Mar 25, 2026

Experienced lifters know something most GLP-1 guides never mention. The medications do not destroy muscle. Bad protocols do. Thousands of researchers have gained strength, added lean mass, and completely transformed their body composition while using semaglutide, tirzepatide, and other GLP-1 receptor agonists. The difference between those who lose muscle and those who build it comes down to a handful of decisions made in the first few weeks of treatment.
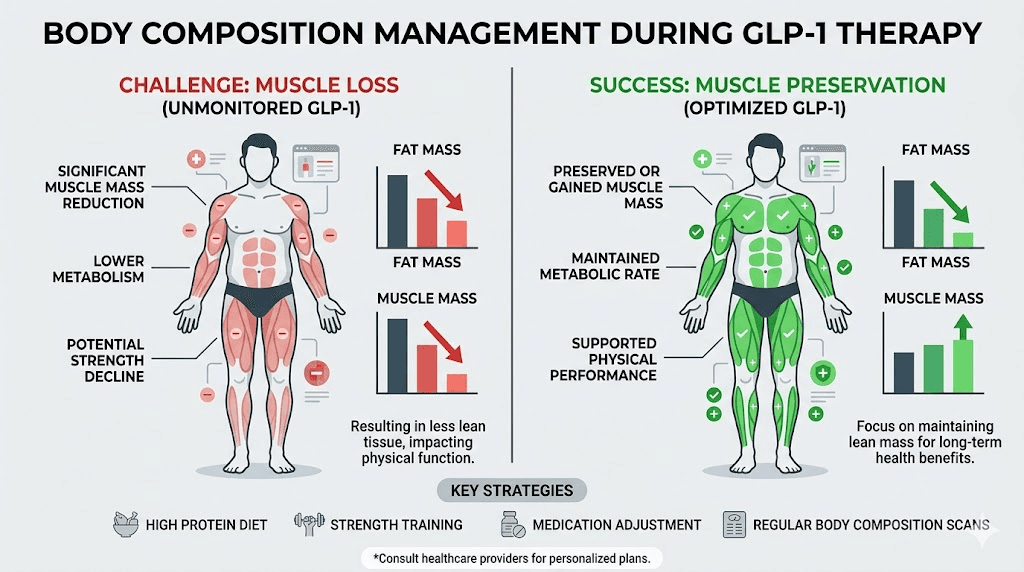
The fear is understandable. Headlines scream about muscle wasting. Forums overflow with worst-case scenarios. And clinical trial data does show that 25 to 40 percent of total weight lost on GLP-1 medications comes from lean body mass. That number sounds alarming in isolation. But context changes everything, because lean mass loss during any calorie deficit is normal, expected, and largely preventable with the right training and nutrition approach.
This guide covers the complete framework for building and preserving muscle on GLP-1 therapy. You will learn the exact resistance training protocols backed by research, the protein targets that prevent catabolism, the supplement strategies that accelerate recovery, and the monitoring methods that keep you on track. Whether you are a seasoned lifter starting GLP-1 treatment or someone picking up weights for the first time, the principles here apply. SeekPeptides has compiled the most current research, clinical trial data, and practical experience from thousands of researchers navigating this exact challenge.
What GLP-1 medications actually do to your muscles
GLP-1 receptor agonists work primarily by mimicking the incretin hormone glucagon-like peptide-1. This hormone slows gastric emptying, reduces appetite through central nervous system signaling, and improves insulin sensitivity. The result is a significant calorie deficit that drives weight loss. But here is the critical detail most people miss. The medications themselves do not target muscle tissue.
Muscle loss on GLP-1 drugs happens for the same reason it happens on any diet. Calorie restriction without adequate protein and resistance training signals the body to break down lean tissue for energy. A 2026 study published in Cell Reports Medicine confirmed this directly, showing that semaglutide-induced weight loss does not result in a disproportionate loss of muscle mass compared to other calorie-restricted weight loss methods. The ratio of fat to lean mass lost mirrors what happens with diet alone.
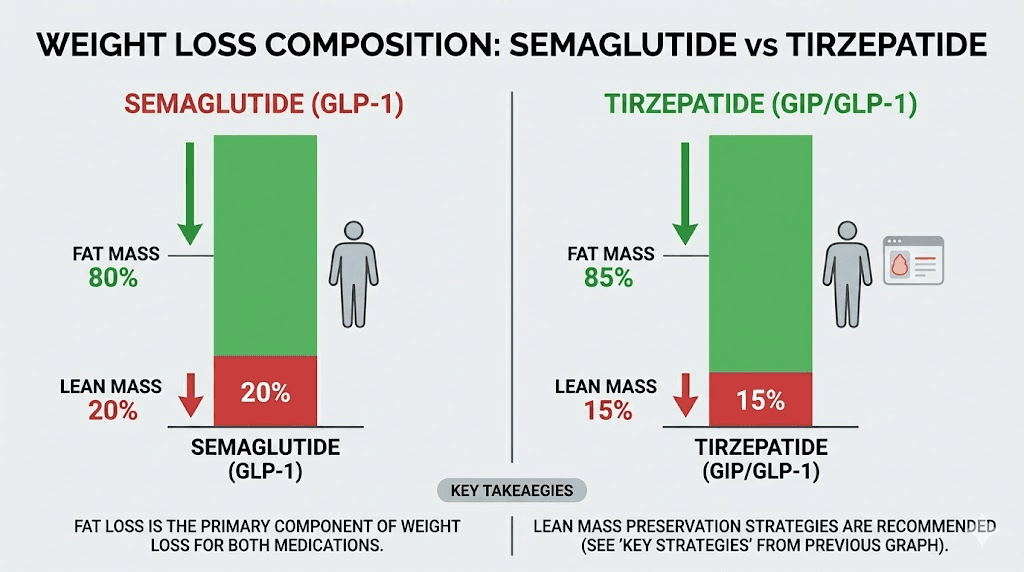
The numbers tell the story clearly. In semaglutide clinical trials, fat mass accounted for approximately 70 percent of total weight lost, while lean body mass accounted for roughly 30 percent. Tirzepatide studies showed similar patterns, with fat mass dropping between 33 and 36 percent and lean mass decreasing by 10 to 11 percent, depending on the age group studied. These ratios are actually favorable compared to many traditional dieting approaches, where lean mass losses can exceed 40 percent of total weight without proper intervention.
Something even more interesting is emerging from recent imaging studies. Tirzepatide may actually improve muscle quality even as overall lean mass decreases slightly. Researchers have observed reduced intramuscular fat infiltration, meaning the muscle that remains becomes more functional and metabolically active. Think of it as cleaning up the muscle rather than shrinking it. This improvement in muscle quality partly explains why many GLP-1 users report feeling stronger and more capable despite weighing less on the scale.
Hand grip strength, one of the most reliable markers of functional muscle capacity, actually increased by approximately 4 kilograms over 12 months in one semaglutide study. That is not muscle loss. That is muscle improvement happening alongside fat loss. The key distinction is between muscle mass and muscle function. You can lose some mass while gaining function, and that trade-off is overwhelmingly positive for health outcomes.
The science behind muscle preservation on GLP-1 therapy
Understanding the research gives you a massive advantage. When you know exactly what happens at the cellular level, you can make smarter decisions about your training, nutrition, and supplementation. The science here is encouraging.
The largest and most comprehensive meta-analysis on GLP-1 weight loss and body composition found that the proportion of lean mass relative to total body weight is often preserved or improved during treatment. This happens because fat loss exceeds lean mass loss by a wide margin in most patients. If you start at 35 percent body fat and lose weight on a GLP-1, your body fat percentage drops significantly while your lean mass percentage actually increases, even if the absolute number on a DEXA scan shows a small decrease in lean tissue.
What the clinical trials actually show
The STEP trials for semaglutide provided some of the most detailed body composition data available. Participants lost an average of 15 to 17 percent of body weight over 68 weeks. Of that loss, approximately 39 percent came from lean body mass in the group that did not exercise. But here is the part that rarely makes headlines. Participants who engaged in regular physical activity, particularly resistance training, preserved significantly more lean mass while losing the same or more total weight.
The SURMOUNT trials for tirzepatide painted an even more favorable picture. At the highest dose of 15 milligrams weekly, participants lost approximately 22 percent of body weight, with lean mass accounting for a smaller proportion of total loss compared to semaglutide. Researchers attributed this partly to tirzepatide dual mechanism of action on both GLP-1 and GIP receptors, with the GIP receptor activation potentially offering some protective effect on lean tissue.
Retatrutide, the triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown the most dramatic weight loss results in early trials. Body composition data from phase 2 studies indicated weight loss of up to 24 percent at 48 weeks. While detailed lean mass preservation data is still limited for retatrutide, the glucagon receptor component may provide metabolic advantages that favor fat oxidation over muscle catabolism. Early bodybuilding community reports suggest favorable body recomposition outcomes, particularly when combined with aggressive resistance training protocols.
The role of insulin sensitivity in muscle building
One mechanism that works in your favor is the improvement in metabolic function that GLP-1 medications provide. Better insulin sensitivity means your muscles respond more effectively to both nutrients and training stimuli. Glucose uptake into muscle cells improves. Protein synthesis signaling becomes more efficient. And the inflammatory environment that characterizes obesity, which actively impairs muscle growth, begins to resolve.
This metabolic improvement is why some researchers actually gain strength on GLP-1 medications despite being in a calorie deficit. Their muscles are finally operating in a hormonal environment that supports growth and repair. The chronic low-grade inflammation associated with excess body fat suppresses muscle protein synthesis. Remove the inflammation by reducing fat mass, and the muscle building machinery starts working properly again. For overweight or obese individuals starting GLP-1 therapy, this creates a window of opportunity for simultaneous fat loss and muscle gain that experienced bodybuilders call recomposition.
Resistance training protocols that actually work on GLP-1s
This is where theory meets practice. Resistance training is not optional if you want to build or preserve muscle on GLP-1 medications. It is the single most powerful tool you have. Multiple systematic reviews confirm that resistance exercise effectively counteracts lean mass loss during weight loss, regardless of the method used to create the calorie deficit.
The signal matters more than the surplus. Your muscles grow in response to mechanical tension, not just excess calories. Progressive overload, the gradual increase in weight, reps, or volume over time, tells your body that it needs to keep its muscle tissue. Without that signal, a calorie deficit gives the body permission to cannibalize lean mass. With it, the body prioritizes fat for fuel and preserves the muscle it needs for the demands you are placing on it.
Training frequency and split
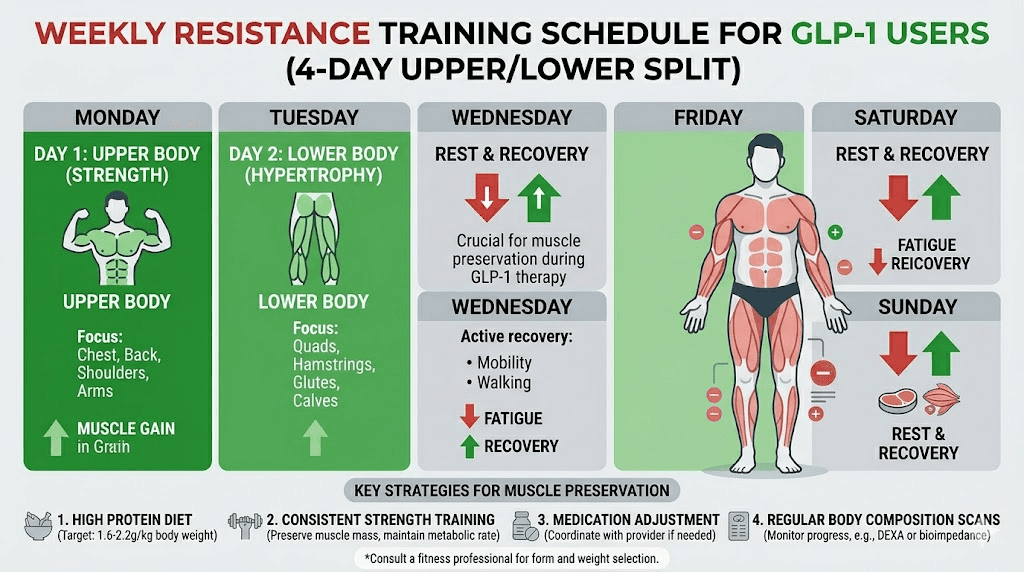
Research on GLP-1 users who preserved the most lean mass consistently shows a training frequency of 3 to 5 resistance sessions per week. A 4-day upper/lower split works exceptionally well for most people on GLP-1 therapy, balancing adequate training stimulus with recovery demands that may be elevated during calorie restriction.
Sample 4-day split:
Day 1 (Upper push/pull): Bench press, overhead press, barbell rows, lat pulldowns, face pulls
Day 2 (Lower): Squats, Romanian deadlifts, leg press, leg curls, calf raises
Day 3: Rest or light walking
Day 4 (Upper push/pull): Incline dumbbell press, cable rows, dumbbell shoulder press, chin-ups, lateral raises
Day 5 (Lower): Deadlifts, Bulgarian split squats, hip thrusts, leg extensions, calf raises
Days 6-7: Rest, light cardio, or active recovery
The emphasis on compound movements is intentional. Squats, deadlifts, bench presses, overhead presses, and rows recruit the most muscle fibers and create the strongest anabolic stimulus. These exercises produce the greatest hormonal response and give you the most return on every calorie you consume. Isolation work has its place, but compound lifts should form the foundation of every session.
Volume and intensity targets
Aim for 10 to 16 hard sets per muscle group per week. This range is well-supported by hypertrophy research and is achievable even when energy levels fluctuate on GLP-1 medications. Distribute these sets across two sessions per muscle group for optimal growth stimulus and recovery.
Intensity matters enormously. Work in the 6 to 12 rep range for most sets, using weights that bring you within 1 to 3 reps of failure. This range optimizes mechanical tension and metabolic stress, the two primary drivers of muscle hypertrophy. Going to absolute failure on every set is not necessary and can actually impair recovery during a calorie deficit. Save true failure sets for the last set of each exercise.
Progressive overload is non-negotiable. Track every workout. Add weight when you hit the top of your rep range with good form. If you prescribed yourself 8 to 12 reps on bench press and you hit 12 reps for all sets, increase the weight by 2.5 to 5 pounds next session. This systematic progression is what separates people who build muscle on GLP-1s from those who just go through the motions.
Managing energy levels during training
One practical challenge is that GLP-1 medications can affect energy levels, particularly in the first few weeks. Some users report fatigue, especially on injection days. Smart scheduling helps. Many experienced researchers train on days when they feel strongest, often 3 to 5 days after their weekly injection when side effects have settled but medication effects are still active.
Pre-workout nutrition becomes critical. Even if you are not hungry, consuming a small meal with protein and carbohydrates 60 to 90 minutes before training provides the fuel your muscles need. A protein shake with a banana or some rice cakes works well when appetite is suppressed. The goal is not a large meal. It is strategic fuel delivery.
If fatigue is severe, consider reducing total training volume temporarily rather than skipping sessions entirely. Three sets instead of four. Three sessions instead of four. Maintaining the habit and the progressive overload stimulus matters more than hitting maximum volume every single week.
Protein requirements for muscle building on GLP-1 medications
Protein is the most important macronutrient for muscle preservation and growth. Period. On GLP-1 medications, it becomes even more critical because reduced appetite often leads to reduced protein intake exactly when your body needs it most. Getting this right is the difference between losing 20 percent lean mass and losing 5 percent or less.
How much protein you actually need
The Endocrine Society presented research in 2025 showing that higher protein intake significantly protects against muscle loss during semaglutide treatment. The specific targets depend on your situation, but the evidence points clearly in one direction. More protein is better.
For muscle preservation during GLP-1 weight loss, aim for 1.2 to 1.6 grams of protein per kilogram of body weight daily. That means a 90-kilogram (200-pound) person needs 108 to 144 grams of protein every day, without exception. For those actively trying to build muscle, not just preserve it, push that target higher to 1.6 to 2.0 grams per kilogram. That same 200-pound person now needs 144 to 180 grams daily.
These numbers can feel daunting when your appetite is suppressed. A common mistake is thinking you need to eat more food. You do not. You need to eat more protein-dense food. Prioritize protein at every meal and use protein shakes to bridge any gaps. Liquid calories are easier to consume when appetite is low, and a well-formulated protein shake delivers 25 to 50 grams of high-quality protein in a few sips.
Protein timing and distribution
Distributing protein across 3 to 5 meals throughout the day is more effective for muscle protein synthesis than consuming it in one or two large meals. Aim for at least 25 to 40 grams of protein per meal to maximize the muscle protein synthesis response. Research consistently shows that a threshold of approximately 2.5 grams of leucine per meal is needed to fully activate the mTOR pathway, the molecular switch that triggers muscle building.
Post-workout protein is especially important. Consuming 30 to 50 grams of high-quality protein within one to two hours after resistance training takes advantage of the elevated muscle protein synthesis window. This does not need to be complicated. A protein shake, chicken breast, or Greek yogurt with nuts all work. The specific food matters less than the total protein content and timing.
For those dealing with significant appetite suppression or bloating, breaking protein into smaller, more frequent servings of 20 to 30 grams every 3 to 4 hours can be more manageable. This still hits the leucine threshold and keeps amino acid availability elevated throughout the day.
Best protein sources when appetite is suppressed
Not all protein sources are equal when you are eating less. Prioritize options that pack the most protein into the smallest volume:
Whey protein isolate: 25 to 30 grams per scoop, highly bioavailable, easy to consume
Greek yogurt: 15 to 20 grams per serving, well-tolerated on GLP-1 medications
Egg whites: 26 grams per cup, virtually no fat, easy to digest
Chicken breast: 31 grams per 100 grams, the gold standard
Cottage cheese: 14 grams per half cup, slow-digesting casein protein
Tuna: 30 grams per can, convenient and calorie-efficient
Bone broth protein: 20 grams per serving, gentle on the stomach
Many GLP-1 users find that soft, moist foods are easier to eat than dry or dense options. Smoothies made with protein powder, frozen berries, spinach, and Greek yogurt deliver 40 to 50 grams of protein and go down easily even when appetite is minimal. These are not cheat meals. They are strategic nutrition tools.
The complete nutrition framework for body recomposition on GLP-1
Building muscle on GLP-1 medications requires a more nuanced approach to nutrition than simply eating less. The calorie deficit created by the medication handles the fat loss side. Your job is to make sure every calorie you do eat works toward muscle preservation and growth.
Calorie targets for muscle building
Calorie intake on semaglutide and tirzepatide naturally drops as appetite decreases. The key is ensuring it does not drop too low. Extreme calorie restriction, below 1200 calories daily for women or 1500 for men, dramatically increases muscle loss risk. Even on GLP-1 therapy, aim to keep total calories above these minimums.
For active individuals doing resistance training, a moderate deficit of 500 to 750 calories below maintenance is ideal. This allows approximately 1 to 1.5 pounds of weight loss per week, slow enough to preserve muscle while fast enough to see meaningful progress. Losing more than 1 percent of body weight per week significantly increases lean mass loss risk. If the scale is dropping faster than that, you need to eat more, not less.
Body recomposition, simultaneously losing fat and gaining muscle, is most achievable for beginners to resistance training, people returning after a long layoff, and those with higher body fat percentages. If you fall into any of these categories and you are on a GLP-1 medication, you are in the sweet spot for dramatic body composition changes.
Macronutrient ratios that support muscle growth
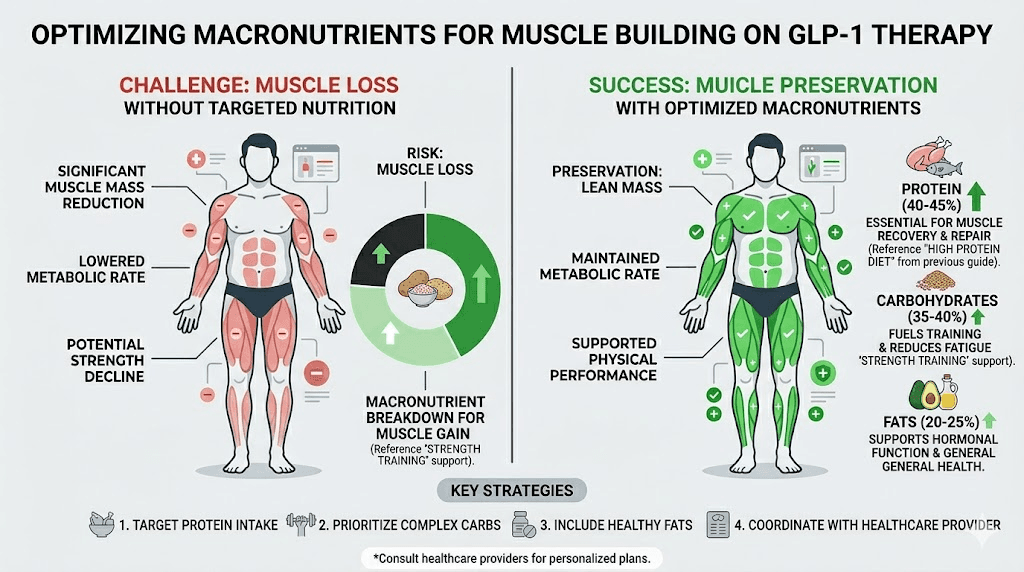
Protein first. Always. After hitting your protein target of 1.6 to 2.0 grams per kilogram, distribute remaining calories between carbohydrates and fats based on preference and tolerance. A good starting point for most GLP-1 users engaged in resistance training is:
Protein: 30 to 40 percent of total calories
Carbohydrates: 30 to 40 percent of total calories
Fat: 20 to 30 percent of total calories
Carbohydrates are not the enemy. They fuel resistance training, support recovery, and improve training performance. The best approach is to time carbohydrate intake around workouts. Consume the majority of your daily carbohydrates in the meals before and after training to maximize energy availability and glycogen replenishment.
Some researchers following a ketogenic diet with semaglutide report good fat loss results, but keto is generally not optimal for muscle building. The reduced glycogen stores limit training intensity, and the restriction makes it harder to hit protein targets when total food volume is already low. If muscle preservation is a priority, include at least moderate carbohydrate intake.
Meal timing around workouts
Strategic meal timing becomes a powerful tool when appetite is suppressed. Structure your largest meals around training sessions when nutrient demand is highest and digestion tends to be more comfortable.
Pre-workout (60 to 90 minutes before):
25 to 35 grams protein
30 to 50 grams carbohydrates
Low fat (under 10 grams) for faster digestion
Example: protein shake with oats and banana
Post-workout (within 1 to 2 hours):
30 to 50 grams protein
40 to 80 grams carbohydrates
Moderate fat acceptable
Example: chicken breast, rice, and vegetables
If nausea or digestive issues prevent eating solid food before training, liquid options work just as well. A protein shake with a banana and a tablespoon of honey provides everything you need. The goal is fuel availability, not a feast.
Supplements that support muscle growth during GLP-1 therapy
Supplements do not replace training and nutrition. But when the foundation is solid, the right supplements can provide a meaningful edge. Several have strong evidence specifically in the context of GLP-1 use and muscle preservation.
Creatine monohydrate
Creatine and GLP-1 therapy is one of the most well-supported combinations for muscle preservation. Creatine is the single most researched supplement in sports nutrition history, with decades of evidence showing it increases strength, supports lean mass, and improves workout performance. On GLP-1 medications, these benefits become even more valuable.
Creatine works by increasing phosphocreatine stores in muscle cells, allowing you to perform more reps and lift heavier weights. That additional training stimulus translates directly to better muscle preservation during a calorie deficit. Take 3 to 5 grams of creatine monohydrate daily. No loading phase needed. No cycling required. Just consistent daily intake.
Combining creatine with tirzepatide is safe and well-tolerated. The supplement does not interact with GLP-1 receptor agonists and does not exacerbate common side effects like nausea or constipation. It may cause a slight increase in scale weight due to intramuscular water retention, which is not fat gain and is actually a positive sign that your muscles are fully hydrated and primed for performance.
Essential amino acids and BCAAs
If you struggle to hit protein targets through whole food, essential amino acid (EAA) supplements provide a concentrated dose of the building blocks your muscles need. EAAs are particularly useful during fasting windows or when appetite is severely suppressed in the first weeks of GLP-1 treatment.
BCAAs alone are less effective than full EAA supplements because muscle protein synthesis requires all essential amino acids, not just leucine, isoleucine, and valine. If you choose between the two, EAAs deliver more value. Take 10 to 15 grams of EAAs between meals or during training to maintain positive nitrogen balance throughout the day.
Vitamin D
Vitamin D deficiency is shockingly common and directly impairs muscle function and growth. Research shows that inadequate vitamin D levels reduce muscle protein synthesis, increase inflammation, and impair recovery. Many overweight and obese individuals starting GLP-1 therapy are already deficient because vitamin D gets sequestered in adipose tissue.
Get your levels tested. Target a serum 25(OH)D level of 40 to 60 ng/mL. Most people need 2000 to 5000 IU of vitamin D3 daily to reach and maintain this range. Take it with a meal containing fat for optimal absorption.
Electrolytes
Electrolyte balance on GLP-1 therapy is often overlooked but critically important for muscle function. Reduced food intake means reduced mineral intake. Sodium, potassium, and magnesium all play essential roles in muscle contraction, nerve signaling, and recovery. Deficiencies in any of these can cause muscle cramps, weakness, and impaired performance.
Magnesium glycinate at 200 to 400 milligrams daily supports both muscle function and sleep quality. An electrolyte supplement or simply adding more salt to food can prevent the dizziness and lightheadedness that many GLP-1 users experience during training.
B vitamins
Many GLP-1 formulations now include B12 or methylcobalamin for good reason. B vitamins support energy metabolism, nervous system function, and red blood cell production. All of these contribute to training performance and recovery. If your GLP-1 medication does not include B12, supplement with 1000 to 2500 micrograms of methylcobalamin daily.
Vitamin B6 also plays a role in protein metabolism and the synthesis of neurotransmitters that affect mood and energy levels. A B-complex supplement covers all bases and is inexpensive insurance against deficiency during periods of reduced food intake.
What not to waste money on
Fat burners, thermogenics, and most "muscle-sparing" supplements marketed to GLP-1 users have little to no evidence behind them. Your GLP-1 medication is already creating the calorie deficit you need. Adding stimulant-based fat burners on top of reduced calorie intake risks increased heart rate, anxiety, and sleep disruption, all of which impair muscle recovery. Stick with the fundamentals above and save your money.
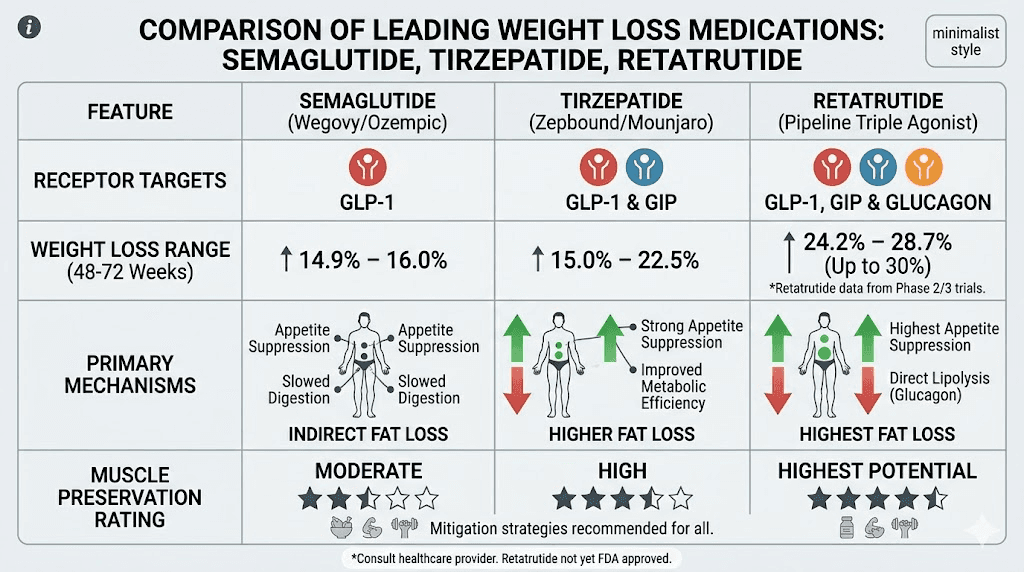
How different GLP-1 medications compare for muscle preservation
Not all GLP-1 medications are created equal when it comes to body composition. The receptor profile, weight loss rate, and metabolic effects differ significantly between options. Understanding these differences helps you set realistic expectations and adjust your approach accordingly.
Semaglutide and muscle
Semaglutide produces approximately 15 to 17 percent body weight loss at therapeutic doses. The STEP trial data showed that roughly 30 to 39 percent of weight lost came from lean body mass in sedentary participants. However, the same data revealed that hand grip strength improved over time, suggesting functional muscle quality increased even as total lean mass decreased modestly.
The semaglutide dosing schedule is weekly, which creates a predictable pattern of side effects and energy levels. Many lifters report that training performance is lowest in the 24 to 48 hours after injection and improves as the week progresses. Planning your most demanding training sessions for days 3 through 6 after injection can optimize performance.
Tirzepatide and muscle
Tirzepatide activates both GLP-1 and GIP receptors, creating a dual mechanism that may offer advantages for muscle preservation. The American Diabetes Association highlighted research showing that newer GLP-1 therapies like tirzepatide enhance the quality of weight loss by improving muscle preservation compared to older single-receptor agonists.
GIP receptor activation has been linked to improved nutrient partitioning, meaning more of the calories you eat get directed toward muscle tissue rather than fat storage. This is particularly relevant for people doing resistance training, as it may amplify the muscle-building response to both food and exercise. The effect on testosterone levels is also noteworthy. Weight loss on tirzepatide has been associated with increases in free testosterone in men, which directly supports muscle protein synthesis and strength gains.
Tirzepatide produces greater total weight loss than semaglutide, up to 22 percent at the highest doses, but the lean-to-fat loss ratio appears more favorable. In practical terms, this means tirzepatide users may retain more muscle for a given amount of total weight loss, making it a potentially better option for those prioritizing body composition over just scale weight.
Retatrutide and body composition
Retatrutide adds a third receptor, glucagon, to the GLP-1 and GIP activation provided by tirzepatide. The glucagon receptor component increases energy expenditure and promotes fat oxidation, which theoretically shifts the body toward burning fat rather than muscle for energy. Phase 2 trial data showed weight loss of up to 24 percent at 48 weeks, the most dramatic results seen with any GLP-1 class medication.
The bodybuilding community has taken particular interest in retatrutide because of its potential for body recomposition. The combination of appetite suppression from GLP-1, nutrient partitioning from GIP, and increased fat oxidation from glucagon creates a metabolic environment that many researchers describe as ideal for cutting while preserving lean mass. The comparison between tirzepatide and retatrutide for muscle preservation is one of the most actively debated topics in the peptide research community.
Which medication is best for lifters?
The honest answer is that it depends on your starting point and goals. For moderate weight loss with favorable body composition, tirzepatide offers advantages over semaglutide based on current evidence. For aggressive weight loss with maximum fat targeting, retatrutide shows the most promise but has less long-term data. For those prioritizing simplicity and the broadest evidence base, semaglutide remains the most studied and well-characterized option.
Regardless of which medication you use, the fundamentals of resistance training and protein intake matter far more than the specific GLP-1 agonist. A researcher doing everything right with semaglutide will preserve more muscle than someone on tirzepatide who skips the gym and eats 80 grams of protein a day. The medication is the catalyst. The work is still yours to do.
Common mistakes that destroy muscle on GLP-1 medications
Knowing what to do is half the battle. Knowing what not to do is the other half. These mistakes are devastatingly common and almost entirely preventable.
Too much cardio, not enough weights
The single biggest mistake GLP-1 users make is defaulting to cardio-heavy exercise routines. Walking, running, cycling. These activities burn calories but provide zero stimulus for muscle preservation. In a calorie deficit, excessive cardio without resistance training actively accelerates muscle loss.
Does this mean you should skip cardio entirely? No. Cardiovascular exercise supports heart health, improves insulin sensitivity, and aids recovery between resistance training sessions. But it should complement your lifting, not replace it. Aim for 150 minutes of moderate-intensity cardio per week, with resistance training taking absolute priority. If you only have time for one type of exercise on a given day, lift weights. Always.
Not eating enough protein
Appetite suppression makes this mistake almost automatic. GLP-1 medications reduce hunger so effectively that many users cut their food intake by 40 to 60 percent. If protein intake drops proportionally, you are creating the perfect environment for muscle catabolism. Track your protein meticulously, especially in the first few months of treatment when appetite changes are most dramatic.
Some researchers report eating fewer than 1000 calories per day on GLP-1 medications and wondering why they feel weak. The medication suppresses hunger, but that does not mean your body stops needing fuel. Prioritizing protein-rich foods ensures that the calories you do consume go toward maintaining lean tissue rather than just surviving the day.
Losing weight too fast
A rapid drop on the scale feels satisfying but comes at a cost. Research consistently shows that losing more than 1 percent of body weight per week significantly increases the proportion of weight loss that comes from lean mass. If you weigh 200 pounds, that means keeping weight loss at or below 2 pounds per week.
The GLP-1 dose titration schedule exists partly for this reason. Starting at a low dose and gradually increasing allows your body to adapt and helps control the rate of weight loss. If you are losing weight faster than the 1 percent threshold, talk to your provider about staying at your current dose longer before increasing. The microdosing approach that some researchers use can help control the rate of loss while maintaining steady progress.
Skipping meals entirely
Some GLP-1 users go entire days without eating because they simply do not feel hungry. This is a disaster for muscle preservation. Extended fasting windows without protein intake push the body into a catabolic state where muscle protein breakdown exceeds synthesis. You do not need to eat large meals. But you do need to eat.
Set protein alarms if necessary. Treat eating as a scheduled activity rather than waiting for hunger signals that may never come. A protein shake between meals takes 30 seconds to prepare and 2 minutes to drink. That small effort can be the difference between preserving your lean mass and losing it.
Ignoring recovery and sleep
Muscles do not grow in the gym. They grow during recovery. Growth hormone, the most powerful anabolic hormone your body produces naturally, releases predominantly during deep sleep cycles. Testosterone, critical for both men and women building muscle, peaks during restorative sleep. Cut your sleep short and you undermine every rep you performed that day.
Target 7 to 9 hours of quality sleep per night. If GLP-1 medications affect your sleep, address this proactively. Magnesium glycinate before bed, consistent sleep and wake times, and limiting caffeine after noon all improve sleep quality. Some users find that timing their injection earlier in the day reduces sleep disruption.
Rest days between training sessions for the same muscle group are equally important. Allow 48 to 72 hours before training the same muscles again. This gives muscle protein synthesis time to complete its cycle and ensures you return to the gym stronger, not still recovering.
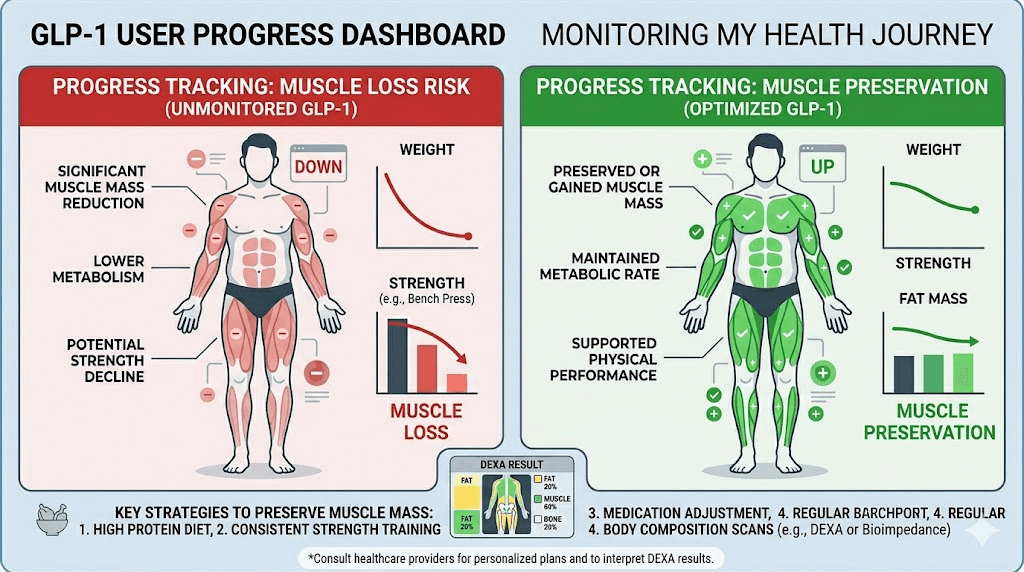
Monitoring your progress the right way
The scale is the worst tool for tracking body composition changes. You can lose fat, gain muscle, and see zero change on the scale, or even see it go up. Relying solely on body weight leads to panic, unnecessary dose increases, and poor decisions. Better tools exist.
DEXA scans
Dual-energy X-ray absorptiometry provides the most accurate body composition data available outside of a research lab. A DEXA scan tells you exactly how much fat, lean mass, and bone mineral density you carry, and it tracks changes over time with high precision.
Schedule a baseline DEXA scan before starting GLP-1 treatment if possible, or as soon as you begin combining the medication with resistance training. Follow-up scans every 3 to 4 months give you objective data on whether your approach is working. If lean mass is declining faster than expected, you know to increase protein intake, training volume, or both before the situation compounds.
Strength tracking
Your gym logbook is the most valuable real-time indicator of muscle preservation. If your strength is maintaining or increasing on key compound lifts, your muscles are being preserved, regardless of what the scale says. Track these lifts consistently:
Squat or leg press
Bench press or chest press
Deadlift or row
Overhead press
If strength drops by more than 10 percent on multiple lifts over a 2 to 4 week period, something is wrong. That usually means calorie intake is too low, protein is inadequate, or recovery is insufficient. Strength loss is your early warning system. Pay attention to it.
Body measurements and photos
Take measurements of your chest, waist, hips, arms, and thighs every 2 to 4 weeks. A shrinking waist with stable or growing arm and thigh measurements is the clearest non-technical indicator of successful body recomposition. This is far more meaningful than scale weight.
Progress photos in consistent lighting, taken monthly, reveal changes that day-to-day mirror checks miss. Use the same pose, same lighting, and same time of day. The visual evidence of recomposition, a more defined physique at a lower body weight, is often dramatic even when the scale barely moves. Before and after comparisons from the GLP-1 community frequently show transformations that the scale alone would never capture.
When to adjust your protocol
Review your data monthly. Ask these questions:
Is strength maintaining or improving? If yes, muscle is being preserved.
Is waist measurement decreasing? If yes, fat is being lost.
Is the rate of total weight loss under 1 percent per week? If yes, the pace is sustainable.
Am I hitting my protein targets daily? If no, fix this first before changing anything else.
If the data shows muscle loss despite adequate protein and training, consider reducing your GLP-1 dose, increasing calorie intake slightly, or consulting with your provider about adjusting the protocol. Home monitoring tools like smart scales with bioimpedance are less accurate than DEXA but can track trends over time when used consistently.
The emerging science of myostatin inhibitors and GLP-1 combinations
The future of GLP-1 therapy and muscle preservation is evolving rapidly. One of the most exciting developments is the combination of GLP-1 medications with myostatin inhibitors, drugs that block the signals telling your body to limit muscle growth.
What myostatin inhibitors do
Myostatin and activin A are the two primary negative regulators of muscle mass. They act as brakes on muscle growth, preventing muscles from growing beyond a certain point. Blocking these signals effectively removes the brakes, allowing muscle to grow more freely, even during calorie restriction.
A landmark 2025 study published in Nature Communications demonstrated that dual blockade of GDF8 (myostatin) and activin A during GLP-1 therapy completely prevented muscle loss while enhancing fat loss in both obese mice and non-human primates. The implications for human therapy are enormous. Instead of losing 30 to 40 percent of weight as lean mass, future GLP-1 users might lose virtually zero muscle while shedding even more fat.
The COURAGE trial results
Regeneron Pharmaceuticals reported interim results from their phase 2 COURAGE trial combining semaglutide with trevogrumab and garetosmab, antibodies that block activin A and myostatin respectively. The results were striking. The combination spared approximately 50 to 80 percent of the lean mass that would have been lost with semaglutide alone, while also increasing fat loss beyond what semaglutide achieved by itself.
In concrete terms, approximately 35 percent of semaglutide-induced weight loss was due to lean mass loss in the control group. The combination group retained most of this lean mass while losing more total weight, meaning a dramatically higher proportion of their weight loss came from fat. This is the holy grail of body recomposition, losing fat without losing muscle.
What this means for you right now
Myostatin inhibitor and GLP-1 combinations are not yet available outside of clinical trials. But they validate the fundamental principle that muscle loss on GLP-1 medications is not inevitable. It is a solvable problem. And while we wait for pharmaceutical solutions, resistance training and adequate protein intake remain the most effective tools for achieving the same goal naturally.
The research also suggests that people who preserve muscle through training and nutrition during GLP-1 therapy may be setting themselves up for even better outcomes if myostatin inhibitors become available in the future. A body that has been trained and nourished to maintain muscle is better positioned to respond to additional anabolic stimuli. Start building the foundation now.
Putting it all together: your complete muscle building protocol on GLP-1
Theory is worthless without execution. Here is the complete, day-by-day framework that brings together everything covered in this guide.
Protocol 1: Muscle preservation for beginners
Goal: Prevent lean mass loss while losing fat on GLP-1 therapy
Training:
3 full-body resistance sessions per week (Monday, Wednesday, Friday)
Focus on machine-based compound movements (leg press, chest press, lat pulldown, cable row)
3 sets of 10 to 12 reps per exercise, 6 to 8 exercises per session
Progressive overload: add weight when all sets hit 12 reps
Nutrition:
Protein: 1.2 to 1.4 grams per kilogram body weight daily
Minimum 3 meals with 25+ grams protein each
Protein shake post-workout
Total calories: at least 1200 (women) or 1500 (men)
Supplements:
Creatine monohydrate: 5 grams daily
Vitamin D3: 3000 IU daily
Electrolyte supplement daily
B-complex vitamin daily
Expected results:
Weight loss: 1 to 2 pounds per week
Lean mass: maintained or slightly decreased (under 15 percent of total loss)
Strength: maintained or improved on all exercises
Protocol 2: Body recomposition for intermediate lifters
Goal: Lose fat and build muscle simultaneously on GLP-1 therapy
Training:
4-day upper/lower split
Compound lifts: squats, deadlifts, bench press, overhead press, rows
4 sets of 6 to 10 reps on compounds, 3 sets of 10 to 15 on accessories
12 to 16 hard sets per muscle group per week
Progressive overload tracked in a logbook
Nutrition:
Protein: 1.6 to 2.0 grams per kilogram body weight daily
4 to 5 meals with 30 to 40 grams protein each
Carbohydrates concentrated around training (pre and post workout)
High-protein meals prioritized at every eating opportunity
Calorie deficit: 500 to 750 below maintenance
Supplements:
Creatine monohydrate: 5 grams daily
Whey protein isolate: 1 to 2 scoops daily as needed
EAAs: 10 grams during training
Vitamin D3: 5000 IU daily
Magnesium glycinate: 400 milligrams before bed
Full supplement stack optimized for GLP-1 use
Expected results:
Weight loss: 1 to 1.5 pounds per week
Lean mass: maintained or slightly increased
Strength: 5 to 15 percent improvement over 12 weeks
Visible body recomposition within 8 to 12 weeks
Protocol 3: Advanced muscle building for experienced lifters
Goal: Maximize lean mass gain while cutting body fat aggressively on GLP-1 therapy
Training:
5-day push/pull/legs or upper/lower/push/pull/legs split
Heavy compound lifts in the 4 to 8 rep range
Moderate accessory work in the 8 to 15 rep range
16 to 20 hard sets per muscle group per week
Periodization: 3 weeks of progressive overload followed by 1 deload week
Nutrition:
Protein: 2.0 to 2.4 grams per kilogram body weight daily
5 to 6 meals with 35 to 50 grams protein each
Carb cycling: higher carbs on training days, lower on rest days
Strategic refeeds: one higher-calorie day per week at maintenance
Calorie deficit: 300 to 500 below maintenance (smaller deficit to preserve muscle)
Supplements:
Creatine monohydrate: 5 grams daily
Whey protein isolate: 2 to 3 scoops daily
EAAs: 15 grams during training
Vitamin D3: 5000 IU daily
Omega-3 fatty acids: 3 grams EPA/DHA daily
NAD+ support for cellular energy
Ashwagandha: 600 milligrams daily for cortisol management
Expected results:
Weight loss: 0.5 to 1 pound per week
Lean mass: maintained or increased by 1 to 3 pounds over 12 weeks
Strength: maintained on all lifts, potential PRs on some
Dramatic visual transformation
Special considerations for different populations
Women building muscle on GLP-1 medications
Women produce significantly less testosterone than men, which affects the rate and magnitude of muscle growth. However, this does not mean muscle building on GLP-1s is harder for women. It simply looks different. Women can and do build muscle effectively during GLP-1 therapy, particularly when protein intake and resistance training are prioritized.
Hormonal fluctuations throughout the menstrual cycle affect energy, strength, and recovery. GLP-1 medications can interact with these cycles, sometimes causing irregularities in the first few months of treatment. Training around your cycle, pushing harder during the follicular phase when energy tends to peak and backing off slightly during the luteal phase, can optimize results while respecting your physiology.
Women on hormone replacement therapy who add GLP-1 medications may experience unique body composition advantages. Estrogen supports lean mass preservation, and the combination of HRT with GLP-1 therapy and resistance training can produce exceptional recomposition results.
Older adults preserving muscle on GLP-1 therapy
Age-related muscle loss (sarcopenia) makes muscle preservation on GLP-1 medications even more critical for adults over 50. The consequences of lean mass loss are more severe in this population, including increased fall risk, reduced functional independence, and accelerated aging. Resistance training intensity should be appropriately challenging while respecting joint limitations. Protein needs are higher in older adults, with targets of 1.6 to 2.0 grams per kilogram being appropriate even for those not engaged in heavy training. Bone health monitoring becomes an additional consideration, as both weight loss and aging affect bone mineral density.
Athletes and bodybuilders on GLP-1 therapy
Competitive athletes using GLP-1 medications for body composition management face unique challenges. Training volumes are typically higher, recovery demands are greater, and any performance decrease has immediate competitive consequences. The off-label use of GLP-1 medications in bodybuilding contexts has grown substantially, with researchers exploring stacking strategies that combine GLP-1 agonists with peptides that support growth hormone release.
The key for athletes is keeping the calorie deficit moderate. Aggressive cuts that work for sedentary individuals will crush training performance and recovery in people training at high volumes. A smaller deficit of 250 to 500 calories, combined with the appetite-suppressing effects of the medication, produces steady fat loss without the performance cliff that larger deficits cause.
Frequently asked questions
Will I lose all my muscle on semaglutide?
No. Studies show that 60 to 70 percent of weight lost on semaglutide comes from fat, not muscle. With proper protein intake and resistance training, lean mass loss can be minimized to under 15 percent of total weight loss, and some researchers actually gain strength during treatment.
How much protein should I eat on GLP-1 medications to build muscle?
Aim for 1.6 to 2.0 grams of protein per kilogram of body weight daily if muscle building is your goal. That is approximately 0.7 to 0.9 grams per pound. Distribute this across 4 to 5 meals, with at least 25 to 40 grams per meal to maximize muscle protein synthesis.
Can I do bodybuilding while taking tirzepatide?
Yes. Tirzepatide may actually offer advantages for body composition compared to semaglutide due to its dual GIP/GLP-1 receptor activation. Many bodybuilders use GLP-1 medications during cutting phases with excellent results when training and nutrition are dialed in.
Should I take creatine while on GLP-1 therapy?
Absolutely. Creatine is safe and effective during GLP-1 use. It supports strength, power output, and lean mass preservation. Take 3 to 5 grams of creatine monohydrate daily. The slight water retention in muscles is beneficial, not harmful.
Is it better to do cardio or weights on GLP-1 medications?
Weights take priority without question. Resistance training provides the mechanical stimulus that tells your body to preserve muscle during a calorie deficit. Include 3 to 5 resistance sessions per week and use moderate cardio as a supplement, not a replacement. Aim for 150 minutes of moderate cardio weekly alongside your lifting program.
How long does it take to see muscle definition on GLP-1 therapy?
Most people notice visible body composition changes within 8 to 12 weeks of combining GLP-1 medication with consistent resistance training and adequate protein. Fat loss reveals existing muscle definition, so the visual transformation can be dramatic even before significant new muscle is built. Check before and after results for realistic expectations.
Does GLP-1 affect recovery from workouts?
Reduced calorie intake can slow recovery, so adequate protein, sleep, and electrolytes become more important during GLP-1 therapy. Some users report muscle soreness lasting longer than usual, particularly during dose increases. Allowing 48 to 72 hours between sessions for the same muscle group prevents overtraining.
Can I gain weight from muscle while the scale shows weight loss on GLP-1?
Yes. The scale measures total body weight, not composition. You can simultaneously lose 3 pounds of fat and gain 1 pound of muscle in a month, showing only a 2-pound loss on the scale while looking dramatically different. This is why DEXA scans and strength tracking are superior to scale weight for monitoring progress.
External resources
American Council on Exercise: GLP-1s and lean mass research review
Endocrine Society: Protein intake and GLP-1 muscle preservation research
PubMed Central: Saving muscle while losing weight on GLP-1 drugs
Frontiers: GLP-1 agonists and exercise for lifestyle prioritization
Nature Communications: Myostatin blockade during GLP-1 therapy
For researchers serious about optimizing their body composition during GLP-1 therapy, SeekPeptides offers the most comprehensive resource available. Members access evidence-based protocols, detailed supplement guides, dosing calculators, and a community of thousands who have navigated this exact challenge successfully. From peptide stacking strategies to maintenance dosing protocols, everything you need to maximize your results is in one place.
In case I do not see you, good afternoon, good evening, and good night. May your muscles stay strong, your protein stay high, and your body composition stay improving.