Mar 25, 2026

What happens if your injection day falls on the worst possible day this week? Maybe you have a wedding on Saturday, a red-eye flight on Friday, or a medical procedure that requires fasting. Your GLP-1 medication sits in the fridge. Your regular injection day is tomorrow. And you are wondering whether you can just take it today instead.
The answer is not as simple as yes or no. It depends on which medication you use, how many hours have passed since your last injection, and whether you plan to shift your schedule permanently or just this once. Getting it wrong does not mean disaster, but it can mean a rough 48 hours of nausea, vomiting, and gastrointestinal distress that makes you regret the decision.
This guide covers everything you need to know about taking your GLP-1 injection early. The minimum hours between doses for every major medication. What actually happens in your body when doses overlap. How to change your injection day safely. And the specific scenarios, from travel to surgery to holidays, where early dosing makes sense and where it does not. SeekPeptides has compiled research from prescribing information, pharmacokinetic studies, and clinical guidelines to give you the most complete answer available.
The short answer: yes, but with rules
You can take most weekly GLP-1 medications a day early. One day ahead of schedule is generally safe for the majority of users. But "safe" comes with conditions.
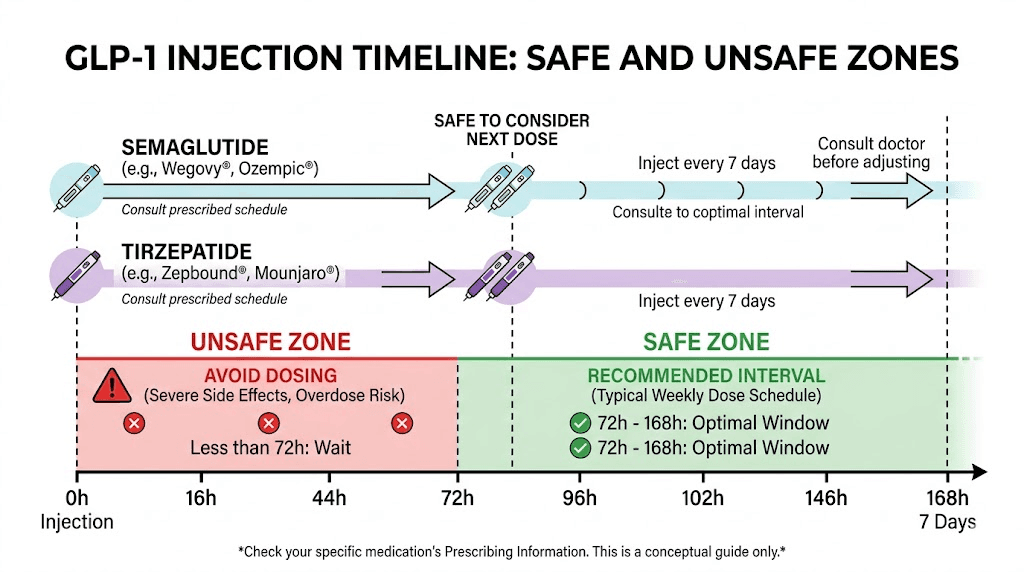
The critical rule is maintaining a minimum gap between injections. For semaglutide, that minimum is 48 hours. For tirzepatide, it is 72 hours. For other weekly GLP-1 agonists like dulaglutide, the standard recommendation is also at least 72 hours between doses.
If you normally inject on Saturday and want to inject on Friday instead, you are shortening your interval from 168 hours to approximately 144 hours. That still leaves a comfortable margin above the 48-hour or 72-hour minimums. You will be fine.
But if you injected on Wednesday and want to inject again on Friday? That is only 48 hours. Technically within the semaglutide minimum, but right at the edge for tirzepatide. And being at the edge means increased risk of bloating, nausea, and other gastrointestinal side effects that make the experience unpleasant.
Think of it this way. Your body processes these medications slowly. The half-life of semaglutide is approximately seven days, meaning half the drug is still in your system a full week later. Tirzepatide has a half-life of roughly five days. When you inject early, you are adding a new dose on top of a higher-than-usual residual level. One day early barely moves the needle. Two or three days early changes the math significantly.
Understanding GLP-1 pharmacokinetics and why timing matters
To understand why you can take a GLP-1 injection early but not too early, you need to understand how these medications move through your body. The pharmacokinetics explain everything.
How weekly GLP-1 medications maintain their levels
Native GLP-1, the hormone your body produces naturally, has a half-life of approximately two minutes. It breaks down almost instantly. That is useless for a medication.
So pharmaceutical engineers modified the structure. They attached fatty acid chains that bind to albumin in your blood, dramatically slowing breakdown. Semaglutide uses a C18 fatty diacid chain. Tirzepatide uses a C20 fatty diacid. These modifications extend the half-life from minutes to days, making once-weekly dosing possible.
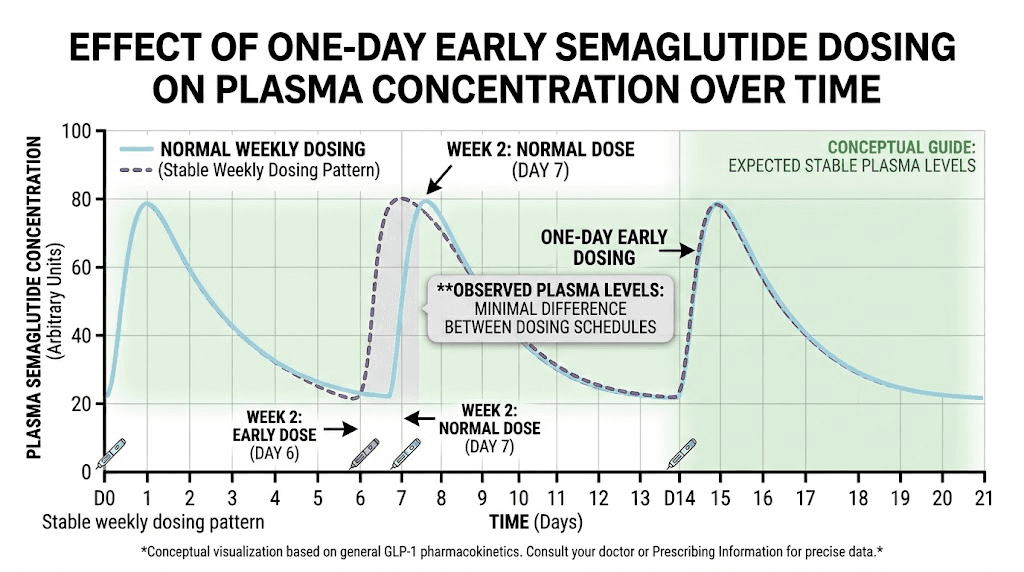
After you inject, the medication absorbs slowly from the subcutaneous tissue into your bloodstream. Peak blood levels occur roughly one to two days after injection. Then levels gradually decline over the following five to seven days until your next dose brings them back up.
This creates a wave pattern. Peak. Gradual decline. New dose. Peak again. Over time, after four to five consistent weekly doses, you reach what pharmacologists call steady state. At steady state, the peaks and troughs stabilize into a predictable rhythm. Your body adapts to this rhythm. Side effects diminish. Appetite suppression becomes consistent. Results become reliable.
When you inject early, you disrupt that rhythm. Not catastrophically, but measurably.
Half-life comparison across GLP-1 medications
Different GLP-1 medications have different pharmacokinetic profiles. This matters because the half-life determines how much drug remains in your system when you inject your next dose.
Medication | Half-life | Steady state | Minimum between doses | Missed dose window |
|---|---|---|---|---|
Semaglutide | ~7 days | 4-5 weeks | 48 hours | 5 days |
Tirzepatide | ~5 days | 3-4 weeks | 72 hours | 4 days |
Dulaglutide | ~5 days | 2-4 weeks | 72 hours | 3 days |
Exenatide ER | ~2 weeks | 6-7 weeks | 72 hours | 3 days |
Liraglutide (daily) | ~13 hours | 3-5 days | N/A (daily) | 12 hours |
Notice the pattern. Longer half-life means more drug overlap when you inject early. Semaglutide, with its seven-day half-life, has the most residual medication in your system at injection time. That is why the minimum spacing for semaglutide is only 48 hours, not 72. The prescribing information accounts for the fact that levels are already sustained.
Tirzepatide, with its shorter five-day half-life, drops faster between doses. The 72-hour minimum gives your body time to clear enough of the previous dose to avoid excessive peak concentrations. If you are using tirzepatide, that 72-hour rule is the one to remember.
What happens at the cellular level when doses overlap
GLP-1 receptor agonists work by binding to GLP-1 receptors on pancreatic beta cells, neurons in the hypothalamus, and cells throughout the gastrointestinal tract. When you inject early, you increase the concentration of drug molecules competing for those receptors.
The receptors do not care whether you took the dose on time or early. They simply respond to concentration. Higher concentration means stronger receptor activation. Stronger activation means more insulin secretion in response to food, slower gastric emptying, and greater appetite suppression.
Sounds good in theory. More appetite suppression. More fat loss. But the gastrointestinal effects scale with concentration too. More receptor activation in the stomach and intestines means slower stomach emptying, which is already the primary mechanism of action. Push it too far and you get the nausea, vomiting, and constipation that make the first few weeks of GLP-1 therapy so challenging.
One day early? The overlap is minimal. The difference in peak concentration is negligible for most people. Two days early on a medication with a 72-hour minimum? Now you are pushing into territory where side effects become noticeably more likely.
Semaglutide: specific early dosing rules
Semaglutide is the most commonly used weekly GLP-1 medication, available as Ozempic for type 2 diabetes and Wegovy for weight management. The early dosing rules differ slightly between the two, even though the active ingredient is identical.
The 48-hour minimum and 2-day flexibility window
According to the prescribing information, you may take semaglutide up to two days before or after your regularly scheduled injection day. If your usual day is Saturday, you can inject anytime from Thursday through Monday.
The absolute minimum spacing between any two doses is 48 hours. This is non-negotiable. Injecting within 48 hours of your previous dose significantly increases the risk of gastrointestinal adverse events and provides no therapeutic benefit.
If you use the semaglutide dosage calculator to determine your exact dose in units, remember that the timing rules apply regardless of dose size. Whether you are on the starting dose of 0.25 mg or a higher maintenance dose, the 48-hour minimum stays the same.
Ozempic vs Wegovy missed dose differences
Here is where it gets specific. The missed dose protocols for Ozempic and Wegovy are slightly different, and understanding them helps you make better decisions about early dosing too.
Ozempic (diabetes): If fewer than five days have passed since your missed dose, take it as soon as you remember. If five or more days have passed, skip it and take the next dose on your regular day.
Wegovy (weight loss): If your next scheduled dose is more than two days away, take the missed dose immediately. If the next scheduled dose is two days or fewer away, skip the missed dose. And here is the important part: if you miss two or more consecutive doses, you may need to restart the full titration schedule from 0.25 mg to avoid severe gastrointestinal side effects.
This tells you something important about early dosing too. The medication is designed with built-in flexibility. One day early is well within the approved window. The system accounts for real-life variability.
What early semaglutide dosing feels like
Most people who take semaglutide one day early notice nothing different. No extra nausea. No change in appetite suppression. No difference in weekly results.
Some people, particularly those still in the titration phase or those sensitive to gastrointestinal effects, report mild increases in nausea. This typically resolves within 24 hours. It is not dangerous. It is uncomfortable.
The people who run into real trouble are the ones who take it two or three days early, effectively creating a five-day or four-day cycle instead of seven. Over time, this leads to consistently higher drug levels, more side effects, and a pattern that can mimic overdosing. If you find yourself frequently injecting early, consider whether you would benefit from a split dosing schedule or a different injection day that works better with your routine.
Tirzepatide: specific early dosing rules
Tirzepatide works differently from semaglutide. It is a dual GIP/GLP-1 receptor agonist, meaning it activates two incretin pathways simultaneously. This dual mechanism affects both its efficacy and its timing requirements.
The 72-hour minimum rule
The prescribing information for tirzepatide (Mounjaro and Zepbound) states clearly: if you want to change the day of the week you take your injection, you must maintain at least 72 hours (three days) between doses. This is stricter than semaglutide.
Why 72 hours instead of 48? Tirzepatide has a shorter half-life of approximately five days compared to semaglutide at seven days. But the dual receptor activation means the gastrointestinal effects can be more intense, particularly during dose escalation. The extra buffer protects against the compounding of side effects that comes from overlapping doses.
If you normally inject on Sunday and want to inject on Saturday instead, you have a gap of approximately 144 hours from your previous Sunday injection. That is well above 72 hours. Completely safe.
If you injected on Thursday and want to inject again on Saturday, that is only 48 hours. Below the 72-hour minimum. Do not do this with tirzepatide.
How to safely take tirzepatide a day early
The process is straightforward. If your regular injection day is a specific day of the week, and you need to inject one day earlier, simply inject and then decide: do you want to keep the new day as your regular day going forward, or do you want to return to your original schedule next week?
Option one: adopt the new day permanently. Inject on Saturday this week, then Saturday next week, and every week after. Your new injection day is Saturday.
Option two: return to your original day. Inject on Saturday this week, then wait until your regular Sunday the following week (eight days later). The gap is longer than usual, which means slightly lower drug levels for that extra day, but it is safe and your schedule returns to normal.
Either option works. The important thing is that you never take two doses within 72 hours of each other. And you never take a double dose to make up for timing changes. One injection per week, period. If you are unsure about your exact dosage in units, calculate it before adjusting timing.
The 4-day missed dose window
If you miss your regular tirzepatide injection entirely, you have four days to take it. After four days, skip it. Do not try to catch up by doubling the next dose. And do not take two doses within 72 hours trying to get back on schedule.
This four-day window is shorter than semaglutide at five days, reflecting tirzepatide shorter half-life. The medication leaves your system faster, so the window for a late dose is narrower. Users who find themselves not seeing results should check whether missed or inconsistently timed doses are part of the problem.
What actually happens when you take GLP-1 a day early
Understanding the theory is useful. Understanding what actually happens in your body is more useful.
Gastrointestinal effects
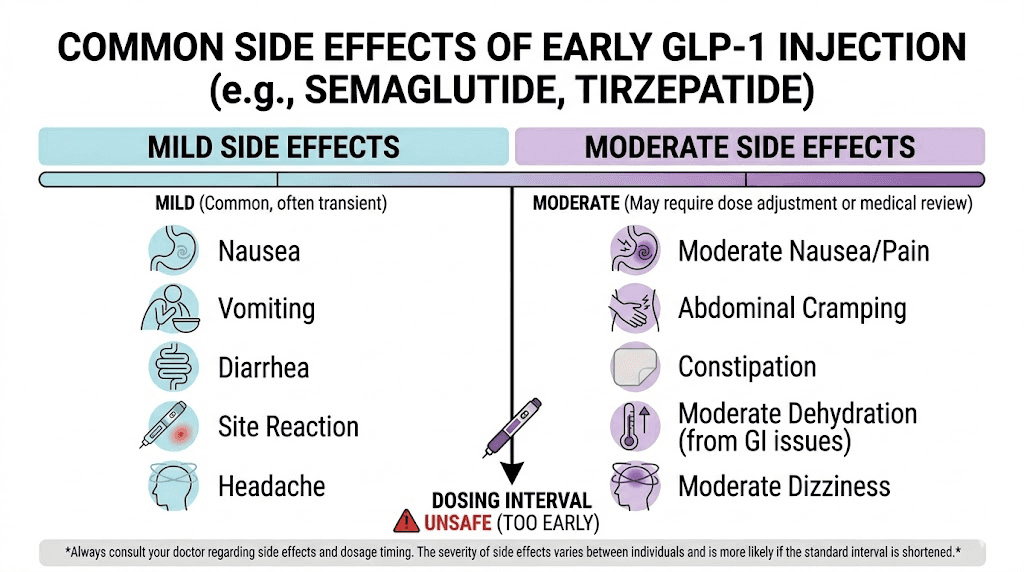
The most common consequence of early dosing is an increase in GI side effects. These are the same side effects you experienced during titration, just temporarily amplified.
Nausea. This is the big one. GLP-1 medications slow gastric emptying, which is part of how they reduce appetite and promote weight loss. When drug levels are temporarily higher due to early dosing, gastric emptying slows further. Food sits in your stomach longer. You feel full, then uncomfortable, then nauseated.
For most people taking their dose one day early, this effect is mild. Maybe a slight queasiness after meals. Maybe a reduced appetite that is more intense than usual for a day or two. It passes.
Vomiting. Less common with one-day-early dosing but possible, especially if you eat a large or fatty meal within hours of injection. The combination of peak drug levels and a full stomach is a recipe for trouble. Keep meals small and bland on the day you inject, especially if you are dosing ahead of schedule.
Constipation. Slower gut motility means things move less. If you already deal with constipation on your GLP-1, early dosing can make it worse for a few days. Stay hydrated. Consider a fiber supplement. And check our guide on the best fiber supplements for GLP-1 users if this is an ongoing issue.
Diarrhea. Paradoxically, some people experience the opposite. The gut responds to higher drug concentrations by speeding things along. This is less common but worth mentioning. If you experience diarrhea after early dosing, it typically resolves within one to two days.
Blood sugar effects
For people using GLP-1 medications for type 2 diabetes, blood sugar is the primary concern with early dosing. Higher drug levels mean stronger insulin secretion in response to meals, which could theoretically cause hypoglycemia.
In practice, GLP-1 agonists are glucose-dependent. They only stimulate insulin release when blood sugar is elevated. This built-in safety mechanism means the risk of hypoglycemia from GLP-1 monotherapy is extremely low, even with slightly early dosing.
The exception: if you take insulin or sulfonylureas alongside your GLP-1 medication. These medications can cause hypoglycemia independently, and the additive effect of higher GLP-1 levels could tip the balance. If you are on combination therapy and plan to take your GLP-1 dose early, monitor your blood sugar more frequently that day. Watch for trembling, sweating, confusion, rapid heartbeat, and dizziness, the classic signs of low blood sugar.
Appetite and energy effects
Some users report that early dosing produces a temporary boost in appetite suppression. This makes pharmacological sense. Higher peak levels mean stronger hypothalamic signaling, which translates to reduced hunger and earlier satiety.
This is not a reason to regularly dose early. The effect is temporary, and the increased side effect risk outweighs any marginal benefit. If you feel your appetite suppression is inadequate on your current schedule, talk to your provider about a dose adjustment rather than timing manipulation.
Fatigue is another reported effect. Some people feel more tired than usual on the day of injection, and this can be amplified when dosing early. The mechanism is likely related to the metabolic changes, reduced caloric intake combined with the body adjusting to higher drug levels. Rest. Hydrate. Eat protein. The fatigue typically lifts within 24 hours.
How to safely change your GLP-1 injection day
Sometimes you do not just want to inject one day early once. You want to permanently change your injection day. Maybe your original day no longer works with your schedule. Maybe you started on a random day and want to align with a more convenient one. Maybe weekends work better than weekdays or vice versa.
Whatever the reason, changing your injection day is straightforward if you follow the rules.
Step-by-step guide for semaglutide
Step 1: Choose your new injection day. Pick a day that works consistently with your weekly routine. Many people prefer the same time on their chosen day for consistency.
Step 2: Calculate the gap. How many hours will pass between your last injection on the old day and your first injection on the new day? It must be at least 48 hours. Ideally, keep it as close to your regular seven-day interval as possible.
Step 3: Inject on the new day. Take your regular dose at your chosen time. Do not adjust the dose amount.
Step 4: Continue on the new day going forward. Your new weekly schedule starts now. Inject on this same day every week.
Example: You currently inject on Wednesdays. You want to switch to Mondays. Inject on Monday instead of Wednesday. That is a five-day gap (well above 48 hours). Next Monday, inject again. Your new schedule is established.
Example going the other direction: You currently inject on Mondays. You want to switch to Thursdays. Inject on Thursday instead of the following Monday. That is only a three-day gap, which is still above 48 hours. Continue on Thursdays going forward.
Step-by-step guide for tirzepatide
The process is identical, but with one key difference: the minimum gap is 72 hours instead of 48.
Step 1: Choose your new injection day.
Step 2: Calculate the gap. Must be at least 72 hours (three full days) from your last injection.
Step 3: Inject on the new day at your regular dose.
Step 4: Continue on the new day weekly.
Example: You inject on Sundays. You want Fridays. Inject Friday instead of Sunday. That is a five-day gap from the previous Sunday. Well above 72 hours. Continue Fridays.
Example where it does not work: You inject on Thursdays. You want to switch to Saturdays. That is only a two-day gap. Below 72 hours. You cannot do this directly. Instead, wait until the following Saturday (nine-day gap), then continue on Saturdays. Or choose a different day that gives you the required minimum.
The one thing you must never do
Never take two doses in the same week to "reset" your schedule. This is the most dangerous timing mistake you can make. Two full doses within days of each other dramatically increases drug levels and can cause severe nausea, vomiting, and gastrointestinal distress. In rare cases, it could increase the risk of pancreatitis.
One dose per week. Always. If you need to change days, adjust the gap between doses, not the number of doses.
Travel scenarios and early dosing
Travel is the number one reason people consider taking their GLP-1 injection early. International flights, time zone changes, airport security concerns, and the logistics of keeping medication refrigerated while traveling all complicate injection schedules.
Flying across time zones
If you fly from New York to London, you lose five hours. If you fly from Los Angeles to Tokyo, you lose seventeen hours (or gain seven, depending on how you count). Time zones can make your injection timing confusing.
The simplest approach: stick with your injection day based on your home time zone for the first week of travel. If you normally inject on Wednesdays at 8 AM Eastern, inject at whatever time is 8 AM Eastern in your new location. That might be 1 PM in London or 10 PM in Tokyo.
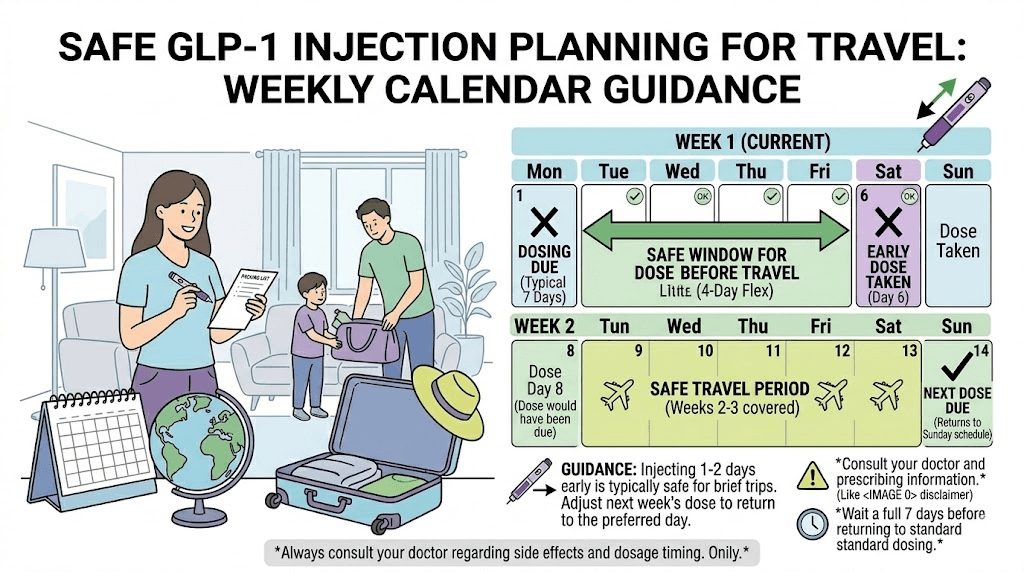
Alternatively, inject one day early before you leave. This gives you maximum flexibility during travel without worrying about timing. Your travel kit stays simpler, and you eliminate the stress of injecting in hotel rooms or airport bathrooms.
If you are traveling with tirzepatide specifically, check our guide on how to travel with tirzepatide for storage and temperature management tips. Keeping your medication at the right temperature is as important as timing. A GLP-1 travel case designed for temperature control makes this much easier.
Weekend events and schedule conflicts
Weddings, holidays, sporting events, social gatherings. Life happens on specific days, and sometimes those days coincide with your injection schedule.
If you know about the conflict in advance, inject one day early. Take your dose on Friday instead of Saturday, or Thursday instead of Friday. The one-day adjustment is well within safe parameters for all weekly GLP-1 medications.
If the conflict is with side effects rather than the injection itself, consider timing your dose so that peak side effects occur on a day when you can manage them. Peak drug levels hit one to two days post-injection. If you normally inject Friday and experience peak nausea on Sunday, and you have a big Sunday event, consider injecting Wednesday instead. Your peak effects will shift to Friday, leaving Sunday more comfortable.
Smart timing is not just about when you inject. It is about understanding your personal side effect pattern and planning around it. Keep a tracking log of your injections and symptoms to identify your pattern.
Medical procedures and fasting requirements
This deserves special attention. GLP-1 medications significantly slow gastric emptying. Many anesthesiologists and surgeons now require patients to hold GLP-1 medications before procedures that require fasting or general anesthesia. The concern is aspiration, food remaining in the stomach despite fasting because the medication has slowed emptying.
Current guidelines from the American Society of Anesthesiologists suggest holding weekly GLP-1 medications for at least one week before elective procedures requiring sedation or anesthesia. Some providers recommend two weeks.
If you have a procedure scheduled, do not take your GLP-1 injection early to "get ahead" of the hold period. Follow your surgical team instructions exactly. The timing of your GLP-1 around surgery is a medical decision, not a scheduling convenience. Check our guide on when to resume semaglutide after surgery for detailed protocols.
Early dosing vs missed dosing: which is worse?
This is a question many users face. Is it better to take your dose a day early or risk missing it entirely? The answer, in almost every scenario, is that early dosing is preferable to missing a dose.
The consequences of a missed dose
Missing a single GLP-1 dose typically produces noticeable effects within two to three days. Appetite returns. Cravings intensify. Blood sugar control loosens for diabetic patients. Weight loss progress stalls.
Missing two consecutive doses is more serious. With semaglutide (Wegovy), two missed doses may require restarting the full titration from the lowest dose. This means weeks of rebuilding to your therapeutic dose, during which your results suffer and you relive the initial side effects all over again. Nobody wants that.
Missing three or more doses effectively resets your body tolerance. You cannot simply resume your previous dose without risking severe side effects. The careful dose escalation that got you to your current level needs to happen again.
Why one day early is almost always the better choice
When you weigh the risks, early dosing wins. One day early carries a small risk of temporarily increased GI side effects. Missing a dose carries the risk of lost therapeutic benefit, potential dose reset, and the frustration of losing momentum.
If you are choosing between "inject today or possibly forget tomorrow," inject today. The minor increase in side effect risk from one-day-early dosing is far less consequential than the cascade of problems from a missed dose.
That said, do not use this as justification for routinely dosing early. The advice applies to occasional schedule adjustments, not a pattern of shortening your injection interval. If you consistently want to inject before your scheduled day, you probably need a permanent schedule change, not repeated early dosing.
Building a reliable injection routine
The best strategy is preventing the dilemma entirely. Set up systems that make forgetting nearly impossible.
Phone alarms work. Set one for the morning of your injection day and another for the evening as a backup. Medication tracking apps provide reminders and create a log you can reference. Some people link their injection to a specific weekly routine, like Sunday evening after dinner or Monday morning before work.
Store your medication somewhere visible but safe. If your semaglutide is in the fridge, put a sticky note on the fridge door on injection day. If you use a syringe rather than a pen, prep your supplies the night before.
Consistency is more important than perfection. Picking a day you can reliably hit every week matters more than picking the "optimal" day. There is no pharmacological advantage to injecting on Monday versus Thursday. The advantage comes from consistency.
Specific medication guides for early dosing
Each GLP-1 medication has its own characteristics that affect early dosing decisions. Here is a comprehensive breakdown for every major option.
Semaglutide (Ozempic, Wegovy, compounded)
Semaglutide has the longest half-life among commonly used GLP-1 medications at approximately seven days. This long half-life provides the widest flexibility window for early dosing.
Minimum between doses: 48 hours
Flexibility window: Up to 2 days early or 2 days late
Missed dose window: 5 days (Ozempic), varies (Wegovy)
One day early risk level: Very low
If you are using compounded semaglutide, the same timing rules apply. The active ingredient is identical regardless of source. Your dosage in units and injection timing follow the same pharmacokinetic principles. Just make sure your medication is properly stored, as compounded formulations may have different stability profiles.
Tirzepatide (Mounjaro, Zepbound, compounded)
Tirzepatide dual GIP/GLP-1 mechanism produces robust weight loss and glycemic control, but the shorter half-life means slightly less flexibility in timing.
Minimum between doses: 72 hours
Flexibility window: Must maintain 3-day minimum gap
Missed dose window: 4 days
One day early risk level: Low (as long as 72+ hours maintained)
Compounded tirzepatide follows the same rules. Whether you use a branded pen or draw from a vial using your syringe dosage chart, the 72-hour minimum applies. If you are in the early weeks of your starting dose, be especially cautious with early dosing since your body has not yet adapted to the medication.
Retatrutide (research phase)
Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors. It is still in clinical trials but has generated significant interest due to exceptional weight loss results in early studies. The pharmacokinetics suggest a half-life comparable to tirzepatide.
Because retatrutide is not yet commercially approved, there are no official prescribing guidelines for early dosing. However, based on its pharmacokinetic profile, a minimum of 72 hours between doses is a reasonable guideline. If you are researching retatrutide dosing, follow the same conservative approach as tirzepatide until official guidelines are published.
For those comparing options, our semaglutide vs tirzepatide vs retatrutide comparison covers the differences in mechanism, efficacy, and side effect profiles.
Liraglutide (Saxenda, Victoza)
Liraglutide is a daily GLP-1 medication with a 13-hour half-life. The early dosing question is different here because you inject every day, not weekly.
Taking liraglutide a few hours early is not a concern. The short half-life means drug levels fluctuate naturally throughout each day. If you normally inject at 8 PM and want to inject at 2 PM instead, the overlap is minimal. If you miss a dose entirely and it has been more than 12 hours, skip it and take your next dose at the regular time. Never double up.
Dulaglutide (Trulicity)
Dulaglutide has a half-life of approximately five days, similar to tirzepatide. The minimum spacing between doses is 72 hours (three days). One day early is safe. The missed dose window is three days, shorter than both semaglutide and tirzepatide.
Managing side effects when you do take it early
Even though one-day-early dosing is safe, you might still experience enhanced side effects. Here is how to manage them.
Nausea management
Eat smaller meals on injection day and the day after. Avoid high-fat, greasy, or heavily spiced foods. These take longer to digest and compound the gastric emptying delay caused by GLP-1 medications.
Ginger tea helps. So does peppermint. Some users find that eating a small amount of bland food, like crackers or toast, 30 minutes before injection reduces nausea. Others prefer to inject on an empty stomach. Experiment to find what works for you.
If nausea is severe enough to affect your daily activities, over-the-counter remedies like bismuth subsalicylate can provide relief. For persistent nausea that does not improve within 48 hours, contact your healthcare provider. Our guide on semaglutide tips covers additional nausea management strategies.
Constipation management
Hydration is the foundation. GLP-1 medications reduce food intake, which means less fiber and less water from food. Compensate by drinking more water than usual, at least eight to ten glasses per day on injection day.
Fiber supplements help. Psyllium husk, methylcellulose, or a dedicated fiber supplement for GLP-1 users can keep things moving. Magnesium citrate is another option, though start with a low dose to avoid overcorrecting into diarrhea.
Light physical activity, even a 20-minute walk after meals, stimulates gut motility and can counteract the slowing effects of elevated drug levels.
Fatigue management
If early dosing leaves you feeling more tired than usual, focus on protein intake and hydration. Adequate protein supports energy levels and prevents the muscle loss that can accompany aggressive caloric restriction on GLP-1 therapy.
Some users find that the right electrolyte supplement makes a significant difference. Reduced food intake means reduced electrolyte intake, which can manifest as fatigue, dizziness, and headaches. Sodium, potassium, and magnesium are the big three to watch.
Injection site management
Early dosing does not directly affect injection site reactions, but it is worth noting that rotating injection sites remains important regardless of timing. Do not inject in the same spot two weeks in a row. Rotate between abdomen, thighs, and upper arms.
If you experience redness, itching, or swelling at the injection site, applying a cold compress for 10-15 minutes before injection can reduce the reaction. Allowing the medication to reach room temperature before injecting also helps. For optimal injection technique, check our complete guide on GLP-1 injection sites.
When you should NOT take your GLP-1 early
There are specific situations where early dosing is a bad idea, regardless of how convenient it might be.
During active side effects from your last dose
If you are still experiencing significant nausea, vomiting, or other side effects from your most recent injection, do not inject early. Your body is telling you it is still processing the current dose. Adding more medication on top of active side effects is a recipe for a very bad day.
Wait until side effects subside. If they persist beyond five days, contact your healthcare provider. You may need a dose adjustment rather than a timing change.
During dose escalation
The first few weeks on any GLP-1 medication are the riskiest for side effects. Your body is adapting to the drug. Each dose increase brings a new wave of potential gastrointestinal symptoms as your receptors adjust to higher concentrations.
During this titration period, stick to your schedule as precisely as possible. Do not inject early. Do not inject late if you can help it. Consistency during dose escalation gives your body the best chance to adapt smoothly. If you have just started your first week on semaglutide or are moving up to a new dose level, keep your timing tight.
Within the minimum time window
This should go without saying, but do not inject within 48 hours (semaglutide) or 72 hours (tirzepatide) of your last dose under any circumstances. There is no emergency that justifies it. If you accidentally injected too early, do not take another dose to "fix" the schedule. Wait the full week from the accidental early dose, then resume your regular timing.
Before surgery or procedures
As discussed earlier, GLP-1 medications should be held before procedures requiring anesthesia. Do not try to "squeeze in" a dose before a surgical hold period. Follow your surgeon and anesthesiologist instructions exactly. The risk of aspiration under anesthesia is real and potentially life-threatening.
If you are pregnant or suspect pregnancy
GLP-1 medications are contraindicated during pregnancy. If you suspect you might be pregnant, stop all GLP-1 medications immediately and contact your healthcare provider. This is not a timing question. It is a safety question. For more information, see our guide on GLP-1 use and pregnancy.
Frequently asked questions about changing injection days
Users on these medications commonly ask more nuanced questions beyond simple early dosing. Here are answers to the most searched questions.
Can I permanently change my injection day?
Yes. You can change your injection day at any time, as long as you maintain the minimum gap between doses (48 hours for semaglutide, 72 hours for tirzepatide). Simply inject on the new day and continue weekly from there. There is no need to inform your pharmacy or get a new prescription. Your dosage and medication remain the same.
What is the best day of the week to inject?
There is no pharmacologically superior day. The best day is whichever day you can consistently remember and that gives you the least disruption from side effects. Many people prefer injecting on Friday evenings so that peak side effects (which hit 24-48 hours after injection) occur over the weekend when they can rest.
Does it matter what time of day I inject?
Clinical trials show no significant difference in outcomes between morning and evening injections. However, many users report that the time of day affects their side effect experience. Some prefer morning injections because nausea is less bothersome when they are active. Others prefer evening injections so they can sleep through the initial side effects. Experiment and find your pattern.
Can I take my GLP-1 every 5 days instead of 7?
This is not recommended unless directed by your healthcare provider. A five-day cycle means consistently higher drug levels, which increases side effect risk without proportional benefit. Some providers do prescribe shortened intervals for specific clinical scenarios, but this should be a medical decision, not a personal one. The standard once-weekly dosing is designed for the optimal balance of efficacy and tolerability.
What if I accidentally took two doses too close together?
Do not panic. Monitor yourself for increased side effects, particularly nausea and vomiting. Stay hydrated. Eat small, bland meals. Do not induce vomiting. Skip your next scheduled dose and resume your regular schedule the following week. If you experience severe symptoms like persistent vomiting, severe abdominal pain, or signs of pancreatitis (intense upper abdominal pain radiating to the back), seek medical attention immediately.
Does early dosing affect weight loss results?
A single instance of early dosing has no meaningful impact on your overall weight loss trajectory. The medication works through sustained exposure over weeks and months. One day of slightly higher drug levels does not accelerate or impede fat loss in any measurable way.
What does affect results is consistency. Regular, on-schedule dosing combined with appropriate nutrition, adequate protein intake, and physical activity produces the best outcomes. Occasional one-day adjustments are noise in the signal.
Can I split my weekly dose into two smaller doses?
Some healthcare providers prescribe split dosing, dividing the weekly amount into two doses given three to four days apart. This approach can reduce peak drug levels and minimize side effects for sensitive patients. Our guides on splitting semaglutide and splitting tirzepatide cover the protocols in detail. This is different from early dosing and should only be done under medical supervision.
How long until I reach steady state after changing my injection day?
A single one-day shift in injection timing does not meaningfully disrupt steady state. Your drug levels will be slightly higher or lower than usual for one cycle, then normalize. True steady state disruption only occurs with missed doses or significant (three or more days) shifts in timing. For semaglutide, steady state takes approximately four to five weeks of consistent weekly dosing to establish. For tirzepatide, approximately three to four weeks.
Tracking your injections and timing
Good tracking prevents timing mistakes. Here are practical systems that work.
Simple tracking methods
A notebook works. Write the date, time, dose, injection site, and any side effects after each injection. Review the log before your next injection to confirm timing.
A calendar app works better. Create a recurring weekly event on your injection day with a reminder set 24 hours before and another one hour before. This prevents both forgetting and accidental early dosing.
Medication tracking apps work best. Apps designed for injection tracking can calculate the exact hours since your last dose, send smart reminders, and flag if you try to log a dose too close to the previous one. Our guide on how to track GLP-1 injections reviews the best options available.
What to track beyond timing
While timing is the focus of this guide, tracking additional data points helps optimize your entire GLP-1 experience.
Side effects. Note which side effects you experience and their severity. Over time, patterns emerge. You might discover that injecting in the evening produces less nausea than morning injections, or that certain foods trigger worse symptoms on injection day.
Injection sites. Rotate systematically. Track which site you used each week to ensure proper rotation and to identify if certain sites produce more or fewer reactions.
Weight and measurements. Weekly weigh-ins on a consistent day and time provide the best data. Home monitoring tools can help track additional metrics like body composition.
Food and hydration. Many users find that their food choices on injection day significantly affect their side effect experience. Tracking what you eat before and after injection helps identify triggers.
The role of your healthcare provider
This guide provides comprehensive information, but it does not replace medical advice. There are situations where talking to your provider before changing your injection timing is important.
When to call your provider
Contact your healthcare provider if you are considering a permanent schedule change and are currently in the titration (dose escalation) phase of treatment. The titration period is when your body is most sensitive to timing variations, and your provider may have specific preferences about when you inject relative to your dose increases.
Also contact your provider if you accidentally took two doses too close together and are experiencing severe side effects. If nausea lasts more than 48 hours after early dosing, or if you experience vomiting that prevents you from keeping food or liquids down, seek medical advice.
If you take insulin or sulfonylureas alongside your GLP-1 medication, discuss any timing changes with your provider. The interaction between these medications and altered GLP-1 levels could affect blood sugar management in ways that need monitoring.
What your provider needs to know
When you discuss timing changes, bring your injection log. Show your provider exactly when you have been injecting, which dose you are on, and any side effects you have experienced. This information helps them give specific, personalized guidance rather than generic recommendations.
For researchers and self-directed users, SeekPeptides provides comprehensive protocol guides, dosage calculators, and evidence-based resources to supplement professional medical guidance. The combination of provider oversight and detailed reference materials produces the best outcomes.
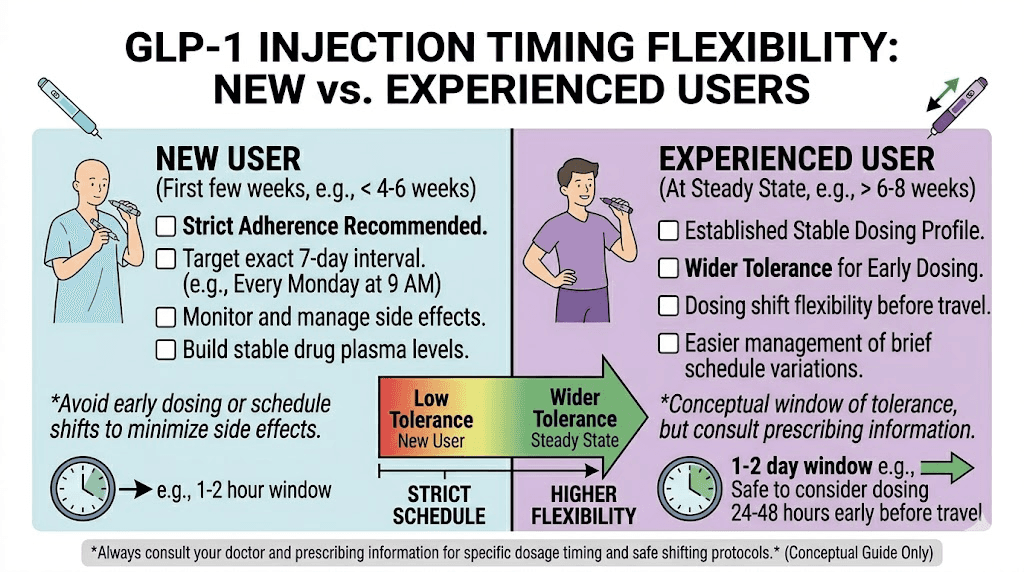
Advanced considerations for experienced users
If you have been on GLP-1 therapy for several months and have a stable side effect profile, there are some nuances worth understanding about injection timing flexibility.
Steady state provides more flexibility
Once you reach steady state (four to five weeks for semaglutide, three to four weeks for tirzepatide), your body has a baseline level of medication that fluctuates within a predictable range. At steady state, the difference between injecting on day six versus day seven is smaller in absolute terms than during the initial titration phase.
This means experienced users generally tolerate early dosing better than new users. Your GLP-1 receptors have adapted to sustained activation. A slightly higher peak from early dosing barely registers compared to the dramatic changes during your first few weeks on the medication.
That does not mean timing stops mattering. It means one-day adjustments become even less consequential over time. Your body has built tolerance. Use that tolerance for occasional flexibility, not habitual early dosing.
Dose-dependent considerations
Higher doses generally mean less flexibility with early dosing. If you are on the maximum dose of semaglutide (2.4 mg for Wegovy) or tirzepatide (15 mg for Mounjaro), your peak drug levels are already near the top of the therapeutic range. Adding an early dose creates a higher absolute peak than the same timing adjustment at a lower dose.
At lower doses, the margin is wider. A one-day-early injection of 0.5 mg semaglutide barely changes your drug level curve. A one-day-early injection of 2.4 mg creates a more noticeable spike.
If you are on a high dose and need to inject early, pay extra attention to side effect management. Smaller meals, more hydration, and electrolyte supplementation become more important. Keep supportive supplements on hand.
Seasonal and lifestyle considerations
Some users find that their injection timing preferences shift with seasons. Summer heat can affect medication storage and injection comfort. Winter holidays disrupt schedules. Vacation seasons create travel scenarios.
Rather than making frequent one-off timing adjustments, consider whether a permanent schedule change would better align with your seasonal routines. If you always struggle with Friday injections during summer travel season, maybe Tuesday is a better permanent choice year-round.
The key insight is that stability beats optimization. A consistent, imperfect schedule outperforms a theoretically perfect schedule that you cannot maintain. Pick a day and time that works 90% of the time and adjust occasionally for the other 10%. That is the approach that produces the best long-term results with the least stress.
Quick reference guide for every scenario
Here is a decision tree for the most common timing scenarios. Bookmark this section for quick reference.
Scenario | Semaglutide action | Tirzepatide action |
|---|---|---|
1 day early (planned) | Safe. Inject normally. | Safe if 72+ hours since last dose. |
2 days early (planned) | Safe if 48+ hours since last dose. | Safe if 72+ hours since last dose. |
3+ days early | Not recommended. Too close to minimum. | Not recommended. Exceeds guidelines. |
1 day late | Safe. Inject and continue schedule. | Safe. Inject and continue schedule. |
2-3 days late | Safe. Inject and resume regular day. | Safe within 4-day window. Inject and resume. |
5+ days late (sem.) | Skip dose. Resume next regular day. | N/A |
4+ days late (tirz.) | N/A | Skip dose. Resume next regular day. |
Travel across time zones | Inject 1 day early before travel OR follow home time zone. | Same, ensuring 72-hour gap. |
Before surgery | Follow surgeon instructions. Do NOT inject early to "get ahead." | Same. Hold per medical team guidance. |
Permanent day change | Inject on new day (48+ hour gap). Continue weekly. | Inject on new day (72+ hour gap). Continue weekly. |
Active side effects | Do NOT inject early. Wait for resolution. | Do NOT inject early. Wait for resolution. |
Print this table or save it to your phone. When the timing question comes up, you will have the answer in seconds rather than spending 20 minutes searching for guidance.
Nutrition and hydration around early dosing
What you eat and drink on injection day matters more when you dose early. Your body is processing a slightly higher concentration of medication, and the right nutrition strategy can make the difference between a comfortable transition and an unpleasant 48 hours.
Injection day nutrition
On the day you inject early, focus on these principles:
Small, frequent meals. Instead of three large meals, eat five or six smaller ones. This reduces the volume of food in your stomach at any given time, decreasing the likelihood of nausea from delayed gastric emptying.
Lean protein focus. Protein takes longer to digest than simple carbohydrates, but it does not trigger the same level of GI distress as fats. Chicken breast, fish, eggs, and Greek yogurt are good choices. For detailed meal planning, check our GLP-1 recipe guide.
Avoid trigger foods. Greasy, fried, heavily spiced, and very sweet foods are common triggers for GLP-1 related nausea. Foods to avoid on semaglutide and foods to avoid on tirzepatide overlap significantly, and they become even more important to avoid when dosing early.
Hydrate aggressively. Aim for at least 80-100 ounces of water on injection day. If plain water is unappealing, electrolyte drinks, herbal tea, and broth all count. Dehydration amplifies every GLP-1 side effect, from nausea to constipation to lightheadedness.
The day after early injection
Peak drug levels hit approximately 24-48 hours after injection. This means the day after early dosing is when you are most likely to feel enhanced side effects.
Continue the small meals approach. Continue aggressive hydration. If you feel nauseated, ginger in any form, tea, candied, supplements, helps. So does fresh air and light physical activity like walking.
By 48-72 hours after your early injection, drug levels settle into the same range as they would have been with regular timing. The enhanced effects are temporary. They pass.
Comparing GLP-1 injection timing to other peptide schedules
If you are familiar with peptide protocols beyond GLP-1 medications, understanding how their timing rules compare provides useful context.
Most research peptides follow completely different timing patterns. Peptide dosage charts show that many peptides require daily or twice-daily administration due to their short half-lives. BPC-157, for example, has a half-life of hours, not days. There is no concept of "early dosing" because you are injecting every day.
The weekly GLP-1 medications are unusual in the peptide world because of their engineered long half-lives. This is what makes them convenient for patients, one injection per week is much more manageable than daily injections, but it also creates the timing questions that do not arise with shorter-acting peptides.
For those researching peptide protocols more broadly, SeekPeptides offers comprehensive guides covering everything from reconstitution to storage to stacking protocols. Understanding the pharmacokinetics of each compound you use, whether GLP-1 or otherwise, is the foundation of effective and safe protocol management.
Common myths about GLP-1 injection timing
Misinformation about injection timing circulates widely on social media and forums. Let us correct the most persistent myths.
Myth: Taking it early makes it work faster
False. GLP-1 medications work through sustained receptor activation over weeks and months. A single early dose does not accelerate weight loss or improve blood sugar control. The medication works at the same rate regardless of whether you inject on day six or day seven of your cycle.
Myth: You should inject at the exact same time every week
Not necessary. While consistency in timing helps with remembering your dose, the pharmacokinetics of weekly GLP-1 medications are forgiving. A few hours earlier or later makes no meaningful difference. The important consistency is injecting on approximately the same day each week, not the exact same hour.
Myth: Early dosing leads to tolerance and reduced effectiveness
Also false. Tolerance to GLP-1 medications is not dose-frequency dependent. Some people experience reduced effectiveness over time, but this is related to metabolic adaptation and dose adequacy, not injection timing. One-day-early dosing does not accelerate tolerance development.
Myth: Morning injections are more effective than evening ones
Clinical data does not support this. Multiple studies have found no significant difference in HbA1c reduction or weight loss between morning and evening injection timing. The best time is whatever time works for your schedule and produces the fewest side effects for you personally.
Myth: You can take extra doses to speed up results
Dangerous and false. Taking extra doses increases the risk of serious adverse events including severe gastrointestinal distress, pancreatitis, and unpredictable blood sugar changes. More is not better with GLP-1 medications. Follow your prescribed dose and schedule. If your current dose is not producing adequate results, talk to your provider about a formal dose increase through the approved titration schedule.
Frequently asked questions
Can I take my GLP-1 shot 12 hours early?
Yes. Twelve hours is well within the acceptable window for all weekly GLP-1 medications. Whether you inject Sunday morning instead of Sunday evening, or Saturday night instead of Sunday morning, the difference in drug levels is negligible. This is the smallest adjustment you can make and carries virtually no additional risk.
What if I took my semaglutide 3 days early by accident?
If at least 48 hours have passed since your previous dose, you are within the approved minimum interval for semaglutide. Do not take another dose on your originally scheduled day. Either adopt the new day going forward or wait 8-10 days until your original day comes around again (ensuring at least 48 hours between any two doses). Monitor for increased nausea and bloating.
Is it safe to take tirzepatide 2 days early?
Only if at least 72 hours have passed since your last injection. If your normal schedule is Sunday, and you last injected Sunday, then injecting on Friday (five days later) gives you 120+ hours, which is safe. But if you last injected Wednesday and want to inject Friday, that is only 48 hours, which is below the 72-hour tirzepatide minimum. Check our detailed guide on taking tirzepatide 2 days early.
Will taking my injection early cause more nausea?
Possibly, but usually mild. The closer your doses are spaced, the higher the peak drug concentration, which can intensify the gastric emptying delay that causes nausea. One day early produces minimal additional nausea for most users. Eating bland foods, staying hydrated, and avoiding large meals around injection time helps prevent it.
Can I take my GLP-1 before a vacation and then take it late when I return?
Yes. Inject one day early before your trip, then take your next dose up to two days late after you return (semaglutide) or up to four days late (tirzepatide missed dose window). This gives you a 10-12 day gap between doses, which is longer than ideal but within the range where you can resume without retitrating. Just do not make a habit of this pattern.
Does the type of GLP-1 (oral vs injectable) change the early dosing rules?
Oral GLP-1 medications like oral semaglutide (Rybelsus) are daily medications with different pharmacokinetics than weekly injectables. Taking oral semaglutide a few hours early is fine. The early dosing concerns in this guide apply specifically to weekly injectable GLP-1 formulations where the long interval between doses creates the potential for significant overlap.
Should I adjust my diet on the day I take my injection early?
Yes. Eating smaller meals, focusing on lean protein, avoiding fatty and spicy foods, and increasing water intake all reduce the likelihood of enhanced side effects from early dosing. Our complete food guide for semaglutide and tirzepatide meal guide provide specific food recommendations.
How do I know if I have reached steady state?
Steady state occurs after four to five consistent weekly doses for semaglutide (about five weeks) and three to four doses for tirzepatide (about four weeks). You can estimate it using a GLP-1 plotter tool that visualizes drug levels over time. Clinically, steady state often correlates with a stabilization of side effects. If you no longer experience the same intensity of nausea or appetite changes after each dose, you have likely reached steady state.
External resources
Mayo Clinic - Semaglutide prescribing information and dosing guidelines
Mayo Clinic - Tirzepatide prescribing information and dosing guidelines
Cleveland Clinic - GLP-1 agonists overview and patient information
PMC - Comprehensive review of GLP-1 receptor agonist pharmacokinetics
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosage calculators, detailed protocol libraries, and a community of thousands who have navigated these exact questions about timing, dosing, and schedule management.
In case I do not see you, good afternoon, good evening, and good night. May your injection timing stay consistent, your side effects stay manageable, and your results stay on track.