Feb 8, 2026
Some researchers see results in 2 weeks. Others wait months. The difference? One word: dosage.
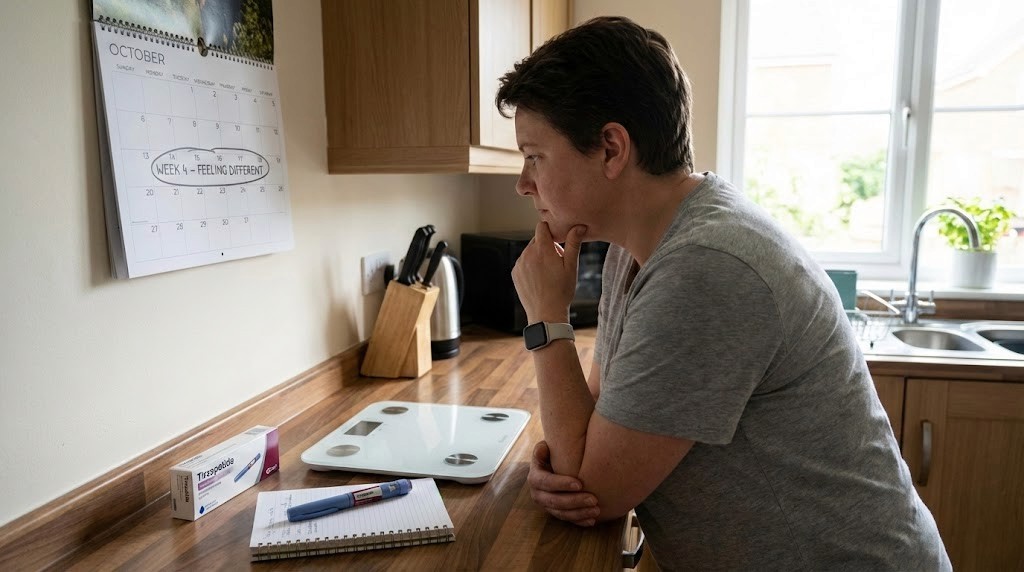
Tirzepatide is not a light switch. You do not inject it once and wake up lighter. Most people feel appetite changes within 1-2 weeks. Measurable weight loss shows up around week 4. But the question everyone actually wants answered is this: when will I see the results I came for? The answer depends on dose, metabolism, and how long you stick with the escalation schedule. This guide breaks down the real timeline based on clinical trial data, not marketing promises or social media anecdotes.
We will walk through the week-by-week progression, explain why the dose escalation takes 20 weeks to reach maximum strength, and show you what the SURMOUNT trials revealed about speed of response. You will also learn why some people lose 5% body weight by week 12 while others need 72 weeks to hit the same target. If you have been wondering whether tirzepatide is working fast enough for you, or if your progress is normal, this article gives you the data to compare against.
The real timeline: what the clinical trials show
The SURMOUNT-1 trial tracked 2,539 people for 72 weeks. Participants started at 2.5 mg weekly and escalated to either 5 mg, 10 mg, or 15 mg over a 20-week titration period. Results were measured at multiple checkpoints to capture the speed of response. Here is what happened at each milestone.
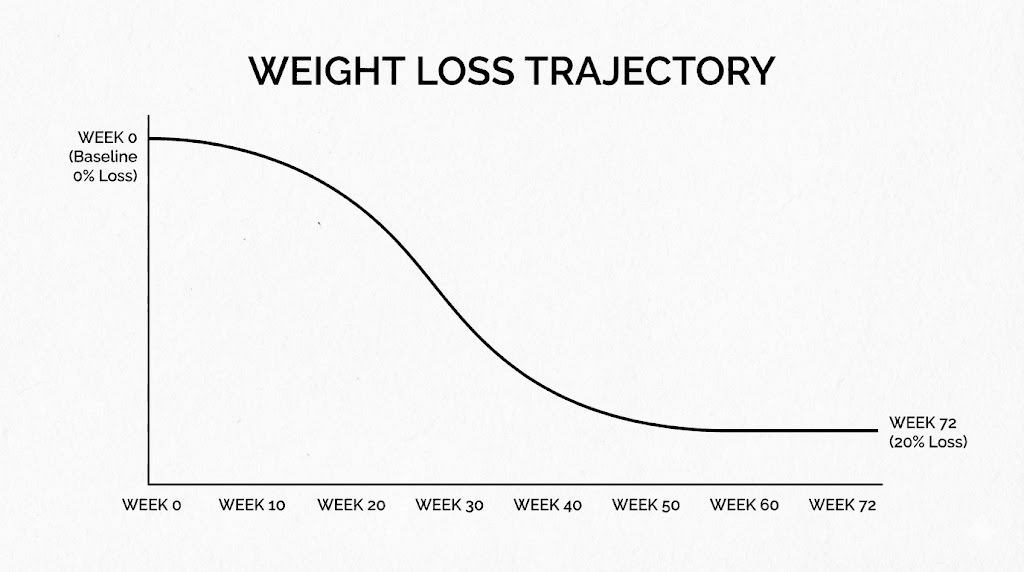
At week 4, the average weight loss was about 4% of starting body weight. At week 8, it reached 6%. By week 12, participants on the 10 mg dose had lost an average of 8% body weight, while those on 15 mg hit 9%. The majority of weight loss occurred between weeks 12 and 40, with the curve flattening out after 60 weeks. Final results at 72 weeks showed 16% weight loss for the 5 mg group, 21.4% for 10 mg, and 22.5% for 15 mg.
The SURMOUNT-4 trial looked at what happens when you continue tirzepatide long-term. Participants first went through a 36-week lead-in period where everyone received tirzepatide, losing an average of 21.1% body weight. Then half continued tirzepatide while the other half switched to placebo. The tirzepatide group continued losing weight, reaching 26% total weight loss by week 88. The placebo group regained 14% of their body weight.
These trials show that tirzepatide dosing follows a predictable curve. You will see appetite suppression first, then weight loss, then metabolic improvements. The speed depends heavily on which dose you reach and how long you stay on it. Understanding how peptides work helps explain why the escalation schedule is structured the way it is.
The trials also revealed that slow responders do catch up if they stick with the protocol. About 10% of participants were classified as slow responders at week 12, defined as less than 5% weight loss. By week 72, 90% of those slow responders had achieved at least 5% weight loss, and many exceeded 15%. This means that if you are not seeing fast results in the first few months, it does not mean tirzepatide will not work for you. It just means your body needs more time to adapt.
One critical finding: the speed of weight loss does not predict the final amount of weight lost. Some people drop weight quickly in the first 12 weeks, then plateau. Others lose slowly and steadily for the full 72 weeks. The key variable is adherence to the dosing schedule and staying on the medication long enough to reach your target dose. If you want to compare tirzepatide speed to other options, check out semaglutide vs tirzepatide for a side-by-side breakdown.
Another important note: the trials used subcutaneous injections administered once weekly. Results may differ with oral tirzepatide, though data on oral formulations is still limited. Most people following a research protocol will use injectable tirzepatide and follow the same escalation schedule the trials validated.
The bottom line from the trials: tirzepatide works faster than most other weight loss medications, but it still requires months to see peak effects. If you are tracking your progress, use peptide calculator tools to compare your timeline against the clinical averages. That way you know if you are on track or if adjustments are needed.
Week by week breakdown of tirzepatide effects
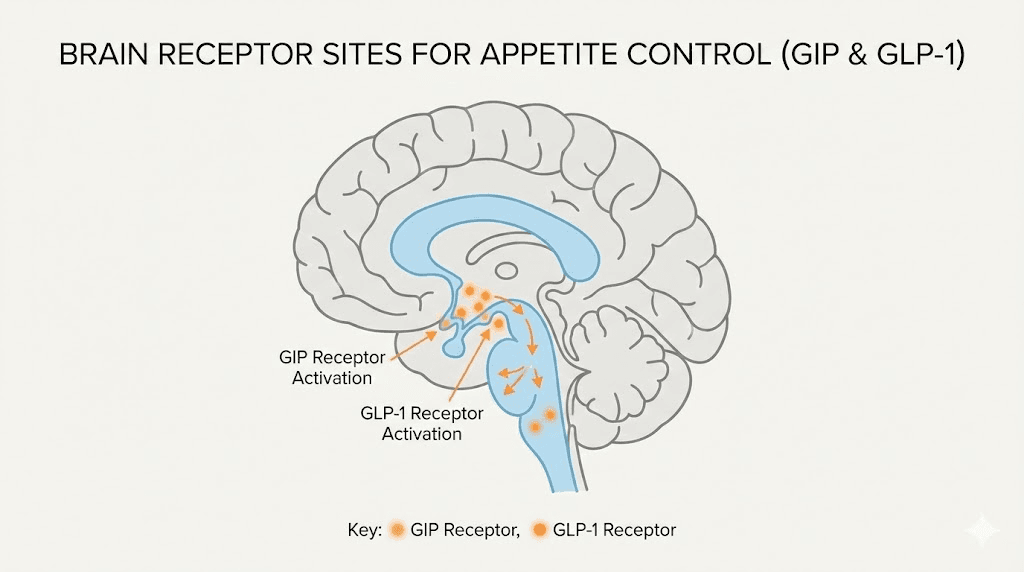
Week 1 is when you first notice the difference. Most people report feeling less hungry within the first few days. This is because tirzepatide activates GIP and GLP-1 receptors almost immediately after injection. The receptors slow gastric emptying and send satiety signals to the brain. You will not lose measurable weight yet, but you will probably eat less without consciously trying.
Week 2 to week 4 is when the first physical changes appear. You might notice clothes fitting slightly looser or the scale dropping 1-2 pounds per week. The 2.5 mg starting dose is intentionally low to minimize gastrointestinal side effects while your body adjusts. Some people experience mild nausea or changes in bowel movements during this phase. These side effects usually resolve within the first month.
Week 4 is when the first dose increase happens. You move from 2.5 mg to 5 mg. This is when weight loss becomes more noticeable. Clinical trial data shows an average of 4% body weight loss by week 4. If you started at 200 pounds, that is about 8 pounds. The appetite suppression becomes stronger at this dose level, and many people report needing smaller portions to feel full.
Week 8 brings another dose increase to 7.5 mg. By this point, you should be down about 6% of starting body weight if you are responding as expected. Your energy levels may fluctuate as your body adapts to a lower calorie intake. Some people feel more energized because they are eating cleaner foods, while others feel sluggish from the calorie deficit. Using tirzepatide dosing for weight loss in units helps you track whether your injections are dosed correctly.
Week 12 is a critical checkpoint. The clinical definition of a responder is someone who has lost at least 5% body weight by week 12. Most people on tirzepatide exceed this threshold, with average weight loss around 8-9% depending on dose. This is also when metabolic markers start improving significantly. Blood sugar levels stabilize, insulin sensitivity increases, and inflammation markers often drop.
Week 16 to week 20 is when you reach the higher doses of 10 mg, 12.5 mg, or 15 mg. This is the period where weight loss accelerates for most people.
The dual action of GIP and GLP-1 receptor activation is fully engaged, and the medication is working at peak efficiency. By week 20, many people have lost 12-15% of their starting weight if they followed the escalation schedule without pauses or reductions.
Week 24 to week 40 is the phase where the most dramatic changes happen. This is when people post their before-and-after photos. You will notice facial fat loss, reduced waist circumference, and improved muscle definition if you are combining tirzepatide with strength training. The medication is no longer just suppressing appetite, it is actively improving how your body processes fat and glucose. If you want to see what realistic results look like, check out tirzepatide before and after timelines from real users.
Week 40 to week 72 is the maintenance phase. Weight loss slows down, but it does not stop. Most people continue losing 0.5-1% body weight per week during this period. The key is staying consistent with injections and not reverting to old eating habits. The SURMOUNT trials showed that people who stayed on tirzepatide for the full 72 weeks continued to see improvements in metabolic health even after weight loss plateaued.
One thing to note: the week-by-week timeline assumes you follow the standard escalation schedule without pauses. If you experience side effects and need to stay at a lower dose longer, your timeline will be slower. That is perfectly normal. The goal is not to race through the doses, it is to find the dose that works for your body without causing intolerable side effects. For detailed dose schedules, see tirzepatide dose chart.
If you are tracking your progress week by week, use peptide dosage chart tools to compare your results against the clinical averages. This helps you know if you are on track or if you need to adjust your approach. Some people also combine tirzepatide with other peptides to enhance results, which you can explore in peptide stack calculator.
How the dose escalation schedule affects your timeline
The dose escalation schedule is not arbitrary. It is designed to minimize side effects while maximizing efficacy. Tirzepatide is a potent dual GIP/GLP-1 receptor agonist, and starting at a high dose would cause severe nausea, vomiting, and gastrointestinal distress for most people. The escalation schedule allows your body to adapt gradually.
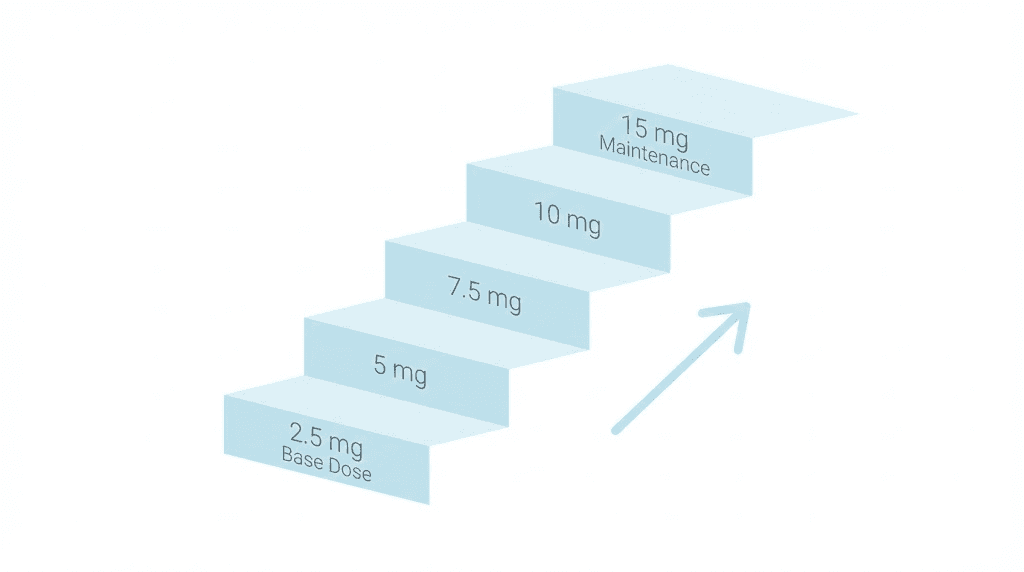
The standard schedule looks like this: 2.5 mg for weeks 0-4, 5 mg for weeks 4-8, 7.5 mg for weeks 8-12, 10 mg for weeks 12-16, 12.5 mg for weeks 16-20, and 15 mg for weeks 20 and beyond. Each dose level is maintained for 4 weeks before increasing. This gives your GIP and GLP-1 receptors time to adjust to the increased signaling before ramping up again.
If you skip steps in the escalation schedule, you will likely experience more severe side effects. Some people try to speed up their results by jumping directly to 10 mg or 15 mg. This almost always backfires. The nausea and vomiting can be so severe that people have to stop the medication entirely. Then they have to restart at a lower dose, which delays their progress even more.
On the other hand, some people need to slow down the escalation schedule. If you experience persistent nausea, vomiting, or diarrhea that does not resolve after a few days, you may need to stay at your current dose for an extra 2-4 weeks before increasing.
This is called a modified escalation schedule, and it is completely acceptable. The goal is to find the highest dose you can tolerate, not to reach 15 mg as fast as possible.
The dose you reach also determines how fast you lose weight. Clinical data shows that the 15 mg dose produces faster and greater weight loss than the 10 mg or 5 mg doses. In SURMOUNT-1, the 15 mg group lost 22.5% body weight by week 72, while the 5 mg group lost 16%. That is a 6.5% difference in total weight loss, which translates to about 13 pounds for someone who started at 200 pounds.
But here is the catch: not everyone can tolerate 15 mg. Some people find that 10 mg or even 7.5 mg is their maximum tolerable dose. That does not mean tirzepatide will not work for them, it just means their results will be closer to the 16-18% range instead of the 22.5% range. That is still clinically significant weight loss and enough to improve most metabolic health markers.
If you are following a microdosing approach instead of the standard escalation schedule, your timeline will be different. Microdosing involves using smaller, more frequent doses to minimize side effects while maintaining steady blood levels. For more on this approach, see microdosing tirzepatide chart.
Another factor that affects your timeline: injection technique and reconstitution accuracy. If you are using research-grade tirzepatide and mixing it yourself, dosing errors can slow your progress. A dose that is too low will not produce the expected effects, while a dose that is too high will cause more side effects. Use peptide reconstitution calculator to ensure you are mixing correctly. For step-by-step instructions, see how to reconstitute peptides.
The escalation schedule also affects when you see metabolic improvements. Blood sugar levels start improving immediately, even at the 2.5 mg dose. But significant A1C reductions usually require at least 8-12 weeks at a therapeutic dose of 5 mg or higher. If you are using tirzepatide primarily for blood sugar control, you may see results faster than someone using it purely for weight loss.
One final note on escalation: some people stay at a lower dose indefinitely once they reach their target weight. For example, if you lose 20% of your body weight on 10 mg and feel good at that dose, there is no need to increase to 15 mg. Maintenance dosing is a valid strategy, and many people find that staying at 7.5 mg or 10 mg long-term is sufficient to keep the weight off.
When appetite suppression kicks in
Appetite suppression is the first effect most people notice. It starts within 1-2 weeks of the first injection. The mechanism is straightforward: tirzepatide activates GLP-1 receptors in the brain that regulate hunger and satiety. It also slows gastric emptying, which means food stays in your stomach longer. You feel full faster and stay full longer.
But the speed at which appetite suppression kicks in varies. Some people report feeling less hungry within 24 hours of their first injection. Others do not notice a difference until week 2 or week 3. The variability depends on individual receptor sensitivity, baseline metabolic rate, and how much food you were eating before starting tirzepatide.
The intensity of appetite suppression also increases with dose. At 2.5 mg, you might notice you can skip a snack without feeling hungry. At 5 mg, you might find yourself eating half your usual portion at meals. At 10 mg or 15 mg, many people report needing to remind themselves to eat because hunger signals are almost completely absent. This is why some people experience tirzepatide making them tired, they are not eating enough calories to fuel their activity level.
The appetite suppression is not just psychological. Tirzepatide reduces ghrelin, the hormone that signals hunger, and increases leptin sensitivity, which signals fullness. It also affects the reward pathways in the brain that drive cravings for high-calorie foods. Many people report that foods they used to crave, like pizza, ice cream, or chips, suddenly seem unappealing.
One thing to watch for: overly aggressive appetite suppression can backfire. If you are eating fewer than 1,000 calories per day because you have zero appetite, you risk muscle loss, nutrient deficiencies, and metabolic slowdown. The goal is not to eat as little as possible, it is to eat the right amount for sustained weight loss while preserving lean mass. If you are struggling to eat enough, consider splitting your meals into smaller, more frequent portions.
Appetite suppression also affects hydration. Many people forget to drink water because thirst signals are blunted along with hunger signals. Dehydration can cause headaches, fatigue, and constipation, which are often mistaken for side effects of tirzepatide itself. Make a conscious effort to drink at least 64 ounces of water per day, even if you do not feel thirsty.
Another factor: appetite suppression may fluctuate throughout the week. Tirzepatide has a half-life of about 5 days, which means blood levels peak 1-2 days after injection and taper off toward the end of the week. Some people notice they are less hungry on days 2-4 and slightly hungrier on days 6-7. This is normal. If hunger becomes problematic toward the end of the week, it may be a sign that you need a higher dose.
If you are not experiencing appetite suppression within 2 weeks, there are a few possible explanations. First, your dose may be too low. The 2.5 mg starting dose is intentionally conservative, and some people need to reach 5 mg or 7.5 mg before they notice a significant effect. Second, you may have higher baseline GLP-1 receptor resistance, which is common in people with longstanding obesity or insulin resistance. Third, your tirzepatide may be improperly stored or expired, which reduces its potency. For more on this, see how long tirzepatide lasts in the fridge.
If you want to compare how quickly appetite suppression happens with tirzepatide versus other medications, check out how long does it take for tirzepatide to suppress appetite versus how long for semaglutide to suppress appetite. The timelines are similar, but tirzepatide tends to produce slightly stronger appetite suppression due to its dual GIP/GLP-1 mechanism.
One final note: appetite suppression is not permanent. If you stop taking tirzepatide, hunger signals will return to baseline within 1-2 weeks. This is why the SURMOUNT-4 trial showed significant weight regain in the placebo group after stopping tirzepatide. The medication is managing your appetite, not curing it. Long-term maintenance requires either staying on tirzepatide indefinitely or developing new eating habits that do not rely on the medication.
Blood sugar and metabolic effects speed
Tirzepatide starts lowering blood sugar within hours of the first injection. The mechanism is twofold: it increases insulin secretion in response to glucose, and it decreases glucagon secretion. Glucagon is the hormone that tells your liver to release stored glucose. By suppressing glucagon, tirzepatide prevents blood sugar from spiking after meals.
The speed at which blood sugar improves depends on your starting glucose levels. If you have type 2 diabetes with an A1C above 9%, you will likely see significant improvements within the first 2-4 weeks. If your A1C is in the prediabetic range (5.7-6.4%), improvements may be more gradual because there is less room for change.
In the SURPASS-5 trial, participants with type 2 diabetes saw A1C reductions of 2.0% with the 5 mg dose, 2.4% with the 10 mg dose, and 2.34% with the 15 mg dose over 40 weeks. Most of the A1C reduction happened in the first 12 weeks, with smaller incremental improvements after that. This means that if you are using tirzepatide for blood sugar control, you will see the bulk of the benefit within the first 3 months.
One important note: the speed of blood sugar improvement is faster than the speed of weight loss. You can see your fasting glucose drop by 20-30 mg/dL within the first week, even if the scale has not moved yet. This is because tirzepatide improves insulin sensitivity and glucose metabolism independently of weight loss. The weight loss amplifies the effect over time, but the initial metabolic changes happen fast.
The time to reach specific A1C targets depends on your starting point. If your A1C is 9% and your goal is 7%, you will likely reach it within 8 weeks on a therapeutic dose. If your goal is 6.5%, it may take 12 weeks. If your goal is below 6%, it may require 6 months or more, along with strict dietary control.
Tirzepatide also improves other metabolic markers beyond blood sugar. Triglycerides typically drop within the first 8-12 weeks. HDL cholesterol may increase slightly, while LDL cholesterol often decreases. Blood pressure tends to improve within 4-8 weeks, especially if you are losing weight during that time. Inflammation markers like C-reactive protein (CRP) often drop within 12 weeks.
If you are tracking metabolic improvements, it is worth testing your blood work at baseline, week 12, and week 24. This gives you a clear picture of how fast tirzepatide is affecting your metabolic health. Some people see dramatic improvements across all markers, while others see selective improvements in glucose but slower changes in lipids or blood pressure.
One factor that affects speed: concurrent medications. If you are taking metformin, SGLT2 inhibitors, or other diabetes medications, tirzepatide may work faster because the medications have complementary mechanisms. On the other hand, if you are taking medications that raise blood sugar (like corticosteroids), tirzepatide may work slower because it has to overcome the opposing effect.
Another factor: diet quality. If you continue eating a high-carb, high-sugar diet while on tirzepatide, your blood sugar will improve, but not as much as it would if you cleaned up your diet. Tirzepatide is powerful, but it is not magic.
You still need to give it something to work with. For more on how to maximize metabolic improvements, see peptides for fat loss strategies.
If you are comparing tirzepatide to semaglutide for blood sugar control, tirzepatide tends to reach A1C targets about 4 weeks sooner. This is because the GIP receptor activation provides an additional mechanism for glucose control that semaglutide does not have. For a detailed comparison, see semaglutide vs tirzepatide.
One final note: if your blood sugar is dropping too fast, you may experience hypoglycemia (low blood sugar). Symptoms include shakiness, sweating, rapid heartbeat, and confusion. This is more common in people who are also taking insulin or sulfonylureas. If you experience hypoglycemia, you may need to reduce your other diabetes medications. Do not stop tirzepatide, just adjust the supporting medications.
Side effects timeline: what happens when
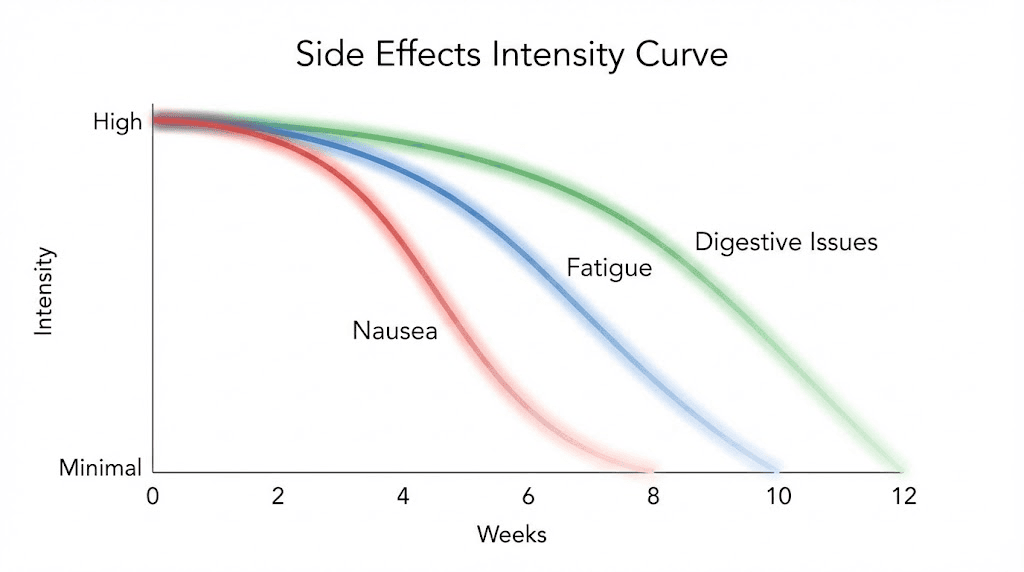
The most common side effects of tirzepatide are gastrointestinal: nausea, diarrhea, constipation, and vomiting. These side effects follow a predictable timeline that maps onto the dose escalation schedule. Understanding when side effects peak and when they resolve helps you manage them more effectively.
Week 1 is when most people first experience nausea. The 2.5 mg starting dose is low enough that nausea is usually mild, more of a queasy feeling than full-on sickness. It tends to be worst on days 1-3 after injection and fades by days 5-7. Eating smaller, more frequent meals and avoiding high-fat foods can reduce nausea during this phase.
Week 4 is when the first dose increase happens, and side effects often intensify. Moving from 2.5 mg to 5 mg causes a noticeable jump in GI symptoms for many people. Nausea may return even if it had resolved at the lower dose. Some people also experience diarrhea or constipation during this transition. The side effects usually peak within 2-3 days of the first 5 mg injection and taper off over the next 1-2 weeks.
Week 8 brings another dose increase to 7.5 mg, and the pattern repeats. You may experience a few days of intensified nausea, bloating, or changes in bowel movements. By this point, your body is adapting to the medication, so the side effects are usually less severe than they were at the 5 mg transition. Most people find that side effects resolve within a few days at each new dose level.
Week 12 to week 20 is when you move through the higher doses: 10 mg, 12.5 mg, and 15 mg. Each dose increase can trigger a brief recurrence of GI symptoms, but they tend to be milder than the early transitions. By the time you reach 15 mg, your GIP and GLP-1 receptors are fully adapted, and side effects are usually minimal. However, some people find that 15 mg is too strong and causes persistent nausea or vomiting. In that case, they drop back to 10 mg or 12.5 mg as their maintenance dose.
The timeline for specific side effects varies. Nausea affects about 24-30% of users and is most common during the first month and after each dose increase. Diarrhea affects 18-24% and tends to appear within the first week of a new dose. Constipation affects 16-17% and is more common at higher doses, probably because people are eating less fiber due to reduced appetite. Vomiting is less common (5-10%) but can occur if you eat too much or eat high-fat foods shortly after an injection.
Most GI side effects resolve within 4-6 weeks of starting tirzepatide or increasing the dose. If you still have persistent nausea or diarrhea after 6 weeks at a stable dose, it may indicate that the dose is too high for you. In that case, consider dropping back to the previous dose or extending the time between dose increases.
Non-GI side effects are less common but still worth tracking. Some people experience fatigue, especially in the first few weeks. This is usually due to eating fewer calories, not a direct effect of tirzepatide. Making sure you are eating enough protein and staying hydrated can reduce fatigue. If you are experiencing persistent tiredness, see does tirzepatide make you tired for troubleshooting strategies.
Headaches are another occasional side effect, usually in the first 2-4 weeks. They are often related to dehydration or rapid changes in blood sugar. Drinking more water and eating consistent meals can help. If headaches persist, check your blood pressure, tirzepatide can lower blood pressure, and if it drops too much, it can cause headaches.
Hair loss is a rare but documented side effect, usually appearing around 3-6 months after starting tirzepatide. This is not caused by the medication itself but by rapid weight loss and calorie restriction. The medical term is telogen effluvium, and it is temporary. Hair typically regrows once weight stabilizes and calorie intake normalizes. For more on this, see GLP-1 hair loss complete guide.
One thing to note: side effects are more common and more severe if you escalate doses too quickly. If you are experiencing intolerable side effects, slow down the escalation schedule. Stay at your current dose for an extra 4 weeks before increasing. This gives your body more time to adapt and reduces the likelihood of severe nausea or vomiting.
If you are experiencing severe or persistent side effects that do not resolve within a few weeks, it may be a sign that tirzepatide is not the right medication for you. Some people do better with semaglutide, which has a slightly different side effect profile. Others may need to try retatrutide or a different class of medication entirely.
Why some people respond faster than others
Responder variability is one of the most frustrating aspects of tirzepatide. Some people lose 10% body weight in the first 12 weeks. Others need 40 weeks to hit the same target. The clinical trials identified several factors that predict speed of response, and understanding them can help you set realistic expectations.
Baseline body mass index (BMI) is the strongest predictor. People with higher starting BMIs tend to lose weight faster in absolute terms but slower in percentage terms. For example, someone starting at a BMI of 40 might lose 30 pounds in 12 weeks, but that is only 10% of their starting weight. Someone starting at a BMI of 30 might lose 18 pounds in 12 weeks, which is 12% of their starting weight. The higher BMI person lost more pounds but is still classified as a slower responder in percentage terms.
Sex is another predictor. Men tend to lose weight faster than women in the first 12-24 weeks.
This is partly because men have higher metabolic rates and more lean muscle mass, which burns more calories at rest. However, by week 72, the gap narrows significantly.
Women eventually catch up in percentage weight loss, even if they lose more slowly in the early phases.
Insulin resistance affects response speed. People with higher baseline insulin resistance lose weight more slowly because their bodies are less efficient at metabolizing fat. They also tend to have more inflammation, which slows metabolic adaptation. Over time, as insulin sensitivity improves, weight loss accelerates. This is why some people are slow responders in the first 12 weeks but become fast responders by week 40.
Waist circumference is a proxy for visceral fat, and people with higher waist circumferences tend to lose weight more slowly. Visceral fat is metabolically stubborn and resistant to mobilization. It also produces inflammatory cytokines that interfere with GLP-1 and GIP receptor signaling. As visceral fat decreases, the medication becomes more effective, and weight loss speeds up.
Genetic factors also play a role. Some people have naturally higher GLP-1 receptor sensitivity, which means they respond to lower doses. Others have lower receptor sensitivity and need higher doses to see the same effects. There is no easy way to test for receptor sensitivity before starting tirzepatide, so the escalation schedule is designed to accommodate both types of responders.
Diet quality affects response speed. People who switch to a high-protein, moderate-carb diet while on tirzepatide lose weight faster than people who continue eating processed foods and simple carbs. This is because tirzepatide improves insulin sensitivity, and a clean diet amplifies that effect. On the other hand, a poor diet can partially negate the medication benefits.
Physical activity level matters too. People who incorporate resistance training and aerobic exercise lose more fat and preserve more lean muscle mass. This leads to faster metabolic improvements and better long-term weight maintenance. Exercise also enhances insulin sensitivity, which makes tirzepatide more effective. For more on combining peptides with training, see peptides for athletic performance.
Sleep quality affects hormone regulation, and poor sleep can slow tirzepatide response. Sleep deprivation raises cortisol and ghrelin, both of which interfere with weight loss. It also reduces leptin sensitivity, which makes it harder to feel full. If you are not sleeping at least 7 hours per night, your tirzepatide results will likely be slower than expected.
Stress is another underestimated factor. Chronic stress raises cortisol, which promotes fat storage and reduces fat mobilization. It also increases cravings for high-calorie comfort foods, which can partially override the appetite suppression from tirzepatide. Managing stress through meditation, exercise, or therapy can speed up your response.
Medication interactions can slow response. Some medications interfere with GLP-1 signaling or promote weight gain. These include antipsychotics, antidepressants (especially mirtazapine and paroxetine), corticosteroids, and beta-blockers. If you are taking any of these, your tirzepatide response may be slower. Talk to your prescriber about whether adjustments are possible.
One final factor: adherence. People who miss injections or inconsistently follow the dosing schedule lose weight more slowly. Tirzepatide has a 5-day half-life, so missing a dose causes blood levels to drop and hunger to return. If you miss more than one dose per month, you are essentially resetting your adaptation process each time, which slows overall progress.
If you are a slow responder, do not panic. The SURMOUNT trials showed that 90% of slow responders eventually achieved clinically meaningful weight loss if they stayed on tirzepatide for the full 72 weeks. The key is patience and consistency. If you want to compare your progress against clinical benchmarks, use peptide calculator tools to track your timeline.
What to do if tirzepatide seems slow to work
If you have been on tirzepatide for 12 weeks and have not lost at least 5% of your starting body weight, you are classified as a slow responder. This does not mean tirzepatide will not work for you, it just means you need to troubleshoot your approach. Here are the most common reasons for slow response and how to fix them.
First, check your dose. Are you actually at a therapeutic dose? The 2.5 mg starting dose is sub-therapeutic for weight loss, it is only meant to help your body adjust. Most people need to reach at least 5 mg before seeing significant weight loss. If you are still at 2.5 mg after 12 weeks, that is your problem. Follow the escalation schedule to reach a higher dose.
Second, verify your reconstitution and dosing accuracy. If you are using research-grade tirzepatide and mixing it yourself, errors in mixing or dosing can drastically reduce effectiveness. A 10% error in reconstitution means you are getting 10% less medication than you think. Use peptide reconstitution calculator to double-check your math. For detailed mixing instructions, see how to mix peptides with bac water.
Third, check your storage. Tirzepatide degrades rapidly if stored incorrectly. It must be kept in the fridge at 2-8 degrees Celsius at all times, both before and after reconstitution. If your fridge is too warm, or if the vial has been left out for more than 2 hours, the peptide may be partially degraded. For more on this, see does tirzepatide need to be refrigerated and how long tirzepatide lasts in the fridge.
Fourth, evaluate your diet. Are you eating in a calorie deficit? Tirzepatide suppresses appetite, but if you are eating calorie-dense foods like nuts, cheese, and oils, you can still consume maintenance-level calories without feeling full. Track your food intake for a week using an app like MyFitnessPal. If you are eating more than 1,500-2,000 calories per day, you may need to adjust portion sizes.
Fifth, check for hidden sources of calories. Liquid calories like fruit juice, soda, alcohol, and sweetened coffee drinks do not trigger the same satiety signals as solid food. You can drink 500 calories in 5 minutes without feeling full, which completely undermines the appetite suppression from tirzepatide. Switch to water, black coffee, or unsweetened tea.
Sixth, evaluate your activity level. If you are sedentary, your calorie expenditure is low, and weight loss will be slower. Adding 30-60 minutes of walking per day can increase your daily calorie burn by 200-400 calories, which accelerates weight loss. Resistance training is even better because it preserves muscle mass and boosts metabolic rate.
Seventh, check for medication interactions. If you are taking medications that promote weight gain or interfere with insulin signaling, tirzepatide may be less effective. Common culprits include antipsychotics, antidepressants, corticosteroids, and beta-blockers. Talk to your prescriber about whether adjustments are possible.
Eighth, consider adding a complementary peptide. Some people stack tirzepatide with other peptides to enhance fat loss. For example, combining tirzepatide with AOD 9604 or FTPP peptide adipotide can target stubborn fat deposits more aggressively. For more on stacking, see peptide stack calculator.
Ninth, check your hormonal status. Hypothyroidism, low testosterone, high cortisol, and estrogen dominance can all slow weight loss. If you have not had recent blood work, get a comprehensive hormone panel. Optimizing thyroid and sex hormones can dramatically improve tirzepatide response.
Tenth, evaluate your sleep and stress. Poor sleep and chronic stress raise cortisol, which promotes fat storage and slows fat loss. If you are sleeping less than 7 hours per night or dealing with chronic stress, those factors may be more limiting than the tirzepatide dose.
If you have addressed all of these factors and are still not losing weight, it may be time to increase your dose. Some people need 12.5 mg or 15 mg to see significant results, especially if they have longstanding obesity or severe insulin resistance. Do not be afraid to escalate to the higher doses if you are tolerating the medication without severe side effects.
If you are still stuck after 24 weeks at the maximum dose, consider switching to a different medication. Some people respond better to retatrutide, which is a triple agonist that also activates the glucagon receptor. Others may benefit from combining tirzepatide with cagrilintide and semaglutide for a synergistic effect. For more on alternative options, see why not losing weight on tirzepatide.
Tirzepatide speed compared to semaglutide
Semaglutide and tirzepatide are the two most popular GLP-1-based medications for weight loss. Both work by activating GLP-1 receptors, but tirzepatide has an additional mechanism: it also activates GIP receptors. This dual action gives tirzepatide a speed advantage in most clinical comparisons.
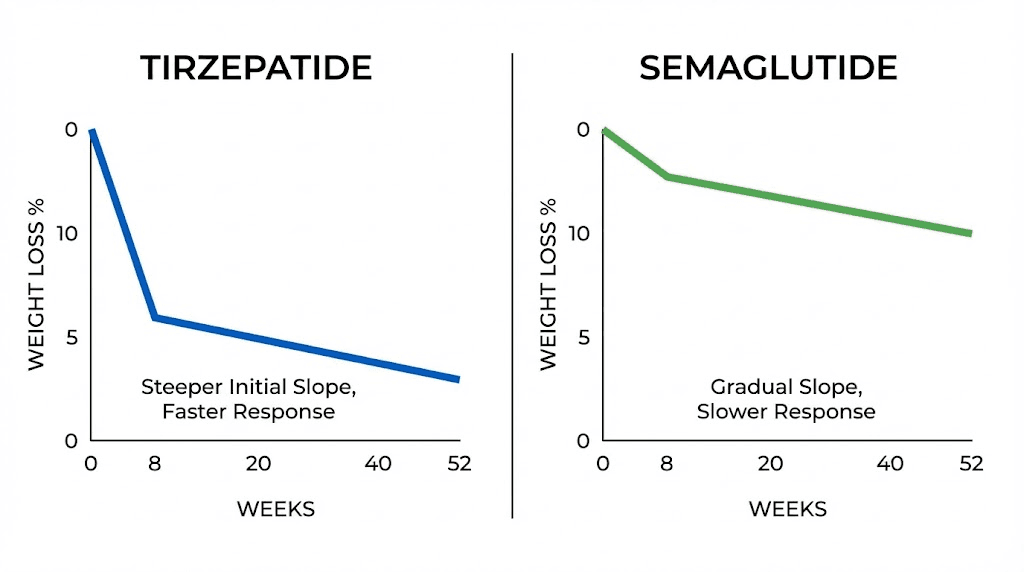
In head-to-head trials, tirzepatide produces faster and greater weight loss than semaglutide. The SURMOUNT-1 trial showed that tirzepatide 15 mg resulted in 22.5% weight loss over 72 weeks. The STEP trials for semaglutide 2.4 mg showed 14.9% weight loss over 68 weeks. That is a 7.6% difference in total weight loss, which translates to about 15 pounds for someone starting at 200 pounds.
The speed of onset is also faster with tirzepatide. Most people on semaglutide start seeing weight loss around week 4-6. With tirzepatide, weight loss typically starts by week 4. The difference is not dramatic, but it is measurable. If you are looking for the fastest possible results, tirzepatide has the edge.
Appetite suppression also kicks in faster with tirzepatide. Most people feel less hungry within 1-2 weeks on tirzepatide, whereas semaglutide often takes 2-3 weeks. This is likely due to the additional GIP receptor activation, which enhances satiety signaling. For more on this, compare how long does it take for tirzepatide to suppress appetite versus how long for semaglutide to suppress appetite.
Blood sugar control is another area where tirzepatide works faster. In the SURPASS trials, tirzepatide reached target A1C levels about 4 weeks sooner than semaglutide. The 15 mg dose of tirzepatide reduced A1C by 2.34% over 40 weeks, compared to 1.86% for semaglutide 1 mg. If you are using the medication primarily for diabetes management, tirzepatide is the faster option.
Side effects are comparable between the two medications, but tirzepatide tends to cause slightly more nausea in the first few weeks. About 30% of tirzepatide users experience nausea, compared to 24% of semaglutide users. However, the nausea resolves at about the same rate for both medications, usually within 4-6 weeks.
One advantage of semaglutide: it has a longer track record. Semaglutide has been on the market longer and has more long-term safety data. Tirzepatide is newer, and while the clinical trial data looks excellent, there is less real-world experience with it. If you are risk-averse and want the most established option, semaglutide may be the better choice.
Cost is another factor. Research-grade semaglutide is generally cheaper than research-grade tirzepatide because semaglutide has been available longer and is more widely produced. If budget is a concern, semaglutide may be more accessible. For more on cost comparisons, see peptide therapy cost complete guide.
Switching between the two medications is possible, though it requires careful dose adjustment. If you are switching from tirzepatide to semaglutide, you will need to adjust your dose because the two medications are not directly equivalent. For guidance on this, see switching from tirzepatide to semaglutide and tirzepatide vs semaglutide dosage chart.
One final consideration: response variability. Some people respond better to semaglutide, while others respond better to tirzepatide. There is no way to predict who will respond better without trying both. If you have been on semaglutide for 6 months and are not seeing the results you want, switching to tirzepatide is worth considering. The reverse is also true, if tirzepatide is not working, semaglutide may be a better fit.
For a comprehensive comparison of the two medications, including speed of onset, side effects, cost, and efficacy, see semaglutide vs tirzepatide and how fast does semaglutide work.
How to maximize tirzepatide effectiveness
Tirzepatide is powerful, but it is not a standalone solution. The people who get the best results combine the medication with strategic diet, exercise, and lifestyle optimization. Here is how to maximize tirzepatide effectiveness and accelerate your timeline.
Prioritize protein intake. Protein preserves lean muscle mass during weight loss and increases satiety. Aim for at least 1 gram of protein per pound of target body weight. If your goal weight is 150 pounds, eat at least 150 grams of protein per day. High-protein foods include chicken, fish, eggs, Greek yogurt, cottage cheese, and protein powder. For more on nutrition strategies, see peptides for fat loss.
Incorporate resistance training. Lifting weights 3-4 times per week preserves muscle mass and keeps your metabolic rate high during weight loss. Muscle is metabolically active tissue, so maintaining it helps you burn more calories at rest. It also improves insulin sensitivity, which amplifies the metabolic benefits of tirzepatide. For training guidance, see peptides for muscle growth.
Track your food intake. Even with appetite suppression, it is possible to eat too little or too much. Use a food tracking app like MyFitnessPal or Cronometer for at least a few weeks to get a sense of your actual calorie and macronutrient intake. You may be surprised by how many calories you are consuming from snacks, sauces, and cooking oils.
Optimize injection timing. Some people find that injecting tirzepatide on the same day each week at the same time helps maintain steady blood levels. Others prefer to inject on a day when they can rest for 24-48 hours in case they experience nausea. Experiment with timing to find what works best for your schedule and side effect tolerance.
Stay hydrated. Dehydration slows fat metabolism and makes side effects worse. Drink at least 64 ounces of water per day, more if you are exercising. Electrolyte drinks can help if you are experiencing muscle cramps or headaches. Avoid sugary sports drinks, they add unnecessary calories.
Manage stress. Chronic stress raises cortisol, which promotes fat storage and slows fat mobilization. Practice stress management techniques like meditation, deep breathing, yoga, or therapy. Even 10 minutes of daily meditation can lower cortisol and improve your tirzepatide response.
Optimize sleep. Sleep deprivation raises ghrelin (hunger hormone) and lowers leptin (fullness hormone), which makes it harder to stick to a calorie deficit. Aim for 7-9 hours of quality sleep per night. If you struggle with sleep, consider supplements like magnesium, glycine, or melatonin. For more on sleep and peptides, see peptides for anti-aging.
Limit alcohol. Alcohol adds empty calories, disrupts sleep, raises cortisol, and impairs fat metabolism. Even moderate drinking can slow your weight loss by 20-30%. If you want to maximize tirzepatide effectiveness, limit alcohol to special occasions or eliminate it entirely.
Add complementary supplements. Certain supplements can enhance fat loss and metabolic health. Consider adding vitamin D, omega-3 fish oil, berberine, chromium, or alpha-lipoic acid. These supplements improve insulin sensitivity, reduce inflammation, and support fat metabolism. Always check with your prescriber before adding supplements to ensure there are no interactions.
Track your progress beyond the scale. Weight is not the only metric that matters. Take weekly measurements of waist circumference, hip circumference, and body fat percentage. Take progress photos every 4 weeks. Track how your clothes fit. Track your energy levels, sleep quality, and mood. Sometimes the scale does not move for weeks, but you lose inches and feel dramatically better. Check out before and after tirzepatide weight loss results and men before and after tirzepatide for realistic timeline expectations.
Avoid extreme calorie restriction. Eating fewer than 1,000 calories per day slows your metabolic rate, causes muscle loss, and makes it harder to lose weight long-term. Aim for a moderate deficit of 300-500 calories below your maintenance level. This allows for steady weight loss while preserving muscle and metabolic rate.
Consider stacking with other peptides. Some people combine tirzepatide with fat-loss peptides like AOD 9604 or recovery peptides like BPC-157 and TB-500. Stacking can accelerate results if done correctly. For guidance on stacking, see peptide stack calculator and peptide stacks guide.
Adjust your dose based on response. If you have been at the same dose for 8 weeks and weight loss has stalled, it may be time to increase. If you are experiencing intolerable side effects, it may be time to decrease or stay at your current dose longer. Tirzepatide dosing is not one-size-fits-all, you need to find the dose that works for your body. For unit conversions, see tirzepatide dosage in units and how many units is 2.5 mg of tirzepatide.
Plan for long-term maintenance. Tirzepatide is not a short-term fix. If you stop the medication after reaching your goal weight, you will likely regain the weight within 6-12 months. The SURMOUNT-4 trial showed 14% weight regain in the placebo group after stopping tirzepatide. Plan to stay on a maintenance dose indefinitely or develop sustainable eating habits that do not rely on the medication. For more on related long-term strategies, see peptide cycle planning guide and best peptides for weight loss.
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides offers the most comprehensive resource available. Members access detailed dosing protocols, semaglutide dosage calculators, progress tracking tools, and a community of thousands who have navigated these exact questions. Whether you are a first-time user or fine-tuning an advanced protocol, SeekPeptides provides the evidence-based guidance you need to get the fastest, safest results from tirzepatide.
Frequently asked questions
How long does it take for tirzepatide to start working?
Most people notice appetite suppression within 1-2 weeks of the first injection. Measurable weight loss typically starts around week 4, with about 4% of starting body weight lost by that point. Significant results appear by week 8-12, with 6-8% weight loss on average. Full effects take 4-6 months as you escalate to your maximum tolerated dose. Blood sugar improvements happen even faster, often within the first week. For more on the timeline, see how long does it take for tirzepatide to work.
Why am I not losing weight on tirzepatide?
Common reasons include being at too low a dose (2.5 mg is sub-therapeutic for weight loss), incorrect reconstitution or dosing, poor storage leading to peptide degradation, eating calorie-dense foods despite reduced appetite, liquid calories from drinks, sedentary lifestyle, medication interactions, hormonal imbalances, poor sleep, or chronic stress. Start by verifying your dose, reconstitution accuracy, and storage conditions. Then evaluate diet, activity level, and other lifestyle factors. For detailed troubleshooting, see why not losing weight on tirzepatide.
How fast does tirzepatide work compared to semaglutide?
Tirzepatide works slightly faster than semaglutide. Clinical trials show weight loss starting around week 4 for tirzepatide versus week 4-6 for semaglutide. By week 72, tirzepatide 15 mg produces 22.5% weight loss compared to 14.9% for semaglutide 2.4 mg. Appetite suppression also kicks in 1-2 weeks with tirzepatide versus 2-3 weeks with semaglutide. Blood sugar control is achieved about 4 weeks sooner with tirzepatide. For a detailed comparison, see semaglutide vs tirzepatide.
What is the fastest way to lose weight on tirzepatide?
The fastest approach is to follow the standard dose escalation schedule without delays, reach your maximum tolerated dose (ideally 15 mg), combine tirzepatide with a high-protein diet (1 gram per pound of target body weight), incorporate resistance training 3-4 times per week, stay hydrated (64+ ounces of water daily), optimize sleep (7-9 hours per night), manage stress, and avoid alcohol and liquid calories. Some people also stack tirzepatide with complementary peptides like AOD 9604 for additional fat loss. For stacking strategies, see peptide stack calculator.
Can I speed up the dose escalation schedule?
No, speeding up the escalation schedule usually backfires. Increasing doses faster than every 4 weeks causes more severe gastrointestinal side effects like nausea, vomiting, and diarrhea. Many people who try to escalate too quickly end up having to stop the medication entirely due to intolerable side effects. Then they have to restart at a lower dose, which delays their progress even more. The standard schedule (2.5 mg for 4 weeks, then 5 mg for 4 weeks, then 7.5 mg, and so on) is designed to minimize side effects while maximizing effectiveness. Stick to the schedule unless your prescriber recommends otherwise. For the full schedule, see tirzepatide dosing guide.
How long does it take to reach the maximum dose of tirzepatide?
It takes 20 weeks to reach the maximum dose of 15 mg following the standard escalation schedule. The schedule is: 2.5 mg for weeks 0-4, 5 mg for weeks 4-8, 7.5 mg for weeks 8-12, 10 mg for weeks 12-16, 12.5 mg for weeks 16-20, and 15 mg for week 20 and beyond. Some people need to extend the escalation period if they experience side effects, which can add an extra 4-8 weeks to the timeline. For detailed dose schedules, see tirzepatide dose chart.
What if I am a slow responder to tirzepatide?
Slow responders are defined as people who lose less than 5% body weight by week 12. However, clinical trials show that 90% of slow responders eventually achieve clinically meaningful weight loss if they stay on tirzepatide for the full 72 weeks. Slow responders tend to be men, have higher starting BMI, have greater waist circumference, or have higher insulin resistance. If you are a slow responder, do not give up. Stick with the protocol, reach your maximum tolerated dose, and give it at least 6 months before evaluating effectiveness. For more on slow responders, see why not losing weight on tirzepatide.
How long do side effects last when starting tirzepatide?
Most gastrointestinal side effects like nausea, diarrhea, and constipation peak within 1-3 days after each injection or dose increase and resolve within 4-6 weeks. Nausea is most common during the first month and after each dose escalation. If side effects persist beyond 6 weeks at a stable dose, it may indicate the dose is too high. In that case, consider dropping back to the previous dose or extending the time between dose increases. For side effect management strategies, see peptide safety and risks.
External resources
For additional reading on tirzepatide speed and effectiveness, these authoritative sources provide peer-reviewed research and clinical data:
SURMOUNT-1 trial published in The New England Journal of Medicine
JCI Insight: Tirzepatide as an imbalanced dual GIP and GLP-1 receptor agonist
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay controlled, your metabolism stay optimized, and your progress stay consistent.