Feb 6, 2026

The before and after photos look too good to be real. A woman stands in a clinical hallway, holding up jeans that could fit two of her. Numbers at the bottom claim 84 pounds lost, 17 dress sizes gone, labs completely normalized. You scroll to the comments section. Half the people call it fake. The other half want to know how fast it happened, what dose she used, whether the results will last.
Most tirzepatide before and after stories fall into predictable patterns that researchers have documented across thousands of participants. Some lose 25% of their body weight in 72 weeks while others plateau at 8%. Some drop four dress sizes in six months while others struggle past month two. The difference between dramatic transformation and modest results comes down to factors you can measure, track, and in many cases, control.
Understanding what determines success matters more than looking at transformation photos. The photos show outcomes but hide the protocols behind them.
This guide examines real tirzepatide weight loss results across every timeframe from week one through year two, breaks down the factors that predict whether you will be a strong responder or a late bloomer, and provides the specific strategies that separate people who lose 40 pounds from people who lose 80.
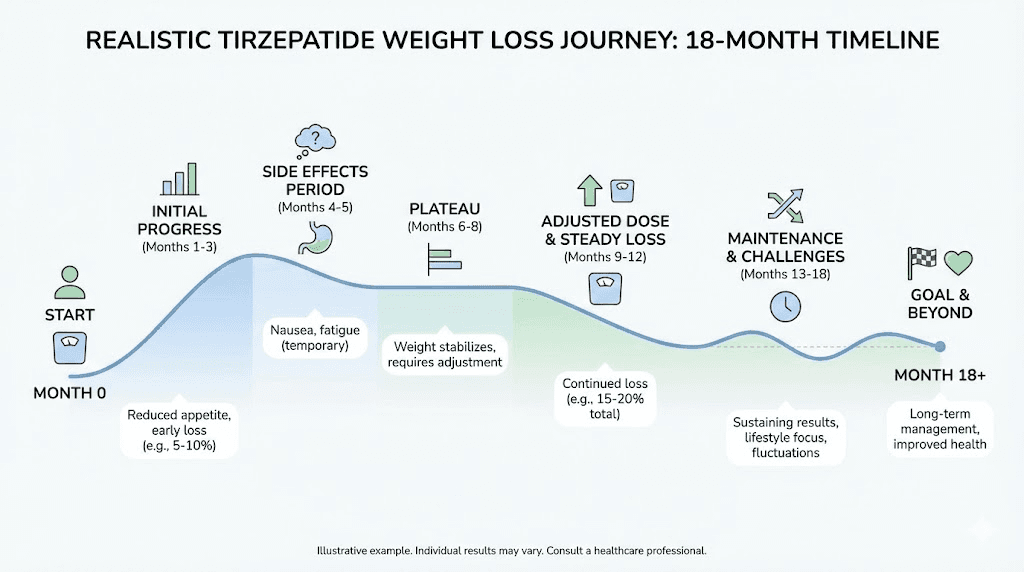
How tirzepatide weight loss progresses week by week
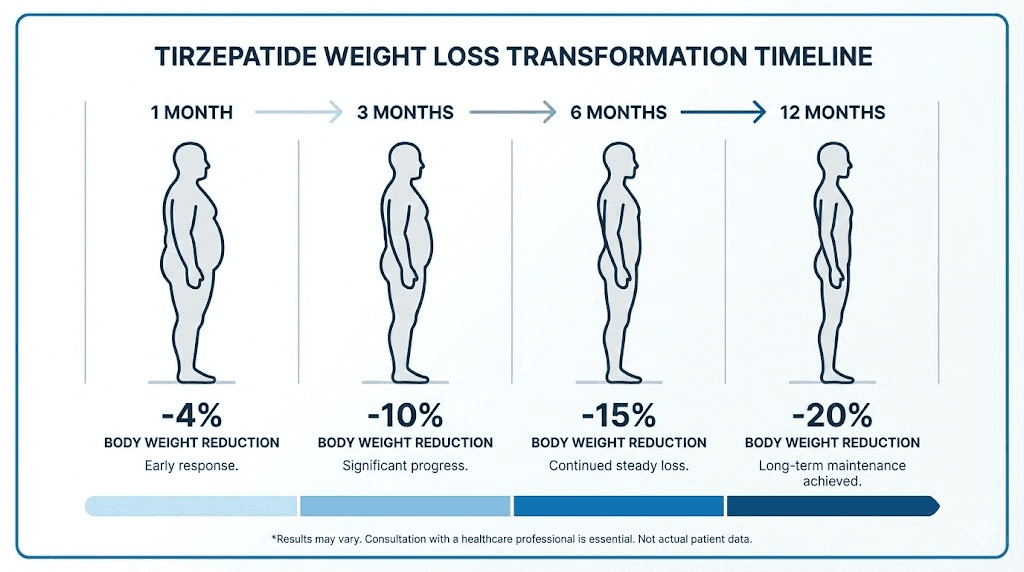
Understanding the week-by-week progression helps set realistic expectations. Most dramatic before and after photos represent 6-12 months of consistent use, but changes start appearing much earlier.
Weeks 1-2: appetite suppression begins
The first noticeable change happens internally. Appetite drops within 7-10 days for most people. Food that used to trigger cravings stops generating the same compulsion. Portions that felt normal suddenly feel excessive. Your body signals fullness faster and maintains that signal longer between meals.
This shift happens because tirzepatide activates GIP and GLP-1 receptors that slow gastric emptying and enhance satiety signals. The peptide essentially recalibrates how your brain interprets hunger and fullness cues. Most researchers notice this change before they see any movement on the scale.
Weight loss during weeks 1-2 typically ranges from 2-4 pounds, though some people see more dramatic drops due to water weight reduction. The real value in this phase comes from behavioral changes. When appetite drops naturally, adherence to caloric deficits becomes significantly easier compared to traditional weight loss approaches.
Weeks 3-4: visible changes emerge
By week three, the scale starts moving consistently. Most people lose 1-2 pounds per week during this phase, bringing total weight loss to 5-8 pounds by the end of month one. Clothes fit differently. Faces appear slightly slimmer. Energy levels often improve as initial side effects from tirzepatide dosing begin to subside.
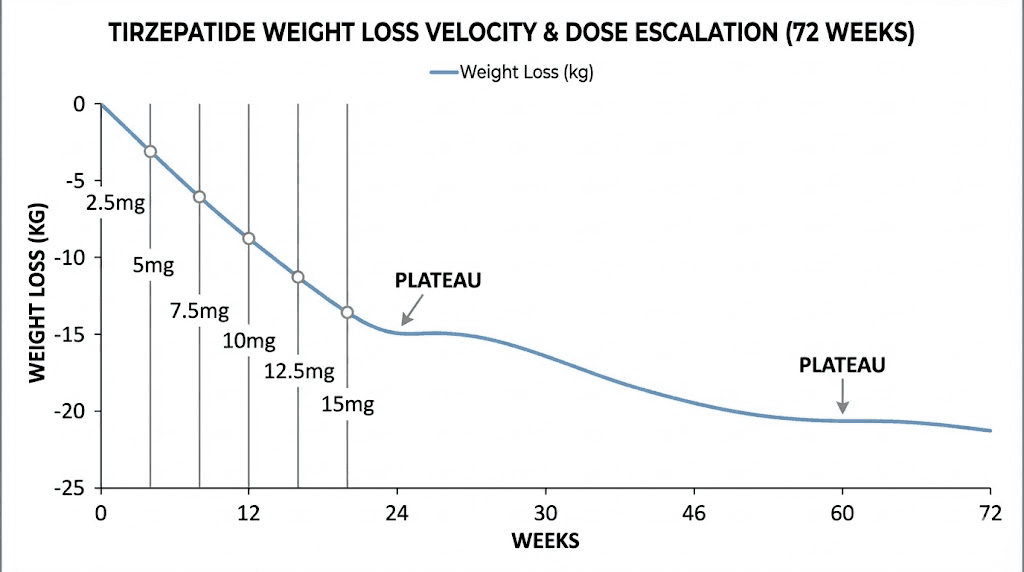
This timeline represents what happens on the starting dose, typically 2.5mg per week. Researchers who begin with microdosing approaches may see slower initial progress but better tolerance. Those who jump straight to higher doses sometimes experience faster weight loss but also more severe gastrointestinal effects that interfere with consistency.
Weeks 5-8: acceleration phase
Most protocols increase the dose at week 4 or 5. This escalation marks the beginning of accelerated weight loss. Average weekly loss increases to 2-3 pounds for many people during weeks 5-8. Total weight reduction by the end of month two typically reaches 8-12 pounds, though responses vary widely based on starting weight, metabolic factors, and adherence to tirzepatide diet recommendations.
The second month represents a critical period. Researchers who experience significant nausea or other tirzepatide side effects during dose escalation sometimes pause progress or reduce their dose. Those who titrate slowly and manage side effects proactively tend to maintain better consistency and achieve superior long-term outcomes.
Weeks 9-12: the three-month checkpoint
Clinical trials consistently show that the 12-week mark provides the first reliable predictor of long-term success. People who lose at least 5% of their body weight by week 12 typically achieve clinically significant results by month 6. Those who fail to reach this threshold require protocol adjustments, whether through dose optimization, dietary modifications, or investigation of potential issues affecting response.
Average weight loss at three months ranges from 10-20 pounds for most people, translating to 6-12% of starting body weight for someone beginning at 200 pounds. Before and after comparisons at this stage show noticeable but not dramatic changes. Waistlines shrink, faces slim down, energy improves, but the transformation remains subtle enough that distant acquaintances might not comment yet.
Early response matters more than most people realize. Research examining tirzepatide effectiveness timelines found that late responders still achieved meaningful weight loss, just to a lesser extent than early responders. If you are not seeing results by week 12, the protocol needs adjustment, not abandonment.
Three month results: the first major checkpoint
The three-month mark separates early responders from late responders. Clinical data shows that people who achieve at least 5% weight reduction by week 12 continue losing weight at higher rates through month 6 and beyond. Those who fall short of this threshold typically remain late responders throughout treatment, achieving lower total weight loss despite continuing the protocol.
Average weight loss at 3 months by dose
Dose level significantly influences three-month outcomes. The SURMOUNT trials provide the most reliable data on expected results across different dose ranges. Participants on 5mg lost an average of 15 pounds by week 12. Those on 10mg lost approximately 21 pounds. The 15mg group averaged 24 pounds lost.
These numbers represent clinical trial averages under controlled conditions with regular monitoring and support. Real-world results often vary. Some people exceed clinical trial averages due to aggressive dietary modifications or exercise protocols. Others fall below averages due to inconsistent dosing, poor diet adherence, or metabolic factors that blunt response.
Starting weight matters for interpreting three-month results. A 250-pound person losing 20 pounds achieves 8% body weight reduction, while a 150-pound person losing the same amount achieves 13% reduction. Percentage-based metrics provide better comparison than absolute pounds when evaluating whether your response falls within expected ranges for tirzepatide weight loss.
What three-month before and after photos reveal
Visual changes at three months show moderate but clear transformation. Face photos reveal reduced puffiness, more defined jawlines, and decreased fat around the neck and cheeks. Full-body photos show smaller waistlines, less abdominal distension, and improved body proportions. Clothes that fit snugly at baseline now hang loosely, though most people have not yet needed to replace their entire wardrobe.
The psychological impact of three-month changes often exceeds the visual impact. Energy levels improve significantly for most people. Physical activities that felt exhausting become manageable. Joint pain decreases as load on knees, hips, and ankles reduces. Sleep quality often improves. These non-scale victories motivate continued adherence even when weight loss temporarily slows during plateau periods.
Factors predicting strong vs weak response at 3 months
Early response patterns correlate with specific baseline characteristics. Research examining thousands of tirzepatide users found several predictors of robust three-month results. Higher starting BMI predicted greater absolute weight loss but similar percentage reduction. Female sex associated with slightly better early response rates. Absence of insulin resistance or metabolic syndrome predicted stronger initial drops.
Behavioral factors outweigh demographic predictors for many people. Consistent weekly dosing matters enormously. Missing even one dose per month can reduce total weight loss by 2-3 percentage points over six months. Dietary adherence plays a massive role. People who track calories or macros lose significantly more weight than those who rely solely on appetite suppression to create deficits.
Exercise intensity and frequency also influence three-month outcomes. Moderate cardio activity combined with resistance training protocols preserves muscle mass while accelerating fat loss. People who remain sedentary still lose weight through caloric deficit but experience less favorable body composition changes and slower overall progress.
Six month transformations: where dramatic changes appear
The six-month mark represents the sweet spot for tirzepatide before and after comparisons. Visual changes become dramatic enough that friends and family comment unprompted. Wardrobe replacement becomes necessary. Health markers like blood pressure, glucose, and lipids show substantial improvements.
Expected weight loss at 6 months
Clinical trial data shows that participants on 10mg tirzepatide lost an average of 38-42 pounds by week 24, representing roughly 15-17% of starting body weight for someone beginning at 240 pounds. Those on 15mg achieved even greater reductions, averaging 45-52 pounds or 18-21% of baseline weight.
Real-world outcomes span a wider range. Strong early responders sometimes exceed clinical trial averages, losing 50-60 pounds or more by month six. Late responders typically achieve 25-35 pounds of loss, still clinically meaningful but below trial averages. Non-responders who fail to lose at least 10-12% of body weight by this point need comprehensive protocol evaluation to identify barriers.
The distribution of weight loss matters as much as the total amount. People who lose weight consistently across all six months experience better results than those who see dramatic drops in months 1-3 followed by prolonged plateaus. Understanding your dose escalation schedule and adjusting when progress stalls helps maintain steady downward trends.
Six month before and after photo analysis
Six-month transformation photos show changes that casual observers immediately notice. Face photos reveal dramatic differences in cheek definition, jawline sharpness, and overall facial structure. Neck and shoulder areas show significant fat reduction. Full-body photos document substantial decreases in waist and hip circumferences, often amounting to 4-6 inches or more.
Clothing size changes at six months typically range from 2-4 sizes for most people. Someone who started in size 16 pants might now wear size 10-12. A person who began wearing XXL shirts might fit comfortably in large. These changes necessitate wardrobe updates and provide tangible evidence of progress beyond scale numbers.
Body composition shifts become visible at six months for people who incorporate strength training alongside tirzepatide. Muscle definition improves as overlying fat decreases. Shoulders and arms show improved tone. Core definition begins appearing as abdominal fat reduces. These changes create more aesthetically pleasing transformations compared to weight loss through diet alone.
Metabolic improvements alongside weight loss
The before and after story at six months extends beyond appearance. Blood work changes tell a compelling parallel narrative. HbA1c levels drop significantly for people with prediabetes or type 2 diabetes, often declining 1-2 percentage points. Fasting glucose normalizes for many participants. Triglycerides decrease substantially. HDL cholesterol typically improves while LDL declines.
Blood pressure responds dramatically to weight loss in most people. Someone who required medication for hypertension at baseline might achieve normal readings by month six without pharmaceutical intervention. Joint pain decreases as mechanical load on weight-bearing joints reduces. Mobility improves. Physical activities that felt impossible at baseline become routine.
Energy levels at six months often exceed pre-treatment baselines dramatically. Many people report feeling better than they have in years. Sleep quality improves. Mood stabilizes. Mental clarity increases. These subjective improvements matter as much as objective metrics for sustaining motivation through the remainder of the protocol.
Twelve month results and long-term outcomes
The 12-month checkpoint provides the most reliable data on tirzepatide efficacy and sustainability. Clinical trials extended through 72 weeks show that most people reach their maximum weight loss between months 9-14, followed by a maintenance phase where weight stabilizes.
Peak weight loss: when it happens and what determines it
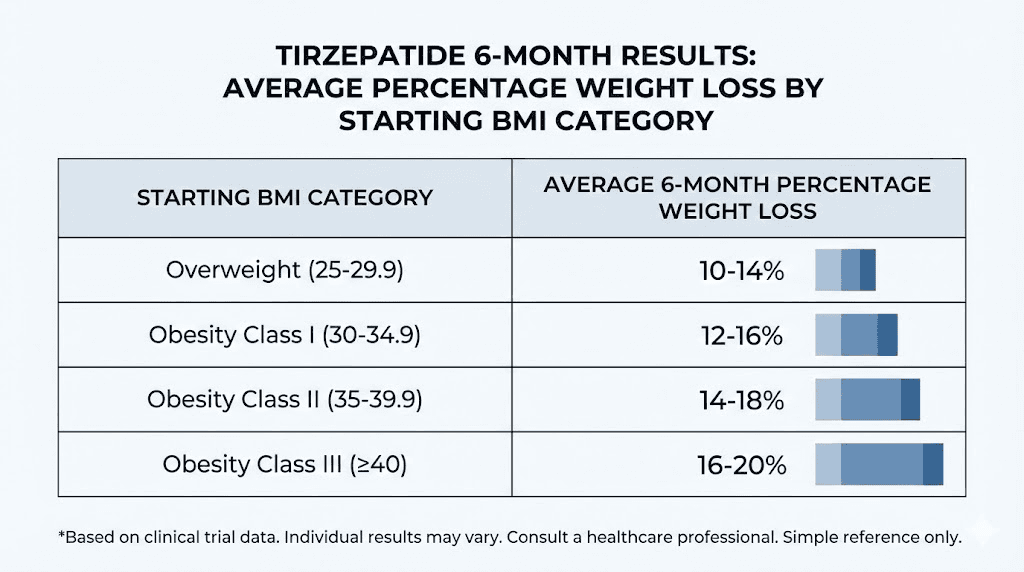
Research examining time to weight plateau found that median time varies by baseline BMI and demographic factors. People with overweight BMI (25-29.9) reached plateau around 24 weeks. Those with class I obesity (BMI 30-34.9) plateaued around 28 weeks. Class II obesity (BMI 35-39.9) reached plateau at approximately 32 weeks. Class III obesity (BMI 40+) continued losing weight until 36 weeks on average.
These timelines reflect population averages from controlled trials. Individual variation remains substantial. Some people plateau much earlier while others continue losing weight well past 40 weeks. Factors influencing plateau timing include dose level, adherence consistency, dietary quality, exercise habits, sleep patterns, stress levels, and underlying metabolic health.
Higher doses of tirzepatide consistently predicted later plateau and greater total weight loss. Female sex associated with later plateau compared to males. White race correlated with later plateau while Asian race predicted earlier stabilization. The physiological mechanisms behind these demographic differences remain unclear but likely involve variations in receptor expression, metabolic rate, and hormonal responses.
Average 12-month weight loss across dose levels
The SURMOUNT-1 trial provides the gold standard data for 72-week outcomes. Participants on 5mg tirzepatide lost an average of 16% of body weight. Those on 10mg lost 21%. The 15mg group achieved 23% reduction. For someone starting at 220 pounds, these percentages translate to 35, 46, and 51 pounds respectively.
Real-world outcomes compiled from medical weight loss clinics show similar patterns with slightly wider ranges. Strong responders on 15mg sometimes achieve 25-30% weight reduction, losing 60-75 pounds or more. Moderate responders typically land in the 18-22% range. Late responders or those with metabolic complications might achieve 12-15% reduction, still clinically meaningful but below trial averages.
The distribution of outcomes follows a predictable curve. Roughly 15-20% of people achieve exceptional results exceeding 25% weight loss. About 60-70% cluster around trial averages of 18-23% reduction. Another 10-15% fall below 15% loss despite consistent protocol adherence. Understanding where you fall on this distribution curve helps set appropriate expectations and determine whether protocol adjustments might improve outcomes.
Twelve month before and after transformations
One-year transformation photos document dramatic changes that fundamentally alter appearance. Face photos show complete restructuring of facial contours with prominent cheekbones, defined jawlines, and elimination of double chins. Body photos reveal transformations that friends describe as unrecognizable compared to baseline. Clothing sizes change by 4-6 sizes or more for many people.
The psychological and social impact of 12-month transformations extends far beyond physical appearance. Confidence improves. Social anxiety decreases. Career opportunities sometimes expand as appearance-based discrimination (conscious or unconscious) reduces. Relationship dynamics shift. Physical intimacy improves for many couples. These secondary effects motivate continued maintenance even after active weight loss phases end.
Body composition at 12 months separates people who incorporated strength training from those who relied on diet alone. Researchers who lifted weights throughout treatment maintain significantly more muscle mass, creating more aesthetic proportions and better metabolic health. Those who focused solely on calorie restriction often appear thin but lack muscle definition, sometimes described as skinny fat despite substantial weight loss.
Men vs women: how before and after results differ
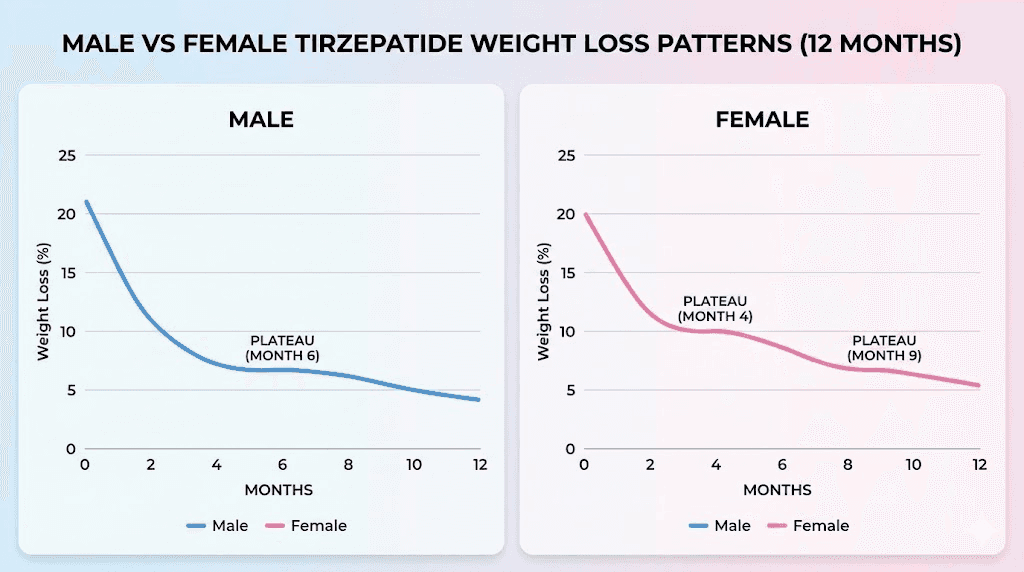
Sex-based differences in tirzepatide response emerge consistently across clinical trials and real-world data. Women typically achieve slightly higher percentage weight loss than men, plateau later in treatment, and experience different patterns of fat distribution changes. Men lose weight faster in absolute terms early in treatment but show more variable long-term maintenance.
Male response patterns and typical transformations
Men tend to lose weight more rapidly during the first 3-4 months of tirzepatide treatment compared to women starting at similar BMI levels. This early advantage stems from higher baseline metabolic rates, greater muscle mass, and hormonal factors that facilitate fat mobilization. However, male weight loss often plateaus earlier than female loss, typically around weeks 28-32 versus weeks 32-36 for women.
Male before and after photos show distinctive patterns. Abdominal fat reduction happens dramatically for most men, with waist circumferences dropping 6-8 inches or more by month 6. Face transformations reveal jawline definition and elimination of neck fat. Chest and shoulder areas slim down substantially. Men who incorporate resistance training protocols often achieve impressive muscle definition as overlying fat disappears.
Testosterone levels sometimes improve as weight decreases in men, particularly those starting with obesity-related hypogonadism. This hormonal shift creates a positive feedback loop where weight loss improves testosterone, which then facilitates better body composition changes and maintenance. Men with persistently low testosterone despite weight loss might benefit from investigating peptide combinations or conventional hormone replacement.
Female response patterns and body composition changes
Women achieve slightly higher percentage weight loss than men on average, though absolute pound reduction often appears lower due to smaller starting weights. Female plateau timing occurs later, allowing for more extended weight loss phases. Women also show more consistent maintenance once plateau occurs, with fewer dramatic rebounds in the 6-12 months following treatment.
Female fat distribution changes follow different patterns than male loss. Waist and hip reductions happen more gradually but ultimately achieve similar percentage decreases. Breast tissue changes vary widely, with some women experiencing substantial size reduction while others maintain most breast volume. Thigh and arm fat decreases substantially for most women by month 6-12.
Hormonal fluctuations influence female tirzepatide response more than male outcomes. Women in perimenopause or menopause sometimes experience slower progress due to declining estrogen levels and metabolic shifts. Menstrual cycle phase affects appetite and water retention, creating weekly fluctuations that make progress tracking more challenging. Consistent weekly dosing helps smooth out these variations.
Age-related differences in outcomes
Younger adults (18-40) typically achieve faster weight loss and greater total reductions compared to older adults (60+), though older individuals still achieve clinically meaningful results. The age-related difference stems from declining metabolic rate, reduced muscle mass, hormonal changes, and accumulated metabolic damage from years of obesity.
Before and after transformations in younger adults often appear more dramatic due to better skin elasticity and faster tissue remodeling. Skin tightens more effectively in 20-40 year olds compared to people over 50. Younger researchers also tend to incorporate exercise more consistently, improving body composition outcomes. Older adults benefit tremendously from tirzepatide but might need additional interventions to address loose skin or optimize body composition.
Factors that predict exceptional vs average results
The difference between someone who loses 20% body weight and someone who loses 35% often comes down to modifiable factors rather than genetics or luck. Research examining predictors of exceptional outcomes identifies specific behaviors, characteristics, and protocol details that separate strong responders from average ones.
Baseline characteristics that influence response
Starting BMI shows complex relationships with outcomes. Higher baseline BMI predicts greater absolute weight loss but similar percentage reductions. Someone starting at BMI 45 might lose 80 pounds (reaching 30% reduction) while someone at BMI 32 loses 40 pounds (achieving 25% reduction). Both represent excellent responses despite different absolute numbers.
Metabolic health at baseline significantly influences tirzepatide response. People with preserved insulin sensitivity tend to respond better than those with severe insulin resistance or long-standing type 2 diabetes. Individuals without metabolic syndrome typically achieve 2-4 percentage points higher weight loss than those meeting multiple metabolic syndrome criteria. These differences persist even when controlling for starting weight and demographics.
Previous weight loss attempts influence outcomes in counterintuitive ways. People who failed multiple diets before tirzepatide sometimes achieve better results than diet-naive individuals, possibly because they bring accumulated knowledge about nutrition and behavior change. However, those with extreme yo-yo dieting histories occasionally show blunted responses due to metabolic adaptations from repeated weight cycling.
Behavioral factors determining success
Adherence to weekly dosing represents the single strongest predictor of successful outcomes. Missing even one dose monthly reduces total weight loss by 2-3 percentage points over 6-12 months. People who maintain perfect adherence for 12 months lose significantly more weight than those who miss 10-15% of doses, even when controlling for all other variables.
Dietary quality matters as much as caloric deficit for many people. Researchers who consume high-protein diets (1.2-1.6g per kg body weight) preserve significantly more muscle mass during weight loss compared to those eating lower protein intakes. This preservation improves body composition outcomes and facilitates better long-term maintenance by protecting metabolic rate.
Exercise consistency separates exceptional transformations from average ones. People who engage in 150+ minutes weekly of moderate cardiovascular activity combined with 2-3 resistance training sessions achieve 4-6 percentage points greater weight loss than sedentary individuals. The exercise advantage compounds over time, with differences becoming most apparent in months 6-12 when purely diet-driven weight loss often plateaus.
Protocol optimization strategies
Dose escalation timing influences outcomes significantly. Aggressive escalation (increasing dose every 2-3 weeks) sometimes produces faster early results but often leads to side effects that interrupt adherence. Conservative escalation (monthly increases) generates slower initial progress but better long-term consistency and ultimately superior total weight loss for many people.
Managing side effects proactively separates people who complete 12 months of treatment from those who discontinue early. Using anti-nausea strategies, adjusting meal timing and composition, staying hydrated, and addressing constipation helps maintain protocol adherence through difficult phases. People who power through severe side effects without intervention typically abandon treatment within 3-4 months.
Tracking and monitoring habits correlate strongly with exceptional outcomes. Researchers who weigh themselves weekly, track food intake at least sporadically, and monitor non-scale victories (measurements, photos, energy levels) lose more weight than those who avoid tracking entirely. The self-monitoring provides real-time feedback that enables rapid course correction when progress stalls.
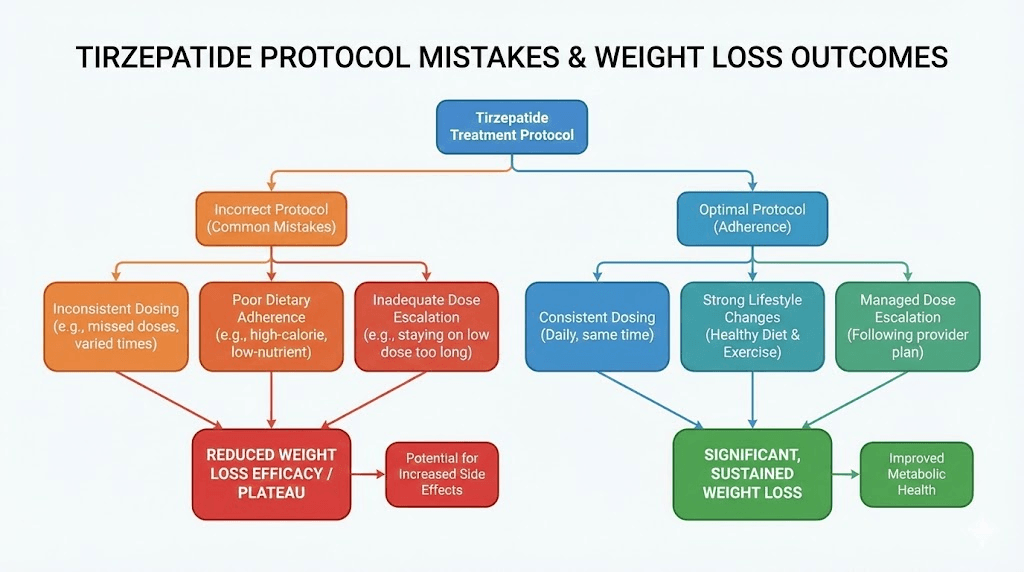
What derails progress: common pitfalls in before and after stories
Dramatic before and after transformations grab attention, but many tirzepatide users achieve modest results or abandon treatment early. Understanding common failure modes helps avoid preventable mistakes that limit outcomes.
Dose escalation mistakes
Escalating too quickly represents one of the most common errors. People who jump from 2.5mg directly to 7.5mg or higher often experience severe nausea, vomiting, and gastrointestinal distress that forces treatment discontinuation. The recommended titration schedule exists for good reasons. Rushing past these guidelines rarely produces better outcomes and frequently causes problems.
Conversely, escalating too slowly limits results for some people. Staying on 2.5mg for 3-4 months when side effects remain minimal wastes time at suboptimal doses. Most protocols recommend monthly increases until reaching 10-15mg or until side effects necessitate holding at current dose. People who remain overly cautious about escalation sometimes plateau early and miss potential for greater weight loss.
Nutritional mistakes that limit results
Relying entirely on appetite suppression without conscious nutritional planning leads to suboptimal outcomes for many people. While tirzepatide dramatically reduces hunger, some researchers still consume calorie-dense low-nutrient foods when they do eat. Choosing processed snacks, fast food, and sugary beverages wastes limited caloric intake on foods that provide little satiety or nutrition.
Protein intake falls too low for many tirzepatide users. When appetite drops and meal frequency decreases, total protein consumption sometimes plummets to 40-60g daily for people who need 100-120g to preserve muscle mass. This deficit accelerates muscle loss during weight reduction, creating unfavorable body composition changes and reducing metabolic rate. Prioritizing protein-rich foods at each meal helps prevent this outcome.
Exercise avoidance and sedentary patterns
Many people assume that tirzepatide alone provides optimal results without exercise. While weight loss certainly occurs through diet alone, body composition outcomes suffer dramatically. People who remain sedentary lose substantial muscle mass alongside fat, often reducing metabolic rate by 200-300 calories daily by month 12. This metabolic suppression makes maintenance significantly harder once active weight loss ends.
Inadequate resistance training represents a specific subset of this problem. Cardiovascular exercise helps caloric deficits but does little to preserve muscle mass during weight loss. People who walk daily but never lift weights often achieve disappointing body composition outcomes despite significant scale weight reduction. Incorporating strength training protocols 2-3 times weekly preserves muscle and improves transformation quality.
Inconsistent dosing and treatment gaps
Missing doses destroys consistency and limits results. Every missed weekly injection represents 14% of monthly treatment absent. People who miss one dose monthly effectively reduce their annual dose by 12%, translating to 2-4 percentage points less total weight loss. Treatment gaps of 2-3 weeks during vacations or periods of disorganization can erase a month of progress.
Stopping treatment prematurely prevents achieving maximum potential results. Some people discontinue at month 6 after losing 30-40 pounds despite being on track to lose 60+ pounds by month 12. Early discontinuation often stems from unrealistic timelines, frustration during temporary plateaus, or side effects that could be managed with protocol adjustments.
Maintaining results after reaching goal weight
The transition from active weight loss to maintenance represents a critical juncture where many people regain significant weight. Understanding maintenance strategies helps preserve transformation results long-term.
Continuing vs stopping tirzepatide
Research examining weight maintenance after tirzepatide discontinuation shows substantial regain for most people who stop treatment. The SURMOUNT-4 trial found that participants who stopped tirzepatide after achieving significant weight loss regained approximately two-thirds of lost weight within 12 months. Those who continued treatment maintained 95% of their weight loss over the same period.
These findings suggest that tirzepatide works best as a long-term intervention rather than a temporary tool. Obesity represents a chronic condition with strong biological drivers that persist after weight loss. Stopping the medication removes the pharmacological support that helped achieve the transformation, leaving individuals fighting against increased appetite, reduced metabolic rate, and hormonal changes that promote weight regain.
Some people successfully maintain weight loss after stopping tirzepatide by transitioning to intensive behavioral interventions. The SURMOUNT trials showed that participants who engaged in structured lifestyle programs maintained better results than those who simply stopped medication without support. However, even intensive behavioral interventions rarely match the weight maintenance achieved by continuing medication at lower doses.
Dose reduction strategies for maintenance
Many clinicians recommend reducing tirzepatide dose by 25-50% once goal weight is achieved. Someone who lost weight on 15mg weekly might transition to 7.5-10mg for maintenance. This strategy reduces medication costs and side effects while providing sufficient appetite suppression and metabolic support to prevent regain.
The optimal maintenance dose varies individually. Some people maintain perfectly on 5mg weekly while others need 10-12.5mg to prevent regain. Monitoring weight weekly and adjusting dose based on trends helps find the minimum effective maintenance dose. Small regains of 2-3 pounds signal need for dose increases before larger regains develop.
Behavioral strategies that support maintenance
Successful weight maintenance requires continued attention to the behaviors that supported initial weight loss. Weekly weighing helps catch small regains before they become large ones. People who weigh themselves weekly catch upward trends at 2-3 pounds and course correct immediately. Those who avoid the scale sometimes regain 10-20 pounds before recognizing the problem.
Sustained dietary consciousness remains important even with continued tirzepatide. The medication suppresses appetite but does not eliminate the possibility of overeating calorie-dense foods. Maintaining protein intake at 1-1.2g per kg body weight helps preserve muscle mass. Limiting ultra-processed foods keeps overall calorie intake reasonable despite reduced hunger signals.
Exercise becomes even more critical during maintenance than during active weight loss. Regular physical activity (150+ minutes weekly of cardio plus 2-3 resistance sessions) helps maintain metabolic rate, preserves muscle mass, improves insulin sensitivity, and provides psychological benefits that support long-term adherence. People who exercise consistently during maintenance maintain better results than those who become sedentary after reaching goals.
Realistic expectations: what before and after photos do not show
Transformation photos dominate social media and marketing materials, but they hide important information about the tirzepatide journey. Understanding what before and after images do not reveal helps set appropriate expectations.
The timeline behind dramatic transformations
Most impressive before and after photos represent 12-18 months of consistent effort, not the 3-4 months that headlines sometimes imply. Marketing materials occasionally show 6-month results but cherry-pick exceptional responders whose outcomes exceed population averages. Typical results take longer and involve more effort than photos suggest.
The before photo often represents someone at their heaviest weight after months or years of progressive gain. The after photo captures them at their lowest weight, possibly after additional effort beyond tirzepatide alone. These photos represent two extreme points on a weight trajectory rather than a simple cause-and-effect relationship between medication and outcome.
Side effects and challenges during treatment
Dramatic transformations omit the nausea, vomiting, constipation, fatigue, and other side effects many people experience during treatment. The perfect after photo does not show the weeks spent managing gastrointestinal distress or the adjustments needed to find tolerable protocols. Most people experience some side effects, particularly during dose escalations.
Plateaus and stalls happen for almost everyone during weight loss. Before and after photos show beginning and end points but hide the 3-4 week periods where weight barely moves despite perfect adherence. These plateaus frustrate and demoralize but represent normal physiology rather than protocol failure. Understanding that plateaus happen to everyone helps maintain motivation during challenging phases.
Body composition realities
Transformation photos sometimes hide loose skin, which develops in people who lose large amounts of weight rapidly. The extent of loose skin depends on age, genetics, starting weight, rate of loss, and skin quality. Younger people with good skin elasticity often experience complete skin retraction. Older individuals or those losing 100+ pounds frequently develop some degree of loose skin requiring surgical intervention for optimal cosmetic outcomes.
Muscle loss accompanies fat loss for almost everyone, though the ratio varies dramatically based on protein intake and exercise habits. Before and after photos rarely disclose that someone lost 50 pounds of fat but also 10-15 pounds of muscle, creating a final result that looks thin but lacks definition. Prioritizing muscle preservation strategies throughout weight loss produces more aesthetically pleasing transformations.
The role of additional interventions
Many dramatic before and after photos omit that the person also worked with personal trainers, nutritionists, and other professionals alongside using tirzepatide. The medication provided critical appetite suppression and metabolic support, but the transformation also involved professional exercise programming, meal planning, psychological coaching, and sustained effort across multiple domains.
Some transformation photos involve additional peptides or interventions beyond tirzepatide alone. People sometimes stack peptides or use additional medications to optimize results. Others undergo cosmetic procedures after weight loss to address loose skin or body contours. These additional interventions contribute to final outcomes but rarely receive disclosure in before and after marketing.
Comparing your results to averages and clinical data
Understanding how your outcomes compare to clinical trial data and real-world averages helps determine whether your response falls within expected ranges or signals need for protocol adjustments.
Clinical trial benchmarks by timeframe
The SURMOUNT trials provide gold standard benchmarks for expected outcomes. At 12 weeks on 5mg, average weight loss was 6-8% of body weight. At 24 weeks on 10mg, average loss reached 15-17%. By 72 weeks on 15mg, participants lost 20-23% on average. These represent mean outcomes with substantial individual variation above and below averages.
Your results should roughly track with clinical trial timelines adjusted for dose differences. If you are on 10mg at month 6 but have only lost 8% of body weight, you are underperforming trial averages by roughly half. This gap signals need to investigate potential barriers like inconsistent dosing, inadequate caloric deficit, medication interactions, or metabolic factors limiting response.
Exceeding clinical trial averages by 20-30% represents excellent response but not necessarily cause for concern. If you lose 25% by month 9 while trial averages show 18% at that timeframe, you are simply a strong responder. Exceptional results become concerning only if accompanied by excessive side effects, dangerous behaviors like severe caloric restriction, or signs of disordered eating.
When to investigate poor response
Losing less than 5% body weight by week 12 despite consistent dosing and reasonable dietary adherence signals need for evaluation. Poor early response predicts lower total weight loss even if treatment continues. Potential causes include medication interactions (particularly with diabetes medications), thyroid dysfunction, severe insulin resistance, genetic factors affecting GLP-1 receptor function, or gastrointestinal issues preventing medication absorption.
Working with SeekPeptides helps identify and address factors limiting response. Comprehensive evaluation might reveal addressable issues like inadequate dose escalation, suboptimal injection technique, medication storage problems affecting potency, or dietary patterns sabotaging caloric deficits. Sometimes simple protocol adjustments dramatically improve outcomes.
Individual variation in response patterns
Even with perfect adherence and protocol optimization, some people respond better than others due to factors beyond conscious control. Genetic variations in GIP and GLP-1 receptor function influence how strongly individuals respond to tirzepatide. Differences in gut microbiome composition affect medication absorption and metabolic effects. Variations in baseline hormone levels, insulin sensitivity, and metabolic rate all contribute to individual response differences.
Recognizing that 10-15% of people will remain low responders despite optimal protocols helps set realistic expectations. A low responder achieving 12-15% weight loss over 12 months has succeeded in medical terms even if outcomes fall below population averages or personal hopes. This level of loss provides substantial health benefits including improved glucose control, reduced cardiovascular risk, and better quality of life.
Frequently asked questions
How much weight do most people lose on tirzepatide in 6 months?
Clinical trials show average weight loss of 15-17% of body weight at 6 months on 10mg weekly doses. For someone starting at 200 pounds, this translates to approximately 30-34 pounds. Individual results vary widely, with some people losing 40-50 pounds and others achieving 20-25 pounds by this timeframe. Starting dose level, adherence consistency, dietary habits, and exercise engagement all influence six-month outcomes.
When do before and after changes become visible to others?
Most people notice changes in their own appearance by weeks 6-8, but friends and family typically comment unprompted around months 3-4. By month 6, nearly everyone notices dramatic differences assuming weight loss reaches 25-40 pounds or more. Face changes become visible earlier than body changes for most people, with jawline definition and reduced facial puffiness appearing by month 2-3.
Can you achieve better results than clinical trial averages?
Yes. Clinical trials represent average outcomes across diverse populations. Strong responders routinely exceed trial averages by 20-40%, losing 25-30% of body weight versus trial averages of 18-23%. Factors that predict superior outcomes include aggressive dose escalation, high protein intake, consistent resistance training, perfect medication adherence, and younger age. Working with SeekPeptides helps optimize protocols for maximum results.
What percentage of people achieve dramatic transformations?
Research suggests that 15-20% of tirzepatide users achieve exceptional results exceeding 25% body weight reduction, creating dramatic before and after transformations. Another 60-70% achieve solid results in the 15-23% range. The remaining 10-20% experience modest outcomes below 15% loss. Predicting which category you will fall into remains difficult before starting treatment, though baseline metabolic health and behavioral factors influence outcomes significantly.
How long does it take to reach maximum weight loss?
Most people reach their weight loss plateau between months 9-14, with timing varying by starting BMI. Those starting with BMI 25-30 plateau around 24-28 weeks. Class II-III obesity typically plateaus around 32-40 weeks. Plateau timing correlates with maximum dose reached and represents the transition from active weight loss to maintenance. Continuing treatment after plateau helps maintain results rather than promoting additional loss.
Do men and women show different before and after results?
Yes. Women typically achieve slightly higher percentage weight loss than men and plateau later in treatment. Men lose weight faster initially but often plateau earlier. Female response patterns show more consistent maintenance while male outcomes vary more widely. Sex-based differences in body composition, hormones, and metabolism all contribute to these patterns.
What happens to results if you stop tirzepatide?
Research shows that people who discontinue tirzepatide typically regain approximately two-thirds of lost weight within 12 months. The SURMOUNT-4 trial demonstrated that continuing treatment maintains 95% of weight loss while stopping leads to substantial regain for most individuals. Some people maintain better results through intensive behavioral interventions, but continuing medication at reduced doses provides the most reliable maintenance strategy.
How do tirzepatide transformations compare to other weight loss methods?
Tirzepatide produces weight loss roughly 2-3x greater than diet and exercise alone, comparable to bariatric surgery outcomes for many people. Compared to semaglutide, tirzepatide generates 15-25% greater weight loss on average. Behavioral interventions alone rarely achieve more than 5-10% sustained weight loss, while tirzepatide consistently produces 15-23% reduction in clinical trials. Only bariatric surgery reliably exceeds tirzepatide outcomes.
External resources
New England Journal of Medicine - Triple Hormone Receptor Agonist Retatrutide Trial
NIH - Weight Reduction Over Time in Tirzepatide-Treated Participants
NIH - Time to Weight Plateau with Tirzepatide Treatment
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, detailed before and after case studies with protocol breakdowns, and a community of thousands who have navigated these exact questions about achieving and maintaining dramatic transformations.
In case I do not see you, good afternoon, good evening, and good night. May your transformations stay sustainable, your protocols stay optimized, and your results stay maintained.