Mar 24, 2026

Some people start semaglutide and feel nothing. No nausea. No headaches. No change at all except the number on the scale slowly dropping. Others stand up from the couch and the room tilts sideways. The floor feels uncertain. Their vision narrows for a second or two, and they grab the nearest wall just to stay upright.
That lightheaded feeling is not rare. In clinical trials, approximately 8% of patients using semaglutide reported dizziness or lightheadedness as a side effect. That number likely underrepresents reality, because many people experience mild episodes they never bother reporting. The sensation ranges from a brief wooziness when standing too fast to a persistent foggy feeling that lingers through the afternoon. And while it is almost always manageable, understanding why it happens makes the difference between suffering through it and preventing it entirely.
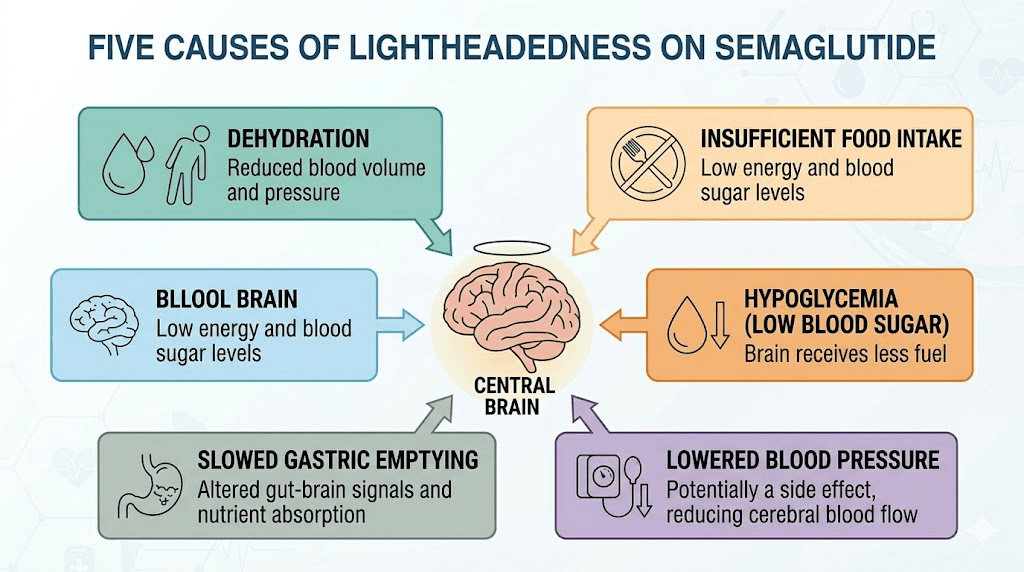
The causes are not mysterious. They come down to five core mechanisms that interact with how semaglutide changes your body. General dizziness on semaglutide covers broad territory, but lightheadedness specifically points to reduced blood flow to the brain. That distinction matters. It changes how you respond, what you eat, how you move, and when you should worry. This guide covers every angle, from the biology behind it to the practical protocols that stop it from disrupting your day.
Why semaglutide makes you feel lightheaded
Lightheadedness is not a single problem with a single cause. It is the brain sending a distress signal that something in the supply chain has gone wrong. Blood pressure too low. Blood sugar dropping. Not enough fluid in the system. Sometimes all three at once. Semaglutide creates conditions where each of these can happen more easily than usual, and understanding the specific mechanism behind your lightheadedness is the first step toward fixing it.
Blood sugar drops and hypoglycemia
Semaglutide works by mimicking GLP-1, a hormone that stimulates insulin release when blood sugar rises. This is the core mechanism that makes the medication effective. But it also means your body becomes more efficient at clearing glucose from the bloodstream, and sometimes it clears too much.
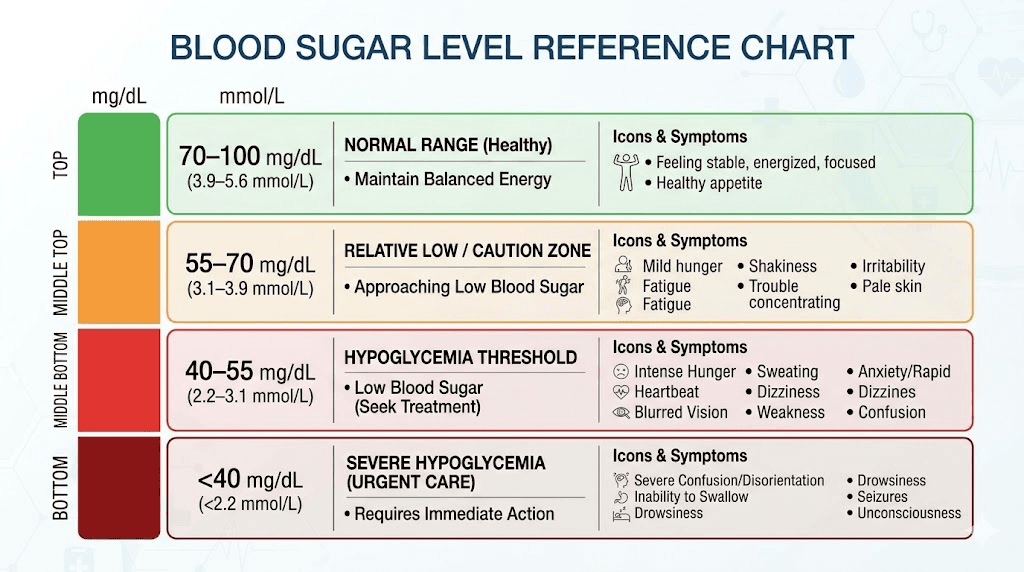
The brain runs almost entirely on glucose. When blood sugar drops below about 70 mg/dL, the brain starts rationing its fuel supply. The result is lightheadedness, confusion, shakiness, and that strange feeling of being disconnected from your own body. For people who do not have diabetes, semaglutide rarely causes dangerous hypoglycemia on its own. The medication stimulates insulin in a glucose-dependent manner, meaning it should not push insulin levels beyond what your blood sugar warrants.
But here is where it gets complicated.
Semaglutide dramatically reduces appetite. Many people find themselves eating far less than they used to, sometimes skipping meals entirely without realizing it. When you combine reduced food intake with a medication that enhances insulin sensitivity, blood sugar can drift lower than your body is accustomed to. You might not technically be hypoglycemic by clinical standards, but if your body is used to running at 110 mg/dL and suddenly operates at 80 mg/dL, you will feel the difference. That relative drop triggers lightheadedness even though the absolute number looks normal on paper.
The risk increases substantially when semaglutide is combined with other glucose-lowering medications. If you take phentermine alongside semaglutide or use insulin, the hypoglycemia risk multiplies. A real-world pharmacovigilance analysis found that GLP-1 receptor agonists combined with insulin or sulfonylureas significantly increased hypoglycemic events compared to GLP-1 therapy alone.
Dehydration from reduced food and fluid intake
This is the most common and most underestimated cause of lightheadedness on semaglutide. People focus on the nausea. They focus on the appetite suppression. What they miss is how dramatically their total fluid intake drops when they stop eating as much.
Roughly 20% of daily water intake comes from food. When semaglutide cuts your appetite and you eat half your normal volume, you lose a significant chunk of hydration without ever feeling thirsty. Add in the gastrointestinal side effects of semaglutide, particularly nausea, vomiting, and diarrhea, and fluid losses accelerate further. The digestive disruptions from semaglutide compound the problem, pulling water into the gut and reducing absorption.
Dehydration reduces blood volume. Less blood volume means less pressure in the system. Less pressure means the brain receives less blood flow, especially when you change positions. Stand up too fast when dehydrated and gravity pulls blood away from your head before your cardiovascular system can compensate. The result is that familiar lightheaded rush.
Most people on semaglutide need to actively increase their water intake by 16 to 32 additional ounces per day beyond what they were drinking before starting the medication. This is not optional. It is the single most effective intervention for preventing lightheadedness.
Blood pressure changes and orthostatic hypotension
Semaglutide lowers blood pressure. For many people, this is a benefit. Research published in the Journal of Clinical Medicine found that semaglutide reduces systolic blood pressure by an average of 2.5 to 5 mmHg in patients without diabetes. In patients with obesity and hypertension, the reductions can be more pronounced as weight comes off.
Lower blood pressure is generally healthy. But when it drops too far or too fast, lightheadedness follows.
Orthostatic hypotension is the medical term for a blood pressure drop that happens when you stand up. Normally, your body compensates within seconds by constricting blood vessels and increasing heart rate. But when overall blood pressure is already lower than usual, when you are dehydrated, and when you have lost weight rapidly, this compensatory mechanism struggles. According to the Wegovy prescribing information, adverse reactions related to hypotension were reported in 1.3% of semaglutide-treated patients compared to 0.4% on placebo. That risk increases further if you take higher doses of semaglutide or use blood pressure medications simultaneously.
The pattern is predictable. You sit for a while. You stand up. The room goes gray for a moment. You steady yourself. It passes in 5 to 15 seconds. If this sounds familiar, orthostatic hypotension is likely your primary trigger.
Electrolyte imbalances
Sodium, potassium, and magnesium do not get enough attention in conversations about semaglutide side effects. These minerals regulate nerve signaling, muscle contraction, and fluid balance. When they fall out of range, lightheadedness is one of the first symptoms.
Semaglutide can disrupt electrolyte balance in several ways. Reduced food intake means fewer dietary sources of these minerals. Gastrointestinal side effects like the fatigue and weakness from semaglutide often accompany electrolyte depletion. Vomiting and diarrhea directly flush electrolytes from the body. And increased water intake without electrolyte replacement dilutes what remains, a condition called hyponatremia.
Low sodium causes lightheadedness, confusion, and in severe cases, seizures. Low potassium adds muscle weakness and heart palpitations to the mix. Low magnesium contributes to muscle cramps, which is why some people also experience leg cramps on semaglutide alongside their lightheadedness.
Caloric restriction and rapid weight loss
When weight comes off quickly, the body makes adjustments that can trigger lightheadedness independently of the other mechanisms listed above. Rapid caloric restriction activates the sympathetic nervous system differently. Metabolic rate shifts. Hormonal cascades change. The body enters a state of adaptation that takes time to stabilize.
People who lose more than 2 to 3 pounds per week consistently are at higher risk for positional lightheadedness. The body has not had time to recalibrate its blood pressure regulation for a smaller body mass. Blood vessels that were calibrated for a larger body now have excess capacity, reducing effective pressure. This is one reason why weight loss plateaus on semaglutide sometimes come with a reduction in side effects, because the body has caught up to its new baseline.
If you are losing weight rapidly and feeling lightheaded, the solution is not to stop losing weight. It is to ensure you are eating enough protein (a minimum of 60 to 80 grams per day), staying hydrated, and replenishing electrolytes. The semaglutide diet plan should account for these needs specifically.
Lightheadedness versus dizziness: understanding the difference
People use these words interchangeably. Doctors do not. The distinction matters because the causes and treatments differ.
Lightheadedness is the sensation of feeling faint or woozy. The world does not spin. Instead, you feel like you might pass out. Your vision may narrow or dim briefly. It typically worsens when you stand and improves when you sit or lie down. This type of symptom almost always relates to blood flow, whether from blood pressure, blood sugar, or blood volume issues.
Dizziness involves a spinning sensation, also called vertigo. The room seems to rotate around you, or you feel like you are tilting or falling even while sitting still. This type relates more to the inner ear and vestibular system. A large real-world cohort study found that semaglutide and tirzepatide were both associated with an increased risk of vestibular disorders, suggesting these medications may affect the inner ear through mechanisms that are still being studied.
If your symptoms are primarily positional (they happen when you stand or change positions), you are most likely dealing with lightheadedness related to blood pressure or blood sugar. If the room spins regardless of position, that is dizziness with a different underlying cause, and it warrants a conversation with your healthcare provider. Our guide on semaglutide and dizziness covers the vertigo and vestibular side in detail.
When lightheadedness starts and how long it lasts
Timing matters. When the lightheadedness appears in your semaglutide journey tells you a lot about what is causing it and how long you can expect it to last.
The first two weeks at starting dose
Most lightheadedness appears within the first 7 to 14 days of starting semaglutide. The body is adjusting to a new medication, appetite is dropping rapidly, and eating patterns are shifting before hydration habits have caught up. This initial phase accounts for the majority of lightheadedness reports.
At the starting dose of 0.25mg, lightheadedness is usually mild. Most people describe it as a brief wooziness when standing or a vague spacey feeling in the afternoon. These early symptoms typically resolve within 2 to 4 weeks as the body adapts and as you learn to adjust your eating and drinking habits. Understanding how quickly semaglutide takes effect helps set expectations for this adjustment period.
Dose escalation periods
Every time the dose increases, there is a new adjustment window. Moving from 0.25mg to 0.5mg, from 0.5mg to 1mg, and especially from 1mg to the higher therapeutic doses can each trigger a recurrence of lightheadedness. The pattern is predictable: you increase the dose, appetite drops further, food intake decreases, and the body needs another week or two to recalibrate.
This is why dose escalation is done gradually. The standard protocol moves up every 4 weeks, giving the body time to stabilize at each level. Rushing through dose escalation increases the risk of lightheadedness and other side effects significantly. Checking whether your dose is appropriate can help you determine if the lightheadedness relates to dosing that is too aggressive for your body.
Timeline for resolution
For most people, lightheadedness follows this pattern:
Days 1 to 7: Most likely to appear if it is going to occur. Peak intensity during this window.
Days 7 to 14: Gradually improving as the body adapts and as you implement management strategies.
Days 14 to 28: Mostly resolved for the majority of people. Residual episodes are usually tied to specific triggers like skipping meals or dehydration.
Beyond 4 weeks: If lightheadedness persists past the first month at a stable dose, something else is likely contributing. This warrants evaluation of blood pressure, blood sugar, and electrolyte levels.
The timeline for semaglutide to reach full effectiveness mirrors the side effect adaptation curve. As the drug reaches steady state, so does your body.
How to prevent lightheadedness on semaglutide
Prevention is more effective than treatment. Once you feel lightheaded, you are already behind. The blood sugar has already dropped. The dehydration has already accumulated. The blood pressure has already fallen. The goal is to keep these systems stable throughout the day so the lightheadedness never arrives in the first place.
Hydration strategies that actually work
Telling someone to drink more water is not a strategy. Here is what actually works.
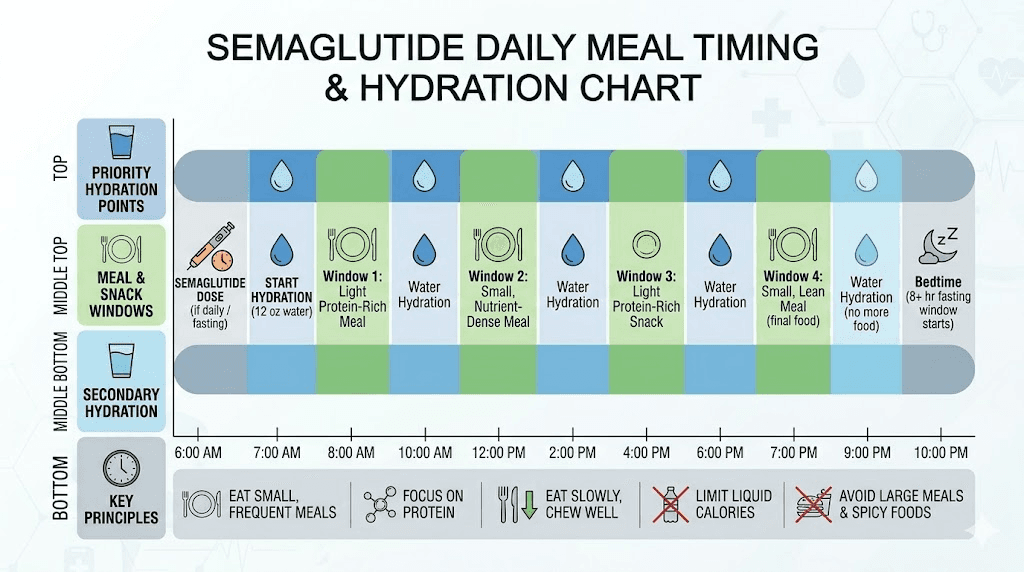
Start your day with 16 ounces of water before anything else. Your body has been fasting and dehydrating for 6 to 8 hours overnight. That morning deficit is when many people experience their first lightheaded episode of the day.
Set a timer for every 90 minutes during waking hours. Drink 8 to 12 ounces each time. Do not wait until you feel thirsty, because semaglutide can blunt thirst signals just as it blunts hunger signals. By the time you feel thirsty, you are already mildly dehydrated.
Track total intake. Aim for a minimum of 80 ounces per day, more if you exercise, live in a hot climate, or experience GI side effects from semaglutide. Some people need 100 to 120 ounces to stay ahead of fluid losses.
Add electrolytes to at least one serving of water per day. Plain water without electrolytes can actually worsen the problem by diluting sodium levels. A pinch of salt and a squeeze of lemon in your water is the simplest approach. Commercial electrolyte packets work too, but avoid ones loaded with sugar.
Eating patterns and blood sugar management
The appetite suppression from semaglutide is powerful. So powerful that many people simply forget to eat. This is a problem when it comes to lightheadedness, because your brain needs a steady supply of glucose to function properly.
Do not skip meals. Even if you are not hungry, eat something every 4 to 5 hours. Small meals are fine. A handful of nuts and a piece of fruit counts. What matters is keeping blood sugar from dropping into the zone that triggers lightheadedness. The recommended foods for semaglutide users emphasize protein and complex carbohydrates for exactly this reason.
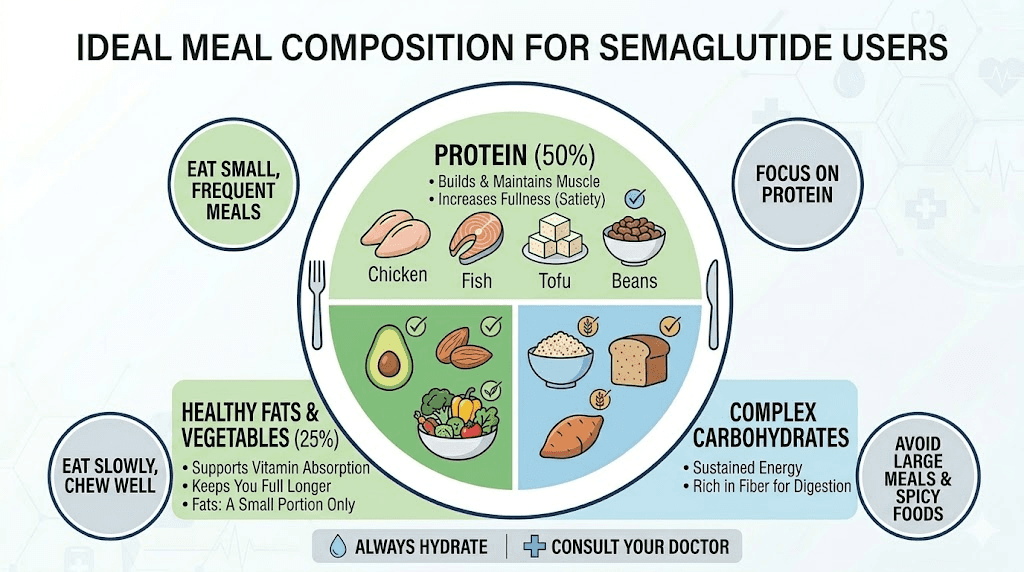
Prioritize protein at every meal. Protein stabilizes blood sugar more effectively than carbohydrates alone and keeps levels steady for longer. Aim for 20 to 30 grams per meal. Eggs, Greek yogurt, chicken, fish, and legumes are excellent choices that are usually well-tolerated even with reduced appetite.
Avoid simple carbohydrates in isolation. A piece of white bread or a handful of crackers will spike blood sugar quickly and then drop it just as fast, creating the exact rollercoaster that triggers lightheadedness. Pair carbohydrates with protein or fat to slow the absorption curve. Understanding the foods to avoid while on semaglutide can help you make better choices.
Standing up slowly and managing orthostatic changes
This sounds too simple to be important. It is actually one of the most effective strategies.
When you have been sitting or lying down, follow the 3-stage method. First, sit up for 10 seconds. Second, move to the edge of your seat and pause for another 10 seconds. Third, stand up slowly while holding onto something stable. This gives your cardiovascular system time to adjust blood distribution before gravity takes over.
If you work at a desk, stand up at least once every 30 to 45 minutes. Prolonged sitting followed by sudden standing is the highest-risk combination for orthostatic lightheadedness. Regular position changes keep the compensatory mechanisms active and responsive.
Compression socks can help. They prevent blood from pooling in the lower legs when standing, maintaining more volume in the central circulation where the brain can access it. This is especially useful for people who are also taking blood pressure medication.
Electrolyte supplementation protocol
A basic daily electrolyte protocol for semaglutide users who experience lightheadedness includes:
Sodium: 1,000 to 2,000mg supplemental sodium per day, adjusted based on sweat loss and diet. If you are eating less food, you are getting less dietary sodium. Replace it deliberately. Bone broth, salted nuts, and electrolyte drinks are practical sources.
Potassium: 2,000 to 3,000mg total daily intake from food and supplements combined. Bananas, avocados, potatoes, and spinach are potassium-rich foods that most semaglutide users tolerate well.
Magnesium: 200 to 400mg supplemental magnesium glycinate or citrate at bedtime. This also helps with muscle cramps from semaglutide and may improve sleep quality on semaglutide.
If you experience ongoing lightheadedness despite adequate hydration and food intake, ask your provider to check a basic metabolic panel. This simple blood test reveals sodium, potassium, and other electrolyte levels that pinpoint the specific deficiency.
Timing your dose for fewer side effects
When you take your weekly semaglutide injection can influence whether you experience lightheadedness. The medication reaches peak blood levels approximately 1 to 3 days after injection, and side effects tend to cluster around this peak.
Many people find that taking their injection on a day when they can rest the following day reduces the impact of side effects. Friday evening injections, for example, allow the peak to occur over the weekend when physical demands are typically lower. The best time of day to take semaglutide varies by individual, but consistency matters more than the specific day. Some people report less lightheadedness when injecting in the evening versus the morning, possibly because sleep covers the initial absorption period.
Choosing the right injection site for semaglutide can also influence absorption rate and therefore side effect timing, though the effect on lightheadedness specifically is modest.
What to eat when semaglutide makes you lightheaded
When lightheadedness hits, you need to respond quickly. The right foods can restore blood sugar and provide electrolytes within 15 to 30 minutes. The wrong foods will spike and crash your blood sugar, making the problem worse an hour later.
Immediate response foods
If you feel lightheaded right now, eat one of these combinations:
Option 1: A small handful of salted almonds with 4 to 6 ounces of orange juice. The juice provides fast glucose while the almonds add protein and fat to sustain the blood sugar rise.
Option 2: Half an avocado with a pinch of salt on whole grain toast. This provides potassium, sodium, complex carbohydrates, and healthy fat in one serving.
Option 3: A cup of bone broth with a handful of crackers. The broth delivers sodium and fluid simultaneously while the crackers provide quick glucose.
The key is combining a fast-acting carbohydrate source with protein or fat. Pure sugar (candy, soda) will resolve the lightheadedness temporarily but create a rebound drop 60 to 90 minutes later. Always pair quick carbohydrates with something that slows absorption.
Blood sugar stabilizing meals
Building meals around blood sugar stability prevents lightheadedness from occurring in the first place. Each meal should contain three components: protein (at least 20 grams), complex carbohydrates (whole grains, vegetables, legumes), and healthy fat (olive oil, avocado, nuts). This combination creates a slow, steady glucose release that keeps levels stable for 3 to 5 hours.
Some practical meal ideas that work well even with reduced appetite include scrambled eggs with spinach and toast, Greek yogurt with berries and a tablespoon of nut butter, or a small portion of salmon with sweet potato and steamed vegetables. The complete semaglutide diet plan provides more detailed meal frameworks.
SeekPeptides members access detailed nutritional protocols designed specifically for people on GLP-1 medications, including meal plans that prioritize blood sugar stability and lightheadedness prevention alongside optimal weight loss.
Hydrating foods that count toward fluid intake
When drinking enough water feels like a chore, eating water-rich foods helps bridge the gap. Cucumbers (96% water), watermelon (92% water), strawberries (91% water), and celery (95% water) all contribute meaningful fluid volume. Soups and broths count as both food and hydration, making them ideal for semaglutide users who struggle with appetite.
Smoothies work particularly well because they combine hydration, electrolytes from fruit, protein from yogurt or protein powder, and easy digestibility for people experiencing appetite suppression from semaglutide. A basic anti-lightheadedness smoothie might include a cup of coconut water, half a banana, a scoop of protein powder, a handful of spinach, and a pinch of salt.
Lightheadedness at different semaglutide doses
Not all doses carry the same risk. Understanding what to expect at each level helps you prepare and respond appropriately.
Starting dose: 0.25mg
This is the lowest dose, designed primarily for body acclimation rather than therapeutic effect. Lightheadedness at this dose is relatively uncommon but does occur, especially in people who are sensitive to blood sugar changes or who have low baseline blood pressure. If you experience significant lightheadedness at 0.25mg, it is worth checking blood pressure and blood sugar before escalating. Use the semaglutide dosage calculator to verify your dosing is appropriate for your body weight.
Escalation dose: 0.5mg
The first real dose increase is where lightheadedness most commonly appears. Appetite suppression intensifies noticeably at 0.5mg, and the gap between old eating habits and new reduced intake widens. Most people who will experience lightheadedness on semaglutide first notice it at this dose level. Proactive hydration and meal scheduling during the first two weeks at 0.5mg prevents most episodes.
Therapeutic dose: 1mg and above
At 1mg, semaglutide reaches its initial therapeutic range for weight loss. Side effects that were managed at lower doses can intensify. Lightheadedness at this level often reflects cumulative dehydration or electrolyte depletion that has been building throughout the dose escalation period rather than a new acute reaction to the higher dose itself. Understanding unit conversions for semaglutide helps ensure accurate dosing at each level.
For people using compounded semaglutide at higher concentrations, the reconstitution ratios matter. Incorrect mixing can lead to accidentally higher or lower doses, which directly affects side effect severity including lightheadedness.
Higher doses: 1.7mg and 2.4mg
The maximum recommended dose of 2.4mg for weight management produces the strongest appetite suppression and the most significant metabolic changes. Lightheadedness at these doses is more common and more persistent. People at higher doses need to be especially vigilant about hydration, nutrition, and electrolyte intake. Converting 1.7mg to units or 2.4mg to units accurately ensures you are getting the intended dose.
If lightheadedness becomes unmanageable at higher doses despite proper hydration and nutrition, discuss dose reduction with your provider. A lower dose that you can tolerate and maintain consistently produces better long-term outcomes than a higher dose that makes you miserable or puts you at risk for falls.
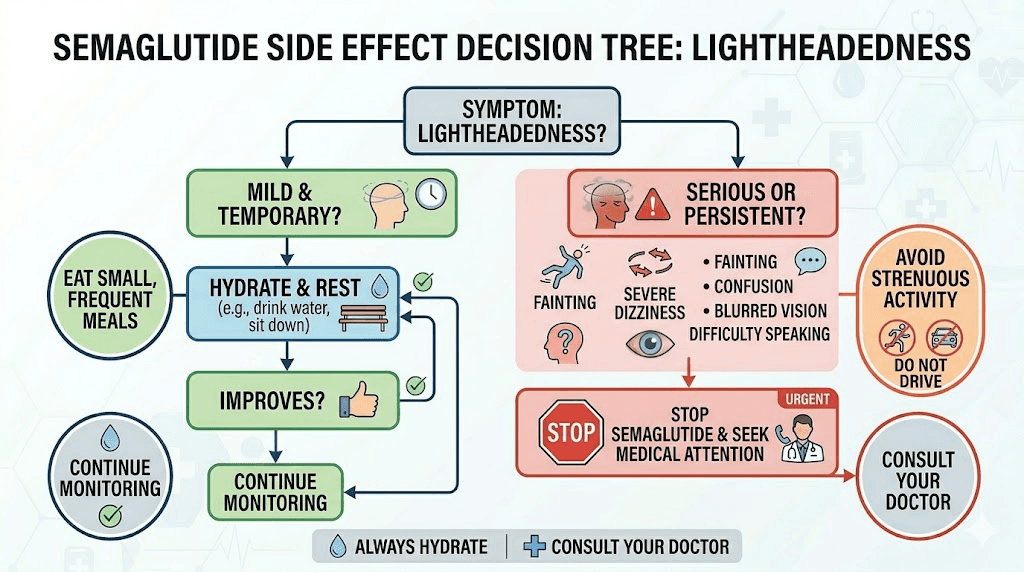
When lightheadedness signals something serious
Most lightheadedness on semaglutide is benign. Annoying, yes. Concerning, sometimes. Dangerous, rarely. But certain patterns and accompanying symptoms require immediate medical attention. Do not dismiss these.
Signs of severe hypoglycemia
Mild lightheadedness from low blood sugar resolves with food. Severe hypoglycemia does not respond as easily and can progress to dangerous territory. Watch for these escalating symptoms:
Confusion or inability to think clearly. Slurred speech. Excessive sweating with cold, clammy skin. Rapid heartbeat or heart palpitations. Visual disturbances beyond brief dimming. Extreme weakness or inability to stand. Loss of consciousness.
If blood sugar drops below 54 mg/dL, this is a medical emergency regardless of whether you lose consciousness. The risk is highest when semaglutide is combined with insulin, sulfonylureas, or other glucose-lowering medications. People with diabetes should have glucagon available and ensure someone in their household knows how to administer it.
Signs of dangerous dehydration
Dehydration exists on a spectrum. Mild dehydration causes lightheadedness. Severe dehydration can damage kidneys and cause cardiovascular collapse. Warning signs that dehydration has progressed beyond mild include:
Dark amber urine or producing very little urine despite drinking fluids. Dry mouth and cracked lips that do not improve with water. Rapid heart rate at rest (above 100 beats per minute). Sunken eyes. Persistent lightheadedness that does not improve after lying down and drinking fluids for 30 minutes.
The GI side effects of semaglutide, particularly persistent vomiting or diarrhea, can push dehydration into dangerous territory quickly. If you cannot keep fluids down for more than 12 hours, contact your healthcare provider. Intravenous fluid replacement may be necessary.
Syncope and fall risk
Syncope means actually passing out. Pre-syncope is that feeling of nearly passing out, where your vision tunnels and your hearing fades. If you have experienced either on semaglutide, this is a conversation to have with your provider before continuing at your current dose.
Falls are the real danger, especially for older adults. A lightheaded moment while standing can lead to a fall, which can cause fractures, head injuries, or worse. People over 65, those with a history of falls, and anyone taking blood pressure medications alongside semaglutide should be especially cautious about positional changes.
Consider avoiding situations where a sudden lightheaded episode could be dangerous: climbing ladders, operating heavy equipment, or driving immediately after standing up. These precautions are temporary and usually only necessary during dose initiation and escalation periods.
When to call your doctor
Contact your healthcare provider if:
Lightheadedness persists for more than 4 weeks at a stable dose despite implementing prevention strategies. Episodes are increasing in frequency or severity rather than improving. You experience actual fainting or near-fainting episodes. Lightheadedness is accompanied by chest pain, severe headache, or shortness of breath. You notice a rapid or irregular heartbeat during episodes. Blood sugar readings consistently fall below 70 mg/dL.
These patterns may indicate that your dose needs adjustment, that an underlying condition is contributing, or that a medication interaction needs to be addressed.
Drug interactions that worsen lightheadedness
Semaglutide does not exist in isolation. Most people taking it also take other medications, and several common combinations increase the risk of lightheadedness significantly.
Blood pressure medications
This is the most common interaction leading to lightheadedness. If you take antihypertensives (ACE inhibitors, ARBs, beta blockers, calcium channel blockers, or diuretics) and start semaglutide, your blood pressure may drop more than intended. Semaglutide contributes its own blood pressure-lowering effect through weight loss, improved insulin sensitivity, and direct vascular effects. Combined with a blood pressure medication dosed for your pre-semaglutide weight and metabolism, the total effect can be excessive.
Work with your provider to monitor blood pressure closely during semaglutide dose escalation. Many people who start semaglutide eventually need their blood pressure medications reduced or discontinued as weight comes off. This is a positive outcome, but the medication adjustments need to keep pace with the changes.
Insulin and sulfonylureas
These medications actively lower blood sugar, and adding semaglutide to the mix compounds the glucose-lowering effect. Sulfonylureas (glipizide, glyburide, glimepiride) stimulate insulin release regardless of blood sugar level, creating a higher risk of hypoglycemia. Insulin dose requirements often decrease substantially when semaglutide is added, and failure to reduce insulin doses proactively leads to hypoglycemic episodes with lightheadedness as a primary symptom.
If you take insulin and start semaglutide, expect that your insulin requirements will decrease. Work with your prescriber on a proactive dose reduction plan rather than waiting for hypoglycemic events to force the adjustment.
Diuretics
Diuretics reduce blood volume by increasing urine output. Combined with semaglutide-induced dehydration from reduced food and fluid intake, plus potential GI fluid losses, diuretics can push total blood volume dangerously low. Hydrochlorothiazide, furosemide, and spironolactone all contribute to this interaction. The result is orthostatic lightheadedness that is more severe and more persistent than what semaglutide causes alone. Monitoring your semaglutide dosage carefully becomes even more important when diuretics are part of the picture.
Alcohol
Alcohol compounds every mechanism that causes lightheadedness on semaglutide. It dehydrates. It lowers blood sugar. It drops blood pressure. It impairs the cardiovascular reflexes that compensate for positional changes. If you are experiencing lightheadedness on semaglutide, alcohol will make it meaningfully worse. The comprehensive guide on drinking alcohol on semaglutide covers the specific risks and practical guidelines.
Exercise and physical activity considerations
Exercise is important during weight loss. It preserves muscle mass, improves metabolic health, and supports cardiovascular fitness. But exercise also challenges the same systems that semaglutide is already stressing, specifically hydration, blood sugar, and blood pressure regulation.
Adjusting workouts when lightheaded
Do not exercise through severe lightheadedness. This is a safety issue. A lightheaded moment during a heavy squat or while running on a treadmill can result in injury. Modify your routine during periods when lightheadedness is active.
Switch from high-intensity to moderate-intensity exercise. Walking, cycling, swimming, and yoga are lower-risk alternatives to heavy weightlifting or HIIT during adjustment periods. People who wonder whether they can lose weight on semaglutide without exercise should know that the medication works for weight loss regardless, but maintaining physical activity preserves lean mass and metabolic health.
Pre-exercise nutrition matters more on semaglutide than it does normally. Eat a small snack containing 15 to 20 grams of carbohydrates and 10 to 15 grams of protein about 60 to 90 minutes before exercise. Drink 16 ounces of water with electrolytes in the hour leading up to your workout. Post-exercise, replenish with both fluids and food within 30 minutes.
When to avoid exercise entirely
Skip the workout if you feel lightheaded before starting. If you have not been able to eat enough in the previous 6 hours. If you are in the first 48 hours after a dose increase. If the temperature is above 85 degrees and you plan to exercise outdoors. These are temporary restrictions, not permanent limitations.
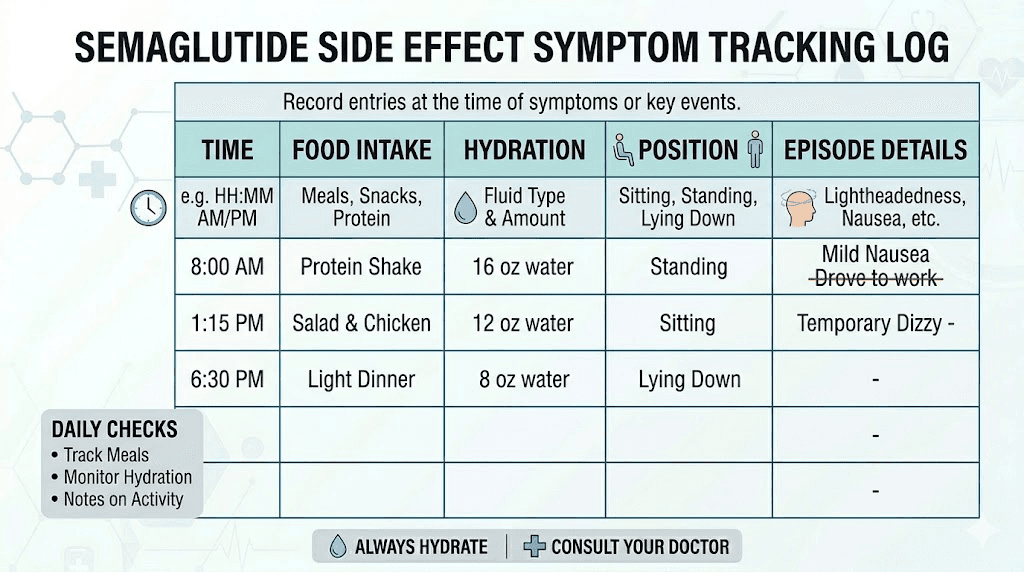
Tracking and monitoring your symptoms
A symptom log makes the difference between guessing at causes and identifying them definitively. Track the following for at least two weeks if lightheadedness is an issue.
Record what time of day episodes occur, what you ate in the preceding 4 hours, how much water you drank that day, whether the episode was positional (triggered by standing), and how long it lasted. Also note your semaglutide dose day, which day of the injection cycle you are on, and any other medications you took that day.
Patterns emerge quickly. You might discover that your lightheadedness always occurs on day 2 after injection, or always in the afternoon when you have skipped lunch, or always after taking your blood pressure medication in the morning. Once you identify the pattern, the solution becomes obvious.
Blood pressure monitoring at home can be particularly valuable. Take your blood pressure lying down, then immediately after standing. If the systolic (top number) drops by more than 20 mmHg or the diastolic drops by more than 10 mmHg upon standing, you have orthostatic hypotension and should discuss this with your provider.
The SeekPeptides platform provides tracking tools and symptom management protocols specifically designed for GLP-1 users, helping members identify patterns and optimize their experience with evidence-based adjustments.
Comparing lightheadedness across GLP-1 medications
Semaglutide is not the only GLP-1 receptor agonist that causes lightheadedness. Understanding how it compares to alternatives helps contextualize the side effect and may inform decisions about switching medications if lightheadedness proves unmanageable.
Semaglutide versus tirzepatide side effects differ in important ways. Tirzepatide, a dual GIP/GLP-1 agonist, carries a similar lightheadedness risk profile but may cause more GI side effects at higher doses, which indirectly increases dehydration risk. The full semaglutide versus tirzepatide comparison breaks down the differences across all side effect categories.
Oral semaglutide (Rybelsus) absorbs differently than injectable forms. The bioavailability is lower and the absorption curve is different, which can mean a different side effect profile. Some people who experience lightheadedness on injectable semaglutide find that oral semaglutide options are better tolerated, though the evidence on this is mostly anecdotal.
Switching from semaglutide to tirzepatide or vice versa is increasingly common. If lightheadedness is one reason for considering a switch, the switching protocols and conversion charts provide the dosing guidance needed for a smooth transition.
Special populations and additional risk factors
Older adults
People over 65 face higher risks from lightheadedness because their cardiovascular reflexes are slower to respond to positional changes, they typically take more concurrent medications, and falls carry more serious consequences including hip fractures and head injuries. Older adults using semaglutide should implement all prevention strategies proactively rather than waiting for symptoms to appear.
People with existing low blood pressure
If your baseline blood pressure is already on the low side (systolic below 100), semaglutide may push it lower enough to cause frequent lightheadedness. Discuss this with your provider before starting the medication. More frequent blood pressure monitoring, a more gradual dose escalation, and higher sodium intake may all be appropriate.
People with eating disorders or disordered eating patterns
The appetite suppression from semaglutide can enable extremely low caloric intake in susceptible individuals. When caloric intake drops below 800 calories per day, lightheadedness becomes almost guaranteed regardless of hydration or electrolyte status. If you find yourself consistently eating less than 1,000 calories per day while on semaglutide, this is both a lightheadedness risk factor and a broader health concern that needs to be addressed with your provider.
Pregnant or breastfeeding individuals
Semaglutide is not recommended during pregnancy or breastfeeding. However, some people discover pregnancy while on the medication or have questions about timing. For those navigating these situations, understanding how semaglutide affects menstrual cycles and reproductive health is important context.
Long-term management strategies
Most lightheadedness on semaglutide is a short-term adjustment issue. But some people deal with it on an ongoing basis, especially at higher doses or when multiple contributing factors are present. Long-term strategies differ from acute management.
Building sustainable habits
The hydration and nutrition strategies described above need to become automatic habits, not just responses to symptoms. This takes about 3 to 4 weeks of consistent practice. Set phone reminders for water intake. Meal prep protein-rich snacks for the week. Keep electrolyte packets in your bag, car, and desk. The goal is to create a system where prevention happens without you having to think about it.
Regular check-ins with your provider
Blood pressure, fasting blood sugar, and a basic metabolic panel should be checked at each dose escalation and every 3 months at a stable dose. These objective measurements catch drifting values before they cause symptoms. Many people are surprised to learn that their blood pressure has dropped significantly or that their potassium is borderline low, findings that explain ongoing lightheadedness and point to simple solutions.
For people managing their own compounded semaglutide, proper reconstitution technique and accurate unit-to-milligram conversions are critical for consistent dosing that minimizes side effect variability.
Knowing when to reduce the dose
Tolerating side effects is not a virtue. If lightheadedness significantly impacts your quality of life, interferes with work or driving, or creates fall risk, a lower dose may be the better path. Research shows that sustained use of semaglutide at a tolerable dose produces better outcomes than intermittent use at a dose that causes problems. The semaglutide plateau guide discusses how dose adjustments interact with weight loss trajectories.
The connection between lightheadedness and other semaglutide side effects
Lightheadedness rarely occurs in complete isolation. It clusters with other side effects that share the same underlying mechanisms, and understanding these connections helps you address multiple symptoms simultaneously.
Fatigue on semaglutide and lightheadedness often appear together. Both can stem from inadequate caloric intake, dehydration, or blood sugar instability. Addressing the lightheadedness through better nutrition and hydration frequently resolves the fatigue as well. The broader experience of GLP-1-related fatigue follows similar patterns across the medication class.
Headaches on GLP-1 medications are another common companion symptom. Dehydration causes headaches through the same mechanism that causes lightheadedness, namely reduced blood flow. A headache that arrives alongside lightheadedness is almost certainly dehydration-related until proven otherwise.
GI symptoms like nausea, constipation, and digestive disturbances create a vicious cycle with lightheadedness. Nausea reduces food and fluid intake, which causes dehydration, which causes lightheadedness, which causes more nausea. Breaking this cycle usually requires addressing the nausea first, either through dietary modifications, timing adjustments, or antiemetic support from your provider.
Energy changes on semaglutide are closely related to the blood sugar and caloric intake patterns that drive lightheadedness. When you stabilize blood sugar through consistent eating and address dehydration, both lightheadedness and energy levels tend to improve together.
Supplementation that may help
Beyond basic electrolyte replacement, certain supplements may support the body systems that lightheadedness involves.
B12: Semaglutide combined with B12 is an increasingly popular formulation because B12 supports energy metabolism and red blood cell production. B12 deficiency can cause lightheadedness independently, and reduced food intake on semaglutide may decrease dietary B12 absorption. A sublingual B12 supplement or a semaglutide-methylcobalamin compound addresses this directly.
Glycine: Semaglutide with glycine formulations are designed to reduce nausea, and since nausea drives dehydration which drives lightheadedness, reducing nausea upstream can help prevent lightheadedness downstream.
Iron: Rapid weight loss and reduced food intake can unmask or worsen iron deficiency, particularly in menstruating women. Iron deficiency anemia causes lightheadedness through reduced oxygen-carrying capacity of the blood. If your lightheadedness does not respond to hydration and electrolyte strategies, ask your provider to check a ferritin level.
For those researching the broader landscape of peptide-based weight management, understanding how different formulations and combinations affect side effect profiles helps inform better choices.
What the research says about semaglutide and cardiovascular effects
The cardiovascular profile of semaglutide is actually one of its strengths. The SELECT trial demonstrated cardiovascular benefits including reduced risk of major adverse cardiovascular events. However, the blood pressure-lowering effect that contributes to these benefits is the same effect that causes lightheadedness in some users.
A systematic review and meta-analysis of semaglutide studies in patients without diabetes found consistent blood pressure reductions. The magnitude of reduction correlated with degree of weight loss, meaning the more weight you lose, the more blood pressure drops. For people starting from a normal or already-low blood pressure baseline, this can push levels into a range where orthostatic symptoms occur.
This is an important nuance. The blood pressure reduction is not a malfunction. It is the medication working as intended. The lightheadedness is a side effect of a beneficial cardiovascular change, not a sign of something going wrong. Managing it through hydration, electrolytes, and positional awareness allows you to get the cardiovascular benefits without the functional impairment. Comparing phentermine versus semaglutide shows how different weight loss medications affect the cardiovascular system in very different ways.
Quick reference: the lightheadedness prevention protocol
For easy reference, here is the complete daily protocol for preventing lightheadedness on semaglutide:
Morning: 16 ounces of water with a pinch of salt immediately upon waking. Eat breakfast within 60 minutes even if not hungry, prioritizing protein and complex carbohydrates. Take blood pressure if monitoring.
Midday: Continue drinking 8 to 12 ounces of water every 90 minutes. Eat lunch or a substantial snack by early afternoon. Include one serving of electrolyte-enhanced water.
Afternoon: This is the highest-risk window for lightheadedness. If you tend to experience episodes in the afternoon, have a protein-rich snack between 2 and 4 PM. Continue hydration schedule. Avoid prolonged sitting followed by sudden standing.
Evening: Eat dinner with adequate protein. Continue hydration but taper in the last 2 hours before bed to avoid disrupting sleep. Take 200 to 400mg magnesium glycinate before bed.
Weekly: Time semaglutide injection for when you can rest the following day. Monitor blood pressure at least twice weekly during dose escalation. Track symptoms in a log to identify patterns.
Monthly: Review symptom log with provider. Request basic metabolic panel if lightheadedness persists. Adjust blood pressure medications as weight changes warrant.
For researchers who want the most comprehensive guidance, SeekPeptides offers complete protocol management tools, detailed side effect guides, and a community of experienced users who have navigated these exact challenges.
Frequently asked questions
Is lightheadedness a common side effect of semaglutide?
Yes. Clinical trials reported dizziness and lightheadedness in approximately 8% of patients. Real-world rates are likely higher because mild episodes often go unreported. It is one of the more common non-GI side effects and typically appears during the first few weeks or during dose escalation. Most episodes are mild and resolve with proper management strategies.
How long does lightheadedness from semaglutide last?
Individual episodes typically last 5 to 30 seconds if positional (triggered by standing up) or up to several hours if caused by sustained low blood sugar or dehydration. As a recurring symptom, most people find lightheadedness resolves within 2 to 4 weeks at a stable dose as the body adapts. Understanding how long semaglutide takes to work helps set timeline expectations.
Can lightheadedness on semaglutide be dangerous?
In most cases, no. However, severe episodes can lead to falls and injuries, which is a genuine safety concern especially for older adults. If lightheadedness is accompanied by confusion, slurred speech, chest pain, or actual fainting, seek medical attention. The primary danger is not from the lightheadedness itself but from what happens if you fall because of it.
Should I stop taking semaglutide if I feel lightheaded?
Do not stop without consulting your provider. Lightheadedness is usually manageable through hydration, nutrition, and lifestyle adjustments. Abruptly stopping semaglutide can cause withdrawal-like effects including appetite rebound. Talk to your provider about dose adjustment if prevention strategies are not resolving the issue.
Does lightheadedness get worse at higher doses?
It can, but it does not always. Higher doses produce more appetite suppression, which can lead to greater reductions in food and fluid intake. The appropriate dose level varies by individual. Some people tolerate 2.4mg without lightheadedness while others experience it at 0.5mg. The key variable is how well you compensate with hydration and nutrition at each dose level.
What should I eat immediately when I feel lightheaded on semaglutide?
A combination of fast-acting carbohydrates and protein works best. A glass of orange juice with a handful of nuts, crackers with cheese, or a banana with peanut butter will raise blood sugar quickly while the protein prevents a rebound crash. Avoid pure sugar sources like candy, which spike and crash blood sugar. The complete food guide for semaglutide has more options.
Can dehydration cause lightheadedness on semaglutide?
Absolutely. Dehydration is the single most common cause of lightheadedness on semaglutide. The medication reduces appetite, which reduces food intake, which reduces the 20% of daily water that comes from food. Combined with potential GI fluid losses, total hydration drops significantly. Aim for at least 80 ounces of water daily and include electrolytes.
Is feeling lightheaded on semaglutide the same as dizziness?
No. Lightheadedness is the sensation of feeling faint or woozy, usually triggered by standing and related to blood flow. Dizziness involves a spinning sensation (vertigo) related to the inner ear. The causes, treatments, and implications differ. If your room is spinning, read the semaglutide dizziness guide for vertigo-specific information.
External resources
Mayo Clinic - Semaglutide side effects and dosage information
PMC - Vestibular disorders with semaglutide and tirzepatide: real-world cohort study
Journal of Clinical Medicine - Semaglutide blood pressure effects meta-analysis
For researchers serious about optimizing their semaglutide experience, SeekPeptides offers the most comprehensive resource available, with evidence-based protocols, side effect management guides, and a community of thousands who have navigated these exact challenges.
In case I do not see you, good afternoon, good evening, and good night. May your blood sugar stay stable, your hydration stay consistent, and your balance stay steady.