Feb 20, 2026

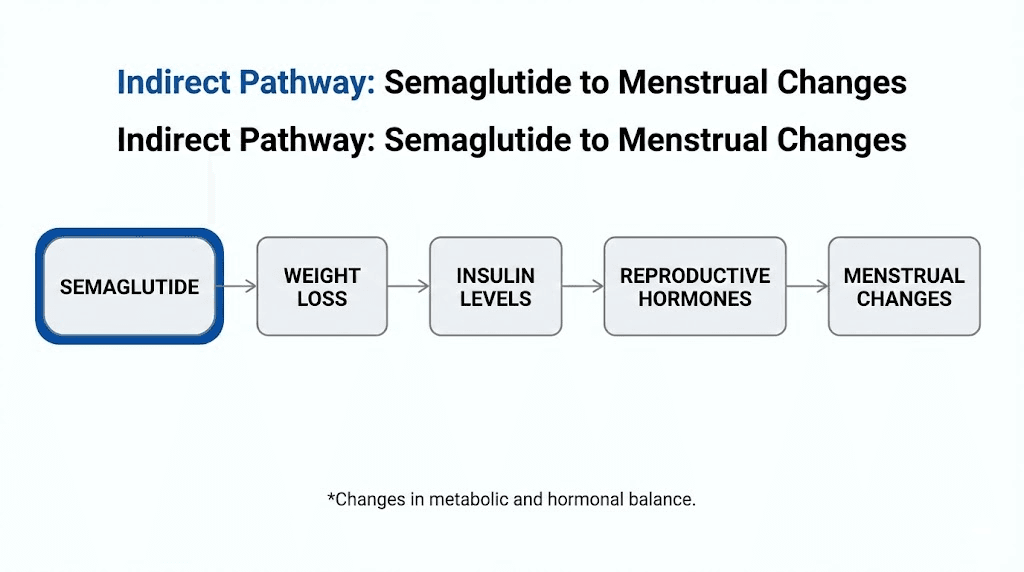
What if the medication helping you lose weight is also quietly reshaping your menstrual cycle? Not directly. Not through some hidden hormonal pathway. But through a cascade of metabolic changes that ripple outward from fat cells to the hypothalamus to the ovaries, touching nearly every system that governs when, how, and whether your period arrives each month.
That question keeps coming up. Women start semaglutide for weight loss or blood sugar management, and within weeks, something shifts. A period arrives early. Or late. Or heavier than usual. Or it disappears entirely for a month. The experience varies so widely that online forums are filled with contradictory stories, some women reporting the most regular cycles of their lives while others wonder if something has gone seriously wrong.
Here is what the research actually shows. Semaglutide does not directly affect reproductive hormones. No clinical trial has found that it alters estrogen, progesterone, or luteinizing hormone levels on its own. But the metabolic changes it triggers, particularly rapid weight loss, improved insulin sensitivity, and shifts in fat-stored hormones, absolutely can and do change menstrual patterns. Understanding the difference between a direct drug effect and an indirect metabolic consequence matters enormously for making informed decisions about your health.
This guide covers every mechanism, every study, every practical scenario. From the hormonal cascade that connects your fat cells to your ovaries, to the specific side effects women report at each dose, to the surprising connection between GLP-1 medications and unexpected pregnancies. Whether you are managing PCOS, concerned about birth control interactions, or simply trying to understand why your cycle changed after starting treatment, the answers are here.
The short answer with critical nuance
Semaglutide does not directly alter your menstrual cycle. The FDA prescribing information does not list menstrual irregularities as a side effect. Clinical trials for both Ozempic and Wegovy focused on blood sugar, weight loss, and cardiovascular outcomes rather than reproductive health, so the data on menstrual effects remains limited.
But that does not mean your period will stay the same.
The indirect effects are real and well-documented. When you lose 5-10% of your body weight, hormonal shifts follow. Estrogen levels change because adipose tissue stores and produces estrogen. Insulin sensitivity improves, which alters androgen production. Leptin levels drop as fat mass decreases, which can affect the hypothalamic-pituitary-ovarian axis that controls your entire reproductive cycle.
These are not theoretical concerns. A study of 27 obese women with PCOS taking semaglutide 0.5mg weekly found that almost 80% of treatment-responsive patients experienced menstrual cycle normalization. Another recent study combining semaglutide with metformin showed a 72.5% rate of menstrual cycle recovery at 16 weeks, compared to 42.3% with metformin alone. The medication does not touch your hormones directly, but the metabolic changes it creates touch everything.
So the real answer is this: semaglutide probably will affect your period. Not because of what the drug does to your reproductive system, but because of what weight loss and improved metabolic health do to the hormonal environment your cycle depends on.
How semaglutide changes your hormones without touching them directly
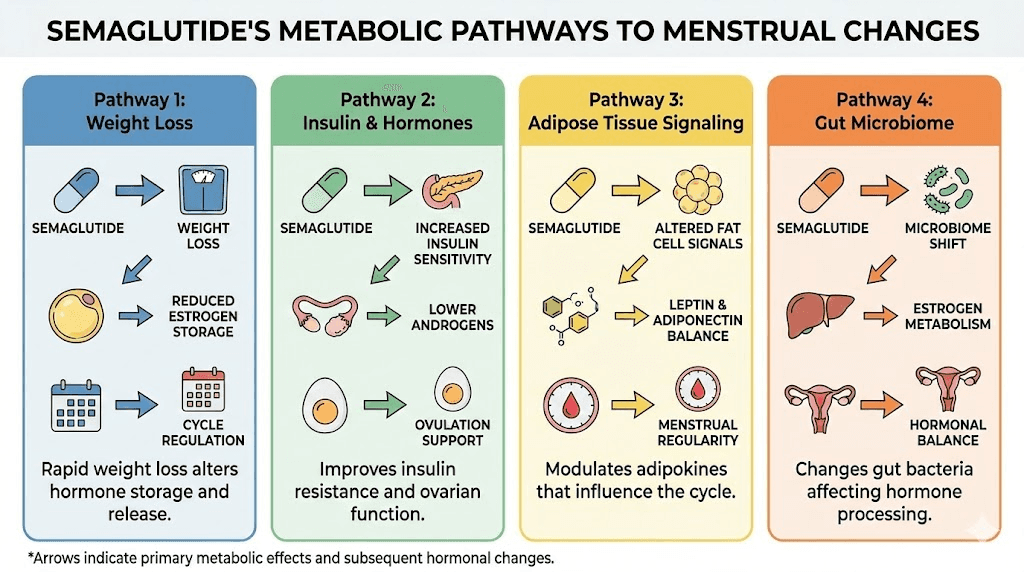
Understanding why your period changes on semaglutide requires understanding four separate mechanisms. None of them involve the drug binding to reproductive hormone receptors. All of them involve downstream metabolic effects that eventually reach the reproductive system.
The weight loss and estrogen connection
Fat tissue is not passive storage. It is an active endocrine organ that produces and stores estrogen through a process called aromatization, where androgens convert to estrogen inside adipocytes. The more fat tissue you carry, the more estrogen your body produces outside the ovaries.
When semaglutide triggers significant weight loss, often 10-15% of body weight within the first year, that estrogen production drops. For some women, this means estrogen levels normalize after being chronically elevated. For others, especially those who lose weight rapidly, estrogen can temporarily drop below optimal levels.
The result depends on where you started. Women with obesity-related elevated estrogen often see their cycles become more regular. Women who lose weight very quickly may experience missed periods or lighter flow as their bodies adjust to a new hormonal baseline.
Research shows that losing more than 10-15% of stable adult body weight can trigger what researchers call weight loss-related amenorrhea, the temporary cessation of periods. A landmark study found that 70% of women who lost more than one-seventh of their stable adult weight developed menstrual gaps exceeding 90 days. This is not a semaglutide-specific finding. It happens with any rapid weight loss method. But because semaglutide is remarkably effective at producing significant weight loss, the effect shows up frequently in women using it.
Insulin resistance and androgen reduction
This mechanism matters most for women with PCOS, but it affects anyone with insulin resistance.
High insulin levels directly stimulate the ovaries to produce excess androgens, including testosterone. This is one of the core mechanisms driving PCOS symptoms: irregular cycles, anovulation, acne, and excess hair growth. The ovaries essentially respond to high insulin by overproducing male hormones.
Semaglutide improves insulin sensitivity through multiple pathways. It enhances pancreatic beta-cell function, reduces hepatic glucose output, and suppresses appetite leading to caloric reduction. As insulin levels normalize, the ovaries receive less stimulation to produce androgens.
Studies show that GLP-1 receptor agonists reduce total testosterone and dehydroepiandrosterone sulfate (DHEAS) in women with PCOS while simultaneously increasing sex hormone binding globulin (SHBG). The testosterone drop ranges from 20-30% in published research. Lower androgens mean less interference with ovulation, which translates directly to more regular periods.
For women managing early semaglutide treatment, this androgen reduction often produces noticeable cycle changes within the first 8-12 weeks, sometimes before significant weight loss occurs. The insulin pathway acts faster than the weight loss pathway.
Leptin, GnRH, and the hypothalamic connection
Leptin is a hormone produced by fat cells that tells your brain how much energy you have stored. Your hypothalamus uses leptin levels to decide whether conditions are safe enough for reproduction. High leptin from excess fat? The hypothalamus gets a confused signal. Low leptin from rapid fat loss? The hypothalamus may decide reproduction is too risky.
Here is how the cascade works. Leptin levels drop as fat mass decreases during semaglutide treatment. The hypothalamus detects this drop. If it falls below a critical threshold, the hypothalamus reduces its pulsatile release of gonadotropin-releasing hormone (GnRH). Less GnRH means less follicle-stimulating hormone (FSH) and less luteinizing hormone (LH) from the pituitary. Less FSH and LH means impaired follicle development, delayed or absent ovulation, and reduced estrogen production from the ovaries.
This is the same mechanism behind hypothalamic amenorrhea in athletes and people with eating disorders. The body essentially shuts down reproduction when it perceives an energy deficit. The good news: over 80% of women regain ovulatory cycles within nine months of reaching a stable weight, even after years of amenorrhea.
For women on semaglutide, this means the speed of weight loss matters as much as the total amount. Losing weight gradually gives the hypothalamus time to adjust. Plateaus, while frustrating for weight loss goals, actually give your reproductive system a chance to recalibrate.
Gastric emptying and medication absorption
Semaglutide slows gastric emptying, the rate at which food moves from your stomach to your small intestine. This is one of the mechanisms behind its appetite-suppressing effects. But slower gastric emptying also affects how other medications are absorbed.
This matters specifically for oral contraceptives. When the stomach empties more slowly, the timing and absorption profile of medications taken by mouth can shift. A 2015 pharmacokinetic study published in the Journal of Clinical Pharmacology specifically tested this concern. The result: semaglutide did not reduce the bioavailability of ethinylestradiol or levonorgestrel, the two most common components of combination birth control pills. The overall exposure to both hormones remained the same, even though peak levels arrived slightly later.
This is an important distinction from tirzepatide, which showed approximately a 20% decrease in overall oral contraceptive exposure in similar studies. If you are using semaglutide rather than tirzepatide, the birth control interaction risk appears lower based on available evidence. But if you are switching between medications, this difference matters for contraceptive planning.
What menstrual changes to expect on semaglutide
The specific changes women experience depend on their starting weight, rate of weight loss, hormonal baseline, and whether they have conditions like PCOS. But patterns emerge across thousands of user reports and the limited clinical data available.
Lighter periods or missed periods
This is the most commonly reported change. As body fat decreases and estrogen production from adipose tissue drops, the uterine lining often becomes thinner. A thinner lining means lighter menstrual flow. In cases of rapid weight loss, periods may disappear entirely for one to three cycles.
Missed periods on semaglutide most frequently occur during phases of rapid weight loss, typically in the first 3-6 months when the dose is escalating and caloric intake has dropped significantly. Women who experience significant fatigue alongside missed periods may be experiencing a more pronounced energy deficit that their body is responding to by temporarily pausing ovulation.
This pattern tends to resolve. As weight stabilizes and the body adjusts to its new metabolic baseline, most women see their periods return within one to three months. If periods remain absent for longer than three months, a medical evaluation is warranted.
Heavier or longer periods
Less commonly reported but equally important. Some women experience heavier flow in the first few months of treatment, particularly those with previously irregular or light periods who had underlying anovulation.
The mechanism here is different. When ovulation resumes after a period of anovulation (common in women with insulin resistance or PCOS), the uterine lining that has been building without being shed can produce a heavier-than-normal period. This is actually a sign that the reproductive system is reactivating properly, though it can be alarming if unexpected.
Women who experience heavier periods after starting semaglutide should consider whether they previously had irregular or absent cycles. If so, the heavier flow may actually represent a normalization process. Proper nutrition including iron-rich foods becomes especially important during this phase.
Irregular cycle timing
Cycles that were predictably 28-30 days may shift to 25 days one month and 35 the next. This irregularity typically reflects the body recalibrating its hormonal rhythms in response to changing body composition.
The dose escalation schedule of semaglutide plays a role here. Most protocols start at 0.25mg weekly and increase every four weeks. Each dose increase can produce a new wave of metabolic adaptation, and the reproductive system often reflects this with temporary irregularity. Women who experience gastrointestinal side effects at each dose increase may also notice more cycle disruption during those same periods, as the body is managing multiple adjustments simultaneously.
Irregular timing usually stabilizes within two to three cycles at a maintenance dose. Keeping a cycle tracking log helps distinguish between normal adjustment patterns and changes that warrant medical attention.
Changes in PMS symptoms
This gets less attention but matters to many women. The premenstrual symptoms you are accustomed to may shift. Some women report reduced cramping and bloating as inflammation decreases with weight loss. Others report new or different PMS symptoms during the adjustment period.
GLP-1 receptor agonists have demonstrated anti-inflammatory properties beyond their metabolic effects. Reduced systemic inflammation can translate to less painful periods, less severe bloating, and fewer mood fluctuations. This benefit often becomes more apparent after 3-6 months of treatment when weight loss and metabolic improvements have stabilized.
Changes in digestive symptoms can also overlap with and sometimes mimic PMS symptoms, making it harder to distinguish between medication side effects and menstrual changes in the early weeks of treatment.
Semaglutide and PCOS: where the research is strongest
If there is one area where the connection between semaglutide and menstrual health is genuinely encouraging, it is polycystic ovary syndrome. The data here moves beyond anecdotal reports into actual clinical trials with measurable outcomes.
What the studies show
A 2023 study evaluated low-dose semaglutide (0.5mg subcutaneously once weekly) in 27 obese women with PCOS who had not responded to lifestyle interventions. Over six months, the mean body weight loss was 11.5 kg, with BMI dropping from 34.4 to 29.4. In treatment-responsive patients, menstrual cycle normalization occurred in almost 80% of cases.
That 80% figure is remarkable. These were women whose cycles had remained irregular despite previous attempts at diet and exercise. Semaglutide, even at a dose lower than what many weight management protocols use, restored regular periods in four out of five women who responded to treatment.
A more recent study examined semaglutide combined with metformin versus metformin alone. At 16 weeks, the combination therapy group achieved a 72.5% rate of menstrual cycle recovery compared to 42.3% with metformin alone. The semaglutide group also showed greater improvements in insulin resistance markers, androgen levels, and inflammatory markers.
For women with PCOS who have been struggling with weight loss and irregular periods simultaneously, these results suggest that semaglutide may address both problems through the same metabolic pathways. The weight loss improves insulin sensitivity. Better insulin sensitivity reduces androgen production. Lower androgens allow normal ovulation. Normal ovulation produces regular periods.
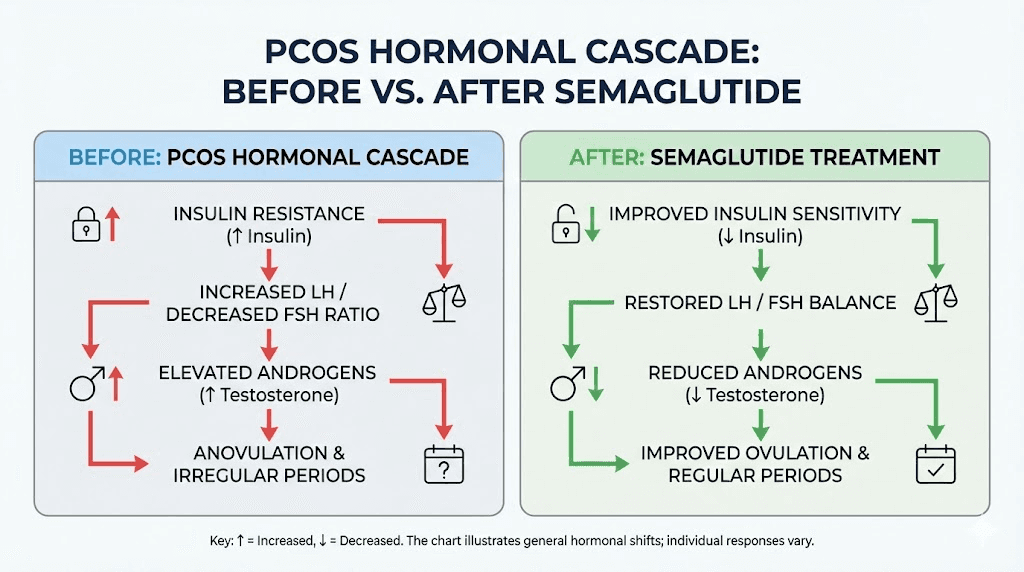
Why PCOS responds differently
Women with PCOS experience the opposite pattern from many other women on semaglutide. Instead of losing periods due to rapid weight loss, they often gain regular periods for the first time in years.
The reason comes down to the starting hormonal environment. PCOS creates a state of chronic elevated insulin, which drives elevated androgens, which disrupts ovulation. Semaglutide breaks this cycle at the insulin level. As semaglutide treatment improves insulin sensitivity, the entire downstream cascade shifts toward normal.
Preclinical research also suggests that GLP-1 receptor agonists may exert effects directly on the hypothalamic-pituitary-gonadal axis. Studies in animal models show that GLP-1 and its analogs can act on the gonadal axis through the hypothalamic kiss-1 system, influencing reproductive efficiency. Whether this direct pathway contributes meaningfully in humans remains under investigation.
For women with PCOS, the practical implication is important: improved menstrual regularity on semaglutide often means improved fertility. This is welcome news for those trying to conceive, but it also means that women with PCOS who are not trying to conceive need to be extra vigilant about contraception, something that brings us to one of the most discussed topics in GLP-1 therapy.
Timeline of menstrual changes by treatment phase
Knowing what to expect at each stage helps distinguish normal adjustment from something that needs medical attention. These timelines are based on commonly reported patterns and the standard semaglutide dosing schedule.
Weeks 1-4: the 0.25mg initiation phase
Most women notice no menstrual changes during the first month. The 0.25mg dose is a titration dose designed to help your body adjust to the medication with minimal side effects. Weight loss at this stage is typically modest, often 1-3 pounds.
Some women do report subtle changes: a period arriving a day or two early, slightly different flow volume, or mild differences in PMS symptoms. These are generally attributable to the body adjusting to the new medication rather than significant hormonal shifts.
The biggest variable during this phase is dietary change. Many women dramatically alter their eating patterns when they start semaglutide, either because of reduced appetite or because they are intentionally improving their diet. Sudden caloric restriction alone can affect your cycle independent of the medication.
Weeks 5-12: dose escalation and early weight loss
This is when most menstrual changes begin. The dose typically increases to 0.5mg at week 5 and may reach 1mg by week 9. Weight loss accelerates, and the metabolic shifts described earlier start producing noticeable effects.
Common changes during this phase include a shorter or longer cycle by 2-5 days compared to your baseline, lighter flow than usual, increased or decreased PMS symptoms, and occasional spotting mid-cycle. Women who experience significant gastrointestinal side effects during dose increases may notice more pronounced cycle changes during the same periods.
If you have PCOS, this is often when you first notice cycles becoming more regular. The insulin sensitivity improvements from semaglutide can begin shifting androgen levels within 4-8 weeks, sometimes before major weight loss occurs.
Months 3-6: peak weight loss phase
Weight loss is typically most rapid during months 3-6. This is also when menstrual changes are most pronounced. Women losing 1-2 pounds per week, which is common during this phase, are experiencing the metabolic shifts most likely to affect their cycles.
Some women experience their first missed period during this phase. If you are losing weight rapidly and miss one period, it is likely the body responding to a perceived energy deficit. Two consecutive missed periods warrant a conversation with your doctor, both to rule out pregnancy (which is a real possibility, discussed below) and to assess whether the rate of weight loss should be adjusted.
Women who are planning long-term treatment should expect this phase to be the most variable for their cycles. Tracking your period dates, flow volume, and symptoms during this time provides valuable data for your healthcare provider.
Months 6-12 and beyond: stabilization
As weight loss slows and the body reaches a new equilibrium, menstrual cycles typically stabilize. The hormonal environment adjusts to the new body composition, leptin levels find a new baseline, and the hypothalamic-pituitary-ovarian axis recalibrates.
Most women report that their cycles at 6-12 months are more regular and predictable than they were before starting semaglutide, even if they experienced irregularity during the active weight loss phase. This is consistent with research showing that moderate weight loss (5-10% of body weight) generally improves menstrual regularity across populations.
Women who reach the maintenance dose and achieve stable weight often report the most predictable cycles of their adult lives. The combination of healthier body composition, improved insulin sensitivity, and reduced systemic inflammation creates an optimal hormonal environment.
The Ozempic babies phenomenon: fertility, weight loss, and unplanned pregnancy
It has become one of the most discussed topics in GLP-1 therapy. Women who struggled with infertility for years suddenly becoming pregnant after starting semaglutide, sometimes completely unexpectedly. Media outlets have coined the term "Ozempic babies," and fertility specialists are paying close attention.
How weight loss restores fertility
The connection is not mysterious. Excess body weight is one of the most common reversible causes of reduced fertility. Fat tissue produces excess estrogen that disrupts the FSH/LH ratio needed for ovulation. Insulin resistance suppresses ovulation through elevated androgens. Chronic low-grade inflammation from excess adipose tissue creates a hostile environment for implantation.
When semaglutide produces significant weight loss, every one of these factors improves. Estrogen normalizes. Insulin sensitivity improves. Androgens drop. Inflammation decreases. For women who were anovulatory, ovulation can resume, sometimes within weeks of reaching a threshold of weight loss.
The clinical implications are clear. Unplanned pregnancies on GLP-1 medications are being reported with increasing frequency. This is not because the medications are fertility drugs. It is because the weight loss restores natural fertility in women whose excess weight was the primary barrier to conception.
Birth control considerations on semaglutide
This is where practical guidance matters most. If you are taking semaglutide and do not want to become pregnant, understanding the birth control landscape is critical.
Oral contraceptives and semaglutide: A pharmacokinetic study demonstrated that semaglutide does not reduce the bioavailability of combination oral contraceptives containing ethinylestradiol and levonorgestrel. Peak absorption is delayed slightly due to slower gastric emptying, but total exposure remains the same. Based on current evidence, semaglutide should not reduce oral contraceptive effectiveness.
However, if you are experiencing significant gastrointestinal side effects including vomiting or severe diarrhea, those symptoms themselves can reduce oral contraceptive absorption regardless of semaglutide. Vomiting within 2-3 hours of taking a pill means the hormones may not have been fully absorbed.
Important distinction from tirzepatide: Studies show that tirzepatide decreased overall oral contraceptive exposure by approximately 20%. Women switching between these medications should discuss contraceptive implications with their provider.
Non-oral contraceptive options: IUDs, implants, injections, and patches are not affected by gastric emptying changes. For women who want absolute certainty about contraceptive reliability while on GLP-1 therapy, non-oral methods eliminate the absorption question entirely. This is particularly relevant for women who are actively losing weight and may be restoring fertility they did not know had been compromised.
What the FDA says about pregnancy and semaglutide
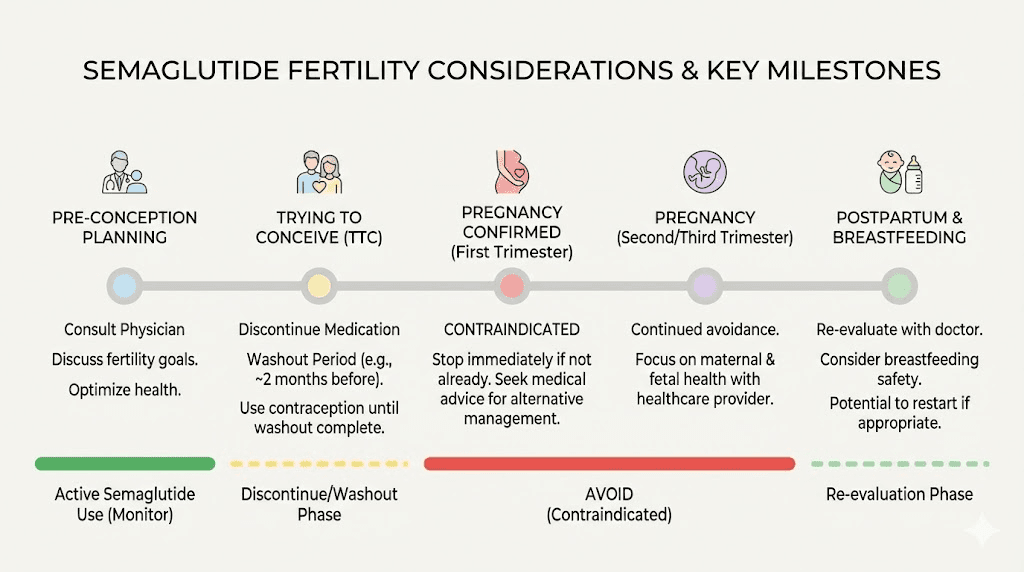
The FDA recommends discontinuing semaglutide at least two months before a planned pregnancy. Animal reproduction studies showed adverse effects on embryo-fetal development at exposures below the maximum recommended human dose. While there is no long-term human safety data on semaglutide exposure during pregnancy, the precautionary principle applies.
Women who discover they are pregnant while taking semaglutide should stop the medication immediately and contact their prescriber. The two-month washout recommendation exists because semaglutide has a long half-life, approximately one week, and it takes multiple half-lives for the drug to clear the system completely.
For women of reproductive age taking semaglutide, this creates a practical protocol. Use reliable contraception throughout treatment. If planning pregnancy, stop semaglutide at least two months before attempting to conceive. If an unplanned pregnancy occurs, stop immediately and seek medical guidance.
Semaglutide vs tirzepatide: how they compare for menstrual effects
Women often ask how semaglutide compares to tirzepatide when it comes to menstrual changes. The two medications work through related but distinct mechanisms, and the differences matter for both cycle effects and contraceptive planning.
Semaglutide is a pure GLP-1 receptor agonist. Tirzepatide is a dual GLP-1/GIP receptor agonist. The dual mechanism means tirzepatide typically produces faster and greater weight loss, which in turn means more pronounced and rapid hormonal shifts. Women on tirzepatide may experience more dramatic menstrual changes simply because the weight loss is more aggressive.
The contraceptive interaction is the most clinically significant difference. As noted earlier, semaglutide does not reduce oral contraceptive bioavailability, while tirzepatide shows a roughly 20% reduction. This makes semaglutide the more straightforward choice for women relying on oral birth control, though non-oral contraceptive methods sidestep this issue entirely for both medications.
Both medications share the same indirect mechanisms for menstrual changes: weight loss-related hormonal shifts, improved insulin sensitivity, and reduced inflammation. The side effect profiles overlap significantly, though tirzepatide users tend to report slightly different gastrointestinal patterns. Women experiencing sleep disruption or body aches on tirzepatide may find these compound their menstrual symptom changes in ways that differ from semaglutide.
For PCOS specifically, both medications show promise. The choice between them depends on many factors beyond menstrual effects, including cost, dosing convenience, and individual response. Discussing PCOS-specific considerations with a healthcare provider familiar with both medications will yield the best personalized guidance.
Age-specific considerations for menstrual changes
Your age and reproductive stage significantly influence how semaglutide affects your cycle. A 25-year-old with PCOS and a 48-year-old in perimenopause will have completely different experiences, even on the same dose.
Reproductive age (18-35)
Women in their peak reproductive years typically have the most resilient menstrual cycles. Temporary disruptions from semaglutide-related weight loss usually resolve within 2-3 cycles. However, this age group faces the highest risk of unplanned pregnancy if fertility is restored by weight loss, so contraceptive planning is essential.
Women in this age group with PCOS are the most likely to experience significant positive changes. The combination of improved insulin sensitivity and weight loss can restore regular ovulation for the first time in years. If you are in this group and your cycles suddenly become regular after starting semaglutide, treat this as a fertility restoration event and plan accordingly.
Young women concerned about hair loss on GLP-1 medications should know that the same hormonal shifts affecting the menstrual cycle can also affect hair growth patterns. Both are typically temporary and related to the rate of weight loss rather than the medication itself.
Late reproductive age (35-45)
Women in this age group may have declining ovarian reserve alongside metabolic concerns. Weight loss from semaglutide can temporarily improve egg quality markers by reducing oxidative stress and inflammation, but the underlying age-related decline in fertility continues regardless.
Menstrual changes in this age group can be harder to distinguish from early perimenopause. If cycles become irregular on semaglutide and you are over 40, hormone testing (FSH, estradiol, AMH) can help determine whether changes are medication-related or age-related. Your dosing protocol should account for these additional variables.
Perimenopause (typically 45-55)
Perimenopausal women already experience irregular cycles due to fluctuating hormone levels. Adding semaglutide-related metabolic changes to an already variable hormonal environment can create a confusing picture. Is that missed period from weight loss, perimenopause, or pregnancy?
The answer matters because perimenopausal women can still become pregnant. The assumption that fertility has ended simply because cycles are irregular is one of the most common reasons for surprise pregnancies in this age group. Weight loss from semaglutide can temporarily improve ovulatory function even in perimenopausal women.
For women in perimenopause, tracking symptoms becomes even more important. Distinguishing between hot flashes from perimenopause and the warming sensation some women report from GLP-1 medications, or between perimenopause-related mood changes and medication adjustment effects, requires careful documentation. Nutritional support designed for GLP-1 therapy should also account for the additional calcium and vitamin D needs of perimenopausal women.
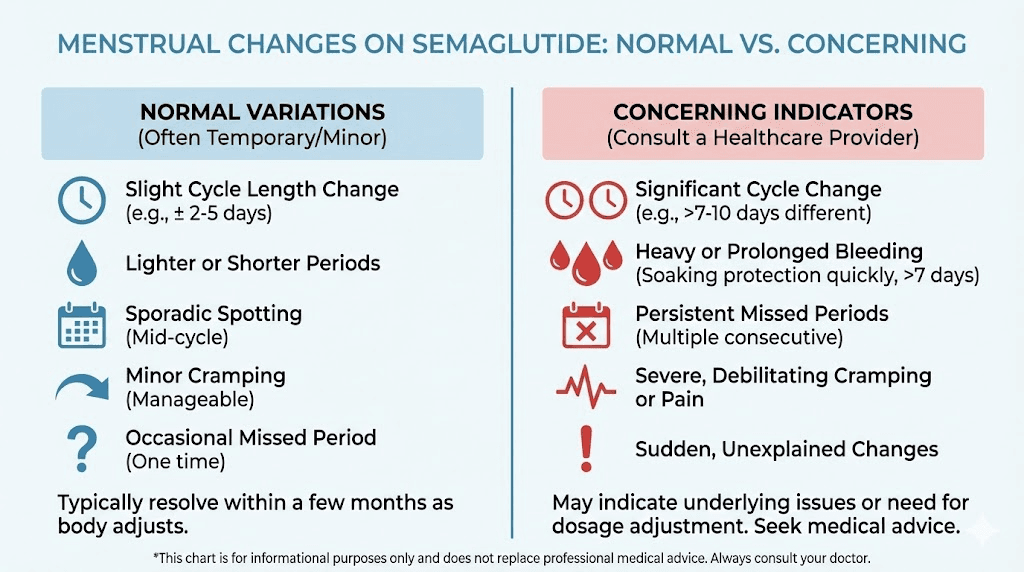
When menstrual changes are normal vs concerning
Not every change requires a doctor visit. But some changes demand prompt attention. Knowing the difference saves unnecessary anxiety on one end and prevents delayed diagnosis on the other.
Normal and expected on semaglutide
Cycle length varying by 2-7 days from your baseline during the first 3-6 months is normal. Lighter flow during active weight loss is expected. One missed period during a phase of rapid weight loss is common. Reduced PMS symptoms as inflammation decreases is a positive sign. More regular cycles if you previously had irregular ones, especially with PCOS, is actually the desired outcome.
These changes reflect the body adapting to a new metabolic environment. They typically self-correct as weight stabilizes and the hormonal environment reaches a new equilibrium. Patience during the first months of treatment is important.
See a doctor if you experience these changes
Two or more consecutive missed periods require evaluation. Pregnancy must be ruled out first, especially if you have been losing weight and potentially restoring ovulation. Beyond pregnancy, prolonged amenorrhea may indicate that the rate of weight loss needs adjustment or that a separate underlying condition requires attention.
Very heavy bleeding that soaks through a pad or tampon hourly for several hours is not a normal semaglutide side effect. This could indicate uterine polyps, fibroids, or other structural issues that the metabolic changes have unmasked or worsened.
Severe pelvic pain that is new or significantly worse than your normal menstrual cramps warrants urgent evaluation. While mild cramping changes are expected, sharp or debilitating pain could indicate ovarian cysts (which can occur when ovulation resumes after a period of anovulation) or other conditions.
Bleeding after menopause is never normal, regardless of medication use. If you are postmenopausal and experience vaginal bleeding after starting semaglutide, see your doctor promptly.
Any menstrual change accompanied by other concerning symptoms, including severe fatigue, significant hair loss, extreme mood changes, or rapid heart rate, suggests that the metabolic changes may be more aggressive than your body can comfortably manage. Your provider may recommend slowing the dose escalation or adjusting your nutrition plan.
How to track and manage cycle changes on semaglutide
Systematic tracking transforms vague concerns into actionable data. Whether you are monitoring for your own peace of mind or preparing information for a doctor visit, consistent tracking makes all the difference.
What to track each month
Start by recording cycle dates. Mark the first day of each period and how many days it lasts. Note any mid-cycle spotting. Compare each cycle length to your pre-semaglutide baseline. A simple spreadsheet or period tracking app works for this.
Track flow volume. Use a consistent scale: light, moderate, heavy, or very heavy. Note whether flow volume has changed compared to before treatment. Track how many days of each flow level you experience per cycle.
Document PMS symptoms and their severity. Cramping, bloating, mood changes, breast tenderness, headaches. Rate each on a 1-10 scale so you can spot trends over time. These subjective measures become more useful when tracked consistently.
Record your semaglutide dose and any dose changes. Note the date of each injection. When you can overlay your dose escalation timeline with your menstrual tracking data, patterns often become clear. Many women notice that cycle changes cluster around dose increases.
Also track your weight weekly. The relationship between rate of weight loss and cycle changes is one of the strongest predictors. Weeks where you lose more than 2 pounds are more likely to be followed by cycle irregularity.
Nutrition strategies for hormonal support
What you eat while on semaglutide directly affects how your hormonal system responds to the metabolic changes. Because semaglutide reduces appetite, intentional nutrition planning becomes more important, not less.
Prioritize protein. Adequate protein intake supports hormone production and helps preserve lean mass during weight loss. Aim for 25-30 grams per meal. Protein shakes designed for GLP-1 users can help meet targets when solid food intake is limited by reduced appetite.
Include healthy fats. Cholesterol is the precursor to all steroid hormones, including estrogen and progesterone. Extremely low-fat diets during semaglutide treatment can compound the hormonal disruption from weight loss. Include avocado, olive oil, nuts, and fatty fish in your semaglutide eating plan.
Do not skip iron. If your periods become heavier during the adjustment phase, iron needs increase. Red meat, spinach, lentils, and fortified cereals help maintain iron stores. Women experiencing heavier flow should consider having their ferritin levels checked.
Support with micronutrients. Vitamin D, zinc, magnesium, and B vitamins all play roles in menstrual cycle regulation. Supplementation strategies for GLP-1 users should include these along with the standard recommendations.
The semaglutide dosage calculator on SeekPeptides can help you understand your current dose in context. Pairing accurate dosing with proper nutrition creates the foundation for the smoothest possible menstrual transition during treatment.
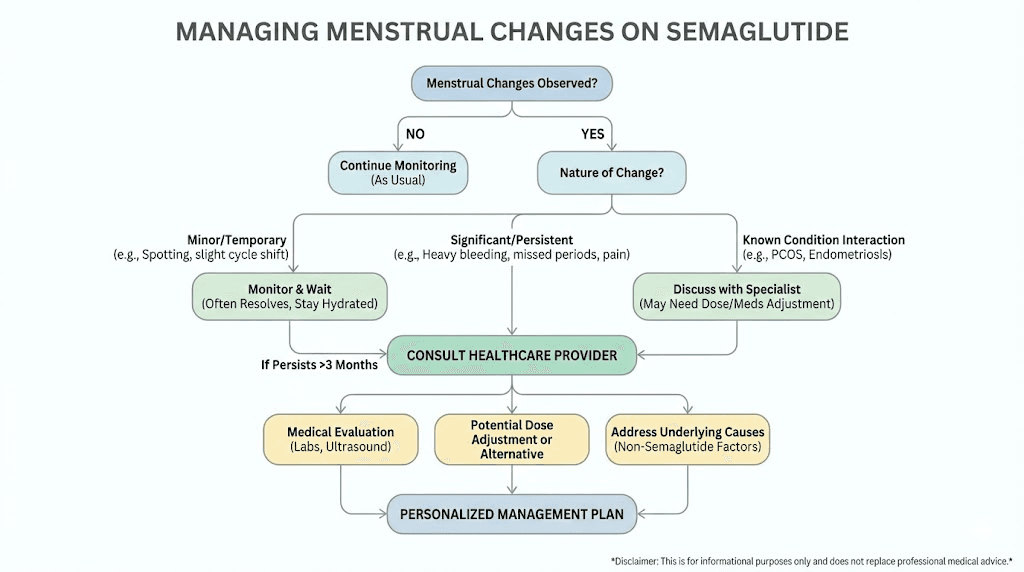
When to adjust your protocol
If menstrual changes are severe or persistent, your treatment protocol may need modification. This does not mean stopping semaglutide. It may mean slowing the dose escalation, holding at a current dose longer before increasing, or adjusting caloric intake to slow the rate of weight loss.
A common approach is to pause at the current dose for an extra 4-8 weeks before the next increase, giving the body more time to adapt. Some women find that extending the timeline of dose escalation results in fewer side effects overall, including less menstrual disruption.
Increasing caloric intake slightly during weeks of rapid weight loss can also help. The goal is not to eliminate the caloric deficit but to prevent the body from interpreting the deficit as a survival threat. Adding 200-300 calories of nutrient-dense food during weeks when you are losing more than 2 pounds can help maintain the hormonal signaling needed for regular cycles.
If you are managing combination therapy or taking other medications alongside semaglutide, discuss the interplay between all your medications and your menstrual health with your prescriber. The more variables in play, the more important coordinated medical oversight becomes.
What semaglutide does not cause
It is worth addressing misconceptions directly, because fear of side effects that do not actually exist can prevent women from benefiting from treatment.
Semaglutide does not cause early menopause. Weight loss-related cycle changes are temporary and reversible. The ovarian reserve is not affected by the medication. If your cycles are absent during rapid weight loss, they will resume when your body reaches a stable weight in the vast majority of cases.
Semaglutide does not cause endometriosis or fibroids. These are structural conditions that develop independently of GLP-1 therapy. However, metabolic changes from weight loss can sometimes change the symptom profile of existing conditions, making them more or less noticeable.
Semaglutide does not permanently damage fertility. In fact, the opposite is more common. By improving metabolic health, reducing insulin resistance, and normalizing body weight, semaglutide often improves fertility markers. The challenge is not that it reduces fertility but that it can restore it unexpectedly.
Semaglutide does not cause hormonal imbalance in the way that exogenous hormones might. It does not add estrogen, testosterone, or progesterone to your system. The hormonal changes that occur are your own body responding to improved metabolic conditions. This distinction matters because it means the changes are self-regulating. Your body will find its new hormonal equilibrium.
Practical protocols for different situations
Because every woman starting semaglutide has different concerns, here are specific guidance frameworks for common scenarios.
Protocol for women with regular cycles who want to stay regular
Goal: Minimize menstrual disruption during semaglutide treatment.
Follow the standard dose escalation schedule but consider extending each dose level by 2 weeks if you notice cycle changes. Maintain caloric intake above 1,200 calories daily, even with reduced appetite. Ensure at least 60 grams of protein per day. Include healthy fats at every meal. Track cycles weekly. If you miss a period, slow the dose escalation and increase calories by 200-300 per day until the next period arrives.
Protocol for women with PCOS hoping to regulate cycles
Goal: Use semaglutide-related metabolic improvements to normalize menstrual function.
Standard dose escalation is appropriate. Monitor for the return of regular ovulation, which typically begins within 8-12 weeks. Keep in mind that restored ovulation means restored fertility, so use contraception if pregnancy is not desired. Consider asking your doctor about cycle day 21 progesterone testing to confirm ovulation. Combine with the semaglutide nutrition plan emphasizing low-glycemic foods to further support insulin sensitivity improvements.
Protocol for women concerned about contraception
Goal: Ensure reliable birth control throughout semaglutide treatment.
If using oral contraceptives with semaglutide specifically, current evidence suggests no significant absorption reduction. If using oral contraceptives and experiencing frequent vomiting, consider switching to a non-oral method. If switching to or from tirzepatide, discuss contraceptive implications with your provider since the interaction profile differs. Non-oral methods (IUD, implant, injection, patch) are not affected by gastric emptying changes and provide the highest certainty.
Protocol for women trying to conceive
Goal: Use semaglutide to improve metabolic health before pregnancy.
Work with both a reproductive endocrinologist and your prescribing provider. Use semaglutide to reach a metabolic health target (improved insulin sensitivity, reduced weight, normalized androgens). Plan to stop semaglutide at least two months before attempting conception to allow complete drug clearance. Monitor cycle regularity as an indicator of improving reproductive health. Once cycles are regular and metabolic markers have improved, transition off semaglutide and begin conception efforts.
For more information on GLP-1 medications and pregnancy, our guide on GLP-1 and breastfeeding safety covers the postpartum considerations as well.
The role of dose and formulation
Not all semaglutide formulations are identical, and the dose you take influences the degree of menstrual change you might experience.
Standard dose escalation effects
The approved dosing schedule for weight management starts at 0.25mg weekly and increases to 0.5mg, 1mg, 1.7mg, and finally 2.4mg over approximately 16-20 weeks. Each increase can trigger a new round of metabolic adaptation, and menstrual changes often cluster around these transitions.
Women who experience significant menstrual changes at lower doses may want to discuss a slower titration with their provider. There is no clinical requirement to reach 2.4mg, the maintenance dose depends on individual response and tolerability. Some women achieve their therapeutic goals at 1mg or 1.7mg with fewer side effects than at full dose.
Compounded vs brand-name formulations
Compounded semaglutide from 503A and 503B pharmacies has become widely used. These formulations may include additional compounds like vitamin B12, glycine, or methylcobalamin. While the active ingredient is the same, differences in bioavailability between compounded products mean that effective doses may vary.
If you are using compounded semaglutide and experiencing unexpected menstrual changes, consider whether your effective dose might be different from what you think. Using the semaglutide dosage calculator to verify your dose in mg relative to the standard protocol can help identify whether a dose adjustment might explain your symptoms.
Oral vs injectable semaglutide
Oral semaglutide and sublingual formulations have different absorption profiles than injectable versions. The oral formulations used for diabetes management (Rybelsus) achieve lower bioavailability than injections, which generally means less dramatic weight loss and potentially less menstrual disruption.
However, compounded sublingual drops aim to improve oral bioavailability, and women using these formulations may experience effects closer to injectable versions depending on the dose and absorption rate.
Long-term menstrual health on semaglutide
Women taking semaglutide for extended periods (12+ months) generally report stable, predictable menstrual cycles. The initial adjustment period, the chaotic months of changing flow and timing, gives way to a new normal that is often healthier than the pre-treatment baseline.
Long-term research on GLP-1 agonists and menstrual health is still limited. Most clinical trials last 68-72 weeks, and menstrual tracking is rarely a primary or secondary endpoint. What we know comes largely from observational data and patient-reported outcomes.
The available evidence suggests that the menstrual benefits, improved regularity, reduced PMS symptoms, and normalized hormonal profiles, persist as long as the metabolic improvements from treatment are maintained. Women who discontinue semaglutide and regain weight may see their previous menstrual patterns return, including irregularity associated with insulin resistance and elevated BMI.
For women with PCOS, the menstrual improvements appear to persist as long as insulin sensitivity remains improved. This argues for a long-term treatment approach that maintains metabolic gains rather than short courses of therapy.
SeekPeptides members get access to detailed protocol guides, dosing calculators, and expert-reviewed resources that account for these long-term considerations. For women navigating the intersection of GLP-1 therapy and reproductive health, having comprehensive, evidence-based guidance makes the difference between anxiety and informed confidence.
The bigger picture: metabolic health and reproductive health are connected
Here is what gets lost in the specific discussions about semaglutide and periods. Your menstrual cycle is a vital sign. It reflects your overall metabolic health, stress level, nutritional status, and hormonal balance. When semaglutide changes your cycle, it is showing you that the metabolic environment in your body is shifting.
For most women, that shift goes in a positive direction. Weight loss improves insulin sensitivity. Better insulin sensitivity normalizes hormone production. Normalized hormones produce more regular cycles. More regular cycles indicate a healthier reproductive system.
The temporary disruptions along the way, the irregular month here, the missed period there, are the cost of transition. The body needs time to adapt to a dramatically improved metabolic environment. Just as weight loss results take time to appear, menstrual regularity takes time to establish at your new baseline.
The women who fare best are those who track their changes, communicate with their healthcare providers, maintain adequate nutrition, and view menstrual changes as data rather than danger signals. Not every change needs intervention. But every change deserves attention.
For researchers serious about understanding how GLP-1 therapy affects their complete health picture, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, protocol databases, and a community of thousands navigating these exact questions.
Frequently asked questions
Can semaglutide make your period come early?
Yes, some women report periods arriving several days earlier than expected, particularly during the first 2-3 months of treatment. This is typically related to metabolic shifts from early weight loss and changes in estrogen levels as fat mass decreases. The timing usually normalizes within 2-3 cycles at a stable dose.
Does semaglutide affect fertility?
Semaglutide is not a fertility drug, but the weight loss and metabolic improvements it produces can restore natural fertility in women whose excess weight was a barrier to ovulation. Women with PCOS see the most dramatic improvements, with up to 80% experiencing cycle normalization in clinical studies. If you are not trying to conceive, use reliable contraception throughout treatment.
Should I stop semaglutide if my period is late?
Do not stop semaglutide without consulting your prescriber. A single late or missed period during active weight loss is common and typically not concerning. Take a pregnancy test to rule out pregnancy, then continue treatment. If you miss two or more consecutive periods, schedule a medical evaluation. Your provider may recommend slowing the dose escalation or adjusting your caloric intake.
Does semaglutide interact with birth control pills?
Pharmacokinetic studies show that semaglutide does not reduce the bioavailability of combination oral contraceptives. However, if you experience vomiting within a few hours of taking your pill, absorption may be reduced. Non-oral contraceptive methods are not affected by semaglutide at all. Note that tirzepatide has a different interaction profile and may reduce oral contraceptive exposure by approximately 20%.
How long do menstrual changes last on semaglutide?
Most women experience the most significant menstrual changes during the first 3-6 months of treatment, corresponding with the dose escalation phase and most rapid weight loss. Cycles typically stabilize within 1-3 months of reaching a maintenance dose and stable weight. Women with PCOS often see ongoing menstrual improvement rather than disruption.
Can semaglutide cause heavy periods?
Some women experience heavier periods, particularly in the first few months. This is more common in women who previously had anovulatory cycles (common with PCOS or insulin resistance). When ovulation resumes, built-up uterine lining sheds more heavily than usual. This typically normalizes within 2-3 cycles. If heavy bleeding persists or you are soaking through a pad hourly, see your doctor.
Is it safe to take semaglutide during my period?
Yes. Your semaglutide injection schedule does not need to change based on your menstrual cycle. Take your weekly dose on the same day each week regardless of where you are in your cycle. Some women prefer to avoid injecting on days with the worst PMS symptoms simply for comfort, but this is personal preference rather than medical necessity.
Will my period go back to normal if I stop semaglutide?
If your menstrual changes were caused by semaglutide-related weight loss, your period patterns will depend on what happens to your weight after discontinuation. Women who maintain their weight loss typically maintain the menstrual improvements. Women who experience weight regain, which commonly occurs after stopping, may see their previous menstrual patterns return, including any irregularity associated with higher BMI and insulin resistance.
External resources
Semaglutide Treatment of Excessive Body Weight in Obese PCOS Patients (NIH/PMC)
Effects of GLP1RAs on Pregnancy Rate and Menstrual Cyclicity in Women with PCOS (NIH/PMC)
Semaglutide Does Not Reduce Bioavailability of Combined Oral Contraceptive (NIH/PMC)
Weight Loss-Related Amenorrhea: Health Effects and Therapeutic Approaches (NIH/PMC)
In case I do not see you, good afternoon, good evening, and good night. May your cycles stay regular, your hormones stay balanced, and your health stay informed.