Mar 8, 2026

Some people lose 15% of their body weight on semaglutide. Others barely see the scale move after months of injections. The difference is not the dose. It is not genetics. It is not willpower. It is what they eat.
That statement might sound oversimplified, but research backs it up. A study presented at ENDO 2025 found that people taking semaglutide who consumed higher amounts of protein lost significantly less muscle mass than those who did not prioritize their nutrition. Up to 40% of the weight lost on semaglutide can come from lean tissue, including muscle, when dietary choices are poor. That is not just a cosmetic problem. Losing muscle reduces your metabolic rate, weakens your body, and can actually undermine the blood sugar improvements that semaglutide is supposed to deliver.
The medication does its job. It suppresses appetite, slows gastric emptying, and changes how your brain responds to food cues. But what you do with those changes, how you fill the smaller plate, what nutrients you prioritize when you are eating less overall, that determines whether you come out of this process leaner and healthier or just lighter on the scale with less muscle to show for it.
This guide covers everything. The specific foods that work with semaglutide rather than against it. The protein targets that protect your muscle mass. The dietary strategies that prevent nausea, constipation, and the other gastrointestinal side effects that make so many people miserable during their first weeks. And the phase-based approach that evolves as your body adapts to the medication. Whether you are in your first week on semaglutide or months into your protocol, your diet is the variable that separates good results from transformative ones.
How semaglutide changes the way you eat
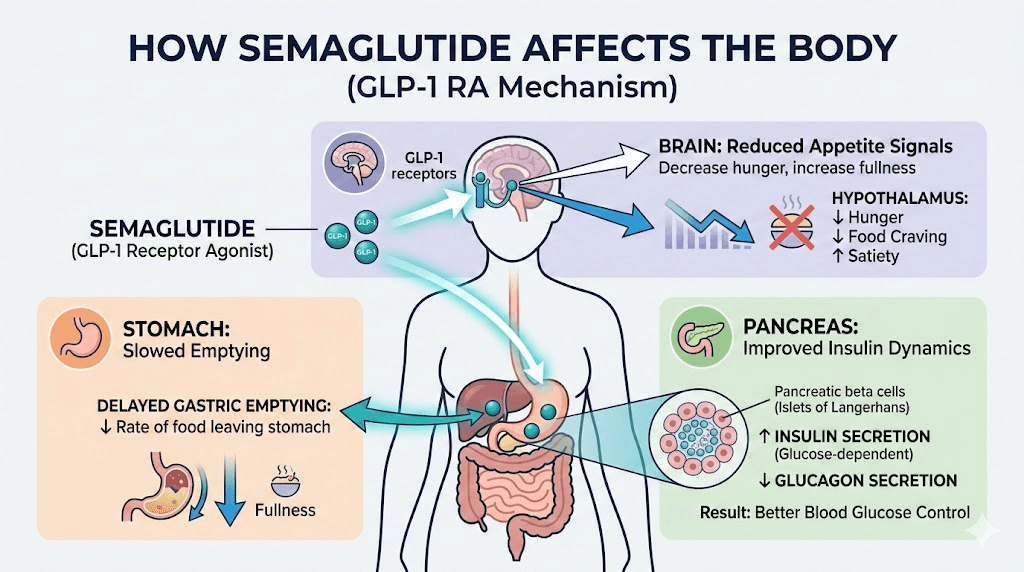
Before diving into specific foods, you need to understand what semaglutide actually does to your digestive system and appetite. This is not a simple appetite suppressant. It fundamentally rewrites the rules of how your body processes food.
Semaglutide is a GLP-1 receptor agonist. GLP-1 receptors exist throughout your digestive tract, your pancreas, and your brain. When semaglutide activates these receptors, three major things happen simultaneously. First, gastric emptying slows dramatically. Food stays in your stomach longer, which means you feel full faster and stay full for hours after eating. Second, your brain receives different satiety signals, reducing cravings and changing how you think about food at a neurological level. Third, insulin secretion improves while glucagon production decreases, which directly affects how your body handles carbohydrates and blood sugar.
What does this mean for your diet?
It means everything changes. The portions that used to feel normal now feel enormous. Foods that never bothered your stomach before might suddenly trigger nausea. Your window for eating might shrink because your appetite simply does not show up the way it used to. And here is the critical part that most people miss: when you are eating significantly less food overall, every single bite matters more. You cannot afford to waste your reduced caloric intake on nutritionally empty foods. Each meal needs to deliver maximum nutritional value because you are working with fewer meals and smaller portions than before.
Understanding how semaglutide makes you feel helps you plan meals that work with the medication rather than against it. The people who struggle most are the ones who try to eat the same way they did before, just less of it. That approach fails because your digestive system is operating under entirely different rules now.
The protein problem nobody talks about
This is the most important section of this entire guide. Read it carefully.
When you lose weight on semaglutide, you do not just lose fat. Research consistently shows that 26% to 40% of the weight lost on GLP-1 receptor agonists comes from lean mass, which includes muscle. That percentage is not a minor detail. It is a potentially serious problem that can undermine your entire reason for starting semaglutide in the first place.
The ENDO 2025 study from the Endocrine Society found something crucial. After accounting for total weight loss, researchers identified three factors linked to greater muscle loss on semaglutide: being older, being female, and eating less protein. That third factor is the one you can control. And controlling it makes a measurable difference.
Why muscle loss matters beyond appearance
Muscle is not just for aesthetics. It is your metabolic engine. Every pound of muscle burns more calories at rest than a pound of fat. When you lose muscle, your resting metabolic rate drops. This means the weight loss that felt easy at first becomes harder over time, because your body is burning fewer calories at baseline. People who experience a semaglutide plateau are often dealing with this exact issue, their metabolism has slowed because they lost too much lean tissue along with fat.
Muscle loss also reduces insulin sensitivity. This is ironic, because improved blood sugar control is one of the primary benefits of semaglutide. The ENDO 2025 researchers found that participants who lost more muscle showed less improvement in HbA1c levels compared to those who preserved lean mass. In other words, losing muscle can partially cancel out the metabolic benefits you are taking semaglutide to achieve.
For older adults, excessive muscle loss creates additional risks. Sarcopenia, the age-related decline of muscle mass and strength, accelerates when you lose weight rapidly without adequate protein. This increases fall risk, reduces functional independence, and worsens long-term health outcomes.
How much protein you actually need
General dietary guidelines suggest around 0.8 grams of protein per kilogram of body weight daily. That is not enough when you are on semaglutide and losing weight actively. Research suggests higher targets are necessary to protect lean mass during GLP-1 mediated weight loss.
Studies examining protein intake during semaglutide use show effective ranges between 1.2 and 1.5 grams of protein per kilogram of body weight daily, with some specialists recommending up to 1.6 to 2.3 grams per kilogram of fat-free mass. As a practical target, aim for 25 to 30 grams of protein per meal, spread across three to four eating occasions throughout the day.
For a 180-pound (82 kg) person, that translates to roughly 98 to 123 grams of protein daily. For a 150-pound (68 kg) person, roughly 82 to 102 grams daily. These numbers might seem high, especially when your appetite is suppressed. That is exactly why protein must be the foundation of every meal, not an afterthought. If you only eat one thing at each meal, make it protein.
Track your protein intake for at least the first month. Most people dramatically overestimate how much protein they consume. A food diary or tracking app reveals the real numbers quickly, and they are often sobering. People who think they are getting enough protein are frequently hitting only 40 to 60 grams daily, which is well below the threshold for muscle preservation during active weight loss.
The semaglutide dosage calculator helps you dial in your medication amounts, but your protein calculator is equally important for outcomes. Many SeekPeptides members track both their dosing protocols and their daily protein intake as part of their overall optimization strategy.
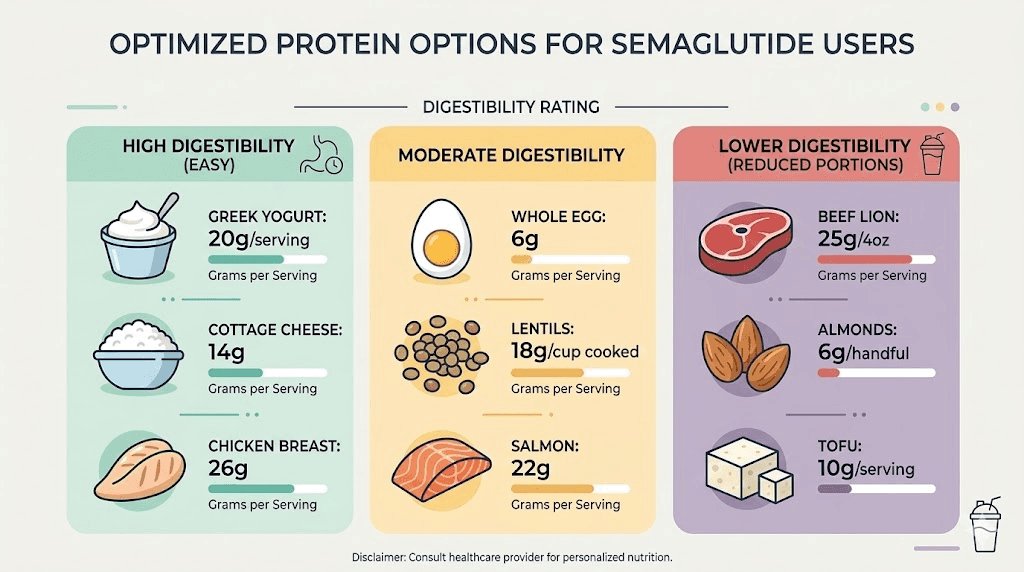
Best protein sources for semaglutide users
Not all protein sources are equal when you are dealing with slowed gastric emptying. Heavy, fatty proteins like ribeye steak or fried chicken can sit in your stomach for hours and trigger nausea. Lean, easily digestible protein sources work best, especially in the early weeks of treatment.
Top-tier protein sources (easily digestible, high protein per calorie):
Chicken breast (31g protein per 4 oz)
Turkey breast (30g protein per 4 oz)
White fish like cod, tilapia, or sole (26g protein per 4 oz)
Egg whites (26g protein per cup)
Greek yogurt, plain nonfat (17g protein per 6 oz)
Cottage cheese, low-fat (14g protein per half cup)
Shrimp (24g protein per 4 oz)
Strong protein sources (good balance of protein and other nutrients):
Salmon (25g protein per 4 oz, plus omega-3 fatty acids)
Whole eggs (6g protein each, plus choline and B vitamins)
Lean ground turkey (22g protein per 4 oz)
Tofu, firm (20g protein per cup)
Lentils (18g protein per cup cooked)
Edamame (17g protein per cup)
Many people find that protein shakes for GLP-1 users become essential, particularly in the early weeks when solid food tolerance is limited. A high-quality whey or plant-based protein shake delivers 25 to 30 grams of protein in a form that is easier on the stomach than whole foods. This is not a replacement for real food long-term, but it is a strategic tool for hitting protein targets when appetite is at its lowest.
Building your semaglutide nutrition foundation
Protein is the priority. But it is not the entire picture. Your overall dietary foundation on semaglutide should follow a simple hierarchy: protein first, fiber second, healthy fats third, and complex carbohydrates last. This is not an arbitrary ordering. It reflects both nutritional science and the practical reality of eating with suppressed appetite and slower digestion.
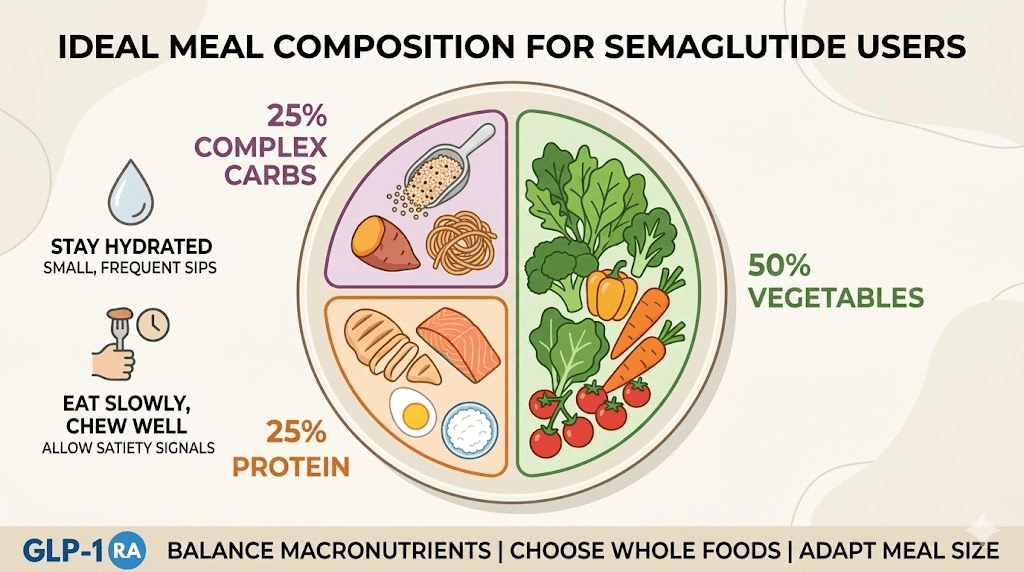
The plate method for semaglutide users
Forget complicated calorie counting or macro tracking apps if they overwhelm you. The simplest approach is the modified plate method. At every meal, fill your plate this way:
Half the plate: non-starchy vegetables (fiber, micronutrients, minimal calories)
Quarter of the plate: lean protein (25 to 30 grams per meal target)
Quarter of the plate: complex carbohydrates or healthy fats (sustained energy)
Eat in that order too. Protein first, then vegetables, then carbohydrates. When your stomach fills up quickly, and it will on semaglutide, you want the most nutritionally valuable food to go in first. People who eat bread or rice first often fill up before touching their protein, which is exactly backwards for optimizing weight loss on semaglutide.
Fiber: your second priority
Fiber does double duty on semaglutide. Soluble fiber feeds beneficial gut bacteria, supports digestive regularity, and helps stabilize blood sugar between meals. Insoluble fiber adds bulk to your stool, which directly addresses one of the most common complaints on semaglutide: constipation.
Research on dietary fiber shows that soluble fibers specifically can reduce appetite and short-term energy intake, complementing what semaglutide already does. Prebiotic fibers, found in foods like garlic, onions, leeks, asparagus, and bananas, support the gut microbiome during a period when your digestive system is under significant stress from the medication.
Aim for 25 to 35 grams of fiber daily, but increase gradually. Adding too much fiber too quickly on top of semaglutide is a recipe for severe bloating and abdominal pain. If you are currently eating 10 grams of fiber daily, do not jump to 35. Increase by 5 grams per week until you reach your target.
Best fiber sources for semaglutide users:
Leafy greens (spinach, kale, Swiss chard)
Cruciferous vegetables (broccoli, cauliflower, Brussels sprouts)
Berries (raspberries, blackberries, blueberries)
Chia seeds (10g fiber per 2 tablespoons)
Ground flaxseed (4g fiber per 2 tablespoons)
Lentils (15g fiber per cup cooked)
Black beans (15g fiber per cup cooked)
Oats (4g fiber per half cup dry)
For detailed food lists and specific recommendations, see our comprehensive guide on foods to eat while on semaglutide.
Healthy fats: quality over quantity
Fats slow digestion even further on top of what semaglutide already does. This makes fat selection critical. You want fats that deliver nutritional benefits without sitting in your stomach like a brick.
Focus on unsaturated fats from whole food sources:
Avocado (half an avocado provides fiber, potassium, and healthy monounsaturated fats)
Olive oil (use for cooking and dressings, but moderate portions)
Nuts and seeds (almonds, walnuts, pumpkin seeds, in small handfuls)
Fatty fish like salmon, sardines, and mackerel (omega-3 fatty acids reduce inflammation)
A handful of nuts daily, roughly one ounce, provides healthy fats, vitamins, minerals, fiber, and protein in a compact package. Research shows that regular nut consumption promotes satiety and supports weight management even beyond what the calorie count would suggest, because your body does not absorb all the calories from whole nuts.
Complex carbohydrates: the supporting role
Carbohydrates are not the enemy. But they need to earn their place on your plate when calories are limited. Refined carbohydrates like white bread, pasta, and pastries spike blood sugar, provide minimal nutrition, and work against what semaglutide is trying to do metabolically. Complex carbohydrates, on the other hand, provide sustained energy and important nutrients.
The best carbohydrate sources on semaglutide:
Quinoa (also provides 8g protein per cup cooked)
Sweet potatoes (rich in vitamin A and fiber)
Brown rice (sustained energy without blood sugar spikes)
Steel-cut oats (slow-digesting, excellent for breakfast)
Whole grain bread, in moderation (choose varieties with at least 3g fiber per slice)
Resistant starches deserve special mention. Foods like cooled cooked potatoes, slightly green bananas, and cooked and cooled rice contain resistant starch that feeds beneficial gut bacteria similarly to fiber. Healthcare professionals increasingly recommend incorporating resistant starches into semaglutide diet plans for their prebiotic benefits.
What to eat on semaglutide: the complete food guide
Theory is useful. But you need specifics. Here is a detailed breakdown of exactly what to eat, organized by meal occasion.
Breakfast options that work
Mornings on semaglutide can be tricky. Many people wake up with zero appetite, especially in the first few weeks. That does not mean you should skip breakfast entirely, but it does mean your first meal might look different than it used to.
High-protein breakfast options:
Two-egg omelet with spinach, mushrooms, and a sprinkle of feta (20g protein)
Greek yogurt parfait with berries and a tablespoon of chia seeds (22g protein)
Protein smoothie: whey protein, half banana, spinach, almond milk (25-30g protein)
Cottage cheese with sliced peaches and a drizzle of honey (14g protein per half cup)
Overnight oats made with protein powder, chia seeds, and almond milk (25g protein)
For more ideas specifically designed around GLP-1 breakfast approaches, see our dedicated guide. The key principle is the same regardless of which option you choose: protein first, always.
If you truly cannot eat solid food in the morning, a protein shake is acceptable. Just make sure it delivers at least 25 grams of protein. That single habit, starting the day with adequate protein, sets the tone for hitting your daily target.
Lunch strategies
By midday, most semaglutide users have some appetite return, though it is typically reduced compared to pre-medication levels. Lunch is often the easiest meal to optimize because you have more energy and less nausea than morning or evening.
Strong lunch options:
Grilled chicken salad with mixed greens, cucumber, tomato, avocado, and olive oil dressing (35g protein)
Turkey and vegetable wrap in a whole grain tortilla with hummus (28g protein)
Salmon over quinoa with roasted vegetables (32g protein)
Lentil soup with a side of Greek yogurt (24g protein combined)
Shrimp stir-fry with mixed vegetables over brown rice (30g protein)
Keep portions moderate. The biggest mistake at lunch is overeating because you feel hungrier than you did at breakfast. Semaglutide slows gastric emptying, so that meal sits in your stomach longer than you expect. Eat slowly, take at least 20 minutes per meal, and stop when you feel comfortably satisfied rather than full. The difference between satisfied and full on semaglutide is the difference between a productive afternoon and three hours of nausea.
Dinner approaches
Dinner is where many people struggle most. The timing of your semaglutide injection can affect appetite at different times of day. If you inject in the morning, appetite suppression might be strongest in the afternoon and evening. If you inject at night, mornings might be the hardest.
Dinner options designed for reduced appetite:
Baked cod with roasted asparagus and a small sweet potato (28g protein)
Turkey meatballs over zucchini noodles with marinara sauce (30g protein)
Chicken breast with steamed broccoli and quinoa (35g protein)
Tofu stir-fry with bell peppers, snap peas, and cashews over cauliflower rice (22g protein)
Lean beef burger, no bun, over a bed of mixed greens with tomato and avocado (28g protein)
Keep dinner lighter than lunch when possible. Your digestive system is already dealing with accumulated food from earlier in the day. A heavy dinner on top of delayed gastric emptying is the most common trigger for semaglutide bloating and nighttime discomfort.
Snacks that serve a purpose
On semaglutide, snacking should be strategic rather than habitual. You are eating less overall, so every snack needs to deliver nutrients, not just calories.
Smart snack options:
A small handful of almonds (6g protein, healthy fats)
Hard-boiled egg (6g protein, portable and easy)
String cheese (7g protein per stick)
Apple slices with a tablespoon of almond butter (4g protein, fiber)
Cucumber slices with hummus (fiber, easy to digest)
Beef or turkey jerky, low sodium (10g protein per ounce)
If your appetite is so suppressed that you cannot handle snacks at all, that is fine. Focus on getting adequate protein at your main meals instead. Forcing yourself to eat when you have no appetite often triggers nausea and does more harm than good.
Foods to avoid while taking semaglutide
Just as important as knowing what to eat is knowing what to avoid. Some foods that were perfectly fine before semaglutide become problematic because of how the medication changes your digestive process. This is not about willpower or discipline. It is about biochemistry. Certain foods interact poorly with slowed gastric emptying and altered gut motility.
Greasy and fried foods
Fatty, fried foods are the single biggest trigger for nausea on semaglutide. High-fat foods already take longer to digest than protein or carbohydrates. When you add semaglutide-induced gastroparesis on top of that, greasy food can sit in your stomach for six to eight hours. The result is persistent nausea, bloating, and sometimes vomiting.
Foods to avoid or minimize:
French fries and other deep-fried items
Fried chicken
Pizza with thick, oily crust
Fast food burgers
Cream-based sauces and gravies
Butter-heavy dishes
This does not mean you can never eat these foods again. It means that during active treatment, especially in the first two to four months, these foods are likely to make you miserable. As your body adapts to semaglutide and you find your tolerance levels, you may be able to reintroduce small amounts. But most long-term users report that their desire for greasy food decreases permanently, which is actually one of the neurological effects of GLP-1 receptor activation.
For a complete breakdown of foods that cause the most problems, check our guide on foods to avoid on semaglutide.
Refined carbohydrates and added sugars
White bread. Pastries. Sugary cereals. Soda. Candy. These foods were already nutritionally poor before semaglutide, but now they are actively counterproductive.
Semaglutide improves insulin secretion and blood sugar regulation. Refined carbohydrates and added sugars spike blood glucose rapidly, forcing your body to work harder to manage the surge. This creates a cycle of blood sugar spikes and crashes that increases cravings, undermines energy levels, and fights against the metabolic improvements semaglutide is trying to deliver.
Beyond the metabolic effects, sugary foods offer calories without protein, fiber, or meaningful micronutrients. When you are eating fewer total calories because of appetite suppression, every calorie from sugar is a calorie that could have been protein protecting your muscle mass or fiber supporting your digestive health. The opportunity cost is enormous.
Carbonated beverages
Carbonated drinks, including diet soda and sparkling water, can exacerbate burping on semaglutide and increase the sensation of bloating. The carbon dioxide gas adds volume to an already slow-emptying stomach. Many users find that switching from carbonated to still beverages resolves a significant portion of their gastrointestinal complaints.
Alcohol
Alcohol on semaglutide requires careful consideration. The medication can intensify the effects of alcohol because of slowed gastric emptying, meaning alcohol stays in contact with your stomach lining longer and absorbs differently. Many users report feeling the effects of alcohol faster and more intensely than before.
Beyond the physiological interactions, alcohol provides empty calories (7 calories per gram, almost as much as fat at 9 calories per gram) and impairs judgment about food choices. One or two drinks can derail an entire day of careful eating. For a detailed analysis of drinking on semaglutide, including which beverages cause the fewest problems, see our dedicated guide.
Spicy foods in the early weeks
Spicy foods are not universally problematic, but during the first two to four weeks of semaglutide use, when gastrointestinal side effects peak, spicy foods can amplify nausea and stomach discomfort. Many users find they can reintroduce moderate spice levels after the initial adjustment period. Listen to your body and reintroduce gradually.
Very high-fiber foods in large quantities
This one surprises people. Fiber is important, we covered that already. But consuming large amounts of high-fiber foods all at once, think a massive raw vegetable salad or a huge serving of beans, can worsen bloating and abdominal discomfort on semaglutide. The key is moderate, consistent fiber intake rather than large boluses.
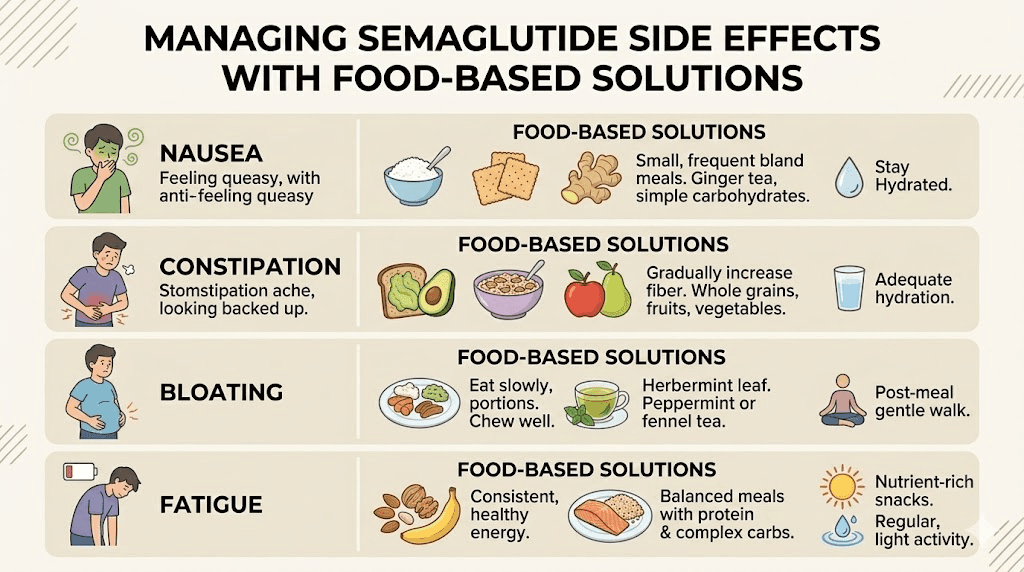
Managing side effects through diet
Nearly every semaglutide user experiences some gastrointestinal side effects, particularly in the first two to four weeks and after dose increases. Research from the STEP trials shows that nausea affects 40% to 44% of participants, while constipation, diarrhea, and vomiting are also common. Most of these side effects are transient, resolving as your body adapts. But dietary choices can dramatically reduce their severity and duration.
Nausea management through food
Nausea is the single most reported side effect. It typically peaks within the first few days after a dose and gradually improves over two to four weeks at each dose level. Understanding when side effects hit after taking semaglutide helps you plan your meals strategically.
Dietary strategies for nausea:
Eat smaller, more frequent meals. Instead of three standard meals, try five to six smaller eating occasions spread throughout the day. Smaller volumes put less pressure on a stomach that is already emptying slowly. This is the single most effective dietary change for managing semaglutide nausea.
Choose bland foods during peak nausea periods. The BRAT approach, bananas, rice, applesauce, and toast, is a classic recommendation for managing nausea from any cause. These foods are easily digestible, unlikely to trigger additional stomach upset, and provide enough calories to prevent low blood sugar.
Ginger works. This is not folk medicine. Ginger contains gingerols and shogaols, compounds with clinically demonstrated anti-nausea properties. Add fresh ginger to tea, sip ginger ale (flat, to avoid carbonation issues), or take ginger chews before meals. Multiple clinical guidelines recommend ginger as a first-line dietary intervention for nausea management on GLP-1 receptor agonists.
Peppermint is another evidence-based option. Peppermint tea or peppermint oil capsules can soothe stomach discomfort and reduce the sensation of nausea. Sip peppermint tea between meals rather than during meals to avoid filling up on liquid before food.
Avoid lying down immediately after eating. When gastric emptying is delayed, lying down increases the chance of acid reflux and worsens nausea. Stay upright for at least 30 minutes after eating. A gentle walk after meals helps stimulate digestion and reduces nausea more effectively than sitting still.
Constipation solutions
Slowed gastric emptying means slowed transit through the entire digestive tract. Constipation on semaglutide is extremely common and can become severe if not addressed proactively through diet.
Dietary approaches for constipation:
Increase water intake. Dehydration is the number one contributor to constipation on semaglutide. When you are eating less food, you are also getting less water from food sources. Most healthcare providers recommend at least 64 ounces (about 2 liters) of water daily, and many semaglutide users need more. Carry a water bottle everywhere. Set reminders if you have to. This single habit prevents more constipation than any supplement or medication.
Add fiber gradually. We covered this earlier but it bears repeating in the context of constipation specifically. Ground flaxseed (2 tablespoons daily mixed into yogurt or a smoothie) provides both soluble and insoluble fiber. Chia seeds do the same. Prunes remain one of the most effective natural remedies for constipation, with sorbitol providing an osmotic laxative effect alongside fiber.
Include magnesium-rich foods. Magnesium citrate has a natural stool-softening effect. Foods high in magnesium include dark leafy greens, pumpkin seeds, dark chocolate (in moderation), avocados, and almonds. If dietary sources are not enough, a magnesium supplement may help, but discuss this with your healthcare provider first.
Bloating and gas reduction
Bloating on semaglutide often results from food fermenting in a slow-moving digestive system. Reducing gas-producing foods during the adjustment period helps significantly.
Common gas producers to moderate initially: cruciferous vegetables in large quantities (broccoli, cauliflower, cabbage), beans and lentils in large servings, sugar alcohols (found in many sugar-free products), and dairy products if you have any degree of lactose intolerance.
Cooking vegetables rather than eating them raw reduces gas production because heat breaks down some of the fibers that gut bacteria ferment. Soaking dried beans overnight and draining the water before cooking also reduces their gas-producing potential.
Fatigue and energy management
Fatigue on semaglutide can have dietary roots. When you are eating significantly fewer calories than your body is accustomed to, energy drops are expected. But certain dietary patterns make fatigue worse than it needs to be.
Blood sugar stability is key. Eating regular meals with balanced macronutrients, especially combining protein with complex carbohydrates, prevents the blood sugar crashes that cause afternoon energy slumps. Skipping meals entirely and then eating one large meal is the worst approach for energy levels, even though some semaglutide users fall into this pattern because of suppressed appetite.
Iron and B-vitamin intake often decreases when overall food intake decreases. These nutrients are critical for energy production. If you notice persistent fatigue on GLP-1 medications, have your healthcare provider check blood levels of iron, ferritin, B12, and folate. Supplementation may be necessary.
Several compound formulations of semaglutide include B12 specifically to address this issue. Semaglutide with B12 and semaglutide with methylcobalamin are popular options that combine the GLP-1 receptor agonist with vitamin supplementation.
Phase-based eating on semaglutide
Your diet on semaglutide should not be static. As your body adapts to the medication and as your dose increases, your dietary needs and tolerances change. A phase-based approach acknowledges this reality and evolves with you.
Phase 1: weeks 1 through 4 (the adjustment period)
This is the hardest phase for most people. Your body is encountering a GLP-1 receptor agonist for the first time, and the gastrointestinal effects are at their peak. During the first week on semaglutide, many people struggle to eat anything at all.
Phase 1 dietary priorities:
Survival comes first. Do not worry about optimizing macros perfectly during the first week. Focus on keeping food down, staying hydrated, and hitting a minimum protein threshold. If you can consume 60 to 80 grams of protein daily during this phase, you are doing well.
Choose the simplest, blandest foods. Plain chicken breast, white rice, scrambled eggs, broth-based soups, crackers, bananas, applesauce. This is not the time for culinary ambition. It is the time for functional eating that keeps your body fueled without triggering nausea.
Eat five to six small meals instead of three standard ones. Portions should be roughly half of what you would normally eat. Think snack-sized meals rather than full plates.
Drink water between meals rather than during meals. Filling your stomach with liquid while eating can intensify the feeling of uncomfortable fullness. Sip water consistently throughout the day, but taper off 15 to 20 minutes before eating and wait 20 to 30 minutes after eating to resume drinking.
Protein shakes become your best friend during this phase. When you cannot tolerate solid food, a GLP-1 protein shake provides critical amino acids in a form that is much easier on the stomach.
Phase 2: weeks 5 through 12 (building momentum)
By week five, most people have adapted to the initial dose and gastrointestinal side effects have diminished significantly. Your appetite is still suppressed, but you can tolerate a wider variety of foods. This is when dietary optimization really begins.
Phase 2 dietary priorities:
Increase protein targets to the full 1.2 to 1.5 grams per kilogram of body weight. Now that your stomach can handle more, prioritize hitting this target consistently. Track your intake for at least two weeks to establish whether you are actually meeting your goals.
Expand vegetable variety. Move beyond the bland survival foods of Phase 1 and incorporate a full spectrum of colorful vegetables. Different colors indicate different phytonutrients, and variety ensures you are covering your micronutrient bases.
Introduce healthy fats more deliberately. Avocado, olive oil, nuts, and fatty fish should become regular parts of your diet. These foods support hormone production, brain function, and absorption of fat-soluble vitamins, all of which are important during active weight loss.
Start paying attention to meal timing around your injection. Some users find that eating lighter on injection day and the day after reduces side effects when semaglutide suppresses appetite most intensely. Others find no difference. Experiment and find what works for your body.
If you experience dose-increase side effects during this phase (nausea returning temporarily after stepping up from 0.25 mg to 0.5 mg, for example), temporarily revert to Phase 1 eating strategies for three to five days until your body adjusts.
Phase 3: months 3 through 6 (optimization)
You are now an experienced semaglutide user. Your weight loss is progressing, your body has adapted to the medication, and you know which foods your stomach handles well. This is the phase where dietary optimization has the biggest impact on your results.
Phase 3 dietary priorities:
Fine-tune protein distribution. Rather than trying to hit your entire protein target in one or two meals, distribute it evenly across the day. Research on muscle protein synthesis suggests that 25 to 40 grams of protein per meal, consumed every three to four hours, maximizes muscle preservation. This is more effective than eating 80 grams at dinner and 20 grams at breakfast.
Address any nutrient deficiencies. By month three, reduced food intake can lead to subclinical deficiencies in iron, calcium, vitamin D, B vitamins, and zinc. Ask your healthcare provider about blood work to check levels. Supplementation is often necessary during extended semaglutide use.
Incorporate resistance training nutrition. If you are exercising, and you should be for muscle preservation, your nutritional needs increase. Consuming 20 to 30 grams of protein within an hour after resistance training supports muscle repair and growth. This is especially important on semaglutide, where the default trajectory is muscle loss alongside fat loss.
Begin exploring long-term dietary sustainability. The eating patterns you develop during this phase should be ones you can maintain indefinitely, not just while on the medication. Consider whether your current approach is something you would enjoy and follow for years, not just months.
Phase 4: maintenance and beyond
Whether you plan to stay on semaglutide long-term or eventually taper off, your dietary habits need to be sustainable. Research shows that weight regain after discontinuing semaglutide is common, often occurring within three to six months. The people who maintain their results are the ones who built lasting dietary habits during treatment rather than treating semaglutide as a temporary fix.
Understanding how long to stay on semaglutide involves considering both your weight goals and your dietary readiness for eventual discontinuation. If your current diet depends entirely on semaglutide-suppressed appetite to maintain, you are not ready to stop the medication.
Transition strategies include gradually increasing portion sizes to test your natural hunger signals, practicing mindful eating techniques that help you recognize true hunger versus habitual eating, and maintaining the protein-first approach even after appetite returns to pre-medication levels.
For users who experience semaglutide withdrawal symptoms including appetite rebound, having an established dietary framework is crucial. The dietary habits you build during treatment are your safety net.
Hydration: the overlooked essential
Water deserves its own section because dehydration on semaglutide is surprisingly common and causes a cascade of problems that people blame on the medication itself.
When you eat less food, you get less water from food. Most people do not realize that food contributes roughly 20% of daily water intake. Fruits, vegetables, soups, and cooked grains all contain significant water. When your overall food volume drops by 30% to 50% on semaglutide, your water intake from food drops proportionally unless you compensate by drinking more.
Dehydration on semaglutide manifests as headaches, dizziness, constipation, fatigue, dry mouth, and dark urine. These symptoms overlap with semaglutide side effects, so many people assume the medication is causing them when the real culprit is inadequate fluid intake.
Hydration guidelines for semaglutide users:
Aim for at least 64 ounces (2 liters) of water daily as a baseline
Add 8 ounces for every 30 minutes of exercise
Add 8 ounces for every caffeinated beverage consumed (caffeine is a mild diuretic)
In hot weather or at altitude, increase by an additional 16 to 32 ounces
Monitor urine color as a hydration indicator: pale yellow is the target
Drink water between meals rather than during meals. Filling an already slow-emptying stomach with liquid alongside food increases the sensation of uncomfortable fullness and can trigger nausea. Take small sips throughout the day rather than drinking large volumes at once.
Electrolytes matter too. When you eat less and drink more water, you can dilute your electrolyte balance. Adding a pinch of salt to water, drinking bone broth, or using a low-sugar electrolyte supplement helps maintain sodium, potassium, and magnesium levels. This is particularly important if you experience muscle cramps, which are sometimes reported alongside fatigue on semaglutide.
Supplements to consider on semaglutide
A well-structured diet covers most nutritional needs. But when you are eating significantly less food overall, gaps emerge. These are the supplements most commonly recommended by healthcare providers for semaglutide users.
Essential supplements
Multivitamin: A basic insurance policy against micronutrient deficiencies. Choose one that includes iron, zinc, selenium, and B vitamins. Take it with a meal that contains some fat for better absorption of fat-soluble vitamins (A, D, E, K).
Vitamin D: Deficiency is extremely common in the general population and becomes more likely on reduced caloric intake. Many healthcare providers recommend 1,000 to 2,000 IU daily, though individual needs vary based on blood levels, sun exposure, and geographic location.
Vitamin B12: Critical for energy production and nerve function. Semaglutide can reduce B12 absorption by slowing gastric emptying and altering the stomach environment. Some compound formulations include B12 directly. If yours does not, supplementation or regular B12 injections are worth discussing with your provider. Learn more about the benefits of semaglutide with B12.
Calcium: Reduced food intake often means reduced calcium intake. If you are not consuming two to three servings of dairy daily, or equivalent calcium-rich foods, supplementation supports bone health during weight loss.
Conditionally beneficial supplements
Magnesium citrate: Supports bowel regularity (addresses constipation), muscle function, sleep quality, and stress management. A dose of 200 to 400 mg daily in the evening is commonly recommended.
Omega-3 fatty acids: If you do not eat fatty fish at least twice per week, an omega-3 supplement supports anti-inflammatory pathways, brain health, and cardiovascular function. Choose a supplement that provides at least 1,000 mg of combined EPA and DHA.
Probiotics: Semaglutide alters gut motility, which can disrupt the microbiome. A broad-spectrum probiotic may support digestive health during treatment. Our guide on the best probiotics for semaglutide covers specific strains and products that pair well with GLP-1 treatment.
Fiber supplements: If you cannot hit your fiber target through food alone, a psyllium husk supplement (like Metamucil) provides soluble fiber that supports both bowel regularity and blood sugar management. Start with a small dose and increase gradually.
Some semaglutide formulations include complementary compounds beyond B12. Options like semaglutide with glycine, semaglutide with L-carnitine, and semaglutide glycine B12 blends aim to provide complementary nutritional support alongside the GLP-1 receptor agonist.
Common dietary mistakes on semaglutide
After analyzing thousands of semaglutide user experiences and consulting current research, certain dietary mistakes appear repeatedly. Avoiding these pitfalls accelerates your results and makes the experience significantly more comfortable.
Mistake 1: not eating enough
This sounds counterintuitive for a weight loss medication, but under-eating is one of the most common and most damaging mistakes. When appetite is severely suppressed, some people eat only 500 to 800 calories daily for weeks at a time.
This is too low. Severely restricting calories accelerates muscle loss, tanks your metabolism, depletes micronutrients, crashes energy levels, and sets you up for a massive rebound when appetite eventually returns. Most healthcare providers recommend that semaglutide users consume at least 1,200 to 1,500 calories daily for women and 1,500 to 1,800 for men, even when appetite is minimal.
The people who wonder why they are not losing weight on semaglutide sometimes discover that extreme under-eating has slowed their metabolism to the point where even reduced intake does not produce a deficit. Your body adapts to starvation-level calories by burning less. This is not what you want.
Mistake 2: ignoring protein
We covered this extensively in the protein section, but it bears repeating as a mistake because it is so widespread. The average semaglutide user who does not actively track protein intake gets roughly 40 to 60 grams daily. That is 30% to 50% below the recommended range for muscle preservation during weight loss.
Make protein tracking non-negotiable for at least the first three months. After that, most people develop enough intuition about their protein intake to maintain adequate levels without tracking.
Mistake 3: drinking calories
When solid food is hard to tolerate, many people turn to calorie-containing beverages: fruit juices, smoothies loaded with honey and fruit, sugary coffee drinks, and regular soda. These beverages provide calories without satiety, spike blood sugar, and displace protein from the diet.
The exception is protein shakes, which serve a functional purpose. Everything else should be calorie-free or very low calorie. Water, black coffee, unsweetened tea, and zero-calorie electrolyte drinks are your best options. If you drink smoothies, ensure they are protein-based rather than fruit-based, with at least 25 grams of protein and limited added sugars.
Mistake 4: skipping meals entirely then overeating
The suppress-and-binge cycle is common on semaglutide. You feel no hunger all morning and afternoon, skip meals, then suddenly get ravenous at dinner and eat a massive meal. This pattern is problematic for several reasons.
A large meal overwhelms an already slow digestive system, causing severe bloating, nausea, and discomfort. Your protein intake clusters into one meal instead of distributing throughout the day, which is less effective for muscle protein synthesis. And the feast-or-famine pattern disrupts blood sugar stability, creating energy crashes and mood swings.
Even when you are not hungry, eating small, planned meals at regular intervals produces better outcomes than waiting for hunger to strike. Set meal times rather than relying on appetite cues, especially during the first few months when those cues are dramatically suppressed.
Mistake 5: giving up on food variety
Some people find three or four foods that feel safe on semaglutide and eat nothing else for months. Chicken breast. Rice. Bananas. Repeat. While this approach avoids nausea, it virtually guarantees micronutrient deficiencies and makes the dietary experience unsustainable long-term.
After the initial adjustment phase, deliberately expand your food repertoire. Try one new food each week. Cook vegetables in different ways. Experiment with herbs and spices. The goal is building a diverse, sustainable dietary pattern, not surviving on a handful of bland foods indefinitely.
Mistake 6: not adjusting diet when dose increases
Every dose increase is essentially a mini-restart of the adjustment period. Gastrointestinal side effects often return temporarily, appetite suppression intensifies, and food tolerances may shift. The people who do best are the ones who temporarily revert to Phase 1 eating strategies, simpler foods, smaller meals, more frequent eating, for three to five days after each dose increase.
Review the semaglutide dosage guide to understand what to expect at each dose level, and plan your dietary adjustments accordingly.
Meal timing and injection day considerations
When you eat matters almost as much as what you eat on semaglutide. The medication follows a specific pharmacokinetic pattern, and aligning your meals with that pattern improves both results and comfort.
Injection day eating
Most semaglutide users find that appetite suppression peaks within 24 to 48 hours after injection. Planning accordingly makes a difference. Consider eating your most protein-rich meal before your injection, when appetite is relatively stronger. Keep injection day meals simple and easily digestible. Have bland backup foods available in case nausea hits.
The best time of day to take semaglutide may depend partly on your eating schedule. Some users inject in the morning and find their appetite is lowest at dinner. Others inject at bedtime and find breakfast the most difficult meal. Experiment with timing to find the pattern that allows you to hit your nutritional targets most consistently.
Eating window considerations
Some semaglutide users naturally gravitate toward intermittent fasting patterns because their appetite simply does not show up for 14 to 16 hours at a stretch. While there is nothing inherently wrong with condensed eating windows, the critical concern is whether you can hit your protein targets within the shorter eating period.
If your eating window is 8 hours and you need 100 grams of protein daily, you need to average 12.5 grams of protein per hour of eating. That is very achievable with three meals during that window, each containing 33 grams of protein. If your eating window shrinks to 4 hours, hitting 100 grams becomes much harder without protein supplementation.
Do not force intermittent fasting on top of semaglutide unless it happens naturally and you can still meet your nutritional requirements. The medication already restricts intake enough. Adding deliberate fasting on top can push caloric intake dangerously low.
Pre-and post-exercise nutrition
Exercise, particularly resistance training, is strongly recommended during semaglutide use for muscle preservation. Your pre-and post-workout nutrition supports this effort.
Before exercise: Eat a small meal or snack containing both protein and carbohydrates 60 to 90 minutes before training. A banana with a tablespoon of peanut butter, or a small portion of Greek yogurt with berries, provides enough fuel without overwhelming your stomach. If exercising first thing in the morning with no appetite, even a protein shake is better than training completely fasted.
After exercise: Consume 20 to 30 grams of protein within 60 minutes of completing resistance training. This timing takes advantage of the post-exercise window when muscle protein synthesis is elevated. A protein shake is ideal if solid food is unappealing after training.
For users exploring whether they can lose weight on semaglutide without exercise, the answer is yes, but the quality of weight loss, specifically the ratio of fat to muscle lost, is significantly worse without resistance training. Diet and exercise work together on semaglutide to produce the best body composition outcomes.
Special dietary considerations
Vegetarian and vegan diets on semaglutide
Plant-based diets can absolutely work on semaglutide, but they require more careful planning to hit protein targets. Plant proteins are generally less bioavailable than animal proteins and often lack one or more essential amino acids.
Plant-based protein strategies:
Combine complementary proteins (rice and beans, hummus and pita) to get complete amino acid profiles
Prioritize high-protein plant foods: tempeh (31g per cup), seitan (25g per 3.5 oz), edamame (17g per cup), lentils (18g per cup)
Use pea or soy protein powder to supplement intake
Include tofu at multiple meals (it is versatile and well-tolerated on semaglutide)
Vegan diets are also typically lower in B12, iron, calcium, zinc, and omega-3 fatty acids, all of which are already at risk of deficiency during semaglutide use. Supplementation is strongly recommended for plant-based eaters on GLP-1 medications.
Diabetes-specific dietary considerations
Semaglutide was originally developed for type 2 diabetes management, and many users take it for blood sugar control rather than weight loss alone. If you are using semaglutide for diabetes, your dietary approach needs to account for blood sugar management alongside weight optimization.
Carbohydrate consistency is important. Rather than eliminating carbohydrates, focus on consuming consistent amounts at consistent times. This allows your semaglutide dose to work predictably alongside your meal pattern. Dramatic swings between very low-carb days and high-carb days can cause blood sugar instability.
Monitor blood sugar more frequently during dietary changes. Adding or removing foods, changing meal timing, or adjusting portion sizes can all affect how semaglutide interacts with your blood sugar. Your healthcare provider may need to adjust your dose as your diet evolves.
The glycemic index of your carbohydrate sources matters more for diabetic users than for those taking semaglutide purely for weight loss. Choose low-glycemic carbohydrates (sweet potatoes, steel-cut oats, quinoa, most vegetables) over high-glycemic options (white rice, white bread, potatoes) to minimize blood sugar spikes.
Managing food aversions
Semaglutide frequently causes food aversions that did not exist before treatment. Previously enjoyed foods may suddenly seem repulsive. Common aversions include meat (particularly red meat), eggs, coffee, and sweet foods. These aversions are neurological, not gastrointestinal, and they are mediated by the same brain pathways that semaglutide uses to reduce appetite.
If you develop an aversion to a major protein source, replace it rather than simply eliminating it. If chicken repulses you, switch to fish. If eggs make you nauseous, try Greek yogurt. If all animal protein is off-putting, plant-based protein shakes and tofu become your primary protein vehicles.
Most food aversions stabilize after two to three months on a consistent dose. Some resolve completely. Others persist throughout treatment. Being flexible and willing to adapt your diet rather than fighting your body produces better long-term outcomes.
Comparing semaglutide dietary needs to other GLP-1 medications
If you are considering switching medications or curious about how dietary requirements differ between GLP-1 options, the principles are broadly similar but the intensity varies.
Semaglutide versus tirzepatide represents the most common comparison. Tirzepatide activates both GLP-1 and GIP receptors, which can produce even stronger appetite suppression and potentially greater gastrointestinal side effects. The dietary strategies outlined in this guide apply to both medications, but tirzepatide users may need to be even more aggressive about small, frequent meals during the adjustment phase. Our guide on tirzepatide diet plans covers the specifics.
The side effect profiles between these medications differ somewhat, which affects dietary management. Tirzepatide users may experience more pronounced appetite suppression but potentially different patterns of gastrointestinal symptoms. The food strategies for managing foods to avoid on tirzepatide overlap significantly with semaglutide recommendations.
For users comparing their options more broadly, understanding how semaglutide and tirzepatide dosing compares can help contextualize why dietary experiences differ at various dose levels. Higher relative doses of either medication generally require more careful dietary management.
Newer options like retatrutide add a third receptor (glucagon) to the mix, which may further affect dietary needs and tolerances. As these medications evolve, the core dietary principles remain consistent: protein first, nutrient density matters, and eating with the medication rather than against it produces the best results.
Building a sustainable relationship with food
Here is the truth that most semaglutide diet guides ignore. The medication changes your appetite, but it does not automatically change your relationship with food. Emotional eating, stress eating, habitual snacking, comfort food patterns, these do not disappear because your appetite is suppressed. They just get overridden temporarily.
When semaglutide is eventually discontinued, or when your body adapts to a dose and appetite partially returns, those underlying patterns resurface. This is why weight regain after stopping semaglutide is so common in the research, occurring in three to six months for many users.
Use the period of suppressed appetite as an opportunity to rebuild your food habits from the ground up. You are essentially getting a neurological reset on hunger signals and food cravings. Take advantage of it.
Practical strategies for lasting change
Practice mindful eating at every meal. Put your fork down between bites. Chew thoroughly. Pay attention to the taste, texture, and satisfaction level of what you are eating. Semaglutide makes this easier because you are eating more slowly anyway, and the urgency around food diminishes.
Learn to cook simple, nutritious meals if you do not already know how. Dependency on takeout and processed food makes it nearly impossible to control nutrition quality and nearly guarantees that caloric intake will creep up when appetite returns. Three to five go-to meals that you can prepare in 30 minutes or less form the backbone of a sustainable diet.
Identify and address emotional eating triggers. If you used to eat when stressed, bored, anxious, or lonely, find alternative coping mechanisms now while food is less appealing. Exercise, meditation, social connection, creative outlets, whatever replaces the function that food used to serve. This work is what separates people who maintain their results from people who regain.
Consider working with a registered dietitian, particularly one experienced with GLP-1 medications. A professional can personalize your nutrition plan, identify deficiency risks, and provide accountability throughout the process. SeekPeptides members access comprehensive nutritional guidance as part of their protocol resources, helping bridge the gap between generic dietary advice and individualized nutrition planning.
Tracking your progress beyond the scale
Weight is the most obvious metric, but it is not the most important one when your diet on semaglutide is working correctly. Track these additional indicators to get a complete picture of your progress.
Body composition: If possible, get regular body composition measurements (DEXA scan, bioelectrical impedance, or even simple body measurements) to ensure you are losing fat while preserving muscle. The scale does not differentiate between five pounds of fat loss and five pounds of muscle loss, but your health outcomes are dramatically different between those two scenarios.
Energy levels: Rate your daily energy on a 1 to 10 scale. If energy consistently drops below 5, your diet likely needs adjustment, either more calories, more protein, or addressing a specific nutrient deficiency. People who track semaglutide results week by week often notice that energy patterns correlate closely with dietary quality.
Digestive comfort: Track which foods cause problems and which are well-tolerated. This personalized food diary becomes your most valuable dietary tool within weeks. Everyone responds differently to semaglutide, and your optimal food list will be unique to you.
Strength and physical function: If you are resistance training (and you should be), track whether your strength is maintaining or declining. Declining strength despite consistent training usually indicates insufficient protein intake or excessive caloric restriction.
Blood markers: Regular blood work (every three to six months) monitors vitamin levels, metabolic markers, kidney and liver function, and blood sugar control. These objective measurements provide feedback that subjective feelings cannot.
Use the peptide calculator and other tools on SeekPeptides to stay on top of your dosing protocols while implementing these dietary strategies. The combination of precise dosing and optimized nutrition produces outcomes that neither approach achieves alone.
Sample daily eating patterns
These are not rigid meal plans. They are templates showing how a well-structured day of eating on semaglutide looks in practice. Adjust portions, foods, and timing based on your individual needs and tolerances.
Sample day: early weeks (Phase 1)
7:00 AM: Protein shake (whey protein, almond milk, half banana), 25g protein
10:00 AM: Greek yogurt with a sprinkle of granola, 15g protein
12:30 PM: Scrambled eggs (2) with toast, 14g protein
3:30 PM: String cheese and a few crackers, 7g protein
6:00 PM: Chicken noodle soup (homemade with extra chicken), 18g protein
Daily total: approximately 79g protein, 1,100-1,300 calories
Sample day: momentum phase (Phase 2)
7:30 AM: Overnight oats with protein powder, chia seeds, and berries, 28g protein
12:00 PM: Grilled chicken salad with avocado, mixed greens, and olive oil dressing, 35g protein
3:30 PM: Hard-boiled eggs (2) and an apple, 12g protein
6:30 PM: Baked salmon with roasted broccoli and quinoa, 32g protein
Daily total: approximately 107g protein, 1,400-1,600 calories
Sample day: optimization phase (Phase 3)
7:00 AM: Veggie omelet (3 eggs, spinach, peppers, mushrooms) with whole grain toast, 24g protein
10:00 AM: Cottage cheese with sliced peaches and walnuts, 16g protein
1:00 PM: Turkey and avocado wrap with a side of lentil soup, 34g protein
4:00 PM: Post-workout protein shake, 25g protein
7:00 PM: Grilled shrimp with sauteed vegetables and brown rice, 28g protein
Daily total: approximately 127g protein, 1,600-1,800 calories
Notice the progression. Phase 1 focuses on getting any protein in, using simple foods and small portions. Phase 2 introduces more variety and brings protein closer to target. Phase 3 distributes protein evenly across the day, includes pre-and post-workout nutrition, and provides enough total calories to support an active lifestyle while still maintaining a weight loss deficit.
For more structured meal planning resources, our guides on semaglutide diet plans and best foods on semaglutide provide additional frameworks and recipes.
When to seek professional help with your diet
While this guide provides a comprehensive framework, certain situations warrant professional dietary guidance. Consult a registered dietitian or your healthcare provider if:
You are losing more than 3 pounds per week consistently (may indicate excessive restriction)
You cannot keep any food down for more than 48 hours
You experience persistent gastrointestinal symptoms that do not improve after four weeks at a given dose
You have a history of eating disorders (semaglutide appetite suppression can trigger disordered patterns)
You have diabetes and are struggling to balance blood sugar with dietary changes
Blood work reveals nutrient deficiencies despite supplementation
You experience significant hair loss, which can indicate protein or nutrient deficiency (see our guide on GLP-1 and hair loss)
You hit a weight loss plateau lasting more than four weeks despite dietary compliance
If you are struggling with results, understanding what to do when semaglutide does not work after four weeks often comes down to dietary optimization. The medication provides the appetite suppression and metabolic benefits. Your diet determines how effectively you capitalize on those benefits.
For researchers and self-directed users looking for more comprehensive guidance, SeekPeptides offers evidence-based protocols, detailed nutritional guides, and a community of experienced users who have navigated these exact dietary challenges. Having access to proven frameworks and real-world feedback from thousands of users shortens the learning curve considerably.
Frequently asked questions
Can I eat normally on semaglutide?
You can eat most foods on semaglutide, but your definition of normal will change. Portions will be smaller, greasy and sugary foods will likely cause discomfort, and your appetite will be significantly reduced. The goal is not to eat normally but to eat optimally, prioritizing protein, fiber, and nutrient-dense foods within a reduced caloric window. Most users find their eating habits naturally shift toward healthier patterns because the medication reduces cravings for processed foods.
How many calories should I eat on semaglutide?
Most healthcare providers recommend at least 1,200 to 1,500 calories daily for women and 1,500 to 1,800 for men during semaglutide treatment. Going below these minimums increases the risk of fatigue, muscle loss, nutrient deficiencies, and metabolic slowdown. A safe rate of weight loss on semaglutide is 1 to 2 pounds per week. If you are losing faster than that consistently, you may be eating too little.
Should I count calories or macros on semaglutide?
Tracking protein intake is the most important single metric. If you only track one thing, track protein, aiming for 1.2 to 1.5 grams per kilogram of body weight daily. Full macro tracking is helpful but not essential for most users. Calorie counting can become counterproductive if it leads to obsessive restriction. The plate method, half vegetables, quarter protein, quarter complex carbs, provides a simpler framework that works well for most people.
What happens if I eat too much on semaglutide?
Overeating on semaglutide is uncomfortable because of slowed gastric emptying. Symptoms include severe bloating, nausea, stomach pain, and sometimes vomiting. Your body generally prevents significant overeating through intense fullness signals, but pushing past those signals, particularly with greasy or heavy foods, leads to several hours of discomfort. If you accidentally overeat, stay upright, sip water slowly, and walk gently. The discomfort will pass as digestion eventually processes the food.
Is intermittent fasting safe with semaglutide?
Intermittent fasting is not inherently dangerous with semaglutide, but it is often unnecessary because the medication already restricts intake naturally. The main risk is that a condensed eating window makes it harder to hit protein targets. If you naturally gravitate toward eating within an 8-hour window and can still consume adequate protein, that pattern is fine. Deliberately restricting your eating window further, to 4 or 6 hours, on top of semaglutide-suppressed appetite risks excessive caloric restriction.
What should I eat on my first day of semaglutide?
Start simple. A protein shake for breakfast, a small chicken and rice meal for lunch, and a light soup for dinner is a reasonable first-day approach. Have ginger tea, crackers, and bananas on hand in case nausea hits. Do not plan an elaborate or heavy meal on injection day. Read our complete guide on your first week on semaglutide for day-by-day guidance on what to expect and how to eat during those initial days.
Can I drink coffee on semaglutide?
Yes, coffee is generally safe on semaglutide. Black coffee or coffee with a small amount of milk is fine. Avoid large sugary coffee drinks (frappuccinos, mochas) as they add significant empty calories. Some users find that coffee on an empty stomach worsens nausea, so try having a small amount of food before your coffee if this is an issue. Caffeine is a mild diuretic, so compensate with extra water intake.
Does semaglutide work without dieting?
Semaglutide produces weight loss even without deliberate dieting because it naturally reduces appetite and caloric intake. However, the quality of weight loss, specifically how much fat versus muscle you lose, depends heavily on dietary choices. Users who prioritize protein and nutrient-dense foods lose more fat and less muscle than those who eat whatever they want in smaller amounts. The medication does the heavy lifting on appetite, but your food choices determine whether you emerge healthier or just lighter.
External resources
Endocrine Society - Higher protein intake protects against muscle loss on semaglutide (ENDO 2025)
PMC - Clinical recommendations to manage gastrointestinal side effects of GLP-1 receptor agonists
PMC - Gastrointestinal tolerability of semaglutide 2.4 mg (STEP trials analysis)
For researchers serious about optimizing their semaglutide protocols and nutrition, SeekPeptides offers the most comprehensive resource available, with evidence-based dosing guides, detailed nutritional frameworks, personalized protocol tools, and a community of thousands who have navigated these exact dietary questions successfully.
In case I do not see you, good afternoon, good evening, and good night. May your protein stay abundant, your digestion stay comfortable, and your results stay lasting.