Feb 21, 2026

Tired of reading five different microdosing tirzepatide articles and walking away with five completely different schedules? You are not alone. The internet is flooded with conflicting information about microdosing tirzepatide, and most of it glosses over the one thing that actually matters. The schedule. Not just what dose to take, but when to take it, how long to stay at each level, and what signals tell you it is time to move up, hold steady, or pull back.
Here is the reality. Standard tirzepatide protocols start at 2.5 mg weekly and push you up to 5 mg after just four weeks.
For some people that works perfectly. For others, that pace triggers nausea so severe they quit before the medication ever has a chance to work. Microdosing offers a different path, one that begins at doses as low as 0.25 mg and climbs at a pace your body can actually tolerate. But without a clear schedule, even the gentlest approach can go sideways. Too fast and you are back to hugging the toilet. Too slow and you spend months at doses too low to activate the GLP-1 and GIP receptors that make tirzepatide effective in the first place.
This guide lays out exactly how to structure a microdose tirzepatide schedule from the very first injection to maintenance. Week-by-week protocols, timing strategies, schedule modifications for specific situations, and the clinical data behind why slower titration can produce better long-term outcomes. Whether you are working with a compounded formulation or adjusting a standard prescription with your provider, you will find a schedule that fits. SeekPeptides has compiled the most comprehensive scheduling resource available, drawing from clinical trial data, practitioner protocols, and real-world community experience.
What microdosing tirzepatide actually means (and why the schedule matters more than the dose)
Microdosing tirzepatide means starting at doses significantly below the FDA-approved 2.5 mg weekly starting point and escalating more slowly than standard protocols recommend. Some practitioners define microdosing as any starting dose under 2.5 mg. Others reserve the term for ultra-low protocols beginning at 0.125 mg to 0.5 mg weekly. The exact definition varies, but the principle stays consistent. Start lower. Go slower.
Why does the schedule matter so much?
Because tirzepatide is a dual-acting peptide that activates both GLP-1 and GIP receptors simultaneously. These receptors control appetite signaling, insulin sensitivity, gastric emptying, and metabolic rate. When you flood them with a dose your body is not prepared for, the gastrointestinal system rebels. Nausea, vomiting, constipation, bloating, and acid reflux are the most common reasons people abandon tirzepatide treatment altogether.
The schedule determines everything. It determines how quickly those receptors adapt, how severe your side effects will be, how consistently you can stay on treatment, and ultimately how much weight you lose. A well-designed microdose schedule does not just reduce discomfort. It builds a foundation for long-term success by allowing your digestive system, appetite centers, and metabolic pathways to adjust incrementally rather than all at once.
Think of it this way. Standard titration is like jumping into a cold pool. Microdosing is like walking in from the shallow end. You end up in the same water. But one approach is a lot less likely to make you jump back out.
Standard tirzepatide schedule vs microdose schedule compared
Before diving into specific microdose protocols, you need to understand what you are modifying and why. The standard tirzepatide dosing schedule follows a fixed escalation pattern designed to reach therapeutic doses as quickly as possible while maintaining some degree of tolerability.
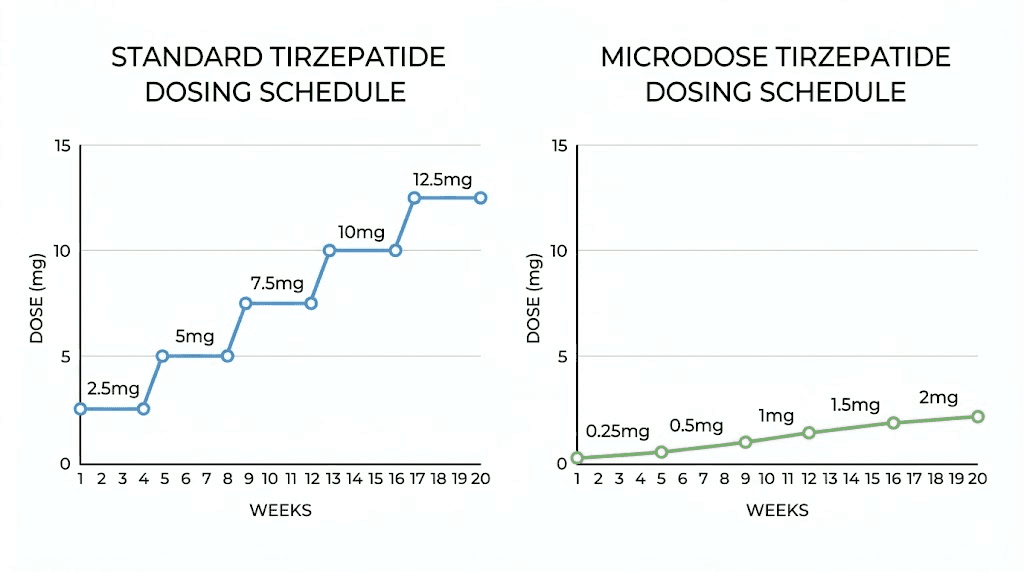
The standard FDA-approved schedule
The manufacturer-recommended titration looks like this. Start at 2.5 mg weekly for four weeks. Increase to 5 mg weekly for another four weeks. Then escalate to 7.5 mg, 10 mg, 12.5 mg, and finally 15 mg in four-week intervals. This means a patient following the standard schedule reaches the maximum dose of 15 mg by week 20, just five months after starting.
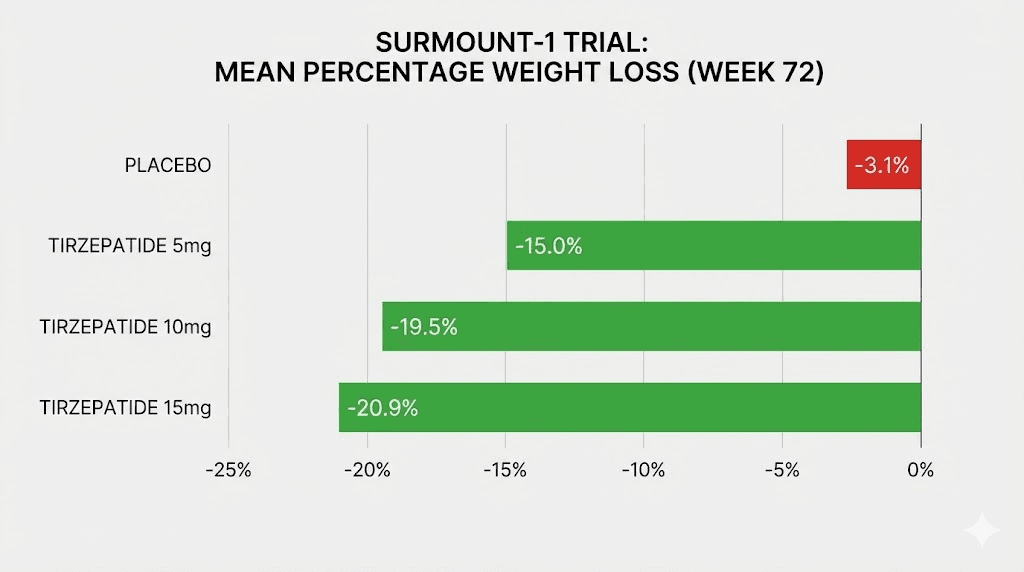
In the SURMOUNT-1 clinical trial published in the New England Journal of Medicine, participants on the 5 mg dose achieved an average weight loss of 16% of body weight over 72 weeks. Those on 10 mg lost approximately 19.5%, and the 15 mg group achieved roughly 20.9%. These are impressive numbers. But they come with a cost.
Across all SURMOUNT trials, gastrointestinal side effects affected a significant percentage of participants. Nausea hit roughly 25-33% of participants depending on the dose. Diarrhea affected 15-23%. Vomiting occurred in 5-13%. And these numbers represent the clinical trial environment where patients received careful monitoring and support. Real-world discontinuation rates tend to be even higher.
The microdose alternative
A microdose schedule fundamentally changes two variables. The starting dose drops below 2.5 mg, sometimes dramatically. And the time spent at each dose level extends from the standard four weeks to six, eight, or even twelve weeks. Some practitioners also split doses into smaller, more frequent injections rather than one weekly shot, although this approach remains less common.
The trade-off is straightforward. You lose speed but gain tolerability. A microdose schedule might take 12-16 weeks to reach the same 5 mg dose that standard titration hits in eight weeks. But if standard titration makes you so miserable that you quit at week three, the slower path that keeps you on treatment wins every time.
Here is a side-by-side comparison:
Factor | Standard schedule | Microdose schedule |
|---|---|---|
Starting dose | 2.5 mg weekly | 0.25-1.0 mg weekly |
Time to reach 5 mg | 4-8 weeks | 8-16 weeks |
Dose increase interval | Every 4 weeks | Every 4-8 weeks |
GI side effect severity | Moderate to high | Mild to moderate |
Dropout risk | Higher early on | Lower overall |
Time to meaningful weight loss | 4-8 weeks | 6-12 weeks |
Long-term adherence | Variable | Typically higher |
Neither approach is universally better. The right schedule depends on your GI sensitivity, your weight loss goals, your timeline, and your tolerance for discomfort. But the data increasingly suggests that patients who can stay on treatment longer achieve better outcomes regardless of how quickly they reach their target dose.
The complete week-by-week microdose tirzepatide schedule
This is the core of what you came here for. A detailed, week-by-week microdose tirzepatide schedule that takes you from your very first sub-therapeutic dose all the way to a clinically effective maintenance level. This schedule draws from practitioner protocols, community experience, and the general principles of GLP-1 receptor agonist titration established in clinical trials.
One critical note before we begin. This schedule requires a compounded formulation of tirzepatide or a provider willing to prescribe custom doses. The branded products (Mounjaro and Zepbound) come in pre-filled pens with fixed doses of 2.5, 5, 7.5, 10, 12.5, and 15 mg. You cannot microdose with a pre-filled pen. Compounded tirzepatide from a licensed pharmacy allows the flexibility to draw precise doses from a multi-use vial.
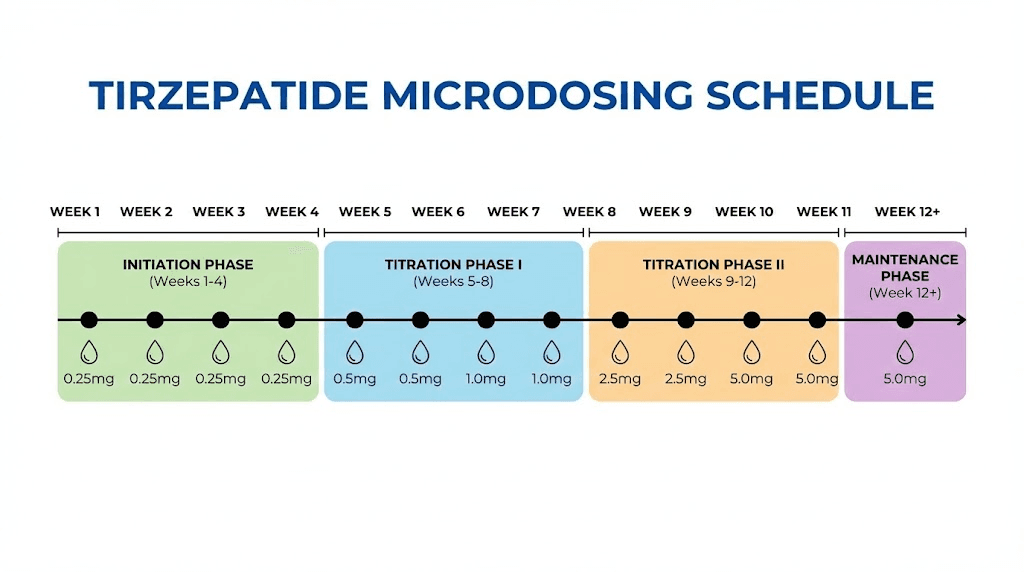
Phase 1: introduction (weeks 1-4)
The introduction phase is about one thing and one thing only. Teaching your body that this new molecule exists. You are not trying to lose weight yet. You are not even trying to suppress appetite. You are building a baseline of tolerance.
Week 1: 0.25 mg
Your first injection. One-tenth of the standard starting dose. At this level, most people feel absolutely nothing. No appetite suppression. No nausea. No change whatsoever. That is exactly the point. You are introducing the peptide to your GLP-1 and GIP receptors without overwhelming them. Inject on your chosen day (more on timing below), note how you feel over the next 48 hours, and move on.
Week 2: 0.5 mg
Double the first dose, still one-fifth of standard. Some people report the faintest whisper of reduced hunger around this dose. Most still notice nothing significant. If you experienced any headaches or mild nausea in week 1, stay at 0.25 mg for another week before moving up. The schedule is a guide, not a prison.
Week 3: 0.75 mg
Now you are at roughly one-third of the standard starting dose. This is where some individuals begin noticing subtle changes. Slightly smaller portions at meals. A bit less interest in snacking. The effect is gentle, almost easy to miss. Pay attention to it. This subtle shift is your body beginning to respond.
Week 4: 1.0 mg
The one-milligram mark. Still below standard starting dose by 60%, but now in a range where meaningful receptor activation begins. Mild appetite reduction is common here. Some people notice changes in energy levels. If you have been tolerating each increase without issues, you are building a solid foundation for the next phase.
Phase 2: building (weeks 5-10)
The building phase is where the schedule gets interesting. You are now entering dose ranges that start producing noticeable effects, both therapeutic and potential side effects. Move through this phase at whatever pace your body allows. Some people breeze through in six weeks. Others need eight or ten. Both timelines are fine.
Week 5-6: 1.5 mg
This is the first dose level where most people notice real appetite suppression. Meals become smaller naturally. The constant background noise of food thoughts quiets down. This is also where the first GI effects can appear. Mild nausea after eating, some burping or bloating, or occasional constipation. If these are manageable, stay for two weeks and prepare to advance. If nausea is more than mild, stay an extra week or two.
Week 7-8: 2.0 mg
Close to the standard starting dose now, but your body has had seven weeks of gradual preparation instead of zero. The difference in tolerability is usually dramatic. People who crashed at 2.5 mg on day one often sail through 2.0 mg after a proper microdose ramp-up. Appetite suppression should be clearly noticeable. You might find yourself forgetting to eat or feeling full much sooner than usual.
Week 9-10: 2.5 mg
Welcome to the official starting dose, except you are arriving here after ten weeks of preparation rather than on day one. This is where the microdose schedule begins to converge with standard protocols. The difference is that your receptors have been gently primed, your GI tract has adapted to the medication mechanism, and your body knows what to expect. Most people experience significantly fewer side effects reaching 2.5 mg through microdosing compared to starting cold at this level. You should notice meaningful appetite suppression, some early changes in body composition, and improved blood sugar control if that was an issue.
Phase 3: optimization (weeks 11-18)
Now you are in therapeutic territory. From here, the microdose approach rejoins something closer to the standard titration schedule, but you can still move more slowly than the four-week jumps if your body prefers it.
Weeks 11-14: 5.0 mg
The 5 mg dose is where clinical trials show real weight loss begins. In SURMOUNT-1, participants at this dose lost an average of 16% of body weight over 72 weeks. Appetite suppression becomes strong and consistent. Early morning hunger often disappears entirely. Portion sizes drop significantly. This is a maintenance dose for some people. If you are losing weight steadily, feeling good, and tolerating the dose well, there is no requirement to go higher. Check your tirzepatide dosing in units carefully to ensure accuracy at this level.
Weeks 15-18: 7.5 mg
If weight loss has stalled at 5 mg or you want additional metabolic effects, moving to 7.5 mg is the next step. This dose sits in a range that many practitioners consider the sweet spot, strong enough for significant results but lower than the doses most associated with severe GI effects. Some people stay here long-term as their maintenance dose and achieve excellent outcomes.
Phase 4: maintenance (week 19 onward)
Maintenance is not a single dose. It is the dose at which you achieve steady, sustainable weight loss or weight maintenance with tolerable side effects. For some people that is 5 mg. For others it is 10 mg or even 15 mg. The microdose schedule has given your body the gradual preparation to find that sweet spot without the turbulence of aggressive escalation.
If you need to continue increasing beyond 7.5 mg, maintain four-week intervals between increases (7.5 mg to 10 mg, then 10 mg to 12.5 mg, then 12.5 mg to 15 mg). The microdose advantage is that by the time you reach these higher doses, your body has had months of adaptation. Patients who microdosed through the early phases typically report much better tolerance at higher doses compared to those who rushed through standard titration.
Three practical microdosing protocols for different goals
Not everyone needs the same schedule. Your goals, timeline, and sensitivity determine which protocol fits best. Here are three distinct approaches based on the most common situations researchers and patients encounter.
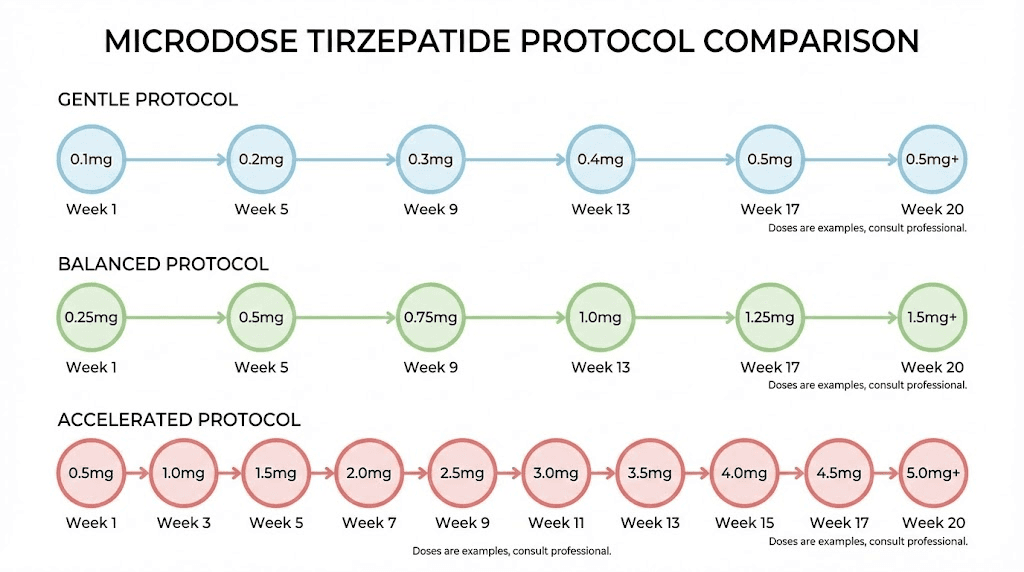
Protocol 1: the gentle start (for GI-sensitive individuals)
Goal: Minimize side effects completely while building to a therapeutic dose
Best for: People with histories of medication sensitivity, IBS, acid reflux, or those who tried standard tirzepatide and could not tolerate it
Complete schedule:
Weeks 1-2: 0.125 mg weekly
Weeks 3-4: 0.25 mg weekly
Weeks 5-6: 0.5 mg weekly
Weeks 7-8: 0.75 mg weekly
Weeks 9-10: 1.0 mg weekly
Weeks 11-14: 1.5 mg weekly
Weeks 15-18: 2.0 mg weekly
Weeks 19-22: 2.5 mg weekly
Weeks 23-26: 5.0 mg weekly
Time to therapeutic dose: 22-26 weeks
Expected results: Minimal GI discomfort, gradual appetite reduction beginning around weeks 7-10, meaningful weight loss starting around weeks 15-18
This protocol takes nearly six months to reach 5 mg, but for someone who previously abandoned treatment due to side effects, six months on treatment beats three weeks of misery followed by quitting. If anxiety or insomnia appear at any stage, that is a signal to hold the current dose for an additional two to four weeks before advancing.
Protocol 2: the balanced approach (most common)
Goal: Reduce side effects while reaching therapeutic doses in a reasonable timeframe
Best for: First-time users, people who want a smoother experience than standard titration, those working with compounded formulations
Complete schedule:
Weeks 1-2: 0.25 mg weekly
Weeks 3-4: 0.5 mg weekly
Week 5: 1.0 mg weekly
Weeks 6-7: 1.5 mg weekly
Week 8-9: 2.0 mg weekly
Weeks 10-13: 2.5 mg weekly
Weeks 14-17: 5.0 mg weekly
Time to therapeutic dose: 13-17 weeks
Expected results: Mild GI effects at most transitions, noticeable appetite suppression by weeks 6-8, meaningful weight loss beginning around weeks 10-13
This is the protocol most practitioners recommend when patients specifically request microdosing. It roughly doubles the time to reach 5 mg compared to standard titration but cuts GI side effect severity dramatically. Most people on this protocol describe the transition as smooth and manageable. You can use the compounded tirzepatide dosage calculator to verify your exact injection volumes at each stage.
Protocol 3: the accelerated microdose (for mild sensitivity)
Goal: Slightly gentler than standard without adding months to the timeline
Best for: People with mild concerns about side effects, those who tolerated other GLP-1 medications like semaglutide but want a slightly easier start with tirzepatide
Complete schedule:
Weeks 1-2: 0.5 mg weekly
Weeks 3-4: 1.0 mg weekly
Weeks 5-6: 1.5 mg weekly
Weeks 7-10: 2.5 mg weekly
Weeks 11-14: 5.0 mg weekly
Time to therapeutic dose: 10-14 weeks
Expected results: Some mild nausea during the first two to three increases, clear appetite suppression by week 5, weight loss beginning around weeks 7-10
This protocol adds only a few weeks compared to standard titration but provides a meaningful buffer during the critical early weeks when side effects are most likely to drive people away from treatment. If you respond quickly to tirzepatide, this protocol gives you enough cushion without dragging out the timeline unnecessarily.
Choosing your injection day and timing
The day you inject matters more than most guides acknowledge. Tirzepatide has a half-life of approximately five days, which means the medication remains active throughout the entire week between injections. But blood levels peak roughly 8-48 hours after injection, and this peak is when side effects are most likely to occur. Smart scheduling around this peak can make a significant difference in your day-to-day experience.
Best day of the week to inject
Choose a day where the 24-48 hours after injection fall on a period when you can rest if needed. For most people, that means injecting on Friday evening or Saturday morning. If nausea hits, it peaks over the weekend when you are not at work or managing demanding obligations. By Monday, blood levels have stabilized and any GI discomfort has typically passed.
Another approach is to inject on a day that strategically manages your appetite through the week. Since appetite suppression is strongest in the 24-72 hours after injection, some people inject on Sunday evening so the peak suppression hits during the workweek when structured eating is easier to maintain. Then appetite returns slightly on Friday and Saturday, allowing more relaxed weekend eating.
There is no universally correct day. Pick one that works with your lifestyle, then stick with it consistently. Consistency matters more than the specific day.
Best time of day to inject
Morning injections and evening injections both have advocates. Timing your GLP-1 shot correctly can influence how you experience side effects during the critical first 24 hours.
Morning injection advantages: You can monitor how you feel throughout the day. If nausea appears, you are awake and can manage it with ginger tea, small sips of water, or light food. Some people find that morning injection followed by a light breakfast reduces nausea compared to injecting on an empty stomach.
Evening injection advantages: If nausea is your primary concern, injecting before bed means you sleep through the initial peak absorption period. Many people who experience daytime nausea after morning injections find that evening doses eliminate this problem entirely. The trade-off is that some people report difficulty sleeping after injection, though this is less common at microdoses.
Injection site considerations
For subcutaneous injection, the three primary sites are the abdomen, front of the thigh, and back of the upper arm. Each site has slightly different absorption characteristics. The abdomen typically provides the most consistent absorption, which is why most tirzepatide injection guides recommend it as the primary site. Rotate between sites to prevent lipohypertrophy (tissue hardening) at any single location.
During the microdose phase, absorption differences between sites are largely academic because the doses are so small. But building good injection habits early, including proper rotation, correct injection technique, and sterile preparation, pays dividends later when you are working with higher doses where precision matters more.
How to adjust your schedule when side effects appear
No microdose schedule survives first contact with your body perfectly intact. Side effects will appear at some point during titration, and knowing how to adjust your schedule in response is the difference between a temporary bump and a treatment-ending crisis.
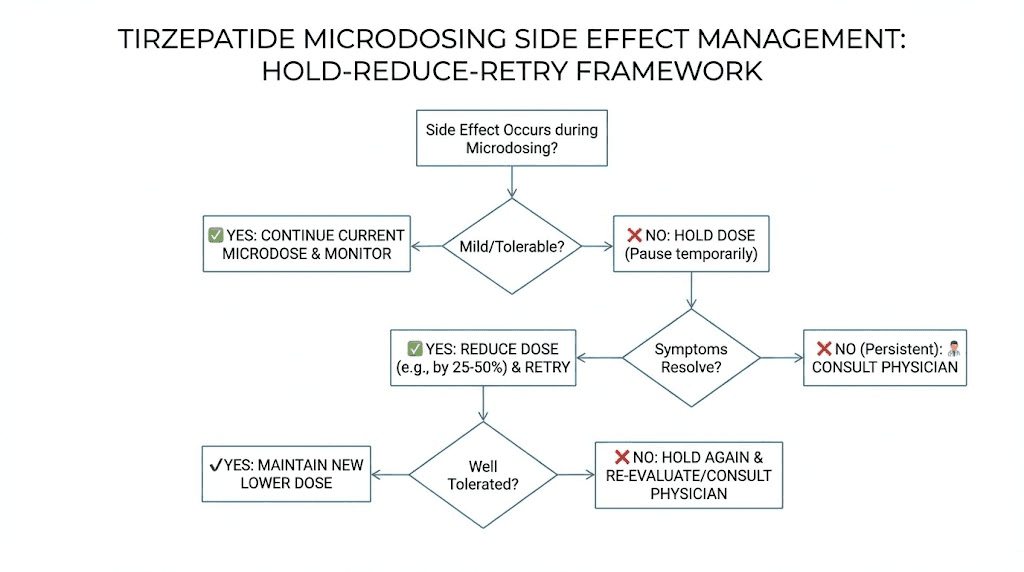
The hold, reduce, retry framework
When side effects appear at any dose level, follow this three-step process.
Step 1: Hold. Do not increase your dose at the next scheduled interval. Stay at the current dose for one to two additional weeks. Many side effects are transient, appearing when a dose is new and fading as your body adapts. A week or two of holding often resolves mild nausea, body aches, or digestive discomfort without requiring any dose change at all.
Step 2: Reduce (if holding does not resolve it). Drop back to the previous well-tolerated dose for two to four weeks. This is not failure. This is data. Your body is telling you that the jump was too much, and going back to let it stabilize is the intelligent response. After two to four weeks at the lower dose, try advancing again, this time perhaps with a smaller increment.
Step 3: Retry. Attempt the dose increase again after the hold or reduction period. If the same side effects return, consider splitting the dose (discussed below) or accepting the lower dose as your current ceiling and holding there longer before trying again in four to six weeks.
Managing specific side effects during microdosing
Nausea: The most common side effect at every dose level. During microdosing, nausea is typically mild, a queasy feeling rather than active vomiting. Eat small, frequent meals. Avoid fatty or greasy foods. Stay hydrated. Follow a tirzepatide-friendly diet plan focused on lean proteins, complex carbohydrates, and easily digestible foods. If nausea persists for more than two weeks at the same dose, that dose is your current ceiling.
Constipation: Tirzepatide slows gastric emptying, which can lead to constipation. This is dose-dependent and often more pronounced at higher levels, but some people experience it even at microdoses. Increase water intake to at least 80-100 ounces daily. Add fiber gradually (too fast causes bloating). Magnesium citrate (200-400 mg daily) is a common and effective countermeasure. See our complete tirzepatide constipation treatment guide for detailed strategies.
Fatigue: Some people report feeling tired during the first few days after increasing their dose. This usually resolves within one to two weeks. If persistent tiredness from tirzepatide becomes an issue, ensure you are eating enough protein (at least 0.7-1.0 grams per pound of body weight) and that caloric restriction is not too aggressive. The medication reduces appetite, but you still need adequate fuel, especially during the adaptation period.
Headaches: Usually related to reduced food intake and mild dehydration rather than the medication itself. Increase water intake and ensure you are consuming adequate electrolytes. If headaches persist beyond the first week at a new dose, hold at that level before advancing further.
Muscle pain and body aches: Less common but reported by some users, particularly at higher microdose levels (1.5 mg and above). Muscle pain from tirzepatide can sometimes indicate that protein intake is insufficient relative to the reduced caloric intake the medication causes. Ensure adequate protein, stay active with moderate exercise, and consider adding the right supplements to support recovery.
The science behind slower titration
Microdosing is not just a comfort strategy. There is a growing body of evidence suggesting that slower titration may produce better long-term outcomes through several distinct mechanisms.
Receptor desensitization and adaptation
GLP-1 receptors can become temporarily desensitized when exposed to high agonist concentrations too quickly. This desensitization is one reason some patients experience a plateau effect where appetite suppression weakens despite increasing doses. By introducing the agonist gradually, microdosing may allow receptors to upregulate rather than downregulate, potentially maintaining sensitivity longer.
This is theoretical rather than proven in controlled trials specifically for tirzepatide microdosing. But the principle of gradual receptor adaptation is well-established in pharmacology across multiple drug classes. Beta-blockers, antidepressants, and even caffeine all demonstrate better long-term receptor responses when introduced slowly.
Gastric adaptation
Tirzepatide slows gastric emptying, the rate at which food moves from the stomach into the small intestine. This mechanism is central to both its appetite-suppressing effects and its GI side effects. When gastric emptying decelerates too quickly, the result is nausea, bloating, and that uncomfortable feeling of food sitting like a brick in your stomach.
Gradual dose escalation allows the gastric motility system to adapt incrementally. Think of it as training your stomach to operate at a new speed rather than slamming on the brakes. Patients who microdose through the early weeks typically report much less GI distress at therapeutic doses compared to those who started at 2.5 mg immediately.
Improved long-term adherence
This is the argument with the strongest practical evidence. A retrospective academic study on GLP-1 dose titration found that real-world adherence to recommended titration schedules is often suboptimal, with GI side effects being a primary driver of both dose delays and treatment discontinuation. Any protocol that reduces early side effects and keeps patients on treatment longer should, in theory, produce better outcomes over months and years.
The SURMOUNT clinical trials showed that tirzepatide effectiveness is strongly correlated with treatment duration. Participants who stayed on treatment for the full 72 weeks achieved dramatically better results than those who discontinued early, regardless of dose. Weight loss continued accumulating through the entire study period, with many patients still losing weight at the 72-week mark. This suggests that staying on treatment, not reaching the highest dose fastest, is the critical variable for success.
Metabolic adaptation without extreme caloric restriction
At very low microdoses, the metabolic effects of tirzepatide begin before significant appetite suppression occurs. Early improvements in insulin sensitivity, blood glucose regulation, and metabolic flexibility can begin at doses below those needed for appetite reduction. This means the body starts becoming more metabolically efficient before caloric intake drops significantly, which may reduce the metabolic adaptation (metabolic slowdown) that sometimes accompanies rapid weight loss.
Understanding how tirzepatide affects metabolism helps explain why some practitioners believe microdosing creates a healthier metabolic transition than aggressive dosing. The body shifts toward better fuel utilization before it is forced to deal with dramatically reduced food intake.
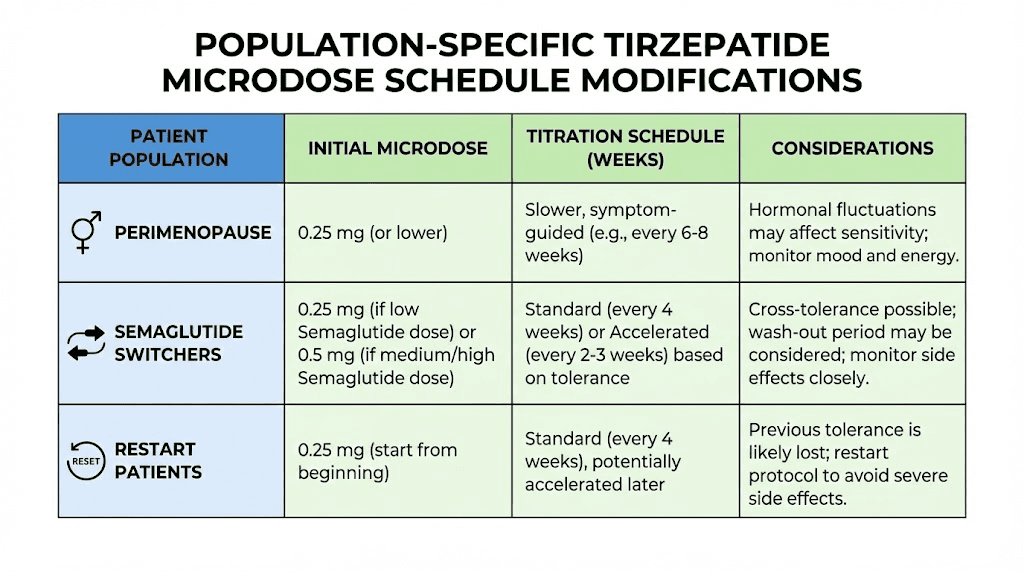
Schedule modifications for specific populations
The standard microdose schedule works well as a baseline, but certain populations benefit from specific modifications. If you fall into any of these categories, discuss modifications with your prescriber.
Women in perimenopause or menopause
Hormonal fluctuations during perimenopause can amplify GI sensitivity and make side effects less predictable. Estrogen fluctuations affect GLP-1 receptor sensitivity, which means the same dose might produce different effects at different points in the hormonal cycle. Women in this category often do best with Protocol 1 (the gentle start) with an additional modification: extending each dose level by one to two weeks during periods of noticeable hormonal fluctuation. Tirzepatide can also affect menstrual cycles, so tracking both your dosing schedule and your cycle helps identify patterns.
People switching from semaglutide
If you are switching between GLP-1 medications, your body already has some receptor adaptation from the previous drug. This means you may be able to start at a higher microdose level (0.5-1.0 mg instead of 0.25 mg) and advance more quickly through the early phases. However, tirzepatide also activates GIP receptors, which semaglutide does not. The dual mechanism means GI effects can surprise people who thought they knew what to expect. Use the tirzepatide vs semaglutide dosage chart to find equivalent starting points, then apply Protocol 3 (accelerated microdose) with the understanding that you should still hold or reduce if new GIP-related side effects appear.
People with a history of eating disorders
Microdosing is particularly important for this population because the aggressive appetite suppression of standard doses can trigger disordered eating patterns. A very gradual schedule allows the person and their treatment team to monitor the psychological response to reduced appetite alongside the physical effects. Protocol 1 with extended holds at each level and regular check-ins with a mental health professional is the safest approach.
People restarting after a break
If you stopped tirzepatide for any reason and are restarting after more than two weeks off, do not jump back to your previous dose. The body loses adaptation quickly once the medication clears. If you were at 5 mg before stopping, restart at 1.0-2.0 mg and work back up over four to six weeks. If you were at 2.5 mg, restart at 0.5-1.0 mg. The tirzepatide not working anymore guide covers restart protocols in more detail.
People with diabetes or insulin resistance
Tirzepatide was originally developed for type 2 diabetes (Mounjaro) before being approved for weight management (Zepbound). For people using it to manage blood glucose alongside weight loss, microdosing requires additional monitoring. Blood sugar can drop at any dose level, not just therapeutic ones, because even small amounts of tirzepatide improve insulin sensitivity. Monitor blood glucose more frequently during the introduction phase (weeks 1-4) and adjust diabetes medications under your provider supervision to avoid hypoglycemia.
Common scheduling mistakes and how to avoid them
Even with a clear schedule in hand, people make predictable mistakes that undermine their microdosing results. These are the most common ones and the fixes for each.
Mistake 1: increasing too fast because "nothing is happening"
This is the most common mistake by far. You hit weeks 3-4 of your microdose schedule, feel absolutely nothing, and conclude the dose is too low to be doing anything useful. So you skip ahead. Big mistake.
The whole point of the early weeks is subtherapeutic dosing for receptor preparation, not immediate results. Feeling nothing is the expected outcome at 0.25-0.75 mg. It does not mean the medication is failing or that your body does not respond. It means the dose is doing exactly what it should, introducing the molecule without triggering a strong response. Jumping ahead eliminates the tolerance-building advantage that makes microdosing work.
Mistake 2: inconsistent injection timing
Tirzepatide works best with consistent weekly dosing. Taking it Tuesday one week, Friday the next, and Sunday the following week creates irregular blood level patterns that increase side effect risk and reduce effectiveness. Pick a day. Stick with it. If you need to shift your injection day, do it by moving one day at a time over successive weeks rather than making a sudden three to four day change.
Mistake 3: not eating enough
Microdosing reduces appetite gradually. But some people combine microdosing with aggressive caloric restriction, essentially using both a medication and a strict diet to create an extreme deficit. This approach backfires. Severe caloric restriction during microdosing leads to fatigue, muscle loss, hair loss, and metabolic slowdown. Let the medication guide your appetite naturally. Eat when hungry, prioritize protein (aim for at least 100-120 grams daily), and do not force a deficit beyond what the medication creates on its own. Refer to our tirzepatide meal plan for structured eating guidance during treatment.
Mistake 4: ignoring the reconstitution math
When working with compounded tirzepatide vials, the difference between 0.25 mg and 2.5 mg comes down to careful measurement. A miscalculated reconstitution can mean injecting ten times your intended dose. Use a proper reconstitution chart and double-check your math every single time. Use insulin syringes with clear unit markings. When in doubt, have someone verify your calculation before drawing the dose. The peptide dosage calculation guide covers the math in detail.
Mistake 5: comparing your schedule to someone else
Online communities are full of people sharing their dosing timelines. Someone always seems to be tolerating higher doses faster, losing weight more quickly, or experiencing zero side effects. Comparing your microdose schedule to theirs is pointless because response to tirzepatide varies dramatically between individuals based on genetics, body composition, metabolic health, diet quality, and dozens of other factors. Your schedule works for your body. Their schedule works for theirs. The only comparison that matters is how you are responding to your current dose.
Mistake 6: stopping too soon
Some people microdose for eight to ten weeks, see modest results, and conclude the medication does not work for them. But they never reached a therapeutic dose. At 1.0-1.5 mg, you are still in the sub-therapeutic range. Real, clinically significant weight loss typically begins at 2.5 mg and accelerates at 5 mg. If you abandon the protocol before reaching at least 2.5-5.0 mg, you have not given the medication a fair trial. Understanding how long tirzepatide takes to work is critical for setting realistic expectations during microdosing.
Tracking your progress on a microdose schedule
Because microdosing is a longer process than standard titration, tracking becomes especially important. You need objective data to know whether to advance, hold, or reduce, and you need it organized in a way that reveals patterns over weeks and months.
What to track daily
Keep a simple daily log. Nothing elaborate. Just four data points each day.
Appetite level (1-10 scale): Rate your overall hunger and food interest each evening. A 10 means ravenous, thinking about food constantly. A 1 means zero interest in eating. Track this number daily and watch for trends. A gradual decline from 7-8 down to 4-5 over a few weeks indicates the medication is building effectiveness.
GI symptoms (yes/no plus severity): Note any nausea, constipation, bloating, acid reflux, or digestive discomfort. Rate severity as mild (noticeable but not limiting), moderate (affects daily activities), or severe (cannot function normally). This data is your primary input for hold/reduce/retry decisions.
Energy level (1-10 scale): Track energy alongside appetite. A drop in energy often precedes noticeable appetite suppression by a few days. If energy drops without appetite changes, it may indicate inadequate caloric or protein intake rather than a medication effect.
Weight (morning, after bathroom, before eating): Daily weight fluctuates wildly based on water, sodium, hormones, and bowel movements. Do not react to any single day reading. Instead, track a 7-day rolling average. The average trend over weeks is what matters. Weight may not change significantly during the first 6-10 weeks of microdosing, and that is completely normal.
What to track weekly
At the end of each week, review your daily logs and note the following.
Average appetite score for the week: Compare to previous weeks. A decline of 1-2 points from one week to the next typically indicates the medication is working. Stable scores suggest adaptation to the current dose.
Number of GI symptom days: More than three to four days of symptoms in a week after holding for two weeks suggests the dose is your current ceiling.
Weekly average weight: Plot this on a graph. Do not obsess over it during the sub-therapeutic microdose phases. Weight loss is not the primary goal during weeks 1-8. Tolerance building is.
Measurements (optional but valuable): Waist circumference and hip circumference can reveal body composition changes before the scale moves. Measure in the same spot, at the same time, once per week.
The SeekPeptides platform provides tracking tools and protocol guidance that can simplify this process. Members get access to structured tracking templates, progress analysis, and community support from others following similar schedules.
When to increase, hold, or decrease your dose
This section provides clear decision criteria for each scenario. Ambiguity about when to change doses is one of the biggest sources of frustration in microdosing, so use these guidelines as your framework.
Increase when all three conditions are met
You have been at the current dose for at least the minimum time specified in your chosen protocol. Your average GI symptom severity for the past week is none to mild. And your appetite score has stabilized (not declining further at the current dose). All three conditions must be true simultaneously. If any one is not met, hold.
Hold when any of these apply
You are still experiencing moderate GI symptoms after two weeks at the current dose. Your schedule says it is time to increase but you have only been symptom-free for less than one week. You are experiencing life stressors (illness, travel, major schedule disruption) that make assessing true medication effects difficult. Or you are happy with your current rate of progress and see no reason to push higher.
Holding is not falling behind. Many people achieve excellent results at moderate doses they could have passed through weeks ago. The clinical data shows that tirzepatide results correlate more strongly with treatment duration than with dose magnitude. Spending extra weeks at a lower dose that you tolerate well often produces equivalent long-term outcomes to rushing to higher doses that cause compliance issues.
Decrease when any of these apply
Severe GI symptoms that do not respond to two weeks of holding. Any symptom that significantly impairs daily functioning. New symptoms that appear for the first time at a higher dose (such as joint pain or significant muscle pain) and do not resolve within one to two weeks. Or if you are losing weight too rapidly (more than 1-2% of body weight per week consistently), which increases the risk of gallstones, muscle loss, and metabolic disruption.
When decreasing, drop back to the last dose that you tolerated well and stay there for at least four weeks before attempting to increase again. Track carefully during this hold period to establish a firm baseline.
Dose splitting: an alternative scheduling approach
Some microdosing practitioners use a technique called dose splitting, where instead of one weekly injection, the total weekly dose is divided into two or three smaller injections spread throughout the week.
How dose splitting works
Instead of injecting 2.5 mg once on Friday, you would inject approximately 0.83 mg on Monday, Wednesday, and Friday. Or split it into two doses: 1.25 mg on Monday and 1.25 mg on Thursday. The total weekly dose remains the same, but blood levels stay more stable throughout the week rather than spiking after injection and tapering before the next dose.
Potential benefits of splitting
More stable blood levels mean fewer peaks and troughs. The post-injection peak is when side effects are worst, so reducing that peak by splitting into smaller doses can reduce nausea and GI discomfort. Some users report more consistent appetite suppression throughout the week rather than strong suppression for three days followed by returning hunger for two days before the next injection.
Practical considerations
Dose splitting requires more injections per week, which some people find burdensome. It also requires more precise reconstitution calculations since you are drawing smaller volumes more frequently. And it is important to keep injection times consistent even when splitting, for example, always injecting around 8 AM on your chosen days rather than randomly throughout the day.
This approach works best with reconstituted vials from compounding pharmacies. Pre-filled pens cannot be split. Use a reconstitution chart to verify exact draw volumes for split doses, and always store the vial properly between uses. Check our guide on tirzepatide refrigeration and room temperature stability to ensure potency between injections.
Transitioning from microdose to standard maintenance
At some point, your microdose schedule converges with standard therapeutic dosing. This transition deserves its own discussion because the psychological and practical shift from "microdosing" to "regular dosing" can create unnecessary anxiety.
The convergence point
Once you reach 2.5-5.0 mg weekly, you are no longer microdosing by any definition. You are on a standard therapeutic dose that has been reached through a non-standard route. Everything from this point forward follows the same principles as standard tirzepatide treatment, with one important advantage: your body is better prepared for higher doses thanks to the gradual build-up.
Deciding your maintenance dose
Not everyone needs to go to 15 mg. The clinical trials tested multiple dose levels and all produced significant weight loss. At 5 mg, average weight loss was 16% of body weight. At 10 mg, 19.5%. At 15 mg, 20.9%. The difference between 10 mg and 15 mg is only about 1.4 percentage points of additional weight loss, but the side effect burden often increases more substantially.
Your maintenance dose is the one where three things align: you are achieving your goals (weight loss, blood sugar control, or both), side effects are tolerable, and you can maintain consistent weekly dosing without disruption. For many people who microdosed through the early phases, that sweet spot falls at 5.0-7.5 mg rather than the maximum 15 mg.
Use the tirzepatide dosing for weight loss in units guide to translate milligrams into syringe units at your maintenance dose, and review the tirzepatide dosage in units reference to ensure measurement accuracy.
Long-term schedule considerations
Tirzepatide is currently indicated for long-term use. Stopping the medication typically results in weight regain, as the SURMOUNT-4 trial demonstrated. Participants who switched from tirzepatide to placebo after 36 weeks regained approximately half their lost weight over the following 52 weeks. This means your microdose schedule is not just a pathway to a dose, it is the beginning of a long-term treatment relationship.
Plan your schedule accordingly. Establish a sustainable injection routine you can maintain for months or years. Build it into your weekly habits like any other recurring commitment. The long-term GLP-1 treatment considerations guide provides additional context for planning extended use.
Supporting your microdose schedule with nutrition and lifestyle
A microdose tirzepatide schedule does not exist in a vacuum. What you eat, how you move, and how you manage stress all influence how well the medication works and how well you tolerate dose increases.
Nutrition during microdosing phases
During the introduction phase (weeks 1-4), eat normally. The medication is not suppressing your appetite yet, and there is no reason to restrict calories prematurely. Focus on establishing good baseline habits: adequate protein, plenty of vegetables, consistent hydration.
During the building phase (weeks 5-10), appetite begins declining. This is when nutritional strategy becomes important. Prioritize protein at every meal because as total food intake drops, getting enough protein becomes harder but more critical. Aim for 100-120 grams daily for most adults. Good protein sources include lean meats, fish, eggs, Greek yogurt, and legumes. The complete guide to eating on tirzepatide provides meal-by-meal recommendations.
During optimization and maintenance (weeks 11 onward), your eating pattern will have naturally shifted to smaller portions and less frequent meals. Many people move to two meals plus a snack rather than three full meals. Avoid the temptation to skip meals entirely. Even on days when appetite is low, eating at least two small, protein-rich meals protects muscle mass and prevents the metabolic slowdown that comes from severely undereating.
For detailed meal planning, our food guide for GLP-1 users covers optimal food choices, and the foods to avoid on tirzepatide resource identifies specific items that worsen GI side effects.
Exercise considerations
Exercise during microdosing follows a simple principle: do not add aggressive new exercise routines simultaneously with dose increases. Your body is already adapting to a new medication. Stacking a new high-intensity workout program on top of a dose increase creates too many variables and makes it impossible to determine whether fatigue, nausea, or muscle soreness comes from the medication or the exercise.
Keep your exercise routine stable during dose transitions. If you want to increase exercise intensity, do it during weeks when your dose is holding steady, not during the week you increase. Walking 30-60 minutes daily is the single best exercise during any phase of tirzepatide treatment, safe at any dose, beneficial for metabolism, and unlikely to cause problems.
Hydration
Hydration affects tirzepatide tolerability more than most people realize. Dehydration amplifies nausea, constipation, headaches, and fatigue, all common side effects during dose escalation. Aim for a minimum of 80-100 ounces (2.4-3 liters) of water daily. More during hot weather or exercise days. Keep water accessible at all times and sip consistently rather than trying to catch up with large volumes at once.
Supplements that support the schedule
Certain supplements work well alongside tirzepatide. Key ones include:
Magnesium citrate (200-400 mg daily): Helps prevent constipation, supports sleep quality, and reduces muscle cramps
B12 or methylcobalamin: GLP-1 agonists can reduce B12 absorption over time, and some compounded formulations include B12 in the compound for this reason
Electrolytes: Sodium, potassium, and magnesium supplementation helps offset the dehydration risk from reduced food intake
Protein powder: A practical way to maintain protein targets when appetite makes eating full meals difficult
Some compounded formulations include additional ingredients like glycine, niacinamide, or glycine plus B12 combinations. These additions may offer benefits during the microdosing process, though evidence is still limited.
Comparing oral vs injectable microdose schedules
Most microdosing discussion focuses on injectable tirzepatide because that is the standard delivery method. But oral tirzepatide and sublingual drops have entered the conversation as alternative delivery routes that some people use for microdosing.
Injectable microdosing
Subcutaneous injection remains the gold standard for tirzepatide administration. Bioavailability is high and consistent, dose accuracy is precise, and the once-weekly injection schedule aligns perfectly with microdose titration protocols. The downsides are the injection itself (some people dislike needles) and the need for proper storage and reconstitution when using compounded vials.
For detailed injection guidance, see the complete peptide injection guide and how to inject GLP-1 for step-by-step technique instructions.
Oral and sublingual microdosing
Oral and sublingual tirzepatide formulations have lower bioavailability than injections, meaning a higher nominal dose is needed to achieve the same blood levels. This complicates microdosing calculations. The oral vs injection comparison and tablets vs injections comparison explore these differences in detail.
For microdosing specifically, oral formulations present challenges. Absorption varies based on food intake, stomach pH, and timing, making it harder to achieve the precise dose control that microdosing requires. If you prefer oral delivery, work closely with your provider to establish equivalent doses and monitor response carefully. The sublingual dosage chart provides conversion guidance.
What the research says about microdosing effectiveness
Let us be direct about the evidence base. There are currently no randomized controlled trials specifically studying tirzepatide microdosing protocols. This means the approach is based on pharmacological principles, clinical observation, and real-world reports rather than gold-standard evidence.
What the clinical trials tell us indirectly
The SURMOUNT clinical trial program provides indirect evidence that lower doses can be effective. In SURMOUNT-1, the 5 mg dose group lost an average of 16% of body weight, and 30% of those participants achieved weight loss of 20% or more. The 5 mg dose is the lowest therapeutic dose tested, and it produced clinically significant results in most participants.
The SURMOUNT-4 trial demonstrated that continued tirzepatide treatment is necessary to maintain weight loss. When participants switched from tirzepatide to placebo after initial weight loss, they regained approximately 14% of body weight over the following year. This finding is relevant to microdosing because it suggests that staying on any effective dose long-term matters more than reaching the highest dose quickly.
The upcoming SURMOUNT-MAINTAIN trial, expected to report results around mid-2026, will specifically compare the 5 mg maintenance dose against higher doses for weight maintenance after initial loss. This trial may provide the first direct evidence about whether lower maintenance doses are sufficient for long-term results, which would strongly support the microdosing philosophy of finding the minimum effective dose rather than pushing to the maximum.
What practitioners observe
Multiple clinical practices that offer tirzepatide microdosing protocols report anecdotally that patients who microdose through the introduction phase have significantly better long-term compliance. Dr. Shamsah Amersi, an OB-GYN specializing in metabolic health, describes microdosing GLP-1 medications as "a gentle, effective metabolic reset" and reports that her patients experience fewer GI side effects and better treatment continuity.
Several compounding pharmacy-affiliated clinics have published their microdosing protocols online, and while they vary in specifics, the general pattern is consistent: start lower, go slower, achieve similar long-term outcomes with better tolerability during the escalation phase.
What community experience shows
Online communities of tirzepatide users provide a large volume of real-world data, though obviously uncontrolled and subject to reporting bias. Community reports consistently describe 10-15% body weight loss with microdosing protocols, with users emphasizing the dramatically reduced side effect burden compared to their experiences with standard titration. Many users also report that microdosing allowed them to find a "sweet spot" dose (often 5.0-7.5 mg) where they achieved satisfactory results without needing to push to 10 mg or 15 mg.
These reports align with the clinical trial data showing that the majority of weight loss occurs at the 5 mg dose level, with diminishing returns at higher doses relative to the increased side effect burden.
Compounded vs brand-name tirzepatide for microdosing
The regulatory landscape for compounded tirzepatide changed significantly in March 2025 when the FDA ended enforcement discretion for compounded versions. This has direct implications for anyone planning a microdose schedule.
Brand-name limitations for microdosing
Mounjaro and Zepbound come in pre-filled auto-injector pens with fixed doses (2.5, 5, 7.5, 10, 12.5, and 15 mg). These pens cannot be partially administered. You either inject the full dose or you do not inject at all. This makes true microdosing (starting below 2.5 mg) impossible with brand-name products.
The closest thing to microdosing with brand-name products is extending the time at the 2.5 mg level. Instead of moving to 5 mg after four weeks, some providers prescribe 2.5 mg for eight to twelve weeks before advancing. This is not microdosing in the strict sense, but it applies the same principle of slower escalation. The tirzepatide dosing guide covers extended titration options within brand-name constraints.
Compounded formulations for microdosing
Compounded tirzepatide from a licensed compounding pharmacy provides the flexibility needed for true microdosing. These formulations come in multi-use vials at concentrations that allow precise drawing of any desired dose. Common concentrations include 5 mg/mL and 10 mg/mL, from which microdoses as small as 0.125 mg can be accurately measured using insulin syringes.
When using compounded formulations, always verify the concentration of your vial and use the reconstitution chart to calculate exact draw volumes. At microdose levels, the difference between 0.25 mg and 2.5 mg might be only a few units on an insulin syringe, making accuracy critical. The units to mg conversion guide helps prevent dosing errors.
Storage considerations
Compounded vials require proper storage to maintain potency throughout your microdosing schedule. A multi-use vial at low doses will last longer than at higher doses, potentially several weeks. Follow tirzepatide refrigeration guidelines carefully, and understand expiration considerations for reconstituted products. Most compounded tirzepatide maintains potency for 28-42 days when refrigerated at 36-46 degrees F (2-8 degrees C).
Building a weekly microdose schedule template
Here is a practical weekly template you can use to structure your microdose tirzepatide schedule. Customize the specific dose and day to match your chosen protocol.
Sample weekly template
Sunday: Review previous week log. Compare appetite scores, GI symptoms, weight trend, and energy levels. Make a decision: advance dose next week, hold, or reduce. Update your tracking log.
Monday: Normal day. Track appetite, energy, GI symptoms.
Tuesday: Normal day. Track same metrics. Prepare injection supplies if your injection day is Wednesday.
Wednesday (injection day example): Inject at your consistent time (morning or evening). Note any immediate reactions. Track all daily metrics. Eat normally, do not skip meals on injection day.
Thursday: Peak absorption day. This is when side effects are most likely. Keep meals light if nausea appears. Stay hydrated. Track metrics. This is important data for dose decisions.
Friday: Most immediate side effects should be resolving. Track metrics. Resume normal activity if you rested Thursday.
Saturday: Medication levels stabilizing. Good day for exercise. Track metrics. Enjoy normal eating.
This template adapts to any injection day. The key principle is that the 24-48 hours after injection are the critical monitoring window, and your weekly review on Sunday sets up the following week plan.
How microdose scheduling relates to other peptide protocols
If you are interested in peptide research beyond tirzepatide, the principle of gradual dose escalation applies broadly. Many peptides benefit from slow introduction, and the scheduling concepts covered in this guide transfer to other compounds.
For weight management specifically, tirzepatide is the most studied option, but other peptides for weight loss follow similar titration principles. Semaglutide, for instance, uses a built-in escalation schedule starting at 0.25 mg monthly before reaching the 2.4 mg treatment dose. Semaglutide titration is inherently more gradual than tirzepatide standard dosing, which may be one reason it is often better tolerated initially despite ultimately reaching lower peak doses.
Other peptides in the GLP-1 family, including retatrutide, cagrilintide, and mazdutide, each have their own titration requirements. Understanding the microdose scheduling framework makes navigating any new peptide protocol more intuitive.
For broader peptide education, SeekPeptides provides comprehensive guides covering peptide dosing, cycle planning, stacking strategies, and safety considerations. The getting started with peptides guide is an excellent foundation for anyone new to this space.
Frequently asked questions
How long should a microdose tirzepatide schedule last before reaching a therapeutic dose?
Most microdose schedules take 10-26 weeks to reach a standard therapeutic dose of 2.5-5.0 mg, depending on which protocol you follow. The gentle protocol takes the longest (22-26 weeks), the balanced approach takes 13-17 weeks, and the accelerated version takes 10-14 weeks. There is no deadline. The schedule lasts as long as your body needs it to.
Can I microdose with Mounjaro or Zepbound pens?
Not in the traditional sense. Pre-filled pens deliver fixed doses starting at 2.5 mg and cannot be partially administered. The closest alternative is asking your provider to extend the 2.5 mg phase to 8-12 weeks instead of the standard 4 weeks. True sub-2.5 mg microdosing requires compounded tirzepatide from a licensed pharmacy.
What if I feel nothing during the first few weeks of microdosing?
That is completely expected. At 0.25-0.75 mg, the dose is intentionally sub-therapeutic. The purpose of these early weeks is receptor priming and GI tract adaptation, not appetite suppression or weight loss. Feeling nothing is the correct response at these doses. Do not skip ahead. The foundation matters.
Is microdosing tirzepatide supported by clinical evidence?
There are currently no randomized controlled trials specifically studying tirzepatide microdosing. The approach is based on general pharmacological principles (gradual receptor adaptation improves tolerability) and clinical observation. The broader peptide research landscape supports slow titration for improved adherence, and the SURMOUNT-MAINTAIN trial may provide relevant data when it reports results.
Can I drink alcohol on a microdose tirzepatide schedule?
Small amounts of alcohol are generally tolerated, especially at lower microdoses. However, alcohol can worsen nausea, contribute to dehydration (which amplifies side effects), and add empty calories that work against your goals. Many people find their alcohol tolerance changes significantly on tirzepatide. If you choose to drink, start with less than you normally would and see how you respond.
Should I take any supplements alongside my microdose schedule?
Magnesium citrate, B12, and electrolytes are the most commonly recommended supplements during tirzepatide treatment at any dose. A high-quality protein supplement can also help maintain protein targets when appetite is reduced. Review the complete supplements guide for tirzepatide users for specific recommendations.
How do I store my compounded tirzepatide between microdose injections?
Compounded tirzepatide should be stored in the refrigerator at 36-46 degrees F (2-8 degrees C). Since microdose volumes are small, a single vial may last several weeks. Refrigerated tirzepatide typically maintains potency for 28-42 days after reconstitution. Never freeze the solution, and minimize the time spent at room temperature.
What happens if I miss a dose on my microdose schedule?
If you miss by one to two days, inject as soon as you remember and resume your regular schedule the following week. If you miss by more than three to four days, inject at your normal dose and consider the week a partial dose. If you miss an entire week, inject at your normal dose and continue. Do not double up to "catch up." Missing a dose during the microdose phase is less disruptive than during maintenance because the sub-therapeutic doses are not producing strong effects that would be lost.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access personalized scheduling tools, dosing calculators, and expert guidance that takes the guesswork out of building an effective tirzepatide schedule.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your doses stay precise, your schedule stay consistent, and your results stay lasting.