Mar 22, 2026

Some people on tirzepatide eat 900 calories a day and feel proud of themselves. Others eat 1,800 and panic that it is too much. Both groups are making mistakes, just in opposite directions. And both are sabotaging the very results they are chasing.
The calorie question is the single most common concern among tirzepatide users. It makes sense. The medication suppresses appetite so dramatically that your relationship with food changes almost overnight. Meals that once felt normal now feel enormous. Portions shrink. Hunger fades. And somewhere in that shift, people lose track of what their body actually needs to function, to preserve muscle, to keep energy levels stable, and to lose fat rather than everything else.
Here is the truth that most guides skip over. There is no single calorie number that works for everyone on tirzepatide. Your ideal intake depends on your starting weight, your activity level, your age, your sex, and how far along you are in treatment. A 220-pound man starting his first dose needs a fundamentally different calorie target than a 160-pound woman six months into her protocol. What they share is the need for a calculated, intentional approach rather than guessing or simply eating as little as possible.
This guide breaks down exactly how to determine your personal calorie target on tirzepatide, backed by clinical research and practical strategies that prevent the most common pitfalls. You will learn how to calculate your baseline, adjust as you progress through different doses, protect your muscle mass, and structure meals that keep you nourished even when your appetite has all but disappeared. SeekPeptides has compiled the research, the real-world data, and the practical frameworks so you do not have to piece it together from scattered forums and conflicting advice.
How tirzepatide changes your calorie needs
Tirzepatide does not just reduce hunger. It fundamentally rewires how your brain responds to food. A 2025 study published in Nature Medicine found that after just six weeks, participants consumed an average of 658 fewer calories during a single lunch meal compared to baseline. That is not a subtle change. That is a complete restructuring of eating behavior.
The mechanism involves dual action on both GLP-1 and GIP receptors. While semaglutide targets only GLP-1, tirzepatide hits both pathways simultaneously. This dual approach slows gastric emptying, signals satiety to the hypothalamus, and reduces the neural reward response to high-fat, high-sugar foods. Brain imaging studies confirm that tirzepatide actually lowers the brain activation patterns that drive cravings.
But here is where people get confused.
A reduced appetite does not mean you should eat as little as possible. The medication creates an opportunity, a window where eating less feels natural and sustainable. Your job is to use that window wisely, not to push caloric restriction to dangerous extremes. Research from the Diabetes Care journal shows that tirzepatide reduces spontaneous energy intake by approximately 525 to 856 calories per day compared to placebo. This built-in reduction, combined with a moderate intentional deficit, is where the magic happens.
A separate Cell Metabolism study from 2025 revealed something fascinating about tirzepatide and metabolic rate. Unlike what happens with calorie restriction alone, tirzepatide did not significantly worsen metabolic adaptation in human participants. It did, however, increase fat oxidation, meaning your body becomes better at burning fat for fuel rather than carbohydrates. This finding has direct implications for how you should structure your calorie intake and macronutrient ratios.
The practical takeaway is straightforward. Tirzepatide handles a large portion of the calorie reduction automatically through appetite suppression. You do not need to white-knuckle your way through extreme restriction. Instead, you need a strategic calorie target that maintains nutrition, preserves lean tissue, and works with the medication rather than against it.
General calorie targets for tirzepatide users
Before diving into personalized calculations, here are the evidence-based ranges that most clinical protocols and nutrition experts recommend for tirzepatide weight loss.
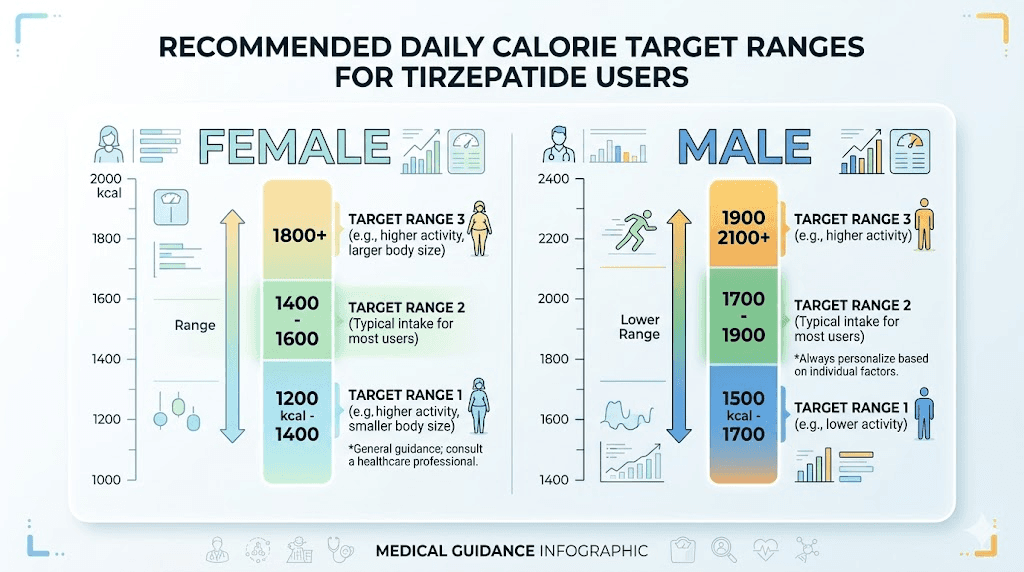
For women: 1,200 to 1,500 calories per day during active weight loss phases.
For men: 1,500 to 1,800 calories per day during active weight loss phases.
These ranges create a deficit of approximately 500 to 750 calories below total daily energy expenditure, which supports a safe loss rate of one to two pounds per week. Combined with the additional appetite-driven reduction from tirzepatide itself, total weight loss often exceeds this baseline rate, particularly in the early months of treatment.
But these numbers are starting points, not absolute rules. Several factors push you toward the higher or lower end of these ranges.
Factors that increase your calorie needs
If you exercise regularly, particularly resistance training, your body requires more fuel to support muscle repair and recovery. Active individuals should aim for the higher end of their range or even slightly above it. A sedentary 150-pound woman might do well at 1,200 calories. A 150-pound woman who lifts weights three times per week and walks daily needs closer to 1,500 or beyond.
Height matters too. Taller individuals have more lean tissue and higher baseline metabolic rates. Age is another consideration, though perhaps not in the direction most people assume. While metabolism does slow with age, the more critical factor is that older adults lose muscle more easily during calorie restriction. This means adequate protein and calories become even more important, not less, as you age.
Factors that decrease your calorie needs
As you lose weight, your calorie needs drop. This is basic physics. A smaller body requires less energy to maintain itself. The metabolic rate decreases by approximately 50 to 100 calories for every 10 pounds lost. Someone who started at 2,000 calories and has lost 30 pounds may now need only 1,700 to 1,850 calories to maintain the same deficit.
Sedentary lifestyles also push calorie needs lower. If your daily activity consists primarily of desk work with minimal movement, you burn fewer calories than someone who walks 8,000 steps daily or has a physically demanding job.
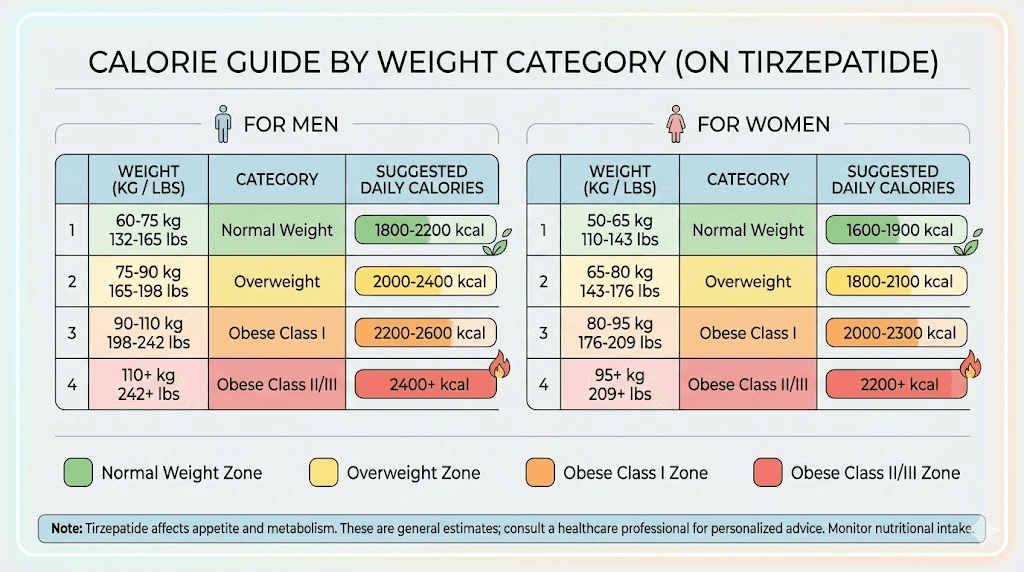
Calorie targets by body weight category
Starting weight | Women (calories/day) | Men (calories/day) | Deficit target |
|---|---|---|---|
150-180 lbs | 1,200-1,350 | 1,500-1,650 | 500 cal/day |
180-220 lbs | 1,300-1,450 | 1,600-1,750 | 500-600 cal/day |
220-260 lbs | 1,350-1,500 | 1,650-1,800 | 600-750 cal/day |
260+ lbs | 1,400-1,600 | 1,700-1,900 | 750 cal/day |
These ranges assume moderate activity levels. Adjust upward by 100 to 200 calories if you exercise regularly, and consider the lower end if you are largely sedentary. The goal is always a sustainable deficit, never an extreme one. Extreme caloric restriction leads to fatigue, muscle wasting, nutrient deficiencies, and ultimately the kind of metabolic damage that makes regaining weight almost inevitable.
How to calculate your personal calorie target
Generic ranges help as guardrails. But your actual target should come from a personalized calculation. Here is how to do it step by step.
Step 1: Calculate your basal metabolic rate
Your basal metabolic rate, or BMR, represents the calories your body burns at complete rest. It is the energy required just to keep your organs functioning, your heart beating, and your lungs breathing. The most widely used formula is the Mifflin-St Jeor equation.
For women: BMR = (10 x weight in kg) + (6.25 x height in cm) - (5 x age) - 161
For men: BMR = (10 x weight in kg) + (6.25 x height in cm) - (5 x age) + 5
For example, a 40-year-old woman who weighs 200 pounds (91 kg) and stands 5 feet 6 inches (168 cm) would calculate: (10 x 91) + (6.25 x 168) - (5 x 40) - 161 = 910 + 1,050 - 200 - 161 = 1,599 calories. That is her BMR, the bare minimum her body needs at rest.
Step 2: Factor in activity level
Nobody lies in bed all day. Your actual energy expenditure, called total daily energy expenditure or TDEE, accounts for all movement and exercise. Multiply your BMR by an activity factor.
Activity level | Description | Multiplier |
|---|---|---|
Sedentary | Desk job, minimal movement | 1.2 |
Lightly active | Light exercise 1-3 days/week | 1.375 |
Moderately active | Moderate exercise 3-5 days/week | 1.55 |
Very active | Hard exercise 6-7 days/week | 1.725 |
Using our example, if this woman is lightly active (walks regularly, does some light exercise): 1,599 x 1.375 = 2,199 calories. That is her TDEE, the total energy she burns in a day.
Step 3: Subtract your deficit
For safe, sustainable weight loss on tirzepatide, subtract 500 to 750 calories from your TDEE. This creates a deficit that supports one to two pounds of weekly weight loss without triggering excessive metabolic slowdown or muscle loss.
Continuing our example: 2,199 - 500 = 1,699 calories per day. This would be her target, falling comfortably within the general guidelines for women.
A critical note here. Tirzepatide already reduces spontaneous calorie intake by 500 to 850 calories through appetite suppression. If you are consistently eating well below your calculated target without trying, you may be in too deep a deficit. This is where many people make their biggest mistake. They assume less is always better. It is not. A deficit beyond 1,000 calories per day risks significant muscle loss, nutritional deficiencies, and hormonal disruption.
The SeekPeptides dosage calculators can help you understand your medication protocol, but for calorie calculations, the formula above gives you a solid, research-backed starting point.
Step 4: Set your floor
Regardless of what the math says, certain minimums exist for safety. Women should not go below 1,200 calories per day. Men should not go below 1,500 calories per day. Any intake below 800 calories requires direct medical supervision and is generally not recommended even with tirzepatide.
These floors exist because it becomes extremely difficult to meet micronutrient needs below these thresholds. Vitamins, minerals, electrolytes, essential fatty acids, and adequate fiber all require a baseline volume of food. Dropping below these floors for more than a few days risks deficiencies that can cause body aches, hair loss, sleep disruption, and immune suppression.
Macronutrient breakdown for tirzepatide users
Calories matter. But where those calories come from matters just as much, especially when you are on a medication that reduces total food intake. Every bite counts more when you are eating less.
The optimal ratio
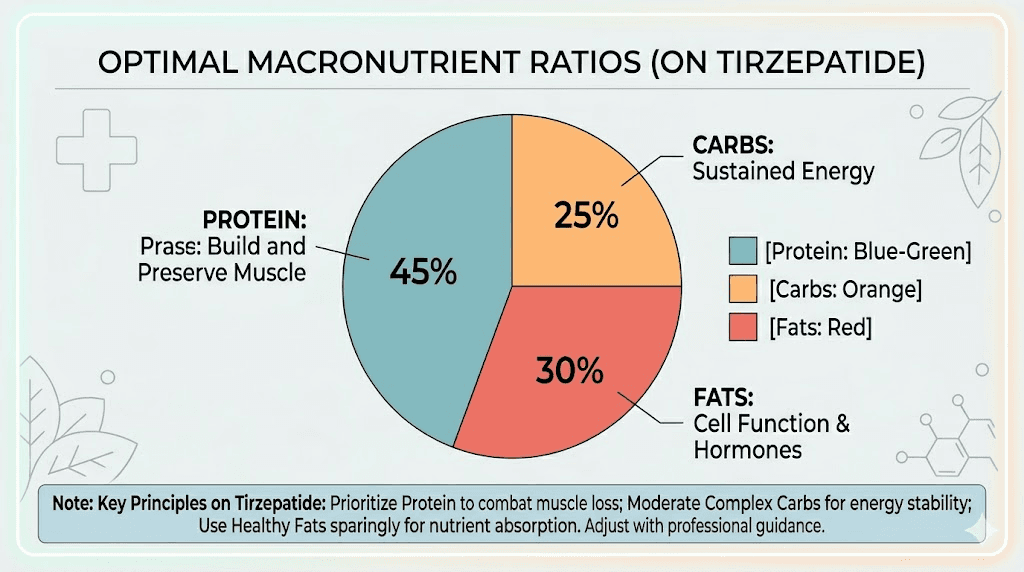
Based on current research and clinical nutrition guidelines for GLP-1 agonist users, the recommended macronutrient breakdown is:
Protein: 30 to 35 percent of total calories
Carbohydrates: 35 to 40 percent of total calories
Fat: 25 to 30 percent of total calories
This ratio differs significantly from the standard dietary recommendations (which typically suggest 50 percent carbohydrates, 20 percent protein, 30 percent fat). The shift toward higher protein is deliberate and critical for tirzepatide users.
At 1,500 calories per day with this ratio, your macros would look like this:
Macronutrient | Percentage | Grams at 1,200 cal | Grams at 1,500 cal | Grams at 1,800 cal |
|---|---|---|---|---|
Protein | 30-35% | 90-105g | 113-131g | 135-158g |
Carbohydrates | 35-40% | 105-120g | 131-150g | 158-180g |
Fat | 25-30% | 33-40g | 42-50g | 50-60g |
Why the protein emphasis? Because tirzepatide-driven weight loss, like all weight loss, involves some degree of lean mass reduction. Clinical data from the SURMOUNT trials showed that approximately 25 to 30 percent of weight lost on tirzepatide comes from lean mass rather than fat. Higher protein intake is the single most effective strategy for minimizing this ratio and keeping more of the weight loss in the fat category.
Carbohydrate quality matters
Not all carbohydrates affect your body the same way. On tirzepatide, avoiding high-glycemic carbohydrates becomes even more important. The medication already affects blood sugar regulation through its GIP receptor activity. Pairing this with low-glycemic carbohydrates, things like sweet potatoes, quinoa, oats, legumes, and non-starchy vegetables, creates a more stable blood sugar environment.
High-glycemic foods (white bread, sugary cereals, processed snacks) can trigger bloating, blood sugar spikes and crashes, and worsen the gastrointestinal side effects that tirzepatide already tends to cause. Fiber-rich carbohydrates also help with constipation, one of the most common side effects, by adding bulk and promoting gut motility.
Fat selection
Fats should come primarily from unsaturated sources: olive oil, avocados, nuts, seeds, and fatty fish. These provide essential fatty acids and support hormone production, which becomes especially important during sustained calorie restriction. Avoid large amounts of saturated and fried fats, which can worsen digestive symptoms that tirzepatide users commonly experience.
Keep fat portions moderate at each meal. Because fat is calorie-dense (9 calories per gram versus 4 for protein and carbohydrates), it is easy to overshoot your target with just a tablespoon or two of oil. This does not mean avoiding fat. It means measuring it rather than eyeballing it.
Protein requirements and muscle preservation
This section deserves its own spotlight because protein is arguably the single most important nutritional consideration for anyone on tirzepatide. Get this wrong, and you risk losing muscle along with fat. Get it right, and you protect your metabolic engine while the medication handles fat reduction.
How much protein you actually need
The research is clear. Standard protein recommendations (0.8 grams per kilogram of body weight) are insufficient for people undergoing significant weight loss. For tirzepatide users, the evidence supports substantially higher intake.
Minimum target: 1.2 grams per kilogram of ideal body weight per day
Optimal target: 1.4 to 1.6 grams per kilogram of ideal body weight per day
Per-meal target: 25 to 40 grams of protein at each eating occasion
Note the distinction between current body weight and ideal body weight. Using current body weight for someone at 280 pounds would yield protein targets that are unnecessarily high and difficult to achieve within calorie limits. Instead, calculate based on your target or ideal weight.
Here is what this looks like in practice:
Ideal body weight | Minimum protein (1.2g/kg) | Optimal protein (1.4-1.6g/kg) |
|---|---|---|
130 lbs (59 kg) | 71g/day | 83-94g/day |
150 lbs (68 kg) | 82g/day | 95-109g/day |
170 lbs (77 kg) | 92g/day | 108-123g/day |
190 lbs (86 kg) | 103g/day | 120-138g/day |
210 lbs (95 kg) | 114g/day | 133-152g/day |
Why muscle preservation matters beyond aesthetics
Muscle is not just about looking toned. It is your primary metabolic tissue. Every pound of muscle burns approximately 6 to 7 calories at rest, compared to 2 calories per pound of fat. Lose 10 pounds of muscle, and your daily calorie burn drops by 60 to 70 calories permanently. Over a year, that seemingly small difference translates to over 7 pounds of potential weight regain.
A 2025 systematic review published in PMC examined tirzepatide and skeletal muscle mass across multiple clinical trials. The findings showed that approximately 70 to 75 percent of weight lost on tirzepatide is fat mass, with 25 to 30 percent being lean mass. This ratio is consistent with other weight loss interventions, but it can be improved with adequate protein intake and resistance training.
A Lancet Diabetes and Endocrinology post-hoc analysis of the SURPASS-3 trial revealed something encouraging. Tirzepatide treatment led to significant reductions in muscle fat infiltration and preserved fat-free muscle volume within clinically acceptable ranges over 52 weeks. This means the medication may actually improve muscle quality even as overall body weight decreases, provided nutritional support is adequate.
Practical protein strategies when appetite is low
Here is the challenge. Tirzepatide kills your appetite. Eating 120 grams of protein when you barely want to eat at all feels impossible some days. These strategies help.
Front-load protein. Make your first meal of the day protein-heavy. A breakfast with 35 to 40 grams of protein (eggs, Greek yogurt, protein shakes) sets the foundation. Even if later meals are smaller, you have already covered a third of your target.
Prioritize protein density. Choose foods that deliver the most protein per calorie. Chicken breast (31g protein per 165 calories), egg whites (11g per 52 calories), Greek yogurt (17g per 100 calories), and whey protein isolate (25g per 110 calories) all deliver substantial protein without using up your calorie budget.
Liquid calories can help. When solid food feels unappealing, a protein shake goes down easier. Blend whey protein with water or unsweetened almond milk, add some frozen berries, and you have 30 grams of protein in a form that requires minimal appetite.
Spread it across 4 meals. Instead of three large meals, try four smaller ones. Hitting 30 grams at each sitting is more manageable than 40 grams at three meals, and the more frequent eating pattern can help with gastrointestinal comfort on tirzepatide.
How calorie needs change as you lose weight
Your calorie target is not a set-and-forget number. It needs to evolve as your body changes. This is one of the most misunderstood aspects of long-term weight management on tirzepatide.
The recalculation schedule
Recalculate your calorie target under any of these conditions:
Every 10 to 15 pounds of weight loss. Every 8 to 12 weeks regardless of weight change. Any time your tirzepatide dose changes. Any time your activity level changes significantly.
The math is simple but important. For every 10 pounds you lose, your daily energy expenditure drops by approximately 50 to 100 calories. Someone who started at 240 pounds and has lost 40 pounds now burns 200 to 400 fewer calories per day than when they began. If they are still eating the same calorie target they started with, the deficit has narrowed substantially, and weight loss will slow or stall.
This is often the real explanation when people say tirzepatide stopped working. The medication is still working. The calorie math just shifted underneath them.
Metabolic adaptation on tirzepatide
Here is some genuinely good news from the research. The 2025 Cell Metabolism study found that tirzepatide did not significantly worsen metabolic adaptation in human participants. Metabolic adaptation, sometimes called adaptive thermogenesis or starvation mode, is the phenomenon where your metabolism slows beyond what weight loss alone would predict. It is the body actively fighting back against calorie restriction.
With tirzepatide, this fight appears to be less intense. The medication also increased fat oxidation, meaning your body shifts toward burning fat preferentially. This is a meaningful advantage over diet-only approaches, where metabolic adaptation can be aggressive and frustrating.
However, this does not mean you are immune to metabolic slowdown. It means the slowdown is proportional to your weight loss rather than exaggerated. You still need to recalculate. You still need to adjust. You just have a more cooperative metabolism to work with.
The plateau adjustment protocol
When weight loss stalls for two or more weeks despite consistent adherence, run through this checklist before making any changes:
First, verify your tracking accuracy. Are you measuring portions or estimating? Estimation errors of 20 to 30 percent are common and can erase an entire deficit. Liquid calories, cooking oils, and condiments are the most frequently undercounted items.
Second, recalculate your TDEE using your current weight. If you have lost significant weight since your last calculation, this alone may reveal the problem.
Third, assess your activity levels honestly. Have you been less active recently? Even small reductions in daily movement, fewer steps, skipping workouts, more sedentary weekends, can narrow the deficit.
Fourth, consider whether a dose adjustment with your healthcare provider might be appropriate. Higher tirzepatide doses provide stronger appetite suppression, which can reinstate a natural calorie deficit that has faded over time.
Only after addressing these factors should you consider dropping your calorie target. And when you do, reduce by no more than 100 to 150 calories at a time. Dramatic cuts lead to dramatic rebounds.

Common calorie mistakes on tirzepatide
After analyzing hundreds of tirzepatide protocols and outcomes, certain patterns emerge. These are the mistakes that derail progress most frequently.
Mistake 1: Eating too little
This is the most common mistake by far. It sounds counterintuitive. How can eating less be bad for weight loss?
Because extreme restriction triggers a cascade of problems. Below 1,000 calories, most people cannot meet basic nutritional needs. The body responds by downregulating thyroid function, reducing non-exercise activity thermogenesis (you fidget less, move less spontaneously, feel more lethargic), and breaking down muscle for amino acids. The result is crushing fatigue, poor sleep, irritability, and a metabolism that slows far more than the weight loss warrants.
The muscle loss is particularly devastating. You lose weight on the scale, but your body composition worsens. You end up lighter but with a higher body fat percentage. When you eventually return to normal eating, whether after stopping tirzepatide or reaching your goal, the reduced muscle mass means a lower calorie burn and faster regain.
Mistake 2: Not tracking at all
The opposite extreme. Some people assume tirzepatide handles everything and stop paying attention to what they eat entirely. While the medication does reduce appetite, it does not guarantee optimal nutrition. You can eat 1,200 calories of nutritionally empty food and technically be in a deficit while starving your body of what it needs.
Track for at least the first 4 to 8 weeks. After that, if you have established solid habits and understand portion sizes intuitively, you can relax the tracking. But during the adjustment period, when your appetite is shifting dramatically and your eating patterns are being rebuilt from scratch, tracking provides essential feedback.
Mistake 3: Ignoring protein
When appetite is low, people gravitate toward whatever sounds appealing. Often that means crackers, toast, soup, fruit, or other foods that are easy to eat but protein-poor. After weeks of this, muscle loss accelerates, energy drops, and the scale might look good but the mirror and strength levels tell a different story.
Make protein your non-negotiable. Build every meal around a protein source first, then add vegetables, then carbohydrates and fats. If you only have room for 400 calories at a meal, at least 120 to 160 of those should come from protein. This is the single most important dietary principle on tirzepatide.
Mistake 4: Drinking your calories without realizing it
A smoothie here. A latte there. A glass of juice with dinner. Liquid calories add up fast and provide minimal satiety. When you are working with a limited calorie budget, every calorie should earn its place. Sweetened drinks, fruit juices, regular sodas, and calorie-dense coffee drinks can consume 200 to 400 calories of your daily budget while providing almost no nutritional value.
Exception: protein shakes. These are liquid calories worth consuming because they solve the protein problem when appetite is low. Just choose low-sugar options and count them in your daily total.
Mistake 5: Weekend amnesia
Five days of 1,400 calories followed by two days of 2,500 calories creates a weekly average of about 1,714 calories, far less of a deficit than the weekday number suggests. Weekends account for 29 percent of your week. Consistency across all seven days matters more than perfection on weekdays alone.
You do not need to be rigid on weekends. But you do need to be honest. If you tend to eat more on Saturdays and Sundays, plan for it by eating slightly less during the week or by keeping weekend indulgences modest.
Meal planning strategies for your calorie target
Knowing your number is one thing. Hitting it consistently is another. These strategies bridge the gap between theory and daily practice.
The plate method
Fill half your plate with non-starchy vegetables (broccoli, spinach, peppers, green beans, cauliflower). Fill one quarter with lean protein (chicken, fish, turkey, tofu, eggs). Fill one quarter with complex carbohydrates (brown rice, sweet potato, quinoa, whole grain bread). Add a small amount of healthy fat (olive oil drizzle, quarter avocado, handful of nuts).
This visual approach works even when you are not counting calories precisely. It naturally creates meals in the 350 to 450 calorie range with solid macronutrient ratios. Three plates plus one snack puts you right in the target zone for most people.
Meal prepping for appetite fluctuations
Tirzepatide appetite varies day to day and week to week. Some days you feel almost normal hunger. Others you can barely look at food. Having pre-prepared meals eliminates the decision fatigue that leads to poor choices on both ends.
Prep 4 to 5 protein options at the start of each week. Grilled chicken, hard-boiled eggs, baked fish, and pre-portioned Greek yogurt give you grab-and-go protein regardless of how you feel. Add pre-washed vegetables and pre-cooked grains, and you can assemble a balanced meal in under three minutes.
On low-appetite days, having prepared food means you can eat something nutritious even when nothing sounds good. On higher-appetite days, portioned meals prevent overcompensation. Either way, planning beats improvising when calories and macros matter.
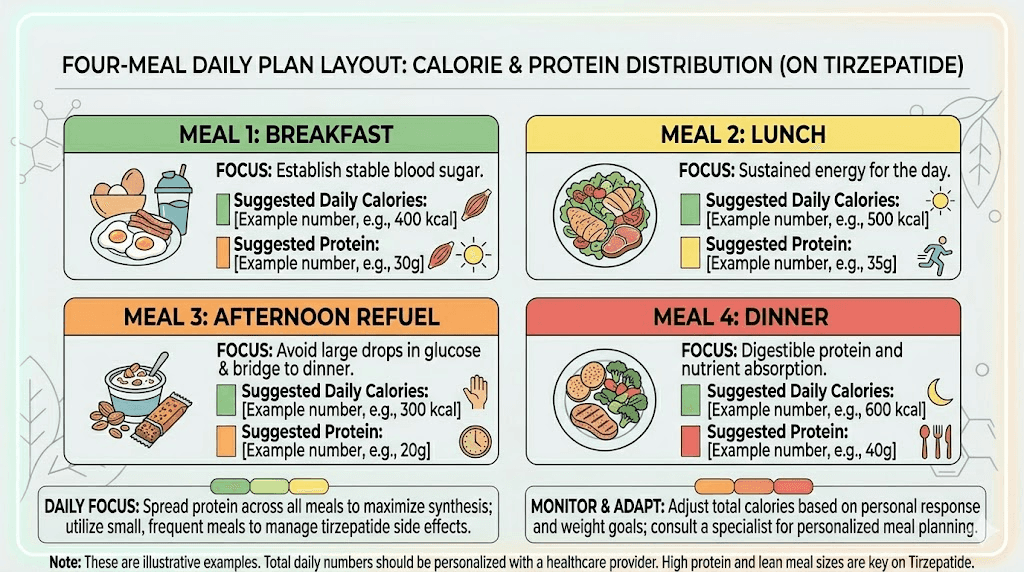
The 4-meal approach
Many tirzepatide users find that three standard meals are too large for their suppressed appetite. Switching to four smaller meals, each in the 300 to 400 calorie range, feels more manageable and keeps nutrition spread throughout the day.
Meal 1 (7-8 AM): 350 calories, 35g protein
Meal 2 (11 AM-12 PM): 350 calories, 30g protein
Meal 3 (3-4 PM): 350 calories, 30g protein
Meal 4 (6-7 PM): 350 calories, 30g protein
Total: 1,400 calories, 125g protein. Adjust portion sizes up or down to match your personal target. The key is even distribution, not front-loading or back-loading all your calories into one or two meals.
For detailed meal plans and sample menus, including specific recipes optimized for tirzepatide users, check our comprehensive meal planning guide. And for GLP-1 optimized recipes, our recipe collection offers options that prioritize protein density within calorie-appropriate portions.
Sample meal plans at different calorie levels
Theory without examples leaves people guessing. Here are concrete meal plans at three common calorie targets, each meeting the protein and macronutrient guidelines discussed above.
1,200 calorie plan (lower range for women)
Breakfast (300 calories, 30g protein): Two scrambled eggs with one egg white, half cup of sauteed spinach, one slice of whole grain toast. This combination provides complete amino acids plus iron and fiber from the spinach.
Lunch (300 calories, 32g protein): Four ounces of grilled chicken breast over two cups of mixed greens with cucumber, cherry tomatoes, and one tablespoon of olive oil vinaigrette. Simple, protein-dense, and easy to eat even on low-appetite days.
Afternoon snack (200 calories, 25g protein): One cup of plain Greek yogurt with a quarter cup of mixed berries. The yogurt delivers protein while berries add antioxidants and natural sweetness without excessive sugar.
Dinner (400 calories, 33g protein): Five ounces of baked salmon with one cup of roasted broccoli and half cup of quinoa. The omega-3 fatty acids from salmon support inflammation management, which can help with some of the body aches tirzepatide users sometimes report.
Daily totals: 1,200 calories, 120g protein, approximately 90g carbohydrates, 40g fat.
1,500 calorie plan (mid-range)
Breakfast (375 calories, 35g protein): Protein smoothie with one scoop whey protein, one cup unsweetened almond milk, one small banana, one tablespoon almond butter, and ice. This works particularly well on days when solid food feels unappealing.
Lunch (400 calories, 35g protein): Turkey and vegetable wrap with four ounces of sliced turkey breast, lettuce, tomato, avocado slices, and mustard in a whole wheat tortilla. A portable option that travels well for work lunches.
Afternoon snack (250 calories, 20g protein): Two hard-boiled eggs with one ounce of almonds. Quick, requires no preparation, and delivers both protein and healthy fats.
Dinner (475 calories, 38g protein): Six ounces of lean ground turkey stir-fry with mixed vegetables (bell peppers, snap peas, mushrooms) over three quarters cup of brown rice, with soy sauce and ginger.
Daily totals: 1,500 calories, 128g protein, approximately 130g carbohydrates, 50g fat.
1,800 calorie plan (higher range for active men)
Breakfast (450 calories, 40g protein): Three-egg omelet with vegetables and one ounce of cheese, one slice of whole grain toast with half an avocado. A substantial start that fuels morning activity.
Lunch (475 calories, 38g protein): Grilled chicken Caesar salad with five ounces of chicken, romaine, cherry tomatoes, two tablespoons of light Caesar dressing, and one ounce of parmesan. Include whole grain croutons for additional carbohydrates.
Afternoon snack (300 calories, 30g protein): Protein shake with one scoop protein powder, one tablespoon peanut butter, one small banana, and water. Ideal for post-workout nutrition if you exercise in the afternoon.
Dinner (575 calories, 42g protein): Seven ounces of grilled steak (sirloin), one large baked sweet potato, one cup of steamed asparagus with a drizzle of olive oil. The higher calorie count accommodates the energy needs of active men without sacrificing nutritional quality.
Daily totals: 1,800 calories, 150g protein, approximately 155g carbohydrates, 58g fat.
These are templates, not prescriptions. Swap proteins, vegetables, and carbohydrate sources based on your preferences. The structure matters more than the specific foods. Protein at every meal. Vegetables at every meal. Controlled portions of quality carbohydrates and fats. That framework works regardless of which specific ingredients you choose.
What to do when you cannot eat enough calories
This is one of the most underappreciated challenges of tirzepatide treatment. The conversation usually focuses on eating too much. But for many users, especially in the first few weeks and after dose increases, the problem is the opposite. You cannot eat enough.
The first dose hits and food loses its appeal. Completely. The sight, the smell, the thought of eating becomes neutral at best, unpleasant at worst. Some people go entire days on 600 to 800 calories without meaning to. This is not a feature. It is a problem that needs addressing.
Warning signs you are eating too little
Watch for these indicators that your calorie intake has dropped too low:
Persistent fatigue beyond normal adjustment periods. Some tiredness is expected in the first week or two, but ongoing exhaustion suggests inadequate fuel.
Hair thinning or increased shedding starting 2 to 3 months into treatment. This is a telltale sign of nutritional deficiency, particularly protein, iron, and biotin.
Feeling cold all the time. When calorie intake drops too low, your body reduces thyroid hormone output and peripheral blood flow to conserve energy. Chronic coldness is a red flag.
Muscle weakness or rapid strength loss. If you are losing strength in the gym or struggling with activities that were previously easy, your body is likely breaking down muscle tissue for energy.
Dizziness or lightheadedness, especially when standing up quickly. This often indicates dehydration combined with insufficient caloric intake and electrolyte imbalance.
Strategies to increase calorie intake when appetite is absent
Calorie-dense foods. When you can only eat small amounts, make each bite count. Nuts, nut butters, avocado, olive oil, cheese, and fatty fish pack significant calories into small volumes. A tablespoon of olive oil adds 120 calories to any meal without adding bulk.
Liquid calories. Smoothies, protein shakes, bone broth, and soups go down easier than solid food when appetite is suppressed. A well-made smoothie can deliver 400 calories and 30 grams of protein in a form that feels more like a drink than a meal.
Smaller, more frequent meals. Instead of forcing three full meals, eat five or six mini-meals of 200 to 300 calories each. Grazing throughout the day often feels more manageable than sitting down to a plate that looks overwhelming.
Timing around medication. Some users find that appetite is strongest in the morning and weakest in the evening, or vice versa. Others notice a pattern related to injection timing. Eat your largest meal during your window of highest appetite, whatever that happens to be for you. For more on timing, see our guide on the best time of day to inject tirzepatide.
Set alarms. When hunger signals disappear, you need external reminders to eat. Set phone alarms every 3 to 4 hours as prompts to consume something, even if it is just a protein shake or a handful of nuts.
Adjusting calories by tirzepatide dose
As your tirzepatide dose increases through the standard titration schedule, your appetite typically decreases further. This means your calorie approach needs to adapt at each dose level.
Dose-by-dose calorie considerations
2.5 mg (starting dose): Appetite suppression is usually mild at this introductory dose. Most people can eat close to their calculated target without much difficulty. Focus on establishing good habits, tracking intake, and building protein-rich meal patterns. You may not even need to force yourself to eat. Think of this as your calibration phase.
5 mg: Appetite suppression becomes more noticeable. Many people report their first significant shift in eating behavior at this dose. Calorie intake may naturally drop by 200 to 300 calories below pre-treatment levels. If you find yourself falling below your floor (1,200 for women, 1,500 for men), implement the liquid calorie and calorie-dense food strategies immediately. This is when adjustment patterns typically emerge.
7.5 mg: Appetite suppression intensifies significantly for most users. This is the dose where eating too little becomes a real concern. Prioritize protein above all else. If you can only manage 1,000 calories, make sure 400 of those come from protein. Track daily to ensure you are meeting minimums.
10 mg: Strong appetite suppression. Many users report struggling to eat even three meals. The four to five mini-meal approach works best at this dose level. Front-load calories earlier in the day when appetite tends to be slightly higher.
12.5 and 15 mg: Maximum appetite suppression. These higher doses require the most dietary vigilance. Some users at these doses benefit from calorie-dense protein bars, meal replacement shakes, or fortified foods to ensure minimum intake. If you consistently cannot eat above 800 calories, discuss this with your healthcare provider, as a dose adjustment may be necessary.
The irony of tirzepatide is that the medication becomes so effective at suppressing appetite that it can actually create nutritional problems. This is not a reason to avoid higher doses if they are medically appropriate. It is a reason to be proactive about nutrition planning at every dose level.
Exercise and calorie adjustments
Exercise changes the calorie equation. And on tirzepatide, it changes it in ways that require specific attention.
Why exercise matters more on tirzepatide
Without exercise, the 25 to 30 percent of weight loss that comes from lean mass could be even higher. Resistance training is the most powerful tool for shifting this ratio toward fat loss. Studies consistently show that people who combine tirzepatide with structured resistance training preserve significantly more muscle than those who rely on the medication alone.
Additionally, exercise improves energy levels, mood, sleep quality, and insulin sensitivity, all of which support better outcomes on tirzepatide. The medication handles appetite. Exercise handles body composition. Together, they produce results that neither achieves alone.
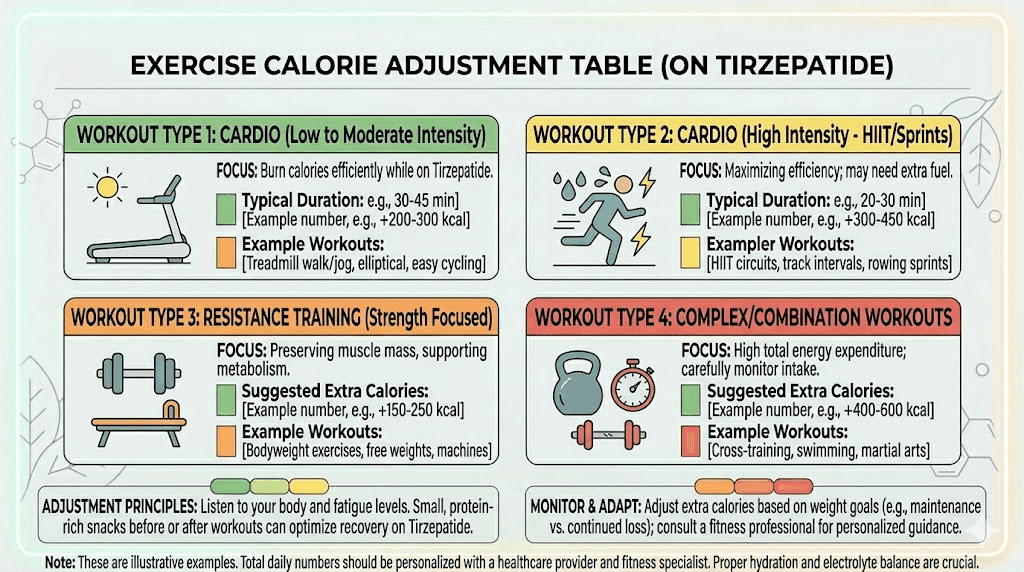
Calorie adjustments for exercise
If you are doing regular resistance training (3 or more sessions per week), add 100 to 200 calories to your baseline target on training days. These additional calories should come primarily from protein and carbohydrates, not fat. Pre-workout carbohydrates fuel performance. Post-workout protein supports recovery and muscle synthesis.
For cardio-focused exercise (walking, jogging, cycling), the calorie adjustment depends on intensity and duration. Moderate cardio for 30 to 45 minutes burns approximately 200 to 300 calories. You do not need to eat all of those back, but consider adding 50 to 100 calories on heavy cardio days to prevent excessive deficit.
Here is a practical framework:
Exercise type | Calorie adjustment | Macro focus |
|---|---|---|
Resistance training | +150-200 cal on training days | Extra protein + carbs |
Moderate cardio (30-45 min) | +50-100 cal | Extra carbs |
Light walking (30 min) | No adjustment needed | Standard macros |
High-intensity training | +200-300 cal | Extra protein + carbs + hydration |
The biggest mistake exercisers make on tirzepatide is not eating enough to support their activity. A 45-minute weight training session on 1,000 calories is a recipe for muscle pain, poor recovery, and eventual burnout. If you are going to invest time in exercise, invest the calories to support it.
For those exploring additional support for body composition goals, SeekPeptides members access detailed fat loss protocols, muscle preservation strategies, and evidence-based stacking guides that complement tirzepatide therapy.
Hydration and its impact on calorie management
Water is not a macronutrient, but it plays a crucial role in calorie management on tirzepatide. Many users report increased thirst on the medication, and inadequate hydration can mimic hunger, worsen side effects, and confuse your body signals about what it actually needs.
Aim for a minimum of 64 ounces (about 2 liters) of water daily, with increases for exercise and warm weather. Some practitioners recommend half your body weight in ounces as a baseline. So a 180-pound person would target 90 ounces daily.
Dehydration on tirzepatide can cause headaches, constipation, dizziness, and fatigue, all of which get blamed on the medication when they are actually hydration issues. Drinking a full glass of water before each meal also helps with portion management and nutrient absorption.
Avoid counting sweetened beverages, juice, or alcohol toward your water intake. These contribute calories without addressing hydration effectively. If plain water feels boring, add lemon slices, cucumber, or mint for flavor without calories.
Special considerations for different populations
Women over 40
Hormonal changes during perimenopause and menopause affect metabolism, body composition, and how the body responds to calorie restriction. Women in this group should prioritize protein even more aggressively (targeting the higher end of 1.4 to 1.6 grams per kilogram) and include calcium-rich foods to support bone health. If tirzepatide is affecting menstrual patterns, calorie intake may need to be higher during certain phases of the cycle.
Men focused on body composition
Men typically have more muscle mass and higher calorie needs. Male tirzepatide users should rarely go below 1,500 calories and should target the higher end of protein recommendations, especially if combining tirzepatide with testosterone support or regular strength training.
Older adults (60+)
Sarcopenia risk increases with age. Older adults on tirzepatide face the highest risk of clinically significant muscle loss during weight reduction. Calorie floors should be maintained strictly, protein targets should be at the upper end of recommendations (1.4 to 1.6 grams per kilogram), and resistance training becomes essentially mandatory rather than optional.
People with diabetes
Tirzepatide was originally developed for type 2 diabetes management. If you are using it for both blood sugar control and weight loss, calorie and carbohydrate management interact with your medication in complex ways. Work closely with your healthcare provider and consider monitoring blood glucose responses to different calorie levels. Hypoglycemia risk increases when combining tirzepatide with very low calorie diets, especially if you are also on insulin or sulfonylureas.
Supplements that support calorie management on tirzepatide
When calorie intake drops, certain nutrients become harder to obtain from food alone. These supplements help fill the gaps.
Multivitamin: A comprehensive multivitamin provides insurance against micronutrient deficiencies. Look for one with at least 100 percent daily value of iron, zinc, B vitamins, and vitamin D.
Fiber supplement: Meeting the 25 to 35 gram daily fiber target is difficult at lower calorie intakes. A psyllium husk or fiber supplement can help maintain digestive regularity and support gut health.
Electrolytes: Sodium, potassium, and magnesium levels can drop when food intake decreases. Electrolyte imbalances cause muscle cramps, dry mouth, fatigue, and heart palpitations. An electrolyte supplement or bone broth can help maintain balance.
Protein powder: When appetite makes it impossible to eat enough protein-rich food, whey protein, casein, or plant-based protein powders offer a concentrated, easy-to-consume alternative. This is a supplement in the truest sense, supplementing what your diet cannot provide.
Omega-3 fatty acids: If fatty fish consumption drops due to reduced appetite, a fish oil supplement ensures adequate omega-3 intake for inflammation management and cardiovascular health.
Tracking tools and methods
Successful calorie management requires some form of tracking, at least initially. Here are the most practical approaches.
App-based tracking: MyFitnessPal, Cronometer, and Lose It are the most popular options. Set your calorie target, log your meals, and review macronutrient breakdowns daily. Cronometer is particularly useful because it tracks micronutrients as well, helping you identify deficiency risks.
Hand-portion method: For those who find app tracking tedious, the hand-portion method offers a reasonable alternative. One palm-sized portion of protein (approximately 4 ounces). One fist-sized portion of vegetables. One cupped-hand portion of carbohydrates. One thumb-sized portion of fat. Four to five of these combinations per day approximates a 1,400 to 1,600 calorie intake with adequate protein.
Weekly weigh-ins plus photo tracking: The scale shows total weight change but does not distinguish between fat loss and muscle loss. Combining weekly weigh-ins with progress photos and, ideally, body composition measurements gives you a more complete picture of whether your calorie strategy is working.
For tirzepatide-specific tracking tools and progress monitoring, SeekPeptides provides members with personalized protocol builders and monitoring resources designed specifically for GLP-1 and GIP agonist users.
When to talk to your healthcare provider about calories
Self-management works for most situations. But certain scenarios warrant professional guidance.
Contact your healthcare provider if you consistently cannot eat above 800 calories per day for more than three consecutive days. This level of restriction, even if unintentional, risks serious nutritional deficits and may indicate that your current tirzepatide dose needs adjustment.
Seek guidance if you are losing more than 3 pounds per week after the first month. Rapid weight loss beyond this rate typically involves excessive lean mass loss and can stress the gallbladder, liver, and kidneys. Gallbladder issues are a known concern with rapid weight loss on GLP-1 agonists.
Get professional input if you have a history of eating disorders. Tirzepatide extreme appetite suppression can trigger or worsen disordered eating patterns. A healthcare provider or registered dietitian experienced with GLP-1 medications can help establish safe boundaries.
Discuss your calorie plan if you are on other medications that affect blood sugar, especially insulin or sulfonylureas. The combination of tirzepatide plus calorie restriction plus other glucose-lowering medications can create dangerous hypoglycemia.
And schedule a nutrition review if your weight loss has completely stalled for more than four weeks despite consistent adherence to your calorie target. A stall this long usually indicates that your body has adapted and your plan needs recalibration, something best done with professional guidance rather than guesswork.
Long-term calorie strategy and maintenance
Weight loss is not the finish line. Maintenance is. And the calorie strategy that gets you to your goal weight is different from the one that keeps you there.
Transitioning from deficit to maintenance
When you reach your target weight, do not abruptly jump to maintenance calories. Your metabolism, your hormones, and your gut have adapted to lower intake over months. A sudden increase triggers rapid regain and digestive distress.
Instead, increase calories by 100 to 150 per week until you find the level where your weight stabilizes. This process, called reverse dieting, takes 4 to 8 weeks and allows your metabolism to gradually upregulate. Track your weight weekly during this transition. If weight starts climbing, you have gone too high. Pull back by 50 to 100 calories and wait two weeks before adjusting again.
Maintenance calorie estimates
Most people maintain their new weight at approximately 12 to 14 calories per pound of body weight if moderately active. A person who has reached 160 pounds would maintain at roughly 1,920 to 2,240 calories daily. If on a maintenance dose of tirzepatide, the appetite suppression continues to some degree, making adherence easier than with diet alone.
For a comprehensive guide on maintaining weight loss after tirzepatide, including what happens if you decide to discontinue the medication, our detailed maintenance guide covers everything from calorie recalculation to metabolic support strategies.
The role of continued protein emphasis
Even in maintenance, protein remains king. The muscle you preserved during weight loss needs ongoing support. Drop protein too aggressively after reaching your goal, and you risk gradual muscle loss that slowly lowers your metabolic rate and creates a path back to weight gain.
Maintain protein intake at a minimum of 1.0 grams per kilogram of body weight during maintenance, even if you reduce total calories from the active weight loss phase. This is the floor, not the ceiling. If you continue resistance training (and you should), keep protein at 1.2 to 1.4 grams per kilogram.
Comparing calorie needs: tirzepatide vs semaglutide
Many people wonder whether calorie targets differ between tirzepatide and semaglutide. The general calorie frameworks are similar, but there are meaningful differences worth understanding.
Tirzepatide typically produces stronger appetite suppression than semaglutide at equivalent therapeutic doses. The 2025 Nature Medicine trial showed that while both medications reduced appetite scores similarly, tirzepatide produced greater overall weight loss. The researchers suggested that tirzepatide may work through additional mechanisms beyond appetite suppression alone, including enhanced fat oxidation and possible effects on energy expenditure.
In practical terms, this means tirzepatide users may need to be more vigilant about eating enough, while semaglutide users may find it slightly easier to hit their calorie targets. The calorie floors (1,200 for women, 1,500 for men) remain the same for both medications. The macronutrient recommendations are identical. The protein targets are identical.
If you are switching between medications, recalculate your calorie needs based on your current weight rather than carrying over targets from your previous protocol. The transition between GLP-1 agonists often involves temporary changes in appetite patterns that require a fresh assessment. Our conversion guide covers the dosing transition, but calories should be recalculated independently.
Frequently asked questions
Is 1,000 calories a day enough on tirzepatide?
No. While tirzepatide may suppress your appetite to the point where 1,000 calories feels like plenty, this level is too low for most people to meet nutritional needs. Sustained intake below 1,200 calories for women or 1,500 for men risks muscle loss, nutrient deficiencies, and metabolic slowdown. If you are consistently unable to eat more, speak with your healthcare provider about adjusting your tirzepatide dose.
Should I eat less on higher tirzepatide doses?
Not intentionally. Higher doses suppress appetite more aggressively, so your intake may naturally decrease. But your calorie floor should remain the same regardless of dose. The goal is to eat enough to meet your nutritional needs, not to eat as little as the medication allows. Monitor your intake closely during dose escalations and use calorie-dense foods and protein supplements if needed.
Can I do intermittent fasting while on tirzepatide?
Technically yes, but it requires careful management. Tirzepatide already limits your eating window naturally through appetite suppression. Adding a formal fasting protocol on top of this can make it very difficult to consume adequate calories and protein. If you practice intermittent fasting, ensure you are still hitting your calorie and protein targets within your eating window. Many users find that tirzepatide essentially creates its own form of reduced meal frequency without the need for a formal fasting structure.
How many calories should I eat on my tirzepatide injection day?
The same as any other day. There is no evidence that calorie needs change specifically on injection day. However, many users experience slightly stronger gastrointestinal side effects for 24 to 48 hours after injection. If this affects your appetite, focus on easily digestible, protein-rich foods during this window. Do not skip eating entirely.
Will eating too few calories on tirzepatide cause weight gain?
Not directly, but indirectly, yes. Extreme calorie restriction causes metabolic adaptation, muscle loss, and hormonal changes that make weight regain almost inevitable once you return to normal eating. The body becomes hyperefficient at storing calories after prolonged restriction. A moderate, sustainable deficit produces better long-term results than aggressive restriction followed by rebound. For more on this topic, see our guide on why tirzepatide might not be working.
Do I need to count calories forever on tirzepatide?
No. Most people benefit from tracking for the first 8 to 12 weeks while they learn portion sizes and develop new eating habits. After that, the plate method or hand-portion method provides enough structure for most users to maintain appropriate intake without daily logging. Some people find that checking in with detailed tracking for one week every month helps them stay on course without the burden of daily counting.
What if I gained weight on tirzepatide despite eating within my calorie target?
First, verify your tracking accuracy by measuring everything for one week. Common culprits include cooking oils, condiments, beverages, and restaurant meals. If tracking is accurate, consider water retention, hormonal fluctuations, or supplementation effects. Weight fluctuations of 2 to 4 pounds from water are normal and do not indicate fat gain. If genuine weight gain persists for more than three weeks, consult your healthcare provider.
External resources
Tirzepatide and Metabolic Adaptation in People with Obesity - Cell Metabolism
Tirzepatide on Ingestive Behavior in Adults with Overweight or Obesity - Nature Medicine
Effects of Tirzepatide on Skeletal Muscle Mass - PMC Systematic Review
Tirzepatide Once Weekly for the Treatment of Obesity - New England Journal of Medicine
For researchers serious about optimizing their tirzepatide protocols and nutrition strategies, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized protocol builders, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your calories stay calculated, your protein stay prioritized, and your results stay sustainable.