Mar 21, 2026

Tired of hearing that your weight gain is "just your thyroid" while every diet fails and every exercise plan stalls? You are not imagining it. Hashimoto thyroiditis rewires your metabolism in ways that make conventional weight loss strategies feel impossible. The fatigue alone makes consistent exercise a daily battle. The inflammation keeps your body locked in a pattern of resistance. And the frustration of watching the scale refuse to move, even when you are doing everything right, is enough to make anyone question whether progress is even possible.
That is exactly why GLP-1 receptor agonists have caught the attention of both patients and clinicians in the autoimmune thyroid space.
Medications like semaglutide and tirzepatide are producing dramatic weight loss results in clinical trials, but the question that matters most for Hashimoto patients goes deeper than pounds on a scale. Can these medications actually influence the autoimmune process itself? Can they reduce the thyroid antibodies driving your disease? Can they address the systemic inflammation that makes Hashimoto so much more than just a thyroid problem?
The answers are more nuanced than most articles will tell you. A 2025 narrative review analyzing 68 studies found zero dedicated clinical trials studying GLP-1 receptor agonists specifically for autoimmune thyroid disease. Zero. But that does not mean the research cupboard is bare. There is compelling mechanistic evidence, emerging clinical observations, and real patient experiences that paint a picture worth understanding, especially if you are navigating GLP-1 related fatigue concerns alongside your thyroid condition. This guide covers all of it, every mechanism, every study, every practical consideration, so you can have an informed conversation with your endocrinologist about whether GLP-1 therapy belongs in your Hashimoto management strategy.
What Hashimoto thyroiditis actually does to your metabolism
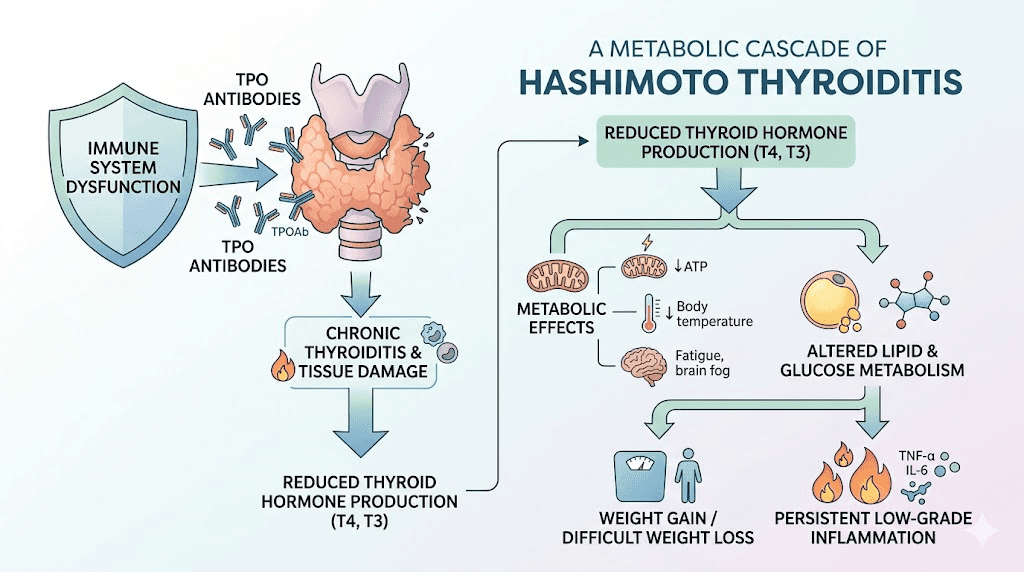
Before diving into GLP-1 medications, you need to understand why Hashimoto makes weight management so uniquely difficult. This is not garden-variety hypothyroidism. Hashimoto is an autoimmune disease where your immune system produces antibodies, primarily thyroid peroxidase (TPO) antibodies and thyroglobulin (TgAb) antibodies, that attack your own thyroid gland. The destruction is gradual. Progressive. Relentless without intervention.
The metabolic consequences cascade far beyond low thyroid hormone levels.
Your basal metabolic rate drops. Insulin resistance develops. Leptin signaling becomes dysregulated. Systemic inflammation elevates C-reactive protein, TNF-alpha, and IL-6 throughout your body. Your gut microbiome shifts toward inflammatory species. And the relationship between your gut health and thyroid function, what researchers call the gut-thyroid axis, becomes increasingly disrupted.
This is why levothyroxine alone often fails to restore normal weight. You can optimize your TSH to a perfect 1.5, take your medication exactly as prescribed, and still find that the metabolic damage from years of autoimmune inflammation does not simply reverse when hormone levels normalize. The inflammation persists. The insulin resistance persists. The metabolic set point has shifted.
Understanding this context matters because GLP-1 medications do not just suppress appetite. They operate through multiple pathways that directly intersect with the metabolic dysfunction Hashimoto creates. And that intersection is where the conversation gets genuinely interesting.
How GLP-1 receptor agonists work (and why it matters for autoimmunity)
GLP-1 receptor agonists mimic glucagon-like peptide-1, a hormone your gut naturally produces after eating. The pharmaceutical versions, including semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound), last far longer than natural GLP-1 and produce more pronounced effects.
Most people know these medications for weight loss. That is the headline. But the mechanism goes deeper.
GLP-1 receptors are not just in your pancreas and brain. They exist on macrophages, monocytes, endothelial cells, and throughout your immune system. When these receptors are activated, a cascade of anti-inflammatory signaling begins that has nothing to do with appetite or blood sugar. This is what researchers call the "pleiotropic" effects of GLP-1 receptor agonists, benefits that extend well beyond their primary metabolic function.
For someone with Hashimoto, these pleiotropic effects touch nearly every mechanism driving their disease. The appetite suppression matters, yes. The fat burning mechanisms matter. But the immunomodulatory effects, the anti-inflammatory signaling, the gut microbiome changes, these may matter even more for someone whose core problem is autoimmune, not just metabolic.
The three mechanisms that connect GLP-1 to thyroid autoimmunity
Mechanism one: NF-kB pathway inhibition. Nuclear Factor-kappa B is often called the master switch of inflammation. When NF-kB translocates into cell nuclei, it activates transcription of pro-inflammatory cytokines like TNF-alpha, IL-6, and IL-1beta, the exact inflammatory mediators elevated in Hashimoto patients. GLP-1 receptor activation prevents this nuclear translocation. It effectively keeps the master switch in the "off" position, reducing production of the cytokines driving thyroid destruction.
Mechanism two: NLRP3 inflammasome suppression. The NLRP3 inflammasome is the molecular machinery responsible for amplifying inflammatory responses into what researchers describe as a "cytokine storm." In chronic inflammatory conditions like Hashimoto, the NLRP3 inflammasome maintains a persistent state of immune activation. GLP-1 agonists create a blockade against NLRP3 assembly, dampening the sustained inflammatory signaling that perpetuates autoimmune thyroid destruction.
Mechanism three: regulatory T-cell enhancement. Regulatory T-cells (Tregs) are your immune system brakes. They prevent excessive immune responses and maintain self-tolerance, the ability of your immune system to recognize your own tissues as friendly. In Hashimoto disease, Treg function is impaired, which is partly why your immune system attacks your thyroid in the first place. GLP-1 receptor agonists enhance Treg function while simultaneously suppressing Th1 and Th17 cell polarization, the immune cell types most responsible for driving autoimmune thyroid inflammation.
These three mechanisms working together represent a fundamentally different approach to Hashimoto than simply replacing thyroid hormone. They address the immune dysregulation at the root of the disease. Whether they address it enough to produce meaningful clinical outcomes is the question research has not yet definitively answered.
What the research actually shows about GLP-1 levels in Hashimoto patients
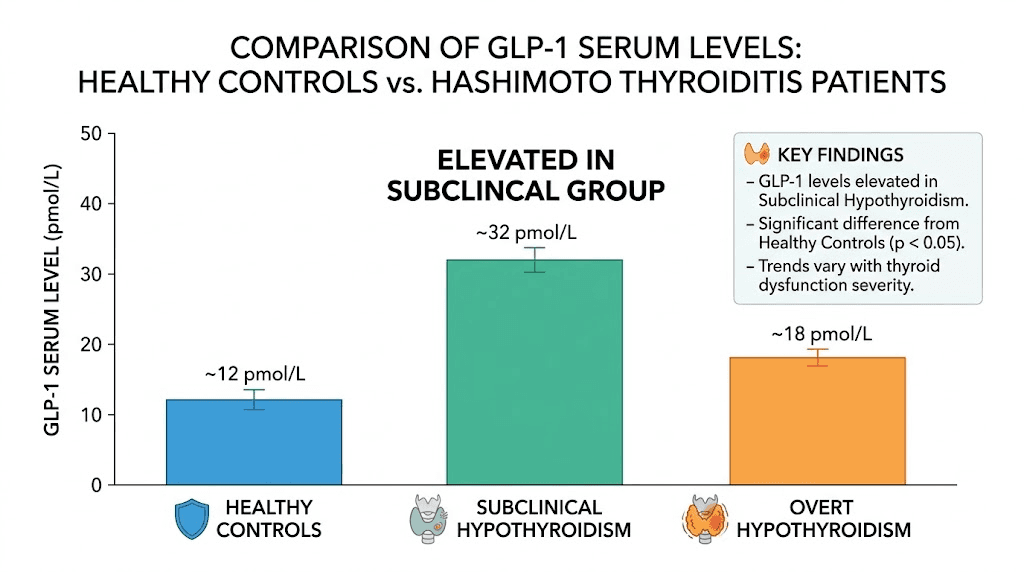
Here is where things get specific. A study published in the journal Peptides examined serum GLP-1 levels across three groups: 24 healthy controls, 24 patients with subclinical hypothyroidism from Hashimoto, and 24 euthyroid Hashimoto patients (those with antibodies but still-normal thyroid function).
The findings were unexpected.
Patients with subclinical hypothyroidism showed significantly elevated GLP-1 levels compared to controls. The mean log GLP-1 was 1.22 plus or minus 0.23 pmol/L in the subclinical hypothyroidism group versus 1.06 plus or minus 0.16 pmol/L in controls (P = 0.024). Statistically significant. Clinically intriguing.
Why would GLP-1 levels be higher in Hashimoto patients? The researchers could not establish a clear correlation between elevated GLP-1 and thyroid hormone levels (FT3 and FT4). The elevation appeared independent of thyroid function itself, suggesting something about the autoimmune or inflammatory state might be driving increased GLP-1 production, perhaps as a compensatory anti-inflammatory response.
This is a small study. Twenty-four patients per group. But it raises a critical question that larger research needs to answer: if your body is already upregulating GLP-1 production in response to autoimmune thyroid inflammation, what happens when you dramatically amplify that signal with pharmaceutical GLP-1 receptor agonists?
The answer, based on emerging clinical observations rather than randomized trials, suggests the amplification may indeed produce benefits beyond weight loss. Some thyroid clinicians report observing decreased TPO and thyroglobulin antibodies in patients using compounded semaglutide or brand-name GLP-1 medications. These observations lack the rigor of controlled trials, but they align perfectly with the mechanistic predictions. If GLP-1 receptor activation suppresses the immune pathways driving antibody production, antibody levels should decrease. And in at least some clinical settings, that is exactly what practitioners are seeing.
The anti-inflammatory pathways that matter most for Hashimoto patients
Understanding which inflammatory markers GLP-1 medications target helps you evaluate whether they might address your specific situation. Not all inflammation is the same, and Hashimoto creates a very specific inflammatory profile.
C-reactive protein reduction
CRP is a general marker of systemic inflammation. Elevated CRP is common in Hashimoto patients and correlates with disease severity, cardiovascular risk, and the persistent fatigue that makes daily functioning so difficult. GLP-1 receptor agonists consistently reduce CRP levels across multiple clinical trial populations. This reduction occurs through both direct anti-inflammatory signaling and indirect effects from fat loss, since adipose tissue is a major source of inflammatory cytokines.
For Hashimoto patients specifically, CRP reduction may translate to improved energy, reduced joint pain, better mood stability, and decreased cardiovascular risk. These are quality-of-life improvements that matter enormously even if they do not directly modify the autoimmune process.
TNF-alpha and IL-6 suppression
TNF-alpha and IL-6 are the workhorses of Hashimoto inflammation. TNF-alpha directly damages thyroid cells and promotes further immune cell recruitment to the thyroid gland. IL-6 drives the acute-phase inflammatory response and contributes to the systemic symptoms, the brain fog, the muscle aches, the feeling of being perpetually unwell, that Hashimoto patients know too well.
GLP-1 receptor activation reduces production of both cytokines through NF-kB pathway inhibition. This is not a theoretical mechanism. Multiple studies in diabetic and obese populations have documented measurable reductions in TNF-alpha and IL-6 with GLP-1 receptor agonist therapy. The question is whether these reductions are sufficient to meaningfully impact thyroid-specific autoimmune processes.
Macrophage polarization
Your immune system contains two broad categories of macrophages. M1 macrophages promote inflammation and tissue destruction. M2 macrophages promote healing, tissue repair, and anti-inflammatory responses. In Hashimoto disease, the balance shifts heavily toward M1, maintaining the destructive inflammatory state in your thyroid.
GLP-1 receptor agonists promote M2 polarization. They nudge macrophages toward the healing, anti-inflammatory phenotype rather than the destructive one. For thyroid autoimmunity, this shift could theoretically reduce the rate of thyroid tissue destruction, potentially preserving more thyroid function over time.
Could. Theoretically. These words matter. No one has demonstrated this effect specifically in thyroid tissue during GLP-1 therapy. But the mechanism is sound, the pathway is documented in other tissues, and the logic connecting them to Hashimoto is reasonable.
Adipokine rebalancing
Fat tissue is not passive storage. It is an active endocrine organ producing hormones that directly influence immune function. In Hashimoto patients, excess adipose tissue produces elevated leptin, which drives Th1 and Th17 immune responses, the exact immune cell types attacking your thyroid. Simultaneously, adiponectin, which promotes Treg function and immune tolerance, is suppressed.
Weight loss from GLP-1 medications reverses this imbalance. Leptin decreases. Adiponectin increases. The immune environment shifts from pro-autoimmune to anti-autoimmune. This may be one of the most straightforward mechanisms by which GLP-1 therapy benefits Hashimoto patients, even if it operates indirectly through progressive weight loss rather than direct immune modulation.
Weight loss with GLP-1 when you have Hashimoto
Let us address the elephant in the room. Can you actually lose weight on GLP-1 medications when your thyroid is working against you?
Yes. Most women with Hashimoto who use GLP-1 receptor agonists lose between 10 and 20 percent of their body weight over time, according to clinical observations from thyroid-focused medical practices. This is significant because many of these patients have failed multiple previous weight loss attempts due to the metabolic headwinds created by their autoimmune condition.
The reason GLP-1 medications work where diets fail for Hashimoto patients comes down to mechanism. Caloric restriction alone does not address insulin resistance, does not reduce leptin-driven inflammation, and does not improve the hormonal environment perpetuating weight gain. GLP-1 medications hit all three simultaneously.
What to expect timeline-wise
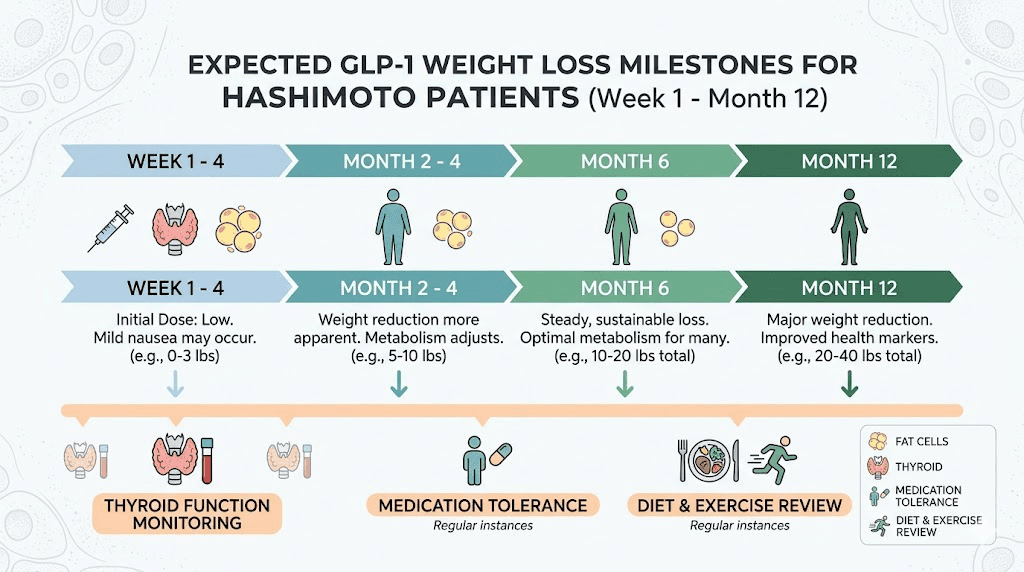
Hashimoto patients may respond differently than the general population. Some important considerations for your weight loss timeline:
Weeks 1 through 4: Appetite suppression begins. Nausea and GI side effects are most common in this period. Weight loss typically starts, though it may be slower than in patients without thyroid conditions. First month results vary widely. Do not compare your progress to social media transformations from people without autoimmune conditions.
Weeks 4 through 12: This is the critical window. Your body begins adapting to the medication, side effects typically diminish, and a more consistent weight loss pattern emerges. During this period, your thyroid labs need rechecking, because weight loss itself changes how your body processes thyroid hormone. More on this shortly.
Months 3 through 6: Sustained weight loss continues. If you are going to see inflammatory marker improvements, they typically become apparent in this window. Some patients report reduced joint pain, improved energy, and better cognitive function, improvements that go beyond what weight loss alone would explain.
Months 6 through 12: Weight loss plateaus are common and normal. If you hit a semaglutide plateau or stall on tirzepatide, it does not necessarily mean the medication has stopped working. Metabolic adaptation occurs in everyone, and Hashimoto patients may plateau earlier due to their underlying metabolic dysfunction.
Why some Hashimoto patients do not lose weight on GLP-1
Not everyone responds. If you find yourself not losing weight on semaglutide or not losing weight on tirzepatide, your thyroid condition may be a factor. Undertreated hypothyroidism, poorly optimized levothyroxine dosing, or unaddressed T3 deficiency can all blunt GLP-1 response.
Before concluding that GLP-1 medication is not working, ensure your thyroid optimization is complete. Check not just TSH but also free T3, free T4, reverse T3, and thyroid antibodies. The metabolic environment must support weight loss for GLP-1 medications to produce their full effect.
How GLP-1 medications affect thyroid hormones and TSH
This section matters more than most articles acknowledge. GLP-1 medications change your thyroid hormone dynamics, and if your provider is not monitoring appropriately, you could end up over-medicated on levothyroxine without realizing it.
Here is what happens. When you lose weight, your body requires less thyroid hormone. This is basic physiology. Less tissue means less metabolic demand means lower thyroid hormone requirements. A Pharmacy Times study found that patients on semaglutide who lost more than 5 pounds experienced an average TSH decrease of 0.55 mU/L. That is clinically significant. If your TSH was sitting at a well-optimized 1.5 before starting GLP-1 therapy, a 0.55 decrease could push it below 1.0, potentially into the hyperthyroid range.
This means your levothyroxine dose may need to decrease as you lose weight. Not might. May.
The symptoms of levothyroxine over-medication can mimic GLP-1 side effects: acid reflux, insomnia, anxiety, heart palpitations, dizziness, and tremor. If you develop these symptoms after starting a GLP-1 medication, do not automatically assume they are GLP-1 side effects. Get your thyroid labs checked. You might be over-replaced on thyroid hormone rather than experiencing medication intolerance.
The levothyroxine absorption question
GLP-1 medications slow gastric emptying. That is one of their primary mechanisms for reducing appetite and blood sugar spikes. But slower gastric emptying also means medications you take orally spend more time in your stomach before reaching the small intestine where absorption occurs.
Does this affect levothyroxine absorption? The data is mixed. Semaglutide might change how your body absorbs levothyroxine, which is why thyroid specialists recommend checking thyroid labs before starting GLP-1 therapy and again 6 to 8 weeks after initiation. If your TSH rises unexpectedly after starting a GLP-1 medication, impaired levothyroxine absorption could be the culprit.
Practical solutions exist. Taking levothyroxine at bedtime rather than morning can help separate it from the peak gastric motility effects of GLP-1 medications. Some patients find that liquid levothyroxine or soft-gel formulations absorb more reliably than tablets when gastric motility is altered. Discuss these options with your prescriber if absorption becomes a concern.
The estrogen connection
Adipose tissue produces estrogen through aromatase activity. When you lose significant fat mass on GLP-1 medications, your systemic estrogen levels may decrease. This matters for Hashimoto patients because estrogen influences thyroid-binding globulin (TBG) levels, which affects how much free (active) thyroid hormone is available to your tissues.
The relationship is complex. Semaglutide and estrogen levels interact in ways that can influence your thyroid labs and symptoms. If you are taking oral estrogen (birth control or HRT), the interaction becomes even more nuanced because oral estrogen increases TBG, which increases levothyroxine requirements. Losing fat on GLP-1 therapy while taking oral estrogen creates opposing forces on your thyroid hormone economy.
Bottom line: thyroid management during GLP-1 therapy requires more frequent monitoring than most patients realize. Every significant weight change, every medication adjustment, warrants a lab check.
Semaglutide versus tirzepatide for Hashimoto patients
Which GLP-1 medication is better if you have Hashimoto? This is the question everyone asks, and the honest answer is that no head-to-head trials exist in this specific population. But we can reason from the available data.
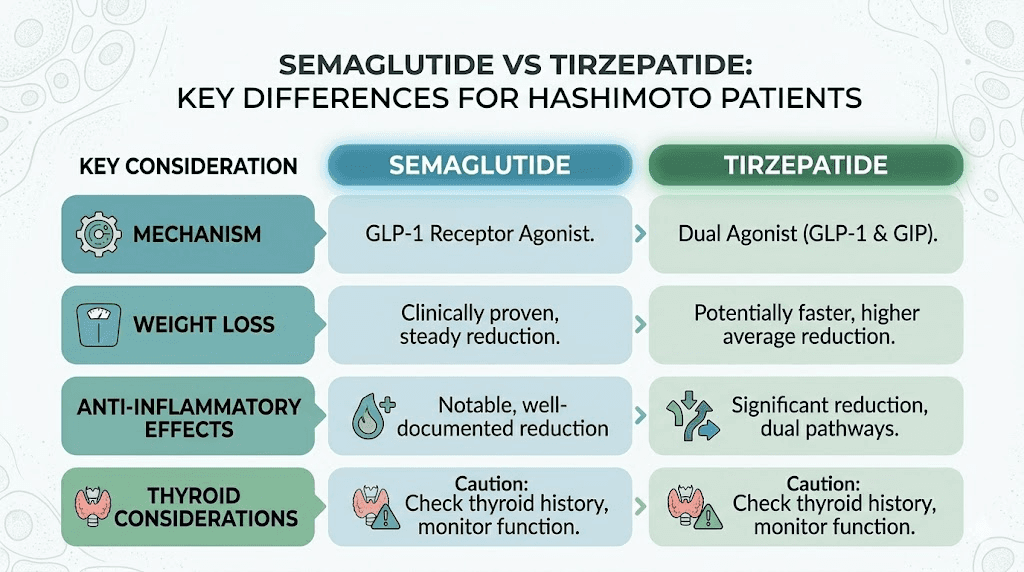
Semaglutide is a pure GLP-1 receptor agonist. It targets only GLP-1 receptors and produces its effects through a single pathway. The semaglutide versus tirzepatide comparison starts here, with mechanism of action.
Tirzepatide is a dual agonist, targeting both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. This dual mechanism produces greater weight loss in head-to-head trials and may offer additional metabolic benefits through GIP receptor activation.
For Hashimoto patients specifically, several factors deserve consideration:
Weight loss magnitude. Tirzepatide produces approximately 5 to 7 percent greater weight loss than semaglutide in clinical trials. Greater weight loss means greater reduction in inflammatory adipose tissue, greater leptin reduction, and potentially greater improvement in the metabolic dysfunction driving your autoimmune condition. If maximum weight loss is your primary goal, tirzepatide has the stronger evidence. Check tirzepatide before and after results for real-world outcomes.
Anti-inflammatory effects. Both medications reduce inflammatory markers. Whether tirzepatide dual agonism provides additional anti-inflammatory benefit beyond what semaglutide achieves is not yet clear from the literature. The GIP receptor component may add immunomodulatory effects, but this has not been studied specifically in autoimmune populations.
Side effect profile. Side effect differences between semaglutide and tirzepatide matter when you already have GI symptoms from your thyroid condition. Hashimoto patients frequently experience constipation, bloating, and altered gut motility. GLP-1 medications can worsen these symptoms, at least initially. Some patients tolerate one medication better than the other, and there is no way to predict which without trying.
Thyroid safety data. Both semaglutide and tirzepatide carry the same boxed warning about thyroid C-cell tumors based on rodent studies. The risk in humans appears minimal, as human thyroid cells show little to no GLP-1 receptor expression. However, the warning exists, and tirzepatide and thyroid nodule concerns should be discussed with your endocrinologist. One case report described tirzepatide-associated thyroiditis, though this was an isolated finding.
Cost and access. Both medications are expensive without insurance. If you are considering compounded versions, understand the regulatory landscape. Compounded tirzepatide options and compounded semaglutide exist but carry their own considerations around quality and consistency. Insurance coverage for GLP-1 varies widely and often requires specific diagnostic criteria.
Microdosing GLP-1 for autoimmune conditions
An emerging approach that deserves attention is microdosing GLP-1 for autoimmune conditions. The concept is straightforward: use lower-than-standard doses to capture anti-inflammatory benefits while minimizing side effects and excessive weight loss.
For Hashimoto patients, this approach has theoretical appeal. If the goal is immune modulation rather than maximum weight loss, lower doses might achieve sufficient receptor activation to produce anti-inflammatory effects without the significant GI side effects that make standard doses difficult for some patients to tolerate.
The evidence for microdosing in autoimmune conditions is preliminary at best. No clinical trials have evaluated low-dose GLP-1 therapy specifically for immune modulation. But some integrative and functional medicine practitioners are exploring this approach with their Hashimoto patients, reporting anecdotal improvements in antibody levels, energy, and inflammatory markers at doses well below the standard weight loss protocols.
If you are interested in this approach, microdosing tirzepatide charts and microdose tirzepatide schedules provide starting frameworks, though any autoimmune application should be supervised by a knowledgeable provider.
TPO antibody changes: what thyroid clinics are observing
This is the section that will matter most to many readers. Are GLP-1 medications actually reducing thyroid antibodies?
The short answer: some clinicians are observing antibody decreases, but the evidence is observational, not from controlled trials.
Modern Thyroid Clinic has reported that patients using GLP-1 medications show decreased TPO and thyroglobulin antibodies, with some patients achieving what they describe as remission. These are clinical observations from a practice specializing in thyroid care, not published peer-reviewed data. But they are observations from physicians who understand thyroid immunology and are tracking these markers systematically.
The mechanism is plausible. If GLP-1 medications reduce the inflammatory drivers of antibody production (NF-kB mediated cytokines, Th1/Th17 cell activity, leptin-driven immune activation), antibody levels should decrease as a downstream consequence. The immune system produces fewer antibodies when the signals telling it to produce those antibodies diminish.
However, correlation is not causation. Patients using GLP-1 medications are also losing weight, improving their diets, exercising more consistently, and potentially making other lifestyle changes that independently reduce thyroid antibodies. Separating the GLP-1 specific effect from the weight-loss-and-lifestyle effect requires the kind of controlled trials that do not yet exist.
What we can say with confidence is this: weight loss itself, regardless of how it is achieved, tends to reduce autoimmune antibody levels. Less adipose tissue means less inflammatory signaling, which means less immune activation, which means less antibody production. GLP-1 medications may provide additional immune-modulating benefit beyond weight loss, but proving that requires controlling for weight loss as a variable, and no study has done that for thyroid autoimmunity.
The gut-thyroid axis and how GLP-1 fits in
The connection between gut health and thyroid function is one of the most active areas of autoimmune thyroid research. And it is directly relevant to GLP-1 therapy.
Hashimoto patients frequently have altered gut microbiomes compared to healthy controls. They show reduced diversity, decreased populations of short-chain fatty acid (SCFA) producing bacteria, and increased intestinal permeability, commonly called "leaky gut." These gut changes are not just a consequence of thyroid dysfunction. They may actively drive the autoimmune process by allowing bacterial components to enter the bloodstream and trigger immune responses that cross-react with thyroid tissue.
GLP-1 receptor agonists influence the gut microbiome in several ways. Research shows they produce favorable shifts in gut bacteria composition, including enrichment of SCFA-producing species. They also improve gut barrier integrity by enhancing tight junction protein expression, potentially reducing the intestinal permeability that contributes to autoimmune activation.
For Hashimoto patients, these gut effects represent another pathway through which GLP-1 therapy might influence their autoimmune condition. Better gut barrier function means fewer immune triggers crossing into the bloodstream. More SCFA-producing bacteria means more anti-inflammatory metabolites. A healthier microbiome means better immune regulation overall.
Supporting your gut during GLP-1 therapy amplifies these benefits. Choosing the right probiotic for semaglutide therapy matters. Fiber supplementation during GLP-1 use supports SCFA production. And managing common GI side effects like semaglutide constipation or tirzepatide constipation is especially important for Hashimoto patients whose gut function is already compromised.
Practical gut support during GLP-1 therapy for Hashimoto patients
Your gut needs extra attention when you are combining GLP-1 medication with an autoimmune thyroid condition. Both Hashimoto and GLP-1 medications affect gut motility, and stacking those effects without support can create significant digestive discomfort.
Focus on fiber-rich foods that your slowed digestion can handle. Foods to eat on semaglutide and foods for tirzepatide users overlap significantly with anti-inflammatory dietary recommendations for Hashimoto. Prioritize cooked vegetables over raw, fermented foods for probiotic support, and adequate protein to prevent the muscle loss that both conditions can promote.
Avoid the foods that worsen both your thyroid condition and your GLP-1 side effects. Foods to avoid on semaglutide and foods to avoid on tirzepatide include highly processed foods, excessive sugar, and fatty fried foods, all of which also drive inflammation in autoimmune conditions. Many Hashimoto patients also benefit from reducing gluten and dairy, though this is individualized and not universally necessary.
Safety considerations specific to Hashimoto patients
GLP-1 medications are generally considered safe for Hashimoto patients, but several specific considerations warrant careful discussion with your endocrinologist.
The thyroid C-cell tumor warning
Every GLP-1 receptor agonist carries a boxed warning about thyroid C-cell tumors, specifically medullary thyroid carcinoma (MTC). This warning comes from rodent studies where GLP-1 receptor activation caused C-cell hyperplasia and tumors. The concern is not theoretical, it is real enough to warrant the FDA strongest warning category.
However, context matters enormously. Rodent thyroid C-cells express GLP-1 receptors at much higher density than human C-cells. Humans show minimal or absent GLP-1 receptor expression in thyroid follicular cells. Large-scale clinical trials (SUSTAIN, STEP, SURPASS) and extensive post-marketing surveillance have not demonstrated increased MTC incidence in humans taking GLP-1 medications.
For Hashimoto patients, the relevant question is whether pre-existing thyroid inflammation or autoimmunity changes the risk profile. The answer, based on current evidence, is that it does not appear to. But this has not been studied specifically, and patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) should absolutely not use GLP-1 medications regardless of their Hashimoto status.
Bone density concerns
Rapid weight loss from any cause can reduce bone density. Hashimoto patients may already have compromised bone metabolism due to thyroid hormone fluctuations. Tirzepatide and bone loss is an active area of investigation. Adding GLP-1-induced rapid weight loss to an already-compromised skeletal situation requires monitoring.
Ensure adequate calcium and vitamin D intake. Consider a DEXA scan before starting GLP-1 therapy if you have additional risk factors for osteoporosis. Resistance training helps preserve both bone density and lean muscle mass during weight loss, both of which are important for Hashimoto patients.
Muscle mass preservation
GLP-1 medications cause weight loss that includes both fat and lean mass. For Hashimoto patients who may already struggle with muscle weakness and fatigue, losing additional muscle is counterproductive. Adequate protein intake becomes critical. Supplements to take with GLP-1 therapy should include protein supplementation if dietary intake is insufficient, along with creatine for lean mass support.
Fertility and pregnancy considerations
GLP-1 medications require discontinuation before conception. Semaglutide should be stopped at least 2 months before attempting pregnancy. Tirzepatide requires at least 1 month of washout. For Hashimoto patients planning pregnancy, which already requires careful thyroid hormone management, the timing of GLP-1 discontinuation adds another variable to coordinate with your reproductive endocrinologist.
Interestingly, some patients report unexpected fertility improvements on GLP-1 therapy, potentially due to improved ovulation from weight loss and reduced inflammation. Getting pregnant on tirzepatide is a real scenario that Hashimoto patients should plan for, not be surprised by.
Menstrual cycle effects
Both Hashimoto and GLP-1 medications can independently affect menstrual cycles. Semaglutide and menstrual changes are well-documented, and tirzepatide and period changes occur as well. When you stack these effects with the hormonal fluctuations of autoimmune thyroid disease, menstrual irregularity becomes more likely. Track your cycle carefully and report changes to your provider.
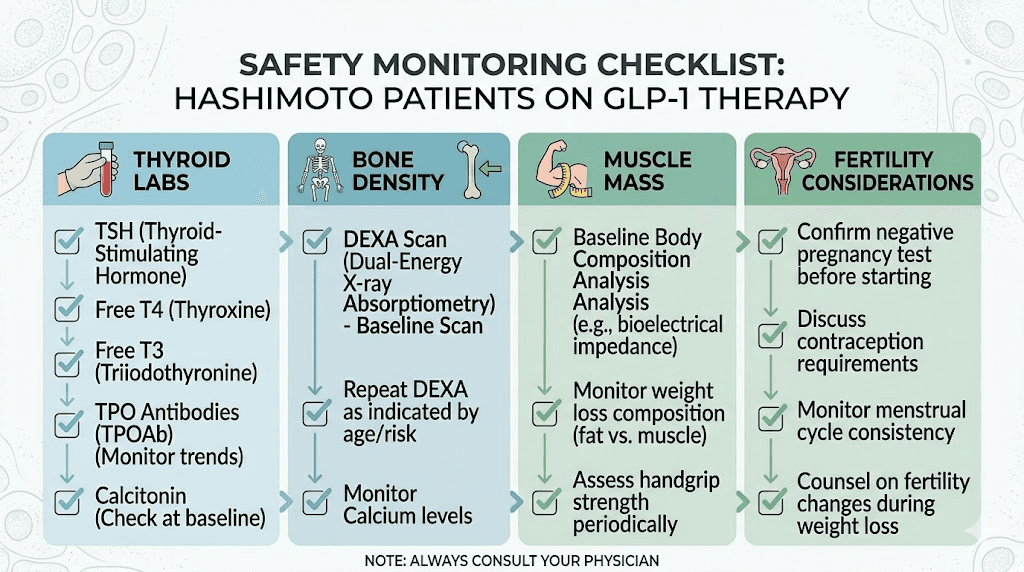
The monitoring protocol every Hashimoto patient on GLP-1 needs
If you are using or considering GLP-1 therapy with Hashimoto, rigorous monitoring is not optional. Here is what should be tracked and when.
Before starting GLP-1 therapy
Baseline labs: TSH, free T4, free T3, reverse T3, TPO antibodies, thyroglobulin antibodies, fasting insulin, HbA1c, comprehensive metabolic panel, CBC, CRP, and lipid panel. This comprehensive baseline allows you to track which markers change and by how much.
Body composition assessment: Weight alone is insufficient. Track body fat percentage, lean mass, and waist circumference. This matters because Hashimoto patients need to preserve lean mass during weight loss more aggressively than the general population.
Current levothyroxine dose and timing: Document exactly what you are taking, when you take it, and how you take it (empty stomach, with food, time of day). This baseline becomes critical when adjustments are needed later.
At 8 to 12 weeks after starting
This is the most critical monitoring window. Thyroid labs should be rechecked at this point, including TSH, free T4, and free T3. If you have lost more than 5 pounds, expect TSH changes. If TSH has dropped below your target range, levothyroxine dose reduction is likely needed.
Also recheck CRP at this point. An early decrease in CRP suggests the anti-inflammatory effects of GLP-1 therapy are active, which may predict longer-term benefit for your autoimmune condition.
After major weight changes
Any time you lose 10 or more pounds, repeat thyroid labs. The TSH study mentioned earlier showed that every significant weight change event correlates with thyroid hormone requirement changes. Hashimoto patients are more sensitive to these shifts because their remaining thyroid tissue has limited reserve capacity.
Every 3 to 6 months on stable therapy
Once your weight and GLP-1 dose have stabilized, standard monitoring every 3 to 6 months is appropriate. Include thyroid antibodies (TPO and TgAb) at these intervals to track whether the autoimmune process is improving, stable, or progressing despite therapy.
Symptoms to report immediately
Certain symptoms during GLP-1 therapy in Hashimoto patients warrant urgent attention. Heart palpitations, severe anxiety, tremor, and heat intolerance could indicate thyrotoxicosis from levothyroxine over-replacement. A case report published in PMC documented semaglutide-associated iatrogenic thyrotoxicosis, where weight loss reduced thyroid hormone requirements but the levothyroxine dose was not adjusted, leading to hyperthyroid symptoms.
Neck swelling or pressure could indicate thyroid inflammation. Severe fatigue on semaglutide that worsens rather than improves could mean your thyroid function is declining faster than your medication is compensating. New or worsening hair loss could indicate either thyroid deterioration or the effects of rapid weight loss on hair growth cycles.
Practical considerations for getting started
If you and your endocrinologist decide GLP-1 therapy is worth trying alongside your Hashimoto management, here are the practical details that matter.
Which medication form to choose
GLP-1 medications come in injectable and oral forms. For Hashimoto patients already taking daily oral levothyroxine, the injection format is often preferable because it avoids any potential interaction with oral medication absorption.
If you choose injectable semaglutide, understanding the best injection sites and proper injection technique matters for consistent absorption. GLP-1 injection site selection affects both absorption speed and comfort.
Oral semaglutide drops and sublingual semaglutide are alternatives for patients who prefer to avoid injections, but they add complexity to an oral medication routine that already includes levothyroxine. Timing becomes critical when you have two oral medications with specific absorption requirements.
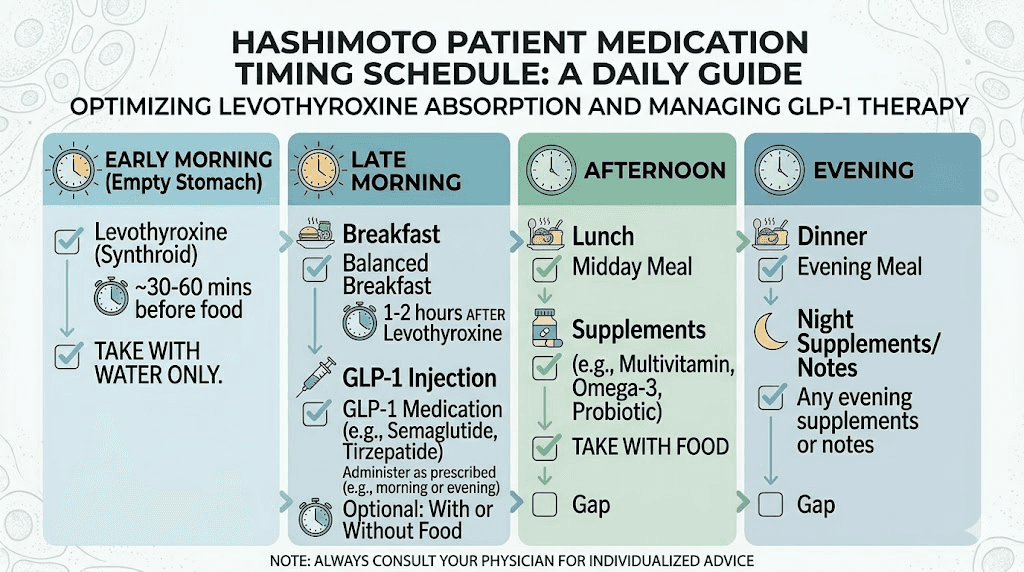
Timing your medications
Levothyroxine requires an empty stomach and at least 30 to 60 minutes before food or other medications. GLP-1 oral formulations have their own timing requirements. Separating these medications adequately can be challenging.
A practical approach: take levothyroxine first thing in the morning on an empty stomach. Wait at least 60 minutes. Then proceed with your normal routine. If you are using injectable GLP-1, the injection can happen at any time that is convenient. The best time to take semaglutide for Hashimoto patients is whenever it does not interfere with levothyroxine absorption.
Some patients find that taking levothyroxine at bedtime (at least 3 hours after their last meal) works better when GLP-1 medications are slowing morning gastric emptying. This separates the two medications entirely and may improve levothyroxine absorption.
Managing side effects alongside thyroid symptoms
Nausea, constipation, and fatigue are common with both GLP-1 initiation and Hashimoto disease. When you experience these symptoms, determining the cause matters for management.
GLP-1 nausea typically improves over 2 to 4 weeks. Hashimoto nausea is more constant. Sulfur burps on GLP-1 are a medication-specific side effect. GLP-1 headaches may occur during initiation but should resolve; persistent headaches warrant thyroid lab checks.
Keep a symptom journal during the first 12 weeks. Note timing, severity, and relationship to meals and medications. This data helps your provider distinguish GLP-1 side effects from thyroid dysfunction and adjust both treatments appropriately.
Supplement considerations
Several supplements are particularly relevant when combining GLP-1 therapy with Hashimoto management. Supplements for tirzepatide users and supplements for GLP-1 users overlap with Hashimoto supplement protocols in many areas.
Selenium supports thyroid peroxidase function and has evidence for reducing TPO antibodies independently. Vitamin D deficiency is common in both autoimmune thyroid disease and obesity, making supplementation doubly important. Zinc supports both thyroid hormone conversion and immune regulation. B12 with semaglutide is worth considering because both Hashimoto and GLP-1 medications can affect B12 status.
Iron supplementation should be separated from both levothyroxine and GLP-1 oral medications by at least 4 hours, as it interferes with levothyroxine absorption and GLP-1 medications may further complicate iron uptake.
When GLP-1 therapy might not be appropriate for Hashimoto patients
GLP-1 medications are not universally appropriate, and several Hashimoto-specific situations warrant caution or avoidance.
Personal or family history of medullary thyroid carcinoma or MEN2. This is an absolute contraindication. No exceptions. No nuance. If you have this history, GLP-1 medications are not for you.
Actively unstable thyroid function. If your Hashimoto is in a destructive phase with rapidly changing thyroid levels, adding a GLP-1 medication creates too many moving variables. Stabilize your thyroid function first, then consider GLP-1 therapy once your levothyroxine dose has been consistent for at least 3 months.
Severe gastroparesis. Some Hashimoto patients develop gastroparesis from thyroid-related autonomic dysfunction. GLP-1 medications further slow gastric emptying, which can worsen gastroparesis to a dangerous degree. If you have delayed gastric emptying from any cause, discuss this specifically with your prescriber.
History of pancreatitis. GLP-1 medications carry a warning for pancreatitis risk. Hashimoto does not increase this risk, but if you have a personal history of pancreatitis, the GLP-1 warning applies regardless of your thyroid status.
Pregnancy or active fertility treatment. As discussed earlier, GLP-1 medications must be discontinued before conception. If you are actively trying to conceive or undergoing fertility treatment, GLP-1 therapy is not appropriate during that period. Breastfeeding on GLP-1 is similarly contraindicated.
Underweight or insufficient body fat. If your Hashimoto has not caused weight gain, or if you are already at a healthy weight, the rationale for GLP-1 therapy weakens considerably. The anti-inflammatory benefits, while real, are largely tied to adipose tissue reduction and metabolic improvement. If you do not have excess adipose tissue to reduce, the risk-benefit calculus shifts unfavorably.
The real-world evidence gap and why it matters
Let us be direct about what we do not know.
The 2025 narrative review in Cureus analyzed 68 articles on GLP-1 receptor agonists and autoimmune thyroid disease. Among all 68 studies reviewed, zero were randomized controlled trials specifically evaluating GLP-1 medications for autoimmune thyroid disease. Zero. The evidence base consists of mechanistic studies in non-thyroid tissues, secondary analyses from diabetes and obesity trials, case reports, and clinical observations.
This does not mean GLP-1 therapy is useless for Hashimoto. It means we lack the evidence quality to make definitive claims. The mechanisms are plausible. The clinical observations are encouraging. The safety profile in thyroid patients appears acceptable. But "plausible" and "encouraging" are not "proven" and "established."
What would change this? Dedicated clinical trials that specifically evaluate GLP-1 receptor agonists in Hashimoto patients, with thyroid antibody trajectories as primary endpoints, weight-loss-controlled comparator arms, and sufficient follow-up to assess disease modification rather than just symptom improvement. Until those trials exist, we are working with informed speculation supported by strong mechanistic rationale.
For patients, this means approaching GLP-1 therapy for Hashimoto with calibrated expectations. If weight loss is your primary goal and you have Hashimoto, GLP-1 medications are evidence-supported for weight loss regardless of thyroid status. If immune modulation is your primary goal, the evidence is hypothesis-generating, not practice-changing. If you are hoping for both, that is reasonable, but monitor your expectations alongside your lab values.
What other autoimmune conditions tell us
While direct evidence for Hashimoto is limited, GLP-1 medications are being studied in several other autoimmune and inflammatory conditions. These parallel investigations provide context for what might be possible in thyroid autoimmunity.
GLP-1 and endometriosis research shows that 64.6% of survey participants reported improvement in at least one endometriosis symptom while on GLP-1 therapy. GLP-1 and lipedema is another autoimmune-adjacent condition where these medications show promise through anti-inflammatory mechanisms.
In cardiovascular disease, GLP-1 receptor agonists have demonstrated clear anti-inflammatory benefits that translate to reduced cardiovascular events, outcomes supported by large randomized trials. In non-alcoholic fatty liver disease, GLP-1 therapy reduces liver inflammation and fibrosis. In psoriasis, another autoimmune condition, case reports describe improvement during GLP-1 therapy.
The pattern across conditions is consistent. GLP-1 receptor activation reduces inflammation. Reduced inflammation improves autoimmune-related outcomes. Whether this pattern holds for thyroid autoimmunity specifically remains to be proven, but the consistency across other conditions is encouraging.
A word of caution about the autoimmune thyroiditis risk signal
Transparency requires discussing a finding that goes against the optimistic narrative. A real-world evidence study using large insurance databases found that patients receiving GLP-1 receptor agonists exhibited a significantly higher risk of autoimmune thyroiditis compared to those taking DPP-4 inhibitors (hazard ratio 1.30, 95% confidence interval 1.24 to 1.38).
This is a concerning signal that deserves explanation rather than dismissal. There are several possible interpretations:
Detection bias. Patients on GLP-1 medications receive more medical attention and more frequent lab monitoring, which could lead to higher detection rates of autoimmune thyroiditis that would otherwise go undiagnosed. This does not mean GLP-1 caused the thyroiditis; it means it was found because someone was looking.
Confounding by indication. Patients prescribed GLP-1 medications tend to have obesity and metabolic dysfunction, conditions that independently increase autoimmune thyroid risk. The association may reflect the patient population rather than the medication effect.
True biological effect. It is possible that GLP-1 receptor activation in certain individuals triggers or unmasks autoimmune thyroid processes. The mechanism could involve immune system modulation that, in some cases, tips the balance toward rather than away from autoimmunity.
This finding does not mean GLP-1 medications cause Hashimoto. But it does mean that thyroid monitoring during GLP-1 therapy is genuinely important, not just a precautionary recommendation. If you develop new thyroid symptoms during GLP-1 therapy, get tested. And if you have known Hashimoto, track your antibody levels to ensure they are moving in the right direction.
Combining GLP-1 with other Hashimoto interventions
GLP-1 therapy does not exist in isolation. Most Hashimoto patients are managing their condition with multiple interventions simultaneously. Understanding how GLP-1 fits into a broader management strategy helps maximize benefit.
GLP-1 plus levothyroxine
This is the most common combination. As discussed, the key considerations are medication timing, absorption monitoring, and dose adjustments as weight changes. Limited observational data suggests GLP-1 receptor agonists do not adversely affect thyroid function in patients maintained on stable levothyroxine. The interaction is primarily pharmacokinetic (absorption changes) rather than pharmacodynamic (opposing effects).
GLP-1 plus low-dose naltrexone (LDN)
Some integrative practitioners use LDN for Hashimoto immune modulation. Combining LDN with GLP-1 therapy has not been studied, but mechanistically they target complementary immune pathways. LDN primarily modulates endorphin signaling and Treg function, while GLP-1 targets NF-kB and inflammasome pathways. The combination could theoretically provide broader immune modulation than either alone.
GLP-1 plus metformin
Many Hashimoto patients with insulin resistance take metformin. Combining metformin with semaglutide is well-studied in the diabetes population and generally well-tolerated. For Hashimoto patients, this combination addresses insulin resistance from two directions, which may provide greater metabolic improvement than either medication alone.
GLP-1 plus dietary interventions
Anti-inflammatory diets (Mediterranean, autoimmune protocol, or modified elimination diets) complement GLP-1 therapy by reducing dietary inflammatory triggers while the medication addresses systemic inflammatory pathways. A semaglutide diet plan or tirzepatide diet plan should be adapted for Hashimoto by incorporating thyroid-supportive foods (selenium-rich brazil nuts, zinc-containing pumpkin seeds, iodine-appropriate seafood) while avoiding potential triggers.
The bottom line for Hashimoto patients considering GLP-1
Let us distill everything into what you actually need to know to make a decision.
The case for trying GLP-1 with Hashimoto: Strong mechanistic rationale for anti-inflammatory and immunomodulatory benefits. Proven weight loss efficacy that addresses a primary Hashimoto symptom. Clinical observations of antibody reductions. Favorable safety profile in thyroid patients when properly monitored. Multiple complementary pathways addressing the metabolic dysfunction that Hashimoto creates.
The case for caution: Zero dedicated clinical trials in Hashimoto patients. A real-world signal of increased autoimmune thyroiditis detection on GLP-1 therapy. Need for more frequent thyroid monitoring than non-thyroid patients. Risk of levothyroxine over-replacement if weight loss is not matched with dose adjustments. Significant cost. Side effects that may compound existing Hashimoto GI symptoms.
The practical path forward: If weight loss is needed and you have Hashimoto, GLP-1 medications are reasonable options with proper monitoring. If you are hoping for autoimmune disease modification, maintain realistic expectations while tracking antibody levels. Work with a provider who understands both GLP-1 pharmacology and thyroid autoimmunity, because the intersection requires expertise in both domains.
For researchers serious about optimizing their peptide protocols and understanding how GLP-1 medications interact with complex conditions like Hashimoto disease, SeekPeptides offers the most comprehensive resource available. SeekPeptides members access evidence-based guides, detailed protocol databases, and a community of thousands who have navigated these exact questions about thyroid autoimmunity and peptide therapy. From semaglutide dosage calculators to comprehensive safety guides, SeekPeptides provides the tools and knowledge base that complex conditions like Hashimoto demand.
Frequently asked questions
Can I take semaglutide or tirzepatide if I have Hashimoto thyroiditis?
Yes, GLP-1 medications are not contraindicated for Hashimoto patients. They are safe for most people with autoimmune thyroid disease, provided you do not have a personal or family history of medullary thyroid carcinoma or MEN2. Work with an endocrinologist who can monitor your semaglutide dosing alongside your thyroid labs.
Will GLP-1 medications cure my Hashimoto disease?
No. GLP-1 medications are not disease-modifying therapies for Hashimoto. They may reduce inflammation and potentially lower antibody levels, but they do not stop the autoimmune process. They are best viewed as complementary tools alongside thyroid hormone replacement and other management strategies.
Do I need to adjust my levothyroxine dose when starting a GLP-1 medication?
Likely yes, but not immediately. As you lose weight, your thyroid hormone requirements typically decrease. Check thyroid labs 8 to 12 weeks after starting GLP-1 therapy and again after every significant weight change (10 or more pounds). Your prescriber may need to reduce your levothyroxine dose to prevent over-replacement.
Which is better for Hashimoto, semaglutide or tirzepatide?
No head-to-head trials exist in Hashimoto patients. Tirzepatide produces greater weight loss in general populations, which may translate to greater inflammatory reduction. Both have similar anti-inflammatory mechanisms. The semaglutide versus tirzepatide comparison comes down to individual tolerance, cost, and access. Try the one your provider recommends and switch if needed.
Can GLP-1 medications reduce my TPO antibodies?
Some thyroid clinics report observing decreased TPO and thyroglobulin antibodies in patients using GLP-1 medications. However, this has not been demonstrated in controlled clinical trials. Weight loss itself tends to reduce autoimmune antibodies regardless of how it is achieved, so separating the GLP-1-specific effect from the weight-loss effect remains unclear.
Will GLP-1 medications interfere with my levothyroxine absorption?
Possibly. GLP-1 medications slow gastric emptying, which can affect how oral medications are absorbed. Monitor thyroid labs after starting GLP-1 therapy. If TSH rises unexpectedly, consider switching levothyroxine to bedtime dosing or using liquid formulations. Timing your semaglutide injection separately from oral medications helps minimize interactions.
Is microdosing GLP-1 effective for Hashimoto autoimmunity?
Microdosing GLP-1 for autoimmune conditions is an emerging concept without clinical trial support. The theory is that lower doses may provide anti-inflammatory benefits with fewer side effects. Some practitioners report positive observations, but this remains experimental and should only be attempted under medical supervision.
How long should I stay on GLP-1 medication if I have Hashimoto?
There is no established duration for GLP-1 therapy in Hashimoto patients. For weight management, how long to stay on semaglutide depends on your individual response, goals, and whether you can maintain weight loss after discontinuation. If anti-inflammatory benefits are observed, longer-term therapy may be justified, but this should be an ongoing discussion with your provider.
External resources
The Thyroid Twist: How GLP-1 Agonists Are Influencing Autoimmune Thyroid Care (Cureus, 2025)
Serum levels of GLP-1 and GLP-2 in patients with Hashimoto thyroiditis (Peptides, 2015)
Implications of GLP-1 Receptor Agonist on Thyroid Function (PMC Literature Review)
GLP-1 Receptor Agonists and Thyroid Disorders: Meta-Analysis (Frontiers in Endocrinology)
How Semaglutide and Tirzepatide Affect the Thyroid (ThyForLife)
In case I do not see you, good afternoon, good evening, and good night. May your antibodies stay low, your energy stay high, and your thyroid stay supported.