Apr 1, 2026

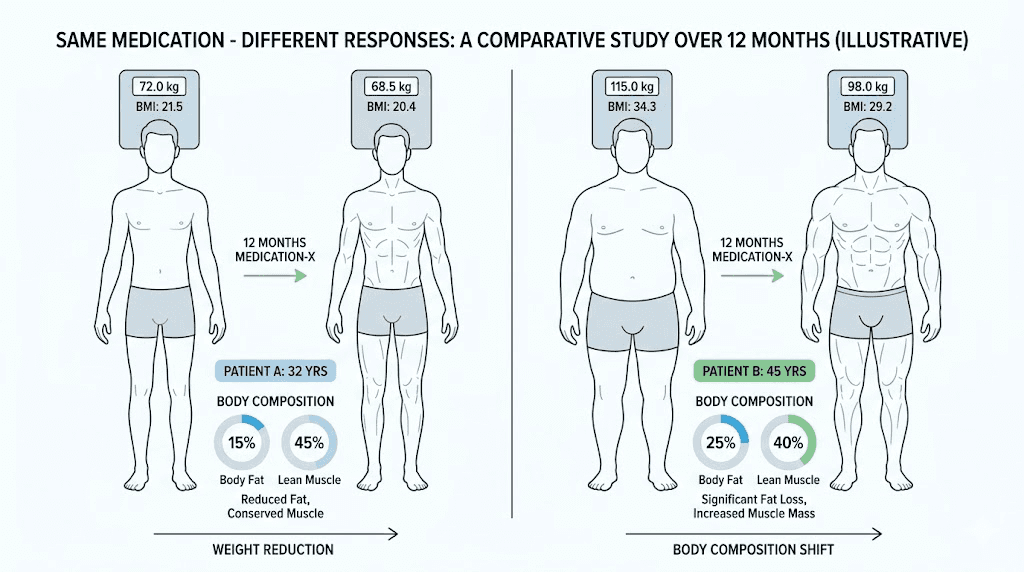
You have done everything right. The weekly injections, delivered on schedule. The dietary changes, followed to the letter. The patience, stretched across weeks that felt like months. And still, the scale has barely moved. The appetite suppression everyone raves about never quite arrived for you. The dramatic before-and-after transformations flooding social media feel like they belong to a different species entirely.
You are not imagining it.
Semaglutide does not work the same way for everyone. Clinical trial data from the landmark STEP program reveals that somewhere between 10 and 23 percent of participants qualified as non-responders, meaning they lost less than 5 percent of their total body weight despite months of consistent treatment. That is not a small number. For every ten people who start semaglutide for weight loss, at least one or two will wonder why the medication that transformed their friend or coworker seems to do almost nothing for them. The reasons span genetics, gut bacteria, hormonal conditions, medication interactions, dosing errors, and lifestyle factors that most prescribers never discuss in a fifteen-minute appointment. This guide breaks down every known factor behind semaglutide non-response, backed by clinical research and real-world data, so you can determine whether your body truly does not respond to this medication or whether something fixable is standing in the way of your results.
What the clinical data actually says about semaglutide non-responders
The word "non-responder" gets thrown around loosely in online forums and social media posts, but clinical researchers use a precise definition. In most major semaglutide clinical trials, a non-responder is someone who loses less than 5 percent of their baseline body weight after a full treatment course. That threshold matters because 5 percent body weight loss is the minimum amount considered clinically meaningful for reducing cardiovascular risk, improving blood sugar control, and lowering blood pressure.
The numbers tell a complicated story.
STEP trial non-responder rates
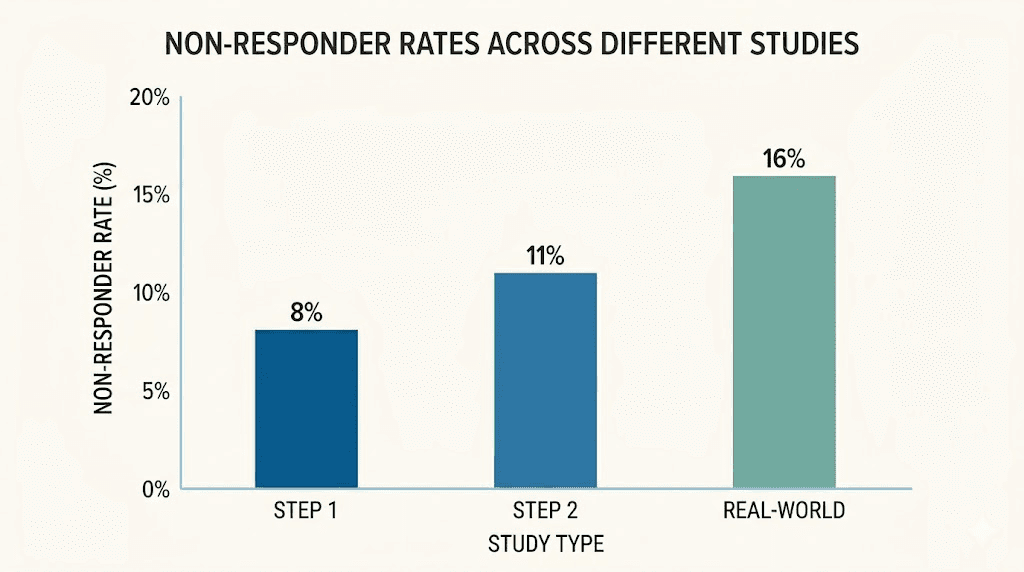
The STEP (Semaglutide Treatment Effect in People with obesity) trials represent the largest and most rigorous body of evidence on semaglutide for weight management. Across these trials, non-responder rates ranged from 10.2 to 16.7 percent, depending on the specific study population and duration. In STEP 1, which enrolled adults with obesity but without diabetes, only 7.6 percent of participants on the 2.4mg weekly dose lost less than 5 percent of their body weight at 68 weeks. That sounds encouraging until you look at STEP 2, which enrolled adults with both obesity and type 2 diabetes. In that population, the non-responder rate jumped to 26.8 percent, meaning more than one in four participants did not achieve clinically meaningful weight loss despite identical dosing protocols.
The difference between those two numbers reveals something important. The presence of type 2 diabetes appears to substantially reduce semaglutide effectiveness for weight loss, likely because the metabolic dysfunction underlying diabetes creates additional barriers that semaglutide alone cannot overcome. Insulin resistance, altered gut hormone signaling, and changes in energy metabolism all contribute to this gap.
Real-world data paints a different picture
Clinical trials are controlled environments. Participants receive regular follow-up, nutritional counseling, and the kind of accountability that most real-world patients simply do not get. So it should not surprise anyone that real-world non-responder rates run higher than trial data suggests.
Observational studies tracking semaglutide outcomes outside of clinical trials report non-responder rates between 17.8 and 22.5 percent. Some analyses suggest the number could be even higher when you account for people who discontinue treatment early due to side effects or perceived lack of results, people who never show up in the final data because they stopped before the study endpoint. The reality of compounded semaglutide not working follows similar patterns, with additional variables related to compounding quality and potency entering the equation.
One retrospective analysis found that among patients prescribed semaglutide in a primary care setting, roughly one in five achieved less than 5 percent weight loss after six months. Another study tracking insurance claims data found that 22 percent of patients discontinued semaglutide within the first three months, many citing insufficient results as their primary reason.
Gender differences in response rates
Perhaps the most striking finding in the non-responder literature involves gender. One study reported a male non-responder rate of 41.6 percent compared to just 14.2 percent for females. That gap is enormous. Men were nearly three times more likely to fail to achieve clinically meaningful weight loss on semaglutide compared to women.
Why? Several theories exist. Men tend to carry more visceral fat, which responds differently to GLP-1 receptor agonism than subcutaneous fat. Testosterone levels influence metabolic rate and fat distribution in ways that may partially counteract semaglutide mechanisms. Men also tend to have higher baseline caloric intake, meaning the appetite suppression from semaglutide, while present, may not create as large a caloric deficit in absolute terms. If you are a male wondering why you are not losing weight on semaglutide, this gender difference in response rates is worth understanding.
Psychiatric comorbidities and non-response
Another factor that emerged from the research is the overrepresentation of psychiatric disorders among semaglutide non-responders. One analysis found that 44.4 percent of non-responders had a documented psychiatric condition, compared to significantly lower rates in the responder group. Depression, anxiety, binge eating disorder, and other mental health conditions can all influence eating behavior in ways that counteract semaglutide appetite suppression. Emotional eating, stress-driven consumption, and medication-induced weight gain from psychiatric drugs create headwinds that a single GLP-1 receptor agonist may not be powerful enough to overcome alone.
This does not mean semaglutide cannot work for people with psychiatric conditions. It means these individuals may need additional support, whether through therapy, medication adjustments, or combination pharmacotherapy, to achieve the same results that metabolically healthier patients achieve with semaglutide alone. Understanding how semaglutide makes you feel can help identify whether the medication is producing any neurological effect at all, even if weight loss has not followed.
The genetics behind semaglutide response
Your DNA plays a bigger role in semaglutide response than most people realize. The medication works by mimicking GLP-1, a naturally occurring hormone that binds to GLP-1 receptors throughout the body. But not everyone has the same GLP-1 receptors. Genetic variations in the receptor itself, in the enzymes that metabolize semaglutide, and in the downstream signaling pathways all influence how effectively the drug does its job.
The GLP-1 receptor gene and known variants
The gene encoding the GLP-1 receptor is called GLP1R, and researchers have identified several single nucleotide polymorphisms (SNPs) within it that affect receptor function. The most studied variant in the context of semaglutide response is rs6923761, which produces what is known as the Gly168Ser substitution. This means that at position 168 of the receptor protein, the amino acid glycine is replaced by serine in individuals carrying this variant.
That single amino acid change matters. It alters the shape of the receptor binding pocket, affecting how tightly semaglutide binds and how efficiently the receptor activates downstream signaling cascades. Individuals carrying the Ser168 variant show reduced GLP-1 receptor signaling in laboratory studies, which translates to blunted appetite suppression, less insulin secretion enhancement, and potentially reduced weight loss outcomes.
This variant has been identified as a potential genetic biomarker for predicting semaglutide non-response, though clinical genetic testing for this purpose is not yet standard practice.
Other GLP1R variants under investigation include rs3765467 and rs10305420, both of which appear to modify receptor sensitivity to GLP-1 agonists. The emerging picture suggests that GLP-1 receptor genetics may account for a meaningful portion of the variability in treatment response, and that someday pharmacogenomic testing could help clinicians predict who will benefit most from semaglutide before they ever take their first week on the medication.
Metabolic enzyme variations
Beyond the receptor itself, genetic differences in how the body processes semaglutide can influence effectiveness. Semaglutide is primarily eliminated through proteolytic degradation and renal excretion, but variations in enzymes involved in these pathways can alter the drug half-life and steady-state concentration. Some individuals may metabolize semaglutide faster than average, resulting in lower circulating levels between weekly doses and reduced therapeutic effect.
This is one reason why semaglutide blood work monitoring can be valuable. While direct semaglutide level testing is not commonly available, markers like fasting insulin, HbA1c trends, and inflammatory markers can provide indirect evidence of whether the medication is producing its expected pharmacological effects.
Appetite regulation genetics
Weight regulation is polygenic, meaning hundreds of genes contribute to how your body manages hunger, satiety, metabolic rate, and fat storage. Variants in genes like MC4R (melanocortin 4 receptor), FTO (fat mass and obesity-associated gene), and LEPR (leptin receptor) all influence baseline appetite and metabolic setpoints in ways that can either enhance or diminish semaglutide effects.
Someone with a strongly appetite-promoting genetic profile might experience semaglutide as mildly helpful rather than transformative. The medication is working, reducing appetite signals by 30 or 40 percent perhaps, but when your baseline appetite drive is exceptionally high, that reduction may not translate to the dramatic results seen in people with more moderate baseline hunger. This helps explain why some individuals report that semaglutide does not suppress appetite immediately or as strongly as they expected.
The bottom line on genetics is sobering but important. An estimated 10 to 20 percent of semaglutide non-response can be attributed to genetic factors. You cannot change your DNA, but understanding its role helps set realistic expectations and guides decisions about alternative treatments.
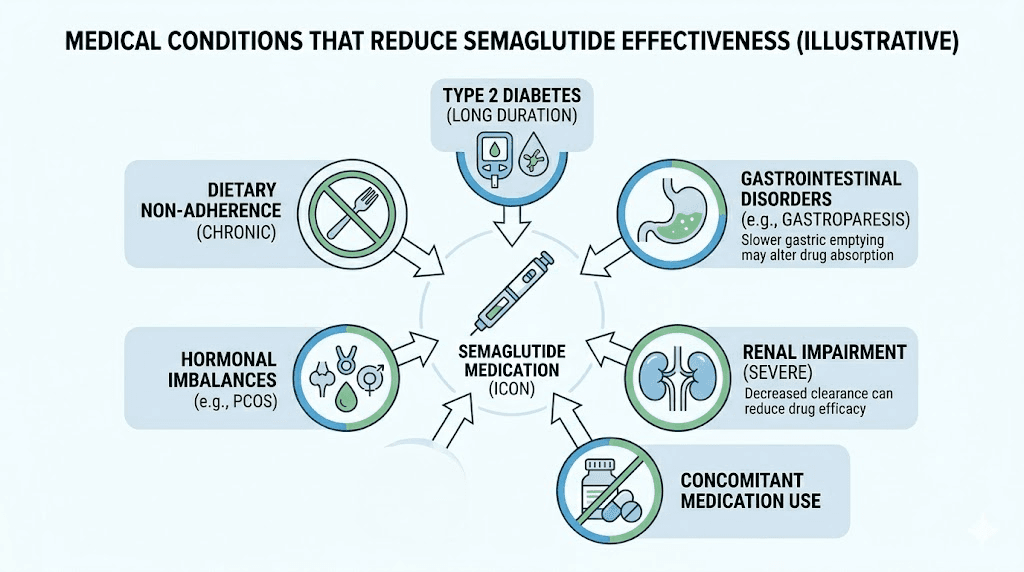
Medical conditions that reduce semaglutide effectiveness
Your body does not exist in a vacuum. Semaglutide enters a complex biological system where existing medical conditions, hormonal imbalances, and metabolic disruptions can all interfere with its mechanism of action. Several conditions stand out as particularly relevant to semaglutide non-response.
Hypothyroidism
The thyroid gland controls metabolic rate. When it underperforms, a condition called hypothyroidism, everything slows down. Calorie burning decreases. Fat storage increases. Energy levels plummet. And weight loss from any intervention, including semaglutide, becomes dramatically harder.
Subclinical hypothyroidism is especially tricky because standard thyroid screening (TSH alone) can miss it. A person might have a TSH of 4.2, technically within the normal reference range at many labs, but functionally high enough to impair metabolism. If you are experiencing semaglutide fatigue alongside poor weight loss results, thyroid function deserves a thorough evaluation including free T3, free T4, and thyroid antibodies, not just TSH.
The good news is that hypothyroidism is treatable. Optimizing thyroid function with appropriate medication can remove this barrier and allow semaglutide to work more effectively. Many people who appeared to be semaglutide non-responders turned out to have undiagnosed or undertreated thyroid conditions masking the medication effects.
Polycystic ovary syndrome (PCOS)
PCOS affects an estimated 8 to 13 percent of women of reproductive age and is strongly associated with insulin resistance, hormonal imbalance, and difficulty losing weight. The insulin resistance component is particularly relevant to semaglutide response because elevated insulin levels promote fat storage and oppose the mechanisms through which semaglutide facilitates weight loss.
Women with PCOS often have elevated androgens, disrupted hunger hormones, and altered gut hormone signaling that collectively reduce GLP-1 agonist effectiveness.
Research suggests that addressing insulin resistance directly, through medications like metformin or lifestyle modifications targeting insulin sensitivity, can improve semaglutide outcomes in this population. The relationship between semaglutide and estrogen levels adds another layer of complexity for women with hormonal conditions, and understanding how semaglutide affects menstrual cycles becomes especially important in this group.
Insulin resistance and metabolic syndrome
Even outside of PCOS and diabetes, standalone insulin resistance can hamper semaglutide results. Insulin resistance means your cells do not respond normally to insulin signaling, leading to higher circulating insulin levels, increased fat storage, and a metabolic environment that actively resists weight loss. The STEP 2 trial data, showing a 26.8 percent non-responder rate in people with type 2 diabetes compared to 7.6 percent in those without, illustrates just how powerfully insulin resistance can blunt semaglutide effectiveness.
Markers of insulin resistance include elevated fasting insulin, a high HOMA-IR score, elevated triglycerides, low HDL cholesterol, and increased waist circumference. If these markers are present, addressing insulin resistance through dietary changes (particularly reducing refined carbohydrates and increasing protein intake), exercise, and potentially combining metformin with semaglutide can improve outcomes.
Cushing syndrome and cortisol dysregulation
Cortisol, the primary stress hormone, directly opposes weight loss when chronically elevated. Cushing syndrome represents the extreme end of cortisol excess, but even subclinical cortisol elevation from chronic stress, sleep deprivation, or adrenal dysfunction can create a metabolic environment hostile to fat loss. Cortisol promotes visceral fat deposition, increases appetite (particularly for high-calorie comfort foods), and impairs insulin sensitivity, all of which work against semaglutide mechanisms.
Sleep apnea
Obstructive sleep apnea disrupts sleep architecture, increases sympathetic nervous system activation, elevates cortisol, promotes insulin resistance, and increases ghrelin (the hunger hormone) while decreasing leptin (the satiety hormone). This constellation of effects can significantly reduce semaglutide effectiveness. Many people with obesity have undiagnosed sleep apnea, and treating it, usually with CPAP therapy, can unlock weight loss results that were previously blocked.
If you experience loud snoring, daytime sleepiness, morning headaches, or observed breathing pauses during sleep, a sleep study could reveal a treatable condition that is undermining your semaglutide response. The relationship between semaglutide and sleep is bidirectional, because poor sleep impairs drug response, and the medication itself can sometimes affect sleep quality.
Medications that interfere with semaglutide
Your medicine cabinet might be sabotaging your semaglutide results. Several commonly prescribed medication classes can directly counteract weight loss or interfere with semaglutide pharmacology. This is an area where many patients and even some prescribers fail to connect the dots.
Corticosteroids
Prednisone, dexamethasone, methylprednisolone, and other systemic corticosteroids are among the most potent weight-gain-promoting medications in existence. They increase appetite dramatically, promote fat deposition (especially in the face, abdomen, and upper back), cause fluid retention, and induce insulin resistance. Even short courses of oral steroids can add several pounds, and chronic use creates a metabolic environment that directly opposes everything semaglutide is trying to do.
Inhaled corticosteroids for asthma and topical steroids for skin conditions are generally less problematic, though high-dose inhaled steroids can have systemic effects in some individuals. If you are on chronic oral corticosteroids, the combination with semaglutide may produce underwhelming results that have nothing to do with semaglutide itself failing.
Antidepressants and mood stabilizers
Several psychiatric medications cause significant weight gain, and this effect can partially or fully negate semaglutide-induced weight loss. The worst offenders include mirtazapine (which can cause 5 to 10 percent body weight gain), paroxetine, certain tricyclic antidepressants (amitriptyline, nortriptyline), lithium, valproic acid, and several atypical antipsychotics (olanzapine, clozapine, quetiapine).
The mechanism varies by drug. Some increase appetite centrally. Others alter metabolism. Some promote insulin resistance. A few do all three. When semaglutide is trying to reduce caloric intake by 20 to 30 percent but a psychiatric medication is simultaneously increasing hunger signals by a comparable amount, the net effect on body weight can be negligible. This helps explain why psychiatric comorbidities are so overrepresented among semaglutide non-responders, as noted in that 44.4 percent statistic.
Importantly, nobody should stop psychiatric medications to improve semaglutide results without careful medical guidance. But a conversation with prescribers about weight-neutral alternatives (bupropion instead of mirtazapine, for example) can sometimes remove a pharmacological barrier to weight loss while maintaining mental health treatment. Understanding all the ways semaglutide affects your body helps contextualize these interactions.
Insulin and sulfonylureas
This seems paradoxical. Insulin and sulfonylureas are diabetes medications, and semaglutide is also used for diabetes. But insulin, by its very nature, promotes fat storage. Sulfonylureas stimulate insulin secretion regardless of blood sugar levels, which can cause hypoglycemia-driven eating and weight gain. When these medications are combined with semaglutide, the weight loss effects of semaglutide can be partially offset by the weight-promoting effects of the diabetes drugs.
This is a known phenomenon in diabetology. The STEP 2 trial participants were on various background diabetes medications, and the higher non-responder rate in that population likely reflects, at least in part, the weight-promoting effects of concurrent diabetes pharmacotherapy.
Antihistamines
Chronic use of certain antihistamines, particularly older first-generation agents like diphenhydramine (Benadryl) and cyproheptadine, can promote weight gain through increased appetite and altered metabolism. The effect is usually modest, perhaps 2 to 5 pounds per year, but in the context of marginal semaglutide response, even small opposing forces matter. Second-generation antihistamines like cetirizine and loratadine have less weight impact, though some data suggests cetirizine may still contribute to modest weight gain with chronic use.
Beta-blockers
Certain beta-blockers, particularly older non-selective agents like propranolol and atenolol, can reduce metabolic rate by 5 to 10 percent and promote weight gain. Newer beta-blockers like carvedilol and nebivolol tend to be more weight-neutral. If you are taking a beta-blocker and experiencing poor semaglutide response, discussing newer alternatives with your cardiologist could be worthwhile.
The key takeaway here is simple. If semaglutide does not seem to be working, a thorough medication review should be one of the first steps. Many people are taking two or three medications that promote weight gain while simultaneously trying to lose weight with semaglutide, creating a pharmacological tug-of-war where nobody wins. Combining certain supplements with semaglutide also requires careful consideration to avoid interactions.
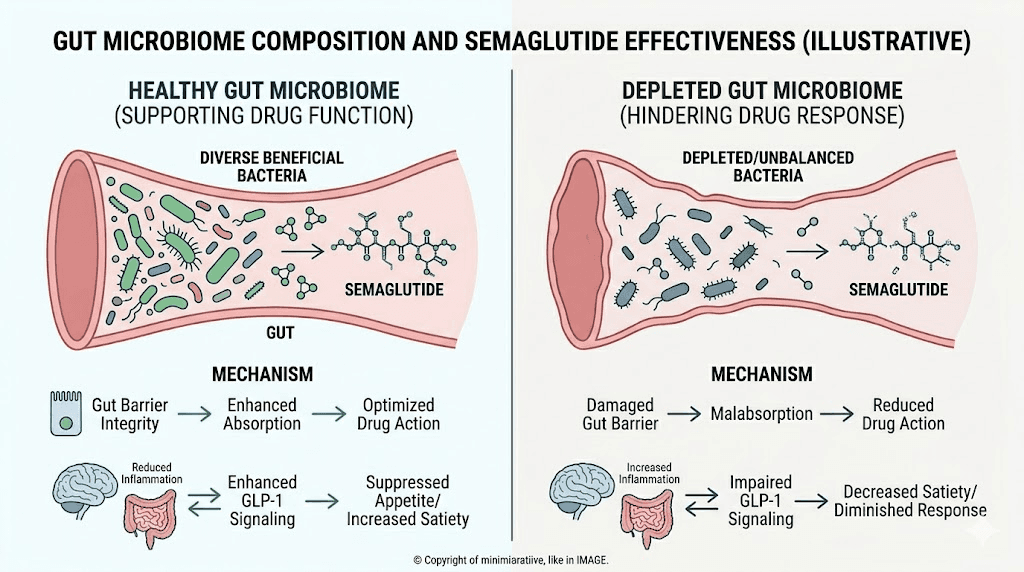
The gut microbiome connection
This is where the science gets fascinating. Your gut bacteria may determine whether semaglutide works for you. And this is not fringe speculation. Multiple peer-reviewed studies have now demonstrated that the composition of the gut microbiome influences GLP-1 receptor agonist response in measurable, predictable ways.
Akkermansia and semaglutide response
The genus Akkermansia, particularly the species Akkermansia muciniphila, has emerged as a key player in metabolic health and drug response. This bacterium lives in the mucus layer of the intestinal wall and plays a crucial role in maintaining gut barrier integrity, regulating inflammation, and modulating metabolic signaling.
Research has found that higher baseline levels of Akkermansia are associated with better outcomes from GLP-1 receptor agonist therapy. Individuals with abundant Akkermansia tend to lose more weight, show greater improvements in metabolic markers, and are less likely to qualify as non-responders. Conversely, individuals with depleted Akkermansia populations tend to respond poorly.
The mechanism appears to involve several pathways. Akkermansia produces short-chain fatty acids that enhance GLP-1 secretion from intestinal L-cells, essentially amplifying the body natural GLP-1 signaling on top of the exogenous semaglutide. It also reduces intestinal permeability ("leaky gut"), which decreases systemic inflammation and improves insulin sensitivity, both of which support weight loss. For those looking to optimize their gut environment, exploring the best probiotics to take with semaglutide is a practical starting point.
Baseline microbiome predicts treatment response
Perhaps the most remarkable finding in this area is that the baseline gut microbiome composition, measured before starting semaglutide, can predict whether someone will respond to treatment. A study analyzing stool samples from participants before GLP-1 agonist initiation found distinct microbiome signatures that differentiated future responders from future non-responders.
Responders tended to have higher microbial diversity, more Akkermansia, more Bacteroidetes relative to Firmicutes, and higher levels of butyrate-producing bacteria. Non-responders showed lower diversity, higher Firmicutes-to-Bacteroidetes ratios, and markers of gut dysbiosis including elevated levels of pro-inflammatory bacterial species.
This raises an exciting possibility. If we can modify the gut microbiome before or during semaglutide treatment, we might be able to convert non-responders into responders. Early evidence supports this idea, though the research is still in its infancy.
Strategies to optimize the gut microbiome for semaglutide
While microbiome science is complex and individualized, several evidence-based strategies can promote a gut environment more favorable to semaglutide response. Increasing dietary fiber intake, particularly prebiotic fibers like inulin, resistant starch, and beta-glucan, feeds beneficial bacteria and promotes short-chain fatty acid production. The best fiber supplements for GLP-1 users target these specific prebiotic compounds.
Fermented foods like sauerkraut, kimchi, kefir, and yogurt introduce beneficial bacteria directly. Polyphenol-rich foods, including berries, green tea, dark chocolate, and olive oil, selectively promote growth of beneficial species while inhibiting pathogenic ones. Reducing ultra-processed food intake is equally important because artificial sweeteners, emulsifiers, and other additives in processed foods can disrupt microbiome composition and reduce the very bacterial populations that support semaglutide effectiveness.
Targeted probiotic supplementation is another option. While general probiotics may not specifically boost Akkermansia (which is an anaerobe difficult to culture), certain multi-strain probiotics containing Lactobacillus and Bifidobacterium species can improve overall microbial diversity and create conditions favorable for Akkermansia growth. Supplements that support GLP-1 therapy often include both probiotic and prebiotic components designed to address this exact issue.
Dosing mistakes that look like non-response
Here is the thing nobody wants to hear. A significant number of people who think semaglutide does not work for them are actually just not using it correctly. Dosing errors, injection technique problems, and inadequate titration periods are among the most common and most fixable causes of apparent non-response.
Insufficient titration time
Semaglutide is designed to be titrated slowly. The standard protocol starts at 0.25mg weekly for the first four weeks, then increases to 0.5mg, then 1.0mg, then 1.7mg, and finally 2.4mg for weight management. Each step is supposed to last at least four weeks, and the total titration from starting dose to maximum dose takes about 16 to 20 weeks.
Many people make the mistake of evaluating semaglutide effectiveness at a dose they have only been on for a few weeks. Clinical evidence suggests that each dose level needs 12 to 16 weeks at maintenance before you can draw meaningful conclusions about whether that dose is working. Starting the 2.4mg dose and declaring semaglutide a failure after four weeks is like test-driving a car in first gear and concluding it is slow.
The dose-response relationship for semaglutide is well established. Higher doses produce greater weight loss in most people. If you are four weeks into semaglutide with no weight loss, it is almost certainly too early to draw conclusions, especially if you have not yet reached the target dose. The compounded semaglutide dose chart provides a clear visual reference for proper titration scheduling.
Incorrect injection technique
Semaglutide is a subcutaneous injection. It needs to reach the fatty tissue beneath the skin, not the muscle, not the dermis, and definitely not the floor of your bathroom because it leaked out after an improper injection. Common injection technique errors include injecting too shallowly (intradermal), injecting too deeply (intramuscular), injecting into scar tissue or areas with minimal subcutaneous fat, failing to hold the needle in place long enough for the full dose to deposit, and using injection sites with poor absorption characteristics.
The best injection sites for semaglutide include the abdomen (at least 2 inches from the navel), the front of the thighs, and the back of the upper arms. Each site has slightly different absorption kinetics, and rotating between sites helps prevent lipodystrophy, which is localized changes in subcutaneous fat that can impair drug absorption over time. For detailed technique guidance, our guide to giving semaglutide injections with a syringe walks through every step.
Reconstitution errors with compounded semaglutide
If you are using compounded semaglutide that comes as a lyophilized powder requiring reconstitution, errors in the reconstitution process can dramatically affect potency. Adding too much bacteriostatic water dilutes the concentration below the intended dose. Adding too little can make it difficult to draw accurate volumes. Using the wrong diluent, reconstituting too vigorously (which can denature the peptide), or contaminating the vial during reconstitution can all compromise the medication before it ever enters your body.
Knowing how to reconstitute semaglutide properly is essential for anyone using compounded formulations. The math matters too. Guides covering how much bacteriostatic water to mix with 5mg semaglutide and how much bacteriostatic water to mix with 10mg semaglutide remove the guesswork from this critical step. The semaglutide dosage calculator can help verify your concentrations and unit conversions are correct.
Storage problems that degrade the medication
Semaglutide is a protein-based medication sensitive to temperature, light, and agitation. Improper storage can degrade the active compound without any visible change to the solution, meaning you might be injecting a full dose of partially or fully inactive medication without knowing it.
The critical storage requirements include refrigeration between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius), protection from direct light, and avoidance of freezing. If your semaglutide has been left out overnight at room temperature, the potency may be compromised depending on the ambient temperature and duration of exposure. Similarly, if your semaglutide arrived hot during shipping, the peptide may have already degraded before you even started using it.
Understanding how long semaglutide lasts in the fridge and whether compounded semaglutide expires helps ensure you are always using a potent product. Visual checks also matter. If you are wondering what color semaglutide should be or noticing that your semaglutide has turned red or discolored, that is a sign something has gone wrong.
Timing and consistency issues
Semaglutide has a half-life of approximately one week, which is why it is dosed weekly. But inconsistent timing, missed doses, or variable intervals between injections can prevent the medication from reaching and maintaining therapeutic steady-state levels. It typically takes four to five half-lives (roughly 4 to 5 weeks of consistent weekly dosing) to reach steady state at any given dose.
Taking your injection at wildly different times each week, skipping doses, or spacing injections more than seven days apart can reduce average circulating drug levels below the therapeutic threshold. The best time of day to take semaglutide is whichever time you can maintain consistently week after week. Whether that is Saturday morning or Tuesday evening matters far less than doing it at the same time every single week.
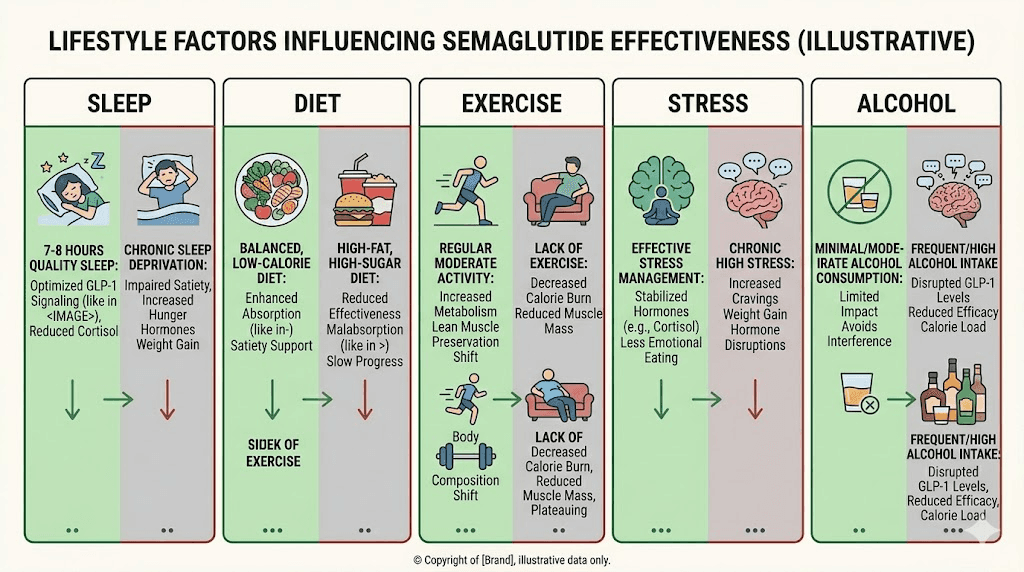
Lifestyle factors that undermine semaglutide results
Semaglutide is powerful. But it is not magic. It reduces appetite and slows gastric emptying, creating conditions favorable for weight loss. What you do with those conditions, how you eat, move, sleep, and manage stress, determines whether those favorable conditions actually produce results.
Diet quality matters more than diet quantity
Semaglutide reduces how much you eat. But it does not control what you eat. And this distinction is critical. Someone eating 1,200 calories per day of ultra-processed food, sugary drinks, and refined carbohydrates will get dramatically different results from someone eating 1,200 calories of whole foods, lean protein, vegetables, and healthy fats.
High-glycemic foods cause blood sugar spikes followed by crashes that trigger hunger and cravings, partially counteracting semaglutide appetite suppression. Ultra-processed foods are engineered to bypass satiety signals, and even semaglutide-enhanced satiety can be overwhelmed by foods specifically designed to make you overeat. Following a structured diet plan while on semaglutide that emphasizes whole foods makes a measurable difference in outcomes.
The best foods to eat on semaglutide share common characteristics: high protein content, high fiber content, low glycemic index, and minimal processing. Equally important is knowing which foods to avoid while on semaglutide, particularly those high in sugar, refined flour, and artificial ingredients that can worsen gastrointestinal side effects while providing minimal nutritional value. A complete list of semaglutide-friendly foods can serve as a practical grocery shopping guide.
Protein intake is non-negotiable
This cannot be overstated. Inadequate protein intake during semaglutide treatment is one of the most common and most consequential lifestyle mistakes. When you are in a caloric deficit (which semaglutide creates through appetite reduction), your body needs to decide what to break down for energy. With sufficient protein, it preferentially burns fat. Without sufficient protein, it happily cannibalizes muscle along with fat.
Muscle loss matters for two reasons. First, it reduces metabolic rate, meaning you burn fewer calories at rest, which slows and eventually stalls weight loss. This creates the classic semaglutide plateau that so many users experience. Second, the weight you lose is less cosmetically and functionally beneficial when a significant portion of it is muscle rather than fat.
Research suggests that semaglutide users should aim for at least 1.0 to 1.2 grams of protein per kilogram of body weight daily, with some experts recommending up to 1.6 grams per kilogram for those also doing resistance training. Given semaglutide-induced appetite reduction, meeting these protein targets requires intentional planning. A semaglutide-specific diet plan can help structure meals to hit protein goals within reduced caloric intake.
Caloric intake can drop too low
This sounds counterintuitive, but eating too little can sabotage semaglutide results. When caloric intake drops below approximately 1,000 to 1,200 calories per day for extended periods, the body activates metabolic adaptation mechanisms: reduced thyroid hormone output, decreased non-exercise activity thermogenesis (NEAT), increased mitochondrial efficiency, and elevated cortisol. These adaptations slow metabolic rate dramatically and can cause weight loss to stall or even reverse.
Some semaglutide users, particularly those on higher doses, find their appetite so suppressed that they struggle to eat even 800 calories daily. While this might seem like it would accelerate weight loss, it often produces the opposite effect over weeks and months. Tracking how many calories you should eat on semaglutide helps ensure you stay in the optimal deficit zone: enough restriction to lose weight steadily, but not so much that your metabolism retaliates.
Exercise, especially resistance training
You can lose weight on semaglutide without exercise. The clinical trials proved that. But exercise, particularly resistance training, amplifies results significantly and protects against muscle loss. Resistance training sends a powerful signal to the body that muscle tissue is needed and should be preserved, even during a caloric deficit.
Cardiovascular exercise contributes too, though its primary benefit is metabolic health rather than direct fat loss. The combination of semaglutide, adequate protein, and regular resistance training produces the most favorable body composition changes: maximum fat loss with minimal muscle loss. Without resistance training, a larger percentage of weight lost will be lean tissue, reducing metabolic rate and making long-term weight maintenance harder.
Sleep deprivation
Sleeping less than seven hours per night increases ghrelin (hunger hormone) by up to 15 percent, decreases leptin (satiety hormone) by a similar amount, impairs insulin sensitivity, elevates cortisol, and increases cravings for high-calorie foods. All of these effects directly oppose semaglutide mechanisms. A person getting five hours of sleep per night is fighting semaglutide with one hand tied behind their back.
Studies on sleep and weight loss consistently show that sleep-deprived individuals lose less fat and more muscle during caloric restriction, even when total weight loss is similar. For semaglutide users, prioritizing seven to nine hours of quality sleep may be one of the highest-return investments they can make in their weight loss outcomes.
Alcohol consumption
Alcohol interferes with semaglutide results in multiple ways. It provides empty calories (7 calories per gram, almost as energy-dense as fat). It impairs inhibition and decision-making, leading to poor food choices. It disrupts sleep architecture even when total sleep time seems adequate. It increases cortisol. And it directly impairs fat oxidation because the liver prioritizes alcohol metabolism over fat metabolism. Understanding whether you can drink on semaglutide involves recognizing that while occasional moderate consumption may not derail results, regular drinking can meaningfully blunt weight loss.
Chronic stress
Stress elevates cortisol, which promotes visceral fat storage, increases appetite (particularly for calorie-dense comfort foods), impairs sleep, and reduces motivation for exercise. Chronic unmanaged stress creates a hormonal environment that resists weight loss from any intervention. Semaglutide can help by reducing the food reward response, but it cannot eliminate stress-driven eating entirely, especially when the underlying stress remains unaddressed.
The combination of lifestyle factors is multiplicative rather than additive. Someone who sleeps poorly, drinks regularly, eats processed food, does not exercise, and lives under chronic stress will likely see minimal results from semaglutide regardless of dose. Someone who optimizes even three or four of these factors will likely see substantially better outcomes. Practical semaglutide tips often focus on these modifiable lifestyle factors because they represent the area where individual effort has the greatest impact on outcomes.
The difference between slow response and no response
There is an important distinction that gets lost in the noise of online discussions. A slow response is not the same as no response. And confusing the two leads people to abandon effective treatment prematurely.
Normal semaglutide timelines
Semaglutide does not produce overnight results. The expectation that semaglutide works right away is one of the most common sources of disappointment. Clinical trial data shows that most weight loss occurs gradually over 12 to 16 months, not in the first few weeks.
During the initial titration phase (weeks 1 through 16), weight loss is typically modest. You are on subtherapeutic doses. The medication is building up in your system. Your body is adapting to its effects. Some people lose significant weight during titration, but many lose little or nothing. This is normal. It does not mean the drug is not working. It means it has not had enough time at a therapeutic dose to produce measurable results.
The timeline for when weight loss begins on semaglutide varies enormously between individuals. Some notice appetite changes within the first week. Others do not feel much different until they reach the 1.0mg or even 2.4mg dose level. Neither pattern predicts long-term success or failure.
What "slow response" looks like
A slow responder might lose 1 to 2 percent of body weight in the first three months rather than the 5 to 8 percent that aggressive responders achieve. They might not notice dramatic appetite suppression but may find that their portion sizes have gradually decreased without conscious effort. They might not see the scale change much but notice that their clothes fit differently, suggesting body composition shifts (fat loss with concurrent muscle preservation) that the scale alone cannot capture.
Slow response can also manifest as metabolic improvements without immediate weight loss. Blood sugar levels improving. Blood pressure dropping. Triglycerides normalizing. Inflammatory markers decreasing. These changes indicate that semaglutide is working at a biochemical level even when the scale has not caught up yet. One-month semaglutide results can be modest but still indicate that the medication is heading in the right direction.
When to suspect genuine non-response
Genuine non-response becomes a reasonable concern when all of the following conditions are met. First, you have been on the maximum tolerated dose (ideally 2.4mg for weight management) for at least 12 to 16 weeks. Second, you have addressed identifiable lifestyle factors including diet quality, protein intake, exercise, sleep, and stress management. Third, you have ruled out medical conditions that could interfere, including thyroid dysfunction, untreated sleep apnea, and medication interactions. And fourth, you have confirmed that your medication is being stored properly, reconstituted correctly (if compounded), and administered with proper injection technique.
If all four conditions are satisfied and you have still not achieved 5 percent or greater body weight loss, you may be a genuine pharmacological non-responder to semaglutide. At that point, exploring alternative medications becomes a reasonable next step.
The danger of premature abandonment
Research on GLP-1 agonist discontinuation shows that most weight regain occurs within the first year after stopping treatment. Understanding semaglutide withdrawal symptoms and the rebound appetite that follows discontinuation is crucial for making informed decisions. If you are considering stopping semaglutide because results seem insufficient, make sure you have genuinely given it enough time and optimized all modifiable factors before concluding it does not work.
Knowing how long to stay on semaglutide for weight loss helps set appropriate expectations. The medication is not a short-term fix. It is a long-term treatment that produces cumulative results over months and years. Evaluating it after a few weeks is like evaluating a retirement savings plan after a few deposits. Patience matters. The realistic rate of weight loss on semaglutide is typically 1 to 2 pounds per week at therapeutic doses, not the 5 to 10 pounds per week that social media might lead you to expect.
What to do when semaglutide is not working
If you have read this far and suspect that semaglutide might truly not be working for you, here is a systematic troubleshooting approach. Work through these steps in order before concluding that you are a non-responder.
Step 1: Verify your medication is real and potent
This sounds basic, but it matters more than ever. Counterfeit and substandard semaglutide products exist in the market. If you are using compounded semaglutide, verify that it comes from a licensed pharmacy with proper quality assurance. Check that it has been stored correctly from the moment of compounding through delivery to your refrigerator. Confirm that your compounded semaglutide has been refrigerated properly throughout the supply chain.
Look at the solution. Is it clear and colorless? Any cloudiness, discoloration, or particulate matter suggests degradation. Check the expiration date. Understanding how long semaglutide remains good and whether expired semaglutide is safe to use can prevent you from injecting inactive medication week after week.
Step 2: Audit your injection technique
Review the basics. Are you injecting subcutaneously? Pinching the skin fold? Inserting the needle at the correct angle? Holding for 5 to 10 seconds after depressing the plunger? Rotating injection sites? Using the correct needle gauge and length for subcutaneous administration? Our GLP-1 injection guide covers proper technique, and understanding where to inject GLP-1 medications ensures optimal absorption. The best GLP-1 injection site for weight loss can vary between individuals based on their body composition.
Step 3: Confirm your dosing is correct
For compounded semaglutide, dosing errors are surprisingly common. The concentration of reconstituted semaglutide depends on the amount of bacteriostatic water used, and even small math errors can result in significantly over- or under-dosing. Verify your calculations using a semaglutide dosage calculator. Review the semaglutide dosage in units to ensure you are drawing the correct volume. Confirm against the semaglutide syringe dosage chart that your syringe markings correspond to the intended dose.
Common dosing questions like whether 20 units of semaglutide is too much or whether 50 units is a lot depend entirely on the reconstitution concentration. Without knowing the concentration, unit numbers are meaningless.
Step 4: Optimize your dose titration
Have you actually reached the target dose? Many people stall at intermediate doses because of side effects and never reach the fully therapeutic level. If gastrointestinal side effects have prevented dose escalation, strategies like splitting the semaglutide dose into twice-weekly injections can sometimes improve tolerability and allow continued titration. Managing side effects like bloating, constipation, acid reflux, and dizziness often allows patients to reach higher doses where weight loss effects become more pronounced.
Step 5: Get comprehensive blood work
Request the following tests from your healthcare provider. A complete thyroid panel including TSH, free T3, free T4, and thyroid peroxidase antibodies. Fasting insulin and glucose to calculate HOMA-IR (insulin resistance). A complete metabolic panel. Lipid panel. HbA1c. Morning cortisol. Vitamin D level. And for women, a hormonal panel including estrogen, progesterone, testosterone, and DHEA-S.
These tests can reveal hidden barriers to weight loss that semaglutide alone cannot overcome. Conditions like Hashimoto thyroiditis are particularly relevant because they directly impair metabolic rate. Monitoring semaglutide effects on liver enzymes can also reveal whether the medication is being metabolized normally.
Step 6: Audit your lifestyle
Track your food intake honestly for two weeks. Not what you think you are eating. What you are actually eating, measured and recorded. Many people underestimate caloric intake by 30 to 50 percent. Track your sleep with a wearable device. Record your exercise (type, duration, intensity). Note your alcohol consumption. Assess your stress levels.
Often, this audit reveals that one or more lifestyle factors are working against the medication. Maybe you are eating 1,800 calories of relatively healthy food but not in a meaningful deficit for your metabolism. Maybe you are sleeping six hours when you need eight. Maybe weekend alcohol consumption is erasing the caloric deficit created during the week. These discoveries are valuable because they point to fixable problems.
Step 7: Consider combination approaches
If semaglutide alone is not producing adequate results after all other factors have been addressed, combination strategies may help. Adding B12 to semaglutide can address the energy depletion and fatigue that some users experience, potentially improving exercise capacity and metabolic function. The semaglutide glycine B12 blend is a compounded formulation designed to provide these synergistic benefits in a single injection.
Other combination approaches include semaglutide with L-carnitine for enhanced fat oxidation, semaglutide with glycine for improved metabolic function, semaglutide with niacinamide for cellular energy support, semaglutide with pyridoxine for B6-dependent metabolic pathways, and semaglutide with methylcobalamin for methylation support. Whether combining phentermine with semaglutide is appropriate depends on individual cardiovascular risk factors and should be discussed with a physician.
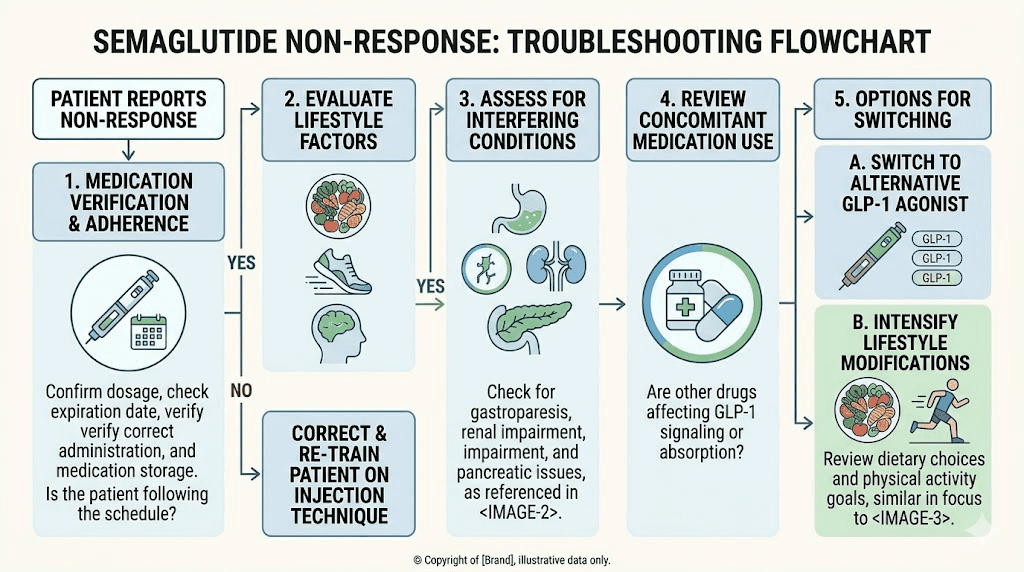
Switching to alternatives when semaglutide fails
When you have genuinely exhausted the troubleshooting process, confirmed proper dosing and technique, optimized lifestyle factors, ruled out medical barriers, and spent adequate time at maximum dose, switching to a different mechanism of action becomes the logical next step. The good news is that semaglutide non-response does not mean all GLP-1-based therapies will fail.
Tirzepatide: the dual-agonist option
Tirzepatide works through a fundamentally different mechanism than semaglutide. While semaglutide is a pure GLP-1 receptor agonist, tirzepatide is a dual GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptor agonist. This dual mechanism engages an entirely additional hormonal pathway that semaglutide does not touch.
Clinical trial data shows that tirzepatide produces greater average weight loss than semaglutide at comparable doses. More importantly for our discussion, some individuals who respond poorly to GLP-1 receptor agonism alone respond well to the combination of GLP-1 and GIP receptor agonism. The question of whether tirzepatide works when semaglutide does not has a nuanced answer: for some people, absolutely yes. The side effect profiles also differ between the two medications, so someone who could not tolerate semaglutide side effects may tolerate tirzepatide better, or vice versa.
Understanding the transition process between these medications is important for anyone considering a switch. Tirzepatide dosing for weight loss follows its own titration schedule, and the timeline for tirzepatide to start working differs from semaglutide. A comprehensive comparison of semaglutide versus tirzepatide versus retatrutide can help inform the decision.
Retatrutide: the triple-agonist frontier
Retatrutide represents the next evolution in incretin-based therapy. It is a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. Early clinical trial data shows weight loss results exceeding both semaglutide and tirzepatide, with some participants losing more than 24 percent of body weight in phase 2 trials.
The addition of glucagon receptor agonism is significant because glucagon promotes hepatic fat oxidation and energy expenditure through mechanisms entirely separate from appetite suppression. This means retatrutide attacks obesity from three angles: reduced appetite (GLP-1), enhanced metabolic signaling (GIP), and increased fat burning (glucagon). For semaglutide non-responders, this triple mechanism offers the most comprehensive pharmacological approach currently available. Understanding the differences between retatrutide and semaglutide helps contextualize why triple agonism might succeed where single agonism failed.
Other GLP-1 alternatives
Beyond tirzepatide and retatrutide, several other options exist for semaglutide non-responders. Phentermine works through an entirely different mechanism (sympathomimetic amine) and can sometimes succeed where GLP-1 agonists fail, though it carries different risk profiles. Tesofensine is a triple monoamine reuptake inhibitor that reduces appetite through serotonin, norepinephrine, and dopamine pathways, offering yet another distinct mechanism of action.
For those interested in peptide-based approaches beyond incretin agonism, the best peptides for weight loss include options like AOD 9604 (a growth hormone fragment that promotes fat metabolism), which can be compared against semaglutide through our AOD 9604 versus semaglutide analysis. Peptide stacking for weight loss combines multiple compounds with complementary mechanisms, sometimes achieving results that no single agent could produce alone.
Combination and alternating approaches
Some clinicians have explored using semaglutide and tirzepatide together or alternating between them to overcome resistance. While these approaches are not yet supported by large-scale clinical trials, the theoretical rationale is sound: different mechanisms of action can produce additive or synergistic effects. Combining HRT with GLP-1 therapy is another approach gaining traction, particularly in perimenopausal and postmenopausal women whose hormonal changes contribute to weight gain and GLP-1 resistance.
If you decide to switch medications, the transition should be managed carefully. Stopping semaglutide abruptly can trigger rebound appetite and rapid weight regain. Understanding whether you can stop semaglutide cold turkey and the protocols for restarting semaglutide after a break helps navigate these transitions safely. A comprehensive compounded semaglutide guide covers the full range of options available.
SeekPeptides members access detailed protocols for medication transitions, combination strategies, and alternative treatment approaches. Making informed decisions about what comes after semaglutide requires the kind of evidence-based guidance and community experience that SeekPeptides provides.
Understanding what realistic success looks like
Part of the non-responder problem is an expectations problem. Social media has distorted what "working" looks like for GLP-1 medications. The dramatic transformations that go viral are outliers, not averages. Setting realistic benchmarks helps you evaluate your own response more accurately.
Average weight loss by timeframe
In the STEP 1 trial, the average weight loss at 68 weeks on semaglutide 2.4mg was approximately 14.9 percent of baseline body weight. But "average" obscures enormous variability. The top quartile of responders lost more than 20 percent. The bottom quartile lost less than 5 percent. Most people fell somewhere in between.
A reasonable expectation for the first three months on semaglutide (including titration) is 3 to 5 percent body weight loss. By six months at therapeutic dose, 8 to 12 percent is typical for responders. By twelve months, 12 to 17 percent represents a good response. These numbers contextualize your own results. Understanding the average GLP-1 weight loss per month provides additional benchmarking data. The GLP-1 fat loss treatment approach involves more nuance than simple scale numbers.
Non-scale victories matter
The scale is one data point. It is not the only data point, and it is often not the most important one. Semaglutide can produce meaningful health improvements, including reduced blood pressure, improved cholesterol profiles, better blood sugar control, decreased inflammation, and reduced cardiovascular risk, even when weight loss is modest.
Body composition changes can occur without the scale moving much. If you are losing fat while gaining or preserving muscle (which happens more with resistance training and adequate protein), the scale might barely budge while your waist circumference decreases, your clothes fit better, and your metabolic markers improve. Before-and-after comparisons using photos and measurements often tell a more complete story than the scale alone.
The role of metabolic adaptation
As you lose weight, your body adapts. Metabolic rate decreases. Appetite regulatory hormones shift. Energy efficiency improves. These adaptations are normal and expected, but they can create the illusion of non-response when in reality you are simply experiencing the natural deceleration that accompanies successful weight loss.
Understanding how long semaglutide suppresses appetite and recognizing that appetite may return somewhat as your body adapts helps maintain realistic expectations. The GLP-1 maintenance dose concept acknowledges that long-term treatment often involves adjusting expectations and strategies as the body reaches new equilibrium points. Knowing whether semaglutide gives you energy or whether semaglutide makes you cold helps distinguish normal side effects from signs of metabolic problems.
Frequently asked questions
What percentage of people does semaglutide not work for?
Clinical trial data shows non-responder rates (less than 5 percent body weight loss) between 7.6 and 26.8 percent, depending on the study population. In people without diabetes, roughly 10 to 12 percent do not respond adequately. In people with type 2 diabetes, that number rises to approximately 20 to 27 percent. Real-world studies suggest rates of 17.8 to 22.5 percent when accounting for early discontinuation and less controlled conditions. The time needed for GLP-1 medications to start working means some apparent non-responders may simply need more time.
How do I know if semaglutide is actually working?
Look beyond the scale. Signs that semaglutide is working include reduced appetite or food noise, feeling full sooner during meals, decreased cravings for high-calorie foods, improved blood sugar readings, reduced waist circumference, and changes in food preferences (many users report decreased interest in sweets and fried foods). If you are experiencing these effects but not seeing scale changes, the medication is pharmacologically active. The weight loss may follow. Appetite suppression timing varies considerably between individuals.
Can I increase my semaglutide dose if it is not working?
If you have not yet reached the maximum dose of 2.4mg weekly (for weight management), increasing the dose is the most obvious next step. Each dose increase should be maintained for at least four weeks, and ideally 12 to 16 weeks, before evaluating effectiveness. The compounded semaglutide dose chart outlines proper titration schedules. Some clinicians also explore doses slightly above 2.4mg in certain cases, though this is off-label.
Does semaglutide work differently for men versus women?
Yes. Research shows significantly different non-responder rates by gender, with men experiencing a 41.6 percent non-responder rate compared to 14.2 percent in women. Hormonal differences, body composition differences (more visceral fat in men), higher baseline caloric needs, and differences in fat distribution all contribute to this gap. Men may need to be more aggressive with lifestyle optimization to achieve results comparable to what women typically see. Understanding the effects of semaglutide on women specifically can help women track their full response profile.
Should I stop semaglutide if it is not working after one month?
No. One month is far too early to evaluate semaglutide effectiveness. During the first month, you are typically on the lowest dose (0.25mg), which is a titration dose not expected to produce significant weight loss. Clinical trials assessed outcomes after 68 weeks. While you should not wait that long to see any effect, a minimum of 12 to 16 weeks at therapeutic dose is needed before drawing conclusions. If you are experiencing no weight loss after four weeks, that alone does not indicate non-response.
Can genetics be tested to predict semaglutide response?
Research has identified genetic variants like rs6923761 (Gly168Ser) in the GLP-1 receptor gene that appear to predict reduced semaglutide response. However, clinical genetic testing for this purpose is not yet widely available or standard practice. As pharmacogenomics advances, it is likely that genetic testing will eventually guide GLP-1 agonist prescribing decisions, but currently, treatment response is determined empirically through trial and observation.
Does the gut microbiome really affect semaglutide results?
Yes. Multiple studies have demonstrated that the gut microbiome composition influences GLP-1 receptor agonist response. Higher levels of beneficial bacteria, particularly the Akkermansia genus, are associated with better outcomes. Baseline microbiome composition can predict treatment response before therapy even begins. The best probiotics for semaglutide users target the bacterial populations most associated with improved drug response.
What is the best alternative if semaglutide does not work?
Tirzepatide is the most common next step because its dual GLP-1/GIP mechanism engages pathways that semaglutide does not. Detailed comparisons of whether tirzepatide works after semaglutide failure show promising results for a meaningful subset of semaglutide non-responders. Retatrutide, with its triple agonist mechanism, represents the most comprehensive alternative for those who do not respond to dual agonism either. Exploring the best peptides for weight loss provides a broader view of available options.
External resources
FDA Drug Safety Communication: Semaglutide Medications (U.S. Food and Drug Administration)
Obesity and Overweight Fact Sheet (World Health Organization)
For researchers serious about optimizing their treatment protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members get access to troubleshooting frameworks, expert guidance, and personalized support for when standard approaches do not produce expected results.
In case I do not see you, good afternoon, good evening, and good night. May your medications stay potent, your protocols stay optimized, and your results stay consistent.