Mar 21, 2026

Tired of conflicting advice about GLP-1 constipation? One source says drink more water. Another says take fiber. A third swears by magnesium citrate at bedtime. You have tried some of these. Maybe all of them. And you are still sitting on the toilet wondering why nothing is moving.
Here is the problem. Most guides treat GLP-1 constipation like ordinary constipation. It is not. When GLP-1 receptor agonists slow your gastric emptying, they change the entire rhythm of your digestive system, from stomach to colon. The strategies that work for general constipation often fall short because they do not account for the specific mechanisms these medications trigger. Your gut motility drops. Water absorption from your stool increases. And if you are eating less because the medication is doing its job suppressing appetite, you are also getting less fiber, less bulk, and less of the natural stimulation your colon needs to do its work.
This guide covers the complete picture. The mechanisms behind GLP-1 constipation. The hydration math most people get wrong. Fiber strategies that account for reduced food intake. Magnesium protocols backed by clinical evidence. Movement patterns that stimulate motility. Probiotics that target the right bacterial strains. And a complete daily protocol you can start using today. Whether you are on semaglutide, tirzepatide, or another GLP-1 medication, the relief strategies are the same. SeekPeptides has compiled the most comprehensive evidence-based approach to solving this problem for good.
Why GLP-1 medications cause constipation in the first place
Understanding the mechanism matters. Not because it is academically interesting, but because it changes which relief strategies actually work for you.
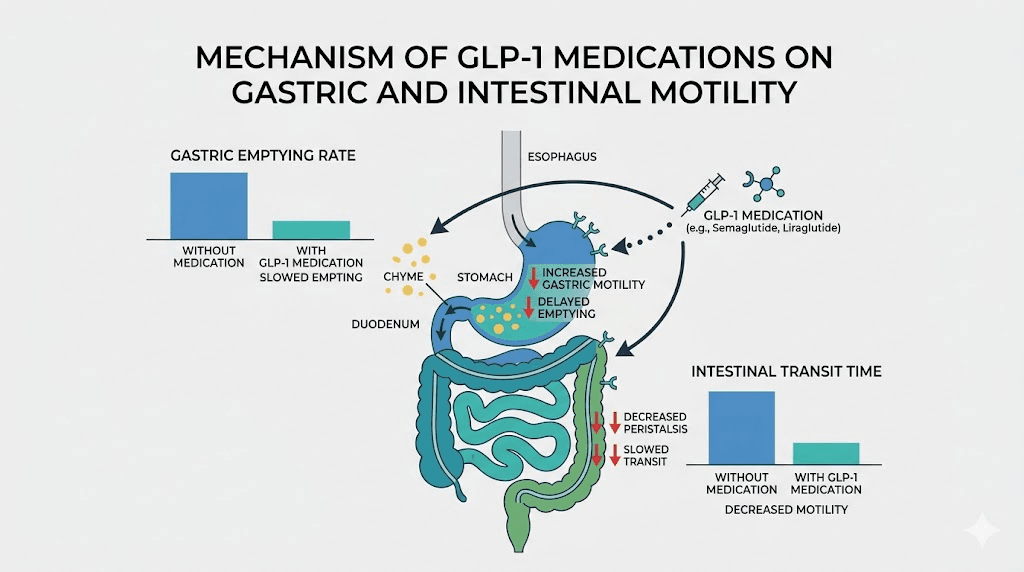
GLP-1 receptor agonists mimic a hormone your body produces naturally called glucagon-like peptide-1. This hormone does several things simultaneously. It signals your pancreas to release insulin. It tells your brain you are full. And, critically for this discussion, it slows gastric emptying, the rate at which food moves from your stomach into your small intestine.
That slowdown is the whole point. It is why you feel appetite suppression. It is why you eat less. But it does not stop at the stomach.
The same receptor signaling that slows gastric emptying also reduces motility throughout your entire gastrointestinal tract. Your small intestine moves food more slowly. Your large intestine absorbs more water from stool because the stool sits there longer. The result is harder, drier stool that becomes difficult to pass. Research published in the journal Diabetes, Obesity and Metabolism confirms that GLP-1 receptor agonists reduce intestinal transit time through direct action on smooth muscle cells lining the gut wall. This is not a bug in the medication. It is an inherent consequence of how the medication works.
There is a secondary mechanism too. Long-term use of GLP-1 receptor agonists may elevate endogenous GLP-2 release, which further reduces antral motility. Think of it as a compounding effect. The longer you take the medication, the more your gut adapts to a slower pace.
The behavioral amplifier most people miss
Here is where it gets worse. GLP-1 medications suppress appetite. That is their primary benefit for weight loss. But eating less means less fiber passing through your system. Less bulk in your stool. Less natural stimulation of the stretch receptors in your colon that trigger peristalsis, the wave-like contractions that move stool toward the exit.
So you have a double problem. The medication directly slows motility. And the reduced food intake removes the natural mechanical stimulus your colon relies on. This is why simply drinking a glass of extra water often does not fix things. You need a multi-pronged approach that addresses both the pharmacological slowdown and the behavioral reduction in gut stimulation.
The medications most commonly associated with this issue include semaglutide (sold as Ozempic and Wegovy), tirzepatide (Mounjaro and Zepbound), retatrutide, and oral GLP-1 formulations. The constipation mechanism is fundamentally the same across all of them, though the severity can vary based on dose, individual biology, and which specific side effect profile you experience.
How common is GLP-1 constipation and how long does it last
You are not alone. Not even close.
Clinical trial data paints a clear picture. In the STEP trials evaluating semaglutide for weight loss, constipation affected roughly 24-29% of participants. Tirzepatide trials showed rates around 12-27% depending on the dose. A systematic review and meta-analysis published in BMC Gastroenterology found that constipation rates with GLP-1 receptor agonists were approximately 2.5 times higher than placebo groups.
These numbers likely understate the real-world prevalence. Clinical trials define constipation strictly, typically as fewer than three bowel movements per week. But many people on GLP-1 medications experience a significant change in their bowel habits without meeting that clinical threshold. Going from daily movements to every other day, for example, can feel profoundly uncomfortable even if it does not technically qualify as constipation by clinical standards.
The timeline you need to know
There is good news buried in the data. Studies on semaglutide (Wegovy) showed that constipation typically lasted about 47 days and leveled off around week 10. This suggests that for many people, the gut eventually adapts to the medication, at least partially. The first few weeks tend to be the worst.
But adaptation is not guaranteed. Some people experience persistent constipation throughout their entire course of treatment. And for those who titrate up to higher doses, the constipation can return or worsen with each dose increase. This is why having a reliable relief protocol matters regardless of where you are in your treatment timeline.
The bottom line is straightforward. If you are taking any GLP-1 medication, you should proactively address constipation rather than waiting for it to become a problem. Prevention is significantly easier than treatment.
The hydration fix most people get wrong
Every guide on GLP-1 constipation starts with hydration. Drink more water. Simple advice. Except most people interpret this as adding one extra glass per day and calling it done.
That is not enough. Not even close.
When GLP-1 medications slow intestinal transit, your colon has more time to absorb water from stool. The stool sits in your large intestine for hours longer than it normally would. During that extended transit time, the colon extracts water relentlessly, leaving behind hard, dry, pellet-like stool that resists passage.
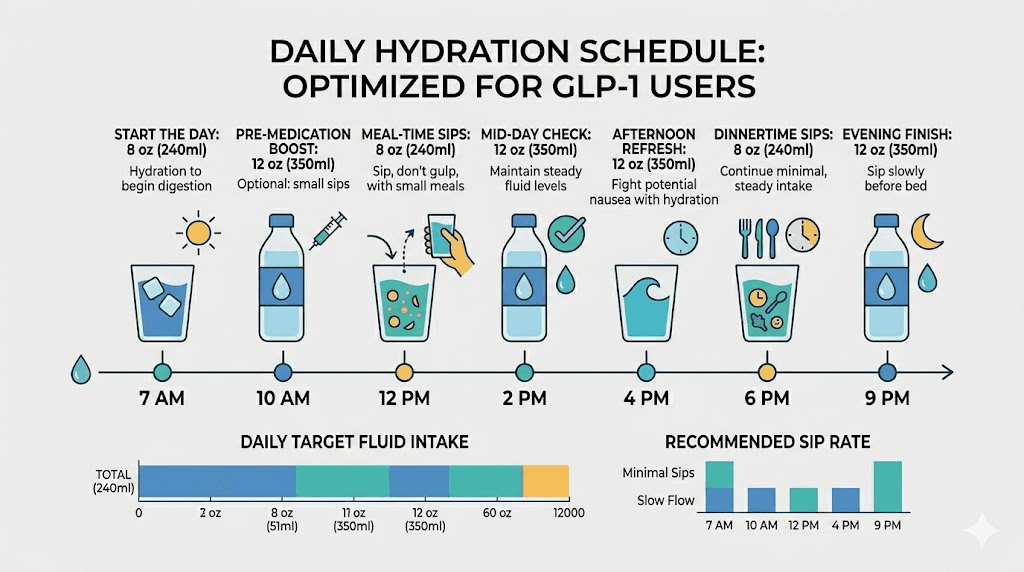
To counteract this, you need to consume enough water to keep stool soft despite the extended absorption time. The general recommendation for people on GLP-1 medications is 2 to 3 liters per day, which translates to roughly 67-100 ounces. For women, aim for at least 91 ounces. For men, at least 125 ounces. These numbers are higher than standard hydration guidelines because your body is actively working against you.
Timing matters more than total volume
Drinking 30 ounces of water at once does very little for constipation. Most of that water gets absorbed in the upper GI tract and never reaches your colon. Instead, distribute your water intake throughout the entire day.
A practical approach. Drink 8-12 ounces immediately upon waking. This triggers the gastrocolic reflex, a natural response where stomach filling signals the colon to make room by initiating a bowel movement. Follow that with consistent sips every 30-60 minutes throughout the day. Keep a water bottle visible. Set reminders if you need to.
Warm water in the morning can be particularly effective. The warmth accelerates the gastrocolic reflex more than cold water does. Some people find that warm water with lemon or a small amount of sea salt provides an additional gentle laxative effect through osmotic mechanisms.
One critical warning. If you are experiencing bloating alongside constipation, gulping large amounts of water quickly can make the bloating worse. Sip steadily rather than chugging. And if you are dealing with acid reflux as a concurrent side effect, avoid large water volumes immediately before or during meals, as this can worsen reflux symptoms while your gastric emptying is already delayed.
What counts toward hydration
Water is ideal. But herbal tea, broth, and water-rich foods like cucumber, watermelon, and celery all contribute. Coffee counts too, despite the old myth about it being dehydrating. Moderate coffee consumption actually has a mild prokinetic effect, meaning it stimulates colonic contractions. One to two cups in the morning may help.
Alcohol does not count. It is a diuretic that pulls water away from your colon. If you are wondering about drinking alcohol on semaglutide or tirzepatide, know that it can worsen constipation significantly in addition to its other interactions.
Fiber strategies that actually work on GLP-1 medications
Fiber is the cornerstone of constipation management. But on GLP-1 medications, the standard advice of just eat more fiber ignores a fundamental problem. You are eating less food overall. Your appetite is suppressed. Adding high-fiber meals when you can barely finish half a plate is impractical.
You need a strategic approach to fiber that accounts for reduced food intake.
Understanding the two types of fiber
Soluble fiber dissolves in water and forms a gel-like substance. It softens stool and makes it easier to pass. Think oats, chia seeds, flaxseeds, and psyllium husk.
Insoluble fiber does not dissolve. It adds bulk to stool and stimulates the stretch receptors in your colon that trigger peristalsis. Think vegetables, whole grains, wheat bran, and nuts.
You need both. But when food intake is limited, prioritizing soluble fiber tends to produce better results because it directly addresses the primary problem, stool that has become too hard and dry.
The fiber targets and how to hit them
Adults should aim for 25-35 grams of fiber per day. On a GLP-1 medication where you might be eating 1,200-1,500 calories instead of your usual 2,000+, hitting that target through food alone is genuinely difficult. This is where supplementation becomes essential.
The best fiber supplements for GLP-1 users include psyllium husk (Metamucil), methylcellulose (Citrucel), and ground flaxseed. Start with one teaspoon of psyllium husk per day in a full glass of water. Increase by one teaspoon every 3-4 days as tolerated. The gradual increase is critical because adding too much fiber too quickly when your gut is already slow will cause painful bloating and gas.
A realistic fiber protocol for GLP-1 users looks like this. Morning: 1-2 tablespoons of chia seeds in water or a smoothie (providing roughly 10 grams of fiber). Midday: one serving of psyllium husk supplement (providing 3-5 grams). Evening: vegetables with dinner (providing 5-10 grams depending on choices). Snack: a handful of almonds or an apple (providing 3-4 grams). Total: approximately 21-31 grams without requiring enormous meals.
Foods that pack the most fiber per bite
When you can only eat small portions, choose foods with the highest fiber density. These are your best options.
Food | Serving | Fiber (grams) | Calories |
|---|---|---|---|
Chia seeds | 2 tablespoons | 10 | 138 |
Split peas (cooked) | 1/2 cup | 8 | 115 |
Lentils (cooked) | 1/2 cup | 8 | 115 |
Black beans (cooked) | 1/2 cup | 7.5 | 114 |
Avocado | 1/2 medium | 7 | 120 |
Raspberries | 1 cup | 8 | 64 |
Pear | 1 medium | 6 | 100 |
Psyllium husk | 1 tablespoon | 5 | 18 |
Ground flaxseed | 2 tablespoons | 4 | 74 |
Notice something. Chia seeds deliver 10 grams of fiber in just 2 tablespoons. That is incredibly efficient when your stomach capacity is limited. Soak them in water for 15 minutes before consuming, as the gel they form actually helps lubricate stool passage. For more guidance on what to eat while managing side effects, see our guides on foods to eat on semaglutide and what to eat on tirzepatide.
The fiber timing rule
Do not take fiber supplements within 1-2 hours of your GLP-1 medication. This applies to both injectable and oral GLP-1 formulations. Fiber can slow absorption of other substances, and while GLP-1 injectables are absorbed subcutaneously rather than through the gut, taking fiber at the same time can worsen the feeling of fullness and nausea that some people experience. Timing your fiber intake between meals tends to work best.
Magnesium protocols for GLP-1 constipation
If hydration and fiber are the foundation, magnesium is the accelerator. It is one of the most effective, well-tolerated, and affordable strategies for GLP-1 constipation relief, and most people on these medications should be taking it.
Magnesium works through osmotic mechanisms. It draws water into the intestinal lumen, which softens stool and increases its volume. That increased volume stretches the intestinal wall, which triggers peristaltic contractions. It is essentially doing what GLP-1 medications are preventing, restoring the water content and mechanical stimulation your colon needs to function.
Which form of magnesium works best
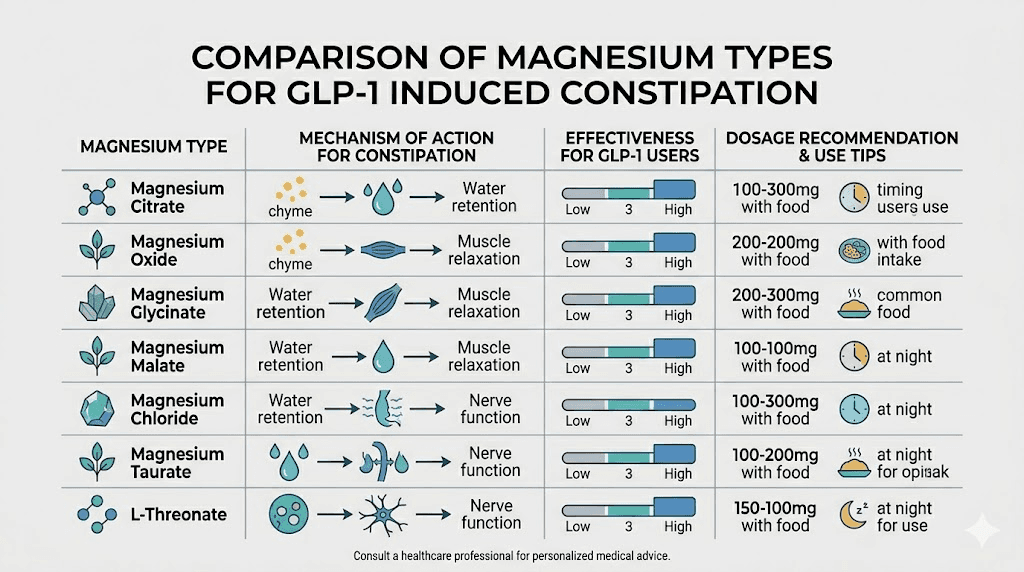
Not all magnesium is created equal. Different forms have dramatically different effects on the gut.
Magnesium form | Primary effect | Best for | Typical dose |
|---|---|---|---|
Magnesium citrate | Strong osmotic laxative | Acute relief | 200-400mg |
Magnesium oxide | Moderate osmotic laxative | Daily maintenance | 400mg at bedtime |
Magnesium glycinate | Minimal laxative effect | Sleep, muscle relaxation | 200-400mg |
Magnesium hydroxide | Strong osmotic laxative | Acute relief (Milk of Magnesia) | As directed on label |
For daily prevention of GLP-1 constipation, 400 milligrams of magnesium oxide taken at bedtime is the standard recommendation from gastroenterologists. It works gently overnight and typically produces a bowel movement within 6-12 hours. This can be done regularly without concern for physical dependency, unlike stimulant laxatives.
For acute episodes when you have not had a bowel movement in 3+ days, magnesium citrate provides faster, more powerful relief. Take 200-400 milligrams and expect results within 2-6 hours. Do not use magnesium citrate daily for extended periods, as it can cause electrolyte imbalances with regular use.
Magnesium and your GLP-1 supplement stack
Many GLP-1 users are already taking various supplements alongside their medication. Magnesium fits well into most stacks. It does not interact negatively with semaglutide, tirzepatide, or other GLP-1 medications. In fact, it complements other common additions like vitamin B12 and glycine.
If you are also taking supplements with tirzepatide, separate your magnesium dose from calcium supplements by at least 2 hours, as they compete for absorption. Take magnesium at night and calcium in the morning for optimal results.
Movement and exercise protocols that restore gut motility
Your colon responds to movement. Physical activity stimulates peristalsis through mechanical vibration, increased blood flow to the gut, and activation of the parasympathetic nervous system. When GLP-1 medications have slowed everything down, targeted movement can help restart the engine.
This is not about intense exercise. You do not need to run a marathon. In fact, extremely intense exercise can temporarily slow digestion by diverting blood flow away from the gut. What works best is consistent, moderate activity with specific timing.
The 15-minute post-meal walk
This is the single most effective exercise strategy for GLP-1 constipation. Walking for 15-20 minutes after meals stimulates the gastrocolic reflex, the same reflex that warm morning water triggers. The combination of food entering the stomach and physical movement creates a powerful signal for your colon to contract.
Studies show that a 15-minute walk after meals can reduce intestinal transit time by up to 30%. For someone on a GLP-1 medication where transit time is already extended, this can make the difference between a comfortable daily bowel movement and going 3-4 days without one.
Timing matters. Walk within 15-30 minutes of finishing your meal. Do not wait an hour. The gastrocolic reflex is strongest immediately after eating. A brisk pace is ideal, fast enough that you could hold a conversation but would prefer not to.
The 150-minute weekly minimum
Beyond post-meal walks, aim for at least 150 minutes of moderate-intensity aerobic activity per week. This is the same recommendation the American Heart Association makes for cardiovascular health, but it has direct benefits for gut motility too. Swimming, cycling, brisk walking, light jogging, or even dancing all qualify.
Spread this across the week rather than cramming it into one or two sessions. Five 30-minute sessions are more effective for gut motility than two 75-minute sessions because the prokinetic effect of exercise is relatively short-lived, lasting roughly 4-6 hours after the activity.
Targeted movements for constipation relief
Certain exercises specifically target the muscles and nerve pathways involved in bowel movements.
Abdominal massage. Lie on your back with knees bent. Using firm but gentle pressure, massage your abdomen in a clockwise direction (following the path of the colon) for 5-10 minutes. Start at the lower right, move up to the ribs, across the top, and down the left side. This physically helps move stool through the colon. Do this first thing in the morning or before attempting a bowel movement.
Knee-to-chest stretches. Lying on your back, bring one knee to your chest and hold for 15-30 seconds. Alternate legs. This compresses the abdomen and stimulates the descending colon.
Deep diaphragmatic breathing. The diaphragm sits directly above the transverse colon. Deep breathing creates a gentle massaging action on the colon from above. Breathe in through the nose for 4 counts, expanding the belly, hold for 4 counts, exhale slowly for 6 counts. Do 10 cycles.
These movements complement your overall GLP-1 management strategy and can be performed daily without any risk of overdoing it. If you are experiencing GLP-1 related fatigue, start with just the abdominal massage and gentle walking before adding more vigorous exercise.
Probiotics and gut health support on GLP-1 medications
Your gut microbiome plays a significant role in bowel regularity, and GLP-1 medications can alter its composition. Research published in Scientific Reports found that GLP-1 receptor agonists affect gut bacterial populations, potentially reducing strains that promote healthy motility while favoring strains associated with slower transit.
Probiotics offer a way to counterbalance these shifts. But not all probiotics help with constipation. Many commercial probiotic supplements target immune function or general gut health without specifically addressing motility. You need strains with demonstrated effects on transit time and stool consistency.
Strains that matter for constipation
Bifidobacterium lactis BB-12. One of the most studied strains for constipation relief. Clinical trials show it increases stool frequency and improves stool consistency. It works by producing short-chain fatty acids that stimulate colonic motility.
Lactobacillus rhamnosus GG. Improves intestinal transit time and stool frequency. Particularly effective when constipation is accompanied by bloating.
Bifidobacterium longum. Helps restore normal gut transit time. Studies in elderly populations, who share some constipation mechanisms with GLP-1 users (slower transit, reduced food intake), showed significant improvements in bowel movement frequency.
Akkermansia muciniphila. This strain has received particular attention in the GLP-1 context because it influences short-chain fatty acid production and may enhance endogenous GLP-1 production. Products like Pendulum GLP-1 Probiotic contain this strain specifically.
For detailed guidance on choosing the right probiotic, see our best probiotic for semaglutide guide, which covers strain selection, dosing, and timing in depth.
Fermented foods as a probiotic source
Supplements are convenient, but fermented foods provide both probiotics and prebiotics in a food matrix that may enhance survival through the stomach. Good options include kefir (especially effective for constipation), sauerkraut, kimchi, yogurt with live cultures, and miso. Aim for at least one serving of fermented food daily.
Prebiotics, the fiber that feeds beneficial bacteria, deserve attention too. Garlic, onions, asparagus, bananas, and Jerusalem artichokes are rich prebiotic sources. When you eat these foods, they pass through your upper GI tract undigested and reach the colon where they feed the exact bacterial strains that promote healthy motility. Products like GLP-1 postbiotic supplements and gut response formulas combine prebiotics and postbiotics specifically for GLP-1 users.
Over-the-counter solutions ranked by effectiveness
When lifestyle changes alone are not enough, over-the-counter solutions can provide meaningful relief. But the options are overwhelming. Osmotic laxatives. Stimulant laxatives. Stool softeners. Bulk-forming agents. Lubricants. Which ones actually work for GLP-1 constipation, and which should you avoid?
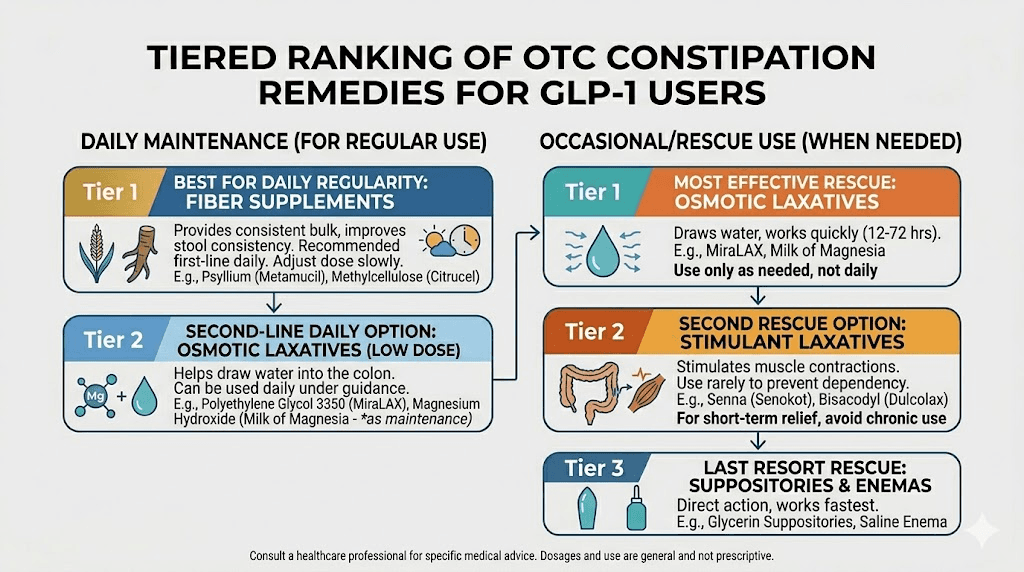
Tier 1: recommended for regular use
Polyethylene glycol (MiraLAX). This osmotic laxative draws water into the colon and is the most commonly recommended OTC option by gastroenterologists for GLP-1 constipation. Take 17 grams (one capful) dissolved in 8 ounces of liquid daily. It typically produces results within 1-3 days. It is non-habit-forming and safe for long-term use. This is the gold standard.
Magnesium oxide (400mg at bedtime). Covered in detail above. Gentle, effective, and provides the additional benefit of magnesium supplementation, which many GLP-1 users need anyway.
Docusate sodium (Colace). A stool softener, not a laxative. It works by allowing water and fats to penetrate stool, making it softer and easier to pass. Take 100mg once or twice daily. Most effective when combined with adequate hydration. Safe for long-term use.
Tier 2: use as needed, not daily
Magnesium citrate. More potent than magnesium oxide. Use for acute episodes only. Can cause electrolyte imbalances with daily use.
Senna (Senokot). A stimulant laxative that works by directly triggering contractions in the colon wall. Effective within 6-12 hours. Use no more than once or twice per week, as regular use can lead to dependency and actually worsen constipation over time.
Bisacodyl (Dulcolax). Another stimulant laxative with similar cautions. Available as tablets or suppositories. Suppositories work faster (15-60 minutes) but tablets are more convenient (6-12 hours).
Tier 3: avoid or use with extreme caution
Mineral oil. A lubricant laxative that can interfere with absorption of fat-soluble vitamins. Not recommended for regular use with GLP-1 medications.
Glycerin suppositories. Only helpful for stool in the rectum. Does not address the broader transit slowdown caused by GLP-1 medications. Can be used occasionally for acute relief when stool is impacted near the exit.
A multidisciplinary expert consensus published in Frontiers in Endocrinology recommends starting with osmotic laxatives (MiraLAX or magnesium) and only escalating to stimulant laxatives if osmotic options prove insufficient after 2-3 weeks of consistent use.
The pelvic floor connection most people miss
This might be the most underrated strategy for GLP-1 constipation relief. Your pelvic floor muscles play a direct role in the final stage of defecation. If those muscles are not coordinating properly, no amount of fiber, water, or magnesium will produce a satisfying bowel movement.
Pelvic floor dysfunction, specifically dyssynergic defecation, occurs when the muscles that should relax during a bowel movement instead tighten. This creates an outlet obstruction. The stool reaches the rectum but cannot exit efficiently. GLP-1 medications do not directly cause pelvic floor dysfunction, but the straining associated with hard, dry stool can trigger or worsen existing coordination problems.
Toilet positioning that actually helps
The modern toilet is poorly designed for defecation. Sitting at a 90-degree angle crimps the anorectal angle, making it harder for stool to pass. The solution is simple but remarkably effective.
Use a stool or platform under your feet to elevate your knees above your hips. This straightens the anorectal angle and allows for easier passage. Lean forward slightly. Place your elbows on your thighs. Relax your belly completely, do not suck it in. Breathe deeply and allow the movement to happen without excessive straining.
This position alone can reduce straining by up to 50% according to research published in the Journal of Clinical Gastroenterology. Products like the Squatty Potty serve this purpose, but any stable platform 6-8 inches high works just as well.
Timing your bathroom attempts
Your colon has natural motility peaks. The strongest occur after waking and within 2 hours after meals. Attempting defecation during these windows, rather than at random times throughout the day, significantly increases the likelihood of success.
A practical routine. Wake up. Drink 8-12 ounces of warm water. Wait 20-30 minutes while performing abdominal massage. Then sit on the toilet with proper positioning for 5-10 minutes. Do not strain. If nothing happens, walk away and try again after breakfast. The key is consistency. Your body learns the routine and begins to anticipate it.
When to consider pelvic floor physical therapy
If you have tried all the strategies in this guide and still experience persistent difficulty with evacuation, pelvic floor physical therapy may be the missing piece. A pelvic floor PT can assess your muscle coordination and teach you biofeedback techniques that retrain the muscles to relax appropriately during bowel movements.
This is especially relevant for GLP-1 users who report feeling like the stool is right there but will not come out, or who experience excessive straining despite having soft stool. These symptoms suggest a coordination problem rather than a transit problem, and they require a different solution set entirely.
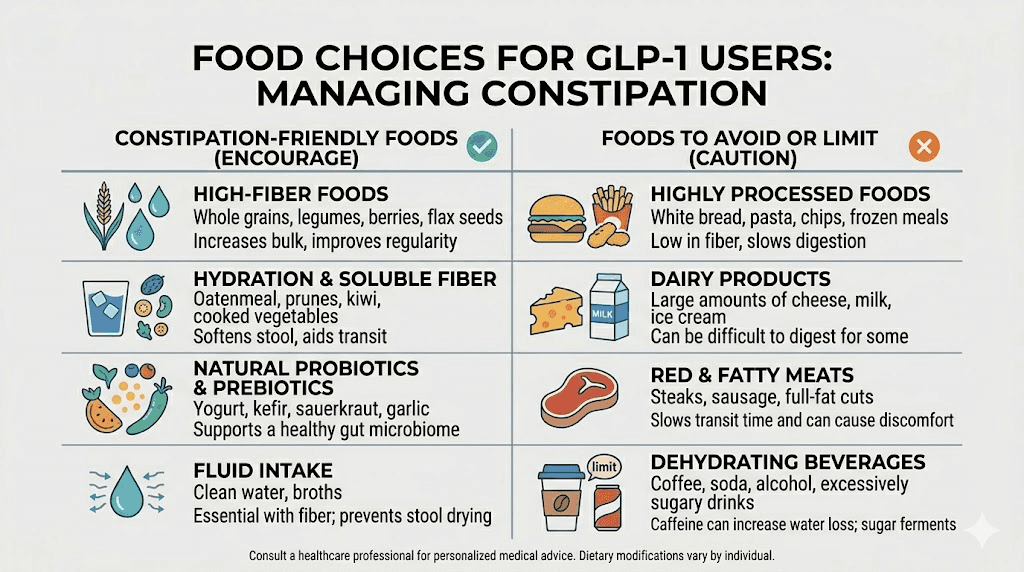
Diet adjustments for better digestion on GLP-1 medications
Beyond fiber, your overall dietary pattern influences how well your gut functions on GLP-1 medications. The goal is to choose foods that promote motility and avoid foods that slow things down further.
Foods that promote bowel regularity
Prunes remain the evidence champion for constipation. They contain sorbitol, a natural sugar alcohol that pulls water into the colon through osmotic action. Three to five prunes per day can increase stool frequency. They also contain fiber and polyphenols that stimulate motility.
Kiwifruit has emerged as a surprising star. A study in the American Journal of Gastroenterology found that two green kiwis per day significantly improved stool frequency and consistency in people with chronic constipation. The enzyme actinidin in kiwi aids protein digestion and may reduce the sensation of sulfur burps that some GLP-1 users experience.
Other helpful foods include cooked sweet potatoes, oatmeal, pears, apples with skin, broccoli, and Brussels sprouts. These provide both soluble and insoluble fiber plus water content that aids stool formation. For complete meal planning guidance, see our semaglutide diet plan and tirzepatide diet plan guides.
Foods that make GLP-1 constipation worse
Some foods actively slow transit or harden stool. These are especially problematic when GLP-1 medications have already reduced your gut motility.
Cheese and dairy. High in casein protein, which can slow transit. If you eat dairy, pair it with high-fiber foods.
Red meat. Takes longer to digest and contains zero fiber. It is not off-limits, but portions should be small and always accompanied by vegetables.
Processed and refined foods. White bread, white rice, crackers, and chips are low in fiber and can act like paste in a slow-moving gut.
Bananas (unripe). Ripe bananas are fine and contain helpful pectin. Green, unripe bananas contain resistant starch that can worsen constipation.
For comprehensive lists of what to eat and avoid, check out our guides on foods to avoid on semaglutide and foods to avoid on tirzepatide.
Healthy fats for lubrication
Dietary fat has a mild lubricating effect on the intestinal lining. It also stimulates bile release, which has a natural laxative effect. Olive oil, avocado, nuts, seeds, and fatty fish are excellent choices. A tablespoon of olive oil on an empty stomach in the morning is a traditional remedy that many GLP-1 users find helpful.
Prioritizing protein intake remains important on GLP-1 medications to prevent muscle loss, but balance your protein sources with adequate fiber and fat to maintain digestive function. For meal ideas that combine all these elements, see our GLP-1 breakfast ideas and dinner recipes.
When to consider adjusting your GLP-1 dose
Sometimes constipation is severe enough that it affects quality of life despite implementing all the strategies above. In those cases, a dose adjustment conversation with your healthcare provider is warranted.
Constipation tends to be dose-dependent with GLP-1 medications. Higher doses slow gastric emptying more aggressively, which means more constipation. If you recently titrated up to a higher dose and your constipation dramatically worsened, that dose increase is likely the primary driver.
Options your provider may consider include extending the time between dose increases to give your gut more time to adapt, temporarily reducing the dose until constipation management strategies take effect, or switching between GLP-1 medications if one produces intolerable side effects. The side effect profiles of semaglutide versus tirzepatide differ enough that switching can help some people. Some users also explore microdosing approaches that maintain benefits while reducing side effects.
Do not adjust your dose on your own. Do not skip doses to get relief. These medications work best with consistent dosing, and irregular use can worsen rebound symptoms when you resume.
For those on compounded formulations, dosing flexibility may be greater. Talk to your provider about whether a slightly lower concentration or split dosing protocol might maintain your weight loss trajectory while easing digestive side effects.
Week-by-week timeline of GLP-1 constipation
Knowing what to expect takes some of the anxiety out of the experience. Here is a general timeline based on clinical data and user reports.
Week 1-2: the onset
Most people notice changes in bowel habits within the first 1-2 weeks of starting a GLP-1 medication. Stools become firmer. Frequency drops. Some people experience no change initially, especially at starting doses. If you are on a starting dose of tirzepatide or the lowest semaglutide dose, you may not notice constipation until the first dose increase.
Week 3-6: peak severity
This is typically when constipation is at its worst. Your body is adjusting to the medication, and if you have recently increased your dose, the effect compounds. This is the window where proactive management matters most. Implement all strategies, hydration, fiber, magnesium, movement, before constipation becomes severe.
Week 6-10: gradual adaptation
For many people, the gut begins to adapt. Bowel function partially normalizes as the body adjusts to the slower transit time. Clinical data on semaglutide shows constipation symptoms plateauing around week 10 for most patients.
Week 10 and beyond: the new normal
Some level of slower transit may persist for the duration of treatment. But with the strategies in this guide consistently applied, most people achieve a comfortable and regular bowel pattern. If constipation persists beyond 12 weeks despite implementing all strategies, consider the pelvic floor evaluation discussed above and consult your healthcare provider about potential dose adjustments.
This timeline is a general pattern. Individual experience varies based on the specific medication (semaglutide versus tirzepatide versus retatrutide), your dose, your baseline gut health, your diet, and how consistently you apply the relief strategies.
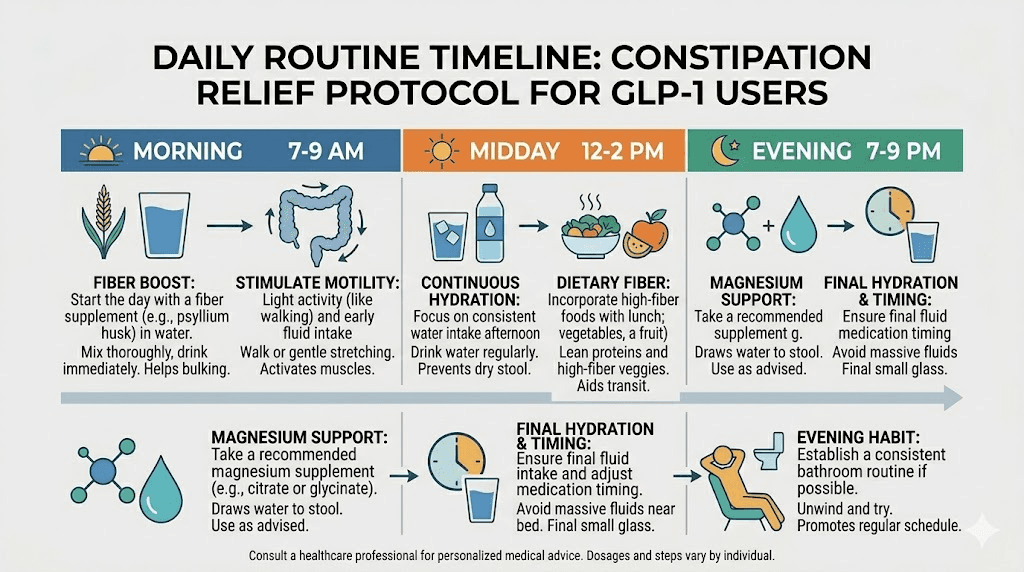
Complete daily protocol for GLP-1 constipation relief
Here is everything pulled together into a practical daily routine. This protocol addresses all the mechanisms driving GLP-1 constipation simultaneously.
Morning routine (within 30 minutes of waking)
1. Drink 8-12 ounces of warm water immediately upon waking.
2. Perform 5 minutes of abdominal massage in a clockwise direction.
3. Sit on the toilet with feet elevated on a stool for 5-10 minutes. Do not strain. Breathe deeply.
4. Eat breakfast including at least one high-fiber component. Chia seed pudding, oatmeal with ground flaxseed, or berries are excellent choices.
5. Walk for 15 minutes after breakfast.
Midday routine
6. Continue sipping water throughout the morning, targeting 30-40 ounces by noon.
7. Take one serving of psyllium husk fiber supplement with a full glass of water between meals (not within 1 hour of eating).
8. Eat lunch with vegetables and a healthy fat source like olive oil or avocado.
9. Walk for 15 minutes after lunch.
Afternoon routine
10. Continue hydrating, targeting 60-70 ounces by mid-afternoon.
11. Have a fiber-rich snack if hungry. An apple, a handful of almonds, or raw vegetables with hummus.
12. If needed, attempt a second bathroom visit during the afternoon motility window (2 hours after lunch).
Evening routine
13. Eat dinner including vegetables and a serving of fermented food (sauerkraut, kimchi, kefir).
14. Walk for 15 minutes after dinner.
15. Take 400mg magnesium oxide with water before bed.
16. Do 5-10 minutes of deep diaphragmatic breathing or gentle stretching.
Weekly additions
17. Accumulate at least 150 minutes of moderate exercise across the week beyond post-meal walks.
18. Eat 3-5 prunes on days when bowel function seems sluggish.
19. Take a probiotic supplement daily with a strain profile targeting motility (Bifidobacterium lactis BB-12, Lactobacillus rhamnosus GG).
20. Track your bowel movements. Frequency, consistency, and ease of passage. Adjust the protocol based on what works.
This protocol works because it attacks GLP-1 constipation from every angle simultaneously. Hydration counteracts increased water absorption. Fiber restores bulk and mechanical stimulation. Magnesium provides osmotic relief. Movement stimulates the gastrocolic reflex. Probiotics support the microbiome. And proper positioning optimizes the mechanics of defecation.
SeekPeptides members access detailed protocol tracking tools and personalized guidance for managing GLP-1 side effects. The platform provides comprehensive resources for optimizing your experience with these medications, from week-by-week result tracking to meal planning templates designed specifically for GLP-1 users.
When constipation signals something more serious
Most GLP-1 constipation is manageable. But in rare cases, constipation can signal a more serious problem that requires medical attention.
Red flags that require immediate medical evaluation
Seek medical help immediately if you experience any of the following while on a GLP-1 medication.
No bowel movement for 7+ days. Extended absence of bowel movements can lead to fecal impaction, a condition where hardened stool becomes lodged in the rectum or colon and cannot be passed without medical intervention.
Severe abdominal pain. Not mild discomfort or cramping, but sharp, severe, or worsening pain. This could indicate a bowel obstruction, a rare but documented adverse event with GLP-1 receptor agonists. A case report in the Canadian Medical Association Journal documented small bowel obstruction associated with GLP-1 RA use in a patient without prior surgical history.
Blood in your stool. Bright red blood on toilet paper may indicate hemorrhoids from straining, which is unpleasant but not dangerous. Dark, tarry, or maroon-colored blood is more concerning and should be evaluated promptly.
Vomiting along with constipation. This combination can indicate an obstruction. If you cannot keep fluids down and have not had a bowel movement in several days, seek emergency care.
Unintended weight loss beyond your GLP-1 goals. If you are losing weight faster than expected and experiencing severe constipation, the combination may indicate something beyond normal medication effects. This is worth discussing with your provider to rule out other causes.
Gastroparesis versus normal GLP-1 effects
There is growing awareness of the distinction between the expected gastroparesis-like effects of GLP-1 medications and actual pathological gastroparesis. GLP-1 medications intentionally slow gastric emptying. But in rare cases, this slowdown becomes so severe that the stomach essentially stops emptying altogether.
Signs that your gastric emptying delay has crossed into problematic territory include persistent nausea that prevents adequate food or fluid intake, visible abdominal distension, feeling full after just a few bites despite hours since your last meal, and severe acid reflux or excessive burping.
If you recognize these symptoms alongside your constipation, contact your healthcare provider. Dose reduction or temporary discontinuation may be necessary.
GLP-1 constipation relief across different medications
While the core strategies apply to all GLP-1 medications, there are nuances worth noting for specific drugs.
Semaglutide (Ozempic, Wegovy)
Semaglutide constipation rates run around 24-29% in clinical trials. The medication has a 7-day half-life, meaning its effects are continuous and cumulative. Constipation tends to worsen with dose titration and stabilize after several weeks at a maintenance dose. For targeted strategies, see our complete semaglutide constipation treatment guide. Understanding how semaglutide makes you feel overall can help you contextualize the constipation within the broader side effect picture.
Tirzepatide (Mounjaro, Zepbound)
Tirzepatide is a dual GIP/GLP-1 agonist, meaning it acts on two receptors instead of one. Constipation rates are 12-27% depending on dose. Some users report that tirzepatide produces less constipation than semaglutide at equivalent efficacy levels, though head-to-head data is limited. Our tirzepatide constipation treatment guide covers medication-specific strategies. If you have switched between medications, see our switching guide for managing side effects during transitions.
Retatrutide
As a triple agonist (GIP/GLP-1/glucagon), retatrutide affects gut motility through multiple receptor pathways. Early clinical data suggests GI side effects are common but manageable. The glucagon component may partially offset constipation through its own gastrointestinal effects, but published data is still limited. Some users report diarrhea rather than constipation with retatrutide, suggesting a different GI side effect profile.
Oral GLP-1 formulations
Oral semaglutide (Rybelsus) and emerging oral tirzepatide formulations may produce slightly different constipation patterns because the drug passes through the GI tract before absorption. Oral drops and sublingual formulations interact directly with the upper GI lining, which can cause more upper GI symptoms (nausea) but sometimes less lower GI disruption (constipation). Results vary significantly between individuals.
Natural remedies and supplements beyond the basics
Beyond fiber, magnesium, and probiotics, several other natural approaches have evidence supporting their use for GLP-1 constipation.
Ginger
Ginger has prokinetic properties, meaning it helps stimulate gastric emptying and intestinal motility. Research shows it works through serotonin receptor pathways in the gut. Fresh ginger tea (steep 1-2 inches of sliced fresh ginger in hot water for 10 minutes), ginger capsules (250mg four times daily), or even crystallized ginger between meals can help. This is particularly useful for GLP-1 users because it addresses both the nausea and constipation that often co-occur.
5-HTP
5-Hydroxytryptophan is a precursor to serotonin, and approximately 95% of the body serotonin is produced in the gut where it plays a critical role in regulating motility. Supplementing with 50-100mg of 5-HTP at bedtime may improve transit time. Published research supports healthier transit times with 5-HTP supplementation. However, do not take 5-HTP if you are on SSRI or SNRI medications, as this can cause serotonin syndrome.
Vitamin C in high doses
Vitamin C has osmotic laxative properties at high doses (1,000-2,000mg). Exceeding your body tolerance level for vitamin C causes loose stools. While this is not ideal as a primary strategy, it can serve as an occasional relief tool. Take it in divided doses throughout the day rather than all at once.
Aloe vera juice
Aloe vera contains anthraquinones, which are natural stimulant laxatives. One to two ounces of inner-leaf aloe vera juice daily may improve bowel regularity. Choose products labeled inner-leaf or purified to avoid latex components that can be too harsh. Start with a small amount to assess tolerance.
For a comprehensive overview of all supplements that pair well with GLP-1 medications, including those that help with other side effects like hair loss, headaches, and fatigue, see our comprehensive supplements guide.
Compound formulations with built-in GI support
Many compounded GLP-1 formulations now include ingredients specifically chosen to offset GI side effects. Semaglutide with glycine may help reduce nausea and GI discomfort. Tirzepatide with glycine and B12 combines metabolic support with GI-friendly amino acids. Semaglutide with niacinamide and tirzepatide with niacinamide formulations also aim to reduce side effects while maintaining efficacy. These combination products can be part of a comprehensive approach to managing constipation alongside other GLP-1 side effects.
Tracking your progress and adjusting your approach
Managing GLP-1 constipation is not a one-size-fits-all proposition. What works for one person may not work for another. The key is systematic tracking and adjustment.
What to track
Keep a simple daily log that records bowel movement frequency (how many per day), stool consistency (use the Bristol Stool Scale, aiming for Type 3 or 4), ease of passage (straining versus comfortable), abdominal symptoms (bloating, cramping, gas), water intake (in ounces), fiber intake (approximate grams), exercise (type and duration), and any supplements or laxatives used.
This data reveals patterns. Maybe you notice that bowel movements consistently happen on days when you walk after all three meals but not on days when you skip the post-dinner walk. Or perhaps magnesium works well for two weeks and then seems to lose effectiveness, suggesting you need to adjust the dose or try a different form.
When to escalate
If you have consistently implemented this entire protocol for 3-4 weeks and still experience fewer than 3 bowel movements per week with significant discomfort, it is time to involve your healthcare provider. They may recommend prescription options like lubiprostone (Amitiza), linaclotide (Linzess), or prucalopride (Motegrity), which work through mechanisms different from over-the-counter options and can be combined with the lifestyle strategies outlined here.
SeekPeptides provides tracking tools and protocol databases that help members systematically optimize their GLP-1 experience. The platform comprehensive side effect management guides cover not just constipation but the full spectrum of GLP-1 side effects, from dizziness to insomnia to menstrual changes.
Frequently asked questions
How long does GLP-1 constipation last?
Clinical data shows GLP-1 constipation typically peaks around weeks 3-6 and begins to stabilize by week 10. For semaglutide specifically, studies found the average duration was about 47 days. However, some people experience persistent constipation throughout their treatment. Proactive management with hydration, fiber, and magnesium can significantly shorten and reduce the severity of this period. See our GLP-1 timeline guide for more details on what to expect.
Is MiraLAX safe to take every day with a GLP-1 medication?
Yes. Polyethylene glycol (MiraLAX) is considered safe for long-term daily use. It does not cause dependence, does not interact with GLP-1 receptor agonists, and works through an osmotic mechanism rather than stimulating the colon directly. It is the most commonly recommended OTC option by gastroenterologists for GLP-1 constipation.
Can I take magnesium and a fiber supplement at the same time?
Yes, but spacing them out is preferable. Take your fiber supplement during the day with meals or between meals, and take magnesium oxide at bedtime. This provides continuous support throughout the day and overnight relief from the magnesium. Taking them at the same time is not harmful, but the timing strategy provides more consistent bowel regulation.
Does semaglutide or tirzepatide cause more constipation?
Clinical trial data suggests roughly similar rates, though individual experiences vary widely. Semaglutide trials reported 24-29% constipation rates while tirzepatide trials showed 12-27%. The difference may partly reflect dose equivalency issues in trials rather than a true pharmacological difference. If constipation is intolerable on one medication, switching to the other may help, but it is not guaranteed. See our side effect comparison for a detailed breakdown.
Will the constipation go away if I stop taking the GLP-1 medication?
In most cases, yes. Since GLP-1 constipation is caused directly by the medication slowing gastric and intestinal motility, bowel function typically returns to baseline within 1-2 weeks of discontinuation. However, stopping the medication also means losing the appetite suppression and weight loss benefits. Talk to your provider about managing side effects rather than discontinuing treatment. Our guide on semaglutide withdrawal symptoms covers what to expect if you do stop.
Should I take a probiotic while on a GLP-1 medication?
Probiotic supplementation is generally beneficial for GLP-1 users experiencing constipation, particularly strains like Bifidobacterium lactis BB-12 and Lactobacillus rhamnosus GG that have demonstrated improvements in transit time and stool consistency. See our best probiotic for semaglutide guide for specific strain recommendations and dosing.
Can I drink coffee for constipation relief while on a GLP-1?
Coffee has mild prokinetic effects and can stimulate colonic contractions. One to two cups in the morning can be part of your constipation management strategy. However, coffee should not be your primary hydration source, and excessive consumption can worsen acid reflux and anxiety that some GLP-1 users experience. Drink it alongside, not instead of, water.
Is exercise really necessary, or can I manage constipation with supplements alone?
While supplements and OTC remedies can help significantly, exercise provides a unique mechanical stimulus to the gut that supplements cannot replicate. The post-meal walk in particular triggers the gastrocolic reflex through a pathway that no supplement activates. For optimal results, combine both approaches. Even a 15-minute daily walk makes a measurable difference in overall GLP-1 outcomes beyond just constipation relief.
External resources
Tirzepatide-induced gastrointestinal manifestations: a systematic review and meta-analysis (PMC)
Effects of GLP-1 receptor agonist on changes in the gut bacterium (Scientific Reports)
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your gut stay comfortable, your transit stay regular, and your relief stay lasting.