Apr 2, 2026

Some new mothers lose the baby weight in weeks. Others fight it for years. The difference is not willpower, genetics, or some secret workout routine that Instagram influencers push between diaper brand sponsorships. The difference, more often than not, comes down to hormones, metabolic shifts, and the biological reality that pregnancy fundamentally rewires how your body stores and releases fat.
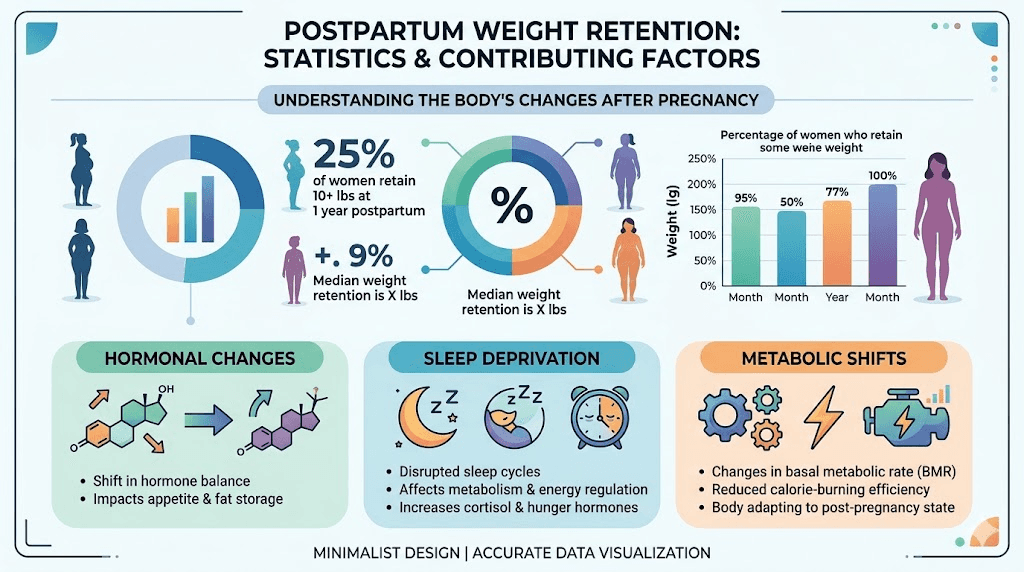
Here is a number that surprises most people. Between 50 and 75 percent of women weigh more than their pre-pregnancy weight a full twelve months after delivery. Half retain at least ten pounds. A quarter hold onto twenty or more. And only about 20 percent of new mothers return to their pre-pregnancy weight within the first three months, despite what social media recovery timelines suggest.
GLP-1 receptor agonists have changed the conversation.
Medications like semaglutide and tirzepatide are now among the most effective tools available for sustained weight loss, and prescriptions for postpartum women have surged dramatically, rising from 0.3 to 14.6 per 1,000 deliveries between 2019 and 2024. That is not a small increase. That is a fundamental shift in how clinicians approach postpartum weight management. But the questions new mothers ask are different from those of the general population. Can you take these medications while breastfeeding? How soon after delivery is it safe to start? Will it affect milk supply? What about recovery from a C-section? These are not hypothetical concerns. They are urgent, practical, deeply personal questions that deserve evidence-based answers rather than vague reassurances or fear-based warnings. This guide covers all of them, with specific timelines, dose protocols, safety data, and the practical realities of using GLP-1 medications while navigating the most demanding period of your life.
Why postpartum weight refuses to leave
The phrase "baby weight" makes it sound temporary. Cute, almost. Like something that arrived with the baby and will leave just as easily. But postpartum weight retention is a clinical phenomenon driven by overlapping biological mechanisms that actively resist weight loss, and understanding why it happens is the first step toward addressing it effectively.
Pregnancy increases your body fat stores deliberately. This is not a flaw. It is a survival mechanism designed to ensure adequate energy reserves for breastfeeding and recovery. Your body deposits fat in the hips, thighs, abdomen, and back during the second and third trimesters, driven by rising progesterone and estrogen levels that signal your metabolism to prioritize storage over expenditure.
After delivery, those hormones crash. Dramatically.
Estrogen and progesterone plummet within 24 to 48 hours of giving birth, creating a hormonal environment that many researchers compare to surgical menopause. This sudden shift affects mood, energy, sleep quality, and, critically, metabolic rate. Your thyroid function may slow temporarily. Cortisol levels often remain elevated for months, particularly if you are dealing with sleep deprivation, which virtually every new parent experiences. And elevated cortisol does one thing exceptionally well: it tells your body to hold onto abdominal fat.
Sleep deprivation alone can stall weight loss completely. When you sleep fewer than six hours per night, which is standard for most new parents during the first several months, your body produces more ghrelin (the hunger hormone) and less leptin (the satiety hormone). You feel hungrier. You crave calorie-dense foods. Your willpower tanks because your prefrontal cortex is running on fumes. This is not a character failure. It is biochemistry working exactly as designed under conditions of sleep stress. Research on peptides for hormone balance explores how these systems interact and how targeted interventions can help restore equilibrium.
Then there is the practical reality of caring for a newborn. Meal prep becomes aspirational. Exercise requires childcare arrangements, physical clearance from your provider, and energy you may not have. Many mothers default to convenience foods, eating whatever is fastest between feedings and diaper changes. The metabolic deck is stacked, and the lifestyle deck is stacked on top of it.
Breastfeeding does burn extra calories, typically between 300 and 500 per day. But it also increases hunger signals to compensate, and many women find that breastfeeding either has no effect on weight loss or actually makes it harder because the hunger it triggers exceeds the calories it burns. The notion that breastfeeding "melts the pounds away" is true for some women and completely false for others. If you fall into the second category, that does not mean you are doing something wrong. It means your body is prioritizing milk production over fat mobilization, which is, from an evolutionary perspective, exactly what it should be doing.
What GLP-1 medications do differently
Most weight loss approaches fight against your biology. Calorie restriction triggers hunger hormones. Exercise increases appetite. Willpower depletes under stress. GLP-1 receptor agonists work with your biology instead, targeting the specific hormonal pathways that regulate appetite, satiety, and metabolic function.
GLP-1 stands for glucagon-like peptide-1. It is a hormone your gut naturally produces after eating, and it does several things simultaneously. It signals your brain that you are full. It slows gastric emptying so food stays in your stomach longer. It improves insulin sensitivity so your body processes glucose more efficiently. And it reduces the reward response to food, meaning you do not just eat less, you actually want to eat less.
That last point matters enormously for postpartum women.
When you are exhausted, stressed, and hormonally disrupted, food becomes one of the few available sources of comfort and quick energy. GLP-1 medications reduce that compulsive pull toward food without eliminating the pleasure of eating entirely. You still enjoy meals. You simply stop thinking about food constantly, stop reaching for snacks out of exhaustion-driven habit, and find it easier to make nutritional choices that support your recovery rather than undermine it. The appetite suppression mechanism works through both central nervous system pathways and peripheral gut signaling, creating a comprehensive effect that diet alone cannot replicate.
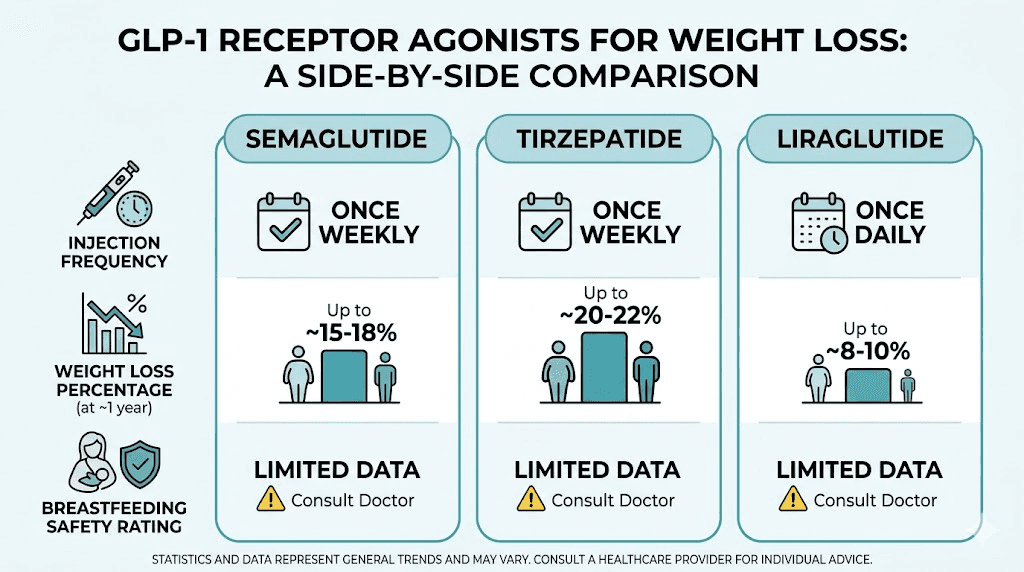
The current GLP-1 medications available include semaglutide (brand names Ozempic and Wegovy), tirzepatide (Mounjaro and Zepbound), and liraglutide (Saxenda). Each works slightly differently. Semaglutide targets the GLP-1 receptor exclusively. Tirzepatide targets both GLP-1 and GIP receptors, which is why it often produces greater average weight loss per month. Liraglutide was the first to market and requires daily injections rather than weekly ones, but it has the longest safety track record and some specific postpartum research that the newer medications lack.
For postpartum women specifically, these medications address the exact mechanisms that make baby weight so stubborn. They counteract elevated ghrelin. They reduce cortisol-driven cravings. They improve insulin sensitivity that pregnancy may have disrupted. And they do all of this without requiring the extreme calorie restriction that would compromise milk supply or recovery. You can learn more about the differences in the SeekPeptides semaglutide versus tirzepatide comparison.
When you can safely start GLP-1 after giving birth
Timing matters. Starting too early introduces unnecessary risk during a vulnerable recovery period. Waiting too long can mean losing the motivational window when many new mothers feel most ready to act. The general clinical consensus falls within a specific range, though individual circumstances can shift that window in either direction.
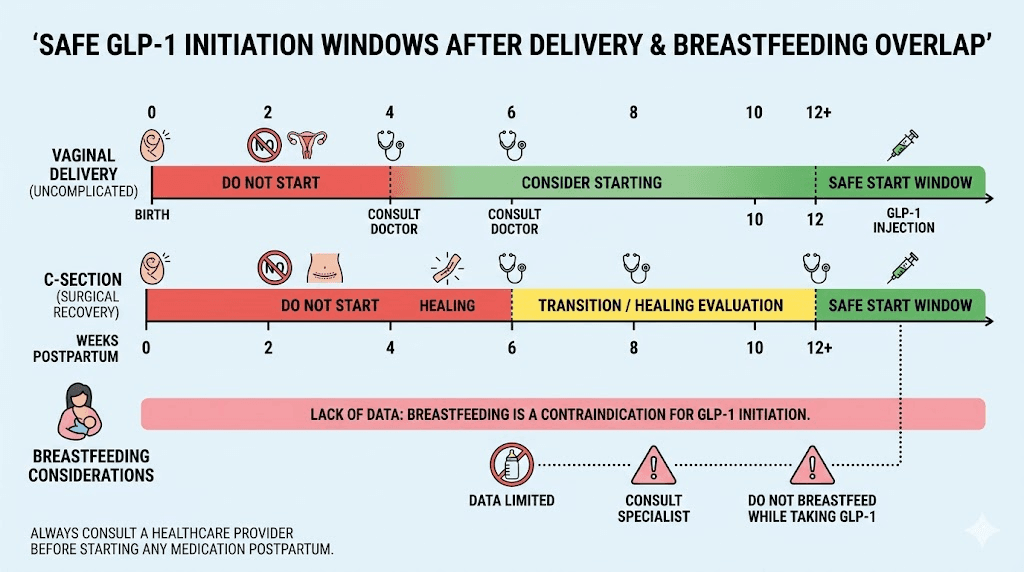
The minimum recommended waiting period is six weeks postpartum. This applies to uncomplicated vaginal deliveries where recovery is progressing normally, bleeding has stopped, and your provider has cleared you at your postpartum checkup. Six weeks allows initial hormonal stabilization, uterine involution, and basic wound healing to complete.
Most clinicians prefer waiting eight to twelve weeks.
This longer window accounts for the fact that postpartum recovery is not linear. You may feel physically recovered at six weeks but still be dealing with significant hormonal fluctuation, disrupted sleep patterns, and the caloric demands of establishing breastfeeding. Starting a medication that suppresses appetite and slows gastric emptying during this adjustment period can create complications that are easily avoided by waiting a few more weeks. If you had a straightforward delivery with no injection complications, the shorter end of this range may be appropriate.
C-section recovery extends the timeline. If you delivered via cesarean, your body is healing from major abdominal surgery. The incision site needs adequate nutrition and blood flow to heal properly. GLP-1 medications can reduce food intake significantly, and caloric restriction during surgical recovery increases infection risk, slows wound healing, and can delay the return to normal physical function. Most providers recommend waiting a full twelve weeks after a C-section, and some prefer sixteen weeks, before introducing any appetite-suppressing medication.
The three-month sweet spot
Three months postpartum represents what many providers consider the ideal starting point for several reasons. By twelve weeks, your body has completed the most dramatic hormonal shifts. If you are breastfeeding, your supply is typically well established and less vulnerable to disruption. You have had time to identify whether your weight is trending downward naturally or has plateaued. And you have enough data about your postpartum baseline, including energy levels, mood stability, and sleep patterns, to make an informed decision about adding a new medication.
Starting at three months also gives your provider time to screen for postpartum thyroid dysfunction, which affects up to 10 percent of new mothers and can cause weight retention that GLP-1 medications will not fully address. If your thyroid is the primary driver, treating that first will be more effective than layering a GLP-1 on top of an undiagnosed condition.
Factors that extend the waiting period
Several situations warrant waiting longer than the standard timeline:
Postpartum hemorrhage or significant blood loss during delivery
Preeclampsia or pregnancy-induced hypertension that has not fully resolved
Active postpartum depression or anxiety that is not yet stabilized with treatment
Difficulty establishing breastfeeding or low milk supply concerns
Ongoing wound complications from C-section or perineal repair
History of eating disorders, which GLP-1 appetite suppression could trigger
Significant nutritional deficiencies identified in postpartum blood work, particularly iron deficiency anemia
The American College of Obstetricians and Gynecologists has not yet issued specific guidelines on postpartum GLP-1 use, which means decisions are being made on a case-by-case basis between patients and their providers. This is not a gap in medical knowledge so much as a reflection of how rapidly GLP-1 adoption has outpaced formal guideline development. Your provider should be your primary decision-maker here, informed by the data we will cover throughout this guide.
GLP-1 and breastfeeding: what the research actually shows
This is the question that keeps new mothers up at night, right alongside the baby. Can you take GLP-1 medications while breastfeeding? The answer is more nuanced than a simple yes or no, and it depends heavily on which specific medication and formulation you are considering.
The most significant data point comes from research on semaglutide excretion in breast milk. Injectable semaglutide was not detectable in breast milk at clinically meaningful levels in the available studies. The maximum relative infant dose, or RID, was projected at 1.26 percent. For context, the accepted safety threshold for medication in breast milk is 10 percent RID. Semaglutide falls well below that line, which is reassuring, though researchers note that more data from larger populations would strengthen this conclusion.
There is an important distinction here. Only injectable semaglutide has this data.
Oral semaglutide contains an absorption enhancer called salcaprozate sodium, which helps the peptide survive the digestive tract and reach the bloodstream. This enhancer may enter breast milk, and its effects on infant gut development are unknown. For this reason, oral semaglutide formulations are generally not recommended during breastfeeding. If you are nursing and considering semaglutide, the injectable form is the appropriate choice.
What about tirzepatide?
Tirzepatide has less breast milk excretion data than semaglutide. The manufacturer advises against use during breastfeeding due to insufficient human data, though animal studies have not shown concerning levels of transfer. This does not mean tirzepatide is dangerous during breastfeeding. It means we do not have enough human data to confirm safety with the same confidence as injectable semaglutide. Our detailed guide on tirzepatide while breastfeeding covers the available evidence in full.
Some clinicians are prescribing tirzepatide to breastfeeding mothers based on its molecular similarity to GLP-1, its large molecular weight (which reduces breast milk transfer), and the favorable animal data. Others prefer to wait until breastfeeding concludes or switch patients to semaglutide, which has slightly more human lactation data. Both approaches are reasonable given current evidence.
Calorie and hydration concerns during breastfeeding
Beyond the direct medication transfer question, there is a practical concern about caloric intake. Breastfeeding demands an additional 300 to 500 calories per day above your baseline needs. GLP-1 medications suppress appetite, sometimes significantly, particularly during the first few weeks of treatment and after dose increases. If appetite suppression leads to caloric intake that falls below what breastfeeding requires, you may experience reduced milk supply, fatigue beyond what is normal postpartum, and nutritional deficiencies that affect both you and your baby.
This is manageable. But it requires attention.
The approach most providers recommend involves tracking caloric intake during the first several weeks on medication, ensuring a minimum of 1,800 calories daily while breastfeeding (some women need more depending on supply demands and body size), and prioritizing protein and nutrient-dense foods over empty calories. You can explore specific meal planning strategies in our calorie guide for semaglutide or our tirzepatide calorie guide.
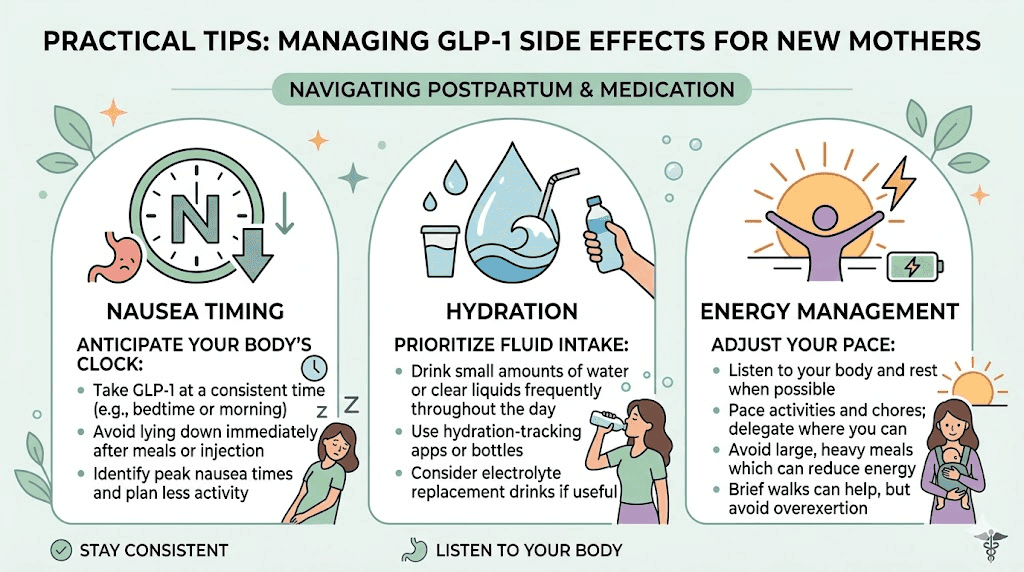
Hydration is equally critical. GLP-1 medications can cause gastrointestinal side effects including nausea, constipation, and reduced fluid intake simply because you are eating and drinking less. Breastfeeding already increases fluid requirements substantially. The combination of decreased oral intake from GLP-1 effects and increased fluid demand from lactation can lead to dehydration faster than you might expect. Aim for a minimum of 80 to 100 ounces of water daily, and monitor for signs of dehydration including dark urine, headache, dizziness, and decreased milk output.
Choosing the right GLP-1 for postpartum weight loss
Not all GLP-1 medications are created equal, and the best choice for a postpartum woman may differ from what works best for the general population. Here is how the three main options compare when viewed through the specific lens of new motherhood.
Semaglutide (Ozempic, Wegovy)
Semaglutide is the most studied GLP-1 receptor agonist overall and has the most breast milk data specifically. It targets the GLP-1 receptor exclusively, producing average weight loss of 15 to 17 percent of body weight over 68 weeks in clinical trials. The weekly injection schedule is convenient for busy new mothers, and the side effect profile is well characterized after years of widespread use.
For postpartum women, semaglutide offers several advantages. The breast milk data showing sub-threshold RID levels provides a degree of reassurance that other GLP-1 medications cannot yet match. The titration schedule is gradual, starting at 0.25 mg weekly and increasing over 16 to 20 weeks, which allows your body to adjust slowly while you are also adjusting to life with a newborn. And the extensive real-world data means your provider has a large evidence base to draw from when managing your treatment. Check the semaglutide dosage calculator for precise dosing based on your starting weight.
Potential downsides include a slower onset of significant weight loss compared to tirzepatide and gastrointestinal side effects, particularly nausea during the first month, that can be challenging when you are already dealing with fatigue and disrupted eating patterns.
Tirzepatide (Mounjaro, Zepbound)
Tirzepatide targets both GLP-1 and GIP receptors, producing greater average weight loss than semaglutide in head-to-head trials, typically 20 to 25 percent of body weight. For women with significant postpartum weight retention, say 30 or more pounds above pre-pregnancy weight, this stronger effect may be appealing. The side effect comparison between the two medications shows some differences worth considering.
The dual receptor mechanism also provides better blood sugar regulation, which is particularly relevant if you developed gestational diabetes, as we will discuss in a later section. Some research suggests tirzepatide may better preserve lean muscle mass during weight loss compared to GLP-1-only agonists, and muscle preservation is important postpartum when your body is already recovering and rebuilding.
The downsides for postpartum use specifically are the limited breast milk data and a side effect profile that some women find more intense during the initial titration period. Bloating and constipation are common early complaints that can add to the gastrointestinal changes many women already experience postpartum.
Liraglutide (Saxenda)
Liraglutide is the oldest GLP-1 medication and requires daily injection rather than weekly, which is less convenient but offers one significant advantage: there is a specific clinical trial studying its use in postpartum women. The study examined 153 women with prior gestational diabetes who received liraglutide 1.8 mg daily plus metformin over 84 weeks. The results showed superior weight loss and glycemic control compared to metformin alone.
This postpartum-specific data is unique among GLP-1 medications. While the overall weight loss with liraglutide is more modest than semaglutide or tirzepatide (typically 8 to 10 percent of body weight), the direct evidence in the postpartum population gives it a clinical credibility that newer medications are still building. The differences between semaglutide and liraglutide extend beyond efficacy to include injection frequency, side effect patterns, and cost considerations.
Quick comparison table
Factor | Semaglutide | Tirzepatide | Liraglutide |
|---|---|---|---|
Injection frequency | Weekly | Weekly | Daily |
Average weight loss | 15-17% | 20-25% | 8-10% |
Breast milk data | RID 1.26% (injectable) | Limited human data | Limited data |
Postpartum-specific study | No | No | Yes (with metformin) |
GI side effects | Moderate | Moderate to high initially | Moderate |
Muscle preservation | Standard | Potentially better | Standard |
Best postpartum candidate | Breastfeeding mothers, moderate weight retention | Non-breastfeeding or done breastfeeding, significant weight retention | Prior gestational diabetes, prefer proven postpartum data |
Your provider can help determine which option fits your specific situation. The full three-way comparison including retatrutide provides additional context for understanding where these medications fall in the broader landscape of metabolic therapeutics.
Starting doses and titration schedules
Postpartum titration is not identical to standard titration. Your body is recovering. Your nutritional demands are elevated. Your sleep is disrupted. And if you are breastfeeding, you have an additional metabolic load that must be accounted for. The general principle is simple: start lower and go slower than standard protocols suggest.
Semaglutide postpartum titration
The standard semaglutide titration begins at 0.25 mg weekly for four weeks, then increases to 0.5 mg. For postpartum women, many providers extend the 0.25 mg phase to six or even eight weeks, particularly if the patient is breastfeeding. This allows time to confirm that the lower dose does not reduce milk supply, cause problematic nausea, or interfere with adequate caloric intake.
A conservative postpartum schedule looks like this:
Weeks 1 through 8: 0.25 mg weekly
Weeks 9 through 16: 0.5 mg weekly
Weeks 17 through 24: 1.0 mg weekly
Weeks 25 and beyond: 1.7 mg weekly (if needed, some women find 1.0 mg sufficient)
Maximum dose: 2.4 mg weekly (Wegovy formulation)
The key difference from standard protocols is patience. You are not racing to the maintenance dose. You are finding the minimum effective dose that produces steady, sustainable weight loss without compromising your recovery or your ability to care for your baby. Use the semaglutide dosage in units guide if you are working with compounded formulations that use unit measurements rather than milligrams.
For information on optimal injection technique, our guide on the best injection site for semaglutide and how to give the injection with a syringe walk through the process step by step. The best time of day to inject can also affect how side effects overlap with your daily routine.
Tirzepatide postpartum titration
Tirzepatide starts at 2.5 mg weekly for the standard population. The same starting dose applies postpartum, but the duration at each level typically extends:
Weeks 1 through 8: 2.5 mg weekly
Weeks 9 through 16: 5 mg weekly
Weeks 17 through 24: 7.5 mg weekly
Weeks 25 and beyond: 10 mg weekly (if needed)
Maximum dose: 15 mg weekly
Many postpartum women find that 5 mg or 7.5 mg is their effective maintenance dose and do not need to escalate to 10 or 15 mg. If you are losing one to two pounds per week at a lower dose, there is no clinical reason to increase. You can reference the tirzepatide dosage in units guide and the compounded tirzepatide starting dose resource for compounded formulation specifics. Timing your injection can reduce side effect overlap with infant care, and the best time to take your tirzepatide shot guide explains why.
Signs you are escalating too fast
Watch for these indicators that your dose is advancing too quickly for your postpartum body:
Persistent nausea lasting more than three days after a dose increase
Inability to consume at least 1,500 calories daily (1,800 or more if breastfeeding)
Noticeable drop in breast milk supply
Fatigue significantly worse than your postpartum baseline
Weight loss exceeding three pounds per week consistently
Dizziness or lightheadedness, especially when standing
If any of these occur, the standard recommendation is to hold at your current dose for an additional four weeks before attempting another increase. Dropping back to the previous dose is also reasonable. Our guide on semaglutide dizziness covers how to manage this specific side effect in detail.
Managing GLP-1 side effects while caring for a newborn
Side effects happen. They are generally manageable and typically improve over time. But managing them while simultaneously caring for an infant requires specific strategies that generic side effect guides do not cover.
Nausea: the most common challenge
Nausea affects 40 to 50 percent of people starting GLP-1 medications, and it tends to peak during the first two weeks at each new dose level. For postpartum women, this is complicated by the fact that nausea can overlap with sleep deprivation effects, hormonal fluctuation, and the general physical demands of new parenthood.
Timing your injection strategically can help. Many postpartum women find that injecting on a Friday evening works well because it puts the peak nausea window (24 to 72 hours post-injection) during the weekend when a partner or family member may be more available to help with the baby. If you do not have weekend support, choose whatever day gives you the most backup during the 48 hours following your injection.
Eat before injecting. Not after.
A small protein-rich meal 30 to 60 minutes before your injection can significantly reduce nausea compared to injecting on an empty stomach. Think a handful of nuts, a hard-boiled egg, or a small portion of chicken with crackers. Bland foods work better than spicy or fatty ones during the first few weeks. Our GLP-1 breakfast ideas and GLP-1 recipe collection include options that are both nausea-friendly and nutritionally adequate for postpartum recovery.
Ginger tea, vitamin B6, and small frequent meals all help. If nausea is severe enough to interfere with eating or caring for your baby, contact your provider. Prescription anti-nausea medications compatible with breastfeeding do exist, and there is no reason to suffer through severe nausea when safe treatments are available.
Constipation: a compounding problem
Postpartum constipation is already common. Slowed gastric motility from GLP-1 medications can make it significantly worse. The combination of hormonal changes, reduced physical activity, potential iron supplementation, and GLP-1-related slowed digestion creates a perfect storm for gastrointestinal discomfort. Our detailed guides on GLP-1 constipation relief and semaglutide-specific constipation treatment provide comprehensive approaches.
Prevention is easier than treatment. Start a fiber supplement before or at the same time you begin GLP-1 medication, not after constipation develops. The best fiber supplement for GLP-1 users guide compares options. Magnesium citrate at 200 to 400 mg daily can also help, and it supports postpartum recovery in its own right. Stay well hydrated, as dehydration is the fastest path to constipation on these medications.
Fatigue: separating medication effects from postpartum exhaustion
Every new parent is tired. GLP-1 medications can add to that tiredness, particularly during the first few weeks and after dose increases. The GLP-1 fatigue guide covers the mechanisms in detail, but the short version is this: reduced caloric intake lowers available energy, metabolic changes take time to normalize, and some degree of fatigue is an expected adjustment effect.
Distinguishing GLP-1 fatigue from postpartum fatigue can be difficult. One useful test is timing. If fatigue worsens specifically in the 24 to 72 hours after your injection and then improves, it is likely medication-related. If it is constant and unrelated to injection timing, it is more likely the baseline exhaustion of new parenthood. For a more thorough exploration, the semaglutide fatigue and tirzepatide fatigue guides offer medication-specific strategies.
Other side effects to monitor
Headaches affect roughly 15 to 20 percent of GLP-1 users and are often linked to dehydration or blood sugar fluctuations. Bloating typically resolves within the first month at each dose level. Hair loss can occur with rapid weight loss and is worth monitoring, as postpartum hair shedding is already a common concern around three to six months after delivery. If you notice increased hair loss beyond normal postpartum shedding, slow your rate of weight loss by holding your current dose rather than increasing. The GLP-1 vitamin guide covers nutritional strategies to support hair health during treatment.
Nutrition requirements on GLP-1 postpartum
This section is non-negotiable. You cannot cut corners on postpartum nutrition, GLP-1 medication or not. Your body is recovering from pregnancy. It may be producing milk for a growing infant. It is rebuilding muscle, replenishing iron stores, and supporting a brain that is forming entirely new neural pathways around caregiving. Adequate nutrition during this period is not about weight loss optimization. It is about fundamental health.
Calorie minimums
Non-breastfeeding postpartum women on GLP-1 medications should aim for a minimum of 1,500 calories daily. This provides sufficient energy for recovery while allowing the medication to create a modest caloric deficit. Going below 1,500 risks nutrient deficiency, excessive fatigue, and metabolic adaptation that will ultimately slow weight loss.
Breastfeeding women need more. Aim for 1,800 to 2,200 calories daily depending on your body size and milk production demands. If you are exclusively breastfeeding a larger or older infant who is consuming more milk, your needs are at the higher end of this range. The semaglutide calorie guide provides formulas for calculating your specific target.
GLP-1 medications can make hitting these minimums difficult, especially at higher doses. You may not feel hungry. You may feel full after a few bites. This is where intentional eating becomes important, treating meals as scheduled events rather than hunger-driven impulses. Small, nutrient-dense meals every three to four hours often work better than trying to eat three large meals when your appetite is suppressed.
Protein: the critical macronutrient
Protein is the most important macronutrient during postpartum GLP-1 treatment. It supports muscle preservation during weight loss. It supports tissue repair from delivery. It provides the amino acid building blocks for breast milk production. And it helps maintain satiety between meals, working with rather than against the GLP-1 medication mechanism.
Target a minimum of 100 grams of protein daily. If you are breastfeeding, aim for 120 to 140 grams. This sounds like a lot, and on a suppressed appetite, it can be challenging. SeekPeptides members access detailed nutritional protocols designed for exactly this situation. The protein guide for semaglutide includes strategies for increasing protein intake when you do not feel like eating, and protein shakes formulated for GLP-1 users can fill gaps when solid food feels unappealing.
Prioritize protein at every meal. Eat protein first, before vegetables or carbohydrates, since GLP-1 medications may cause you to stop eating before you finish. If protein goes in last, it is the most likely to be left on the plate. Easy high-protein options that work well postpartum include Greek yogurt, rotisserie chicken, eggs, cottage cheese, protein shakes, and canned fish. The best foods to eat on semaglutide and what to eat on tirzepatide guides provide comprehensive food lists.
Micronutrients that postpartum GLP-1 users need
Several micronutrients deserve specific attention:
Iron. Postpartum iron depletion is common, and reduced food intake on GLP-1 can worsen it. Have your levels checked at your postpartum visit and supplement if needed. Symptoms of iron deficiency, including fatigue, brain fog, and cold extremities, can overlap with GLP-1 side effects and postpartum symptoms, making it easy to miss.
Vitamin D. Pregnancy depletes vitamin D stores, and most postpartum women are deficient. Supplementing 2,000 to 4,000 IU daily is generally recommended. The GLP-1 vitamin guide includes vitamin D alongside other key nutrients.
B12. Essential for energy metabolism and neurological function. GLP-1 medications can reduce B12 absorption over time, and postpartum demands are already high. The semaglutide with B12 guide and tirzepatide with B12 guide cover supplementation protocols.
Omega-3 fatty acids. Critical for both postpartum brain health and infant neurological development through breast milk. Continue your prenatal DHA supplement or switch to a postnatal formulation.
Electrolytes. Reduced food and fluid intake on GLP-1 medications can cause electrolyte imbalances, manifesting as muscle cramps, headaches, or irregular heartbeat. The best electrolytes for GLP-1 users guide covers which formulations work best. A good probiotic also supports gut health during GLP-1 treatment, and the best probiotic for semaglutide guide compares options.
Foods to focus on and foods to avoid
When appetite is limited, every bite matters. Focus on nutrient-dense options: lean proteins, eggs, leafy greens, berries, sweet potatoes, avocados, nuts, and whole grains. These deliver maximum nutritional value per calorie, which is exactly what you need when total intake is reduced. Detailed food lists are available in the semaglutide food list and semaglutide diet plan.
Avoid highly processed foods, excessive sugar, fried foods, and alcohol. These waste limited stomach capacity on empty calories and can worsen GLP-1 side effects. Carbonated beverages can increase bloating. Spicy and very fatty foods tend to trigger nausea more than bland alternatives, particularly in the first few weeks. The foods to avoid on semaglutide and tirzepatide foods to avoid guides provide complete lists with explanations.
Exercise and recovery on GLP-1 after pregnancy
Exercise after pregnancy is not about burning calories. Not at first. It is about rebuilding the structural integrity of a body that just spent nine months adapting to grow and deliver a human being. Jumping into intense workouts too soon does not accelerate weight loss. It risks injury, pelvic floor dysfunction, and setbacks that can delay your overall recovery by months.
Pelvic floor first, always
Before any other exercise, address your pelvic floor. Pregnancy and delivery (both vaginal and cesarean) affect the pelvic floor muscles, and these muscles must be rehabilitated before you load them with exercise. Symptoms of pelvic floor dysfunction include urinary leakage during activity, pelvic pressure or heaviness, pain during exercise, and difficulty controlling bladder or bowel function.
A pelvic floor physical therapist can assess your specific situation and provide targeted exercises. This is not a luxury. It is a clinical recommendation that prevents long-term complications. Many providers will not clear patients for exercise beyond walking until a pelvic floor assessment has been completed.
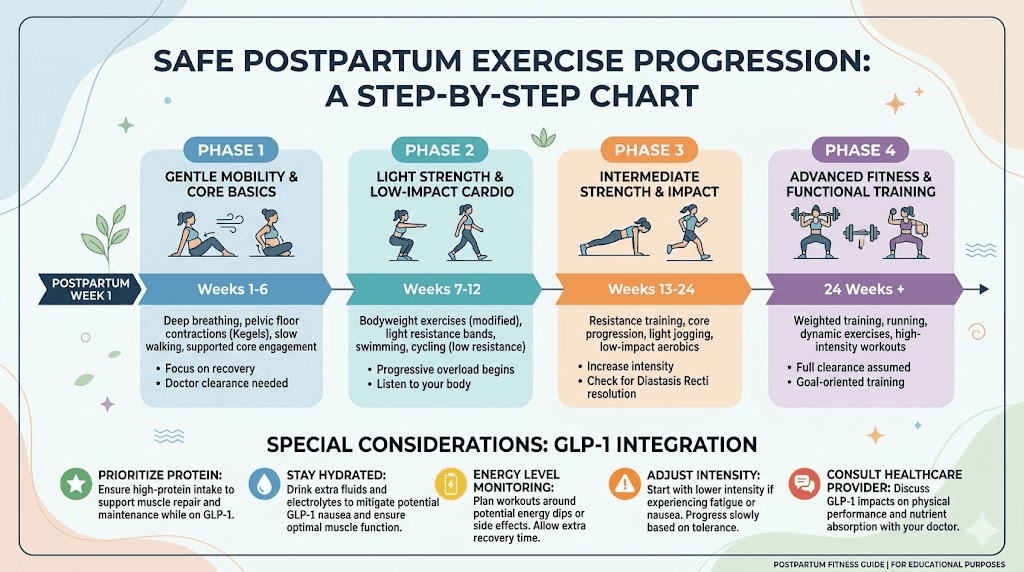
The postpartum exercise progression
Weeks 1 through 6 after delivery should focus exclusively on gentle walking and pelvic floor exercises. This applies regardless of how fit you were before or during pregnancy. Your body needs this time.
Weeks 6 through 12, after provider clearance, you can gradually introduce low-impact activities: longer walks, stationary cycling, swimming (once cleared), light resistance training with body weight, and gentle yoga. This is also the period when many women start GLP-1 medication, so you are adjusting to two new things simultaneously. Go slowly.
Weeks 12 through 24 allow for progressive loading: increasing resistance in strength training, adding moderate-intensity cardio, and returning to pre-pregnancy activities as tolerated. The muscle building on GLP-1 guide covers how to approach resistance training while on these medications, and creatine supplementation during GLP-1 treatment can support muscle recovery and performance.
After 24 weeks, most women can return to full pre-pregnancy exercise intensity, provided pelvic floor function is adequate and there are no ongoing complications.
Exercise and GLP-1 considerations
GLP-1 medications reduce caloric intake, which means you have less fuel available for exercise. High-intensity workouts on a suppressed appetite can cause hypoglycemia, excessive fatigue, and dizziness. The guide to weight loss on semaglutide without exercise demonstrates that exercise is not strictly necessary for weight loss on these medications, which takes the pressure off during the early postpartum months.
That said, exercise provides benefits beyond calorie burning. It improves mood, which matters enormously postpartum. It builds and preserves muscle mass, which GLP-1-related weight loss can compromise. It strengthens bones, supports cardiovascular health, and improves sleep quality. The goal is to find a sustainable activity level that supports your overall health without exceeding your recovery capacity.
Resistance training deserves particular emphasis. Weight loss on GLP-1 medications includes some lean muscle loss alongside fat loss. Resistance training minimizes this muscle loss, preserves metabolic rate, and builds functional strength for carrying, lifting, and caring for a growing child. Even two sessions per week of moderate resistance training can make a meaningful difference in body composition outcomes. Combining resistance training with adequate protein and the right supplements, as outlined in the supplement guide for GLP-1 users, maximizes muscle preservation.
The gestational diabetes connection
If you had gestational diabetes during pregnancy, GLP-1 medications offer a dual benefit that goes beyond weight loss. Gestational diabetes does not simply disappear after delivery. It signals an underlying metabolic vulnerability that significantly increases your risk of developing type 2 diabetes later in life. Up to 50 percent of women with gestational diabetes develop type 2 diabetes within 10 years, and the risk increases with retained postpartum weight.
This is where the liraglutide study becomes particularly relevant.
A clinical trial of 153 women with prior gestational diabetes compared liraglutide 1.8 mg daily plus metformin against metformin alone over 84 weeks. The liraglutide group showed superior outcomes on both fronts: greater weight loss and better glycemic control. This matters because it demonstrates that GLP-1 medications can address both the weight retention and the metabolic dysfunction that gestational diabetes leaves behind, potentially interrupting the progression to type 2 diabetes before it starts.
Semaglutide and tirzepatide do not have equivalent postpartum studies yet, but their mechanisms are similar enough that the principles likely apply. Tirzepatide, with its dual GIP/GLP-1 action, may offer even stronger glycemic benefits, though this remains to be confirmed in a postpartum-specific population. If you had gestational diabetes, ask your provider about starting GLP-1 therapy as part of a broader type 2 diabetes prevention strategy, not just a weight loss plan. The combination of metformin with semaglutide or metformin with tirzepatide may offer the most comprehensive approach for former gestational diabetes patients.
Monitoring blood glucose is important during postpartum GLP-1 treatment, particularly if you had gestational diabetes. Even though GLP-1 medications improve blood sugar regulation, the reduced caloric intake they produce can occasionally cause blood sugar to drop too low, especially if you are also taking metformin. Symptoms include shakiness, sweating, confusion, and irritability, which can be difficult to distinguish from severe sleep deprivation. The GLP-1 monitoring tools guide and injection tracking guide cover practical approaches to keeping tabs on your treatment.
Natural approaches that complement GLP-1 therapy
GLP-1 medications work best as part of a comprehensive approach, not in isolation. Several evidence-based strategies complement the medication effects and can improve both weight loss outcomes and overall postpartum recovery.
Protein optimization
We covered protein targets in the nutrition section, but it deserves reinforcement here. High protein intake is the single most impactful dietary strategy alongside GLP-1 medication. It preserves muscle. It supports satiety. It provides the building blocks for recovery. Research consistently shows that people who prioritize protein on GLP-1 medications lose more fat and less muscle than those who do not. Our semaglutide diet plan and tirzepatide diet plan both place protein at the center of the nutritional framework.
Fiber for gut health and satiety
Fiber serves multiple functions during postpartum GLP-1 treatment. It feeds beneficial gut bacteria, supports regular bowel movements (counteracting GLP-1 constipation effects), and extends satiety between meals. Aim for 25 to 35 grams daily from food sources like vegetables, fruits, legumes, and whole grains, supplemented as needed. The fiber supplement guide covers options that work well alongside GLP-1 medications.
Sleep optimization
"Optimize sleep with a newborn" sounds like a joke. It is not. You cannot control total sleep duration in the early months, but you can optimize sleep quality during the windows you have.
Darken your bedroom completely. Use white noise to mask sounds between feedings. Sleep when the baby sleeps, at least some of the time. Accept help from partners, family, or friends for nighttime feedings when possible, particularly on the nights following your GLP-1 injection when medication side effects may compound sleep disruption. If you are breastfeeding, consider pumping a bottle so someone else can handle one nighttime feeding, giving you a longer uninterrupted stretch.
Even an extra 30 to 60 minutes of consolidated sleep can measurably improve cortisol regulation, hunger hormone balance, and insulin sensitivity. These improvements work synergistically with GLP-1 medication effects.
Stress management
Chronic stress elevates cortisol, which promotes abdominal fat storage and increases appetite for high-calorie comfort foods. GLP-1 medications reduce the appetite component, but cortisol still promotes fat storage independent of caloric intake. Brief stress-reduction practices, even five minutes of deep breathing, a short walk outside, or a few minutes of mindfulness, can meaningfully reduce cortisol levels.
The postpartum period is inherently stressful. The goal is not to eliminate stress but to create small pockets of recovery throughout the day. These micro-recoveries add up and support both weight loss and emotional wellbeing.
Supplements that support GLP-1 therapy
Beyond the essential micronutrients discussed earlier, several supplements have evidence supporting their use alongside GLP-1 medications. Creatine combined with semaglutide supports muscle preservation during weight loss. Glycine supplementation may support sleep quality and joint recovery. Niacinamide with semaglutide and niacinamide with tirzepatide support skin health during rapid weight changes. Collagen peptides during and after pregnancy may support tissue recovery and skin elasticity. A comprehensive overview is available in the tirzepatide supplement guide.
When GLP-1 medications might not be right for you postpartum
GLP-1 medications are powerful tools. They are not universal solutions. Several postpartum situations warrant either delaying treatment or choosing a different approach entirely.
Active postpartum depression or anxiety
Postpartum mood disorders affect up to 20 percent of new mothers. If you are currently experiencing postpartum depression or anxiety that is not yet stabilized with treatment, adding a new medication that affects appetite, energy, and gastrointestinal function can complicate the clinical picture. Some women report mood changes on GLP-1 medications, and separating medication effects from postpartum mood symptoms is difficult when both are active and unstabilized.
Stabilize your mental health first. Then revisit GLP-1 treatment when you have a clear baseline.
History of eating disorders
GLP-1 medications suppress appetite powerfully. For women with a history of anorexia, bulimia, or restrictive eating, this appetite suppression can trigger disordered patterns. The praise and positive feedback that weight loss generates can reinforce harmful behaviors. If you have a history of eating disorders, GLP-1 treatment requires close monitoring by a provider who understands both the medication and the eating disorder dynamics.
Significant nutritional deficiencies
If postpartum blood work reveals significant iron deficiency anemia, severe vitamin D depletion, or other substantial nutritional gaps, address these before starting a medication that will further reduce food intake. You cannot supplement your way around a fundamental caloric and nutritional deficit.
Extremely low body weight or BMI
GLP-1 medications are designed for overweight and obese individuals. If your postpartum weight retention is modest (fewer than 10 pounds above pre-pregnancy weight) and your BMI is in the normal range, the risks and side effects of GLP-1 treatment likely outweigh the benefits. Dietary adjustments, exercise, and time may be sufficient.
Gallbladder concerns
Rapid weight loss increases gallstone risk, and pregnancy itself independently increases gallbladder complications. The combination of postpartum gallbladder vulnerability and GLP-1-driven weight loss can elevate risk further. If you have a history of gallbladder issues or experienced gallbladder symptoms during pregnancy, discuss this specifically with your provider. The tirzepatide and gallbladder guide covers this risk in detail.
Planning another pregnancy soon
If you are planning to conceive again within the next six to twelve months, GLP-1 medications may not be appropriate. These medications should be discontinued at least two months before attempting pregnancy due to their effects on fetal development. Our guides on semaglutide while trying to get pregnant and pregnancy on tirzepatide cover the fertility implications and recommended washout periods. GLP-1 medications can actually increase fertility, as the semaglutide fertility guide explains, so additional contraception is important if you are not planning another pregnancy.
Real postpartum GLP-1 timelines and expectations
Understanding what to expect month by month helps manage expectations and reduces the frustration that leads many people to quit treatment prematurely. Postpartum GLP-1 weight loss follows a somewhat different trajectory than standard GLP-1 weight loss, influenced by hormonal recovery, breastfeeding status, and the unique metabolic environment of the postpartum period.
Month 1: adjustment period
Expect minimal weight loss during the first month. Seriously. The starting dose (0.25 mg semaglutide or 2.5 mg tirzepatide) is a titration dose, not a therapeutic dose. Its purpose is to let your body acclimate to the medication, not to produce significant weight loss. You may lose two to four pounds, mostly from reduced water retention and slightly lower caloric intake. You may also lose nothing. Both are normal.
Side effects are most noticeable this month. Nausea, reduced appetite, occasional headache, and changes in bowel habits are common. They typically improve by week three or four. The first week on semaglutide guide and first dose of tirzepatide guide walk through what to expect in granular detail.
Month 2: early progress
As you move to the second dose level, appetite suppression becomes more noticeable. Weight loss of three to six pounds is typical during month two. You may notice that you naturally reach for healthier foods, not because of willpower, but because the medication reduces the drive toward high-calorie comfort eating. Many women describe this as "food noise quieting down," which is particularly powerful postpartum when stress eating can feel automatic.
Months 3 through 4: momentum builds
This is where meaningful weight loss typically begins. At therapeutic doses, most women lose four to eight pounds per month. You are now in the dose range where the medication is working at its intended level. Clothes fit differently. Energy often improves as body weight decreases. The gap between your current weight and your pre-pregnancy weight starts closing in a way that feels real rather than aspirational. The semaglutide monthly results breakdown and tirzepatide first month results provide benchmarks for comparison.
Months 5 through 6: steady state
Weight loss continues at a steady rate. Most women have lost 10 to 15 percent of their starting weight by this point. Side effects have largely resolved or become manageable background noise. You have established eating patterns that work with the medication rather than fighting against it. If you started at three months postpartum, you are now six to nine months after delivery, which means hormonal recovery is also well advanced and may be contributing to improved results.
Some women hit a plateau around this time. If weight loss stalls for three or more weeks despite adherence, a dose increase or a review of nutritional intake may be warranted. The troubleshooting guide for semaglutide and tirzepatide troubleshooting guide cover common reasons for stalls and how to address them.
Months 7 through 12: approaching goal
By nine to twelve months of treatment, most women have either reached their pre-pregnancy weight or are within striking distance. Total weight loss of 15 to 25 percent of starting weight is typical with consistent treatment. At this point, the conversation shifts from "how much more can I lose" to "how do I maintain this." SeekPeptides provides comprehensive maintenance protocols, and the GLP-1 maintenance dose guide covers strategies for transitioning from active weight loss to long-term maintenance.
The semaglutide before and after results, tirzepatide before and after results, and general GLP-1 before and after pages show real outcomes across different starting points and timelines.
What if you stop the medication?
This is an important conversation to have early. GLP-1 medications do not permanently reset your metabolism. When you stop, appetite returns to baseline and weight regain is common, typically 50 to 70 percent of lost weight over the following year without intervention. The guide on stopping semaglutide, the tirzepatide weaning guide, and the weight maintenance after tirzepatide resource all cover discontinuation strategies that minimize rebound.
Some women choose to continue at a low maintenance dose long-term. Others use GLP-1 treatment as a bridge to establish healthier habits and then taper off gradually. There is no single correct approach, and the duration guide for semaglutide explores the considerations involved. If you need to restart after a break, the restarting semaglutide guide covers how to safely resume.
Postpartum GLP-1 weight loss summary table
Timeline | Expected weight loss | Key milestones |
|---|---|---|
Month 1 | 2-4 lbs | Adjustment phase, managing side effects |
Month 2 | 3-6 lbs | Appetite suppression noticeable, food noise reduces |
Months 3-4 | 4-8 lbs/month | Therapeutic dose reached, consistent loss begins |
Months 5-6 | 3-6 lbs/month | 10-15% total loss, side effects minimal |
Months 7-9 | 2-4 lbs/month | Approaching pre-pregnancy weight, loss slows |
Months 10-12 | 1-3 lbs/month | 15-25% total loss, maintenance planning begins |
These are averages. Your trajectory will be influenced by your starting weight, breastfeeding status, medication choice, dose, activity level, nutrition quality, hormonal recovery, and sleep patterns. A healthy rate of postpartum weight loss is one to two pounds per week. Anything faster than that may indicate excessive caloric restriction, which is not sustainable and not safe during the postpartum period. The semaglutide speed of action guide and tirzepatide speed of action guide set realistic expectations.
Frequently asked questions
How soon after giving birth can I start semaglutide or tirzepatide?
The minimum recommended waiting period is six weeks postpartum for uncomplicated vaginal deliveries. Most providers prefer eight to twelve weeks, and twelve to sixteen weeks after a C-section. Three months postpartum is widely considered the sweet spot for starting, as hormonal stabilization, breastfeeding establishment, and initial recovery are typically well underway by that point. The semaglutide onset timeline and tirzepatide onset timeline help you understand when to expect results once you start.
Will GLP-1 medications affect my breast milk supply?
They can, indirectly. The medications themselves have not been shown to directly suppress milk production. However, the reduced caloric and fluid intake that GLP-1 appetite suppression causes can affect supply if intake drops too low. Maintaining a minimum of 1,800 calories daily, staying well hydrated with 80 to 100 ounces of fluid, and monitoring supply closely during the first few weeks of treatment minimizes this risk. Read more in our complete breastfeeding and GLP-1 guide.
Is injectable semaglutide safe while breastfeeding?
Injectable semaglutide has shown a maximum relative infant dose of 1.26 percent in available research, well below the 10 percent threshold generally considered safe for breastfeeding. However, oral semaglutide contains an absorption enhancer that may enter breast milk with unknown effects, so only injectable formulations are considered appropriate during breastfeeding. Formal large-scale safety studies are still needed.
Which GLP-1 medication is best for postpartum weight loss?
It depends on your specific situation. If you are breastfeeding, injectable semaglutide has the most milk safety data. If you had gestational diabetes, liraglutide has direct postpartum study data. If you need maximum weight loss and are not breastfeeding, tirzepatide typically produces the greatest results. The semaglutide versus tirzepatide comparison helps weigh the options.
Can I take GLP-1 medications if I had a C-section?
Yes, but the waiting period is typically longer, usually twelve to sixteen weeks, to allow adequate surgical healing. Your body needs sufficient nutrition to heal the incision site, and starting an appetite-suppressing medication too soon could compromise wound healing and recovery.
How much weight can I realistically lose on GLP-1 postpartum?
Most women lose 15 to 25 percent of their starting weight over 9 to 12 months of treatment. If you weigh 180 pounds when you start, that translates to 27 to 45 pounds. Postpartum women who are breastfeeding may lose at a slightly slower rate due to higher caloric requirements but typically achieve similar total losses over a longer timeline.
Will GLP-1 affect my hormones or period?
GLP-1 medications can influence hormone levels indirectly through weight loss and metabolic changes. Some women notice changes in their menstrual cycle, and the medications may increase estrogen levels as fat tissue decreases. Our guides on semaglutide and periods, tirzepatide and periods, and semaglutide and estrogen cover these effects in detail.
Can I take GLP-1 with my postpartum medications?
GLP-1 medications are compatible with most postpartum medications, including common antidepressants, thyroid medications, and prenatal vitamins. However, GLP-1 slows gastric emptying, which can affect absorption timing for other oral medications. Take oral medications at least one hour before or after eating, and discuss timing with your pharmacist. If you are on metformin for gestational diabetes management, both semaglutide and metformin and tirzepatide and metformin can be taken together safely.
What if GLP-1 medication does not work for me?
If you have been on a therapeutic dose for at least eight weeks without any weight loss, several factors should be evaluated: medication quality (especially if using compounded formulations), caloric intake that may be too high or too low, thyroid function, sleep quality, and stress levels. Our guides on no weight loss after four weeks on semaglutide, compounded semaglutide not working, and tirzepatide not working anymore cover troubleshooting in depth. The semaglutide to tirzepatide conversion chart and switching guide can help if changing medications becomes appropriate.
Should I tell my pediatrician I am taking GLP-1 medication?
Yes, absolutely. If you are breastfeeding, your pediatrician should know about all medications you are taking. They can monitor your infant for any potential effects and provide additional reassurance or recommendations based on your baby specific health profile.
Can I combine GLP-1 with HRT postpartum?
Hormone replacement therapy is not typically indicated postpartum unless there are specific conditions warranting it. However, if your provider has prescribed hormonal treatment for a postpartum condition, it can generally be used alongside GLP-1 medications. The HRT and GLP-1 combination guide covers the interaction between these treatments.
How do I store my GLP-1 medication as a new parent?
GLP-1 medications require refrigeration before first use and can be kept at room temperature (below 86 degrees Fahrenheit) for a limited period after. Keep medications out of reach of children and away from direct light. Our semaglutide storage guide and travel guide cover storage logistics for busy schedules.
External resources
ACOG: Exercise After Pregnancy - Official guidelines from the American College of Obstetricians and Gynecologists on returning to physical activity postpartum
CDC: Postpartum Depression - Resources for identifying and addressing postpartum mood disorders that may affect treatment decisions
LactMed Database - National Library of Medicine database for checking medication safety during breastfeeding, including GLP-1 receptor agonist entries
NIDDK: Gestational Diabetes - National Institute of Diabetes and Digestive and Kidney Diseases information on gestational diabetes and long-term metabolic health
WHO: Breastfeeding Guidelines - World Health Organization guidance on breastfeeding nutrition and health considerations
For new mothers serious about reclaiming their health safely, SeekPeptides offers evidence-based protocols, dosing calculators, and a community of researchers who understand the unique demands of postpartum recovery. The peptide calculator, semaglutide dosage calculator, and comprehensive guides for women provide the tools you need to approach postpartum weight loss with confidence and clarity. Whether you are exploring peptides for women over 40, investigating peptides for menopause weight loss, or just beginning your research into peptides for fat loss, SeekPeptides is where evidence meets accessibility. The peptide safety and risks resource ensures you approach any treatment with full awareness, and the women-specific weight loss guide addresses the unique considerations that matter most during this chapter of your life.
In case I do not see you, good afternoon, good evening, and good night. May your recovery stay steady, your energy stay strong, and your little one stay healthy.