Mar 20, 2026

You started tirzepatide to lose weight. It is working. The scale keeps dropping, your appetite has quieted, and the results feel real for the first time. But something else is happening. Your arms look smaller. Your strength in the gym has dipped. And that nagging question keeps surfacing: am I losing muscle along with the fat?
You are not imagining it. Research shows that up to 39% of the weight lost on GLP-1 medications can come from lean body mass, not just fat. That is nearly four pounds of muscle for every ten pounds the scale drops. For anyone who has spent years building strength, that number stings.
This is where creatine enters the conversation.
Creatine monohydrate is the most studied sports supplement in existence. Decades of research confirm it preserves muscle, boosts strength, and supports cellular energy production. And here is what matters most for tirzepatide users: creatine does all of this during caloric restriction, exactly the metabolic state your medication creates. No documented drug interaction exists between these two compounds. They operate through completely different mechanisms and metabolic pathways. But combining them effectively requires understanding the details most guides skip entirely, from timing around gastrointestinal side effects to navigating the kidney function questions your doctor will inevitably raise. This guide covers every angle, backed by research, practical protocols, and the specific considerations that make this combination work.
Why muscle loss on tirzepatide is a real problem
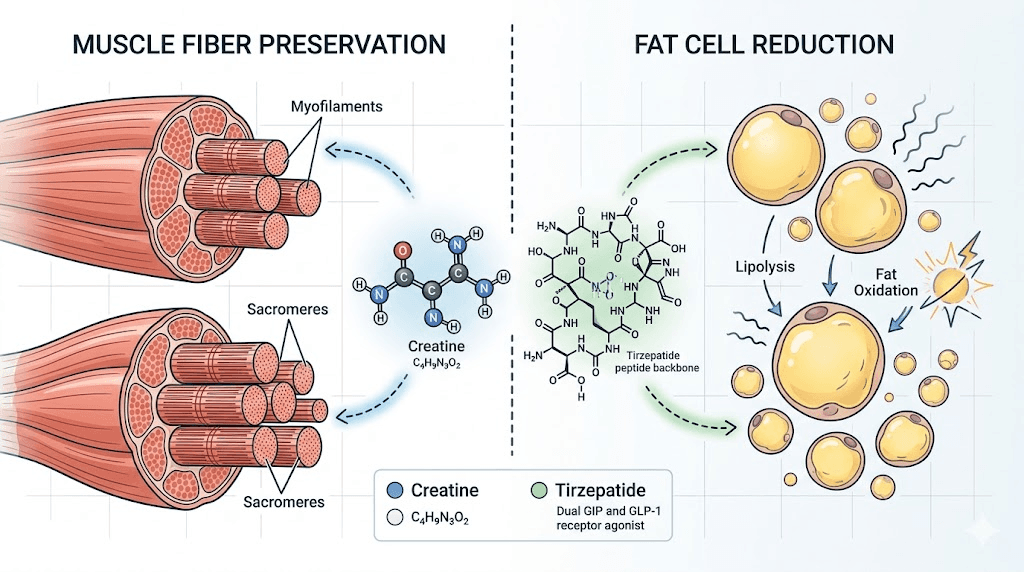
Tirzepatide works through dual GIP and GLP-1 receptor agonism, creating powerful appetite suppression and significant caloric deficits. The weight loss results are impressive. Clinical trials show average losses of 15-25% of body weight. But the body does not exclusively burn fat when calories drop that dramatically.
Lean soft tissue loss comprises 26-40% of total weight loss during treatment with GLP-1 receptor agonists and dual GLP-1/GIP receptor agonists. A case series published in PMC documented this pattern across multiple patients. The percentage varies based on protein intake, exercise habits, and individual physiology, but the trend is consistent. When you eat significantly less, your body cannibalizes muscle for energy.
This matters beyond aesthetics.
Muscle is metabolically active tissue. Every pound of muscle burns roughly 6-7 calories per day at rest, compared to about 2 calories per pound of fat. Lose ten pounds of muscle and your resting metabolic rate drops by 50-70 calories daily. That does not sound like much until you compound it over months and years. It is one of the primary reasons people regain weight after stopping GLP-1 medications. Their metabolism has slowed because they lost the metabolic engine, their muscle, along with the fat.
There is also the functional cost. Less muscle means less strength. Less strength means harder workouts, reduced bone density support, increased injury risk, and accelerated aging. For anyone over 40, muscle loss during rapid weight loss is not just a body composition concern. It is a health concern. The medical community even has a term for it: sarcopenic obesity, where someone carries excess fat but insufficient muscle. Maintaining weight loss after tirzepatide becomes exponentially harder when muscle has been sacrificed in the process.
What creatine actually does in your body
Creatine is not a steroid. It is not a stimulant. It is a naturally occurring compound your body already produces, about 1-2 grams per day, primarily in the liver, kidneys, and pancreas. You also get creatine from dietary sources like red meat and fish, though you would need to eat roughly two pounds of raw beef to get the 5 grams found in a single supplement serving.
Once ingested, creatine is absorbed in the small intestine and transported to muscle tissue, where about 95% of the body total supply is stored. Inside muscle cells, creatine binds with phosphate to form phosphocreatine, also called creatine phosphate. This is where the magic happens.
During intense exercise, your muscles burn through ATP (adenosine triphosphate) rapidly. ATP is the cellular energy currency. When it is depleted, you fatigue. Phosphocreatine donates its phosphate group to regenerate ATP, allowing you to push harder, lift heavier, and recover faster between sets. This ATP regeneration cycle is the primary mechanism behind creatine supplementation benefits.
But creatine does more than fuel workouts.
It increases intracellular water content in muscle cells, creating a more anabolic environment. It supports protein synthesis pathways. It reduces markers of muscle protein breakdown. And critically for tirzepatide users in a caloric deficit, it helps preserve existing muscle tissue even when energy intake is restricted. A meta-analysis examining calorie-restricted subjects found that those supplementing with creatine maintained up to 60% more lean mass than non-supplemented controls over 8 weeks. Combined with resistance training, the effect is even more pronounced, with creatine users maintaining 95% of their muscle mass compared to 85% in control groups.
Is it safe to take creatine with tirzepatide?
Yes. No documented drug interaction exists between creatine and tirzepatide.
This is not a gray area. These two compounds operate through entirely different mechanisms and metabolic pathways. Tirzepatide is a synthetic peptide administered subcutaneously that undergoes proteolytic degradation, meaning enzymes break it down in the body. Creatine is a small molecule absorbed in the small intestine and primarily taken up by skeletal muscle through sodium-dependent creatine transporters. They do not compete for the same receptors, the same enzymes, or the same metabolic pathways.
No clinical trials have specifically studied the combination. That is worth stating clearly. But the absence of specific trials does not indicate danger. It reflects the reality that creatine is classified as a dietary supplement, not a drug, and pharmaceutical companies do not fund studies on supplement-drug pairings when no mechanistic basis for interaction exists.
The FDA prescribing information for tirzepatide does not list creatine as a concern. Major drug interaction databases show no flags. And the millions of people who have used creatine alongside various medications for decades provide a substantial, if informal, safety record.
That said, there are practical considerations that matter. They just involve physiology rather than pharmacology. Understanding which supplements work well with tirzepatide requires looking at these practical overlaps rather than direct drug interactions.
The creatinine and kidney function conversation
This is the question your doctor will almost certainly raise, and it deserves a thorough answer.
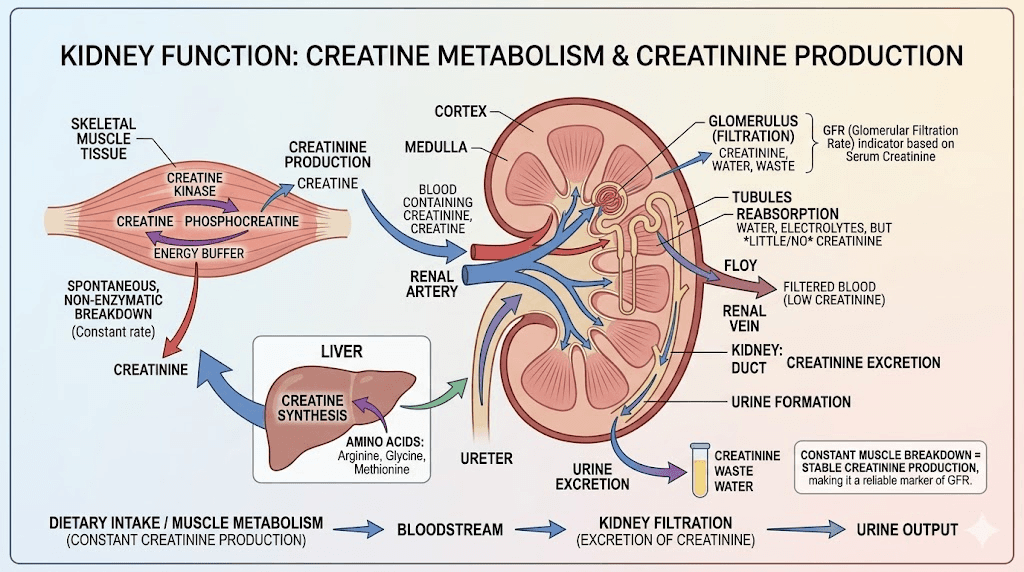
Creatine supplementation can modestly elevate serum creatinine levels in blood tests. Creatinine is a waste product of creatine metabolism, and when you supplement with more creatine, your body naturally produces more creatinine. Doctors use creatinine levels to estimate kidney function through a calculation called eGFR (estimated glomerular filtration rate). Higher creatinine typically suggests worse kidney function.
Here is the critical distinction: in creatine users, elevated creatinine reflects increased creatine metabolism, not impaired kidney function. Your kidneys are working fine. The test just looks abnormal because the input (creatine) has increased.
Multiple long-term studies have confirmed that creatine supplementation does not damage kidneys in healthy individuals. A 2019 review in the Journal of the International Society of Sports Nutrition concluded that creatine remains safe across multiple populations when consumed at recommended doses.
However, there are important nuances for tirzepatide users specifically. Gastrointestinal side effects like diarrhea and vomiting can cause dehydration. Dehydration can lead to prerenal acute kidney injury, a temporary reduction in kidney function caused by inadequate blood flow to the kidneys. If you are already dehydrated from tirzepatide side effects and then add creatine, which increases your water demands, the dehydration risk compounds.
The solution is straightforward: stay hydrated. Most experts recommend 3-4 liters of water daily when combining creatine with GLP-1 medications. If you experience significant gastrointestinal symptoms, prioritize fluid replacement before worrying about creatine timing.
For those with pre-existing kidney disease, particularly an eGFR below 45 mL/min/1.73m2, consult a nephrologist before starting creatine. For healthy individuals with normal kidney function, the combination poses no known renal risk. If your doctor orders bloodwork and your creatinine appears elevated, mention your creatine supplementation. They may choose to order a cystatin C-based eGFR or enzymatic creatinine assay, which provides accurate kidney function assessment unaffected by creatine intake.
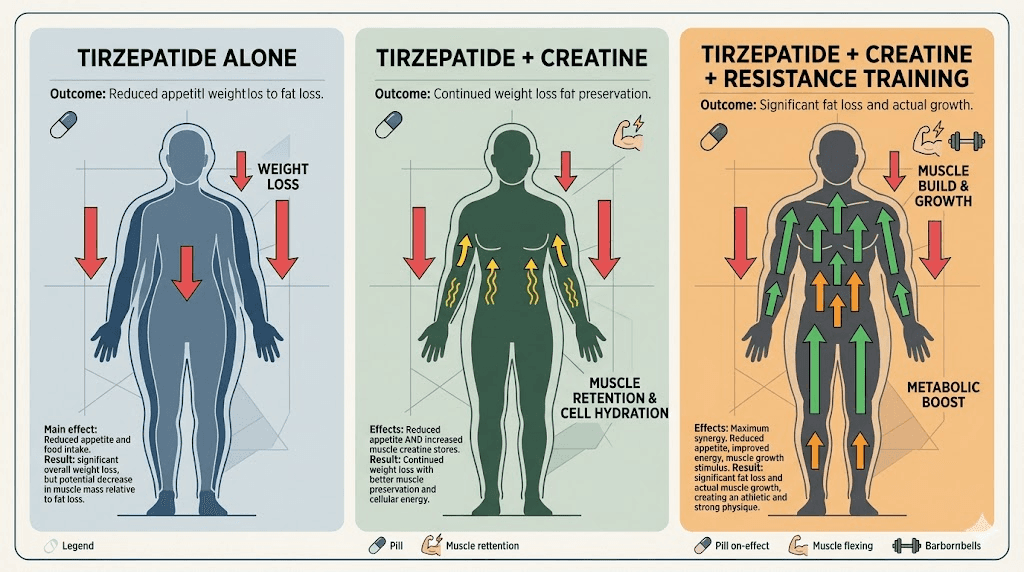
How creatine preserves muscle during tirzepatide weight loss
The synergy between creatine and tirzepatide is not complicated. It is complementary. Tirzepatide creates the caloric deficit that drives fat loss. Creatine provides the cellular support that protects muscle during that deficit. Each compound addresses a different side of the body composition equation.
The ATP regeneration pathway
When calories are restricted, your body has less available energy for everything, including maintaining muscle tissue. Phosphocreatine stores in muscle cells allow you to maintain training intensity even when energy intake is reduced. This matters because training intensity is one of the strongest signals telling your body to keep muscle.
Without adequate phosphocreatine, your sets get shorter, your weights get lighter, and the signal to preserve muscle weakens. Your body reads that as permission to break down muscle tissue for energy. Creatine supplementation keeps phosphocreatine stores saturated, maintaining the intensity signal even in a caloric deficit.
Cellular hydration and anabolism
Creatine draws water into muscle cells through osmosis. This cell swelling is not cosmetic. Research shows that increased intracellular hydration activates mTOR signaling pathways, which promote protein synthesis and inhibit protein breakdown. In simple terms, well-hydrated muscle cells are more resistant to catabolism.
This mechanism is especially valuable for tirzepatide users because the medication can alter hydration patterns through reduced fluid intake (you are eating and drinking less) and increased fluid losses (from gastrointestinal side effects). Creatine partially counteracts these cellular dehydration effects by pulling water directly into the tissues that need it most.
Protein synthesis support
Beyond ATP and hydration, creatine influences muscle protein synthesis directly. Studies show that creatine supplementation increases the expression of myogenic regulatory factors, the proteins that control muscle cell growth and differentiation. It also reduces myostatin levels, a protein that inhibits muscle growth.
During caloric restriction, protein synthesis rates naturally decline. Creatine helps maintain those rates closer to baseline, reducing the net protein loss that leads to muscle wasting. When combined with adequate protein intake and resistance training, this creates a protective effect that significantly limits lean mass loss.
The weight scale paradox: why creatine makes your tirzepatide results look worse (temporarily)
This trips up almost everyone.
You start creatine. Within the first week, the scale goes up 2-4 pounds. You panic. Is the tirzepatide not working anymore? Did the creatine make you gain fat? Should you stop?
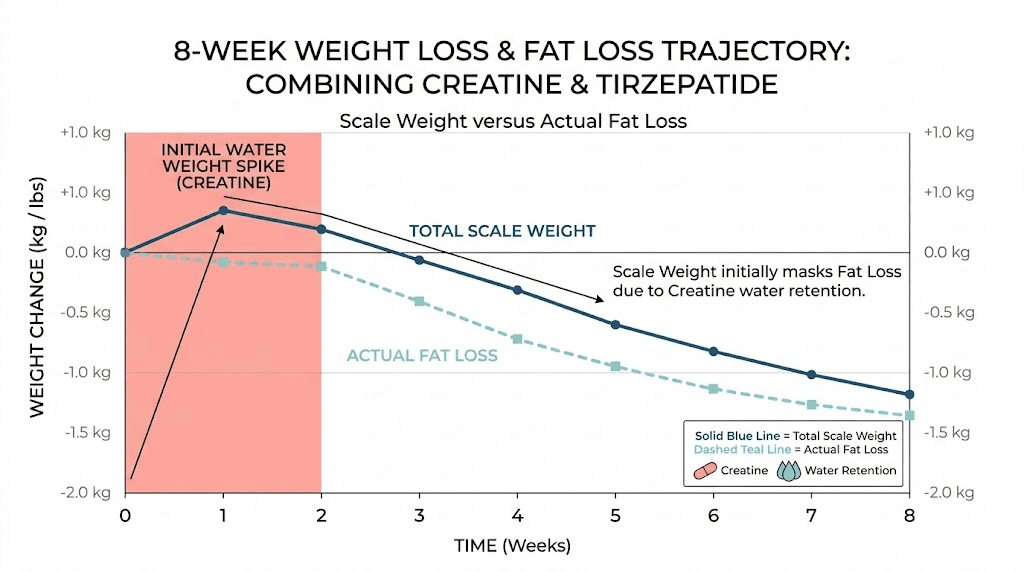
No. What you are seeing is intracellular water retention in muscle tissue. Creatine pulls water into muscle cells. That water has weight. But it is not fat, not subcutaneous water bloat, and not a sign of failure. It is actually a sign that the creatine is working correctly and your muscles are becoming more hydrated and protected.
Here is the practical reality. If tirzepatide is helping you lose 1-2 pounds of fat per week, and creatine adds 2-4 pounds of water weight in week one, the scale will show no progress or even a gain for the first 1-2 weeks. By week 3-4, the fat loss will outpace the water weight, and the scale resumes its downward trend. But during those early weeks, the scale lies.
This is why experienced researchers and fitness coaches recommend tracking body composition through multiple metrics, not just scale weight:
Waist circumference (measured at the navel, first thing in the morning)
Progress photos (same lighting, same time of day, every 2 weeks)
Strength measurements (are your lifts maintaining or improving?)
How clothes fit (often the most reliable day-to-day indicator)
DEXA scans (the gold standard for body composition, every 8-12 weeks)
If your waist is shrinking, your strength is holding, and your clothes are getting looser, the creatine-tirzepatide combination is working exactly as intended, regardless of what the scale says. People who feel like they are not losing weight on tirzepatide after starting creatine are almost always experiencing this temporary water weight effect.
Dosage protocols for creatine with tirzepatide
Creatine dosing is straightforward, but there are specific adjustments worth making when using it alongside tirzepatide.
The standard maintenance protocol (recommended)
Take 3-5 grams of creatine monohydrate daily. Every day, whether you train or not. Consistency matters more than timing. This is the protocol supported by the International Society of Sports Nutrition and decades of research.
For most people on tirzepatide, 5 grams daily is optimal. It saturates muscle creatine stores within 3-4 weeks without requiring a loading phase. The simplicity is the point. One scoop, once a day, mixed into water, a shake, or whatever you can tolerate given your current appetite and dietary patterns.
The loading phase debate
Traditional creatine protocols include a loading phase: 20 grams daily (split into four 5-gram doses) for 5-7 days, followed by the 3-5 gram maintenance dose. Loading saturates muscle stores faster, within about a week compared to 3-4 weeks with maintenance dosing alone.
For tirzepatide users, skipping the loading phase is generally the better choice. Here is why.
Twenty grams of creatine daily increases gastrointestinal stress. Tirzepatide already slows gastric emptying and commonly causes nausea, especially during dose escalation. Adding a large bolus of creatine to an already sensitive stomach is asking for trouble. The first few weeks on tirzepatide are when GI side effects peak. Loading creatine during this window often leads to worse nausea, bloating, and diarrhea.
The practical difference between loading and not loading is 2-3 weeks of saturation time. That is it. After 4 weeks on 5 grams daily, your muscle creatine stores will be identical to someone who loaded. The destination is the same. The loading route is just bumpier when tirzepatide is involved.
Timing considerations
Research on creatine timing is mixed, but practical experience with tirzepatide users suggests these guidelines:
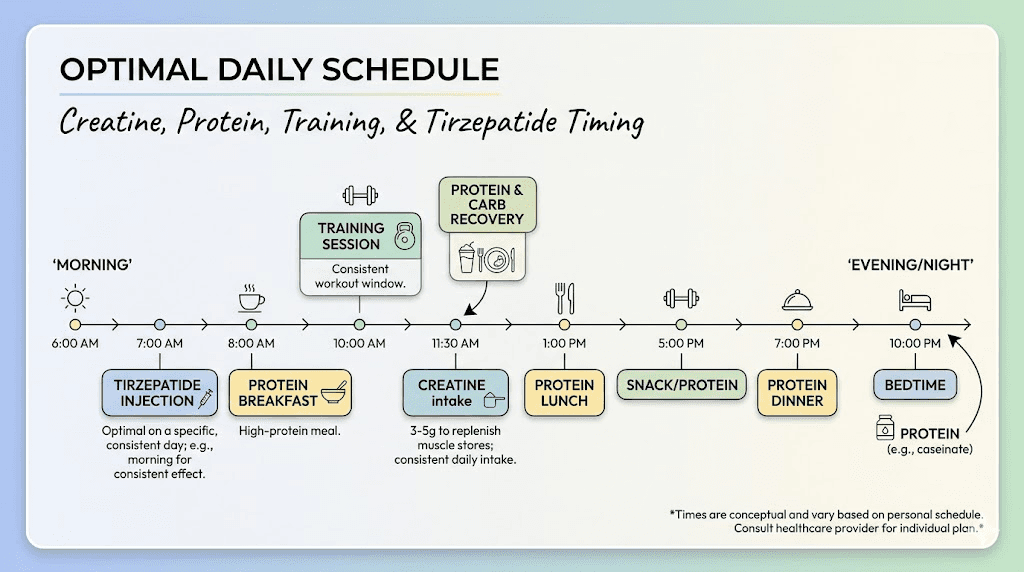
Take creatine with food. This improves absorption and reduces GI discomfort. The insulin response from a meal enhances creatine uptake into muscle cells. Since tirzepatide users often eat smaller meals, take creatine with your largest meal of the day or the meal you tolerate best.
Separate creatine from your tirzepatide injection by at least a few hours. Not because of a drug interaction, but because the hours immediately following injection are when nausea is most likely. Adding anything extra to your stomach during that window can worsen symptoms.
Post-workout is slightly preferable to pre-workout. A study in the Journal of the International Society of Sports Nutrition found marginally better results with post-workout creatine, likely due to increased blood flow and muscle uptake during recovery. But the difference is small. Taking it at any consistent time works.
Which form of creatine to use
Creatine monohydrate. Full stop.
The supplement industry has created dozens of creatine variants: creatine HCL, buffered creatine, creatine ethyl ester, creatine nitrate, and more. None have demonstrated superiority over plain creatine monohydrate in peer-reviewed research. Most cost significantly more. Some actually perform worse.
Creatine monohydrate is the form used in virtually every positive study. It is the cheapest, most available, and most proven option. Look for products with third-party testing certifications like NSF Certified for Sport or Informed Choice. These certifications verify purity and absence of contaminants, which matters more than fancy formulations.
Building your complete muscle preservation protocol
Creatine alone is not enough. It is one piece of a multi-component strategy for preserving muscle during tirzepatide treatment. Here is the complete framework.
Protein intake: the foundation
Nothing replaces adequate protein. Research consistently shows that consuming 1.2-1.6 grams of protein per kilogram of body weight daily significantly reduces lean mass loss during caloric restriction. For a 200-pound (91 kg) person, that translates to 109-146 grams of protein daily.
This is challenging on tirzepatide. Your appetite is suppressed. You may struggle to finish meals. Eating enough protein when you can barely eat at all feels impossible some days. Prioritize protein at every meal. If you can only eat 800 calories in a day, make 400 of them protein. Protein shakes designed for GLP-1 users can bridge the gap when solid food is unappealing. Mix your creatine into your protein shake to simplify the routine.
Resistance training: the non-negotiable signal
Your muscles need a reason to stick around. Resistance training provides that reason. Without it, no amount of creatine or protein will fully prevent muscle loss during significant caloric restriction.
Aim for 2-3 strength training sessions per week. Focus on compound movements: squats, deadlifts, bench press, rows, overhead press. These recruit the most muscle fibers and send the strongest preservation signal. You do not need to train to failure on every set. You need to maintain or approach your previous strength levels.
Expect some strength reduction during the initial weeks of tirzepatide, particularly during dose titration when side effects are strongest. This is normal. The goal is maintaining 85-90% of your baseline strength, not hitting personal records. Creatine helps with exactly this, keeping your phosphocreatine stores full so your working capacity remains as close to baseline as possible.
The complete daily protocol
Morning:
High-protein breakfast or shake (30-40g protein minimum)
Hydration: 500ml water upon waking
Mid-day (with largest meal):
5g creatine monohydrate mixed into food or beverage
Protein-rich meal (30-40g protein)
Training days (2-3x per week):
Compound resistance exercises for 45-60 minutes
Post-workout protein shake (25-30g protein)
Throughout the day:
3-4 liters of water total
Remaining protein distributed across meals/snacks
Tirzepatide injection day:
Take creatine at a meal several hours before or after injection
Reduce training intensity if experiencing significant nausea
Prioritize hydration, especially if GI symptoms are present
When to start creatine relative to tirzepatide
Timing the introduction of creatine matters more than most guides acknowledge.
The most conservative approach, and the one recommended by several clinical sources, is to start tirzepatide first and wait 8-12 weeks before adding creatine. This allows your body to adapt to the medication, lets gastrointestinal side effects stabilize, and gives you a clear baseline for how your body responds to tirzepatide alone.
The more aggressive approach is to start creatine immediately alongside tirzepatide, or to continue existing creatine supplementation when beginning the medication. If you have been taking creatine for months or years and are now starting tirzepatide, there is no reason to stop. Your body is already adapted to creatine, and removing it would actually accelerate muscle loss during the initial weight loss phase.
The middle ground, which works well for most people:
Start tirzepatide at the initial 2.5mg dose. Wait until you have been through at least one dose escalation and your GI symptoms are manageable, typically 4-6 weeks. Then introduce creatine at 3 grams daily (not 5) for the first two weeks. If tolerated, increase to 5 grams daily. This gradual introduction minimizes GI overlap while getting creatine on board before significant muscle loss occurs.
The worst approach? Starting both on the same day at full doses. Creatine loading (20g/day) combined with a first tirzepatide dose is a recipe for miserable gastrointestinal symptoms. One variable at a time allows you to identify what is causing what.
Managing gastrointestinal side effects when combining both
Let us address the elephant in the room. Tirzepatide causes GI side effects in a significant percentage of users. Nausea, diarrhea, constipation, bloating, and acid reflux are all common, especially during dose titration. Creatine, while generally well-tolerated, can contribute to stomach discomfort, bloating, and loose stools in some people, particularly at higher doses.
The combination does not create new side effects. But it can amplify existing ones. Here is how to manage it.
Stomach sensitivity strategies
Never take creatine on an empty stomach. Always consume it with food. The food buffer reduces GI irritation significantly. If your appetite is severely suppressed from tirzepatide, even a small snack, like a few crackers with peanut butter or a small yogurt, is enough to buffer the creatine.
Dissolve creatine completely. Undissolved creatine granules sitting in your stomach increase the likelihood of nausea and bloating. Stir it thoroughly into warm water (which dissolves it faster than cold), or blend it into a shake. Some people find that mixing creatine into their morning oatmeal or yogurt eliminates GI issues entirely.
Split your dose if needed. If 5 grams at once bothers your stomach, split it into two 2.5-gram doses taken at different meals. The total daily amount matters more than the single-dose amount.
Hydration management
Dehydration is the silent amplifier of GI problems when combining creatine and tirzepatide. Both increase your water needs, creatine by pulling water into muscle cells, tirzepatide by causing potential fluid losses through GI symptoms.
Aim for 3-4 liters of water daily. Track it if needed. Early signs of dehydration include dark urine, headaches, dizziness, and worsening nausea. If you notice these while on both compounds, increase fluid intake before adjusting anything else. Dry mouth from tirzepatide is another signal to drink more.
Electrolytes matter too. Plain water is not enough if you are losing significant fluids through GI symptoms. Add a sugar-free electrolyte supplement or simply include sodium, potassium, and magnesium through food or supplementation. This prevents the cramping and weakness that dehydration plus creatine plus caloric restriction can cause.
Creatine and tirzepatide for different goals
Not everyone using tirzepatide has the same objectives. The way you approach creatine supplementation should reflect your specific goals.
Goal: maximum fat loss with muscle preservation
This is the most common scenario. You want to lose as much fat as possible while keeping the muscle you have.
Protocol:
Creatine: 5g daily (no loading)
Protein: 1.4-1.6g per kg body weight
Resistance training: 3x per week, compound movements, moderate to heavy loads
Tracking: Waist circumference, strength logs, monthly progress photos
Duration: Continue creatine throughout entire tirzepatide treatment and beyond
This protocol maximizes the muscle-sparing effect of creatine while tirzepatide handles the fat loss side. Expect to preserve 90-95% of your muscle mass compared to 75-85% without creatine and training. The before and after results will look dramatically different with this approach versus tirzepatide alone.
Goal: body recomposition (lose fat while building some muscle)
True body recomposition while on tirzepatide is difficult but not impossible, especially for those who are new to resistance training or returning after a long break.
Protocol:
Creatine: 5g daily
Protein: 1.6g per kg body weight (the higher end is critical for recomp)
Resistance training: 3-4x per week, progressive overload, full-body or upper/lower split
Tracking: DEXA scans every 8-12 weeks, strength progression logs
Duration: Ongoing
Creatine provides the performance edge that makes progressive overload possible even in a deficit. Without it, adding weight to the bar while eating significantly less is nearly impossible. With creatine maintaining your phosphocreatine stores, you can continue to challenge your muscles and potentially stimulate new growth, even as fat comes off. This is one of the benefits of tirzepatide that goes beyond simple weight loss when combined with the right supplement strategy.
Goal: athletic performance maintenance
Some tirzepatide users are athletes or highly active individuals who started the medication for metabolic health, body composition optimization, or appetite regulation. Their concern is not just muscle loss but performance decline.
Protocol:
Creatine: 5g daily, post-training on workout days
Protein: 1.6-2.0g per kg body weight
Training: Sport-specific, maintained as close to pre-tirzepatide levels as possible
Additional: HMB (beta-hydroxy beta-methylbutyrate) at 3g daily may provide additional anti-catabolic support
Monitoring: Performance metrics specific to sport
For athletes, creatine is non-negotiable during tirzepatide use. The performance benefits are too significant to leave on the table, and the muscle preservation effects directly support athletic capacity. Understanding how tirzepatide affects energy levels helps athletes plan training around potential low-energy windows.
What the research actually says about creatine during caloric restriction
Let us get specific about the evidence, because vague claims help nobody.
Lean mass preservation
A meta-analysis published in the International Journal of Sport Nutrition and Exercise Metabolism examined multiple trials of creatine supplementation during calorie-restricted periods. Subjects in a 20-30% caloric deficit who supplemented with creatine maintained up to 60% more lean mass than non-supplemented controls over 8-week periods. The effect was dose-dependent and consistent across different populations.
Strength maintenance
In calorie-restricted conditions, creatine users maintained approximately 95% of their baseline strength in compound movements over 8 weeks, compared to roughly 85-88% in placebo groups. This 7-10% difference in strength retention translates to meaningfully different training loads, which in turn affects the muscle preservation signal.
Body composition improvements
Several studies demonstrate that creatine supplementation during energy restriction leads to greater fat loss as a percentage of total weight lost. In other words, more of the weight you lose is fat and less is muscle. One trial showed that the creatine group lost 7.2% body fat versus 5.1% in the placebo group over 12 weeks, despite similar total weight loss. The creatine group simply retained more muscle while shedding more fat.
The GLP-1 specific evidence gap
No randomized controlled trial has specifically examined creatine supplementation in a GLP-1 agonist population. This is a limitation worth acknowledging. However, the caloric restriction literature is directly applicable because tirzepatide weight loss is fundamentally driven by reduced caloric intake. The metabolic context, eating significantly less than your body needs, is the same whether the deficit comes from willpower, meal planning, or pharmaceutical appetite suppression.
A narrative review published in a nutritional sciences journal recommended that creatine supplementation with resistance training should be considered as part of a comprehensive GLP-1 receptor agonist care plan, based on the existing evidence for muscle preservation during caloric restriction.
Other supplements worth considering alongside creatine and tirzepatide
Creatine is the strongest evidence-based supplement for muscle preservation, but it works best as part of a broader strategy. Here are the supplements that complement it during tirzepatide treatment, ranked by evidence quality.
Tier 1: strong evidence
Whey protein isolate. Convenient, fast-absorbing, and effective at reaching protein targets when appetite is suppressed. Mixing creatine into whey shakes is the simplest way to take both. Protein shakes formulated for GLP-1 users address specific considerations like reduced appetite and GI sensitivity.
Vitamin D3. Deficiency is common and worsens muscle protein synthesis. Most adults benefit from 2000-4000 IU daily. Important for bone density, which can decline alongside muscle loss during rapid weight loss.
Omega-3 fatty acids. EPA and DHA support anti-inflammatory pathways and may directly support muscle protein synthesis. 2-3 grams of combined EPA/DHA daily from fish oil or algae supplements. These also support the cardiovascular benefits that tirzepatide provides.
Tier 2: moderate evidence
HMB (beta-hydroxy beta-methylbutyrate). A leucine metabolite with anti-catabolic properties. Most beneficial during severe caloric restriction or for older adults. 3g daily, split into three 1g doses. Evidence is stronger for untrained individuals and those in aggressive deficits.
Magnesium. Depletion is common during GLP-1 treatment due to reduced food intake and GI losses. Supports muscle function, sleep quality, and reduces cramping. Magnesium glycinate or threonate forms are best absorbed. 200-400mg daily.
Vitamin B12. GLP-1 medications can reduce B12 absorption through altered gastric function. B12 is essential for energy metabolism and nervous system function. Many compounded tirzepatide formulations already include B12 for this reason. If yours does not, consider 1000mcg sublingual methylcobalamin daily.
Tier 3: emerging evidence
Glycine. An amino acid increasingly included in compounded GLP-1 formulations. Supports collagen synthesis, sleep quality, and may have mild anti-inflammatory effects. Some evidence suggests it supports lean mass during caloric restriction. 3-5g daily.
Berberine. May complement tirzepatide metabolic effects, though evidence for muscle preservation is limited. Exercise caution with this combination and discuss with your provider, as berberine can affect blood sugar levels.
For a complete overview of effective supplements during treatment, the supplements to take with tirzepatide guide covers each option in detail.
Monitoring your results: what to track and when
Combining creatine and tirzepatide requires smarter tracking than just stepping on a scale. Here is a comprehensive monitoring framework.
Weekly measurements
Body weight (understand the creatine water weight caveat): Weigh yourself under the same conditions daily, same time, same clothing (or none), after using the bathroom. Average the seven daily weights for a weekly number. This smooths out water fluctuations and gives a reliable trend line. The first 2-3 weeks after starting creatine will show inflated numbers. Do not adjust tirzepatide dosing based on this temporary effect.
Waist circumference: Measure at the navel, relaxed, first thing in the morning. This is the single best proxy for fat loss that creatine water weight does not affect. If your waist is shrinking, you are losing fat. Period.
Strength logs: Track your working weights and reps for key compound movements. If these numbers are stable or improving, your muscle preservation strategy is working. If they drop significantly (more than 15-20% from baseline), something needs adjustment, likely protein intake or training volume.
Monthly measurements
Progress photos: Same angle, same lighting, same time of day. Monthly photos reveal changes that daily weight fluctuations obscure. The visual difference between losing 20 pounds with muscle preservation versus without is striking.
Blood work: Monitor kidney function (creatinine, eGFR), blood glucose, and metabolic markers. Mention creatine supplementation to your provider so they can interpret creatinine values appropriately. If your provider uses standard blood panels, creatinine-based eGFR may appear artificially low. Request cystatin C-based eGFR if kidney function is a concern.
Quarterly measurements
DEXA scan: The gold standard for body composition. A DEXA scan separates fat mass, lean mass, and bone mineral density with high accuracy. Getting one before starting the creatine-tirzepatide combination and every 3 months thereafter provides the most reliable data on whether your muscle preservation strategy is working.
Common mistakes when combining creatine and tirzepatide
After reviewing hundreds of forum posts, community discussions, and clinical observations, these are the mistakes people make most frequently.
Mistake 1: stopping creatine because of the scale
The 2-4 pound water weight gain triggers panic. People stop creatine, lose the water weight, feel relieved that the scale dropped, and unknowingly accelerate their muscle loss. The scale weight they lost by stopping creatine was water, not fat. The muscle protection they lost by stopping was real. This is the most common and most costly mistake.
Mistake 2: loading creatine during tirzepatide dose escalation
Dose escalation is when tirzepatide GI side effects are worst. Adding 20g of creatine daily on top of that creates unnecessary misery. Start with maintenance dosing (3-5g) and introduce it during a stable dosing period. The tirzepatide dosage schedule has built-in escalation phases, and creatine introduction should happen between escalations, not during them.
Mistake 3: neglecting hydration
Creatine needs water. Tirzepatide causes water loss through GI effects. The combination demands intentional hydration. Under-hydrating leads to worse GI symptoms, headaches, kidney stress, and reduced creatine effectiveness. Track your water intake for the first month until adequate hydration becomes habitual.
Mistake 4: using creatine as a substitute for training
Creatine supplements muscle retention. It does not replace the stimulus. Without resistance training, creatine provides some benefit through its cellular hydration and anti-catabolic properties, but the effect is substantially less. The combination of creatine plus resistance training is what produces the 95% muscle retention numbers cited in research. Creatine alone is maybe 70-75%.
Mistake 5: not eating enough protein
Creatine supports the machinery of muscle preservation, but protein provides the raw materials. If you are eating 50 grams of protein daily while on tirzepatide (common due to appetite suppression), creatine cannot fully compensate. The protein must be there. Use shakes, high-protein snacks, and strategic meal planning from the tirzepatide diet plan guide to hit your targets.
Mistake 6: choosing expensive creatine variants
Creatine HCL, buffered creatine, creatine ethyl ester, liquid creatine. None of these outperform plain creatine monohydrate. Some are less effective. All cost more. Save your money and buy a well-tested creatine monohydrate product. The ingredient is the same regardless of price point, just verify third-party testing.
Creatine and tirzepatide for specific populations
Women
Creatine is equally safe and effective for women. The concern that creatine causes bulking or excessive water retention in women is largely overstated. Women typically experience 1-2 pounds of water weight from creatine versus 2-4 in men, reflecting smaller total muscle mass. The muscle preservation benefits are proportionally similar.
For women on tirzepatide, the muscle preservation argument is actually stronger. Women naturally have less muscle mass than men, meaning they can less afford to lose it. Sarcopenic changes from rapid weight loss are more functionally impactful for women over 40, affecting bone density, fall risk, and metabolic rate disproportionately. Women using tirzepatide who are concerned about hormonal changes during weight loss should know that creatine does not affect menstrual cycles or hormonal balance.
Older adults (50+)
This population benefits most from the creatine-tirzepatide combination, yet is least likely to use it. Age-related muscle loss (sarcopenia) is already occurring. Adding rapid pharmacological weight loss accelerates it. Creatine supplementation in older adults has robust evidence for improving strength, functional capacity, and quality of life, independent of its fat-loss context.
Older adults on tirzepatide should prioritize kidney function monitoring and hydration even more carefully. Start with 3g daily rather than 5g, and increase only if tolerated well. The eventual transition off tirzepatide is smoother when muscle has been preserved throughout treatment.
People with type 2 diabetes
Tirzepatide is FDA-approved for type 2 diabetes (as Mounjaro) as well as weight loss (as Zepbound). Creatine may offer additional benefits for diabetic individuals, as some research suggests it can improve glucose uptake into muscle cells and modestly improve glycemic control. These effects are additive to, not interfering with, tirzepatide metabolic benefits.
However, diabetic individuals should monitor blood glucose more closely when starting creatine, as the combined effect on glucose metabolism could theoretically increase hypoglycemia risk, especially if also taking insulin or sulfonylureas. Discuss with your endocrinologist before adding creatine if you have diabetes.
How creatine compares to other muscle preservation strategies on tirzepatide
Creatine is not the only option for preserving muscle during GLP-1 treatment. Here is how it compares to alternatives.
Strategy | Evidence strength | Muscle preservation | Cost | Side effects | Best for |
|---|---|---|---|---|---|
Creatine monohydrate | Strong | High (60% more lean mass preserved) | $10-15/month | Minimal (water weight, mild GI) | Everyone |
High protein intake | Very strong | Very high | $50-100/month (supplements) | None | Everyone (foundational) |
Resistance training | Very strong | Very high | $0-80/month (gym) | Soreness, time investment | Everyone (foundational) |
HMB | Moderate | Moderate | $20-30/month | Minimal | Older adults, severe deficits |
Moderate | Low to moderate | $15-25/month | Minimal | Fat metabolism support | |
BPC-157 | Emerging | Low (indirect, via recovery) | Variable | Minimal | Injury recovery |
The optimal approach combines the top three: creatine, high protein, and resistance training. Each addresses a different mechanism. Creatine supplies cellular energy and hydration. Protein provides building materials. Training provides the preservation signal. Remove any one and the others work less effectively.
For those exploring the broader landscape of supplements compatible with GLP-1 medications, creatine consistently ranks among the most evidence-based and cost-effective options available.
What happens when you stop creatine while on tirzepatide
Understanding what happens if you discontinue creatine is important for making informed decisions.
Within 4-6 weeks of stopping creatine, your muscle creatine stores return to baseline levels. The 2-4 pounds of intracellular water that creatine maintained will be released, causing a temporary drop in scale weight. This is not fat loss. It is the reverse of the water weight you gained when starting.
More importantly, you lose the muscle preservation benefits. Your phosphocreatine stores deplete, reducing training capacity. The cellular hydration advantage disappears. The anti-catabolic signaling weakens. If you are still on tirzepatide and still in a caloric deficit, your rate of muscle loss will increase relative to when you were supplementing.
There is no physiological reason to cycle creatine. It is not like stimulants where your body builds tolerance. Creatine benefits persist as long as you take it, and there is no evidence of long-term risks from continuous use. The International Society of Sports Nutrition position stand on creatine safety confirms this for supplementation periods extending over several years.
If you need to stop temporarily, for a medical procedure, travel, or personal choice, resume as soon as possible. Your stores will re-saturate within 3-4 weeks at maintenance dosing (5g daily) or about 1 week with a loading protocol.
The creatinine blood test issue: a deeper look
This deserves its own section because it causes unnecessary anxiety and, in some cases, leads doctors to advise against creatine when it is actually perfectly safe.
Creatinine is a waste product of creatine metabolism. Your kidneys filter creatinine from the blood and excrete it in urine. Doctors measure serum creatinine levels to estimate how well your kidneys are filtering, expressed as eGFR.
The math is simple: more creatine intake equals more creatinine production equals higher serum creatinine levels. When a doctor sees elevated creatinine on your blood panel, the default interpretation is impaired kidney function. But in creatine users, the elevation is caused by increased input, not decreased clearance.
Here is a practical example. A healthy 30-year-old male on creatine might show a serum creatinine of 1.4 mg/dL, which translates to an eGFR of approximately 65 mL/min/1.73m2. Technically, this falls into the "mildly decreased" kidney function category. Without creatine supplementation, the same person might show creatinine of 0.9 mg/dL and eGFR of 105, which is perfectly normal.
The solution involves three options:
Option 1: Inform your doctor. Simply telling your provider that you take creatine allows them to interpret the results correctly. Many will note this in your chart and adjust their assessment accordingly.
Option 2: Cystatin C-based eGFR. Cystatin C is another protein filtered by the kidneys, but unlike creatinine, its levels are not affected by creatine supplementation, muscle mass, or diet. A cystatin C-based eGFR provides accurate kidney function assessment regardless of creatine use.
Option 3: Stop creatine temporarily. If accurate creatinine-based testing is needed, stopping creatine for 30 days before bloodwork allows creatinine to normalize. This is inconvenient but eliminates the confounding variable entirely.
For tirzepatide users specifically, kidney monitoring is already part of standard care. Tirzepatide itself shows no direct nephrotoxicity, but the dehydration risk from GI side effects warrants periodic kidney function checks. Adding creatine to the mix makes accurate kidney testing more important, not because of added kidney risk, but because of the measurement artifact.
Creatine and tirzepatide: addressing specific concerns
Will creatine affect how well tirzepatide works for weight loss?
No. Creatine does not interfere with tirzepatide mechanism of action, reduce appetite suppression, or alter the metabolic effects of the medication. The fat loss from tirzepatide continues at the same rate whether you take creatine or not. The only difference is that creatine protects muscle during that fat loss process and temporarily adds water weight that can mask the scale number.
Can creatine worsen tirzepatide nausea?
It can if taken improperly. Taking creatine on an empty stomach, in undissolved form, or at high doses (loading phase) can worsen existing GI sensitivity from tirzepatide. Taken with food at maintenance doses (3-5g), most people experience no additional nausea.
Should I take creatine on tirzepatide injection day?
Yes, but time it away from the injection. The hours immediately following tirzepatide injection are when nausea is most likely. Take your creatine earlier in the day with a meal, or later in the evening after symptoms have settled. The key is consistency, skipping creatine on injection days interrupts the daily routine that keeps your stores saturated.
Does creatine interact with compounded tirzepatide?
No differently than with pharmaceutical tirzepatide. Whether your tirzepatide is compounded with glycine and B12, niacinamide, levocarnitine, or methylcobalamin, creatine remains safe to take alongside it. The active ingredient, the tirzepatide molecule, is the same regardless of compounding additions, and creatine does not interact with any common compounding agents.
Is creatine safe with semaglutide too?
Yes. The safety profile is identical for all GLP-1 receptor agonists. Whether you are on tirzepatide, semaglutide, or considering retatrutide, creatine supplementation follows the same guidelines. Our creatine and GLP-1 guide covers the broader category in depth.
Real-world protocol: putting it all together
Here is a complete, step-by-step protocol for combining creatine and tirzepatide based on the research and practical considerations covered throughout this guide.
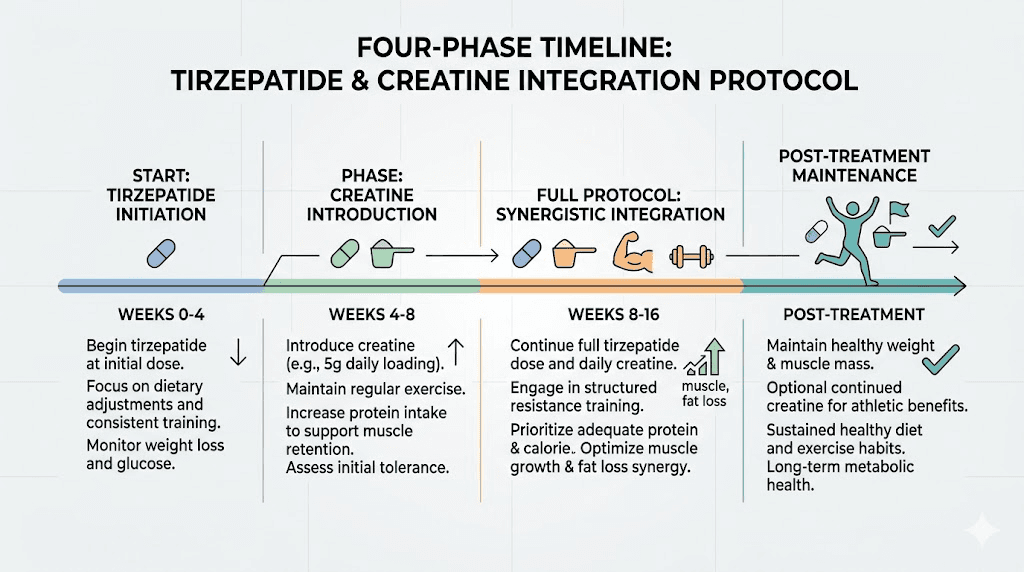
Phase 1: tirzepatide establishment (weeks 1-4)
Focus exclusively on adjusting to tirzepatide. Start at your prescribed dose, manage side effects, establish your eating patterns, and begin or maintain resistance training 2-3 times per week. Prioritize protein intake from day one. Do not add creatine yet.
Track baseline measurements: body weight (daily average), waist circumference, key lift numbers, and progress photos.
Phase 2: creatine introduction (weeks 5-6)
Once GI side effects are manageable (not necessarily gone, just manageable), introduce creatine at 3 grams daily. Take it with your most substantial meal. Increase water intake to 3-4 liters daily. Continue all tracking.
Expect the scale to stall or increase slightly. This is the water weight loading into muscle cells. Your waist measurement should continue decreasing. If it does, everything is working.
Phase 3: full protocol (weeks 7+)
Increase creatine to 5 grams daily if 3 grams was well tolerated. Maintain resistance training, protein intake, and hydration. By this point, your creatine stores should be nearing saturation, and the water weight shift will have stabilized.
Continue this protocol throughout your tirzepatide treatment. There is no need to cycle off creatine or take breaks. Consistency is the single most important factor for creatine efficacy.
Phase 4: post-tirzepatide transition
When you eventually taper off tirzepatide, continue creatine supplementation. The muscle you preserved during treatment becomes even more valuable during maintenance. Higher muscle mass means higher resting metabolic rate, which directly supports weight maintenance without pharmaceutical appetite suppression.
How creatine fits into the broader tirzepatide supplement stack
Many tirzepatide users take multiple supplements. Understanding how creatine fits into the broader picture prevents redundancy and ensures each supplement contributes meaningfully.
A well-structured supplement stack for tirzepatide users might include:
Foundation tier (everyone should consider):
Creatine monohydrate (5g/day) for muscle preservation
Whey protein isolate (as needed to hit protein targets)
Multivitamin (to cover micronutrient gaps from reduced food intake)
Vitamin D3 (2000-4000 IU/day)
Performance tier (active individuals):
Omega-3 fatty acids (2-3g EPA/DHA daily)
Magnesium glycinate (200-400mg/day)
Vitamin B12 (1000mcg/day if not included in compounded formulation)
Optimization tier (advanced users):
HMB (3g/day for additional anti-catabolic support)
Glycine (3-5g/day for collagen support and sleep)
Fiber supplement (for GI regularity)
Probiotics (for gut health during GLP-1 treatment)
Creatine is the most cost-effective supplement on this list. At roughly $10-15 per month for a high-quality product, it provides outsized returns in terms of muscle preservation, strength maintenance, and body composition improvement. Few supplements offer this evidence-to-cost ratio.
SeekPeptides members access detailed supplement protocols, stacking guides, and evidence-based recommendations for optimizing their peptide and GLP-1 treatment outcomes, including comprehensive guidance on combining creatine with various peptide protocols.
The long game: why muscle preservation during tirzepatide matters years from now
It is easy to focus on the immediate: the number on the scale, the way your clothes fit, the compliments from friends. But the muscle preservation decisions you make during tirzepatide treatment have consequences that extend years into the future.
Consider two hypothetical individuals. Both start at 250 pounds. Both use tirzepatide and lose 50 pounds over 6 months.
Person A takes tirzepatide alone. They lose 50 pounds total: approximately 32 pounds of fat and 18 pounds of lean mass (36% lean mass loss, consistent with research averages). Their resting metabolic rate drops by roughly 126 calories per day from the muscle loss alone.
Person B takes tirzepatide with creatine, high protein, and resistance training. They lose 50 pounds total: approximately 45 pounds of fat and 5 pounds of lean mass (10% lean mass loss). Their resting metabolic rate drops by only 35 calories per day from muscle loss.
After stopping tirzepatide, Person A has a 91 calorie per day metabolic disadvantage compared to Person B, purely from muscle loss differences. Over a year, that is roughly 33,000 calories, equivalent to about 9.5 pounds of potential weight regain. Over five years, the gap widens to 47 pounds of metabolic disadvantage.
This is why the weight maintenance phase after tirzepatide is dramatically easier for people who preserved their muscle. Their metabolic engine is still running at near-baseline capacity. The creatine, the protein, the training, they were not just about looking better during weight loss. They were about making the results sustainable.
For researchers and individuals serious about optimizing their peptide and supplement protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
Can I take creatine on an empty stomach while on tirzepatide?
Taking creatine on an empty stomach is not recommended during tirzepatide treatment. The combination of creatine and the medication GI effects increases the likelihood of nausea and stomach discomfort. Always take creatine with food, even if it is just a small snack. If solid food is difficult, mixing creatine into a protein shake works well.
How much water should I drink when taking creatine and tirzepatide together?
Aim for 3-4 liters of water daily. Creatine increases intracellular water demands while tirzepatide can cause dehydration through gastrointestinal side effects. Monitor urine color as a hydration indicator. Pale yellow is ideal. Dark yellow means you need to drink more immediately.
Will creatine make me look bloated on tirzepatide?
No. Creatine causes intracellular water retention inside muscle cells, not subcutaneous water retention that causes visible bloating. If anything, the increased muscle fullness from creatine can make you look more toned as fat decreases. The bloating some people experience is almost always from tirzepatide GI effects, not creatine.
Should I stop creatine before blood tests while on tirzepatide?
Not necessarily. Simply inform your doctor that you supplement with creatine so they can interpret creatinine-based kidney function tests accurately. If precise kidney function assessment is needed, your doctor can order a cystatin C-based eGFR test, which is unaffected by creatine supplementation. Stopping creatine for 30 days before testing is another option but disrupts your supplementation routine.
Can I take creatine if I am just starting tirzepatide at 2.5mg?
It is better to wait 4-6 weeks until your body has adjusted to the medication. The initial dose phase is when GI side effects are most unpredictable. Starting both simultaneously makes it difficult to determine which compound is causing any issues you experience. If you were already taking creatine before starting tirzepatide, you can continue it.
Does creatine help with tirzepatide fatigue?
Fatigue on tirzepatide is primarily caused by reduced caloric intake and the metabolic adjustments your body makes during significant weight loss. Creatine may help indirectly by improving exercise capacity and maintaining muscle energy stores, but it is not a direct solution for medication-related fatigue. Adequate protein, hydration, sleep, and gradual dose titration address fatigue more directly.
Is there a best brand of creatine for tirzepatide users?
Any creatine monohydrate with third-party testing certification (NSF Certified for Sport, Informed Choice, or USP verified) is appropriate. Creapure, a branded form of creatine monohydrate made in Germany, is considered the gold standard for purity. Avoid proprietary blends, flavored versions with artificial sweeteners (which can worsen GI issues), and non-monohydrate forms that lack evidence.
Can I take creatine with oral tirzepatide?
Yes. Whether you use injectable or oral tirzepatide, creatine supplementation follows the same guidelines. The route of administration does not change the safety or compatibility of the combination.
External resources
ScienceDirect: Dietary Supplement Considerations During GLP-1 Receptor Agonist Treatment
National Institute of Diabetes and Digestive and Kidney Diseases: Kidney Disease Information
In case I do not see you, good afternoon, good evening, and good night. May your muscles stay preserved, your body composition stay improving, and your protocols stay evidence-based.