Mar 16, 2026

Of the 461,000 GLP-1 users studied in one retrospective analysis, 12.7% developed a new nutritional deficiency within just six months. By the twelve-month mark, that number climbed to 13.6%. Vitamin D deficiency alone affected 7.5% of users at six months. These are not small numbers. These are not rare edge cases. These are hundreds of thousands of people losing nutrients they did not know they needed to protect.
And the nutrient gap is only part of the problem. Research shows that 25 to 40% of weight lost on GLP-1 medications like semaglutide and tirzepatide can come from lean muscle tissue, not fat.
One study found that 10% muscle mass loss over 68 weeks on a GLP-1 equaled roughly two decades of normal age-related muscle decline. Compressed into just over a year. That should concern anyone serious about long-term health outcomes.
The caloric reduction is dramatic too. GLP-1 users report eating 16 to 39% fewer calories than before treatment. When you eat that much less, hitting your daily vitamin and mineral targets becomes nearly impossible without deliberate supplementation. Yet only 12% of GLP-1 users receive supplement guidance from their healthcare provider. The gap between what people need and what they are told is enormous.
This guide covers every supplement worth considering when using GLP-1 medications. From the essential vitamins that prevent deficiency to the muscle-preserving compounds that protect lean mass, from digestive support that manages common side effects to the specific nutrients that keep hair on your head. Whether you are on semaglutide, tirzepatide, or retatrutide, the nutritional challenges are similar. And the solutions are more straightforward than most people realize. SeekPeptides has compiled the research so you do not have to guess.
Why GLP-1 users need targeted supplementation
GLP-1 receptor agonists work by mimicking a natural hormone that regulates appetite, blood sugar, and gastric emptying. Medications like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) achieve weight loss of approximately 14.9 to 20% of body weight. That is significantly more than the 5 to 7% achieved through traditional methods. But that accelerated weight loss creates nutritional challenges that most prescribers never discuss.
Three mechanisms drive the supplement need. First, appetite suppression reduces total food intake dramatically. When you are eating 16 to 39% fewer calories, you are also consuming 16 to 39% fewer vitamins and minerals. The math is simple. Less food means less nutrition, even when you choose nutrient-dense foods.
Second, GLP-1 medications slow gastric emptying. Food sits in the stomach longer. This affects how certain nutrients are absorbed, particularly vitamin B12 and iron. The delayed transit time can also contribute to constipation and bloating, further reducing the desire to eat.
Third, rapid weight loss itself depletes nutrients. Fat tissue stores fat-soluble vitamins like A, D, E, and K. When fat cells shrink quickly, these vitamins can be mobilized and excreted rather than properly redistributed. People with obesity already face a 35% higher likelihood of vitamin D insufficiency compared to normal-weight populations. Adding rapid weight loss to that baseline deficit creates a compounding problem.
A cross-sectional study of GLP-1 users found significant shortfalls in calcium, iron, magnesium, potassium, vitamins A, C, D, and E, plus choline. Only 43% of users consumed at least 1.2 grams of protein per kilogram of body weight per day. A mere 5% reached the optimal 2.0 grams per kilogram target. These numbers reveal a population that is losing weight but potentially undermining its own health in the process.
The good news? A strategic supplement stack addresses most of these gaps. You do not need twenty different bottles. You need the right ones, at the right doses, at the right times.
Essential vitamins and minerals every GLP-1 user needs
Not all deficiencies are created equal. Some nutrients drop faster than others on GLP-1 therapy. Some carry more serious consequences when depleted. The following vitamins and minerals represent the foundation that every GLP-1 user should consider, regardless of which specific medication they are taking.
Vitamin D: the most common deficiency
Vitamin D deficiency is the single most frequently diagnosed nutritional problem among GLP-1 users. In the large retrospective study of 461,000 users, 7.5% developed vitamin D deficiency at six months and the number kept climbing at twelve months. This matters because vitamin D plays critical roles in bone health, immune function, mood regulation, and muscle preservation.
People with obesity already tend toward low vitamin D levels because the vitamin gets sequestered in adipose tissue. As weight loss accelerates on GLP-1 therapy, the combination of reduced dietary intake and metabolic changes can push levels dangerously low. Some research suggests that adequate vitamin D levels may even improve hemoglobin A1C, making the medication itself work better.
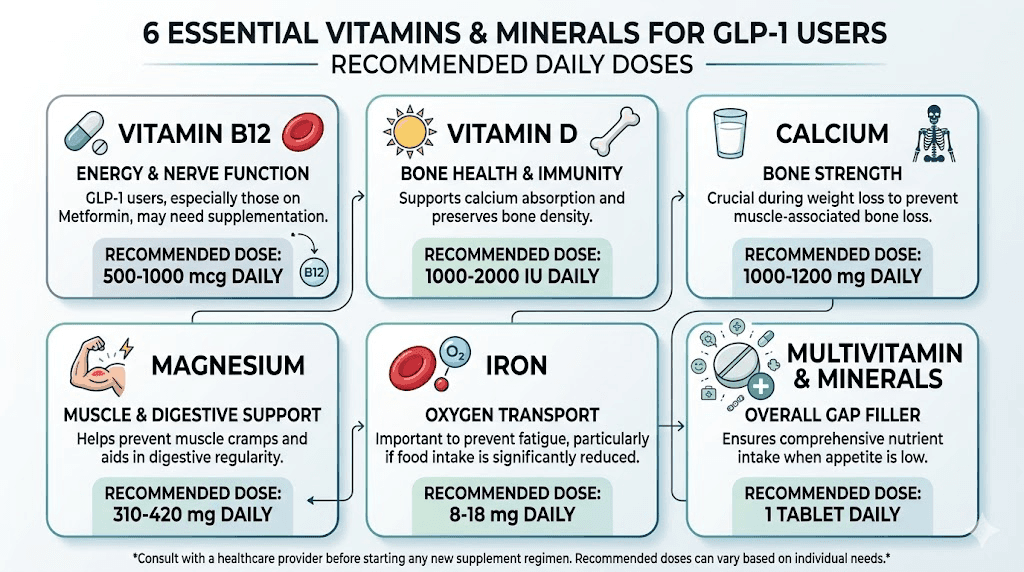
Recommended dose: 2,000 to 4,000 IU daily for maintenance. If already deficient, some protocols call for 50,000 IU weekly under medical supervision until levels normalize. The target serum level is 30 to 50 ng/mL. Get tested before starting and retest at three to six months.
Vitamin B12: absorption matters
Vitamin B12 is critical for nerve function, red blood cell production, and energy metabolism. GLP-1 medications can impair B12 absorption through delayed gastric emptying and altered intrinsic factor activity. The risk compounds significantly for users who also take metformin, as metformin independently reduces B12 absorption.
Symptoms of B12 deficiency develop slowly and can mimic other conditions. Fatigue, brain fog, tingling in hands and feet, and mood changes. Many people attribute these symptoms to the GLP-1 medication itself when the real culprit is a correctable nutrient deficiency. If you are experiencing fatigue on semaglutide or general GLP-1 fatigue, B12 levels should be checked before anything else.
An important note: semaglutide may interfere with B12 assay results, potentially leading to false low readings when used alongside metformin. Discuss this with your provider to ensure accurate testing.
Recommended dose: 500 to 1,000 mcg daily of methylcobalamin (the active form). Sublingual tablets bypass the GI tract entirely, which makes them particularly useful when gastric emptying is delayed. Some compounded formulations already include B12, like semaglutide with B12 and tirzepatide with B12, which simplifies the supplementation process.
Iron: especially important for women
Iron deficiency is common in the general population and GLP-1 therapy can make it worse. Reduced food intake means less dietary iron. Delayed gastric emptying can impair iron absorption. And rapid weight loss may alter iron metabolism in ways researchers are still studying.
Women of reproductive age are particularly vulnerable. If you are taking a GLP-1 and notice unusual fatigue, pale skin, shortness of breath during exercise, or cold hands and feet, iron deficiency should be on your radar. Some GLP-1 users have reported that semaglutide affects menstrual cycles and tirzepatide affects periods, which can further impact iron status through changes in blood loss.
Recommended dose: 18 mg daily for premenopausal women. Men and postmenopausal women should only supplement if testing confirms a deficiency, as excess iron carries its own risks. Take iron on an empty stomach with vitamin C to enhance absorption. Do not take iron within two hours of calcium or dairy products.
Magnesium: the overlooked essential
Magnesium participates in over 300 enzymatic reactions in the body. It supports muscle function, nerve transmission, blood sugar regulation, and sleep quality. GLP-1 medications can deplete magnesium through multiple pathways. Reduced dietary intake is the primary driver. But digestive side effects like diarrhea and vomiting can cause additional losses through the GI tract.
Low magnesium often manifests as muscle cramps, poor sleep, anxiety, and irregular heartbeat. These symptoms overlap with common GLP-1 side effects, which means magnesium deficiency frequently goes undiagnosed. If you are experiencing body aches on tirzepatide or muscle pain, magnesium status is worth investigating.
Recommended dose: 200 to 400 mg daily. Magnesium glycinate is the preferred form for GLP-1 users because it is gentle on the stomach and supports sleep. Magnesium citrate is an alternative that also helps with constipation, which can be a useful secondary benefit. Avoid magnesium oxide, which has poor bioavailability.
Zinc: protecting immune function and metabolism
Research on GLP-1 users found significant decreases in serum zinc levels alongside weight reduction. Zinc supports immune function, wound healing, thyroid hormone production, and testosterone synthesis. It also plays a role in taste and smell perception, which matters when appetite is already suppressed and food needs to be as appealing as possible.
Zinc deficiency can cause hair thinning, weakened immunity, slow wound healing, and reduced appetite, creating a vicious cycle where low zinc makes you eat even less, which further depletes zinc.
Recommended dose: 15 to 30 mg daily, taken with food. Zinc picolinate and zinc glycinate are well-absorbed forms. Do not exceed 40 mg daily from all sources, as excess zinc can interfere with copper absorption.
Calcium: bone protection during weight loss
Rapid weight loss is associated with decreased bone mineral density. GLP-1 medications accelerate this concern through reduced calcium intake and potential changes in calcium absorption. The combination of lower dietary calcium, possible vitamin D deficiency, and reduced mechanical loading on bones as body weight drops creates a perfect storm for bone health problems.
Recommended dose: 1,000 to 1,200 mg daily from food and supplements combined. Split doses are better absorbed, so take 500 to 600 mg twice daily rather than the full amount at once. Calcium citrate is preferred for GLP-1 users because it does not require stomach acid for absorption, which matters when gastric acid production may be altered. Always pair calcium with adequate vitamin D for proper absorption.
Important caution: Some sources recommend consulting with your prescriber before supplementing calcium, as high doses may interact with certain medications. Start with dietary sources first and add supplements only to fill the gap.
Muscle preservation supplements: protecting lean mass
This is arguably the most important supplement category for GLP-1 users. The muscle loss problem is real. It is significant. And it is largely preventable with the right approach.
Here is the uncomfortable truth. Without intervention, roughly 25 to 40% of weight lost on GLP-1 medications comes from lean body mass rather than fat. One clinical study documented 10% muscle mass loss over 68 weeks, equivalent to approximately twenty years of normal age-related muscle decline. That accelerated muscle loss affects metabolic rate, functional strength, bone density, and long-term weight maintenance after stopping the medication.
Resistance training is the single most important countermeasure. But supplements play a critical supporting role, especially when appetite suppression makes it difficult to consume enough protein through food alone.
Protein supplementation: the foundation
Protein is not optional on GLP-1 therapy. It is essential. Research consistently shows that adequate protein intake combined with resistance training can largely prevent the lean mass losses associated with these medications. The problem is actually hitting the targets when you do not feel like eating.
Clinical evidence supports consuming 1.2 to 2.0 grams of protein per kilogram of body weight daily during active GLP-1 treatment. A 12-week randomized controlled trial demonstrated that 1.3 grams per kilogram successfully promoted fat mass reduction while preserving fat-free mass, muscle strength, and resting metabolic rate. Yet only 43% of GLP-1 users even reach the minimum 1.2 gram target, and a mere 5% hit the optimal 2.0 gram goal.
For a person weighing 80 kg (176 pounds), that minimum target is 96 grams of protein daily. The optimal target is 160 grams. When your appetite is suppressed and you are eating 1,200 to 1,500 calories per day, getting that much protein from food alone is extremely difficult. This is where protein supplementation becomes genuinely necessary rather than merely convenient. Protein shakes designed for GLP-1 users can bridge this gap efficiently.
Whey protein has the best bioavailability and the strongest evidence for muscle preservation. If dairy is problematic, and it can be for GLP-1 users experiencing bloating or sulfur burps, pea protein is the next best option. Collagen protein is popular but does not count equally toward muscle-building protein needs because it lacks sufficient leucine.
Recommended dose: 20 to 40 grams of protein powder per serving, one to two servings daily as needed to hit total protein targets. Timing matters less than total daily intake, but consuming protein within two hours of resistance training provides a modest additional benefit.
Creatine: the most studied muscle supplement
Creatine monohydrate is the most extensively researched supplement for muscle preservation and performance. A meta-analysis of 35 randomized trials showed that creatine supplementation significantly increased lean body mass by 0.68 kg overall, rising to 1.1 kg when combined with resistance training. For GLP-1 users actively losing lean mass, that preservation effect is meaningful.
Creatine works by increasing phosphocreatine stores in muscle tissue, which supports energy production during high-intensity exercise. It also draws water into muscle cells, creating an anabolic environment that favors muscle protein synthesis. For people on GLP-1 medications who are eating less and potentially not exercising enough, creatine provides a low-cost, evidence-based insurance policy for muscle tissue.
Recommended dose: 5 grams of creatine monohydrate daily. No loading phase is necessary. Take it at any time of day with water or mixed into a protein shake. Creatine can cause a small increase in scale weight (2 to 4 pounds) due to water retention in muscle, which is not fat gain and should not cause alarm on your weight loss timeline.
HMB: targeted muscle protection
Beta-hydroxy beta-methylbutyrate (HMB) is a metabolite of the amino acid leucine. It works through a different mechanism than creatine, primarily by reducing muscle protein breakdown rather than increasing synthesis. This makes it particularly relevant during caloric restriction, when the body is more prone to catabolizing muscle tissue for energy.
A meta-analysis in older adults found that HMB supplementation significantly increased muscle mass by 0.352 kg with no change in fat mass. While the absolute numbers may seem modest, the anti-catabolic effect during weight loss is what makes HMB valuable for GLP-1 users specifically.
Recommended dose: 3 grams daily, split into three 1-gram doses with meals or taken as a single dose. HMB is often combined with creatine for a synergistic effect, as the two compounds work through complementary pathways. One stimulates synthesis. The other prevents breakdown.
The combined muscle preservation protocol
For GLP-1 users serious about maintaining results long-term, the evidence supports combining these three supplements with resistance training.
Daily muscle preservation stack:
Protein powder: 20-40 grams, one to two servings daily (hit 1.2-2.0 g/kg total daily protein)
Creatine monohydrate: 5 grams daily
HMB: 3 grams daily
Resistance training: Two to four sessions per week minimum
This combination addresses muscle preservation from multiple angles. Protein provides the raw materials. Creatine enhances training performance and creates an anabolic environment. HMB reduces breakdown. And resistance training provides the stimulus that tells your body to prioritize muscle over fat for energy. SeekPeptides members access detailed stacking protocols and personalized guidance for optimizing body composition during GLP-1 therapy.

Digestive support supplements
GLP-1 medications slow gastric emptying. That is how they reduce appetite. But that same mechanism causes the most common side effects users experience. Nausea. Bloating. Constipation. Diarrhea. Sulfur burps. The digestive system is essentially recalibrating to a new speed of operation, and targeted supplements can make that transition significantly smoother.
Fiber: the constipation solution
Constipation is one of the most frequently reported side effects of GLP-1 therapy. When gastric motility slows, stool transit time increases, and water absorption in the colon increases. The result is harder, less frequent bowel movements. Studies confirm that fiber supplementation lasting at least four weeks significantly increases stool frequency and softens stool consistency compared to placebo.
For GLP-1 users specifically, the challenge is that reduced food intake also means reduced dietary fiber intake. Most adults already fall short of the recommended 25 to 38 grams daily even without appetite suppression. On a GLP-1, the shortfall becomes more severe.
Recommended dose: 10 to 15 grams of supplemental fiber daily, building up gradually over two to three weeks to avoid gas and cramping. Psyllium husk is the most studied option and provides both soluble and gel-forming fiber. Partially hydrolyzed guar gum (PHGG) is another option that causes less bloating than psyllium. Always consume fiber with plenty of water, at least 8 to 12 ounces per serving. Follow a structured diet plan that incorporates high-fiber foods alongside supplementation for best results.
Probiotics: supporting the gut microbiome
Changes in gut motility and digestion affect the microbiome. GLP-1 medications alter the environment in which gut bacteria operate, and early research suggests this can shift microbial populations in ways that may contribute to digestive symptoms. Probiotic supplementation aims to support beneficial bacterial populations during this transition.
Research demonstrates that probiotics can significantly promote weight management independent of dietary modifications, which makes them a useful complement to GLP-1 therapy rather than just a digestive aid. The best probiotics for semaglutide users and other GLP-1 users include specific strains with evidence for digestive health.
Recommended strains: Lactobacillus acidophilus and Bifidobacterium lactis are the most commonly recommended strains for GLP-1 users. Multi-strain formulations that include Lactobacillus rhamnosus are also well-supported.
Recommended dose: 10 to 30 billion CFUs daily for moderate support. Doses above 30 billion CFUs are considered high-dose protocols for more severe digestive symptoms. Take probiotics with food to improve survival through stomach acid. Some practitioners recommend the Pendulum GLP-1 Probiotic Pro which was specifically formulated for GLP-1 users.
Ginger: natural nausea management
Nausea is the most common side effect during the first weeks on semaglutide and first doses of tirzepatide. While nausea typically decreases as your body adjusts, it can be significant enough in the early weeks to impact quality of life and nutritional intake.
Ginger has well-established antiemetic properties. It works by blocking serotonin receptors in the gut and accelerating gastric emptying, which directly counteracts the delayed emptying that causes nausea on GLP-1 medications.
Recommended dose: 250 mg of ginger extract four times daily, or 1 to 2 grams of raw ginger root. Ginger tea is another option for those who prefer liquid forms. Vitamin B6 (pyridoxine) at 10 to 25 mg daily can complement ginger for nausea management, and some compounded formulations like semaglutide with pyridoxine and tirzepatide with B6 already include this vitamin.
Hair loss prevention supplements
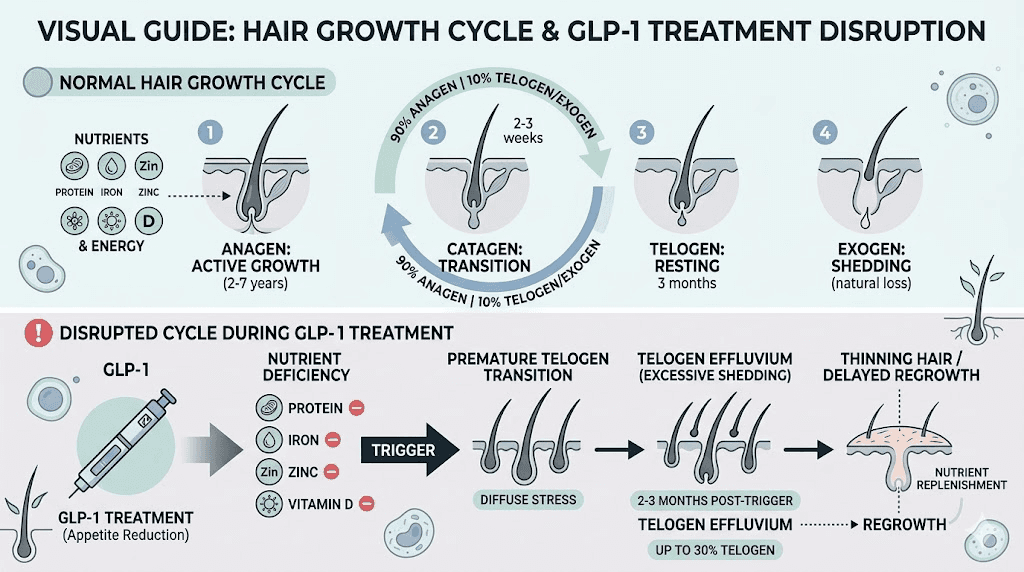
Hair loss on GLP-1 medications is more common than the clinical trials initially suggested. A systematic review found that hair loss associated with GLP-1 receptor agonist use is a documented phenomenon, primarily related to the telogen effluvium triggered by rapid weight loss and nutritional deficiency rather than a direct drug effect.
When the body experiences significant caloric restriction and weight loss, it diverts resources away from non-essential functions like hair growth toward vital organ maintenance. The hair follicle enters a resting phase (telogen), and two to four months later, increased shedding becomes noticeable. The good news is that this type of hair loss is usually reversible once nutritional status stabilizes.
The hair protection nutrient stack
Preventing hair loss on GLP-1 therapy requires addressing the root cause: nutrient deficiency and inadequate protein.
Protein: This is the single most important factor. Hair is made of keratin, a protein. Without adequate protein intake, the body simply cannot maintain hair growth. Aim for 90 to 100 grams of protein daily at minimum, starting before hair loss occurs as a preventive measure rather than a reactive one. Protein shakes make hitting this target much easier.
Biotin: 2,500 to 5,000 mcg daily. Biotin is a B vitamin that supports keratin production. While deficiency is relatively rare, supplementation at these doses has shown benefit for hair density in some studies. Many GLP-1 users include biotin as part of their GLP-1 vitamin protocol.
Vitamin D: As discussed above, 2,000 to 4,000 IU daily. Vitamin D receptors exist in hair follicles, and deficiency is associated with increased hair shedding. Since vitamin D deficiency is the most common nutritional problem on GLP-1 therapy, this supplement serves double duty.
Iron and zinc: At the doses discussed in the essential vitamins section. Both minerals are critical for hair follicle function. Iron deficiency is one of the most common and most reversible causes of hair loss in women. Zinc supports hair tissue growth and keeps the oil glands around hair follicles functioning properly.
Omega-3 fatty acids: 1 to 2 grams daily. Omega-3s support scalp health and may reduce the inflammation that contributes to hair follicle miniaturization. They also improve the quality of existing hair by adding shine and reducing brittleness. Learn more about peptide approaches to hair loss and hair growth peptides for additional strategies.
Anti-inflammatory and recovery supplements
GLP-1 medications have inherent anti-inflammatory properties. That is actually one of their secondary benefits. But the weight loss process itself can trigger inflammatory responses, particularly in joints and connective tissue as the body adapts to carrying less weight. Some users report joint pain on tirzepatide or general body aches during active weight loss. Anti-inflammatory supplements can provide meaningful relief.
Omega-3 fish oil
Omega-3 fatty acids, specifically EPA and DHA from fish oil, support muscle quality and provide anti-inflammatory effects that complement GLP-1 therapy. The research review on supplements during GLP-1 treatment recommends at least 1 gram daily of combined EPA and DHA.
Beyond inflammation, omega-3s support cardiovascular health, brain function, and joint mobility. For GLP-1 users who are exercising regularly to preserve muscle mass, omega-3s may improve recovery between training sessions and reduce exercise-induced soreness.
Recommended dose: 1 to 3 grams of combined EPA and DHA daily. Look for supplements that provide at least 500 mg of EPA per serving, as EPA is the more potently anti-inflammatory component. Take with a fat-containing meal for optimal absorption. Triglyceride form fish oil is better absorbed than ethyl ester form.
Curcumin (turmeric extract)
Curcumin, the active compound in turmeric, has robust anti-inflammatory evidence at supplemental doses. The research review on GLP-1 supplementation specifically includes curcumin at 500 to 1,500 mg daily for its anti-inflammatory effects.
For GLP-1 users experiencing joint discomfort during weight loss, curcumin provides a natural alternative to daily NSAID use. It also has modest benefits for digestive inflammation, which can help with the acid reflux and gut irritation some users experience.
Recommended dose: 500 to 1,500 mg daily of curcumin extract. Look for formulations that include piperine (black pepper extract) or use liposomal delivery, as standard curcumin has notoriously poor bioavailability. Take with a fat-containing meal.
Complete supplement protocols by goal
Not everyone needs every supplement on this list. Your specific protocol should match your goals, your current nutritional status, and your side effect profile. Below are four targeted protocols that cover the most common scenarios for GLP-1 users.
Protocol 1: essential foundation (everyone should consider this)
Goal: Prevent the most common nutrient deficiencies during GLP-1 therapy.
Vitamin D3: 2,000-4,000 IU daily
Vitamin B12: 500-1,000 mcg methylcobalamin daily
Magnesium glycinate: 200-400 mg daily (evening)
Protein supplement: 20-40 grams daily as needed to hit 1.2 g/kg minimum
Fiber: 10-15 grams daily (psyllium husk or PHGG)
Expected benefits: Maintained energy levels, reduced constipation, better sleep quality, protected nerve function. This is the bare minimum stack for anyone on a GLP-1 medication longer than four weeks.
Monthly cost estimate: $30-50 depending on brands chosen.
Protocol 2: muscle preservation focus
Goal: Maximize fat loss while minimizing lean mass loss during GLP-1 treatment.
Everything in Protocol 1, plus:
Protein supplement: Increase to 1.6-2.0 g/kg total daily protein (likely requires 40-80 grams from supplements)
Creatine monohydrate: 5 grams daily
HMB: 3 grams daily
Omega-3 fish oil: 1-2 grams EPA/DHA daily
Expected benefits: Significantly reduced lean mass loss, maintained or improved strength, better metabolic rate preservation, improved body composition outcomes. Pair with resistance training two to four times weekly for best results.
Monthly cost estimate: $60-90.
Protocol 3: side effect management
Goal: Minimize digestive side effects that are limiting adherence or quality of life.
Everything in Protocol 1, plus:
Probiotic: 10-30 billion CFUs daily (multi-strain with Lactobacillus and Bifidobacterium)
Ginger extract: 250 mg four times daily (or 1-2 grams raw ginger)
Vitamin B6: 10-25 mg daily for nausea
Electrolytes: Sodium, potassium, and magnesium if experiencing dizziness or dehydration
Expected benefits: Reduced nausea, more regular bowel movements, less bloating, better tolerance of the medication especially during the early side effect period.
Monthly cost estimate: $40-70.
Protocol 4: hair protection
Goal: Prevent or minimize telogen effluvium (hair shedding) during rapid weight loss on GLP-1 therapy.
Everything in Protocol 1, plus:
Protein: Minimum 90-100 grams daily total (critical, non-negotiable)
Biotin: 2,500-5,000 mcg daily
Iron: 18 mg daily for women (only if indicated by bloodwork for men)
Zinc: 15-30 mg daily
Omega-3: 1-2 grams daily
Expected benefits: Reduced hair shedding, maintained hair density, faster regrowth if shedding has already begun. Start this protocol before noticeable hair loss occurs for maximum preventive benefit.
Monthly cost estimate: $50-80.
Supplement timing guide for GLP-1 users
When you take supplements matters almost as much as which supplements you take. GLP-1 medications alter digestion timing, and some supplement interactions can reduce absorption if taken together. This timing schedule optimizes absorption while keeping the routine simple enough to maintain consistently.
Morning (with breakfast)
Vitamin D3 (fat-soluble, needs food)
Omega-3 fish oil (fat-soluble, needs food)
Vitamin B12 (sublingual, can be taken anytime but morning supports energy)
First fiber serving (with 8-12 oz water, at least 30 minutes before or after other supplements)
Midday (with lunch or protein shake)
Protein powder serving if needed
Iron if supplementing (separate from calcium by 2+ hours)
Creatine (timing is flexible, consistency matters more)
First HMB dose (1 gram)
Afternoon
Second HMB dose (1 gram)
Ginger extract if managing nausea
Probiotic (can be taken anytime with food)
Evening (with dinner)
Magnesium glycinate (supports sleep quality)
Calcium (separate from iron and magnesium by 2+ hours is ideal but not critical)
Zinc (take with food to prevent stomach upset)
Second protein serving if needed
Third HMB dose (1 gram)
Second fiber serving (with water)
Curcumin if supplementing
Key timing rules: Iron and calcium should not be taken at the same time. Fiber should be separated from other supplements by 30 minutes to prevent it from binding to and reducing absorption of other nutrients. Magnesium at night supports sleep. Fat-soluble vitamins (D, omega-3) need dietary fat for absorption.
Supplements to avoid or use with caution on GLP-1 therapy
Not every supplement is helpful during GLP-1 treatment. Some can interfere with the medication, worsen side effects, or provide false reassurance while masking real problems.
Weight loss supplements: Do not stack weight loss supplements (green tea extract, caffeine pills, stimulant fat burners) with GLP-1 medications. The GLP-1 is doing the heavy lifting for appetite suppression and weight loss. Adding stimulant-based supplements can increase anxiety, worsen insomnia, and place unnecessary stress on the cardiovascular system. While catechin-caffeine mixtures can increase energy expenditure by about 4.7 to 4.8%, this marginal benefit does not justify the risks when already on a GLP-1.
Berberine: Berberine and semaglutide together requires caution. Berberine has blood sugar-lowering properties similar to metformin, and combining it with a GLP-1 medication could increase hypoglycemia risk. Consult your provider before adding berberine.
High-dose calcium without testing: As mentioned earlier, do not start high-dose calcium supplementation without bloodwork confirming a need. Excess calcium supplementation has been associated with cardiovascular concerns in some observational studies.
Excessive vitamin A: Fat-soluble vitamins stored in adipose tissue get released during rapid weight loss. Supplementing high-dose vitamin A on top of this mobilization could potentially lead to toxicity. Get levels tested before supplementing beyond what is in a standard multivitamin.
Detox or cleanse products: These are unnecessary, potentially harmful, and can worsen the dehydration and electrolyte imbalances that GLP-1 users are already prone to. They add no value.
Semaglutide-specific supplement considerations
While the core supplement recommendations apply to all GLP-1 medications, semaglutide has some specific considerations worth noting.
B12 interaction with metformin: Many semaglutide users also take metformin for type 2 diabetes management. This combination creates a double risk for B12 deficiency, as both medications can impair absorption through different mechanisms. If you are on both, B12 supplementation is not optional. It is essential. Monitor levels every six months. The semaglutide with methylcobalamin formulation addresses this directly.
Glycine and B12 combinations: Compounded semaglutide with glycine and semaglutide glycine B12 blends are increasingly popular. Glycine is an amino acid that supports collagen synthesis, joint health, and sleep quality. When combined with B12 in the compounded formulation, it reduces the number of separate supplements needed.
L-carnitine addition: Some compounding pharmacies offer semaglutide with L-carnitine, which supports fat metabolism and energy production. L-carnitine may help with the fatigue that some semaglutide users experience by improving mitochondrial energy production.
Niacinamide combinations: Semaglutide with niacinamide (vitamin B3) combinations support NAD+ production and cellular energy metabolism. Niacinamide may also provide modest benefits for skin health during rapid weight loss.
Dosing timeline and supplements: Side effects tend to be most significant during the first week on semaglutide and during dose escalation periods. Prioritize anti-nausea supplements (ginger, B6) during these transitions. Once stabilized on a maintenance dose, the focus can shift to long-term nutritional support. Track your progress with week-by-week result expectations and adjust supplements based on how you feel at each stage.
For the full breakdown on reconstituting semaglutide, dosage charts, and injection site guidance, check our dedicated semaglutide resources. Pair your supplement protocol with proper dietary planning and food selection for the best results.
Tirzepatide and retatrutide supplement notes
If you are using tirzepatide, we have a dedicated guide covering supplements to take with tirzepatide that addresses the specific dual GIP/GLP-1 receptor agonist considerations. Tirzepatide tends to produce more significant weight loss than semaglutide alone, which means the muscle preservation and nutrient deficiency concerns are even more pressing.
Key tirzepatide-specific supplement resources include guidance on tirzepatide with glycine, tirzepatide glycine B12 compounds, tirzepatide with niacinamide, tirzepatide with levocarnitine, and tirzepatide with methylcobalamin. The tirzepatide diet plan and food recommendations should complement your supplement strategy.
For retatrutide users, the triple receptor agonist produces even more dramatic weight loss than either semaglutide or tirzepatide. This means the highest supplement priority of all three medications. The same core protocols apply, but pay particular attention to protein intake and muscle preservation, as the accelerated weight loss increases lean mass loss risk proportionally. Review the retatrutide dosage chart and plan your nutrition strategy from day one.

Should you use a multivitamin instead?
A common question. Can a single multivitamin replace the targeted supplement approach described above?
Partially. A high-quality multivitamin-mineral supplement can serve as a safety net for the essential micronutrients. It will provide baseline amounts of vitamins D, B12, iron, zinc, and other nutrients that GLP-1 users commonly become deficient in. For users who want the simplest possible approach, a multivitamin combined with a protein supplement and fiber covers the absolute basics.
However, multivitamins have limitations for GLP-1 users specifically. The doses of individual nutrients in most multivitamins are too low to correct existing deficiencies. A typical multivitamin contains 400 to 800 IU of vitamin D, when GLP-1 users may need 2,000 to 4,000 IU. Multivitamins do not include therapeutic doses of fiber, probiotics, creatine, HMB, or omega-3s. And some multivitamins include calcium and iron in the same pill, which reduces absorption of both.
The practical approach: use a multivitamin as your baseline, then add targeted supplements based on your specific protocol needs. This gives you broad-spectrum coverage plus focused doses where they matter most. Get bloodwork done at baseline and at three to six months to identify which specific nutrients need higher-dose supplementation. The blood work guide for semaglutide users covers what to test and when.
When to start supplementing
Ideally, before you take your first dose. Starting supplements two to four weeks before beginning GLP-1 therapy builds your nutrient stores and establishes the habits before appetite suppression makes eating and supplementing feel like a chore. This is especially true for protein and fiber, which take time to integrate into daily routines.
If you are already on a GLP-1 medication and have not been supplementing, start now. Nutrient depletion is cumulative. The longer you wait, the deeper the deficits become and the harder they are to correct. Begin with Protocol 1 (the essential foundation) and add targeted supplements based on your symptoms and goals.
For users who are restarting semaglutide after a break or switching between medications, reassess your supplement protocol during the transition. Dose escalation periods increase side effects and may require temporary increases in digestive support supplements.
Monitoring your progress
Supplementation without monitoring is guesswork. The following lab tests provide objective data on whether your protocol is working.
Baseline (before starting GLP-1 or supplements):
25-hydroxyvitamin D (target: 30-50 ng/mL)
Vitamin B12 (target: above 400 pg/mL)
Serum iron, ferritin, and TIBC
Serum magnesium
Serum zinc
Complete metabolic panel
CBC (to check for anemia)
Follow-up testing at 3 and 6 months:
Repeat all baseline labs
Add: body composition measurement (DEXA scan is gold standard) to track lean mass vs fat mass changes
Assess supplement adherence and adjust doses based on results
The cost of basic nutritional bloodwork is minimal compared to the cost of undiagnosed deficiencies. Many GLP-1 users feel unnecessarily terrible for months because nobody checked their B12 or vitamin D levels. Do not be one of them.
SeekPeptides members access comprehensive monitoring guides, supplement tracking tools, and personalized protocol recommendations based on individual lab results and goals.
The supplement-diet connection
Supplements fill gaps. They do not replace food. The most effective approach combines strategic supplementation with intentional food choices that maximize nutrient density per calorie. When you are eating less, every bite counts more.
Focus your reduced caloric intake on:
Lean protein sources: chicken, fish, eggs, Greek yogurt, cottage cheese (aim for 30+ grams of protein per meal)
Dark leafy greens: spinach, kale, Swiss chard (iron, magnesium, calcium, folate)
Fatty fish: salmon, sardines, mackerel twice weekly (omega-3s, vitamin D, protein)
Nuts and seeds: almonds, pumpkin seeds, sunflower seeds (magnesium, zinc, healthy fats)
Colorful vegetables: bell peppers, sweet potatoes, tomatoes (vitamins A, C, potassium)
Detailed guidance on food selection is available in our articles on the best foods to eat on semaglutide, foods to avoid on semaglutide, foods to avoid on tirzepatide, and complete meal planning guides. Proper nutrition combined with targeted supplementation creates a foundation that supports both effective weight loss and long-term health preservation. The GLP-1 breakfast ideas and dinner ideas guides offer specific recipes designed around nutrient density.
Comparing supplement needs across GLP-1 medications
Supplement | Semaglutide | Tirzepatide | Retatrutide | Priority |
|---|---|---|---|---|
Vitamin D3 | 2,000-4,000 IU | 2,000-4,000 IU | 4,000 IU | Essential |
Vitamin B12 | 500-1,000 mcg (higher if on metformin) | 500-1,000 mcg | 500-1,000 mcg | Essential |
Magnesium | 200-400 mg | 200-400 mg | 300-400 mg | Essential |
Protein | 1.2-2.0 g/kg/day | 1.2-2.0 g/kg/day | 1.6-2.0 g/kg/day | Essential |
Fiber | 10-15 g | 10-15 g | 10-15 g | Essential |
Creatine | 5 g | 5 g | 5 g | Recommended |
HMB | 3 g | 3 g | 3 g | Recommended |
Omega-3 | 1-2 g | 1-2 g | 1-2 g | Recommended |
Probiotic | 10-30B CFUs | 10-30B CFUs | 10-30B CFUs | Helpful |
Zinc | 15-30 mg | 15-30 mg | 15-30 mg | Helpful |
Iron | 18 mg (women) | 18 mg (women) | 18 mg (women) | Test first |
Calcium | 500-600 mg 2x | 500-600 mg 2x | 500-600 mg 2x | Test first |
Retatrutide generally requires the most aggressive supplementation because it produces the most significant weight loss of the three medications. Retatrutide vs semaglutide and retatrutide vs Mounjaro comparisons show progressively greater weight loss, which translates to progressively greater nutritional demands.
Users switching between medications should maintain their supplement protocol throughout the transition. The semaglutide to tirzepatide conversion chart can help with dose matching, but supplement needs remain consistent regardless of which GLP-1 medication you use.
Frequently asked questions
What supplements should I take with semaglutide?
At minimum, take vitamin D3 (2,000-4,000 IU), vitamin B12 (500-1,000 mcg), magnesium (200-400 mg), protein supplement (to reach 1.2-2.0 g/kg daily), and fiber (10-15 grams). If you are also on metformin, B12 supplementation is especially critical. Check our complete guide to semaglutide with B12 for detailed protocols.
Can I just take a multivitamin on GLP-1?
A multivitamin is a reasonable starting point but insufficient on its own. Most multivitamins provide doses too low to correct GLP-1-related deficiencies, and they do not include the muscle-preserving supplements (protein, creatine, HMB) or digestive support (fiber, probiotics) that GLP-1 users specifically need.
When should I start taking supplements?
Ideally two to four weeks before starting your GLP-1 medication. This builds nutrient stores before appetite suppression reduces your intake. If you are already on medication, start supplementing now. Deficits are cumulative and worsen over time.
Will supplements interact with my GLP-1 medication?
Most standard supplements do not directly interact with GLP-1 receptor agonists. However, berberine and blood sugar-lowering supplements should be used cautiously due to additive hypoglycemia risk. Always take fiber supplements 30 minutes apart from medications to prevent absorption interference. Consult your prescriber about combining semaglutide with other medications.
How do I prevent hair loss on GLP-1 medications?
Prioritize protein intake (90-100 grams daily minimum), supplement with vitamin D, iron, zinc, biotin, and omega-3s. Starting these supplements before noticeable hair loss is more effective than reacting after shedding begins. See our complete GLP-1 hair loss guide for the full protocol.
How much protein do I need on a GLP-1 medication?
Research supports 1.2 to 2.0 grams of protein per kilogram of body weight daily. For a 180-pound (82 kg) person, that is 98 to 164 grams daily. Most GLP-1 users need protein supplements to hit these targets because appetite suppression makes eating enough protein through food alone very difficult. Protein shakes formulated for GLP-1 users are the most practical solution.
Is creatine safe to take with semaglutide or tirzepatide?
Yes. Creatine monohydrate at 5 grams daily has no known interactions with GLP-1 medications. It may cause a modest scale weight increase of 2 to 4 pounds from water retention in muscle tissue, which is not fat gain. This is a positive sign that the creatine is working.
Do I need different supplements for tirzepatide versus semaglutide?
The core supplement needs are the same for all GLP-1 medications. Tirzepatide users may need to be more aggressive with muscle preservation supplements because tirzepatide typically produces greater weight loss than semaglutide. See our dedicated semaglutide vs tirzepatide side effects comparison for more details.
External resources
Dietary supplement considerations during GLP-1 receptor agonist treatment: A narrative review (PMC)
Nutritional deficiencies and muscle loss in adults using GLP-1 receptor agonists (PMC)
Investigating nutrient intake during GLP-1 receptor agonist use (Frontiers in Nutrition)
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based supplement guides, personalized protocol recommendations, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your nutrients stay balanced, your muscles stay preserved, and your results stay consistent.