Mar 23, 2026

Some women on hormone replacement therapy lose weight effortlessly when they add a GLP-1 medication. Others see no difference at all. And a small group actually experiences reduced hormone levels because nobody warned them about one critical interaction.
The difference between these outcomes comes down to understanding how these two therapies interact at a biological level, and making one simple adjustment that most providers overlook.
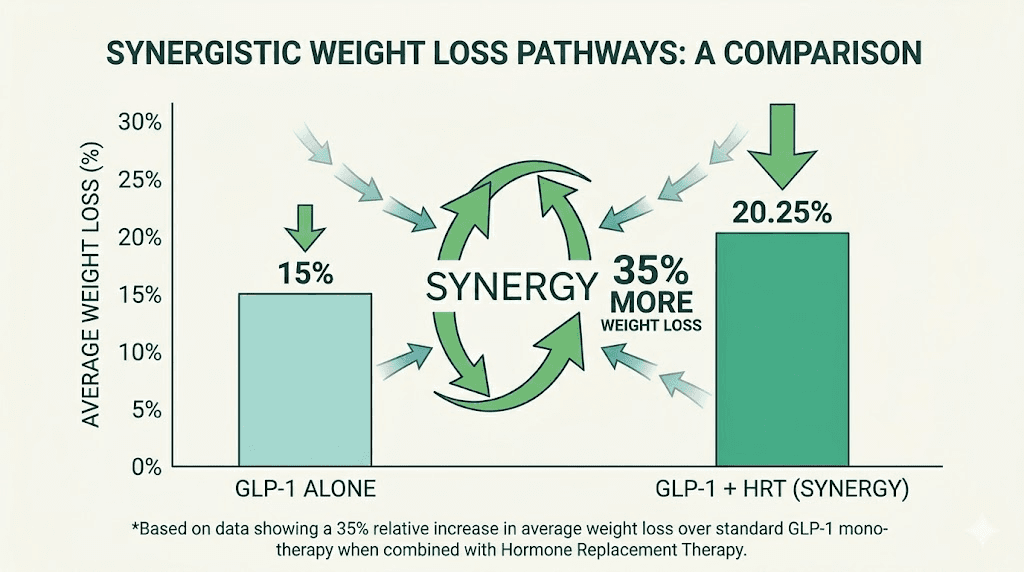
A Mayo Clinic study found that postmenopausal women using menopausal hormone therapy alongside tirzepatide lost approximately 35% more weight than women taking tirzepatide alone. That is not a marginal improvement. That is the difference between losing 20 pounds and losing 27. Between fitting into last year clothes and buying a whole new wardrobe. Between feeling like the medication is "working okay" and feeling like it has genuinely changed your life.
But here is what that headline does not tell you. GLP-1 medications slow gastric emptying. That means oral hormones, including oral estrogen and oral progesterone, may not absorb properly. Tirzepatide was shown to reduce oral contraceptive absorption by approximately 60%. If you are taking oral HRT with a GLP-1 and nobody adjusted your delivery method, you could be getting significantly less hormone than you think.
This guide covers everything you need to know about combining HRT and GLP-1 medications safely. We will walk through the research on semaglutide and tirzepatide with both female and male hormone replacement, the absorption problem with oral delivery, why transdermal hormones solve it, what the latest studies say about synergistic weight loss, and how to work with your provider to optimize both therapies simultaneously. SeekPeptides members get access to detailed protocol guides that cover these combinations in depth, but this article gives you the foundation you need to have an informed conversation with your healthcare team.
Understanding HRT and GLP-1 medications
Before exploring how these therapies work together, it helps to understand what each one does independently. Hormone replacement therapy and GLP-1 receptor agonists target completely different systems in the body. That is precisely why they complement each other so well.
What is HRT?
Hormone replacement therapy replaces hormones that the body stops producing adequately, typically during menopause or andropause. For women, this usually means estrogen, progesterone, or both. For men, it means testosterone. The goal is to restore hormonal balance and address symptoms like hot flashes, night sweats, mood changes, bone density loss, fatigue, and that frustrating redistribution of body fat that seems to happen overnight.
HRT comes in several delivery formats. Oral tablets. Transdermal patches. Topical gels and creams. Pellets implanted under the skin. Vaginal rings or suppositories. Intramuscular injections. Each delivery method has different absorption characteristics, and this distinction becomes critically important when you add a GLP-1 medication to the mix.
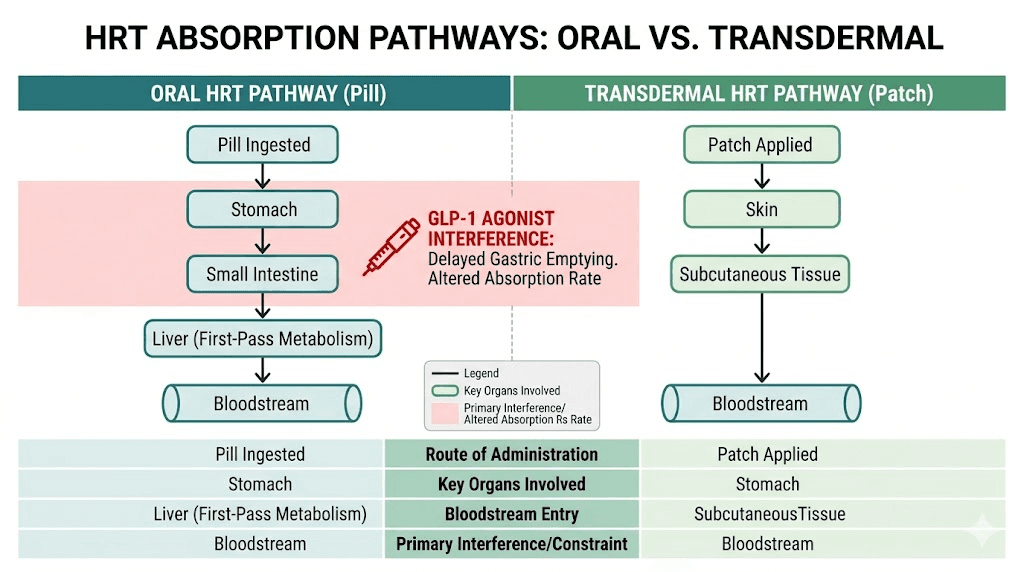
The choice of delivery method matters more than most people realize. Oral estrogen passes through the liver first, a process called first-pass metabolism. Transdermal delivery bypasses the liver entirely and enters the bloodstream directly through the skin. This pharmacokinetic difference has implications for clotting risk, blood clot concerns, and, as we will discuss in detail, drug absorption when combined with medications that slow your digestive system.
What are GLP-1 receptor agonists?
GLP-1 receptor agonists mimic a hormone called glucagon-like peptide-1 that your body produces naturally in the gut after eating. This hormone tells your brain you are full, slows the rate at which food leaves your stomach, and helps regulate blood sugar levels. The pharmaceutical versions, semaglutide and tirzepatide, are significantly more potent and longer-lasting than the natural hormone.
Semaglutide activates GLP-1 receptors. Tirzepatide activates both GLP-1 and GIP receptors, giving it a dual mechanism. Retatrutide, the newest entry, activates three receptors: GLP-1, GIP, and glucagon. Each generation offers potentially greater fat loss treatment effects.
The weight loss from these medications is substantial. Clinical trials show 15-22% total body weight loss with tirzepatide and 12-17% with semaglutide over 72 weeks. But here is the catch that matters for HRT users: these medications significantly slow gastric emptying. Food sits in your stomach longer. So do oral medications.
Why people combine them
The reasons are straightforward. Menopause and low testosterone both promote weight gain, particularly visceral fat around the abdomen. HRT addresses the hormonal root cause. GLP-1 medications address appetite and metabolic function. Together, they attack the problem from two completely different angles.
During the menopausal transition, up to 70% of women gain weight. Falling estrogen levels shift fat storage from the hips and thighs to the abdominal area. This visceral fat wraps around organs and increases the risk of type 2 diabetes, fatty liver disease, and cardiovascular problems. HRT can slow or reverse this shift. GLP-1 medications can dramatically accelerate weight loss per month. The combination addresses both the hormonal trigger and the metabolic consequence.
For men, the story is similar but involves testosterone. Low testosterone promotes fat accumulation, reduces muscle mass, and decreases metabolic rate. Tirzepatide and testosterone together can help men lose fat while preserving the muscle that testosterone supports. Without testosterone replacement, GLP-1 medications alone may cause 15-40% of weight loss to come from lean mass rather than fat.
The research: what the studies actually show
The evidence supporting the combination of HRT and GLP-1 medications has grown substantially. These are not theoretical benefits. Multiple studies now demonstrate measurably better outcomes when the therapies are combined.
The Mayo Clinic tirzepatide study
Researchers at Mayo Clinic published findings showing that postmenopausal women receiving menopausal hormone therapy lost approximately 35% more weight while taking tirzepatide compared to women taking tirzepatide without hormone therapy. The study, led by Dr. Regina Castaneda, found that women on both therapies achieved nearly 20% total body weight loss, while those on tirzepatide alone achieved closer to 15%.
That five percentage point difference might sound small in abstract terms. On a 200-pound woman, it represents the difference between losing 30 pounds and losing 40 pounds. Ten additional pounds of fat loss from the same medication, simply because hormonal balance was addressed simultaneously.
The researchers noted that hormone therapy may not only reduce visceral fat directly but also improve sleep quality, boost mood, and increase the likelihood of staying physically active. All of these factors contribute to sustainable weight loss over time.
Semaglutide and HRT studies
Similar findings emerged with semaglutide. Postmenopausal women who combined semaglutide with hormone therapy experienced approximately 30% greater weight loss than those using semaglutide alone. At every checkpoint, 3 months, 6 months, 9 months, and 12 months, women on combination therapy showed a higher percentage of total body weight loss.
A NewYork-Presbyterian study confirmed that women in menopause benefit from GLP-1 weight loss medications as much as younger women, dispelling the common concern that these medications might be less effective after menopause. When HRT was added, the results actually exceeded what younger women typically achieve with GLP-1 medications alone.
The week-by-week results were particularly telling. Women on combination therapy showed faster initial response, greater total weight loss at every time point, and better maintenance of muscle mass compared to the GLP-1-only group.
The biological mechanism behind the synergy
This is not just a happy coincidence. There is a genuine biological mechanism at work.
Research published in Biochemical Pharmacology found that GLP-1 and estrogen share downstream signaling pathways. Despite binding to different receptors, their effects converge on protein kinases (PKA, PKB, PKC) and transcription factors like PPAR-gamma, a key regulator of lipid metabolism. In simpler terms, estrogen amplifies some of the metabolic effects that GLP-1 medications produce.
Even more interesting, estrogen and GLP-1 regulate each other reciprocally. Studies in ovariectomized mice showed that estrogen replacement increased GLP-1 release from both intestinal L-cells and pancreatic alpha-cells. More estrogen means more natural GLP-1 production. More GLP-1 means better metabolic regulation. The two hormones create a positive feedback loop that neither achieves alone.
Central estrogen receptor alpha (ER-alpha) signaling is necessary for GLP-1 to fully exert its effects on food-reward behavior. This interaction has been localized to specific brain regions: the supramammillary nucleus, the lateral hypothalamus, and the nucleus of the solitary tract. When estrogen levels are low, as they are in menopause, GLP-1 medications may not activate these reward-suppressing pathways as effectively.
This explains why some postmenopausal women feel that semaglutide does not suppress their appetite as strongly as expected. It may not be a problem with the medication. It may be a problem with their estrogen levels.
Testosterone and GLP-1 research
The data for men is equally compelling, though the mechanism differs.
An Endocrine Society study presented at ENDO 2025 found that anti-obesity medications, including semaglutide and tirzepatide, can normalize testosterone levels in men. Among men who were not on testosterone replacement therapy, the proportion with normal total and free testosterone rose from 53% to 77% after achieving approximately 10% weight loss with GLP-1 medications.
That finding has significant implications. Fat tissue converts testosterone to estrogen through an enzyme called aromatase. More body fat means more aromatase activity, which means lower testosterone. By reducing fat mass, GLP-1 medications can naturally raise testosterone levels without exogenous replacement.
For men already on testosterone replacement therapy (TRT), adding a GLP-1 medication provides complementary benefits. Testosterone directly stimulates muscle protein synthesis, particularly fast-twitch muscle fibers. GLP-1 medications primarily drive fat loss. Together, they can help men achieve body recomposition rather than simple weight loss, losing fat while maintaining or even gaining muscle.
Successful combination therapy requires adequate protein intake, typically 1.6-2.2 grams per kilogram of body weight, and consistent resistance training to protect muscle mass. Our guide on how much protein on semaglutide covers the nutritional requirements in detail.
The oral absorption problem nobody talks about
This is the section that could save your hormone therapy from failing.
GLP-1 medications slow gastric emptying. That is how they reduce appetite and help with weight loss. But delayed gastric emptying also affects how oral medications are absorbed. And oral HRT is one of the most commonly prescribed hormone delivery methods.
How GLP-1 medications affect oral drug absorption
When you take an oral medication, it travels to your stomach, dissolves, moves to the small intestine, and gets absorbed into your bloodstream. GLP-1 receptor agonists slow this entire process. Food and medications sit in the stomach longer than normal.
Studies measuring acetaminophen absorption, a standard marker for gastric emptying rate, found that GLP-1 receptor agonists reduced peak plasma concentration (Cmax) by 13-56%. That means any oral medication you take alongside a GLP-1 may reach lower peak levels in your blood.
For most medications, this delay is clinically insignificant. The total amount absorbed remains roughly the same. It just takes longer. But for some medications, including certain hormones, the rate of absorption matters as much as the total amount.
The tirzepatide and oral contraceptive data
The most striking evidence comes from tirzepatide clinical trials. Tirzepatide was found to significantly reduce oral contraceptive pharmacokinetics by approximately 60%. This finding was significant enough that the tirzepatide drug label now advises patients using oral hormonal contraceptives to switch to or add a non-oral contraceptive method when initiating tirzepatide and after each dose escalation.
If tirzepatide can reduce oral contraceptive absorption by 60%, it can affect oral HRT absorption as well. The mechanism is identical: delayed gastric emptying reducing the rate and potentially the extent of oral hormone absorption.
Which HRT delivery methods are affected
Affected by GLP-1 medications (oral delivery):
Oral estrogen tablets (conjugated equine estrogens, estradiol)
Oral progesterone (micronized progesterone, such as Utrogestan)
Oral progestins (norethisterone, medroxyprogesterone)
Oral testosterone (testosterone undecanoate)
NOT affected by GLP-1 medications (non-oral delivery):
Transdermal estrogen patches
Topical estrogen gels and creams
Vaginal estrogen rings or suppositories
Progesterone-releasing IUD (Mirena)
Transvaginal progesterone
Testosterone injections
Testosterone pellets
Testosterone patches or gels
The distinction is simple. Anything that goes through your digestive system can be affected. Anything that bypasses your digestive system cannot.
The progesterone safety concern
This is where things get serious. Oral progesterone in HRT serves a critical safety function: it protects the uterine lining (endometrium) from the effects of unopposed estrogen, which can lead to endometrial hyperplasia and potentially cancer.
If GLP-1 medications reduce oral progesterone absorption, the endometrial protection could be compromised. The British Menopause Society has highlighted this concern, noting that while there is currently no robust data showing that GLP-1 receptor agonists definitively affect oral progestogen dosing requirements, bleeding patterns, or endometrial risk, the theoretical concern is valid and warrants monitoring.
Clinical guidance from NHS Lothian suggests that if you are on oral progesterone and starting a GLP-1 medication, it may be logical to increase the dose from 100 mg daily to 200 mg daily for the first 4 weeks of GLP-1 treatment, after which the gastroparesis risk typically diminishes at a stable dose. Alternatively, switching to non-oral progesterone delivery (Mirena IUD or transvaginal progesterone) eliminates the concern entirely.
The practical solution: switch to transdermal HRT
The simplest way to avoid the absorption problem is to use non-oral hormone delivery. Transdermal HRT, meaning patches or gels, bypasses the digestive system entirely. The hormones absorb directly through the skin into the bloodstream. Semaglutide and tirzepatide cannot affect this pathway because the hormones never enter the stomach.
Transdermal estrogen also carries additional benefits independent of GLP-1 compatibility. It avoids first-pass liver metabolism, which means lower risk of blood clots and a better lipid profile compared to oral estrogen. Many endocrinologists already prefer transdermal delivery for these reasons alone.
If switching delivery methods is not possible, discuss with your provider about timing your oral HRT and GLP-1 injections to minimize overlap. Taking oral hormones several hours before or after your GLP-1 injection may help, though the gastroparesis effect persists throughout the week with weekly formulations.
HRT and GLP-1 for women during menopause
Menopause and weight gain are so tightly linked that most women consider them inseparable. They are not. But addressing menopause-related weight gain requires understanding why it happens and attacking it from multiple angles simultaneously.
Why menopause makes weight loss harder
Declining estrogen changes where and how your body stores fat. Before menopause, women tend to accumulate subcutaneous fat in the hips and thighs. After menopause, fat shifts to the abdomen, particularly the visceral compartment surrounding the organs. This visceral fat is metabolically active, inflammatory, and resistant to traditional weight loss approaches.
Estrogen also influences GLP-1 receptor sensitivity. As we discussed, central estrogen receptor signaling is necessary for GLP-1 to fully suppress food-reward behavior. With declining estrogen, your brain responds less robustly to the satiety signals that GLP-1 medications are designed to amplify. This may explain why some menopausal women report feeling still hungry on tirzepatide or not losing weight on semaglutide.
Muscle mass declines during menopause, which reduces basal metabolic rate. Sleep quality deteriorates, which affects hunger hormones. Mood changes can drive emotional eating. The entire metabolic environment shifts against you.
How the combination addresses each factor
HRT addresses the root cause by restoring estrogen levels. This shifts fat storage patterns back toward a healthier distribution, improves sleep, stabilizes mood, and, critically, restores GLP-1 receptor sensitivity in the brain.
GLP-1 medications address the metabolic consequence by reducing appetite, slowing gastric emptying, and improving insulin sensitivity. Tirzepatide does not just suppress appetite. It actually improves metabolic function at a cellular level.
Together, HRT and GLP-1 create what researchers describe as a synergistic therapeutic effect. The whole is genuinely greater than the sum of its parts.
Perimenopause considerations
Perimenopause presents unique challenges because hormone levels fluctuate unpredictably. One month estrogen may be high, the next it crashes. These fluctuations can affect GLP-1 medication effectiveness, causing periods of strong appetite suppression followed by periods where the medication seems to stop working.
Women in perimenopause may benefit from peptides for perimenopause alongside their GLP-1 protocol. Stabilizing hormones during this transitional period can help maintain consistent GLP-1 responses. Our guide on peptides for menopause covers additional options for this stage.
Semaglutide can affect your period, and tirzepatide can affect your period as well. Weight loss itself changes hormone levels, which can alter menstrual patterns. If you are in perimenopause and using a GLP-1, track your cycles carefully and discuss any changes with your provider.
Choosing the right GLP-1 for menopausal women
Both semaglutide and tirzepatide are effective for menopausal weight loss. The Mayo Clinic data specifically showed benefits with tirzepatide, while other studies demonstrated similar benefits with semaglutide. The choice often depends on individual response, side effect tolerance, and provider preference.
Semaglutide versus tirzepatide side effects may differ in menopausal women compared to the general population. Some women find that one medication causes more fatigue, bloating, or constipation than the other. Since menopause itself can cause similar symptoms, finding the right combination requires patience and careful monitoring.
If semaglutide is not working, tirzepatide may be more effective due to its dual receptor mechanism. The conversion chart from semaglutide to tirzepatide can guide your provider through the transition.
HRT and GLP-1 for men: testosterone replacement and weight loss
The conversation about HRT and GLP-1 is not exclusively about menopause. Men with low testosterone face a remarkably similar metabolic trap, and the combination approach works for them too.
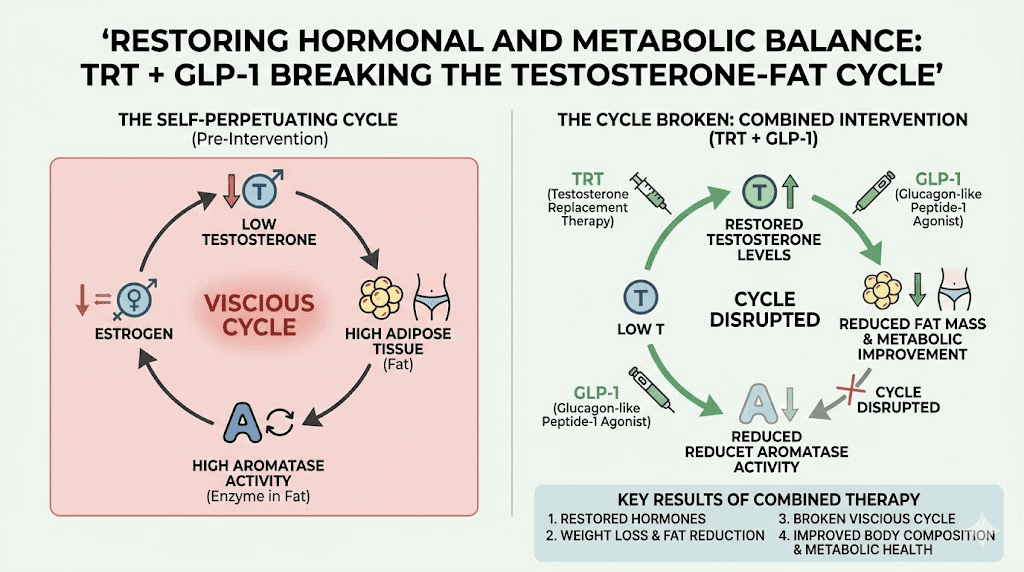
The testosterone and body fat cycle
Low testosterone and excess body fat create a vicious cycle. Fat tissue contains aromatase, an enzyme that converts testosterone into estrogen. More body fat means more aromatase activity, which means lower testosterone and higher estrogen in men. Lower testosterone further promotes fat storage, which further increases aromatase activity. The cycle feeds itself.
This is why many men with obesity also have low testosterone, a condition sometimes called hypogonadal obesity. Breaking the cycle requires addressing both the hormonal deficit and the excess fat simultaneously.
How TRT and GLP-1 complement each other
Testosterone replacement therapy provides the hormonal foundation. It increases muscle protein synthesis, improves energy levels, enhances mood, and shifts body composition toward more muscle and less fat. But TRT alone is not a powerful weight loss tool. It changes body composition gradually.
GLP-1 medications provide the aggressive fat loss component. They reduce appetite, improve insulin sensitivity, and promote significant weight loss. But without adequate testosterone, a substantial portion of that weight loss, potentially 15-40%, comes from muscle rather than fat.
When combined, testosterone protects and builds muscle while GLP-1 medications drive fat loss. The result is genuine body recomposition: less fat, more muscle, better metabolic health. Men using peptides for weight loss and muscle gain often achieve the best results with this combined approach.
Interestingly, GLP-1 medications can improve testosterone levels on their own by reducing body fat. The Endocrine Society research showed that men who lost 10% of body weight with GLP-1 medications saw their normal testosterone proportion rise from 53% to 77%, without any testosterone supplementation. For men with mildly low testosterone, rapid weight loss on semaglutide or tirzepatide may be enough to normalize levels without needing TRT.
Practical considerations for men
Unlike women, men rarely use oral testosterone (the oral form has bioavailability issues independent of GLP-1 effects). Most men receive testosterone via intramuscular injection, topical gel, or subcutaneous pellets. None of these delivery methods are affected by GLP-1-induced gastroparesis, so the absorption concern that affects women on oral HRT does not apply to most men on TRT.
The tirzepatide and testosterone combination is particularly popular because tirzepatide provides stronger weight loss than semaglutide, and the dual receptor mechanism may better preserve lean mass. Our guide on peptides versus TRT explores the differences between these approaches.
Men combining TRT and GLP-1 should monitor their hematocrit levels, as both weight loss and testosterone can affect red blood cell production. Regular blood work every 3-4 months helps catch any issues early. Semaglutide does show up in blood work if specifically tested, and so does tirzepatide, so inform all your providers about every medication you are taking.
Safety profile: is combining HRT and GLP-1 safe?
The short answer is yes, with appropriate monitoring. The British Menopause Society confirms there is no official contraindication to using GLP-1 receptor agonists concurrently with hormone replacement therapy. But "safe" and "optimal" are different things, and a few considerations deserve attention.
No known direct drug interactions
GLP-1 medications and hormone therapies do not directly interact at the receptor or enzyme level. They work through completely different pathways. There is no pharmacodynamic interaction where one medication amplifies or blocks the effects of the other in a dangerous way.
The only interaction of concern is pharmacokinetic: the delayed gastric emptying affecting oral hormone absorption. This is a delivery problem, not a drug interaction, and it is solved by using non-oral hormone delivery methods.
Overlapping side effects to monitor
Some side effects overlap between HRT and GLP-1 medications, which can make it difficult to identify which medication is causing a particular symptom.
Nausea: Both GLP-1 medications and, less commonly, HRT can cause nausea. GLP-1 nausea is usually worst during dose escalation and improves with time. HRT nausea is more common with oral delivery. If nausea is severe, consider whether the timing of side effects correlates with one medication over the other.
Headaches: Both therapies can cause headaches. GLP-1 headaches tend to occur early in treatment and resolve. HRT headaches may be related to hormone levels and require dose adjustment.
Fatigue: Menopause causes fatigue. GLP-1 medications can cause GLP-1 fatigue. And caloric restriction from appetite suppression can cause fatigue. Distinguishing the source requires careful observation and sometimes trial periods where one variable is adjusted at a time.
Mood changes: Both hormone fluctuations and GLP-1 medications can affect mood. Tirzepatide can cause anxiety in some users, and hormone imbalances can do the same. If mood changes are significant, work with your provider to determine whether hormones or GLP-1 dosing need adjustment.
Gastrointestinal issues: GLP-1 medications commonly cause constipation, bloating, and sulfur burps. HRT generally does not cause these symptoms unless oral delivery is irritating the stomach. If GI symptoms are severe, ensure your supplements and GLP-1 are not compounding the problem.
Cardiovascular considerations
Oral estrogen slightly increases the risk of venous thromboembolism (blood clots). Transdermal estrogen does not carry this risk. GLP-1 medications have demonstrated cardiovascular benefits in clinical trials, including reduced risk of major cardiovascular events.
The combination may actually be cardiovascular-protective, particularly if transdermal estrogen is used. The metabolic improvements from GLP-1 medications (weight loss, improved insulin sensitivity, reduced inflammation) combined with the cardiovascular benefits of estrogen replacement create a favorable risk profile. However, individual risk factors like smoking, personal or family history of blood clots, or other cardiovascular risk factors should be evaluated by your provider.
Bone health
This is an area where the combination may offer particular benefit. Estrogen is critical for bone density. Menopause-related estrogen decline accelerates bone loss and increases fracture risk. HRT directly addresses this by maintaining bone density.
Rapid weight loss, however, can also cause bone density loss. This is a known concern with GLP-1 medications, and tirzepatide and bone loss is an active area of research. By maintaining estrogen levels through HRT while losing weight with GLP-1 medications, you may protect bone density better than with GLP-1 medications alone.
Thyroid considerations
GLP-1 receptor agonists carry a boxed warning about thyroid C-cell tumors based on rodent studies. Women with Hashimoto disease and GLP-1 use need careful monitoring. If you have thyroid issues, tirzepatide and thyroid nodules require specific evaluation before starting combination therapy. HRT does not typically affect thyroid function, but oral estrogen can increase thyroid-binding globulin levels, potentially altering thyroid medication requirements.
Practical protocols: how to combine HRT and GLP-1 safely
Theory is useful. Practical implementation is what actually produces results. Here is how to approach combining these therapies.
Starting sequence
If you are starting both therapies simultaneously, most providers recommend establishing HRT first. Get hormones stable over 4-8 weeks before adding a GLP-1 medication. This approach has three advantages:
First, it establishes a hormonal baseline. You will know how HRT alone affects your symptoms, energy, sleep, and mood before adding another variable.
Second, stable hormone levels may improve your initial response to the GLP-1 medication. As we discussed, estrogen enhances GLP-1 receptor sensitivity. Starting GLP-1 after hormones are optimized may produce a stronger appetite-suppressing effect from the first dose.
Third, it simplifies side effect management. If you start both therapies simultaneously and develop nausea, headaches, or fatigue, you cannot determine which medication is responsible.
If you are already on stable HRT, you can add a GLP-1 medication following the standard starting dose protocol. Begin with the lowest dose and titrate up gradually.
Hormone delivery method optimization
Before starting a GLP-1 medication, evaluate your HRT delivery method:
If you are on oral HRT: Talk to your provider about switching to transdermal delivery (patches or gels) for estrogen, and either a Mirena IUD or transvaginal delivery for progesterone. This eliminates the absorption concern entirely.
If switching is not possible: Consider increasing oral progesterone from 100 mg to 200 mg daily for the first 4 weeks of GLP-1 treatment, per clinical guidance. Monitor for any changes in bleeding patterns, as this could indicate reduced progesterone effectiveness.
If you are on transdermal HRT: No changes needed. Your hormone delivery is unaffected by GLP-1 medications. Proceed with standard GLP-1 initiation.
If you are on testosterone injections or pellets (men): No changes needed. These bypass the digestive system entirely.
Dosing considerations
GLP-1 dosing follows standard titration protocols regardless of HRT status. Start low, increase gradually, and find the dose that provides adequate appetite suppression without intolerable side effects.
For semaglutide, the typical starting dose is 0.25 mg weekly, increasing to 0.5 mg, then 1.0 mg, and potentially 2.4 mg over several months. Check our semaglutide dosage in units guide and the semaglutide dosage calculator for precise measurements.
For tirzepatide, the starting dose is 2.5 mg weekly, increasing through 5 mg, 7.5 mg, 10 mg, 12.5 mg, and up to 15 mg. Our compounded tirzepatide dosage calculator helps determine exact syringe dosages.
HRT dosing should be managed by your endocrinologist or prescribing provider based on symptom control and hormone level testing. GLP-1 dosing should not require changes to HRT dosing, and vice versa, unless the oral absorption issue applies.
Monitoring schedule
When combining therapies, more frequent monitoring helps catch issues early:
Month 1: Baseline labs including hormones (estradiol, progesterone, testosterone, FSH), metabolic panel, lipids, thyroid function, and HbA1c. Begin GLP-1 at starting dose.
Month 2-3: Follow-up labs to check hormone levels while on GLP-1. This is particularly important if you are using oral HRT. Any significant drop in hormone levels suggests an absorption problem. Track your weekly results for weight loss trends.
Month 4-6: Reassess both therapies. Adjust GLP-1 dose if weight loss has plateaued. Adjust HRT if symptoms have changed. A semaglutide plateau may indicate that further dose increases or additional interventions are needed.
Ongoing: Every 3-4 months, repeat hormone panels and metabolic labs. Weight loss changes hormone levels. As body fat decreases, estrogen levels may shift (less aromatase activity), and HRT dosing may need adjustment.
Nutrition and lifestyle when combining HRT and GLP-1
Medications provide the foundation. But nutrition and lifestyle determine whether you get good results or great results.
Protein requirements become critical
Both menopause and GLP-1-induced weight loss put muscle mass at risk. When you are losing weight rapidly while simultaneously dealing with declining hormones that support muscle, protein intake becomes non-negotiable.
Aim for 1.2-1.6 grams of protein per kilogram of body weight at minimum. If you are on TRT and doing resistance training, increase to 1.6-2.2 grams per kilogram. Our guides on calories on semaglutide and calories on tirzepatide provide frameworks for maintaining adequate nutrition while appetite is suppressed.
Reduced appetite from GLP-1 medications makes hitting protein targets challenging. Protein shakes for GLP-1 users can help bridge the gap. Focus on complete proteins: eggs, fish, poultry, dairy, or plant-based alternatives with complete amino acid profiles.
Consider a semaglutide diet plan or tirzepatide diet plan that prioritizes protein at every meal. GLP-1 breakfast ideas and dinner ideas can help you maintain nutrition variety while meeting your targets.
Exercise and resistance training
Resistance training is not optional when combining HRT and GLP-1 medications. It is essential.
Without resistance training, up to 40% of weight loss can come from muscle mass. HRT provides hormonal support for muscle, but it cannot prevent muscle loss from caloric deficit and disuse. You need to actively stimulate muscle growth through progressive resistance training at least 3 times per week.
The combination of HRT, GLP-1 medications, adequate protein, and resistance training creates the optimal conditions for body recomposition. You lose fat aggressively while maintaining or building muscle. This is the difference between losing weight and transforming your body composition.
Concerned about losing weight on semaglutide without exercise? It is possible, but the quality of weight loss is significantly worse without resistance training, especially for HRT users whose muscle mass is already vulnerable.
Supplements that support both therapies
Several supplements can enhance outcomes when combining HRT and GLP-1:
Vitamin D: Essential for both bone health (particularly important with declining estrogen) and metabolic function. Most people on GLP-1 medications benefit from supplementation.
Calcium: Supports bone density alongside estrogen and vitamin D. Critical for menopausal women, especially during rapid weight loss.
Magnesium: Supports sleep quality, muscle function, and hormone metabolism. GLP-1 medications can deplete magnesium through changes in appetite and food intake.
Fiber: Helps manage GLP-1 gastrointestinal side effects and supports hormonal balance by aiding estrogen metabolism. Our guide on best fiber supplements for GLP-1 covers the best options.
Probiotics: Support gut health during GLP-1 treatment. Probiotics for semaglutide users may help reduce gastrointestinal side effects.
Check our comprehensive supplements to take with GLP-1 guide and the tirzepatide-specific supplements for tirzepatide guide for detailed recommendations.
Special considerations and edge cases
Breastfeeding and GLP-1 with hormones
Postpartum women sometimes seek GLP-1 medications for weight loss while using hormonal birth control. GLP-1 while breastfeeding is generally not recommended, and tirzepatide while breastfeeding has similar concerns. The combination of hormonal contraception and GLP-1 medications during breastfeeding should be discussed thoroughly with your obstetrician.
If oral contraception is being used and a GLP-1 medication is started, remember the ~60% absorption reduction finding from tirzepatide trials. Switching to a non-oral contraceptive method is strongly recommended to prevent unplanned pregnancy. Pregnancy on tirzepatide does occur, sometimes because oral contraceptive absorption was compromised.
Autoimmune conditions
Some autoimmune conditions, like Hashimoto thyroiditis and lupus, both affect hormone levels and may influence GLP-1 response. GLP-1 for Hashimoto disease requires careful thyroid monitoring, especially when HRT is involved.
Women with endometriosis and GLP-1 use should be aware that weight loss can affect estrogen levels and potentially influence endometriosis symptoms. GLP-1 and lipedema is another area where hormonal factors and weight loss intersect in complex ways.
Microdosing GLP-1 for autoimmune conditions is an emerging approach that some practitioners use alongside hormone therapy. The lower doses may provide anti-inflammatory benefits without the aggressive appetite suppression of full therapeutic doses.
Age-related considerations
For women over 40, the intersection of perimenopause, metabolic changes, and weight management becomes increasingly complex. Peptides for women over 40 may include both GLP-1 medications and other peptides that support hormonal balance.
Older adults (over 65) on HRT and GLP-1 should be particularly vigilant about muscle mass preservation. Age-related sarcopenia, hormone decline, and GLP-1-induced weight loss create a triple threat to lean mass. More aggressive protein intake and resistance training become essential.
Other medications and interactions
If you are combining HRT and GLP-1 with other medications, be aware that GLP-1 gastroparesis can affect any oral medication, not just hormones. Common interactions to discuss with your provider include:
Metformin and semaglutide or metformin and tirzepatide: often combined for diabetes management alongside HRT.
Phentermine and semaglutide or phentermine and tirzepatide: sometimes used short-term for aggressive weight loss, but the combination of three or four medications requires careful oversight.
Berberine and semaglutide or berberine and tirzepatide: natural supplements that may have additive effects on blood sugar regulation.
Wellbutrin and tirzepatide: sometimes combined when mood support and weight loss are both goals.
Estrogen and GLP-1: the deeper science
For those who want to understand the mechanism at a deeper level, the interplay between estrogen and GLP-1 signaling is one of the most fascinating areas of current metabolic research.
Shared signaling pathways
Estrogen and GLP-1 activate different receptors. Estrogen binds to estrogen receptors (ER-alpha and ER-beta). GLP-1 binds to the GLP-1 receptor (GLP-1R). But downstream of these receptors, their signaling cascades converge on several key pathways.
Both hormones activate protein kinases A, B, and C (PKA, PKB, PKC). Both influence the PPAR-gamma transcription factor, which regulates lipid metabolism. Both affect AMP-activated protein kinase (AMPK), a master metabolic regulator. These shared downstream targets explain why the two hormones have synergistic effects on metabolism even though they work through different initial receptors.
Reciprocal regulation
Perhaps most remarkably, estrogen and GLP-1 regulate each other. In ovariectomized mice (an animal model for menopause), estrogen replacement increased GLP-1 secretion from both intestinal L-cells and pancreatic alpha-cells. This means that restoring estrogen through HRT may actually increase your body natural GLP-1 production, amplifying the effects of exogenous GLP-1 medications.
Conversely, GLP-1 signaling influences estrogen receptor expression and activity. This bidirectional regulation suggests that the two systems evolved to work together, and that disrupting one (as happens in menopause) impairs the other.
Brain-level interactions
The interaction between estrogen and GLP-1 in the brain is particularly relevant for appetite control. GLP-1 acts on the nucleus of the solitary tract (NTS) and the hypothalamus to reduce food intake. Estrogen receptors in these same brain regions modulate GLP-1 receptor sensitivity.
When estrogen levels are adequate, GLP-1 signals are amplified. The appetite-suppressing effect is stronger. The food-reward pathways are more effectively dampened. When estrogen is low, as in menopause, GLP-1 signals may not reach their full potential.
Research on GLP-1/estrogen conjugate molecules, where GLP-1 and estrogen are chemically linked, shows even more dramatic effects. These conjugates act specifically in the supramammillary nucleus to reduce food-reward behavior and body weight. While these conjugates are experimental, they demonstrate the power of co-activating both pathways simultaneously.
This research provides a strong biological rationale for combining HRT and GLP-1 medications clinically. You are essentially recreating what the body does naturally in a pre-menopausal state: maintaining adequate estrogen signaling alongside robust GLP-1 activity.
Semaglutide and estrogen levels is a related question many women ask. While semaglutide does not directly increase estrogen, the weight loss it produces can reduce excess aromatase activity and normalize estrogen ratios, particularly in women who are carrying excess visceral fat.
Managing side effects when on both therapies
Side effect management is more nuanced when two therapies are running simultaneously. Here is a practical approach to the most common issues.
Nausea management
GLP-1 nausea typically peaks during the first few weeks at each new dose level. Standard management includes eating smaller meals, avoiding fatty or fried foods, staying hydrated, and taking acid reflux medication if needed.
If nausea is severe, do not assume it is only from the GLP-1 medication. Hormone fluctuations, particularly in perimenopause, can also cause nausea. If nausea correlates with your menstrual cycle or HRT dosing schedule rather than your GLP-1 injection day, the hormones may be contributing.
The best foods on semaglutide and the best foods on tirzepatide can help minimize GI distress. Bland, high-protein, moderate-fiber foods tend to be best tolerated.
Energy and fatigue
Semaglutide and energy is a common concern. Some people feel more energized on GLP-1 medications due to improved metabolic health. Others feel fatigued from reduced caloric intake. HRT typically improves energy levels, so the combination should theoretically be net positive for energy.
If fatigue is a problem despite being on both therapies, check that you are eating enough total calories and protein. Tirzepatide and energy depends heavily on maintaining adequate nutrition despite reduced appetite.
Sleep disruption
Menopause commonly disrupts sleep through hot flashes and night sweats. HRT addresses these symptoms directly. But semaglutide can cause insomnia and tirzepatide insomnia is also reported. If sleep quality worsens after starting a GLP-1 medication, consider timing your injection earlier in the day and ensuring your HRT dose is adequately controlling night sweats.
Hair loss
Both menopause and rapid weight loss can trigger telogen effluvium, a temporary form of hair shedding. GLP-1 and hair loss is a recognized side effect, though typically temporary. When combined with hormonal changes, the risk may be higher during the first 3-6 months.
Ensure adequate protein intake, consider biotin supplementation, and discuss with your provider whether HRT dose adjustments could help. Hair loss usually resolves within 6-12 months as the body adapts to its new weight and hormonal milieu.
Cold sensitivity
Tirzepatide and cold sensitivity and semaglutide and cold sensitivity are common complaints. Fat tissue provides insulation, and as you lose it, you feel colder. Thyroid function should be checked, especially in women with Hashimoto disease on HRT, as hypothyroidism also causes cold intolerance.
When to stop, pause, or adjust
Combination therapy is not set-and-forget. There are situations where adjustments are necessary.
Surgical considerations
If you are having surgery, discuss both medications with your surgical team. GLP-1 medications may need to be paused before surgery due to gastroparesis and aspiration risk. Resuming semaglutide after surgery follows specific guidelines. HRT decisions around surgery are typically made independently based on clot risk and the type of procedure.
Reaching your goal weight
What happens when you reach your target weight? Maintaining weight loss after tirzepatide often involves transitioning to a lower maintenance dose rather than stopping completely. Weaning off tirzepatide should be done gradually.
HRT decisions at goal weight depend on whether you still need hormonal support. Menopausal women typically continue HRT for symptom management regardless of weight. The GLP-1 medication may be reduced or discontinued while HRT continues at the same dose.
Stopping a GLP-1 medication too quickly can lead to semaglutide withdrawal symptoms, including rebound hunger and weight regain. A gradual taper over several months, combined with established exercise and nutrition habits, gives the best chance of maintaining results. The GLP-1 maintenance dose approach may be preferable to complete discontinuation.
Not seeing results
If you are on both HRT and a GLP-1 medication but not seeing expected results, several factors may be at play:
Check hormone levels. If you are on oral HRT and a GLP-1 medication, your hormone levels may be subtherapeutic due to the absorption issue we discussed. Switch to transdermal delivery.
Check GLP-1 dosing. You may need a higher dose. Refer to tirzepatide not working anymore for troubleshooting strategies.
Check caloric intake. Even with reduced appetite, some people unconsciously compensate with calorie-dense foods. Our semaglutide tips guide covers strategies for maximizing weight loss.
Check protein and exercise. Without adequate protein and resistance training, your body composition changes will be suboptimal regardless of medications.
Consider that 4 weeks without weight loss is not necessarily a failure. Some women, particularly those on HRT, experience body recomposition where they lose fat but gain muscle, resulting in stable or even slightly increased weight despite clear improvements in measurements and clothing fit.
Finding the right provider
Combining HRT and GLP-1 medications requires a provider who understands both endocrinology and metabolic medicine. Not all providers are equally comfortable managing this combination.
Ideally, look for a provider who prescribes both HRT and GLP-1 medications in their practice. They will understand the interactions, the monitoring requirements, and the nuances of optimizing both therapies simultaneously.
If your HRT provider does not prescribe GLP-1 medications, or vice versa, ensure that both providers communicate. Share lab results between them. Make sure both know about all medications you are taking.
Know what to say when requesting GLP-1 options. Come prepared with your current medications, lab results, BMI, and a clear explanation of your goals. If your provider is not familiar with the combination approach, you can reference the Mayo Clinic study and the British Menopause Society guidance.
Qualifying for semaglutide typically requires a BMI of 30 or higher (or 27 with a comorbidity). If your BMI is just under the threshold, the addition of HRT for documented hormonal deficiency may support your case for GLP-1 prescription.
For researchers serious about optimizing their protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed combination protocol guides, monitoring tools for home use, and expert-reviewed dosing recommendations that account for the HRT interaction.
Real-world combination scenarios
Understanding the research is one thing. Applying it to specific situations is another. Here are the most common scenarios people face when combining HRT and GLP-1 medications, along with guidance for each.
Scenario 1: Menopausal woman starting both therapies
You are 52, postmenopausal, experiencing hot flashes, sleep disruption, and a 30-pound weight gain concentrated around your midsection. Your doctor agrees that both HRT and a GLP-1 medication are appropriate.
The recommended approach starts with transdermal estrogen (patch or gel) plus either a Mirena IUD or transvaginal progesterone. Allow 6-8 weeks for hormones to stabilize. Monitor symptoms carefully during this period. Once hot flashes have improved, sleep is better, and hormone levels are confirmed in the therapeutic range, begin tirzepatide at the starting dose of 2.5 mg weekly.
During the first month on tirzepatide, expect some nausea and reduced appetite. These effects are normal. Focus on maintaining protein intake of at least 100 grams daily. Begin or continue resistance training at least three times per week. The first dose experience varies, but most women tolerate it well when hormones are already optimized.
After 4 weeks at 2.5 mg, increase to 5 mg if tolerated. Continue titrating upward every 4 weeks until appetite suppression is adequate. Most women find their effective dose between 7.5 mg and 12.5 mg. Check hormone levels at month 3 to confirm HRT is maintaining therapeutic levels. At this point, you should be seeing consistent weight loss of 3-5 pounds per month.
By month 6, expect 10-15% total body weight loss if following the combined protocol with adequate protein and exercise. The Mayo Clinic data suggests you may see up to 35% more weight loss than you would with tirzepatide alone, a difference that becomes increasingly significant over time.
Scenario 2: Man on TRT adding GLP-1
You are 45, on testosterone replacement therapy for diagnosed hypogonadism, and carrying 50 excess pounds of primarily visceral fat. Your endocrinologist recommends adding a GLP-1 medication to accelerate fat loss.
Since your testosterone is delivered via intramuscular injection or topical gel, there is no absorption interaction to worry about. You can begin semaglutide or tirzepatide immediately at the standard starting dose.
The key advantage for men on TRT is muscle preservation. Testosterone directly stimulates muscle protein synthesis, which counteracts the muscle loss that often accompanies rapid weight loss. But this protection is not automatic. You need to pair the medications with 1.6-2.2 grams of protein per kilogram of body weight daily, plus progressive resistance training at least four times per week.
Monitor hematocrit every 3 months. Both TRT and weight loss can affect red blood cell production. If hematocrit rises above 54%, discuss therapeutic phlebotomy or TRT dose adjustment with your provider.
An interesting possibility for men: as body fat decreases, natural testosterone production may increase. If you lose 10% or more of body weight, your provider may want to recheck testosterone levels off TRT to determine if you still need supplementation. Some men find that GLP-1 weight loss alone normalizes their testosterone enough to discontinue TRT.
Scenario 3: Perimenopausal woman on oral HRT switching to GLP-1
You are 47, in perimenopause, currently taking oral estradiol 1 mg daily and oral micronized progesterone 100 mg nightly. You want to start semaglutide for weight management.
This scenario requires the most careful planning because of the oral absorption issue. Before starting semaglutide, discuss switching your HRT delivery method with your provider. The ideal switch would be from oral estradiol to a transdermal estradiol patch (0.05-0.1 mg/day) and from oral progesterone to either a Mirena IUD or transvaginal progesterone capsules.
If switching is not possible or not preferred, a pragmatic approach involves increasing oral progesterone from 100 mg to 200 mg daily for the first 4-6 weeks of semaglutide treatment. After this period, the degree of gastroparesis typically stabilizes, and you may be able to return to 100 mg. Monitor for any unusual bleeding patterns, which could indicate insufficient endometrial protection.
Start semaglutide at 0.25 mg weekly and follow the standard titration schedule. The semaglutide syringe dosage chart will help with precise measurements. Check hormone levels at baseline and again at 8 weeks to ensure your oral HRT is maintaining therapeutic levels despite the GLP-1 effect on absorption.
Scenario 4: Already on GLP-1, considering adding HRT
You are 50, have been on tirzepatide for 6 months with good weight loss (down 35 pounds), but are experiencing increasing menopausal symptoms including hot flashes, night sweats, vaginal dryness, and mood changes. You are wondering if adding HRT would help.
You are already past the initial GLP-1 titration phase, so adding HRT is straightforward. Start with transdermal estrogen to avoid the absorption issue entirely. Your provider will determine the appropriate dose based on symptoms and lab work.
The interesting opportunity in this scenario is that adding HRT may actually boost your remaining weight loss. If you have hit a tirzepatide plateau, restoring estrogen levels could re-sensitize your GLP-1 receptors and restart fat loss without increasing your tirzepatide dose. The 35% improvement in weight loss seen in the Mayo Clinic study applies to women adding hormone therapy, not just those starting both simultaneously.
Additionally, better sleep from reduced hot flashes means better hunger hormone regulation. Improved mood means less emotional eating. Reduced joint pain from estrogen means more ability to exercise. These indirect benefits compound quickly.
Comparing GLP-1 options for HRT users
Not all GLP-1 medications interact with HRT in exactly the same way. Here is how the main options compare.
Semaglutide (Ozempic, Wegovy)
Compounded semaglutide is the most widely prescribed GLP-1 for weight loss. It activates GLP-1 receptors and provides strong appetite suppression with once-weekly dosing. For HRT users, semaglutide has demonstrated approximately 30% greater weight loss when combined with hormone therapy.
Semaglutide causes less severe gastroparesis than tirzepatide at equivalent doses, which may mean slightly less impact on oral medication absorption. However, the difference is not large enough to make oral HRT safe with semaglutide. Transdermal delivery is still recommended.
Oral semaglutide (oral semaglutide drops or semaglutide troches) adds another layer of complexity. If you are taking oral semaglutide alongside oral HRT, both medications are competing for absorption in a slowed digestive system. Injectable semaglutide is preferable for HRT users.
Tirzepatide (Mounjaro, Zepbound)
Tirzepatide activates both GLP-1 and GIP receptors, providing stronger weight loss effects than semaglutide in head-to-head trials. The Mayo Clinic study specifically demonstrated the 35% weight loss improvement with tirzepatide combined with HRT.
However, tirzepatide causes more pronounced gastroparesis than semaglutide. The ~60% reduction in oral contraceptive absorption was specifically documented with tirzepatide. For HRT users on oral hormones, switching to non-oral delivery is even more important with tirzepatide than with semaglutide.
Tirzepatide is available in multiple formats including tirzepatide drops and tirzepatide ODT (orally disintegrating tablets), though injectable remains the most studied form for the HRT combination.
Retatrutide (investigational)
Retatrutide is the newest entrant, activating three receptors: GLP-1, GIP, and glucagon. Early data suggests even greater weight loss than tirzepatide. However, there is currently no published data specifically on the combination of retatrutide and HRT.
Given that retatrutide likely causes similar or greater gastroparesis than tirzepatide, the same oral absorption concerns would apply. The differences between tirzepatide and retatrutide include mechanisms that may differently affect hormonal metabolism, but these interactions have not yet been studied in the context of HRT.
For SeekPeptides members tracking the latest research, retatrutide and HRT combination data will be a critical area to watch as clinical trials progress. The platform provides regular updates on emerging research and its implications for existing protocols.
Long-term outlook and sustainability
The question everyone asks eventually: how long do I need to stay on these medications?
HRT is typically continued for as long as symptoms persist and benefits outweigh risks. For many women, this means years or even decades. The decision is individual and should be revisited periodically with your provider.
GLP-1 medications are increasingly viewed as chronic treatments rather than short-term interventions. Weight regain after discontinuation is common, with studies showing 60-70% of lost weight returning within a year of stopping. How long to stay on semaglutide depends on your goals, response, and long-term weight management strategy.
The combination approach may actually improve long-term sustainability. HRT addresses the hormonal environment that promotes weight gain. If you stop the GLP-1 medication but continue HRT, the hormonal factors that contributed to weight gain are still managed. This may reduce, though not eliminate, the risk of rebound weight gain.
Some practitioners use a strategy of reaching target weight with full-dose GLP-1, then gradually reducing to a GLP-1 maintenance dose while continuing HRT. The microdosing approach may provide enough appetite support to maintain weight without the full dose and its associated costs and side effects. Microdosing tirzepatide may even provide anti-inflammatory benefits that complement HRT for long-term health.
The key to sustainability is building habits during the active weight loss phase that can carry you through maintenance. SeekPeptides members access structured transition protocols that guide you from active loss to maintenance, ensuring that the investment in combination therapy produces lasting results.