. PCOS affects up to 10% of women of reproductive age and is strongly associated with insulin resistance, hormonal imbalance, and difficulty losing weight. The insulin resistance component is particularly relevant because it can make the body resistant to semaglutide mechanisms of action. Women with PCOS often need higher doses, longer treatment durations, or combination approaches to see meaningful weight loss. Understanding how peptides work for women specifically can provide additional context for this challenge.
Insulin resistance. Even outside of PCOS, significant insulin resistance creates a metabolic environment that resists weight loss. Data from the STEP 2 trial, which enrolled participants with type 2 diabetes, showed that these individuals lost less weight than those without diabetes. Specifically, 26.8% of participants with type 2 diabetes on semaglutide lost less than 5% body weight, compared to just 7.6% of participants without diabetes in STEP 1. Insulin resistance is not a fixed condition. It improves with weight loss, exercise, and dietary changes. But it can create a frustrating chicken-and-egg situation where you need to lose weight to improve insulin sensitivity, but insulin resistance prevents weight loss.
Cushing syndrome. This is less common but worth mentioning. Cushing syndrome involves chronic cortisol overproduction, causing weight gain particularly in the face, midsection, and upper back. If you have unexplained weight gain concentrated in these areas along with other symptoms like easy bruising, stretch marks, or muscle weakness, discuss Cushing testing with your provider.
Medication interactions
Certain medications can directly or indirectly interfere with weight loss on semaglutide. Some cause weight gain as a side effect. Others alter metabolism or appetite in ways that counteract the medication.
The most common culprits include certain antidepressants, particularly SSRIs and SNRIs, which can cause weight gain in some users over time. Antipsychotic medications, especially olanzapine and quetiapine, are associated with significant weight gain. Corticosteroids like prednisone promote fat storage and increase appetite. Beta-blockers used for high blood pressure can slow metabolism. Insulin and sulfonylureas, while necessary for some diabetic patients, can promote weight gain. Even antihistamines taken regularly have been linked to modest weight increases in some studies. The solution is not to stop taking necessary medications. It is to work with your healthcare provider to evaluate whether alternatives exist that are less likely to interfere with weight loss. Sometimes a simple medication switch can remove a significant barrier. The peptide safety and risks guide offers broader context for understanding how different compounds interact.
Metabolic adaptation and plateaus
Your body is not designed to lose weight indefinitely. It is designed to defend its current state.
As you lose weight, several adaptations occur. Your resting metabolic rate decreases, not just because you have less body mass to maintain, but because your body actively downregulates energy expenditure to conserve resources. Hormones shift. Leptin, which signals satiety, drops. Ghrelin, which signals hunger, increases. Thyroid function can decrease slightly. The net result is that maintaining a caloric deficit becomes progressively harder. This is called metabolic adaptation, and it is not a failure of semaglutide. It is your body doing exactly what it evolved to do, protect you from starvation. Weight loss plateaus are almost universal. They typically happen after several months of consistent loss. The timeline for results with peptides explores how these adaptation phases affect various protocols. The solution is not to panic or abandon the protocol. It is to adjust. Sometimes a diet break, where you eat at maintenance for one to two weeks, can reset some of these hormonal adaptations. Sometimes increasing activity breaks the plateau. Sometimes patience is the only answer, because weight loss is not linear. The scale might stay the same for weeks, then drop suddenly as fluid retention patterns shift.
Alcohol consumption
Alcohol derails weight loss in multiple ways, and its effects are amplified when combined with semaglutide.
First, alcohol is calorie-dense. At seven calories per gram, it is nearly as energy-rich as fat. A few drinks can add 400 to 800 calories with minimal satiety. Second, alcohol impairs judgment, leading to poor food choices. Third, it disrupts sleep quality, which as discussed earlier, sabotages weight loss through hormonal mechanisms. Fourth, alcohol metabolism takes metabolic priority, meaning your body temporarily stops burning fat and focuses on processing the alcohol instead. And fifth, alcohol can intensify semaglutide side effects, particularly nausea. If you are drinking regularly, even moderately, it may be the variable preventing results. Reducing or eliminating alcohol for a defined period, say 30 to 60 days, can often break a stubborn plateau and reveal whether this was the limiting factor.
Hidden carbohydrate sources and blood sugar spikes
Even without tracking overall calories, certain food choices can prevent weight loss by triggering insulin spikes and subsequent hunger cycles.
Refined carbohydrates and sugars, white bread, pastries, sweetened beverages, candy, cause rapid blood sugar increases followed by crashes. Those crashes trigger hunger, even if you have eaten enough calories. Semaglutide helps regulate blood sugar, but it cannot fully override the effects of a diet dominated by high-glycemic foods. Many people report that switching to a lower-carbohydrate or lower-glycemic-index diet dramatically improves their results on semaglutide, even without consciously reducing total calories. The mechanism is simple. Stable blood sugar means fewer cravings. Fewer cravings mean better adherence to a caloric deficit. You do not need to eliminate carbohydrates entirely. But replacing refined carbs with whole food sources, vegetables, legumes, whole grains, can shift your metabolic response in a way that supports rather than fights the medication.
Not enough protein intake
Protein is the most important macronutrient for weight loss, and most people do not eat enough of it.
Protein has the highest thermic effect of food, meaning your body burns more calories digesting it compared to carbohydrates or fats. It promotes satiety more effectively than other macronutrients. And critically, adequate protein intake preserves muscle mass during weight loss. Without sufficient protein, the weight you lose will include too much lean tissue, which slows your metabolism and makes regaining weight easier. Research suggests that during weight loss, protein intake should be at least 0.7 to 1.0 grams per pound of ideal body weight, sometimes higher for people doing resistance training. If you are eating primarily carbohydrate and fat-based meals, adding more protein, through lean meats, fish, eggs, dairy, legumes, or protein supplements, can improve both the rate of weight loss and body composition outcomes. Many people on semaglutide report that high-protein meals extend the appetite suppression effect and reduce the frequency of hunger breakthrough. The muscle recovery guide discusses how protein intake integrates with muscle growth strategies and overall body composition.
Expecting linear progress
Weight loss is never a straight line down. Never.
The scale measures total body weight, which includes fat, muscle, water, glycogen, and the physical contents of your digestive system. All of these fluctuate daily. You can be in a perfect caloric deficit and still see the scale go up temporarily due to water retention from sodium intake, hormonal changes, exercise-induced inflammation, or constipation. Women experience cyclical water retention related to menstrual cycles. Starting a new exercise program often causes temporary weight gain from muscle inflammation and increased glycogen storage.
Even a high-carbohydrate meal can add several pounds of water weight overnight. These fluctuations are normal. They are not failures. The solution is to focus on trends over time, not daily weigh-ins. If the overall trajectory over two to four weeks is downward, the protocol is working. If you cannot handle the psychological noise of daily fluctuations, weigh yourself less frequently, once per week or once every two weeks. Better yet, track additional metrics like waist circumference, progress photos, or how your clothes fit. These often show progress that the scale temporarily hides.
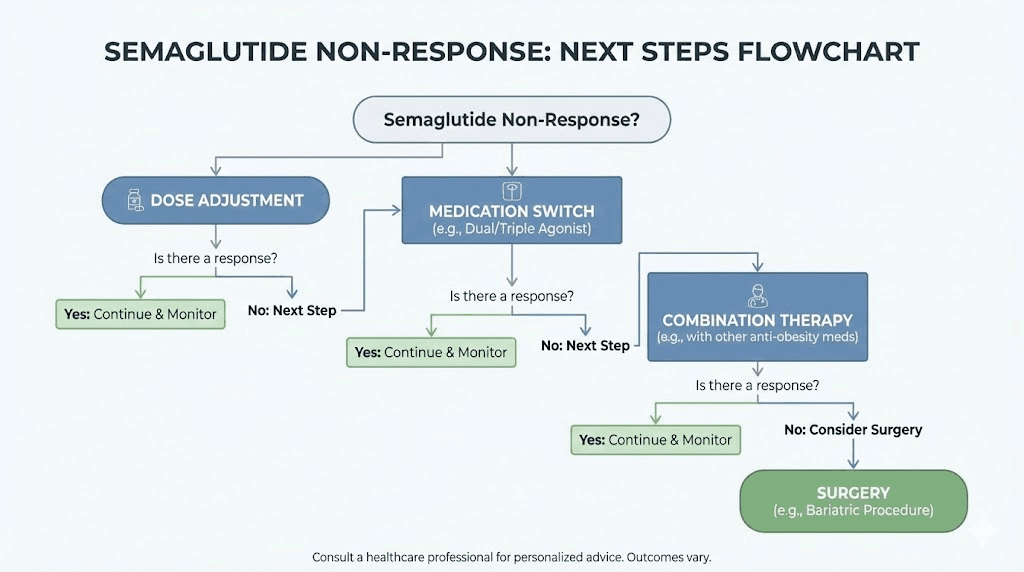
What to do if semaglutide truly is not working
Let us say you have addressed everything above. You have been on semaglutide for six months. You have reached the 2.4 mg dose. You have tracked your food intake. You exercise regularly. You sleep well. You have ruled out medical conditions. And you still have not lost meaningful weight. Now what? This section covers the options for true non-responders, the roughly 10 to 15% of people for whom semaglutide does not produce significant results.
Consider dose adjustment or extended titration
Some providers are now using doses above 2.4 mg in clinical practice, though this is off-label. Research on higher doses is limited but emerging. If you have tolerated 2.4 mg well without significant side effects, discuss with your provider whether a higher dose, say 3.0 mg or even higher, might be appropriate. The risk-benefit calculation changes at higher doses. Side effects may increase. But for someone who has seen zero response at standard doses, the potential benefit may justify the risk. Another option is extended titration. Instead of increasing the dose every four weeks, some people benefit from staying at each dose level for six to eight weeks, allowing their body more time to adapt and respond before escalating further. This is particularly relevant for people with significant insulin resistance or metabolic dysfunction, where the response timeline is slower.
Switch to tirzepatide
Tirzepatide is a dual GIP and GLP-1 receptor agonist. The addition of GIP, glucose-dependent insulinotropic polypeptide, activity appears to produce greater weight loss in clinical trials compared to semaglutide alone. The SURMOUNT-1 trial showed that participants on the highest dose of tirzepatide lost an average of 20.9% of their body weight, compared to 14.9% with semaglutide in STEP 1. More importantly for non-responders, a higher percentage of people achieved meaningful weight loss on tirzepatide. If semaglutide has not worked despite appropriate dose and duration, tirzepatide may produce a different response. The mechanisms overlap but are not identical, and some people respond better to the dual agonist approach. Understanding how different compounds compare can help frame these options. Insurance coverage for tirzepatide may differ from semaglutide, so cost is a consideration. But for true non-responders, switching to a different medication class is a logical next step.
Explore combination therapy
Some providers are beginning to combine GLP-1 agonists with other weight loss medications to produce synergistic effects.
The most common combinations include semaglutide plus phentermine, an appetite suppressant that works through different mechanisms. Another emerging combination is semaglutide plus naltrexone-bupropion, which affects reward pathways in the brain and reduces food cravings. There is also interest in combining GLP-1 agonists with SGLT2 inhibitors, which promote glucose excretion through urine and have modest weight loss effects. These combinations are not yet standard of care, and long-term safety data is limited. But for people who have not responded to monotherapy, combination approaches may unlock results. This requires working with a provider experienced in managing these protocols, as drug interactions and side effect profiles become more complex. For broader context on combination strategies, the peptide stacking guide explores how different compounds work together for optimized weight loss outcomes.
Investigate genetic factors
Emerging research suggests that genetic variations may influence how people respond to GLP-1 agonists.
Certain gene variants related to GLP-1 receptor function, appetite regulation, and metabolism may predict response to semaglutide. While genetic testing for weight loss medication response is not yet widely available or validated, it is an area of active research. If you have access to genetic testing through a research program or specialized clinic, it may provide insights into why you are not responding and suggest alternative approaches tailored to your genetic profile. This is cutting-edge and not standard practice, but for persistent non-responders who have exhausted other options, it represents a future direction worth monitoring.
Address psychological and behavioral components
Sometimes the barrier is not physiological. It is psychological.
Emotional eating, binge eating disorder, food addiction, and other behavioral patterns can override even the strongest appetite suppression. Semaglutide reduces physical hunger, but it does not address the psychological drive to eat for comfort, stress relief, or emotional regulation. If you recognize these patterns in yourself, working with a therapist who specializes in eating behaviors, particularly cognitive-behavioral therapy or dialectical behavior therapy, can be transformative. Addressing the psychological component does not replace medication. It complements it. And for many people, this is the missing piece that allows the medication to finally work as intended. Research on peptides for mental health explores how neurological and psychological factors intersect with metabolic interventions.
Consider surgical options
For people with severe obesity who have not responded to multiple medication trials, bariatric surgery remains the most effective intervention.
Procedures like gastric sleeve or gastric bypass produce average weight loss of 25 to 30% of total body weight, significantly more than any medication. Surgery also has powerful metabolic effects beyond simple calorie restriction, particularly for type 2 diabetes and metabolic syndrome. It is not a decision to make lightly. Surgery carries risks, requires lifelong dietary changes, and is irreversible in most cases. But for people who qualify and who have exhausted non-surgical options, it is a proven, evidence-based solution. Some insurance plans require documented trials of medication like semaglutide before approving surgery, so even if surgery becomes the eventual path, medication trials are often a necessary prerequisite. For those exploring peptides versus other interventions, understanding the full spectrum of options provides important context.
Reassess your weight loss expectations
This is uncomfortable to discuss, but necessary.
Clinical trials report average weight loss of 14.9%, but that average hides enormous variation. Some people lose 25%. Others lose 5%. A 5% weight loss, while it might not feel dramatic, produces measurable health benefits. It improves blood pressure, blood sugar, cholesterol, and reduces the risk of cardiovascular disease and diabetes. If you started at 220 pounds and lost 11 pounds, that is 5% weight loss. It might not feel like success. But metabolically, it is meaningful. The question to ask is not "Why did I not lose 40 pounds?" The question is "Am I healthier than I was before?" If the answer is yes, if your labs improved, if you feel better, if you are more active, then the intervention is working, even if the number on the scale does not match your initial hopes. Weight loss is one marker of health. It is not the only marker. And sometimes recalibrating expectations, while continuing the protocol, allows you to see the benefits that were already happening.
Strategies to maximize your semaglutide results
Whether you are just starting semaglutide or trying to break through a plateau, these evidence-based strategies can improve your outcomes. None of them are magic. All of them work by addressing the physiological, behavioral, and environmental factors that influence weight loss. Think of semaglutide as the foundation. These strategies are the scaffolding that supports and amplifies its effects. Those looking to maximize results with peptides will find many of these principles apply universally.
Prioritize protein at every meal
Aim for 25 to 40 grams of protein per meal, ideally from whole food sources.
Protein increases satiety more than any other macronutrient, meaning you feel fuller longer. It preserves muscle mass during weight loss, which keeps your metabolism higher. And it has the highest thermic effect of food, meaning your body burns more calories digesting it. Prioritizing protein does not mean eliminating carbohydrates or fats. It means structuring meals around a protein source first, then adding vegetables, healthy fats, and carbohydrates as needed. For many people on semaglutide, this single change produces noticeable improvements in energy, satiety, and weight loss rate. The timing guide for peptides explores how nutrient timing can further optimize results.
Incorporate resistance training
Resistance training, lifting weights, bodyweight exercises, resistance bands, is the single most effective way to preserve muscle mass during weight loss.
Without resistance training, roughly 25% of the weight you lose on semaglutide will be lean tissue. With resistance training, that number drops significantly. More muscle means a higher resting metabolic rate, better glucose metabolism, and improved body composition. You do not need to become a bodybuilder. Two to three sessions per week, focusing on major muscle groups, is sufficient for most people. If you are new to resistance training, working with a trainer for even a few sessions can teach proper form and build confidence. Many people report that adding resistance training is the variable that finally broke their plateau. The exercise recovery strategies can support this new training regimen.
Track food intake for at least two weeks
Even if you hate tracking, do it temporarily to recalibrate your understanding of portions and calories.
Use an app like MyFitnessPal, Cronometer, or Lose It. Weigh your food on a kitchen scale. Log everything, including cooking oils, condiments, and beverages. The goal is not to track forever. The goal is to gather data. Most people discover that they are eating more than they thought, often significantly more. Once you have that data, you can make informed adjustments. And even after you stop tracking, you will have a better intuitive sense of portion sizes and calorie density. This awareness alone often produces better results.
Manage stress through structured practices
Stress management is not optional. It is a core component of successful weight loss.
Chronic stress elevates cortisol, which as discussed earlier, promotes fat storage and insulin resistance. Effective stress management does not mean eliminating stress entirely, which is unrealistic. It means building regular practices that lower your baseline stress level. Options include mindfulness meditation, even five minutes per day, yoga, deep breathing exercises, regular physical activity, time in nature, and setting boundaries around work and relationships. The specific practice matters less than consistency. Find something that fits your life and do it regularly. The stress management approaches using peptides provide additional tools for this challenge.
Optimize sleep hygiene
Sleep is not a luxury. It is a biological necessity, and poor sleep directly undermines weight loss.
Create a sleep-friendly environment. Keep your bedroom cool, dark, and quiet. Establish a consistent bedtime and wake time, even on weekends. Limit screen exposure at least one hour before bed, as blue light suppresses melatonin production. Avoid caffeine after early afternoon. If you snore loudly or experience daytime fatigue despite adequate sleep duration, get evaluated for sleep apnea. Treating sleep apnea, often with a CPAP machine, can transform not just your energy levels but your entire metabolic response to weight loss interventions. People often underestimate how much poor sleep is sabotaging their progress until they fix it and see the dramatic difference.
Reduce alcohol consumption
Alcohol is empty calories, sleep disruptor, and judgment impairment all rolled into one.
If you drink regularly, even moderately, consider a temporary elimination, say 30 to 60 days, to see if it breaks a plateau. You do not have to quit forever. But gathering data on how your body responds without alcohol can be revealing. Many people discover that alcohol was a bigger factor than they realized. And even after reintroducing it, they often choose to drink less frequently or in smaller amounts because they have seen the difference. If complete elimination feels impossible, start with reduction. Cut your intake in half and observe the results.
Eat more vegetables and fiber
Vegetables and fiber promote satiety, stabilize blood sugar, and support gut health, all of which enhance semaglutide effectiveness.
Aim for at least five servings of non-starchy vegetables per day. Think leafy greens, broccoli, cauliflower, peppers, zucchini, Brussels sprouts, asparagus. These foods are nutrient-dense and low in calories, meaning you can eat large volumes without exceeding your caloric target. Fiber, whether from vegetables, legumes, whole grains, or supplements, slows digestion and improves satiety. It also feeds beneficial gut bacteria, which emerging research suggests may influence weight loss and metabolic health. The combination of semaglutide slowing gastric emptying and high-fiber foods promoting fullness creates a powerful synergy.
Stay hydrated
Dehydration can mimic hunger, leading to unnecessary calorie intake.
Aim for at least eight cups of water per day, more if you are active or live in a hot climate. Many people find that drinking a glass of water before meals reduces appetite and prevents overeating. Hydration also supports metabolic processes, including fat oxidation. If you struggle to drink plain water, add lemon, cucumber, or herbal tea. Just avoid sugary beverages, which add calories without satiety. The proper storage and handling principles for peptides often emphasize similar attention to environmental factors like hydration.
Consider intermittent fasting
Intermittent fasting, restricting eating to a specific time window each day, can complement semaglutide by naturally reducing calorie intake.
Common approaches include 16:8, where you eat within an eight-hour window and fast for 16 hours, or 14:10 for a less restrictive version. Semaglutide already reduces appetite, so many people find that skipping breakfast or eating dinner earlier feels natural rather than forced. Intermittent fasting is not necessary for weight loss. But for people who respond well to structured eating windows, it can simplify adherence and create a consistent caloric deficit. The key is to listen to your body. If fasting increases hunger, stress, or leads to binge eating, it is not the right approach for you.
Work with a registered dietitian
A registered dietitian who specializes in weight management can provide personalized guidance that generic advice cannot match.
They can analyze your current intake, identify specific barriers, and create a meal plan tailored to your preferences, schedule, and metabolic needs. They can also provide accountability and support, which improves adherence. Many insurance plans cover nutrition counseling, especially for people with obesity or related conditions like diabetes. If cost is a barrier, some dietitians offer sliding scale fees or group programs. The investment often pays for itself in faster, more sustainable results. The guidance on finding legitimate sources applies equally to finding qualified healthcare professionals.
Monitor progress with multiple metrics
The scale is one data point. It is not the only data point.
Track waist circumference, which is a better predictor of health risk than total body weight. Take progress photos every two to four weeks, as visual changes often precede scale changes. Notice how your clothes fit. Monitor energy levels, sleep quality, and mood. Track lab values like fasting glucose, A1C, cholesterol, and blood pressure. These metrics collectively paint a far more accurate picture of progress than the scale alone. Many people who think semaglutide is not working discover, when they review these other metrics, that significant positive changes are happening. The scale just has not caught up yet.
Be patient and consistent
Patience is not passive. It is an active choice to trust the process despite slow or non-linear progress.
Weight loss with semaglutide takes months, not weeks. Plateaus are normal. Fluctuations are expected. The people who succeed are not those who never struggle. They are those who keep going despite struggles. Consistency beats perfection. A protocol followed 80% of the time for six months will always outperform a perfect protocol abandoned after two months. Give yourself grace. Celebrate non-scale victories. And remember that sustainable change happens slowly. Those exploring realistic timelines for results will find that patience is universally required across all interventions.
Frequently asked questions
How long does it take for semaglutide to start working?
Most people begin noticing appetite suppression within one to two weeks of starting semaglutide, though the effect is often subtle at the initial 0.25 mg dose. Significant weight loss typically does not occur until you reach higher doses, usually 1.0 mg or above, which takes 8 to 12 weeks to reach through the standard titration schedule. Clinical trial data shows that the most dramatic results appear between months three and twelve. If you are looking for immediate results within the first few weeks, you will likely be disappointed. The timeline for seeing results explains why patience is critical for any peptide-based intervention. Semaglutide is a long-term intervention, not a quick fix. Early changes may be imperceptible, but cumulative effects over months produce meaningful outcomes.
Can I lose weight on semaglutide without exercise?
Yes, it is possible to lose weight on semaglutide without exercise. Clinical trials included lifestyle interventions but did not require intensive exercise programs. Many participants lost significant weight through diet changes and appetite suppression alone. However, exercise improves outcomes in multiple ways. It preserves muscle mass, which prevents metabolic slowdown. It burns additional calories, expanding your caloric deficit. And it improves insulin sensitivity, which enhances the medication mechanisms of action. People who combine semaglutide with regular physical activity, particularly resistance training, consistently see better results than those who rely on the medication alone. If you are physically able to exercise, even moderate activity like walking 30 minutes per day, it will improve your outcomes. The athletic performance resources provide context for integrating activity into your protocol.
What is the best diet to follow while on semaglutide?
There is no single best diet for everyone on semaglutide. The most effective diet is the one you can sustain long-term while maintaining a caloric deficit. That said, certain dietary patterns tend to work well with semaglutide mechanisms. Higher protein diets, 25 to 40 grams per meal, enhance satiety and preserve muscle mass. Lower glycemic index diets, emphasizing whole foods over refined carbohydrates, stabilize blood sugar and reduce cravings. Diets rich in vegetables and fiber support gut health and promote fullness.
Some people thrive on structured approaches like Mediterranean, low-carb, or intermittent fasting. Others prefer flexible eating with portion control. The key is to find an approach that feels sustainable, not punishing. Work with a registered dietitian if possible to create a personalized plan. And remember that adherence beats perfection. A good diet followed consistently will always outperform a perfect diet abandoned after two weeks.
Why did I lose weight initially but now the scale is not moving?
Plateaus are a normal, expected part of weight loss. After an initial period of consistent loss, your body adapts. Your resting metabolic rate decreases. Hormones shift to defend against further loss. This is metabolic adaptation, and it happens to everyone. The plateau does not mean semaglutide stopped working. It means your body has adjusted to the new caloric intake level. Strategies to break a plateau include increasing physical activity, particularly resistance training. Rechecking food intake to ensure you have not unintentionally increased calories.
Taking a one to two week diet break at maintenance calories to reset hormones. Adjusting macronutrient ratios, such as increasing protein. And simply being patient, as weight loss is not linear and the scale may stay stable for weeks before dropping again as water retention patterns shift. The strategies to maximize results provide additional approaches for breaking through plateaus.
Should I increase my dose if I am not losing weight?
If you have not yet reached the 2.4 mg maintenance dose and you are not experiencing significant side effects, continuing the standard titration schedule to higher doses is appropriate. Many people see minimal results at 0.25 mg or 0.5 mg and assume the medication is not working, when in reality they simply have not reached a therapeutic dose yet. However, once you reach 2.4 mg, the decision to increase further should involve your healthcare provider. Some providers are using higher off-label doses, 3.0 mg or more, for patients who tolerate the medication well but have not achieved sufficient weight loss at standard doses. This is not yet standard practice and carries unknown long-term risks. Before increasing the dose, ensure you have addressed all lifestyle factors, including food intake, exercise, sleep, and stress. If you have optimized those variables and still see no response after several months at 2.4 mg, discuss higher doses or alternative medications with your provider.
Can I drink alcohol while taking semaglutide?
You can drink alcohol while taking semaglutide, but it may interfere with your weight loss and increase side effects. Alcohol adds empty calories that can prevent a caloric deficit. It impairs judgment, leading to poor food choices. It disrupts sleep quality, which sabotages weight loss through hormonal mechanisms. And it can intensify semaglutide side effects, particularly nausea. Some people report that alcohol hits harder or faster while on semaglutide, possibly due to delayed gastric emptying. If you choose to drink, do so in moderation, defined as up to one drink per day for women and two for men. But if you are not seeing results, consider eliminating alcohol entirely for 30 to 60 days to determine if it is a limiting factor. Many people find that temporary elimination reveals how much alcohol was interfering with their progress.
What if I cannot afford to stay on semaglutide long-term?
Cost is a significant barrier for many people. Semaglutide is expensive, often $1,000 or more per month without insurance. If cost is prohibitive, explore these options. Check if your insurance covers semaglutide for weight loss. Some plans do, especially if you have related conditions like diabetes or pre-diabetes. Ask your provider about manufacturer coupons or patient assistance programs. Novo Nordisk, the maker of Wegovy, offers savings programs that can significantly reduce out-of-pocket costs for eligible patients. Consider compounded semaglutide from licensed compounding pharmacies, which is often cheaper than brand-name versions, though quality and regulation vary. Discuss switching to a less expensive GLP-1 agonist if available. And if none of these options work, focus on maximizing results during the time you can afford the medication. Build sustainable habits around diet, exercise, sleep, and stress management so that when you eventually discontinue semaglutide, you have the tools to maintain your progress. The cost calculator can help you plan and budget for long-term protocols.
External resources
For readers seeking additional evidence-based information on semaglutide and weight management, the following resources provide authoritative, peer-reviewed data:
STEP 1 Trial Published in NEJM - The landmark clinical trial demonstrating 14.9% average weight loss with semaglutide 2.4 mg over 68 weeks. Essential reading for understanding the evidence base behind semaglutide for weight management.
Obesity Medicine Association Clinical Practice Statement on GLP-1 Agonists - Comprehensive clinical guidance on using GLP-1 receptor agonists for obesity treatment, including practical management strategies and addressing non-response.
Metabolic Adaptation During Weight Loss: A Systematic Review - Detailed examination of how metabolism adapts during weight loss, explaining why plateaus occur and evidence-based strategies to address them.
The Role of Sleep in Weight Loss and Metabolic Health - Research review demonstrating the critical importance of sleep quality for weight management and metabolic function.
Obesity Action Coalition - Patient advocacy organization providing education, support, and resources for individuals dealing with obesity and weight management challenges.
NIH Guidelines on Managing Overweight and Obesity in Adults - Evidence-based clinical guidelines from the National Institutes of Health on comprehensive obesity treatment, including lifestyle, pharmacological, and surgical interventions.
Moving forward with realistic expectations and evidence-based action
If semaglutide is not working for you right now, that does not mean you are broken. It means there is a variable, or several variables, preventing the medication from doing its job. This guide covered every major reason semaglutide might stall or fail, from dose and timing issues to medical conditions, lifestyle factors, and metabolic adaptation. It also provided specific, actionable strategies to address each barrier. Your next step is not to give up. Your next step is to systematically identify and remove the obstacles in your specific situation. Start with the basics. Are you at a therapeutic dose? Have you given it enough time? Are you tracking your food intake? Are you exercising? Are you sleeping well? Are you managing stress? If the answer to any of those questions is no, that is where you begin. If you have addressed all of those and still see no response, work with your healthcare provider to investigate medical conditions, medication interactions, or alternative treatments like tirzepatide or combination therapy.
Weight loss is not linear. It is not fast. And it is not the same for everyone. But with the right information, the right support, and the right adjustments, most people can achieve meaningful results. [SeekPeptides](https://www.seekpeptides.com/) members access detailed protocols for optimizing GLP-1 agonist therapy, including troubleshooting guides, combination strategies, and personalized support from experts who understand the complexity of weight management. Whether you continue with semaglutide, switch to a different medication, or pursue an entirely different approach, the knowledge you gain here will serve you. Because understanding why something is not working is the first step to making it work. And that understanding, combined with persistence and evidence-based action, is how you finally break through.
The actors in this Truman Show, the clinical trials, the statistics, the mechanisms, have played their parts. Now the script is yours to write. The scale might not cooperate today. It might not cooperate next week. But if you address the variables within your control, stay consistent, and give your body the time it needs to respond, the breakthrough will come. Not because you hoped for it. Because you engineered the conditions that make it inevitable.
That is not magic. That is science. And science, when applied correctly, works.