Feb 5, 2026

A single misread syringe line can waste an entire week of tirzepatide. That is not a hypothetical scenario. It happens constantly. Someone draws up what they believe is 5 mg, but their concentration is 10 mg/mL, not 5 mg/mL. They just injected double their intended dose. The side effects hit hard. The vial runs out in half the expected time. And the cost, which already runs hundreds of dollars per month, effectively doubles overnight.
The core problem is deceptively simple. Tirzepatide doses are prescribed in milligrams, but syringes measure in units. These are not the same measurement. They are not even close to interchangeable. The number of units you draw depends entirely on the concentration of your specific vial, and concentrations vary wildly, from 2.5 mg/mL all the way up to 60 mg/mL. Drawing 50 units from a 5 mg/mL vial gives you 2.5 mg. Drawing 50 units from a 20 mg/mL vial gives you 10 mg. Same syringe reading. Four times the dose.
This confusion costs people real money. A 10 mg vial of compounded tirzepatide is not cheap. If dosing errors cause you to burn through it in two weeks instead of four, you have just thrown away half your investment. Multiply that over months of treatment and the financial waste becomes staggering. But the cost issue pales compared to the safety concern. Peptide safety depends on accurate dosing, and tirzepatide is a potent dual-receptor agonist that demands precision.
This guide eliminates every shred of confusion. You will find complete conversion charts for every common concentration, step by step reconstitution math for lyophilized powder, syringe reading tutorials, and a universal formula you can apply to any vial you ever encounter. Bookmark this page. You will use it every single week.
Understanding tirzepatide units vs milligrams
The confusion between units and milligrams is the single most common source of dosing errors in the peptide community. It trips up beginners and experienced users alike, because the terminology sounds interchangeable even though it is not. Let us break this down from the ground up so there is zero ambiguity moving forward.
Milligrams measure the mass of the active compound. When a protocol calls for 5 mg of tirzepatide, it means 5 milligrams of the actual peptide molecule, regardless of how it is dissolved, what volume of liquid contains it, or what syringe you use to draw it. Milligrams are absolute. They do not change based on your equipment or preparation method.
Units, on the other hand, measure volume on an insulin syringe. A standard U-100 insulin syringe holds exactly 1 mL of liquid, divided into 100 equal markings. Each marking represents 1 unit, and each unit equals 0.01 mL. So 50 units is 0.50 mL. And 100 units is a full 1.00 mL syringe. That is all a "unit" means in this context, a tiny fraction of a milliliter. It tells you nothing about how much tirzepatide you are actually getting.
The bridge between these two measurements is concentration.
Concentration tells you how many milligrams of tirzepatide are dissolved in each milliliter of solution. A vial labeled 10 mg/mL contains 10 milligrams in every 1 mL (100 units). A vial labeled 20 mg/mL packs twice as much peptide into the same volume. This is why calculating peptide dosages correctly requires knowing your concentration before touching a syringe. Without that number, you are guessing. And guessing with a compound as potent as tirzepatide, which acts on both GLP-1 and GIP receptors simultaneously, is a risk nobody should take.
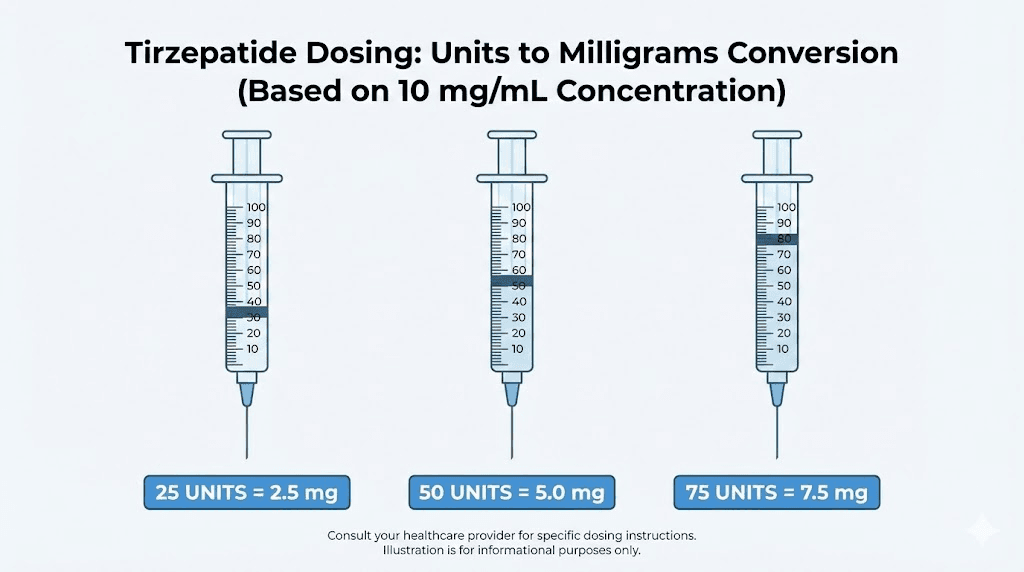
Here is a quick illustration of why concentration matters so much. Imagine three people all drawing exactly 25 units from their respective vials:
Person A has a 5 mg/mL vial: 25 units = 1.25 mg
Person B has a 10 mg/mL vial: 25 units = 2.5 mg
Person C has a 20 mg/mL vial: 25 units = 5.0 mg
Three identical syringe readings. Three vastly different doses. Person C is getting four times the tirzepatide that Person A is getting. If Person C thought they were taking a beginner dose of 2.5 mg, they just quadrupled it. The nausea alone could be debilitating, and the tirzepatide results would not be better for it. Higher doses do not always mean faster progress, especially when the body has not had time to adapt during the proper escalation schedule.
This is exactly why the peptide calculator exists. Plug in your vial concentration, your desired dose in milligrams, and it returns the exact number of syringe units to draw. No mental math. No room for error. For tirzepatide specifically, you can also use the tirzepatide dosing guide in units as a cross reference.
One more critical distinction. Do not confuse insulin syringe "units" with the pharmaceutical concept of international units (IU) used for compounds like HGH or insulin itself. When we say units in the context of tirzepatide dosing, we are always referring to the volume markings on a U-100 syringe. Tirzepatide is not measured in IU. It is measured in milligrams, and you convert those milligrams to syringe volume units using the concentration of your specific vial.
The universal conversion formula
Every conversion chart in this article flows from a single formula. Learn this formula and you can calculate the correct syringe units for any tirzepatide concentration, any dose, any vial. You will never need to memorize a chart again.
Here it is:
Units to draw = (Desired dose in mg / Concentration in mg per mL) x 100
That is it. Three numbers. One calculation.
Let us walk through exactly what each part means. The desired dose is whatever your protocol calls for, measured in milligrams. The concentration is printed on your vial label, measured in milligrams per milliliter. And the multiplication by 100 converts milliliters into syringe units, because a U-100 insulin syringe has 100 units per 1 mL.
Here is a concrete example. You want to take 5 mg of tirzepatide. Your vial is 10 mg/mL. Plug it in: (5 / 10) x 100 = 50 units. You draw to the 50 unit line. Done.
Another example. Same 5 mg dose, but now your vial is 20 mg/mL. The math changes: (5 / 20) x 100 = 25 units. Notice what happened. The dose stayed the same but the syringe volume dropped by half because the concentration doubled. If someone switched vials without recalculating, drawing 50 units from the 20 mg/mL vial would deliver 10 mg instead of 5 mg. That is a full dose tier higher than intended, and it is a mistake that beginners commonly make.
Let us try a more challenging one. You want 7.5 mg from a 30 mg/mL vial. The calculation: (7.5 / 30) x 100 = 25 units. Just 25 units for a fairly substantial dose. Higher concentrations mean smaller volumes, which is why they can be both convenient and dangerous. Convenient because you need less liquid per injection. Dangerous because a tiny misread on the syringe represents a large dosing error.
For those who prefer to think in milliliters first and then convert:
Volume in mL = Desired dose in mg / Concentration in mg per mL
Then simply multiply by 100 to get units. Or remember that 0.10 mL = 10 units, 0.25 mL = 25 units, 0.50 mL = 50 units, and 1.00 mL = 100 units.
This formula works for every peptide dosage you will ever calculate, not just tirzepatide. It works for semaglutide unit conversions, for BPC-157 dosing, for CJC-1295 dosing, for anything reconstituted or pre-mixed in a vial. The peptide reconstitution calculator at SeekPeptides automates this entire process, but understanding the underlying math means you can always verify your numbers independently.
Write this formula on a sticky note. Put it where you prepare your doses. Until it becomes second nature, double check every single time.
Complete tirzepatide dosage charts by concentration
Now we apply the formula to every standard concentration and every dose tier. These charts cover the vast majority of compounded tirzepatide products available. Print the chart that matches your vial concentration and keep it at your preparation station. Cross reference with the microdosing tirzepatide chart if you are starting at sub-clinical doses.
5 mg/mL concentration chart
This is one of the lower concentrations you will encounter. It is common in compounded vials and is often the result of reconstituting lyophilized tirzepatide with a moderate amount of bacteriostatic water. The tradeoff with lower concentrations is that you need more liquid per dose, which means larger injection volumes and faster vial depletion.
Desired dose (mg) | Units to draw | Volume (mL) | Notes |
|---|---|---|---|
1.0 mg | 20 units | 0.20 mL | Sub-clinical / microdose |
2.5 mg | 50 units | 0.50 mL | Starting dose |
5.0 mg | 100 units | 1.00 mL | Full 1 mL syringe |
7.5 mg | 150 units | 1.50 mL | Requires 2 injections |
10.0 mg | 200 units | 2.00 mL | Requires 2 injections |
Notice the problem at higher doses. At 5 mg/mL, anything above 5.0 mg exceeds a single 1 mL syringe. That means splitting the dose across two separate injections at two different sites. This is inconvenient but manageable. Some people inject both within the same session, choosing sites like the left and right sides of the abdomen. Others find the 5 mg/mL concentration impractical for higher dose tiers and switch to a more concentrated product.
If you are using a 5 mg total vial at this concentration, that vial contains just 1 mL of solution. At the starting dose of 2.5 mg per week, you get exactly two weeks of doses from one vial. Plan your supply accordingly and review the peptide therapy cost guide to budget for ongoing treatment. Understanding your peptide cost per dose helps prevent unexpected expenses.
10 mg/mL concentration chart
This is arguably the most popular concentration for compounded tirzepatide. It strikes a balance between manageable injection volumes and reasonable vial utilization. Most peptide dosing guides reference this concentration as the standard.
Desired dose (mg) | Units to draw | Volume (mL) | Notes |
|---|---|---|---|
1.0 mg | 10 units | 0.10 mL | Microdose |
2.5 mg | 25 units | 0.25 mL | Starting dose |
5.0 mg | 50 units | 0.50 mL | Half syringe |
7.5 mg | 75 units | 0.75 mL | Three-quarter syringe |
10.0 mg | 100 units | 1.00 mL | Full 1 mL syringe |
12.5 mg | 125 units | 1.25 mL | Requires 2 injections |
15.0 mg | 150 units | 1.50 mL | Requires 2 injections |
At 10 mg/mL, every dose up to 10 mg fits in a single syringe. That covers the first four escalation tiers without splitting injections. Only the 12.5 mg and 15 mg doses require two draws. This is a significant practical advantage and one reason this concentration remains so widely used.
A 10 mg total vial at this concentration contains 1 mL of solution and provides four weeks of the starting 2.5 mg dose. A 30 mg total vial contains 3 mL and lasts twelve weeks at the starting dose, or six weeks at 5 mg, or three weeks at 10 mg.
Track how many doses remain in your vial to avoid running out mid-escalation, because interrupting a peptide cycle can set back your progress and require restarting at lower doses.
20 mg/mL concentration chart
Higher concentration means smaller volumes. This is the sweet spot for many users on moderate to high dose tiers because even 15 mg fits comfortably in a single syringe. The precision demands increase, though, because each unit mark on the syringe represents more milligrams of tirzepatide.
Desired dose (mg) | Units to draw | Volume (mL) | Notes |
|---|---|---|---|
1.0 mg | 5 units | 0.05 mL | Very small volume |
2.5 mg | 12.5 units | 0.125 mL | Between 12 and 13 unit marks |
5.0 mg | 25 units | 0.25 mL | Quarter syringe |
7.5 mg | 37.5 units | 0.375 mL | Between 37 and 38 unit marks |
10.0 mg | 50 units | 0.50 mL | Half syringe |
12.5 mg | 62.5 units | 0.625 mL | Between 62 and 63 unit marks |
15.0 mg | 75 units | 0.75 mL | Three-quarter syringe |
Notice the half-unit readings at 2.5 mg, 7.5 mg, and 12.5 mg. A standard 1 mL syringe with unit markings does not have half-unit lines. You need to estimate the midpoint between two marks. This is where errors creep in. For the starting dose of 2.5 mg, you are targeting 12.5 units, which sits exactly between the 12 and 13 unit lines. Getting this wrong by even 2 units means a dosing error of 0.4 mg, which is significant at lower doses.
Some users solve this by using a 0.5 mL syringe instead of a 1 mL syringe. The 0.5 mL syringe has the same 100-unit total but spread over half the physical length, so the markings are spaced further apart and easier to read precisely. This is especially useful for the 20 mg/mL concentration where small volume differences matter more. The peptide injections guide covers syringe selection in greater detail.
All doses at 20 mg/mL fit in a single 1 mL syringe, which is a major convenience factor. No dose splitting required at any tier. This concentration works particularly well for those on the weight loss dosing protocol who plan to escalate through all six tiers.
Higher concentrations (30 mg/mL and 60 mg/mL)
These concentrations are less common but do exist in the compounded peptide market. They offer maximum convenience in terms of injection volume but demand extreme precision when drawing doses.
30 mg/mL concentration:
Desired dose (mg) | Units to draw | Volume (mL) |
|---|---|---|
2.5 mg | 8.3 units | 0.083 mL |
5.0 mg | 16.7 units | 0.167 mL |
7.5 mg | 25 units | 0.25 mL |
10.0 mg | 33.3 units | 0.333 mL |
12.5 mg | 41.7 units | 0.417 mL |
15.0 mg | 50 units | 0.50 mL |
At 30 mg/mL, most doses produce awkward fractional unit readings. The 2.5 mg dose requires 8.3 units, which is essentially impossible to measure precisely on a standard syringe. The 5 mg dose at 16.7 units is barely better. Only the 7.5 mg and 15 mg doses land on clean numbers. For this reason, 30 mg/mL is not ideal for beginners, and the getting started with peptides guide recommends more common concentrations for first-time users.
60 mg/mL concentration:
Desired dose (mg) | Units to draw | Volume (mL) |
|---|---|---|
2.5 mg | 4.2 units | 0.042 mL |
5.0 mg | 8.3 units | 0.083 mL |
10.0 mg | 16.7 units | 0.167 mL |
15.0 mg | 25 units | 0.25 mL |
Tiny volumes. At 60 mg/mL, the starting dose of 2.5 mg requires just 4.2 units, a barely visible amount of liquid. One unit of measurement error at this concentration represents 0.6 mg of tirzepatide. That is nearly 25% of the starting dose. The margin for error is razor thin.
High concentration vials are best suited for experienced users on established higher doses who value the convenience of minimal injection volume. If you are new to tirzepatide or still in the early escalation phases, stick with 10 mg/mL or 20 mg/mL. Use the dosage calculator to verify your numbers regardless of concentration.
Reconstituted tirzepatide dosage in units
If you are working with lyophilized (freeze-dried) tirzepatide powder rather than pre-mixed liquid, you control the final concentration based on how much bacteriostatic water you add. This gives you flexibility but also adds another variable that must be calculated correctly. Understanding how to reconstitute peptides is a prerequisite skill here.
The fundamental principle: more water means a lower concentration and larger injection volumes. Less water means a higher concentration and smaller injection volumes. Neither approach changes the total amount of tirzepatide in the vial. You are simply diluting or concentrating the same total peptide mass.
Here is the formula for determining your post-reconstitution concentration:
Concentration (mg/mL) = Total peptide in vial (mg) / Volume of water added (mL)
Then use the universal conversion formula from the previous section to calculate your syringe units for each dose. The free reconstitution calculator handles both steps automatically if you prefer not to do the math manually.
5 mg vial reconstitution
A 5 mg vial is the smallest common size. The amount of bacteriostatic water you add determines everything that follows.
Option A: 5 mg vial + 1 mL bacteriostatic water = 5 mg/mL
Desired dose (mg) | Units to draw | Volume (mL) | Doses per vial |
|---|---|---|---|
2.5 mg | 50 units | 0.50 mL | 2 doses |
5.0 mg | 100 units | 1.00 mL | 1 dose |
Option B: 5 mg vial + 2 mL bacteriostatic water = 2.5 mg/mL
Desired dose (mg) | Units to draw | Volume (mL) | Doses per vial |
|---|---|---|---|
1.25 mg | 50 units | 0.50 mL | 4 doses |
2.5 mg | 100 units | 1.00 mL | 2 doses |
With just 5 mg total peptide, this vial does not last long at standard doses. At 2.5 mg per week, you get two weeks from Option A or the same two weeks from Option B (just with larger volumes per draw). The 5 mg vial is best suited for people wanting to try tirzepatide at the starting dose before committing to a larger purchase. Keep in mind proper peptide storage to maximize the shelf life of your reconstituted solution.
10 mg vial reconstitution
The 10 mg vial is the workhorse of compounded tirzepatide. It offers enough peptide for multiple weeks at lower doses while remaining affordable for a single purchase. How much water to mix with your peptide depends on which dose tier you are targeting and how long you want each injection to last.
Option A: 10 mg vial + 1 mL bacteriostatic water = 10 mg/mL
Desired dose (mg) | Units to draw | Volume (mL) | Doses per vial |
|---|---|---|---|
2.5 mg | 25 units | 0.25 mL | 4 doses |
5.0 mg | 50 units | 0.50 mL | 2 doses |
10.0 mg | 100 units | 1.00 mL | 1 dose |
Option B: 10 mg vial + 2 mL bacteriostatic water = 5 mg/mL
Desired dose (mg) | Units to draw | Volume (mL) | Doses per vial |
|---|---|---|---|
2.5 mg | 50 units | 0.50 mL | 4 doses |
5.0 mg | 100 units | 1.00 mL | 2 doses |
Option A gives you a higher concentration with smaller draw volumes. Four weeks at the starting dose of 2.5 mg per week. Option B doubles the volume per draw but does not change the total number of doses. Both options provide the same amount of tirzepatide, just dissolved differently.
The practical recommendation: use 1 mL of water for the 10 mg/mL concentration unless you find very small volumes difficult to measure accurately. Some people with limited experience reading syringe markings prefer the larger volumes that come with more dilute solutions. As your mixing technique improves, you can transition to less water and smaller draw volumes.
30 mg vial reconstitution
The 30 mg vial is where things get interesting. With more total peptide, you have greater flexibility in choosing your concentration and far more doses per vial. This is the most cost-effective option for those on extended protocols.
Option A: 30 mg vial + 3 mL bacteriostatic water = 10 mg/mL
Desired dose (mg) | Units to draw | Volume (mL) | Doses per vial |
|---|---|---|---|
2.5 mg | 25 units | 0.25 mL | 12 doses |
5.0 mg | 50 units | 0.50 mL | 6 doses |
7.5 mg | 75 units | 0.75 mL | 4 doses |
10.0 mg | 100 units | 1.00 mL | 3 doses |
15.0 mg | 150 units | 1.50 mL | 2 doses |
Option B: 30 mg vial + 1.5 mL bacteriostatic water = 20 mg/mL
Desired dose (mg) | Units to draw | Volume (mL) | Doses per vial |
|---|---|---|---|
2.5 mg | 12.5 units | 0.125 mL | 12 doses |
5.0 mg | 25 units | 0.25 mL | 6 doses |
7.5 mg | 37.5 units | 0.375 mL | 4 doses |
10.0 mg | 50 units | 0.50 mL | 3 doses |
15.0 mg | 75 units | 0.75 mL | 2 doses |
Twelve weeks at the starting dose from a single vial. Six weeks at 5 mg. Three weeks at 10 mg. The 30 mg vial provides genuine long-term supply, especially at lower dose tiers. However, you must consider the shelf life of reconstituted peptides.
Most reconstituted tirzepatide solutions remain stable for roughly 28 to 30 days in a refrigerator. If your vial contains more doses than you will use in that window, you may need to accept some waste or find ways to use it before expiration. The post-reconstitution storage guide covers best practices for extending stability.
One important consideration with the 30 mg vial at 20 mg/mL (Option B): when you are at the 2.5 mg starting dose, you only need 12.5 units. That is a very small volume, and precision matters enormously. Each unit of error equals 0.2 mg. If you are new to peptide preparation, the 10 mg/mL option (Option A) with its larger draw volumes will be more forgiving of slight measurement inaccuracies. Once you are comfortable with the tirzepatide reconstitution process, you can optimize toward smaller volumes.
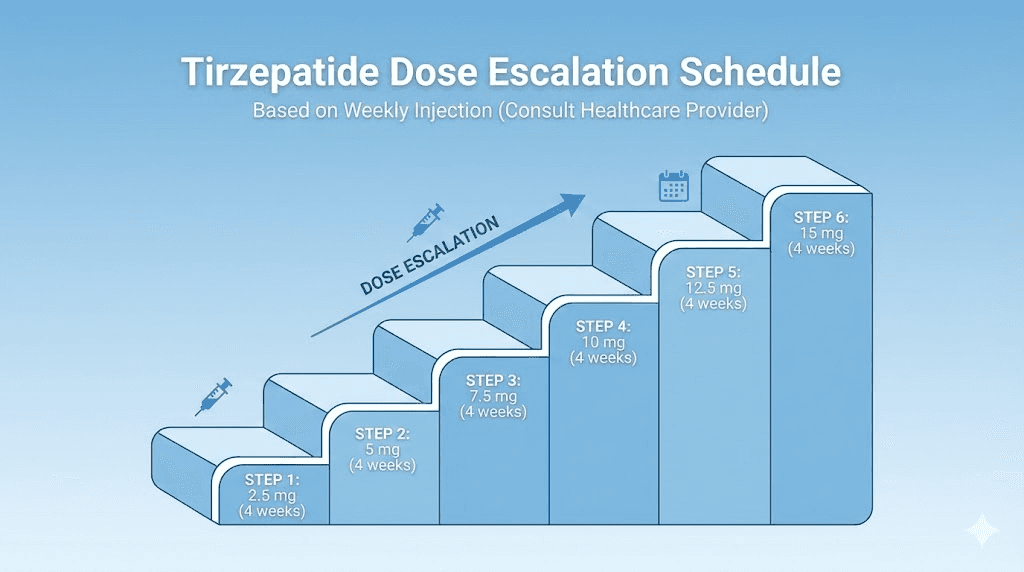
FDA-approved tirzepatide dose escalation schedule
Tirzepatide follows a structured dose escalation protocol. You do not start at your target dose. You build up to it gradually over weeks or months, giving your body time to adapt and minimizing gastrointestinal side effects. This is not optional. Skipping tiers or escalating too quickly is the fastest path to severe nausea, vomiting, and potentially abandoning treatment altogether.
The FDA-approved schedule for Mounjaro and Zepbound follows this pattern:
Tier | Weekly dose | Duration | Purpose |
|---|---|---|---|
1 | 2.5 mg | 4 weeks minimum | Initiation, not therapeutic |
2 | 5.0 mg | 4 weeks minimum | First therapeutic dose |
3 | 7.5 mg | 4 weeks minimum | Intermediate escalation |
4 | 10.0 mg | 4 weeks minimum | Moderate dose |
5 | 12.5 mg | 4 weeks minimum | Higher dose |
6 | 15.0 mg | Maintenance | Maximum approved dose |
The 2.5 mg starting dose is explicitly described as an initiation dose, not a therapeutic dose. Its primary purpose is to let your GI system adjust to the presence of a GIP and GLP-1 receptor agonist. Some people do notice appetite suppression and early weight changes at 2.5 mg, but the meaningful clinical effects typically begin at 5 mg.
Four weeks is the minimum at each tier. Some people stay at a given dose for longer, either because they are still experiencing good results, because side effects have not fully resolved, or because their provider recommends a slower escalation. There is no penalty for staying at a lower dose longer than four weeks. In fact, a conservative dosing approach often leads to better long-term adherence and fewer interruptions from side effects.
Not everyone needs to reach 15 mg. The SURMOUNT-1 clinical trial demonstrated significant results across all dose groups. Participants on just 5 mg lost an average of 15% of their body weight over 72 weeks. The 10 mg group averaged 19.5%. And the 15 mg group achieved 20.9%. The difference between 10 mg and 15 mg was only about 1.4 percentage points, suggesting diminishing returns at the highest doses. Many users find their optimal balance somewhere in the 7.5 mg to 10 mg range, where they achieve meaningful weight loss, which is a key goal for those exploring peptides for fat loss, without the increased side effects that come with maximum dosing.
In the SURMOUNT-1 trial, 91% of participants on 15 mg lost at least 5% of their body weight, and 57% lost 20% or more. These are remarkable numbers. But the real takeaway for dosing purposes is that the escalation schedule is designed for safety, not speed. Trust the process. Let each tier do its work before moving up.
If you are considering tirzepatide alongside other compounds, such as cagrilintide with tirzepatide or combining it with a weight loss peptide stack, the escalation schedule becomes even more important. Layering multiple active compounds without proper titration increases the risk of adverse effects significantly.
Reading your insulin syringe correctly
Having the right numbers from a conversion chart means nothing if you cannot accurately draw that amount into your syringe. Syringe reading errors are among the most common mistakes beginners make with peptides, and the consequences scale directly with concentration. This section teaches you to read your syringe with confidence.
U-100 syringe markings explained
The U-100 designation means the syringe is calibrated for a solution where 100 units equals 1 mL. This is the standard insulin syringe used worldwide and the syringe you will use for tirzepatide injections. It comes in several sizes, but the markings follow the same logic regardless of size.
A full-size 1 mL (100 unit) syringe has markings at every 1 unit interval, with longer lines every 5 units and numbers printed every 10 units. So you will see numbers at 10, 20, 30, 40, 50, 60, 70, 80, 90, and 100. Between each numbered line are nine smaller lines representing individual units.
When reading the syringe, look at the flat bottom edge of the plunger rubber stopper, not the curved top edge. This is critical. Liquid in a syringe forms a slight curved surface called a meniscus, and the rubber stopper itself has a domed shape. The dose measurement point is always the line that aligns with the flat front edge of the plunger tip. Reading from the wrong reference point can introduce a 1 to 2 unit error, which matters more at higher concentrations.
Hold the syringe at eye level with the needle pointing up. Tap the barrel gently to move any air bubbles to the top, near the needle.
Push the plunger slowly until the air is expelled and a tiny drop of liquid appears at the needle tip. Now pull back to your target mark. Check the reading at eye level, not from above or below. Parallax error from viewing at an angle can make you think you have more or less liquid than you actually do.
For tirzepatide doses that fall between unit marks, like 12.5 units or 37.5 units at the 20 mg/mL concentration, aim for the midpoint between the two adjacent lines. This takes practice. Some people find it helpful to draw slightly past the target mark and then push forward to it, as the plunger moves more smoothly in the push direction. This technique can help you dial in those half-unit measurements with greater precision. Reference the peptide injection basics for a visual walkthrough.
Choosing the right syringe size
Not all syringes are the same length, and this directly affects how easily you can read the markings. Here is a breakdown of common U-100 syringe sizes and when to use each:
0.3 mL (30 unit) syringe: Best for very small volumes. The markings are spread out over the barrel, making each unit line easier to distinguish. Ideal for high-concentration tirzepatide (20 mg/mL or higher) at lower doses. If your target is 12.5 units for a 2.5 mg dose at 20 mg/mL, this syringe makes that measurement far easier to nail than a 1 mL syringe would. The drawback is obvious: you cannot draw more than 30 units.
0.5 mL (50 unit) syringe: The versatile middle option. Handles doses up to 50 units with good readability. Works well for 10 mg/mL concentration through the first four dose tiers (up to 50 units for 5 mg). Also excellent for 20 mg/mL concentration at all standard doses except 15 mg (which requires 75 units). Many experienced injectable peptide users consider this their go-to syringe.
1 mL (100 unit) syringe: The standard. Handles any dose up to 100 units (1 mL). Necessary for 10 mg/mL concentration at 10 mg doses (100 units) and for any situation where you need to draw larger volumes. The markings are more compressed, so precision is slightly lower than with smaller syringes. Always use this size if your draw volume exceeds 50 units.
A practical tip: buy syringes in bulk and keep multiple sizes on hand. If your current dose falls in the 20 to 30 unit range, use a 0.3 mL syringe for better accuracy. If you escalate to a dose that requires 50+ units, switch to the 1 mL size. The cost difference is negligible, and the accuracy improvement is meaningful. Proper technique is part of overall peptide safety practice.
Common dosing mistakes and how to avoid them
Mistakes happen. But in the tirzepatide dosing world, the most common mistakes are also the most preventable. Each one ties back to a failure in one of three areas: knowing your concentration, reading your syringe, or following your schedule.
Mistake 1: Using the wrong concentration for your calculation.
This is the big one. Someone receives a new vial with a different concentration than their previous supply. They draw the same number of units as before without recalculating. The dose doubles, or halves, or lands somewhere unexpected. Always, always check the concentration on your vial label before every single draw. If you switched suppliers, switched vial sizes, or reconstituted with a different volume of water than last time, recalculate from scratch. The peptide calculator takes ten seconds to use. There is no excuse for skipping it.
Mistake 2: Confusing mL with units.
A protocol says "draw 0.25 mL" and someone draws to the 25 unit mark on a 1 mL syringe. Those are the same thing. No error there. But what if the protocol says "draw 25 units" and someone uses a 0.5 mL syringe, where the 25 mark actually represents 0.125 mL? Wait. That does not happen, because U-100 syringes are calibrated so that units always equal the same volume regardless of syringe size. Twenty-five units on a 0.3 mL syringe is 0.25 mL. Twenty-five units on a 1 mL syringe is also 0.25 mL. The confusion typically arises when people try to use non-U-100 syringes, like tuberculin syringes marked only in mL, and attempt to convert units in their head. Stick with U-100 insulin syringes. They are designed for exactly this purpose.
Mistake 3: Not accounting for dead space in the syringe.
Every syringe has a small amount of dead space in the hub, the area where the needle connects to the barrel. This dead space holds liquid that does not get injected. For most modern low-dead-space insulin syringes, this volume is negligible, around 0.007 mL. But for some older or cheaper syringes, dead space can be 0.05 mL or more. At high concentrations, 0.05 mL of dead space means you are losing 1 mg of tirzepatide per injection at 20 mg/mL. Over months of treatment, that adds up to significant waste and cost. Use low-dead-space syringes whenever possible. Consider it part of your peptide cost management strategy.
Mistake 4: Drawing air bubbles and not removing them.
Air bubbles reduce the volume of liquid you actually draw. A visible air bubble in the syringe barrel means you have less tirzepatide than the syringe reading suggests. Before injecting, always hold the syringe needle-up, tap the barrel to float bubbles to the top, and push the plunger until the air is expelled. Then verify your volume reading has not changed. If it dropped below your target, pull more liquid from the vial to compensate.
Mistake 5: Eyeballing doses instead of measuring precisely.
This happens more often than people admit. "I will just draw to about the same place as last time." "It looks close enough." These are the words of someone who will eventually overdose or underdose significantly. Precision matters with tirzepatide. The difference between a good dose and a problematic one is often just 5 to 10 units, especially at higher concentrations. Take the extra thirty seconds to check your work. Use good lighting, hold the syringe at eye level, and confirm the reading before you inject.
Mistake 6: Escalating doses too quickly.
Impatience kills protocols. Someone feels fine at 2.5 mg after two weeks, so they jump to 5 mg, then 7.5 mg a week later. The side effects compound. They feel terrible. They stop entirely. The recommended minimum of four weeks per tier exists because tirzepatide has a half-life of approximately five days, meaning it takes about three weeks (roughly five half-lives) to reach steady-state blood levels at any given dose. Until you have been at a dose long enough to reach steady state, you do not actually know how that dose truly affects you. Understanding how long peptides take to work helps set realistic expectations.
Managing side effects during dose escalation
Side effects are the reality of tirzepatide treatment. Most of them are gastrointestinal. Most of them are temporary. And most of them are manageable with the right strategies. But they will happen, especially during the early weeks of each new dose tier, so preparation matters.
The SURMOUNT-1 trial reported the following side effect rates among participants taking tirzepatide:
Nausea: up to 20% of participants
Diarrhea: approximately 16%
Constipation: approximately 11%
Decreased appetite: this is expected and often the desired mechanism of action
Vomiting: approximately 6 to 9%
Injection site reactions: mild, infrequent
Most side effects peak during the first one to two weeks after each dose increase and then gradually subside as the body adapts. This pattern repeats at each escalation tier. Some people breeze through certain tiers with minimal issues and then hit a wall at the next one. Others experience the worst side effects at the starting dose and find subsequent increases surprisingly smooth. The response is highly individual.
Here are evidence-based strategies for managing side effects during escalation:
For nausea: Eat smaller, more frequent meals rather than three large ones. Avoid high-fat, greasy, or heavily spiced foods during the first two weeks at a new dose. Ginger, whether as tea, capsules, or candies, has well-documented anti-nausea properties. Stay hydrated. Some people find that taking their injection in the evening before bed helps them sleep through the worst of the nausea. Timing your injection to coincide with a lighter activity day can also help.
For constipation: Increase fiber intake gradually. Drink more water than you think you need. Magnesium supplements, particularly magnesium citrate, can help. Gentle physical activity stimulates gut motility. If these measures are not sufficient, an over-the-counter osmotic laxative like polyethylene glycol is generally safe.
For diarrhea: This often resolves on its own within the first week. Stay hydrated with electrolyte-containing fluids. Avoid dairy and high-fiber foods temporarily. If diarrhea persists beyond two weeks, it may indicate the dose is too high, too soon.
The relationship between side effects and dosing is not purely linear. Sometimes a lower injection volume at a higher concentration causes fewer GI issues than a larger injection volume at a lower concentration, even at the same milligram dose. This is anecdotal and not clinically proven, but some users report it. The tirzepatide fatigue guide addresses another commonly reported side effect that many people do not anticipate.
If side effects at a new dose are truly intolerable after two full weeks of trying the strategies above, the appropriate response is to step back down to the previous dose for another two to four weeks before attempting the increase again. Do not push through severe symptoms. Do not skip doses to "recover." Consistency at a tolerable dose always produces better long-term results than an erratic pattern of high doses followed by breaks. This is the kind of practical insight that SeekPeptides members learn through comprehensive protocol access, not through trial and error.
For those exploring tirzepatide alongside other health optimization strategies, understanding how different compounds interact with the digestive system is relevant. The peptides for gut health resource provides broader context on gastrointestinal peptide mechanisms, and benefits and risks of peptides for physical and mental health gives an overview of the full spectrum of effects to consider.
Tirzepatide vs semaglutide dosing comparison
Many people considering tirzepatide have either used semaglutide before or are deciding between the two. The dosing systems are different enough to cause confusion, especially for those switching from one to the other. Understanding the comparison helps contextualize where your tirzepatide dose falls in terms of potency and expected effects. The semaglutide vs tirzepatide comparison page provides a full side-by-side analysis, but here we will focus specifically on the dosing differences.
The fundamental difference: tirzepatide is a dual GIP/GLP-1 receptor agonist, while semaglutide targets only GLP-1 receptors. This means tirzepatide activates two metabolic pathways simultaneously, which is why its clinical weight loss results consistently exceed those of semaglutide at comparable stages of treatment. It also means the dose ranges are completely different and should never be compared milligram to milligram.
Parameter | Tirzepatide | Semaglutide |
|---|---|---|
Mechanism | Dual GIP/GLP-1 | GLP-1 only |
Starting dose | 2.5 mg/week | 0.25 mg/week |
Max approved dose | 15 mg/week | 2.4 mg/week |
Dose range | 2.5 to 15 mg | 0.25 to 2.4 mg |
Escalation steps | 6 tiers | 5 tiers |
Common concentrations | 5, 10, 20 mg/mL | 1, 2.5, 5 mg/mL |
Avg weight loss at max | 20.9% (SURMOUNT-1) | 14.9% (STEP 1) |
The milligram numbers for tirzepatide are much higher than semaglutide, but that does not mean tirzepatide is "stronger per milligram." They are different molecules with different binding affinities and different pharmacokinetics. Comparing 5 mg of tirzepatide to 5 mg of semaglutide is like comparing 5 mg of one medication to 5 mg of a completely different medication. The numbers are not interchangeable.
What matters for practical dosing purposes is the syringe unit conversion. Because tirzepatide doses are 10 to 60 times higher in milligrams than semaglutide doses, tirzepatide typically comes in much higher concentrations (10 to 60 mg/mL vs 1 to 5 mg/mL for semaglutide). Despite the higher milligram amounts, the actual injection volumes are often similar between the two compounds. A 5 mg tirzepatide dose at 10 mg/mL requires 50 units. A 1 mg semaglutide dose at 2.5 mg/mL also requires roughly 40 units. Similar syringe readings, vastly different milligram amounts.
If you are transitioning from semaglutide to tirzepatide, do not try to find an "equivalent" dose by milligrams. Instead, start at tirzepatide 2.5 mg regardless of your previous semaglutide dose and follow the standard escalation. Your body needs to adapt to the dual-receptor mechanism, which is a different experience from GLP-1 alone. For those who want to see how semaglutide onset compares to tirzepatide onset, or who are curious about the detailed comparison, those resources cover the topic comprehensively.
One practical advantage of tirzepatide: because the dose range is wider (2.5 to 15 mg vs 0.25 to 2.4 mg for semaglutide), there is more room for fine-tuning. If 10 mg is too much but 7.5 mg is not quite enough, you can try 8 or 9 mg. This granularity is harder to achieve with semaglutide, where the steps are measured in fractions of a milligram. The semaglutide unit conversion guides show just how tight those tolerances are for the GLP-1 only compound.
For those researching the next generation of weight management peptides beyond both tirzepatide and semaglutide, the retatrutide dosage chart covers the emerging triple-agonist that adds a third receptor target to the equation. Understanding retatrutide vs semaglutide and retatrutide dosing further illustrates how the peptide landscape continues to evolve. The amylin receptor agonist class represents yet another avenue being explored for metabolic management.
Storage and stability after reconstitution
Getting your dose right means nothing if the tirzepatide in your vial has degraded before you use it. Peptides are proteins. Proteins are fragile. Temperature, light, and bacterial contamination can all destroy the active compound, leaving you injecting expensive water. Proper storage is not optional, it is a fundamental part of accurate dosing because a degraded peptide at the correct volume still delivers less than the intended dose.
Here are the storage rules for tirzepatide in every form:
Lyophilized (freeze-dried) powder, unreconstituted:
Store in the refrigerator at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit)
Can tolerate brief periods at room temperature during shipping
Keep in the original packaging, away from light
Shelf life: typically 12 to 24 months when stored properly
The peptide expiration guide covers this in more detail
Reconstituted solution:
Refrigerate immediately after reconstitution
Store at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit)
Use within 28 to 30 days of reconstitution
Never freeze reconstituted solution
Keep the vial upright to minimize rubber stopper contact with the solution
Review how long peptides last in the fridge for extended storage guidelines
Pre-mixed liquid (from compounding pharmacy):
Refrigerate upon receipt
Follow the expiration date on the label
Typically stable for 60 to 90 days when refrigerated
Do not use if the solution appears cloudy, contains particles, or has changed color
Temperature excursions are the most common storage failure. Leaving a vial on the counter for a few hours is generally fine. Leaving it in a hot car for an afternoon can destroy the peptide entirely. Room temperature stability is limited, and every hour above recommended storage temperature reduces the effective shelf life of your reconstituted tirzepatide.
Bacteriostatic water contains a small amount of benzyl alcohol (0.9%) that inhibits bacterial growth, which is why it is the preferred reconstitution medium over sterile water for multi-dose vials. If you reconstitute with plain sterile water, the solution must be used within 24 to 48 hours because there is no preservative to prevent bacterial contamination. Always use bacteriostatic water for peptides when reconstituting vials that will be used over multiple days or weeks.
One detail many people overlook: every time you puncture the vial stopper with a needle, you introduce a tiny amount of contamination risk. Use a fresh, sterile needle for every draw. Swab the stopper with an alcohol wipe before each puncture. These are basic practices covered in the peptide injections guide, but they bear repeating because complacency leads to contaminated vials and wasted product.
For those who reconstitute larger vials and worry about using all doses before the 28-day window, here is a practical framework. A 30 mg vial reconstituted to 10 mg/mL yields 3 mL of solution. At 2.5 mg per week (25 units = 0.25 mL per draw), that vial contains 12 doses, enough for 12 weeks. But the reconstituted solution only lasts about four weeks. That means roughly 8 doses (2 mL) will go to waste.
The solution is either to use a smaller vial size that matches your dose cycle, or to reconstitute with less water to create a higher concentration that depletes faster. Alternatively, some users reconstitute only a portion of the powder by splitting the lyophilized cake. This is technically possible but requires careful technique and carries contamination risks. The lyophilized vs liquid peptides comparison discusses the practical tradeoffs in more depth.
When to adjust your tirzepatide dose
Dose adjustment is not a set-it-and-forget-it decision. It requires ongoing assessment based on multiple factors: weight loss progress, side effect tolerance, appetite suppression levels, and overall well-being. Knowing when to go up, when to stay, and when to go down separates a thoughtful protocol from a reckless one.
Signs it is time to increase your dose:
You have been at the current dose for at least four weeks (the minimum)
Weight loss has plateaued for two to three consecutive weeks
Appetite suppression has noticeably diminished
You tolerated side effects well and they have largely resolved
You are not yet at your target weight or metabolic markers
Signs you should stay at your current dose:
You are still losing weight at a satisfactory rate
Appetite suppression remains effective
Side effects are present but manageable and still improving
You have been at this dose for less than four weeks
Signs you should decrease your dose:
Side effects are severe and not improving after two to three weeks
Nausea or vomiting prevents you from maintaining adequate nutrition
You are losing weight too rapidly (more than 1 to 1.5% of body weight per week consistently)
You are experiencing concerning symptoms beyond typical GI effects
Weight loss that is too rapid can lead to gallstone formation, excessive muscle loss, and nutritional deficiencies. The goal is steady, sustainable fat loss that preserves lean mass. Most clinical guidelines suggest 0.5 to 1% of body weight per week as an optimal rate. If you are consistently exceeding that, a lower dose may actually produce better body composition outcomes. This is where understanding the difference between raw weight loss and quality fat loss becomes important, a topic covered in the peptides for weight loss overview.
Women may find that their dose needs differ from men at equivalent body weights.
Hormonal cycles, body composition differences, and metabolic rate variations all influence tirzepatide response. The peptides for weight loss for women guide addresses these gender-specific considerations.
Plateaus are normal and do not always necessitate a dose increase. Before escalating, consider whether you have been consistent with your injection schedule, whether your dietary habits have shifted, and whether stress, sleep, or activity levels have changed. Sometimes the plateau breaks on its own after another week or two. Sometimes non-pharmacological adjustments, like increasing protein intake or adding resistance training, restart progress without requiring a higher dose. The peptides for muscle growth resources discuss how to preserve and build lean tissue during weight management protocols.
Some researchers explore microdosing approaches, where they stay below the standard starting dose or use doses between the established tiers. For example, someone might use 1.5 mg or 3.75 mg rather than jumping from 2.5 mg directly to 5 mg. The microdosing tirzepatide chart provides unit calculations for these non-standard doses. While not FDA-validated, microdosing allows for even more gradual escalation, which some individuals find reduces side effects substantially.
If you are using tirzepatide as part of a broader peptide protocol, dose adjustments become more nuanced. Adding or removing other compounds from your peptide stack can change how you respond to tirzepatide. The principle of conservative adjustment applies: change one variable at a time and observe for at least two weeks before making another change.
Trying to adjust tirzepatide dosing while simultaneously adding a new compound is a recipe for confusion about what is causing what. Understanding whether you can take multiple peptides simultaneously and the implications of doing so is worth reviewing before making protocol changes.
Practical tips for accurate weekly dosing
Theory is useful. Practice is where the results happen. Here are actionable strategies that experienced tirzepatide users employ to keep their dosing consistent, accurate, and as hassle-free as possible week after week.
Set a consistent injection day and time. Tirzepatide is a once-weekly injection. Pick a day that works for your schedule and stick with it. Many people choose Friday evening or Saturday morning so that any first-day side effects coincide with the weekend rather than work days. Consistency matters because the compound has a half-life of approximately five days, and maintaining steady blood levels depends on regular dosing intervals. If you miss your scheduled day, take it as soon as you remember and then resume your regular schedule the following week.
Prepare your workspace. Before every injection, lay out your supplies: vial of tirzepatide, alcohol wipes, a fresh syringe, and a sharps container. Good lighting is essential. A bright, direct light source makes syringe markings far easier to read than dim ambient light. Some people use a magnifying glass or the zoom feature on their phone camera to verify small syringe readings, especially at high concentrations.
Draw slowly, check twice. Rushing the draw process is how measurement errors happen. Insert the needle into the vial, invert it, and draw past your target mark by about 5 units. Then slowly push the plunger forward to your exact target. This approach eliminates the air that often enters during the initial draw and gives you precise control over the final reading. Verify the reading. Then verify it again. Only then do you proceed to injection.
Rotate injection sites. The standard rotation includes the abdomen (avoiding two inches around the navel), the front of the thighs, and the back of the upper arms. Rotating prevents lipodystrophy, the development of lumps or depressions in the tissue from repeated injection at the same spot. Lipodystrophy can also alter absorption rates, meaning the same dose might hit faster or slower depending on the tissue condition at the injection site. Keeping a simple log of which site you used each week helps maintain a consistent rotation.
Track every dose. A simple spreadsheet or notebook entry works. Record the date, the dose in milligrams, the units drawn, the concentration of your vial, and the injection site. Over weeks and months, this log becomes invaluable for identifying patterns, troubleshooting plateaus, and making informed dose adjustments. Members of SeekPeptides gain access to protocol tracking tools that simplify this process, and the peptide cycle planning guide offers a structured framework for long-term tracking.
Label your vials. If you reconstitute your own tirzepatide, write the concentration, reconstitution date, and expiration date (28 days later) directly on the vial with a fine-point permanent marker. Do this immediately after reconstitution, before you put the vial in the refrigerator. A week later, you will not remember whether you added 1 mL or 2 mL of water. That uncertainty leads to dosing errors.
Do not switch concentrations mid-vial. This sounds obvious, but it happens. Someone reconstitutes a new vial at a different concentration while still using their old vial. They grab the wrong one from the fridge. Same syringe reading, different dose. Keep only one reconstituted vial of tirzepatide in your refrigerator at a time. If you must have multiple vials, label them clearly and store them in different positions or containers.
For those who want a deep dive into every aspect of the injection process, from needle gauge selection to proper disposal of sharps, the complete peptide injection guide covers it all. Proper technique is a skill that improves with practice, and small improvements in technique compound over weeks into significantly better dosing accuracy and comfort.
Understanding tirzepatide pharmacokinetics for better dosing
Pharmacokinetics is the study of how a drug moves through your body: how fast it absorbs, how widely it distributes, how it gets metabolized, and how quickly it clears. Understanding even the basics of tirzepatide pharmacokinetics helps explain why the dosing schedule works the way it does and why certain dosing strategies produce better results than others.
Tirzepatide has a half-life of approximately five days. This means that five days after your injection, roughly half the administered dose remains active in your bloodstream. After another five days (ten days total), about one quarter remains. After fifteen days, about one eighth. This relatively long half-life is what makes once-weekly dosing possible. The compound stays active long enough to bridge the gap between injections without dramatic peaks and valleys.
However, the five-day half-life also means it takes time to reach steady-state concentrations. Steady state is the point where the amount entering your system each week equals the amount being cleared. For tirzepatide, this takes approximately four to five weeks at any given dose. This is why the four-week minimum at each escalation tier is not arbitrary. It is the minimum time needed to understand how that dose truly affects you at equilibrium.
During the first two weeks at a new dose, blood levels are still rising. Side effects during this period may be partially attributable to the upward trajectory rather than the final steady-state level. This is why many people experience peak side effects in weeks one and two at a new dose, with gradual improvement in weeks three and four. By week four, you are at or near steady state, and whatever you feel then is a reasonable representation of what that dose will be like long-term.
The absorption rate from subcutaneous injection is not instantaneous.
After you inject, tirzepatide slowly moves from the injection site into the bloodstream over hours. Peak blood levels typically occur 8 to 72 hours after injection, with significant individual variation. This gradual absorption is by design, as the compound includes modifications that slow its release, contributing to the long duration of action.
What does this mean for practical dosing? First, do not judge a dose by how you feel in the first 24 hours after injection. The peak has not arrived yet. Second, if you feel nothing for the first day or two, that is completely normal. The compound is still absorbing. Third, if you are comparing tirzepatide to semaglutide, note that semaglutide appetite suppression onset follows a different timeline because the two molecules have different absorption profiles despite similar half-lives.
For those researching the broader landscape of what peptides are and how they function, understanding pharmacokinetics at this level separates informed users from those who treat dosing as guesswork. Every peptide on the market has its own pharmacokinetic profile, and matching your dosing schedule to that profile is fundamental to getting the results you are after.
Cost optimization through accurate dosing
Tirzepatide is expensive. Compounded versions are more affordable than brand-name Mounjaro or Zepbound, but they still represent a significant ongoing expense. Every milligram wasted to dosing errors, degradation, or dead space is money lost. Accurate dosing is therefore not just a safety concern. It is a financial one.
Here is how dosing accuracy directly impacts cost:
Consider a 10 mg vial purchased for a given price. At 2.5 mg per week, that vial lasts four weeks if dosed accurately. If you consistently overdose by 20% due to syringe reading errors (drawing 30 units instead of 25 from a 10 mg/mL vial), you are actually taking 3 mg per week instead of 2.5 mg. Your four-week vial now runs out in 3.3 weeks. Over a year, you burn through 15.7 vials instead of 13. That extra 2.7 vials cost real money.
At higher doses, the math gets worse. An accidental 20% overdose at 10 mg per week means taking 12 mg. Your supply burns 20% faster across every vial, every month, every year. The peptide cost calculator helps quantify exactly what each dose costs, giving you a clear picture of the financial impact of accuracy.
Dead space waste is another silent cost driver. As mentioned earlier, standard syringes can trap 0.02 to 0.05 mL of liquid in the hub that never gets injected. At 20 mg/mL, 0.05 mL of dead space equals 1 mg of wasted tirzepatide per injection. Over 52 weekly injections, that is 52 mg of pure waste. Low-dead-space syringes cost marginally more per unit but save significantly over time. Reviewing the complete peptide therapy cost guide helps you factor in all these variables when budgeting for long-term treatment.
Choosing the right vial size for your dose tier also matters. If you are on 2.5 mg per week and buying 30 mg vials that expire in 28 days after reconstitution, you can only use 4 doses (10 mg) before the remaining 20 mg degrades. That is a 67% waste rate. Switching to 10 mg vials eliminates this problem entirely. The retatrutide cost guide illustrates similar principles for another high-value peptide compound, and the logic applies universally across all reconstituted peptides.
The bottom line: treating dosing accuracy as a cost control measure reframes the entire preparation process. Every extra minute spent verifying your concentration, checking your syringe reading, and properly storing your vial pays for itself many times over. The tools at SeekPeptides are designed to make this process as efficient and error-free as possible, from reconstitution calculators to dosage charts to comprehensive protocol guidance.
Oral tirzepatide and dosing differences
The development of oral tirzepatide represents a significant evolution in how this compound can be administered. While injectable tirzepatide remains the standard, oral formulations are emerging, and they come with their own dosing considerations that differ markedly from the injection-based system we have been discussing.
Oral peptides face a fundamental challenge: the digestive system is designed to break down proteins. Tirzepatide, being a peptide, would normally be destroyed by stomach acid and digestive enzymes before it could reach the bloodstream. Oral formulations use absorption enhancers and protective technologies to overcome this barrier. As a result, the bioavailability, the percentage of the compound that actually reaches the bloodstream, is much lower for oral versus injectable delivery.
This means oral tirzepatide doses are measured differently than injectable doses. You cannot simply take a 5 mg oral dose and expect it to be equivalent to a 5 mg injection. The oral dose needs to be higher to compensate for the lower absorption rate. The exact conversion factor depends on the specific oral formulation and varies between manufacturers.
For those currently using injectable tirzepatide and considering a switch to oral, the key point is that the dosing knowledge in this guide applies specifically to injectable preparations. The unit-based calculation system, the syringe reading techniques, and the concentration charts are all relevant to subcutaneous injection. Oral tirzepatide will use different dosing tables entirely.
The injectable vs oral peptides comparison provides a thorough analysis of the tradeoffs between these two delivery methods, covering absorption rates, convenience factors, cost differences, and efficacy data. For the broader question of oral peptide development, the GLP-1 patch technology article covers yet another delivery innovation worth watching.
Frequently asked questions
How many units is 2.5 mg of tirzepatide?
It depends entirely on your vial concentration. At 5 mg/mL, 2.5 mg equals 50 units. At 10 mg/mL, 2.5 mg equals 25 units. At 20 mg/mL, 2.5 mg equals 12.5 units. You must know your concentration before you can determine the units. Use the formula: (2.5 / concentration) x 100 = units. For a detailed breakdown specifically of this common starting dose, the 2.5 mg tirzepatide in units guide provides concentration-specific charts.
Can I use a regular syringe instead of an insulin syringe?
Technically, yes, but it is not recommended. Regular syringes (like tuberculin syringes) are marked in milliliters, not units. You would need to convert your dose to milliliters manually and then read the finer gradations on a non-insulin syringe. The markings are often less precise, and the risk of measurement error increases. U-100 insulin syringes are specifically designed for subcutaneous injections of this type. They have finer needles, more precise markings, and a direct unit-to-volume relationship that eliminates an extra conversion step. Stick with insulin syringes.
What happens if I accidentally inject too much tirzepatide?
An accidental overdose of tirzepatide typically intensifies gastrointestinal side effects: severe nausea, vomiting, diarrhea, and potentially dehydration. If you believe you have significantly overinjected (for example, double your intended dose), monitor your symptoms closely. Stay hydrated. Eat small, bland meals. Do not take your next scheduled dose until the extra amount has had time to clear (at least one full week, possibly longer depending on the magnitude of the overdose). If symptoms are severe, especially persistent vomiting or signs of dehydration, seek medical attention. And then figure out what went wrong with your calculation so it never happens again.
Is it safe to split a tirzepatide dose across multiple injections?
Yes. Splitting a dose is necessary whenever the required volume exceeds what a single syringe can hold. For example, 15 mg at 10 mg/mL requires 150 units (1.5 mL), which exceeds a standard 1 mL insulin syringe. You would draw 100 units in one syringe and 50 units in another, injecting at two different sites. Both injections should be done during the same dosing session. There is no pharmacokinetic disadvantage to splitting, though it does mean two needle sticks instead of one.
How do I know if my tirzepatide has gone bad?
Visual inspection is your first line of defense. Reconstituted tirzepatide should be a clear, colorless to slightly yellowish solution. If the liquid appears cloudy, contains floating particles, has changed color significantly, or has visible sediment at the bottom of the vial, do not use it. These are signs of degradation or contamination. Also consider the timeline: if more than 28 to 30 days have passed since reconstitution, discard the vial even if it looks fine. Degradation can occur at the molecular level without visible changes. A gradual loss of efficacy, where the same dose produces less appetite suppression or fewer effects than it used to, can also indicate degradation if all other variables have remained constant. Proper peptide storage practices minimize this risk.
Should I inject tirzepatide at the same time every week?
Consistency helps, but it does not need to be the exact same hour. Tirzepatide has a five-day half-life, so a few hours of variation in injection timing has negligible impact on blood levels. What matters more is maintaining a roughly seven-day interval between doses. If you normally inject on Saturday morning, injecting Saturday evening instead is perfectly fine. Shifting to Monday, however, would create a nine-day gap followed by a five-day gap the next week, which creates unnecessary fluctuation. If you need to change your injection day permanently, the standard approach is to inject the next dose slightly early or slightly late (within a two-day window) and then resume the new schedule from there.
Can I pre-fill syringes for the week or store drawn doses?
Pre-filling is possible but comes with caveats. A drawn syringe can be stored in the refrigerator for 24 to 48 hours in most cases, especially if drawn with sterile technique. However, pre-filling is generally unnecessary with a once-weekly injection. The main risk is that the peptide may interact with the rubber plunger or the syringe material over time, potentially reducing potency. Additionally, a pre-filled syringe is more difficult to verify for air bubbles compared to one freshly drawn. Best practice is to draw and inject in the same session.
Why do some sources give different unit numbers for the same dose?
Because they are referencing different concentrations. A source discussing 10 mg/mL vials will give different unit numbers than one discussing 5 mg/mL or 20 mg/mL vials. There is no universal "units for 5 mg of tirzepatide" because the answer changes with concentration. This is the most important concept in this entire guide. When you see a unit number for a dose, always check what concentration it assumes. If it does not specify the concentration, the information is incomplete and potentially dangerous. The peptide dosage calculation guide reinforces this principle across all injectable peptides.
External resources
SURMOUNT-1 trial publication in the New England Journal of Medicine
World Health Organization obesity and overweight fact sheet
Understanding peptide research and studies helps contextualize how clinical data translates into practical dosing guidelines. The scientific evidence behind tirzepatide is robust, and staying informed on new developments ensures your dosing approach reflects the latest understanding.
Tirzepatide dosing is not a guessing game. It is a precise calculation that depends on three things: your target dose in milligrams, the concentration of your specific vial, and a reliable syringe to measure the result. With the charts, formulas, and practical strategies in this guide, you have everything needed to dose accurately every single week. But knowledge without a system leads to errors, and errors with a compound this potent carry real consequences. SeekPeptides members access structured dosing protocols, calculators tailored to every major concentration, and a community of knowledgeable users who cross-check their work. If tirzepatide is part of your health strategy, having that support system turns accurate dosing from a weekly challenge into an automatic habit.
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay accurate, your concentrations stay labeled, and your protocols stay consistent. Join here.