Apr 3, 2026

Tired of watching the scale refuse to budge while you inject on schedule, eat less than ever, and do everything your provider told you to do? You are not alone. And you are not failing. The GLP-1 stall, that maddening stretch where semaglutide stops producing results, where tirzepatide seems to quit working, where your body appears to dig in its heels against every milligram of medication, is one of the most common and most misunderstood phases of GLP-1 therapy. It happens to nearly everyone. It does not mean the medication has failed. It does not mean your metabolism is broken beyond repair. And it certainly does not mean you should panic, double your dose, or abandon ship. What it means is that your body has activated a deeply ancient set of survival mechanisms, mechanisms that evolved over millions of years to prevent you from losing too much weight too quickly during famine. These mechanisms are powerful.
They are predictable. And once you understand them, they become manageable. This guide covers the complete physiology behind GLP-1 weight loss stalls across every major medication, from semaglutide to tirzepatide to retatrutide. You will learn exactly why stalls happen, when to expect them, what separates a normal stall from a genuine problem, and precisely what to do about each cause. No vague advice. No recycled platitudes. Just the science and the protocols that actually work.
What a GLP-1 stall actually means
Before you can fix a stall, you need to understand what qualifies as one. Not every pause in weight loss is a stall. Not every flat week on the scale means something has gone wrong.
Weight loss is not linear. It never has been.
Your body weight fluctuates by 2 to 5 pounds on any given day based on water retention, sodium intake, bowel contents, glycogen stores, hormonal cycles, and dozens of other variables that have nothing to do with fat loss. A person who weighs 200 pounds on Monday morning might weigh 203 on Tuesday and 198 on Thursday, all while losing fat at a steady rate the entire time. The scale captures a snapshot of total mass, not a measurement of fat tissue specifically, and those two things diverge more often than most people realize.
A true GLP-1 stall meets specific criteria.
The scale has not moved downward for 3 or more consecutive weeks. Body measurements, including waist, hips, and thighs, have remained unchanged during that same period. You have not changed your caloric intake upward. You have not reduced physical activity. And you are still taking your GLP-1 medication consistently at the prescribed dose. If all five of those conditions are true, you are likely experiencing a genuine stall. If only one or two apply, you may simply be witnessing normal weight fluctuation, which resolves on its own within a week or two.
Normal fluctuation versus a real stall
Here is a practical way to tell the difference. Track your weight daily for two weeks. Calculate the 7-day rolling average for each week. If week two average is lower than week one average, even by half a pound, you are still losing. The daily noise just made it invisible. Many people who believe they have stalled for weeks discover, once they look at rolling averages, that they have actually been losing at a slow but consistent rate the entire time.
But if that rolling average has been flat, truly flat, for three weeks or more? That is a stall. And it deserves attention.
The good news is that most GLP-1 stalls are temporary. Research shows they typically last 2 to 8 weeks before weight loss resumes, either on its own or with targeted adjustments. The key is understanding why your specific stall is happening so you can apply the right fix rather than guessing, because the wrong response to a stall can actually make it worse and extend its duration significantly.
The physiology behind GLP-1 weight loss stalls
Your body does not want to lose weight. That statement sounds dramatic, but it is physiologically accurate. Every system in your body, from hormones to neural circuits to cellular metabolism, is calibrated to defend a set point that your brain has decided represents safety. When you start losing weight, especially at the rapid pace that GLP-1 medications enable, those systems activate in force. Understanding these mechanisms is not academic. It is essential for troubleshooting your stall, because different mechanisms require different solutions.
Adaptive thermogenesis: your metabolism fights back
This is the big one.
When you lose weight, your total daily energy expenditure drops. Part of that drop is straightforward physics: a smaller body burns fewer calories simply because there is less tissue to maintain. If you weighed 250 pounds and now weigh 220, your body requires fewer calories at rest, during movement, and during digestion. That accounts for roughly 60% of the reduction in energy expenditure following significant weight loss.
But the other 40% is something far more insidious. It is called adaptive thermogenesis, and it represents your body actively reducing energy output beyond what the change in body size would predict. Research published in major metabolic journals shows that total energy expenditure decreases approximately 15% following a 10% reduction in body weight. If the math suggests you should only be burning 8% fewer calories based on your new size, that extra 7% gap is adaptive thermogenesis, your metabolism deliberately slowing down to conserve energy because it interprets weight loss as a threat to survival.
This affects everything. Your resting metabolic rate drops. The thermic effect of food decreases. Non-exercise activity thermogenesis, the calories you burn through fidgeting, posture maintenance, and unconscious movement, declines substantially. You might not notice that you are moving less, sitting more still, taking fewer steps, and generating less body heat. But your body notices, because your body is orchestrating all of it.
The result is a shrinking gap between calories consumed and calories burned. Eventually, if no adjustments are made, that gap closes entirely. Weight loss stops. A stall begins.
The appetite feedback circuit: how GLP-1 medications change the equation
Here is where the science gets genuinely interesting, and where GLP-1 medications demonstrate their remarkable advantage over traditional dieting.
When you lose weight through calorie restriction alone, your body ramps up hunger signals aggressively. Researchers quantify this using a metric called the appetite feedback gain coefficient, represented as "k." For traditional calorie restriction, that coefficient is approximately 82 kcal per day per kilogram of weight lost. That means for every kilogram you lose through dieting, your body increases your drive to eat by about 82 calories per day. Lose 10 kilograms, and your body is pushing you to eat 820 extra calories daily. That is an enormous pressure, and it explains why diet-only approaches fail so frequently.
GLP-1 receptor agonists dramatically weaken this feedback loop. For semaglutide, the appetite feedback coefficient drops to approximately 49 kcal per day per kilogram. For tirzepatide, it is even slightly lower at around 48 kcal per day per kilogram. That represents roughly a two-fold weakening of the appetite feedback circuit compared to dieting alone.
What does this mean practically?
It means you can lose more weight before the hunger pressure becomes overwhelming. It means the plateau arrives later. And it means that when a stall does occur on GLP-1 therapy, the appetite component is playing a smaller role than it would on a diet, which tells you to look at other factors first. For context, Roux-en-Y gastric bypass surgery weakens this circuit by approximately four-fold, which partly explains why surgical outcomes often exceed pharmaceutical ones in total weight lost. But GLP-1 medications, particularly the newer dual and triple agonists, are closing that gap with each generation.
Lean mass loss: the silent saboteur
This one matters more than most people realize.
When you lose weight, you do not lose only fat. You lose muscle too. And muscle is metabolically expensive tissue. It burns calories at rest, during movement, and during recovery. Every pound of muscle you lose reduces your daily energy expenditure and brings you closer to a stall.
The STEP-1 trial, one of the landmark studies for semaglutide 2.4mg, showed that participants lost approximately 9.7% of their lean mass alongside a 19.3% reduction in fat mass. The SURMOUNT-1 trial for tirzepatide painted a similar picture, with roughly 25% of total weight lost coming from lean tissue and 75% from fat over the 72-week study period. Those ratios are actually better than what you see with calorie restriction alone, where lean mass losses can approach 30-40% of total weight lost. But even at 25%, the metabolic consequences compound over time.
Consider a person who has lost 40 pounds on tirzepatide. If 25% of that loss is lean mass, they have lost 10 pounds of muscle. That is a meaningful reduction in their metabolic engine, a reduction that directly contributes to the caloric deficit shrinking and a stall developing. This is precisely why protein intake and resistance training are not optional during GLP-1 therapy. They are essential anti-stall strategies.
Hormonal recalibration
Weight loss triggers a cascade of hormonal shifts that extend far beyond appetite. Leptin, the hormone produced by fat cells that signals energy sufficiency to the brain, drops in proportion to fat loss. Lower leptin tells your hypothalamus that energy stores are depleting, which triggers a coordinated response: increase hunger, decrease energy output, reduce reproductive hormone production, and conserve resources at every level.
Thyroid function shifts. Specifically, the conversion of T4 to the active T3 hormone can slow during caloric deficit, reducing metabolic rate further. This is particularly relevant for people with Hashimoto thyroiditis or other thyroid conditions who are already operating with compromised thyroid function. Cortisol, the stress hormone, may rise during prolonged caloric deficit, promoting water retention and, in some cases, preferential abdominal fat storage. Insulin sensitivity changes as body composition shifts, which can alter how your body partitions fuel between storage and oxidation.
All of these hormonal adjustments happen gradually. They accumulate. And they create a physiological environment that increasingly resists further weight loss. The stall you experience at month four or month six is not one thing going wrong. It is dozens of subtle adaptations stacking on top of each other until the net effect is zero progress on the scale.
The set point defense system
Your brain maintains a body weight set point, a range it considers normal and safe based on your weight history. When you deviate significantly below this set point, the hypothalamus activates increasingly aggressive defense mechanisms. Some researchers believe this set point can be adjusted downward over time, particularly if the new lower weight is maintained for 12 months or more. Others argue that the set point is remarkably persistent, especially in individuals with a long history of obesity.
What is not debated is that the defense is real. Your brain will fight to return you to its preferred weight range using every tool at its disposal. GLP-1 medications work partly by influencing the brain circuits involved in set point regulation, which is why they produce larger and more sustained weight loss than dietary approaches. But even with pharmaceutical assistance, the set point defense eventually creates enough counterforce to slow or stop weight loss temporarily.
Timeline: when stalls typically happen on each GLP-1
Not all GLP-1 medications behave identically. Their mechanisms overlap, but their potency, receptor targets, and dose escalation schedules differ in ways that affect when and how stalls occur. Understanding the typical timeline for your specific medication helps you distinguish between a normal, expected pause and something that warrants investigation.
Semaglutide stall timeline
Semaglutide, the GLP-1 receptor agonist marketed as Ozempic and Wegovy, follows a well-documented trajectory. Most users experience noticeable appetite suppression within the first week, though weight loss during the initial low doses (0.25mg) is often modest. The real momentum builds during weeks 4 through 16 as the dose escalates through 0.5mg, 1.0mg, and up to 1.7mg or 2.4mg.
The first common stall window hits around months 3 to 5. This often coincides with the body initial adaptive response to rapid weight loss. Many users resolve this stall naturally as their dose continues to increase. The second, more significant stall window typically arrives between months 8 and 14, when the full 2.4mg dose has been reached and the body metabolic adaptations have fully engaged. Clinical data from the STEP trials show that weight loss on semaglutide 2.4mg begins to plateau meaningfully around 24 months, at which point most achievable weight loss has been realized.
First-month results vary widely. Some people lose 5 to 8 pounds. Others see minimal scale movement. Both outcomes can be perfectly normal depending on starting weight, metabolic health, and individual response to the medication.
Tirzepatide stall timeline
Tirzepatide is a dual GIP/GLP-1 receptor agonist, and that dual mechanism produces a somewhat different stall pattern. Because tirzepatide targets two incretin receptors rather than one, its weight loss trajectory tends to be steeper initially, with greater total weight loss over time compared to semaglutide monotherapy.
The first stall window for tirzepatide users commonly occurs around months 2 to 4, often during the dose escalation phase. The medication starts at 2.5mg and escalates through 5mg, 7.5mg, 10mg, 12.5mg, and up to 15mg. Each dose increase typically reignites weight loss momentum, meaning stalls during escalation are often temporary and self-resolving.
The more persistent stall tends to arrive around months 9 to 15 on tirzepatide, particularly once the maximum tolerated dose has been reached. SURMOUNT-1 data shows that tirzepatide at the 10mg dose begins to plateau around 24 months as well, though higher doses may extend the active weight loss window somewhat further. The appetite feedback coefficient for tirzepatide (k=48) is marginally lower than semaglutide (k=49), which means the appetite rebound component may be very slightly less aggressive, potentially contributing to a somewhat longer active loss phase in some individuals.
Retatrutide stall timeline
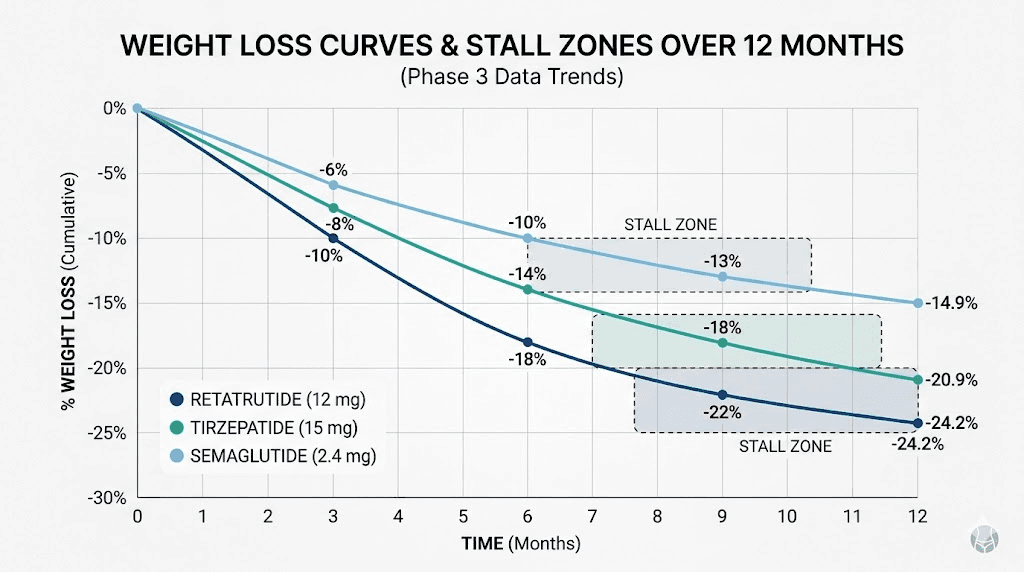
Retatrutide is the newest entrant, a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. Early Phase 2 trial data suggests this triple mechanism produces the most aggressive weight loss of any pharmaceutical approach to date, with some dose groups achieving over 24% body weight reduction in 48 weeks.
Because retatrutide is newer, long-term stall data is limited. However, the glucagon receptor component adds a metabolic dimension that GLP-1 and GIP alone do not provide. Glucagon receptor activation increases energy expenditure directly, potentially offsetting some of the adaptive thermogenesis that drives stalls on other GLP-1 medications. This suggests, though it remains to be proven in longer trials, that the stall window for retatrutide may arrive later and be less pronounced than for single or dual agonists.
The retatrutide dose schedule involves gradual escalation that typically spans several months, during which minor stalls may occur but often resolve with each dose increase.
Calorie restriction comparison
For perspective, weight loss through calorie restriction alone typically plateaus within 6 to 12 months. The appetite feedback coefficient of 82 kcal/day/kg means hunger pressure builds roughly twice as fast as it does on GLP-1 therapy. This is why most diet-only approaches see weight regain beginning within the first year, while GLP-1 medications extend the active loss phase to 18 to 24 months or longer.
That extended window is the medication doing its job. A stall at month 10 on semaglutide is not failure. It is your body catching up to a level of intervention that kept it at bay far longer than diet alone ever could.
Common causes of GLP-1 stalls
The physiology sets the stage. But specific, identifiable factors determine exactly when your stall arrives and how long it lasts. Some of these are within your direct control. Others require provider involvement. All of them are worth evaluating systematically rather than guessing.
Undereating: the counterintuitive problem
This one surprises people.
GLP-1 medications suppress appetite so effectively that many users drastically reduce their caloric intake, sometimes to 600 to 800 calories per day, without realizing how little they are actually eating. In the short term, this produces rapid weight loss. In the medium term, it triggers a disproportionately aggressive metabolic slowdown. Your body interprets severe caloric restriction as starvation, and it responds by slashing energy expenditure, ramping up cortisol, increasing water retention, and downregulating thyroid function, all of which conspire to halt weight loss despite what looks like a massive calorie deficit on paper.
The solution is not to eat more junk food. It is to ensure you are eating enough nutrient-dense food to maintain metabolic function. For most people on GLP-1 therapy, a floor of 1,200 calories per day for women and 1,400 to 1,500 calories per day for men represents the minimum needed to avoid triggering an exaggerated starvation response. Going below this threshold consistently is one of the most common and most fixable causes of GLP-1 stalls.
Protein deficit: losing the wrong kind of weight
Insufficient protein intake is epidemic among GLP-1 users. When your appetite is suppressed and you are eating less overall, protein often takes the biggest hit because protein-rich foods require more effort to prepare and consume than simple carbohydrates. But inadequate protein directly accelerates lean mass loss, which directly accelerates metabolic slowing, which directly accelerates stalls.
The research is clear on targets. You need a minimum of 1.2 grams of protein per kilogram of body weight per day during active weight loss, and ideally closer to 0.6 to 0.75 grams per pound of your goal body weight. For a person targeting 160 pounds, that means 96 to 120 grams of protein daily. Every day. Without exception.
This is not easy when your appetite is suppressed. It requires intentional planning. It often requires prioritizing protein at every meal, eating protein first before anything else on the plate, and potentially using protein supplements to hit targets on days when whole food intake is low. But the payoff is significant: preserving muscle mass keeps your metabolic rate higher, delays stalls, and ensures that a greater percentage of the weight you lose is fat rather than metabolically active tissue.
A study of 200 adults found that participants who combined adequate protein intake with resistance training lost 13% of their body weight but only 3% of their muscle mass. Compare that to the 25% lean mass loss seen in clinical trials without these interventions. The difference is enormous, both for stall prevention and for long-term metabolic health.
Muscle loss without resistance training
Protein alone is not enough. Your muscles need mechanical stimulus to receive the signal that they should be preserved. Without resistance training, your body treats muscle tissue as expendable during a caloric deficit, breaking it down for amino acids and energy while preserving fat stores, because from an evolutionary perspective, fat is more calorically dense and therefore more valuable during a famine.
Resistance training reverses this priority signal. It tells your body, in a language your physiology cannot ignore, that this muscle is being used and must be maintained. Two sessions per week is the minimum threshold supported by research. Three sessions is better. The sessions do not need to be marathon gym visits. Thirty to forty-five minutes of compound movements, squats, deadlifts, presses, rows, done with progressive overload, is sufficient to meaningfully preserve lean mass during GLP-1 therapy.
If you are experiencing a stall and you are not doing resistance training, this is likely a significant contributing factor. It is also one of the easiest to address.
Constipation and bowel stasis
GLP-1 receptor agonists slow gastric motility. That is part of how they work, keeping food in the stomach longer promotes satiety. But this same mechanism can cause significant constipation, particularly at higher doses. And constipation directly masks weight loss on the scale.
A person carrying 3 to 5 extra pounds of stool due to slowed transit is still losing fat. They just cannot see it. This creates a frustrating illusion of a stall when fat loss is actually continuing normally underneath the constipation weight. Semaglutide constipation and tirzepatide constipation are among the most commonly reported side effects, and they deserve targeted management rather than passive tolerance.
Increasing fiber intake through supplementation (particularly psyllium husk), maintaining adequate hydration, and ensuring regular physical movement can all help. A quality fiber supplement taken consistently can make a substantial difference in transit time. If dietary interventions are insufficient, magnesium citrate or an osmotic laxative may be appropriate, but discuss these with your provider first.
Water retention and fluid shifts
Weight loss is not a smooth, continuous process at the cellular level. When fat cells release their stored triglycerides, they often temporarily fill with water, maintaining their volume for days or weeks before finally deflating. This phenomenon, sometimes called the "whoosh effect" in popular fitness communities, means that fat loss can be happening silently for weeks with zero scale movement, followed by a sudden drop of several pounds seemingly overnight.
Sodium intake fluctuations amplify this effect. A single high-sodium meal can cause 2 to 4 pounds of water retention that takes 48 to 72 hours to clear. Hormonal fluctuations, particularly the menstrual cycle in women, can cause regular monthly water retention patterns that completely obscure fat loss for one to two weeks per cycle. Semaglutide can affect menstrual patterns and tirzepatide can alter cycle timing, which may change the water retention pattern you were previously accustomed to.
Bloating on semaglutide and bloating on tirzepatide can also contribute to the perception of a stall even when body fat is decreasing. Electrolyte balance plays a role here as well. Proper electrolyte supplementation can help regulate fluid balance and reduce the masking effect of water retention on scale weight.
Sleep disruption
Poor sleep is a stall accelerator that operates through multiple pathways simultaneously. Sleep deprivation increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone), partially counteracting the appetite-suppressing effects of your GLP-1 medication. It impairs insulin sensitivity, increases cortisol production, and reduces the secretion of growth hormone, which plays a critical role in fat oxidation and muscle preservation during sleep.
Research consistently shows that individuals sleeping fewer than 6 hours per night lose significantly less fat and significantly more muscle during caloric restriction compared to those sleeping 7 to 9 hours. The metabolic penalty of poor sleep compounds over weeks, gradually eroding the caloric deficit that drives weight loss until it reaches zero.
Some GLP-1 users report insomnia on semaglutide or sleep disruption on tirzepatide, which creates a vicious cycle: the medication disrupts sleep, poor sleep promotes a stall, and the stall causes frustration that further impairs sleep quality. If you are experiencing sleep issues, addressing them aggressively, through sleep hygiene protocols, timing adjustments for your injection, or discussion with your provider, should be a top priority.
Chronic stress and elevated cortisol
Cortisol does not cause fat gain directly in the way popular media suggests. But chronically elevated cortisol does promote water retention, impair insulin sensitivity, disrupt sleep, increase cravings for hyperpalatable foods, and signal to your hypothalamus that the body is under threat, all of which collectively create conditions favorable for a stall. Stress management is not a luxury during GLP-1 therapy. It is a metabolic intervention.
Dose plateau: when your current dose has maxed out
GLP-1 medications work in a dose-dependent manner. A dose that produced significant appetite suppression and weight loss three months ago may be insufficient now that your body has adapted. This is normal pharmacological tolerance, and it is one reason these medications use a dose escalation schedule rather than starting at the maximum.
If you are stalling at a sub-maximum dose, a dose increase may be all that is needed. If you are already at the maximum approved dose and experiencing a stall, the options change, and a conversation with your provider about next steps becomes important. The semaglutide dosing structure and tirzepatide dosing guide provide reference frames for understanding where you are in the escalation process.
Some providers explore strategies like splitting the semaglutide dose twice weekly or splitting the tirzepatide dose to maintain more consistent blood levels throughout the week, which may improve efficacy at the same total weekly dose.
Medication timing and absorption issues
While less common as a primary stall cause, inconsistent medication timing can affect blood levels and efficacy. Taking semaglutide at the optimal time and choosing the best time for tirzepatide can help maintain consistent drug levels. Injection technique matters too. Proper injection site selection and correct injection technique ensure that the full dose is delivered subcutaneously where it can be absorbed properly.
For those using compounded formulations, compounded semaglutide may occasionally underperform due to quality or potency variations between pharmacies. This is worth considering if your stall coincides with starting a new batch or switching compounding sources.
Dietary composition beyond calories
Two people eating 1,400 calories per day can have radically different metabolic outcomes depending on what those calories consist of. A diet heavy in refined carbohydrates and ultra-processed foods produces greater insulin spikes, more inflammation, worse gut microbiome diversity, and less favorable body composition changes compared to one centered on whole foods with adequate protein, healthy fats, and fiber.
A well-structured semaglutide diet plan or tirzepatide diet plan that prioritizes protein, includes fibrous vegetables, and limits ultra-processed foods can make the difference between a brief stall and a prolonged one. Foods to avoid on semaglutide and foods to avoid on tirzepatide are worth reviewing if your current dietary approach has not been deliberately optimized.
Supplement gaps
Reduced food intake during GLP-1 therapy often means reduced micronutrient intake. Deficiencies in key nutrients can impair metabolic function in ways that contribute to stalls. Vitamin D deficiency impairs insulin sensitivity. B12 deficiency reduces energy and metabolic efficiency, which is why semaglutide with B12 and tirzepatide with B12 combinations have gained popularity. Magnesium deficiency impairs sleep quality and insulin signaling. Iron deficiency reduces exercise capacity and metabolic rate.
A comprehensive GLP-1 supplement strategy that covers these common gaps can address a subtle but meaningful contributor to stalls. The GLP-1 vitamin guide provides a framework for identifying and addressing the most common deficiencies.
How to break through a GLP-1 stall
Now the actionable part. You know what causes stalls. Here is what to do about them, organized by impact and ease of implementation. Do not try to change everything at once. Instead, identify which causes most likely apply to you and address them systematically, giving each intervention 2 to 3 weeks before evaluating its effect.
Protocol one: fix your protein
This is the single highest-impact change most people can make.
Calculate your target: 0.6 to 0.75 grams of protein per pound of goal body weight. If your goal weight is 160 pounds, you need 96 to 120 grams of protein per day. Track your actual intake for three days using a food scale and a tracking app. Most people are shocked to discover they are getting 40 to 60 grams when they thought they were getting 80 to 100.
Eat protein first at every meal. Before vegetables. Before carbs. Before anything else. This ensures protein targets are met even when appetite suppression limits total intake. High-protein meals on tirzepatide and protein-rich foods on semaglutide become significantly easier when protein is the non-negotiable anchor of every plate.
Practical protein sources that work well with suppressed appetite include Greek yogurt (15-20g per serving), cottage cheese (14g per half cup), protein shakes (25-40g per shake), deli turkey or chicken breast (7g per ounce), eggs (6g each), and collagen peptide powder added to coffee or water (10-20g per scoop). Protein-forward breakfast ideas and high-protein dinner options can help with meal planning when appetite is low.
Protocol two: add resistance training
If you are not currently doing resistance training, starting a basic program is the second highest-impact intervention available. Two to three sessions per week. Compound movements. Progressive overload, meaning you gradually increase weight, reps, or sets over time.
A minimal effective program looks like this. Session A: squats, bench press or push-ups, rows. Session B: deadlifts, overhead press, pull-ups or lat pulldowns. Alternate between sessions. Start with weights that feel manageable and focus on form for the first two weeks, then begin adding weight incrementally.
The study data is compelling: 200 adults who combined adequate protein with resistance training lost 13% of body weight but only 3% of muscle mass. That muscle preservation translates directly into a higher resting metabolic rate, a larger daily calorie burn, and a significantly reduced likelihood of prolonged stalls. Preventing muscle loss is not just cosmetic. It is a metabolic strategy with measurable outcomes.
Some GLP-1 users report muscle pain on tirzepatide or general body aches that make exercise feel daunting. If this applies to you, start lighter than you think you need to. Even bodyweight exercises performed consistently provide meaningful muscle preservation stimulus. The goal is progressive resistance, not punishment.
Protocol three: optimize hydration and electrolytes
Dehydration impairs fat oxidation, reduces exercise performance, increases perceived fatigue, and promotes water retention paradoxically, because a dehydrated body holds onto fluid more aggressively. Aim for a baseline of half your body weight in ounces of water daily, adjusted upward for exercise and climate.
Electrolytes matter as much as water volume. Sodium, potassium, and magnesium all play roles in fluid regulation. When you are eating less food overall, you are also consuming fewer electrolytes through diet, which can throw off your fluid balance. A quality electrolyte supplement designed for GLP-1 users addresses this gap directly.
Gut health support through probiotics also plays a role in fluid balance and bloating reduction, both of which can unmask weight loss that was being hidden by water retention and digestive stasis.
Protocol four: address constipation directly
If you are not having a bowel movement at least once daily, this could be masking pounds of actual fat loss. Here is the escalation protocol.
Start with fiber. A psyllium husk supplement, 5 to 10 grams daily, taken with plenty of water, is the first-line intervention. Add magnesium citrate, 200 to 400mg at bedtime, which serves double duty as a mild laxative and a sleep-quality enhancer. Ensure you are moving daily, even if just a 20-minute walk, as physical movement stimulates peristalsis.
If these measures are insufficient, talk to your provider about osmotic laxatives or adjusting your medication timing. Some people find that taking tirzepatide at night versus morning changes the severity of GI side effects, including constipation.
Protocol five: fix your sleep
Seven to nine hours. Non-negotiable.
If your GLP-1 medication is disrupting sleep, consider these adjustments. Change your injection day or time. Some users report that taking their injection in the morning rather than evening reduces nighttime GI discomfort and sleep disruption. Create a strict sleep schedule with consistent bed and wake times, even on weekends. Eliminate screens 60 minutes before bed. Keep the bedroom cold, 65 to 68 degrees Fahrenheit is optimal for most people. Magnesium glycinate before bed can improve sleep quality while also helping with constipation.
Fatigue on semaglutide and tiredness on tirzepatide often improve with better sleep quality, creating a positive feedback loop where improved rest leads to better energy, more activity, and resumed weight loss. The complete GLP-1 fatigue guide covers additional strategies specific to medication-related tiredness.
Protocol six: evaluate your caloric floor
Track your actual caloric intake for one full week. Use a food scale. Be honest and precise. If your average daily intake is below 1,200 calories for women or 1,400 for men, you may be in a metabolic conservation state that is actively preventing weight loss despite the severe deficit.
The fix is counterintuitive: eat slightly more. Not a lot more. An additional 200 to 300 calories per day from nutrient-dense sources, particularly protein and healthy fats, can sometimes restart a stalled metabolism by signaling to your body that the famine is not as severe as it feared. This is not a free license to overeat. It is a targeted intervention based on the specific cause of undereating-induced metabolic suppression.
Nutrient-dense GLP-1 recipes that pack substantial nutrition into small volumes are especially valuable here, because they allow you to increase caloric and protein intake without needing a large appetite.
Protocol seven: consider dose adjustment or medication change
If you have addressed all of the lifestyle factors above and your stall persists beyond 6 to 8 weeks, it may be time to discuss pharmacological adjustments with your provider.
Options include increasing to the next dose level if you are not yet at maximum. They include switching medications entirely, which resets the receptor desensitization that may have developed. They include adding adjunctive therapies that complement GLP-1 activity through different mechanisms.
Switching from semaglutide to tirzepatide is one of the most common transitions when a stall persists, as the dual receptor mechanism can reignite weight loss even when single-receptor therapy has plateaued. The semaglutide to tirzepatide conversion chart provides dosing guidance for this transition. Similarly, switching from tirzepatide to retatrutide adds a third receptor target that may overcome a dual-agonist plateau.
Some providers explore combination approaches, such as adding metformin to semaglutide or combining metformin with tirzepatide for additional insulin-sensitizing effects. Others may consider berberine alongside semaglutide or berberine with tirzepatide as natural adjuncts with metabolic-supporting properties.
Protocol eight: supplement strategically
Targeted supplementation can address specific metabolic bottlenecks that contribute to stalls. Here are the evidence-backed options.
Creatine supports muscle preservation and performance during resistance training, which indirectly helps prevent metabolic slowdown. Standard dosing is 3 to 5 grams daily. Note that creatine causes 2 to 4 pounds of intracellular water retention in muscle tissue, which will show on the scale but does not represent fat gain. Creatine with semaglutide and creatine with tirzepatide are both generally well-tolerated combinations.
L-carnitine supports fatty acid transport into mitochondria for oxidation. L-carnitine with semaglutide and levocarnitine with tirzepatide are increasingly popular stacks among GLP-1 users seeking to optimize fat oxidation during a stall.
Glycine, an amino acid involved in collagen synthesis and sleep quality, can be a useful addition. Semaglutide with glycine and tirzepatide with glycine combinations support connective tissue health during rapid weight loss while also improving sleep architecture.
Niacinamide (vitamin B3) supports cellular energy metabolism. Some users find that niacinamide with semaglutide or niacinamide with tirzepatide helps maintain energy levels during periods of reduced caloric intake, which supports adherence to exercise programs.
The complete tirzepatide supplement guide covers additional options and dosing recommendations for those wanting a comprehensive approach.
GLP-1 stall versus medication failure: knowing the difference
This distinction matters enormously, because the appropriate response to a stall is fundamentally different from the appropriate response to a medication that genuinely is not working for you.
A stall is temporary. It occurs after a period of successful weight loss. It happens because your body adaptive mechanisms have caught up to the intervention. It typically resolves with lifestyle adjustments, dose changes, or simply time. And it does not mean the medication has stopped working. The medication is still activating GLP-1 receptors, still slowing gastric emptying, still modulating appetite circuits. The stall reflects a new equilibrium between these pharmaceutical effects and your body counterregulatory forces.
Medication failure is different. If you have been on an adequate dose for 12 or more weeks and have experienced virtually no weight loss from the beginning, that may indicate a genuine non-response. Semaglutide does not work for a small percentage of people, typically 10 to 15% of users in clinical trials who are classified as non-responders. The reasons vary from genetic factors affecting receptor sensitivity to metabolic conditions that override GLP-1 signaling to undiagnosed medical issues masking the medication effects.
Here is a simple framework for distinguishing the two scenarios.
If you lost weight initially and then stopped, it is almost certainly a stall, not failure. The medication worked. Your body adapted. That is normal biology.
If you have never lost more than 2 to 3 percent of your body weight despite being on an adequate dose for 3 or more months with good adherence, you may be a non-responder and should discuss alternatives with your provider.
If your weight loss has been extremely slow but consistent, that is not a stall either. Some people lose weight at a fraction of the rate seen in clinical trials and still achieve meaningful total loss over a longer timeframe. GLP-1 medications take variable amounts of time to reach full effect, and individual response curves are wide.
The psychological dimension
Stalls are not just physiological events. They are psychological tests. Weeks of no progress on the scale, after experiencing the dopamine hit of consistent losses, can trigger frustration, self-doubt, disordered eating behaviors, and the temptation to make drastic changes that often backfire.
This is where mindset work becomes a genuine tool. Remind yourself that the stall is evidence the medication worked, because you cannot stall if you never lost weight in the first place. Take body measurements during stalls, because body composition changes (fat loss plus muscle preservation) often continue even when scale weight is static. Look at before and after semaglutide transformations or tirzepatide before and after results and notice how many people report extended stall periods within their overall success stories.
The GLP-1 before and after collection and men before and after tirzepatide show real-world timelines that include stalls, plateaus, and breakthroughs. They normalize the experience in ways that clinical trial averages cannot.
Advanced strategies for persistent stalls
If the foundational protocols above have been implemented faithfully for 4 to 6 weeks and your stall persists, consider these more advanced approaches.
Calorie cycling and refeed days
Rather than eating a consistent caloric deficit every day, some people respond to periodic higher-calorie days. One to two days per week at maintenance calories, with the focus on increased protein and carbohydrates, can signal to your hypothalamus that food is not scarce, temporarily reducing the adaptive thermogenesis response. This is not a cheat day. It is a structured refeed that targets specific hormonal mechanisms, particularly leptin resensitization.
On refeed days, increase total calories by 20 to 30% above your typical intake, primarily through additional protein and complex carbohydrates. Keep fat intake moderate. Return to your standard intake the following day. Some people find that one refeed day per week is sufficient, while others benefit from two, spaced 3 to 4 days apart.
Medication timing experiments
The day of the week you take tirzepatide and the time of day for semaglutide can influence how the medication interacts with your daily eating patterns, exercise schedule, and sleep. Some users report improved efficacy when they switch from evening to morning injections, or vice versa. Others find that aligning their injection day with their most active days of the week produces better outcomes.
This is anecdotal territory, not rigorously studied. But given that the intervention is simple and risk-free, experimenting with timing during a stall is reasonable.
Alternating or combining medications
A growing number of providers are exploring creative pharmacological approaches for persistent stalls. Alternating between semaglutide and tirzepatide on a weekly or monthly basis may prevent the receptor desensitization that contributes to stalls on either medication alone. Using semaglutide and tirzepatide together is less common and carries more risk, but has been explored in clinical practice for refractory cases.
The addition of phentermine to semaglutide or phentermine to tirzepatide is another approach some providers use for short-term stall-breaking. Phentermine acts through different mechanisms, primarily norepinephrine release, and can provide a complementary push past a plateau. However, this combination requires careful monitoring and is not appropriate for everyone.
Hormonal optimization
For some individuals, an unaddressed hormonal issue is the primary driver behind a persistent stall. Hormone replacement therapy combined with GLP-1 medications can be synergistic, particularly for perimenopausal and menopausal women or for men with low testosterone. Testosterone optimization alongside tirzepatide can improve body composition, increase metabolic rate, and help break through stalls driven by hormonal insufficiency.
Thyroid function deserves specific attention during a stall. GLP-1 medications in the context of Hashimoto disease require careful thyroid monitoring, because the metabolic effects of suboptimal thyroid function can completely neutralize the caloric deficit that GLP-1 therapy creates. If you have not had thyroid labs checked since starting your medication, a persistent stall is a good reason to request them.
Alternative delivery methods
Some users experiencing stalls on injectable GLP-1 medications explore alternative delivery routes. Oral tirzepatide, tirzepatide drops, sublingual semaglutide, and oral semaglutide drops offer different pharmacokinetic profiles that may produce a different response pattern. While switching delivery methods is unlikely to overcome a physiological plateau on its own, it can be one piece of a broader adjustment strategy.
Explore the broader peptide landscape
GLP-1 medications are not the only peptide-based approach to fat loss. The best peptides for fat loss include options beyond GLP-1 agonists, and some of these can complement GLP-1 therapy or serve as alternatives for people who have reached the limits of GLP-1 monotherapy. Peptide stacking strategies for weight loss represent an area of active research and clinical innovation.
The fat loss peptide overview at SeekPeptides provides a comprehensive comparison of different peptide approaches, including those that target growth hormone pathways, metabolic rate directly, or body composition through mechanisms entirely distinct from GLP-1 receptor activation. For women dealing with hormonal weight gain, peptides for menopause-related weight loss represent a specialized niche worth exploring.
Special populations and unique stall patterns
Women and hormonal cycle stalls
Women experience predictable stall patterns tied to their menstrual cycle that men do not face. The luteal phase, the roughly two weeks between ovulation and menstruation, is associated with increased progesterone, which promotes water retention, bloating, and increased appetite. Many women see the scale climb 2 to 5 pounds during this phase and then drop dramatically after menstruation begins.
If you are a woman experiencing what appears to be a stall, track your weight against your cycle for two full months before concluding that the stall is real. You may discover that you are losing fat consistently but the cyclical water retention is masking it on the weeks you happen to weigh yourself. Changes in menstrual patterns on semaglutide can further complicate this picture.
People with autoimmune conditions
Autoimmune conditions create unique stall dynamics. Chronic inflammation, immune-modulating medications, and altered metabolic pathways can all affect GLP-1 response. Microdosing GLP-1 for autoimmune conditions is an emerging approach that some providers use to balance weight management with autoimmune disease management. Tirzepatide in the context of autoimmune disease has its own considerations and potential benefits beyond weight loss.
People transitioning between medications
A stall that occurs during or shortly after a medication switch deserves special patience. Switching from tirzepatide to semaglutide or vice versa involves a transition period where receptor signaling adjusts to the new medication profile. Weight loss may pause or even reverse slightly during this adjustment, typically lasting 2 to 4 weeks. This is expected, not pathological, and rarely requires additional intervention beyond giving the new medication time to reach steady state.
Similarly, restarting semaglutide after a break often involves a brief stall period as the medication rebuilds blood levels and begins re-engaging appetite circuits. The semaglutide onset timeline and tirzepatide onset timeline provide reference frames for what to expect when starting or restarting these medications.
Lifestyle factors that quietly extend stalls
Alcohol consumption
Alcohol delivers empty calories, impairs sleep quality, reduces growth hormone secretion, increases cortisol, and temporarily shuts down fat oxidation while your liver prioritizes alcohol metabolism. Even moderate alcohol consumption, two to three drinks per week, can meaningfully extend a stall. Drinking on semaglutide and drinking on tirzepatide is possible but comes with metabolic consequences that directly affect weight loss progress.
During a stall, eliminating alcohol entirely for 4 weeks is one of the most impactful single changes you can make. If complete elimination feels extreme, reducing to one drink per week on a non-consecutive day from your injection provides the best harm-reduction approach.
The keto question
Some GLP-1 users explore ketogenic diets alongside semaglutide as a stall-breaking strategy. The theory is that combining pharmaceutical appetite suppression with ketosis-driven metabolic changes might overcome a plateau. The evidence is mixed. Some users report success. Others find that the extremely low carbohydrate intake of keto is difficult to sustain alongside GLP-1 appetite suppression and can lead to even more severe undereating.
If you explore this approach, monitor your caloric intake closely to ensure you are not dropping below minimum thresholds. The broader semaglutide diet guide covers multiple dietary approaches and their compatibility with GLP-1 therapy, helping you find the framework that works best for your body and preferences.
Side effects that indirectly cause stalls
Some GLP-1 side effects do not directly cause stalls but create conditions where stalls become more likely. Dizziness on semaglutide or lightheadedness can reduce physical activity, which reduces calorie burn. Diarrhea on tirzepatide can cause dehydration and electrolyte imbalances that promote water retention. Sulfur burps and other GI side effects can make eating sufficient protein difficult, accelerating lean mass loss.
Addressing side effects is not just about comfort. It is about removing barriers to the behaviors, adequate protein, regular exercise, proper hydration, and sufficient sleep, that prevent and resolve stalls. Understanding when side effects appear helps you anticipate and manage them proactively.
Hair loss during stalls
One side effect that concerns many GLP-1 users, particularly during or after stalls, is hair thinning. GLP-1-related hair loss is typically telogen effluvium, triggered by the physiological stress of rapid weight loss and caloric restriction. It usually resolves within 3 to 6 months once weight stabilizes or the nutritional deficit is corrected. Retatrutide and hair loss follow similar patterns.
Adequate protein, iron, biotin, and zinc intake can help minimize this effect and support hair recovery during and after a stall period.
The maintenance mindset: stalls as training for maintenance
Here is a perspective shift that most GLP-1 content overlooks entirely.
A stall is actually practice for maintenance.
When you eventually reach your goal weight, or when you and your provider decide to transition to a GLP-1 maintenance dose, the skills you develop during stalls, adjusting protein, maintaining exercise, managing sleep, monitoring hydration, and tolerating the scale not moving, are exactly the skills you will need for long-term weight maintenance. Every stall you navigate successfully builds the behavioral toolkit that prevents regain.
Maintaining weight loss after tirzepatide is the ultimate challenge, and it is the chapter that comes after your weight loss journey, not during it. But the stall is where you rehearse. The people who navigate stalls most successfully, who do not panic, who make measured adjustments, who trust the process, are the people who maintain their results long-term.
Understanding the process of weaning off tirzepatide or adjusting doses downward becomes relevant here. Some users also explore what happens when they stop tirzepatide abruptly versus tapering gradually. The choice between these approaches can affect whether weight regain occurs and how severe it is. Semaglutide withdrawal symptoms and their management are part of this broader conversation about long-term GLP-1 strategy.
Monitoring your progress during a stall
When the scale stops being a useful metric, you need other tools.
Body measurements
Measure your waist at the navel, hips at the widest point, chest at the nipple line, and thighs at the midpoint. Record these weekly, same day, same time, same level of hydration. Many people in a scale stall are still losing inches, because body recomposition, fat loss paired with muscle maintenance or gain, can occur with zero change in total weight.
Progress photos
Take front, side, and back photos in the same lighting, same clothing, same time of day, every two weeks. The mirror adapts to gradual change. Photos do not. Comparing a stall-start photo with a stall-end photo often reveals visible changes that the scale completely missed.
Performance metrics
If you are resistance training, track your lifts. Increasing strength during a stall is strong evidence that you are building or maintaining muscle while losing fat, the best possible scenario even though the scale does not reflect it. Muscle growth support through proper nutrition and training can continue even during a weight loss stall.
Lab work
Periodic blood work provides objective metabolic data that the scale cannot. HbA1c, fasting insulin, lipid panels, thyroid function, and inflammatory markers all tell a story about your metabolic health trajectory that is independent of scale weight. Semaglutide and blood work or tirzepatide and blood work considerations are worth understanding so you can interpret results accurately.
Energy and mood tracking
Rate your energy and mood on a 1-10 scale daily. Improvements in these metrics during a stall confirm that positive metabolic changes are occurring beneath the surface. Semaglutide and energy levels and tirzepatide and energy levels are highly individual, but tracking them provides useful data for evaluating your overall response to therapy.
How semaglutide makes you feel overall, beyond just weight on the scale, is part of evaluating whether your treatment is working even during a stall.
When to talk to your provider
Not every stall requires medical intervention. Most resolve with the lifestyle adjustments outlined above. But certain situations warrant a conversation with your prescribing provider sooner rather than later.
Contact your provider if your stall has lasted more than 8 weeks despite implementing all foundational protocols. Reach out if you are experiencing new or worsening side effects alongside the stall. Contact them if you have significant fatigue, brain fog, or mood changes that suggest a nutritional deficiency or hormonal issue. Reach out if you are at the maximum approved dose and have significant weight remaining to lose. And contact them immediately if you notice signs of more serious complications, including severe abdominal pain, persistent vomiting, or symptoms suggestive of pancreatitis or gallbladder issues.
Your provider can order labs to check thyroid function, metabolic markers, and nutritional status. They can evaluate whether a dose adjustment, medication switch, or adjunctive therapy is appropriate. And they can help you distinguish between a stall that will resolve with patience and one that requires pharmacological adjustment.
Understanding GLP-1 qualification criteria and BMI requirements for GLP-1 therapy can also be relevant if you are considering switching medications or adjusting your treatment plan. Insurance coverage through plans like Anthem or Blue Cross Blue Shield may affect your options for medication changes.
For those exploring compounded options, the GLP-1 purchasing guide provides context on sourcing considerations, and tools like the peptide cost calculator can help evaluate the financial implications of different medication approaches. The peptide reconstitution calculator is useful for those working with compounded lyophilized formulations, and the general peptide calculator can assist with dosing conversions.
Understanding the comparative landscape through resources like the semaglutide versus tirzepatide comparison can inform your conversation with your provider about potential medication switches or adjustments. The relationship between GLP-1 and brand-name medications is also worth understanding to navigate these discussions effectively.
A practical stall-breaking checklist
Use this checklist systematically. Address items in order. Give each intervention 2 to 3 weeks before adding the next. Do not change everything simultaneously, because you need to identify which factors are actually driving your stall.
Week 1-2: Foundations
Calculate and track protein intake. Hit 0.6-0.75g per pound of goal weight daily.
Ensure caloric intake is above 1,200 (women) or 1,400 (men).
Drink half your body weight in ounces of water daily.
Add a fiber supplement if bowel movements are less than daily.
Begin taking body measurements weekly.
Week 3-4: Activity
Start or increase resistance training to 2-3 sessions per week.
Add 20-30 minutes of daily walking if not already active.
Prioritize 7-9 hours of sleep. Address any insomnia.
Add electrolyte supplementation.
Week 5-6: Fine-tuning
Eliminate alcohol entirely for 4 weeks.
Review dietary composition. Reduce ultra-processed foods.
Consider targeted supplements (creatine, L-carnitine, B12).
Experiment with injection timing if applicable.
Week 7-8: Provider involvement
If stall persists, schedule appointment with prescribing provider.
Request thyroid, metabolic, and nutritional lab work.
Discuss dose adjustment or medication switch.
Evaluate whether a calorie cycling protocol is appropriate.
The semaglutide tips guide and the GLP-1 fat loss treatment overview provide additional context for optimizing your protocol during each phase of this checklist.
Whether tirzepatide increases metabolism directly, or simply creates the conditions for metabolic improvement through weight loss and body composition changes, is a question that researchers continue to investigate. What is clear is that active, strategic management of your protocol, rather than passive waiting, produces the best outcomes during stall periods.
Frequently asked questions
How long does a typical GLP-1 stall last?
Most GLP-1 stalls last 2 to 8 weeks. Some last longer, particularly after substantial weight loss of 15% or more of starting body weight. Stalls that persist beyond 8 weeks despite implementing all foundational lifestyle adjustments, including adequate protein, resistance training, proper hydration, sufficient sleep, and caloric floors, warrant a conversation with your provider about dose adjustment or medication changes. The duration depends heavily on the underlying cause, which is why systematic troubleshooting is more productive than simply waiting.
Is a GLP-1 stall different from a weight loss plateau?
The terms are used interchangeably in most contexts, and the underlying physiology is the same. In this guide, "stall" and "plateau" both refer to a period of 3 or more weeks where weight loss has stopped despite continued medication use and adherence to dietary protocols. Some clinicians use "plateau" to describe the eventual leveling off at maximum weight loss (around 24 months for most GLP-1 medications) and "stall" for temporary pauses that occur during the active weight loss phase. Both involve adaptive thermogenesis, hormonal recalibration, and appetite feedback adjustments. The semaglutide plateau guide covers the semaglutide-specific version of this experience in greater detail.
Can eating too few calories cause a GLP-1 stall?
Yes. This is one of the most common and most counterintuitive causes. Severe caloric restriction below 1,000 to 1,200 calories daily triggers an aggressive metabolic conservation response that can halt weight loss even in the presence of a large theoretical calorie deficit. The body reduces resting metabolic rate, decreases non-exercise activity thermogenesis, downregulates thyroid function, increases cortisol, and promotes water retention. Increasing intake to a sustainable floor of 1,200 to 1,500 calories from nutrient-dense, protein-forward foods often restarts weight loss within 1 to 3 weeks.
Should I increase my GLP-1 dose during a stall?
If you are not at the maximum dose of your medication, a dose increase is a reasonable discussion to have with your provider, particularly if lifestyle factors have been optimized. However, dose increases should not be the first intervention for a stall. Address protein intake, resistance training, sleep, hydration, and constipation first. If those factors are all optimized and the stall persists for 4 or more weeks, a dose increase may be appropriate. If you are already at the maximum dose, other strategies including medication switches or adjunctive therapies become the focus.
Why did my weight loss stall after switching from semaglutide to tirzepatide?
A temporary stall during a medication switch is normal and expected. Your body needs 2 to 4 weeks to adjust to the new medication pharmacokinetics, receptor engagement profile, and steady-state blood levels. The medication switching guide covers what to expect during transitions. In most cases, weight loss resumes once the new medication reaches therapeutic levels and the body adapts to the different receptor activation pattern. If the stall persists beyond 6 weeks after switching, consult your provider.
Does exercise help break a GLP-1 stall?
Resistance training is one of the most effective stall-breaking interventions available. It preserves lean mass, which maintains metabolic rate, and the acute metabolic effects of resistance exercise, including excess post-exercise oxygen consumption, contribute additional calorie burn. Cardiovascular exercise also helps, primarily through direct calorie expenditure and improvements in insulin sensitivity, but it is less effective than resistance training at preserving the muscle mass whose loss contributes to stalls. The ideal approach combines both: 2-3 resistance sessions and 150+ minutes of moderate cardiovascular activity per week.
Can constipation really make it look like I have stalled?
Absolutely. Stool can weigh 3 to 5 pounds or more, and GLP-1 medications slow gastric and intestinal motility as part of their mechanism of action. A person who has not had a complete bowel movement in several days may be carrying enough additional weight to completely mask ongoing fat loss. Resolving GLP-1-related constipation through fiber supplementation, hydration, magnesium, and physical activity can produce a dramatic "drop" on the scale that represents the unmasking of fat loss that was happening all along.
How much protein do I really need during GLP-1 therapy?
The research-supported minimum is 1.2 grams per kilogram of body weight per day. The optimal range for muscle preservation during active weight loss is 0.6 to 0.75 grams per pound of goal body weight. For a person targeting 160 pounds, that means 96 to 120 grams of protein daily. This target does not change during a stall, in fact, meeting it consistently becomes even more important during a stall because muscle preservation is the primary lever you have for maintaining metabolic rate. The protein guide for semaglutide users provides specific meal-by-meal strategies for hitting these targets.
What happens if I just wait out the stall without changing anything?
Some stalls do resolve spontaneously as hormonal and metabolic systems recalibrate to a new equilibrium. However, waiting passively is a gamble. If the stall is driven by progressive muscle loss or severe caloric restriction, waiting will make the problem worse, not better, because the metabolic adaptations continue to compound. The safest approach is to implement the foundational protocols, including protein, resistance training, hydration, and sleep optimization, regardless of whether you believe the stall will resolve on its own. These interventions carry no downside risk and significant upside potential.
Is my metabolism permanently damaged from the stall?
No. Adaptive thermogenesis is a reversible physiological response, not permanent metabolic damage. When you increase caloric intake toward maintenance, your metabolic rate recovers, though the timeline varies. Resistance training accelerates metabolic recovery by rebuilding or preserving metabolically active tissue. The concept of permanent metabolic damage has been largely debunked by controlled research, though it remains a persistent myth in weight loss communities. Your metabolism is adaptive, which means it adapted downward during weight loss and it will adapt upward when conditions change.
External resources
PMC: The physiology of weight loss plateaus during obesity pharmacotherapy, a comprehensive analysis of metabolic adaptation mechanisms during GLP-1 receptor agonist therapy, including appetite feedback coefficients and energy expenditure changes.
PubMed: Physiology of the weight loss plateau, detailing the quantitative relationships between weight lost, metabolic adaptation, and the timeline of plateau onset across different intervention types.
The American Journal of Medicine: Mechanisms of GLP-1 receptor agonist weight loss, covering the pharmacological and physiological pathways through which GLP-1 medications produce weight reduction and the mechanisms that eventually limit that reduction.
New England Journal of Medicine: GLP-1 Receptor Agonists, a comprehensive review of GLP-1 receptor agonist pharmacology, clinical outcomes, and emerging therapeutic applications from one of the most respected medical journals in the world.
Members of SeekPeptides access detailed stall-breaking protocols, dose adjustment frameworks, and a community of people navigating the same challenges you are facing right now. When the scale stops moving, having access to structured troubleshooting guides, provider-reviewed protocols, and real-time community support from people who have broken through their own stalls can make the difference between giving up and finding your next breakthrough. The stall is not the end of your progress. It is the beginning of a more strategic, informed approach to reaching your goals.
In case I do not see you, good afternoon, good evening, and good night. May your stalls stay temporary, your muscle stay intact, and your protocols stay optimized.