Mar 16, 2026

Day one, you feel nothing. Maybe a slight pinch at the injection site, maybe a flutter of hope, but otherwise nothing remarkable happens. Day four, your lunch sits differently. You push half the plate away without thinking about it. Day ten, you step on the scale and see a number that makes you pause. Not dramatic. Not life-changing. But real. Day twenty-one, your pants fit differently. Something is shifting. By day thirty, you have data, not just feelings, and that data tells a story most guides get completely wrong.
The first month on tirzepatide is the most misunderstood phase of the entire treatment. Some people expect ten pounds to vanish overnight. Others hear about the 2.5 mg starting dose being "sub-therapeutic" and assume nothing will happen at all. Both groups end up confused, disappointed, or ready to quit before the real results even begin.
Here is what actually happens during those first thirty days. Not the clinical trial summary. Not the marketing version. The week-by-week reality of appetite changes, weight fluctuations, side effects that come and go, and the metabolic groundwork your body is laying for the months ahead. Whether you are on brand-name Zepbound, compounded tirzepatide, or Mounjaro prescribed off-label, this guide covers the real timeline that researchers and users consistently report.
Understanding the 2.5 mg starting dose
Every tirzepatide protocol begins at 2.5 mg per week. This is not an accident. It is not a conservative suggestion from cautious doctors. It is a deliberate, evidence-based approach designed to let your gastrointestinal system adapt to a powerful GLP-1 and GIP dual receptor agonist without overwhelming it.
The 2.5 mg dose is technically sub-therapeutic for weight loss. Read that again. The starting dose was never designed to produce maximum fat loss. Its purpose is tolerability. The SURMOUNT-1 clinical trial, published in the New England Journal of Medicine, tested tirzepatide at 5 mg, 10 mg, and 15 mg for weight reduction. The 2.5 mg dose existed only as a four-week on-ramp to the 5 mg therapeutic dose.
Does that mean nothing happens at 2.5 mg? Not at all.
Even at this introductory dose, tirzepatide activates both GLP-1 and GIP receptors. Your brain receives satiety signals it was not receiving before. Gastric emptying slows. Insulin sensitivity begins to shift. The machinery is turning on. You just will not see the full output yet.
Think of it like warming up an engine. The car is running. The systems are engaging. But you have not hit the highway. Understanding this distinction prevents the most common first-month mistake, which is quitting too early or assuming the medication does not work because the scale has not dropped dramatically.
How tirzepatide differs from semaglutide at the starting dose
If you have researched semaglutide versus tirzepatide, you know both medications belong to the GLP-1 receptor agonist class. But tirzepatide adds something semaglutide does not have. It also activates GIP receptors, creating a dual-action mechanism that influences appetite, insulin, and fat metabolism through two separate pathways.
At the starting dose, this dual mechanism means tirzepatide users often notice appetite suppression slightly earlier than those on semaglutide. The GIP receptor activation contributes to glucose regulation and may enhance the satiety signal even at the lowest dose. Some researchers report feeling "less interested in food" within the first three to five days on tirzepatide, compared to a full week or longer for semaglutide at its 0.25 mg starting dose.
The side effect profiles also differ. Tirzepatide tends to produce slightly less nausea at equivalent therapeutic doses, though this advantage is less pronounced during the starting phase when both medications are at their gentlest. The key difference is trajectory. Tirzepatide typically produces greater total weight loss over time, with the SURMOUNT-1 trial showing average losses of 15 to 22 percent of body weight at higher doses, compared to roughly 15 percent for semaglutide in the STEP trials.
Why the dose escalation schedule matters
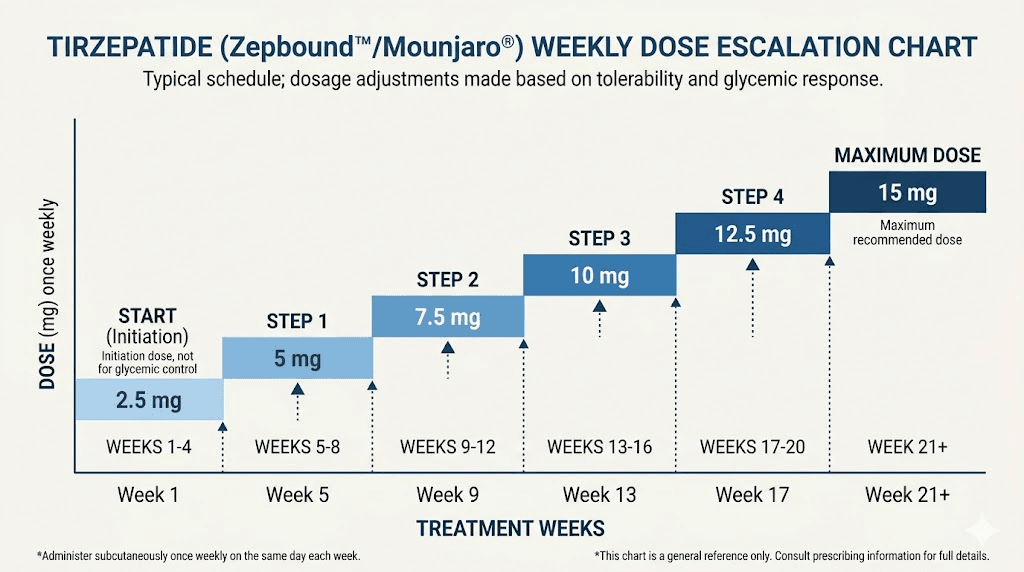
The standard escalation follows a predictable pattern. Four weeks at 2.5 mg, then four weeks at 5 mg, followed by increases to 7.5 mg, 10 mg, 12.5 mg, and potentially 15 mg. Each step lasts a minimum of four weeks, sometimes longer depending on tolerability and response.
This matters for first-month expectations because you will spend the entire first month at the lowest possible dose. Every result you see, every pound you lose, every appetite change you notice, happens at a dose that represents a fraction of the medication full potential. Understanding this context transforms disappointment into patience. Three pounds lost in month one is not a failure. It is the foundation.
For detailed unit conversions at each dose level, our guides on converting 2.5 mg to units and the complete tirzepatide dose chart break down every measurement you need. If you are using compounded tirzepatide, the compounded dosage calculator accounts for different concentrations.
Week one: days 1 through 7
The first injection is anticlimactic for most people. A small subcutaneous injection, typically in the abdomen, thigh, or upper arm. The needle is thin. The volume is small. Some people feel a brief sting. Others feel nothing at all.
Then you wait.
For the first 24 to 48 hours, most users report zero noticeable changes. No appetite suppression. No nausea. No weight change. The medication is absorbing, distributing, and beginning to bind to receptors throughout the body, but the effects have not reached a perceptible threshold yet.
When appetite changes first appear
Around days three to five, subtle shifts begin. You might notice that your usual breakfast feels like too much food. Or you realize at 2 PM that you forgot about the snack you normally eat at 11 AM. These changes are often so gentle that people attribute them to other factors, stress, busy schedules, not feeling well. But when you track your food intake, the numbers tell a different story. Meals get 15 to 25 percent smaller without conscious effort.
This is the appetite suppression mechanism activating. Tirzepatide slows gastric emptying, meaning food stays in your stomach longer. You feel full sooner. You stay full longer. The signal from your gut to your brain shifts from "keep eating" to "that is enough."
Not everyone experiences this in week one. Some people, particularly those with significant insulin resistance or higher body weight, may not notice appetite changes until week two or even week three. This is normal. The medication is still working at the receptor level. Perceptible effects simply take longer for some individuals.
Common week one side effects
The most frequently reported side effects in the first week are mild and often barely noticeable at the 2.5 mg dose.
Mild bloating or fullness after eating is the most common early complaint. Your digestive system is adjusting to slower gastric emptying. Food that previously moved through your stomach in two to three hours now takes longer, and your body has not fully adapted to this new pace.
Mild headaches affect a small percentage of users in the first few days. These typically resolve within 48 to 72 hours and respond well to adequate hydration and standard over-the-counter pain relief. If headaches persist, our tirzepatide headache treatment guide covers evidence-based management strategies.
Injection site reactions are possible but uncommon at this stage. A small red mark or mild tenderness at the injection location is within the normal range. If the area becomes significantly red and itchy, review our injection site reaction treatment guide for appropriate responses.
What about nausea? At 2.5 mg, significant nausea is relatively uncommon. Clinical data from the SURMOUNT trials shows that gastrointestinal side effects are dose-dependent, meaning they increase with higher doses. Most people tolerate the starting dose with minimal or no nausea. When it does occur, it tends to be mild and brief, lasting a few hours rather than days.
Scale expectations for week one
Zero to two pounds. That is the realistic range for week one weight change. Some people see a pound or two drop, often attributable to reduced food intake and mild water loss. Others see no change at all. A small number even see a temporary increase due to normal weight fluctuation, water retention, or hormonal factors unrelated to the medication.
Do not let the scale define week one. The more important metrics are appetite awareness, food choices, and how your body responds to the injection itself. If you tolerate week one without significant side effects, you have successfully cleared the first checkpoint.
Week two: days 8 through 14
Week two is when tirzepatide starts to feel real. The medication has reached steady-state blood levels, meaning the concentration in your system is now consistent rather than building. Your second injection at the end of week one reinforced the receptor activation. And your body is beginning to respond in ways you can actually measure.
Appetite suppression intensifies
The difference between week one and week two appetite is often dramatic. Week one felt like a gentle nudge. Week two feels like someone turned down the volume on hunger. Meals that previously left you satisfied for two hours now keep you full for four. Cravings for high-calorie foods, the ones that used to call your name from the pantry, lose their urgency.
This is not willpower. This is neurochemistry.
Tirzepatide acts on appetite centers in the hypothalamus, reducing the signals that drive food-seeking behavior. The GIP receptor activation adds an additional layer of metabolic regulation that influences how your body processes and stores nutrients. Together, these mechanisms create a measurable reduction in caloric intake without the constant mental battle that characterizes traditional dieting.
Research from the SURMOUNT-1 trial showed that participants reduced their daily caloric intake by approximately 350 to 500 calories per day, even at lower doses. By week two, most users begin to see this reduction reflected in their eating patterns. Portion sizes shrink. Snacking decreases. The mental noise around food quiets considerably.
For guidance on building meals around this new appetite, our tirzepatide diet plan and meal plan guide provide protein-focused frameworks that maximize the medication effectiveness while preserving muscle mass.
Digestive adjustments continue
Week two is when some people first encounter digestive changes. Slower gastric emptying means food sits in the stomach longer, and this can produce several effects that feel unfamiliar but are completely expected.
Constipation is one of the more common week two complaints. When food moves through the digestive system more slowly, water absorption increases in the colon, leading to harder stools and less frequent bowel movements. Increasing water intake, adding fiber-rich foods, and gentle movement can help. If constipation becomes uncomfortable, our dedicated treatment guide covers over-the-counter options and dietary adjustments that work specifically for GLP-1 users.
Some users experience the opposite effect. Diarrhea can occur as the gut adjusts to altered motility signals. This typically resolves within a few days and is more common in people who eat high-fat meals while on the medication. Reducing fatty food intake, which is something the medication often naturally encourages anyway, usually resolves this issue quickly.
Sulfur burps are an unexpected but well-documented side effect that some people encounter for the first time in week two. The delayed gastric emptying allows food to ferment slightly longer in the stomach, producing hydrogen sulfide gas. While unpleasant, this is harmless and tends to improve as the body adapts. Avoiding eggs, cruciferous vegetables, and high-protein meals right before bed can reduce the frequency.
Energy and mood shifts
Week two brings a split in user experiences that is worth understanding. About half of tirzepatide users report stable or improved energy levels. Eating less and eating cleaner naturally reduces post-meal energy crashes. Blood sugar levels stabilize. The afternoon slump that used to demand a sugary snack or a coffee becomes less pronounced.
The other half experience mild fatigue. This makes physiological sense. You are consuming fewer calories. Your body is adapting to a new metabolic state. Some tiredness during this transition is normal and expected. It does not mean the medication is wrong for you. It means your body is adjusting.
If fatigue becomes significant, evaluate your protein intake first. Many people inadvertently cut protein along with overall calories, and inadequate protein intake amplifies fatigue and can accelerate muscle loss. Aim for at least 0.7 grams of protein per pound of body weight daily. Our foods to avoid guide helps identify which foods to cut while preserving the nutrient-dense options your body needs during this transition.
Mood changes, including mild anxiety or irritability, affect a smaller percentage of users. These are usually transient and related to the metabolic adjustment rather than a direct neurological effect. If mood changes persist beyond two weeks or become severe, consult with a healthcare provider.
Scale check: end of week two
By the end of week two, most users have lost between one and four pounds. The average sits around two to three pounds. This number varies significantly based on starting weight, baseline diet quality, activity level, and individual metabolic response.
A 300-pound individual might see three to five pounds in the first two weeks. A 180-pound individual might see one to two pounds. Both results are normal and appropriate. Percentage-based thinking is more useful here. Losing 1 to 1.5 percent of body weight in the first two weeks at the sub-therapeutic starting dose puts you on an excellent trajectory.
If you have not lost any weight by day 14, do not panic. Refer to our guide on why you are not losing weight on tirzepatide for a systematic approach to troubleshooting. In many cases, the scale lag resolves once the dose increases to 5 mg in week five.
Week three: days 15 through 21
Week three is often the plateau week. The initial water weight and caloric deficit have produced their early results. Your body has adapted to the 2.5 mg dose. And the scale may stall or even bounce up a pound. This is the week that separates people who succeed on tirzepatide from those who give up prematurely.
The week three plateau is expected
Your body is not broken. The medication has not stopped working. What is happening is a perfectly normal physiological response to reduced caloric intake. Your body adjusts water retention, glycogen stores shift, and hormonal fluctuations can mask ongoing fat loss. The scale is a lagging indicator that captures water, muscle, food weight, and fat simultaneously. It does not differentiate between them.
During week three, your body is likely still burning fat at a moderate rate. But simultaneous changes in water retention can mask this progress entirely. A person might lose half a pound of fat while retaining an equivalent amount of water, producing a net zero on the scale. This does not represent failure. It represents biology doing what biology does.
Measurements tell a more accurate story. If you are tracking waist circumference, hip measurements, or how your clothing fits, week three often reveals subtle positive changes that the scale misses. A belt notch tighter. A shirt slightly looser. These changes are real, even when the number on the scale refuses to cooperate.
Appetite may stabilize or fluctuate
Some users report that the appetite suppression they experienced in week two feels slightly less intense by week three. This is not the medication wearing off. It is your body finding a new equilibrium at the 2.5 mg dose level. The initial dramatic reduction in hunger gives way to a more subtle, sustained decrease that feels less remarkable simply because you have gotten used to it.
Other users find week three appetite suppression remains strong. Individual variation is significant, and there is no "correct" experience. What matters is whether your overall caloric intake remains lower than your pre-tirzepatide baseline. If you are eating 300 to 500 calories less per day than before starting, the medication is doing its job regardless of how intense the appetite suppression feels subjectively.
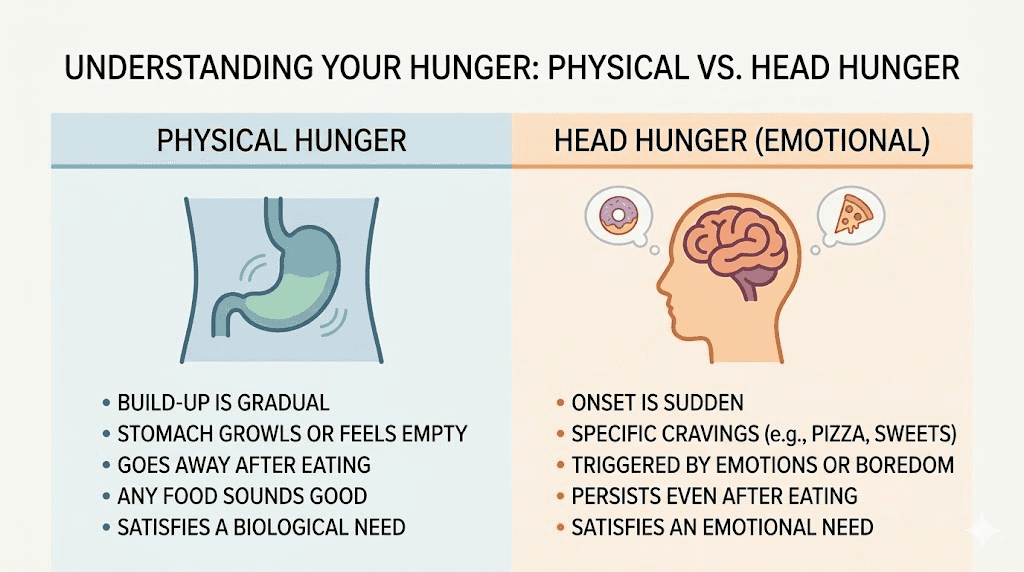
This is also when some people encounter the phenomenon of "head hunger" versus physical hunger. Your body might not need food, but your brain still wants it. The emotional and habitual drivers of eating, boredom, stress, routine, do not disappear because a medication is reducing your physical hunger signals. Recognizing the difference between physical hunger and psychological hunger is one of the most important skills to develop during the first month.
Side effects often peak and then improve
For people who experienced gastrointestinal side effects in weeks one and two, week three often brings relief. The body has had three weeks to adapt to slowed gastric emptying and altered gut motility. Nausea, if it occurred, typically fades. Constipation patterns stabilize. Bloating becomes less frequent.
This improvement is encouraging because it suggests your gastrointestinal system has adapted to the current dose, which means you have a better foundation for tolerating the dose increase that comes in week five. Users who experienced zero side effects at 2.5 mg generally have an easier transition to 5 mg as well.
If you are still experiencing significant body aches, muscle pain, or persistent digestive issues in week three, document these symptoms carefully. They may indicate a need for slower dose escalation when the time comes to increase to 5 mg. Some clinicians recommend extending the 2.5 mg phase to six or eight weeks for patients with sensitive digestive systems, and this conservative approach does not compromise long-term outcomes.
Week four: days 22 through 30
The final week of month one. Your body has spent almost thirty days on tirzepatide. The receptor activation is established. Your eating patterns have shifted. Your digestive system has adapted. And now you stand at a crossroads where data replaces hope as your primary guide.
Realistic first month weight loss numbers
Here is where honest numbers matter more than inspirational stories. Based on clinical trial data and real-world user reports, the realistic weight loss range for the first month on tirzepatide at 2.5 mg is two to seven pounds. The median falls around three to five pounds.
Let me break that down by starting weight, because context determines what these numbers mean.
If you weigh 300 pounds and lose four pounds in month one, that represents approximately 1.3 percent of your body weight. The SURMOUNT-1 trial showed average weight loss of around 1 to 2 percent at the four-week mark across all dose groups that started at 2.5 mg. You are right on track.
If you weigh 200 pounds and lose three pounds, that represents 1.5 percent, also perfectly within the expected range. If you weigh 180 pounds and lose two pounds, that is 1.1 percent, which is still completely normal for a sub-therapeutic starting dose.
The post hoc analysis from SURMOUNT-1, published in PMC, examined early weight loss responders and found that participants who lost more than 1 percent of body weight in the first four weeks tended to achieve better overall results at 72 weeks. But participants who lost less than 1 percent in the first month still achieved significant weight loss over the full treatment course. Early results are correlated with, but do not determine, long-term outcomes.
Non-scale victories that matter more
The scale captures one dimension of a multidimensional process. By week four, pay attention to changes that numbers cannot capture.
Relationship with food. How you think about meals has likely shifted. The constant mental negotiation, should I eat this, can I resist that, how many calories is this, quiets when appetite regulation works properly. Food becomes fuel rather than a source of anxiety. This psychological shift is arguably more valuable than any number on the scale because it is the foundation for sustainable weight management.
Energy patterns. Your energy throughout the day may be more stable. Without the blood sugar spikes and crashes from large meals and high-glycemic snacks, many users report a smoother, more consistent energy curve. Fewer afternoon crashes. Less need for caffeine. Better focus during work.
Sleep quality. Some users report improved sleep by week four, likely related to smaller evening meals and more stable blood sugar levels overnight. Reduced late-night snacking alone can significantly improve sleep architecture. However, a small percentage experience insomnia, particularly if they inject later in the day. If sleep disruption occurs, our guide covers timing adjustments and other strategies.
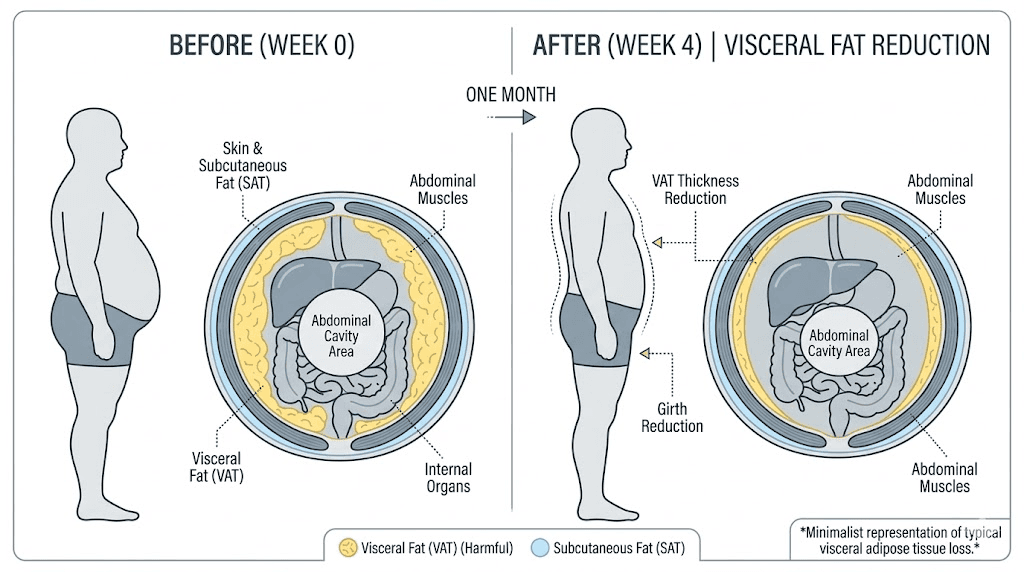
Physical measurements. Waist circumference reductions of half an inch to one inch are common by week four, even when scale changes are modest. Tirzepatide appears to preferentially reduce visceral fat, the metabolically active fat around organs, which reflects in waist measurements before it shows up as dramatic scale changes.
Preparing for the dose increase
As week four ends, you are approaching the transition to 5 mg. This is where your first month of data becomes invaluable. Reflecting on how your body responded at 2.5 mg helps predict and prepare for the next phase.
If you tolerated 2.5 mg with minimal side effects, the transition to 5 mg will likely be smooth. Some temporary increase in appetite suppression and mild GI symptoms may occur, similar to what you experienced in the first week or two, but your body is now primed for GLP-1 and GIP receptor activation and adapts more quickly.
If you had significant side effects at 2.5 mg, discuss with your provider whether extending the starting dose period or using an intermediate dose step might be appropriate. Some compounding pharmacies offer 3.75 mg concentrations that allow a gentler transition. Our guide on compounded tirzepatide starting doses details these intermediate options.
The best time to take your tirzepatide shot may also be worth reconsidering before the dose increase. If you injected in the morning during month one and experienced afternoon nausea, switching to evening injections before the dose increase allows you to sleep through the peak GI effects. Conversely, if nighttime injections disrupted your sleep, morning administration before the higher dose makes sense.
The science behind first month weight loss
Understanding why the first month produces modest results compared to later months requires examining the pharmacology of tirzepatide and the physiology of weight loss. This is not just academic detail. It is the knowledge that prevents premature discontinuation and sets realistic expectations.
Dual receptor mechanism explained
Tirzepatide is the first approved dual GIP and GLP-1 receptor agonist. This dual mechanism is what separates it from semaglutide and other single-mechanism GLP-1 therapies. Understanding what each receptor does clarifies why the medication works the way it does.
GLP-1 receptor activation slows gastric emptying, reduces appetite through hypothalamic signaling, and improves insulin secretion in a glucose-dependent manner. This is the pathway responsible for most of the appetite suppression you feel in the first month. It is also the pathway that can produce nausea when activated too aggressively, which is why the gradual dose escalation exists.
GIP receptor activation adds complementary effects. GIP enhances insulin sensitivity, influences lipid metabolism, and may directly affect adipose tissue. Research suggests that GIP receptor activation contributes to the superior weight loss outcomes seen with tirzepatide compared to GLP-1-only medications. The GIP component appears to be particularly important for metabolic improvements that go beyond simple caloric restriction, including beneficial changes in cholesterol levels, triglycerides, and inflammatory markers.
During the first month at 2.5 mg, both receptor systems are engaged but not maximally stimulated. Think of it as operating at 20 to 30 percent of the medication potential. The appetite reduction, metabolic improvements, and fat oxidation changes are happening. They are just happening at a fraction of the intensity they will reach at therapeutic doses.
Why fat loss accelerates after month one
The escalation to 5 mg in week five represents a significant jump in receptor activation. Clinical data shows that the dose-response curve for tirzepatide is not linear. Moving from 2.5 mg to 5 mg does not simply double the effect. It pushes past a threshold where the weight loss mechanisms engage more fully.
The SURMOUNT-1 trial data reveals this acceleration clearly. At 12 weeks (three months), participants on 5 mg had lost an average of about 7 percent of body weight. At 24 weeks (six months), the loss reached approximately 11 percent. By 72 weeks, the 5 mg group averaged 16 percent total body weight loss. The curve steepens dramatically after the first month.
This acceleration happens because higher doses produce stronger appetite suppression, greater metabolic changes, and more pronounced effects on fat oxidation. The metabolic adaptations that began during your first month, improved insulin sensitivity, altered gut hormone profiles, changes in food preferences, serve as the platform for these accelerated results.
For people who worry their first month results predict their total trajectory, the data is clear. First month weight loss at 2.5 mg is a poor predictor of 12-month outcomes at therapeutic doses. Some of the most successful long-term results come from people who lost very little in month one but responded dramatically once they reached their optimal maintenance dose.
Metabolic changes happening below the surface
The scale does not capture several important metabolic improvements that begin during the first month. These changes contribute to long-term health outcomes and lay the groundwork for sustained weight loss.
Insulin sensitivity improves. Even at 2.5 mg, tirzepatide reduces fasting insulin levels and improves glucose handling. For people with insulin resistance or prediabetes, these changes are clinically meaningful even before significant weight loss occurs. Better insulin sensitivity means your body stores less fat and burns more efficiently.
Metabolic rate adjusts. Unlike simple caloric restriction, which can rapidly decrease metabolic rate, the hormonal effects of tirzepatide appear to partially protect against this adaptive thermogenesis. Your metabolism does not crash the way it would if you simply ate less without pharmaceutical support. This metabolic protection becomes more significant at higher doses and over longer treatment periods.
Inflammatory markers decrease. GLP-1 and GIP receptor activation have anti-inflammatory effects that extend beyond weight loss. C-reactive protein, a marker of systemic inflammation, typically begins decreasing within the first month. This has implications for cardiovascular health, joint comfort, and overall metabolic function.
Gut hormone profiles shift. Tirzepatide alters the balance of several gut hormones beyond GLP-1 and GIP, including glucagon, peptide YY, and others involved in appetite regulation and nutrient absorption. These hormonal shifts take time to fully establish, which is another reason why the first month represents the beginning rather than the full picture of what tirzepatide can do.
Managing side effects during the first month
Side effects at 2.5 mg are generally mild. But "generally mild" does not mean "nonexistent," and understanding what to expect and how to respond makes the first month significantly more manageable.
Nausea: the most discussed side effect
Clinical data from the SURMOUNT trials shows that nausea affects approximately 13 to 24 percent of tirzepatide users, depending on dose. At 2.5 mg, the incidence is at the lower end of this range. Most people at the starting dose either do not experience nausea at all or experience it so mildly that it does not interfere with daily activities.
When nausea does occur at 2.5 mg, it typically follows a pattern. It appears within 24 to 48 hours after injection, peaks in intensity for a few hours, and then gradually fades over the next one to three days. By the second or third injection, the nausea response often diminishes as the body adapts.
Management strategies that consistently work include eating smaller meals throughout the day instead of two or three large ones, avoiding high-fat and greasy foods that slow gastric emptying further, staying well hydrated with small frequent sips rather than large volumes at once, and avoiding lying down immediately after eating.
Bland, easy-to-digest foods like bananas, rice, plain toast, and broth-based soups are gentler on the stomach during nausea episodes. Some users find ginger tea or ginger supplements helpful. Over-the-counter anti-nausea options like meclizine or dimenhydrinate can provide relief for more persistent episodes, though checking with a healthcare provider first is advisable.
The timing of your injection can also influence nausea. Many users find that injecting in the evening, ideally after dinner, allows them to sleep through the initial nausea window. Others prefer morning injections so that any GI effects resolve before bedtime. Experiment during the first month to find your optimal injection day and timing.
Constipation and digestive changes
Constipation is the second most common GI complaint during the first month. Slowed gastric emptying extends through the entire digestive tract, and the colon extracts more water from stool as transit time increases. The result is harder, less frequent bowel movements that can become uncomfortable if not addressed proactively.
Prevention is more effective than treatment. From day one, increase your water intake to at least 80 to 100 ounces daily. Add fiber gradually through vegetables, fruits, and whole grains. A magnesium citrate supplement, typically 200 to 400 mg daily, can help maintain regularity without the harsh effects of stimulant laxatives.
Movement helps as well. Even 15 to 20 minutes of walking daily stimulates intestinal motility and can prevent the sluggish digestion that contributes to constipation. This does not need to be intense exercise. A light walk after meals is often sufficient to keep things moving.
If constipation becomes problematic, our detailed tirzepatide constipation treatment guide covers escalating interventions from dietary changes to over-the-counter options to when to involve a healthcare provider.
Fatigue and energy management
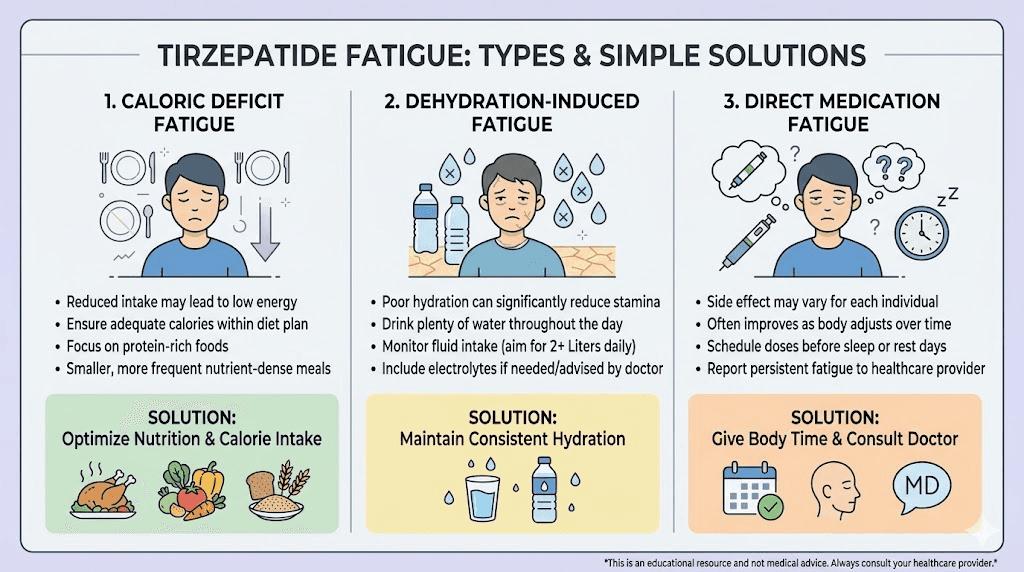
Fatigue during the first month on tirzepatide usually stems from one of three causes, and identifying which one affects you determines the appropriate solution.
Caloric deficit fatigue. If you have dramatically reduced your food intake, your body may simply not have enough fuel. This is especially common in people who cut calories too aggressively in an attempt to accelerate weight loss. The medication already reduces appetite naturally. You do not need to add deliberate restriction on top of it. Eat until comfortably satisfied, focus on nutrient-dense foods, and ensure adequate protein. This type of fatigue resolves when you eat enough.
Blood sugar adjustment fatigue. As tirzepatide improves insulin sensitivity and alters glucose handling, some people experience temporary energy dips related to lower blood sugar levels. This is particularly common in people with prediabetes or insulin resistance whose bodies are accustomed to operating at higher glucose levels. The fatigue typically resolves within two to three weeks as the body adapts to more regulated blood sugar.
Sleep disruption fatigue. If the medication is affecting your sleep quality, whether through insomnia, more frequent waking, or changes in sleep architecture, daytime fatigue follows naturally.
Adjusting injection timing, avoiding late meals, and maintaining consistent sleep hygiene can address this. Our GLP-1 fatigue guide provides a comprehensive framework for identifying and resolving energy issues on GLP-1 medications.
For persistent fatigue that does not respond to these adjustments, understanding tirzepatide energy effects provides additional context and strategies.
Less common first month side effects
Several side effects affect a smaller percentage of users but are worth knowing about so they do not catch you off guard.
Dry mouth can develop as a result of changes in GI fluid dynamics and is sometimes exacerbated by increased water loss. Staying hydrated and using sugar-free lozenges can help.
Feeling unusually cold is a reported side effect that some users notice within the first few weeks. The mechanism is not fully understood but may relate to changes in metabolic heat production as caloric intake decreases and hormonal patterns shift. Layering clothing and maintaining adequate caloric intake can mitigate this.
Joint pain and body aches are occasionally reported, though whether these are direct medication effects or consequences of metabolic changes remains unclear. Adequate hydration, gentle stretching, and anti-inflammatory foods may help. If joint pain is significant, consult with your healthcare provider.
Menstrual changes can occur in the first month. Weight loss and hormonal shifts can alter cycle timing, flow, and symptoms. These changes are usually temporary and stabilize as the body adjusts. If you are concerned about reproductive effects, our guides on tirzepatide while breastfeeding and pregnancy on tirzepatide cover important safety considerations.
Optimizing your first month results
While the 2.5 mg starting dose limits how much weight you can lose in month one, several evidence-based strategies can maximize your results within that framework. These are not shortcuts or hacks. They are foundational habits that compound over time and become increasingly powerful as your dose increases.
Protein is non-negotiable
The single most important nutritional focus during tirzepatide treatment is protein intake. This is not optional. This is not a nice-to-have. Adequate protein is the difference between losing fat while preserving muscle and losing a combination of fat and muscle that leaves you weaker and metabolically compromised.
When you are in a caloric deficit, whether medication-induced or voluntary, your body breaks down tissue for energy. Without sufficient protein and resistance training, up to 25 to 40 percent of weight lost can come from lean mass. With adequate protein, that number drops to 10 to 15 percent or less.
Aim for 0.7 to 1.0 grams of protein per pound of body weight daily. For a 200-pound person, that means 140 to 200 grams of protein per day. This feels like a lot, especially when your appetite is suppressed. Protein shakes, Greek yogurt, lean meats, eggs, and cottage cheese become essential tools. Spreading protein across four to five smaller meals rather than trying to get it all in one or two sittings improves absorption and satiety.
Our best foods guide and GLP-1 breakfast ideas provide practical protein-focused meal frameworks that work well with the reduced appetite tirzepatide produces.
Resistance training preserves muscle mass
If you do one thing beyond taking the medication, make it resistance training. Two to three sessions per week of moderate intensity strength training sends a powerful signal to your body that muscle tissue is needed and should not be broken down for energy.
You do not need an elaborate gym routine. Basic compound movements like squats, deadlifts, presses, and rows, performed with challenging weight for 8 to 12 repetitions, provide sufficient stimulus to preserve and even build muscle during weight loss. Body weight exercises, resistance bands, and home workouts also work if gym access is limited.
The combination of tirzepatide, adequate protein, and resistance training produces a fundamentally different body composition outcome than tirzepatide alone. Clinical trials that included exercise interventions showed participants maintained significantly more lean mass while losing the same or more fat compared to sedentary participants.
Start conservatively in week one. Your body is adjusting to a new medication, reduced calories, and potentially new side effects. Light to moderate resistance training two times per week is sufficient for the first month. Intensity and frequency can increase as your body adapts and your dose escalates.
Hydration amplifies results
Water is involved in virtually every metabolic process affected by tirzepatide. Fat oxidation requires adequate hydration. Digestion depends on it. Temperature regulation, energy production, and waste elimination all improve with proper fluid intake.
During the first month, aim for 80 to 120 ounces of water daily, adjusted upward if you exercise, live in a hot climate, or weigh over 250 pounds. Many first month side effects, including headaches, constipation, fatigue, and dizziness, either improve or resolve entirely with increased water intake.
Electrolytes matter too. As caloric intake decreases and water intake increases, sodium, potassium, and magnesium can become depleted. Adding an electrolyte supplement or simply salting your food adequately prevents the muscle cramps, lightheadedness, and fatigue that electrolyte imbalance can cause.
Sleep and stress management
Poor sleep and chronic stress both increase cortisol levels, which promotes fat storage, increases appetite, and reduces insulin sensitivity, essentially working against everything tirzepatide is trying to accomplish. Prioritizing seven to nine hours of quality sleep and managing stress through whatever methods work for you, exercise, meditation, social connection, time in nature, amplifies the medication effectiveness.
This is especially important during the first month when your body is adjusting to multiple changes simultaneously. The compounded stress of metabolic adjustment, dietary changes, and potential side effects can overwhelm the body adaptive capacity if sleep and stress management are neglected.
What the clinical trials actually show
Let us look at the numbers from the major clinical trials, because these provide the most reliable benchmark for setting expectations.
SURMOUNT-1 trial data
The landmark SURMOUNT-1 trial, published in the New England Journal of Medicine, enrolled 2,539 adults with obesity (BMI of 30 or higher) or overweight (BMI of 27 or higher) with at least one weight-related comorbidity. Participants received tirzepatide at 5 mg, 10 mg, or 15 mg weekly, or placebo, for 72 weeks.
All participants started at 2.5 mg for four weeks before escalating to their assigned dose. This means the first month data from this trial directly reflects the experience you are having right now at the starting dose.
Results at 72 weeks showed dramatic weight loss across all doses. The 5 mg group averaged 16 percent body weight reduction, translating to roughly 35 pounds for a person starting at 220 pounds. The 10 mg group averaged 21.4 percent reduction, approximately 47 pounds. The 15 mg group averaged 22.5 percent, about 50 pounds.
Critically, 89 to 91 percent of participants on the 10 mg and 15 mg doses achieved at least 5 percent weight loss. Between 50 and 57 percent achieved 20 percent or greater weight loss, a threshold associated with significant improvements in metabolic health, cardiovascular risk, and quality of life.
SURMOUNT-4 maintenance data
The SURMOUNT-4 trial, published in JAMA, examined what happens when people continue versus stop tirzepatide after initial weight loss. After a 36-week lead-in period where all participants received tirzepatide and lost an average of 20.9 percent of body weight, participants were randomized to either continue tirzepatide or switch to placebo for another 52 weeks.
Those who continued tirzepatide lost an additional 5.5 percent body weight. Those who switched to placebo regained 14 percent. This trial demonstrates two critical points. First, continued treatment produces continued results. Second, the weight management benefits of tirzepatide require ongoing treatment for maintenance.
For first month users, this data reinforces that the initial four weeks are just the beginning of a longer treatment arc. The modest results at 2.5 mg are not the endpoint. They are the first chapter of a story that unfolds over months and years.
Real world results versus clinical trials
Clinical trial results represent optimal conditions, carefully selected participants, regular monitoring, dietary counseling, and high adherence. Real world results are typically 60 to 80 percent of clinical trial outcomes.
What does this mean for you? If clinical trials show an average of 16 percent body weight loss at 5 mg over 72 weeks, real-world users might expect 10 to 13 percent. If the trials show 22 percent at 15 mg, real-world results might be 14 to 18 percent. These are still remarkable outcomes, just slightly less dramatic than the headline numbers.
For the first month specifically, real-world results tend to mirror trial data more closely because everyone is at the same 2.5 mg dose and the treatment period is too short for adherence differences to significantly impact outcomes. Your first month results are likely representative of what clinical trial participants experienced.
Common first month mistakes to avoid
Certain mistakes are so common during the first month that addressing them directly can save weeks of frustration and prevent premature discontinuation of an effective treatment.
Eating too little
This seems counterintuitive. You want to lose weight. The medication reduces your appetite. Why not eat as little as possible to maximize results? Because extreme caloric restriction triggers adaptive responses that slow metabolism, increase muscle loss, and ultimately sabotage long-term outcomes.
Tirzepatide naturally reduces caloric intake by 300 to 500 calories per day through appetite suppression. This is enough to produce consistent fat loss without triggering starvation responses. Deliberately restricting further, dropping to 800 or 1000 calories per day, adds stress without proportional benefit and increases the risk of nutrient deficiencies, fatigue, and muscle loss.
Eat when hungry. Stop when satisfied. Choose nutrient-dense foods. Let the medication handle appetite regulation while you focus on food quality.
Obsessing over daily scale readings
Daily weigh-ins can be useful for tracking trends over time, but they become destructive when each reading carries emotional weight. Body weight fluctuates by one to five pounds daily based on water intake, sodium consumption, bowel activity, hormonal shifts, and sleep quality. None of these fluctuations reflect actual fat gain or loss.
A better approach is weekly weigh-ins under consistent conditions, same time, same clothing, same scale, after using the bathroom, before eating or drinking. Compare weekly averages rather than individual readings. A downward trend over four weekly readings is meaningful. Daily fluctuations are noise.
If the scale causes anxiety, consider weighing biweekly or monthly and using other metrics, waist circumference, clothing fit, progress photos, energy levels, to track progress.
Comparing your results to others
Social media is filled with tirzepatide transformation stories. "I lost 12 pounds my first month!" "I dropped two pants sizes in three weeks!" While some of these accounts are genuine, they represent statistical outliers, not typical outcomes. Comparing your three-pound first month loss to someone else twelve-pound loss is neither productive nor accurate.
Variables that influence first month results include starting weight and BMI, baseline metabolic rate, insulin resistance level, dietary changes, exercise habits, sleep quality, stress levels, hydration, and individual pharmacogenetic differences in drug metabolism. Two people on the exact same dose can have wildly different outcomes based on these factors.
Your results are your results. Compare your week four to your day one, not to someone else experience.
Neglecting nutrition quality
Reduced appetite does not eliminate the need for nutritional quality. Some people, finding they can only eat half their usual volume, fill that reduced volume with the same processed foods they ate before. Smaller portions of nutritionally poor food still result in inadequate micronutrient intake.
Every bite counts more when you are eating less. Focus on nutrient density. Lean proteins, vegetables, fruits, whole grains, and healthy fats should comprise the majority of your reduced intake. Our foods to avoid on tirzepatide guide identifies specific foods that worsen side effects and provide poor nutritional returns. The supplements to take with tirzepatide guide covers nutritional gaps that commonly develop during treatment.
Skipping or delaying injections
Consistency matters. Taking your injection on the same day each week, at approximately the same time, maintains stable blood levels and produces the most consistent appetite suppression and metabolic effects. Skipping a dose or shifting injection days randomly disrupts the steady-state concentration your body has adapted to.
If you do miss a dose, take it as soon as you remember as long as your next scheduled dose is at least three days away. If it is closer than three days, skip the missed dose and resume your regular schedule. Do not double up on doses.
Our guide on taking tirzepatide a day early covers the flexibility you have with injection timing and how to handle schedule disruptions.
What happens after month one
The first month is the prologue. Understanding what comes next helps contextualize your current results and maintain motivation through the gradual process of dose escalation and accelerating weight loss.
Month two: the 5 mg transition
Moving from 2.5 mg to 5 mg is the most significant dose change in the entire escalation schedule because it represents the transition from a sub-therapeutic to a therapeutic dose. Most users experience a noticeable increase in appetite suppression within the first week at 5 mg, often accompanied by a temporary return of mild GI symptoms as the body adjusts to the stronger receptor activation.
Weight loss typically accelerates during month two. Many users lose four to eight pounds in their second month, roughly double what they lost in month one. The combination of increased appetite suppression, enhanced metabolic effects, and the cumulative impact of lifestyle changes produces visible results that build confidence and reinforce adherence.
Our tirzepatide before and after guide and weight loss results collection show real results at various timepoints, including the accelerating trajectory that begins in month two.
Months three through six: peak acceleration
Months three through six represent the period of fastest weight loss for most tirzepatide users. Doses continue to escalate through 7.5 mg, 10 mg, and potentially 12.5 mg during this window. Each increase brings stronger appetite suppression and greater metabolic effects.
Average weight loss during this period ranges from one to two pounds per week, sometimes more at higher doses. Cumulative weight loss by month six often reaches 10 to 15 percent of starting body weight, a threshold associated with significant improvements in blood pressure, blood sugar, cholesterol, joint pain, sleep apnea, and overall quality of life.
This is also when long-term maintenance planning becomes important. The habits you established during month one, protein prioritization, resistance training, adequate hydration, mindful eating, become the infrastructure for sustaining weight loss over time.
Long-term trajectory
Tirzepatide produces its maximum weight loss effect over 60 to 72 weeks, approximately 14 to 17 months. After this point, most users reach a plateau where their new, lower body weight establishes a new metabolic equilibrium. Continued treatment at a maintenance dose prevents regain, as demonstrated by the SURMOUNT-4 trial data.
For those considering what their long-term relationship with tirzepatide will look like, our guide on how to wean off tirzepatide covers tapering strategies, while the tirzepatide not working anymore guide addresses plateau-breaking strategies for users who feel their results have stalled.
Compounded versus brand name tirzepatide in the first month
Many first-time users begin with compounded tirzepatide due to cost considerations. Understanding the differences between compounded and brand-name formulations helps set appropriate expectations for the first month.
Dosing accuracy considerations
Brand-name Zepbound and Mounjaro come in pre-filled auto-injectors with precise, factory-calibrated doses. Compounded tirzepatide typically comes in multi-dose vials that require drawing up each dose with a syringe. This introduces a small but meaningful variable in dosing accuracy.
For first-month users on compounded tirzepatide, accurate dosing requires understanding your vial concentration, using properly calibrated insulin syringes, and measuring carefully each time. Our tirzepatide syringe dosage guide and compound dosage chart provide step-by-step measurement instructions for various concentrations.
If your compounded tirzepatide arrives as lyophilized powder, you will need to reconstitute it before use. Our reconstitution guide covers the process in detail. For storage requirements, refer to our guides on refrigeration requirements and fridge storage duration.
Cost and accessibility
One of the primary reasons people choose compounded tirzepatide is cost. Brand-name Zepbound can exceed $1,000 per month without insurance coverage. Compounded versions from 503B compounding pharmacies typically cost significantly less, making the first month more accessible.
Our guides on affordable tirzepatide and cheap compounded options compare pricing across multiple sources. For those exploring payment flexibility, tirzepatide Afterpay options provide alternative payment structures.
Formulation differences
Compounded tirzepatide often includes additional ingredients that brand-name versions do not. Common additions include vitamin B12, glycine, niacinamide, and vitamin B6. These additions may provide supplementary benefits, particularly B12 for energy support and niacinamide for metabolic health.
The glycine B12 compound blend is popular among compounding pharmacies and may offer advantages in tolerability during the first month. Levocarnitine blends add another dimension of metabolic support. Our methylcobalamin guide explains the difference between B12 forms used in various compounds.
For users comparing different pharmacy options, our reviews of specific providers like Empower Pharmacy, Peptide Sciences, and Lavender Sky provide detailed comparisons of their tirzepatide formulations, pricing, and user experiences.
Injection technique and timing optimization
How you inject and when you inject can influence both side effect severity and medication effectiveness during the first month. Getting these details right from the beginning establishes good habits for the entire treatment course.
Choosing your injection site
Three primary injection sites work for subcutaneous tirzepatide administration. The abdomen, at least two inches from the navel, is the most popular due to ease of access and consistent absorption. The front of the thigh, roughly midway between hip and knee, is the second most common choice. The upper arm can also be used but is harder to self-administer.
Rotation between sites is important. Using the same spot repeatedly can cause lipohypertrophy, a buildup of fatty tissue that reduces absorption consistency. Rotate between at least two different areas, and within each area, vary the exact injection point by at least one inch each time.
For detailed injection technique, our syringe injection guide covers step-by-step technique, and the injection site overview compares absorption rates at different locations. The broader best GLP-1 injection site guide provides additional context.
Timing your injection for minimum side effects
The best time for your tirzepatide shot depends on your individual side effect pattern. There is no universally optimal time, but patterns emerge during the first month that help guide your decision.
Evening injection, after your last meal of the day, allows you to sleep through the initial four to eight hours post-injection when GI effects are most likely. This works well for people who experience nausea or digestive discomfort after injection.
Morning injection provides consistent blood levels throughout the day when appetite suppression is most needed. This works well for people who do not experience significant GI effects and want maximum daytime appetite control.
The best time of day to inject tirzepatide guide covers additional considerations including exercise timing, work schedules, and meal patterns.
Tracking your progress effectively
What you measure during the first month shapes your understanding of the entire treatment course. Establishing a tracking system now creates the data you will reference at months three, six, and twelve to evaluate your trajectory.
Essential metrics to track
Weight. Weekly, same conditions, same time. Record and calculate weekly and running averages.
Waist circumference. Weekly, at the navel, first thing in the morning. This is often a more reliable indicator of fat loss than scale weight, particularly in the first month when water fluctuations obscure fat changes.
Food intake. At least for the first two weeks, track what and how much you eat. Not to restrict, but to understand how the medication is changing your natural intake patterns. This data helps identify whether you are eating enough protein and whether your caloric deficit is appropriate.
Side effects. Keep a simple log of what you experience, when it occurs, how severe it is, and how long it lasts. This information is invaluable when discussing dose escalation with your provider.
Energy and mood. A daily 1-10 rating of energy and mood takes seconds but reveals patterns over time that individual days cannot show.
Progress photos. Monthly front, side, and back photos in consistent lighting and clothing. These become the most powerful record of your transformation and are often more motivating than scale numbers. Our men before and after and general before and after guides show what typical progress looks like at various timepoints.
Using calculators and tools
SeekPeptides provides several free tools that make first-month tracking easier. The peptide calculator helps with general dosing calculations, while the semaglutide dosage calculator serves those comparing or transitioning between medications. The reconstitution calculator ensures accurate preparation of compounded formulations.
For users considering microdosing approaches, the microdose schedule and microdosing guide cover alternative dosing strategies that some clinicians recommend for patients who are particularly sensitive to GI side effects.
When to contact your healthcare provider
Most first-month experiences on tirzepatide are manageable with self-care strategies. However, certain symptoms warrant medical attention and should not be ignored.
Persistent vomiting that prevents you from keeping food or liquids down for more than 24 hours requires medical evaluation. Dehydration can develop quickly and may necessitate IV fluid administration.
Severe abdominal pain, particularly in the upper right quadrant, could indicate gallbladder issues. GLP-1 receptor agonists are associated with an increased risk of gallstones and cholecystitis, though this risk is more commonly associated with rapid weight loss at higher doses.
Signs of allergic reaction, including difficulty breathing, severe rash, swelling of the face or throat, or widespread hives, require immediate emergency medical attention. These reactions are rare but serious.
Severe hypoglycemia symptoms, including confusion, loss of consciousness, extreme shakiness, or inability to function, warrant urgent medical evaluation. While tirzepatide lowers blood sugar in a glucose-dependent manner that reduces hypoglycemia risk compared to insulin, it can occur, especially in people taking other diabetes medications simultaneously. If you are taking metformin with tirzepatide, discuss blood sugar monitoring with your provider.
Mental health changes, including new or worsening depression, suicidal thoughts, or significant personality changes, should be reported to your provider immediately. While rare, any medication that affects brain chemistry warrants monitoring of mental health effects.
Comparing your first month to other GLP-1 medications
If you are choosing between tirzepatide and other options, or if you have previously tried another GLP-1 medication, understanding how the first month compares across different treatments provides useful context.
Tirzepatide versus semaglutide first month
Both medications start at sub-therapeutic doses, tirzepatide at 2.5 mg and semaglutide at 0.25 mg. Both produce modest first month weight loss. The key differences during month one are subtle.
Tirzepatide users tend to report slightly earlier appetite suppression, possibly due to the dual GIP/GLP-1 mechanism. Semaglutide users sometimes report more pronounced nausea at the starting dose. Neither medication produces dramatic scale changes in the first four weeks.
Our detailed semaglutide versus tirzepatide comparison and dosage chart comparison provide side-by-side analysis. For users considering switching, the conversion chart helps determine equivalent dosing. If you tried semaglutide first and it did not work well, our guide on whether tirzepatide will work if semaglutide did not addresses this common question.
Tirzepatide versus newer options
The GLP-1 medication landscape continues to evolve. Retatrutide, a triple receptor agonist targeting GIP, GLP-1, and glucagon receptors simultaneously, is in late-stage clinical trials and may eventually offer even greater weight loss potential. Our retatrutide versus tirzepatide comparison covers the emerging data.
Survodutide and CagriSema represent other next-generation options with different receptor profiles. Mazdutide is another dual agonist being developed internationally. For users interested in oral alternatives, orforglipron is an oral GLP-1 receptor agonist that may eventually provide a needle-free option.
For those interested in oral tirzepatide formulations, our guides on oral versus injection, tirzepatide drops, and tablets versus injections cover the evolving landscape of administration options.
Building habits that last beyond month one
The first month is a unique window for habit formation. Reduced appetite, increased awareness of food choices, and the motivation of starting something new create conditions where new behaviors take root more easily than at almost any other time.
Meal preparation and planning
Establishing a meal prep routine during month one pays dividends for the entire treatment course. When appetite is reduced and cooking motivation may be low, having prepared protein-rich meals available prevents the default to low-quality convenience foods.
Simple preparation is sufficient. Batch cooking chicken, fish, or eggs on weekends. Pre-cutting vegetables. Portioning Greek yogurt and cottage cheese into grab-and-go containers. Having protein shakes ready for days when solid food feels unappealing.
Our diet plan provides a complete framework, and the meal plan PDF offers a printable reference you can keep on your refrigerator.
Movement as medicine
Exercise during the first month should prioritize consistency over intensity. Walking 20 to 30 minutes daily, two to three resistance training sessions per week, and staying generally active throughout the day builds the movement habit without overwhelming a body that is already adapting to significant metabolic changes.
The combination of tirzepatide metabolic effects and regular exercise produces synergistic benefits. Exercise improves insulin sensitivity, preserves muscle mass, enhances mood, supports sleep quality, and accelerates fat loss. These benefits compound over time, making the first month commitment to regular movement an investment in long-term outcomes.
For SeekPeptides members, detailed exercise protocols designed specifically for GLP-1 users provide structured guidance that accounts for the unique considerations of exercising while on appetite-suppressing medication.
Building a support system
Weight loss is easier with support. Whether through a healthcare provider, a knowledgeable community, or an informed partner, having people who understand what you are going through reduces the isolation that can undermine long-term adherence.
SeekPeptides has become the most trusted platform for peptide education, with thousands of researchers and users relying on evidence-based guides, comprehensive protocols, and a supportive community to navigate their tirzepatide journey safely and effectively. Members access personalized protocol support, dosing guidance, and real-time community interaction that turns the solitary experience of medication management into a guided, supported process.
Frequently asked questions
How much weight will I lose in the first month on tirzepatide?
Most users lose between two and seven pounds during the first month at the 2.5 mg starting dose. The average is three to five pounds. This represents approximately 1 to 2 percent of starting body weight. Results vary based on individual factors including starting weight, diet quality, activity level, and metabolic response.
Is the 2.5 mg starting dose effective for weight loss?
The 2.5 mg dose is technically sub-therapeutic, meaning it was not designed for maximum weight loss. It serves as a tolerability on-ramp to reduce side effects during the transition to therapeutic doses. However, most users still experience meaningful appetite suppression and modest weight loss at this dose.
When will I notice appetite suppression on tirzepatide?
Most users notice reduced appetite within three to seven days of their first injection. Some experience it as early as day two. Others may not notice significant changes until week two or three. The effect typically intensifies when the dose increases to 5 mg in week five.
What are the most common side effects in the first month?
At the 2.5 mg dose, side effects are generally mild. The most common include decreased appetite, mild bloating, occasional constipation, and in some cases mild nausea. Most side effects improve within two to three weeks as the body adapts.
Should I exercise during the first month on tirzepatide?
Yes. Light to moderate exercise, including walking and basic resistance training two to three times per week, helps preserve muscle mass, improves insulin sensitivity, and can accelerate fat loss. Avoid extreme exercise during the first two weeks while your body adjusts to the medication.
Can I drink alcohol during the first month on tirzepatide?
Alcohol is not strictly prohibited, but many users find their tolerance decreases significantly on tirzepatide. Alcohol can also worsen nausea and GI side effects. If you choose to drink, start with small amounts to gauge your response. Our alcohol and tirzepatide guide and best alcohol choices guide cover this topic in detail.
What if I do not lose any weight in the first month?
Not losing weight at 2.5 mg is not uncommon and does not predict long-term outcomes. The starting dose is sub-therapeutic. Many users who see minimal results at 2.5 mg experience significant weight loss once they reach 5 mg or higher. Review our troubleshooting guide for potential adjustments, and discuss dose escalation timing with your provider.
Is it normal to feel tired during the first month?
Mild fatigue is common and usually results from reduced caloric intake, blood sugar adjustment, or sleep changes. Ensuring adequate protein, proper hydration, and consistent sleep typically resolves first-month fatigue within two to three weeks.
External resources
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your first month stay patient, your appetite stay managed, and your trajectory stay upward.