Feb 8, 2026

Day 1 looks the same as every other day. The scale reads the same number. The mirror shows the same body. But something has shifted, something invisible and biochemical, and it will change everything over the next 72 weeks.
Men respond to tirzepatide differently than women. Not dramatically differently, but the nuances matter. Visceral fat patterns differ. Testosterone dynamics shift as fat disappears. Muscle preservation concerns hit harder when you have spent years building a physique you do not want to lose. And the psychological relationship men have with the scale, with hunger, with food as fuel rather than comfort, creates a distinct experience that generic before-and-after stories rarely capture.
This guide exists because of that gap.
We dug into the SURMOUNT-1 trial data, the SURPASS-3 MRI analysis, real-world outcomes from men tracking their progress, and the emerging research on peptides for men to build the most comprehensive picture of what tirzepatide actually does to a male body over time. Not the marketing version. Not the cherry-picked transformation photos. The full, honest, sometimes messy reality of what happens when men start tirzepatide, what the timeline looks like week by week, and how to optimize every phase of the process for the best possible outcome.
SeekPeptides members have been tracking these patterns across thousands of documented protocols, and the data tells a story that is both more nuanced and more encouraging than most sources suggest.
How tirzepatide works differently in men
Tirzepatide is a dual GIP and GLP-1 receptor agonist. That dual mechanism matters. It does not just suppress appetite through one pathway. It hits two, creating a synergistic effect that produces greater weight reduction than either pathway alone.
For men specifically, several factors make this mechanism particularly relevant.
Men carry more visceral fat than women on average. This is the deep abdominal fat that wraps around organs, drives insulin resistance, and correlates strongly with cardiovascular risk. The SURMOUNT-1 trial found that visceral fat mass decreased by 40.1% with tirzepatide compared to just 7.3% with placebo. That is not a marginal improvement. That is a fundamentally different metabolic landscape.
Waist circumference, the most visible marker of male fat distribution, dropped by an average of 18.1 cm in the tirzepatide group. For context, that represents roughly 7 inches off the waistline. Men who started with a 42-inch waist could expect to approach 35 inches. The belt notches tell a story the scale sometimes misses.
But here is where men face a unique challenge. The same visceral fat that drives metabolic disease also converts testosterone to estrogen through an enzyme called aromatase. As that fat disappears, the hormonal environment shifts. And for men, that shift can be profoundly positive.
The testosterone connection
A controlled pilot study on tirzepatide and metabolic hypogonadism found something remarkable. As men lost fat, their testosterone levels climbed. Not by trivial amounts. Research shows substantial weight reduction in obese men can increase endogenous testosterone by approximately 84 to 130 ng/dL.
Think about what that means practically.
A man with obesity-related low testosterone, perhaps sitting at 250 ng/dL with symptoms of fatigue, low libido, and poor recovery, could see his levels rise to 350 to 380 ng/dL simply from the fat loss that tirzepatide produces. Some men reported improvements in erectile function and sexual health alongside the weight loss, which tracks with the hormonal improvements.
This does not mean tirzepatide is a testosterone therapy. It means the fat loss it produces removes a hormonal roadblock that many men do not even realize exists. The excess adipose tissue was actively suppressing their natural hormonal function, and removing it allows the body to recalibrate.
For men already on TRT, the dynamic changes again. Dose adjustments may become necessary as body composition shifts. The estrogen conversion ratio changes. The entire hormonal picture requires monitoring and potential recalibration, which is why working with a knowledgeable provider matters.
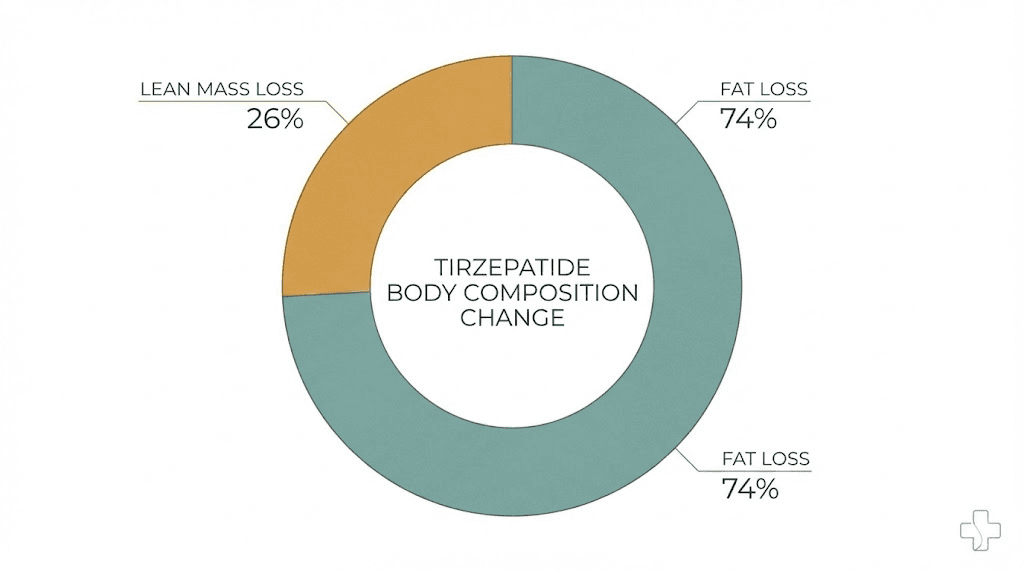
Body composition: fat loss versus muscle loss
This is the question that keeps men awake at night. Will tirzepatide eat my muscle?
The data is more reassuring than the fear suggests. In the SURMOUNT-1 body composition analysis, the proportion of weight lost was 74% fat mass and 26% lean mass in the tirzepatide group. The placebo group showed nearly identical proportions at 75% fat and 25% lean. This means tirzepatide does not preferentially target muscle. The ratio of fat to lean loss stays consistent regardless of whether you are on the medication or losing weight through diet alone.
A systematic review of tirzepatide and skeletal muscle mass concluded that the medication induces significant fat mass loss while preserving a relatively stable proportion of lean mass and improving markers of muscle composition. Reductions in fat-free muscle volume were small and within expected ranges based on UK Biobank reference data.
But proportion is not the whole story.
When total weight loss is 21%, even 26% of that coming from lean mass represents meaningful absolute numbers. A 250-pound man losing 52 pounds would lose approximately 13.5 pounds of lean mass. That is noticeable. That matters. And that is exactly why the strategies we will cover later in this guide, resistance training, protein optimization, and timing, become critical for male users.
Week-by-week timeline: what men actually experience
The clinical trials give us averages. But averages hide the lived experience. Here is what the timeline typically looks like for men, drawn from trial data, real-world reports, and community feedback from forums and tracking platforms.
Weeks 1 through 4: the adjustment phase (2.5 mg)
The first month is about acclimation, not dramatic results. The starting dose of 2.5 mg is intentionally low. It is designed to let your GI system adapt to a medication that fundamentally changes how your gut communicates with your brain.
Most men notice appetite suppression within the first week. Not the dramatic food-is-repulsive experience some describe. More like a quiet dimming of the hunger signal. You eat lunch and realize at 5 PM that you forgot about your afternoon snack. You serve yourself dinner and leave food on the plate without thinking about it.
Weight loss in month one typically ranges from 3 to 8 pounds for men. Some of this is water weight. Some is genuine fat loss. The scale will bounce around. Do not read meaning into daily fluctuations.
Common side effects during this phase include mild nausea, particularly in the first 48 hours after injection. Some men report fatigue. Others notice changes in bowel habits. These effects are usually manageable and often resolve within 2 to 3 weeks as the body adjusts.
What men rarely talk about but frequently experience: the psychological shift. Food noise, that constant background hum of thinking about your next meal, planning meals, wanting meals, quiets down. For men who have never identified as emotional eaters, this can be startling. You did not realize how much mental bandwidth food occupied until it stopped.
Weeks 5 through 8: the first real changes (5 mg)
The dose increases to 5 mg at week 5, and this is typically where men start seeing changes they can measure. Not just on the scale, in the mirror.
Average cumulative weight loss by week 8 is 8 to 15 pounds. But the distribution of that loss matters more than the number. Men tend to lose visceral fat first, which means the belly starts flattening before the scale shows dramatic numbers. Your pants fit differently. The belt moves a notch. The face starts looking leaner.
This is also when tirzepatide dosing adjustments become relevant. Some men respond strongly to 5 mg and their provider may hold at this dose longer. Others need the full escalation to see optimal results. There is no universal best dose, only the dose that produces consistent 1 to 2 pounds of weekly loss without intolerable side effects.
Energy levels often improve during this phase. As insulin sensitivity improves and blood sugar stabilizes, the afternoon energy crashes that many overweight men experience start disappearing. Gym performance may actually improve despite eating less, because the food you are eating gets utilized more efficiently.
Weeks 9 through 16: the transformation window (7.5 to 10 mg)
This is where before-and-after photos start telling a story. The dose moves to 7.5 mg and potentially 10 mg, and the appetite suppression deepens. Weight loss accelerates for most men.
By week 12, average cumulative loss reaches 15 to 25 pounds. The tirzepatide dose chart shows this is where the dose-response curve steepens. Men on 10 mg lose significantly more than those who stay at 5 mg.
Visible changes become undeniable. Coworkers notice. Family comments. Clothes that were snug now hang. The face, neck, and upper body lean out noticeably. For men carrying significant visceral fat, the transformation in abdominal profile can be dramatic, losing 4 to 6 inches off the waist is common by this point.
Side effects may resurface briefly with each dose increase but typically resolve faster than during initial titration. The body has learned to adapt.
This is also when testosterone improvements become measurable. If blood work was done at baseline showing suppressed testosterone, a recheck at week 12 to 16 often reveals meaningful improvement. Not always dramatic, but the trend is upward, and men report subjective improvements in energy, mood, and libido that correlate with these hormonal shifts.
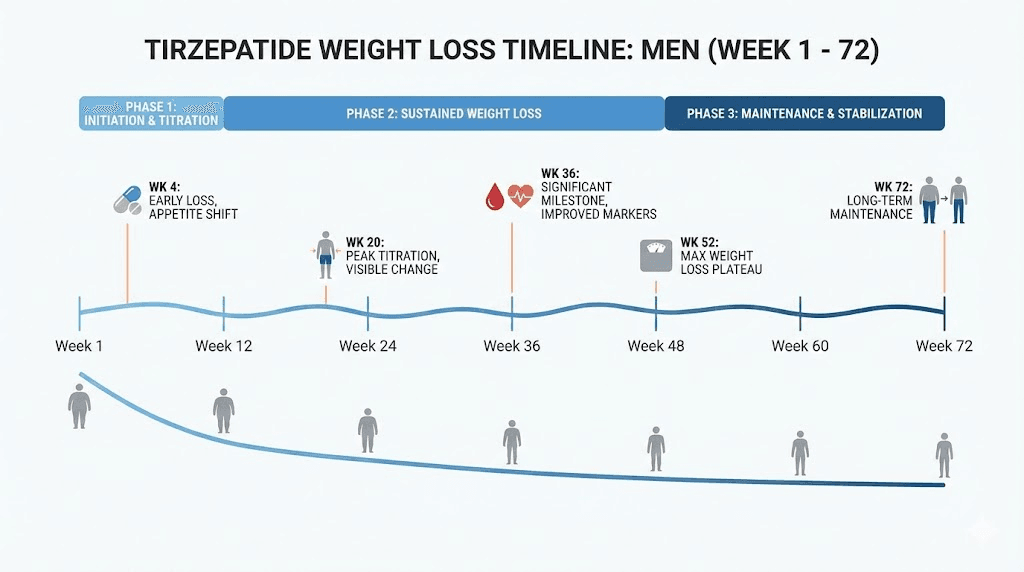
Weeks 17 through 36: the steady grind (10 to 15 mg)
The honeymoon phase ends somewhere around month 4 to 5. Weight loss continues, but the pace often slows. This is normal. It is not a plateau in the true sense. The body is simply recalibrating to a new metabolic baseline.
Men who started at higher body weights continue losing at impressive rates. A man who started at 280 pounds might be approaching 230 by week 24. That is 50 pounds in six months. But the weekly rate has slowed from 2 to 3 pounds to 1 to 1.5 pounds. The math still works. The psychology gets harder.
This phase tests commitment. The dramatic early changes that motivated adherence give way to slow, grinding progress that requires patience. The not losing weight panic sets in for some men, even when they are still losing, just more slowly.
Body recomposition becomes more visible here. Even as the scale stalls occasionally, the mirror keeps changing. Muscle definition emerges. Shoulders look broader relative to a shrinking waist. The V-taper that many men want starts appearing, not because muscle is growing, but because the fat hiding it is disappearing.
For men maintaining a strength training protocol, this phase often brings surprising gym performance. Relative strength, how much you can lift per pound of body weight, typically increases. Movements feel easier because there is less body weight to move. Pull-ups get easier. Running becomes less punishing. The functional benefits of weight loss compound.
Weeks 37 through 72: the long game
Clinical trial data from SURMOUNT-1 shows the full picture at 72 weeks. The average total body weight reduction with tirzepatide was 21.3%. For the 15 mg dose group specifically, that number climbed to approximately 22.5%.
Put that in real terms for men at various starting weights.
A 220-pound man reaches approximately 173 pounds. A 260-pound man approaches 205. A 300-pound man could see 236 on the scale. These are transformative numbers. Not incremental. Life-changing.
At this stage, the before-and-after comparison becomes staggering. Men who commit to the full 72-week protocol, combined with lifestyle modifications, often look like different people. Not just thinner. Younger. More vital. The combination of fat loss, improved posture from carrying less weight, better skin quality from improved metabolic health, and increased confidence creates a compound transformation that goes beyond what the scale measures.
The research also shows that late responders, men who lost weight more slowly in the first 12 weeks, still achieved remarkable results by week 72. Ninety percent of late responders achieved at least 5% body weight reduction, and the majority went well beyond that threshold. The message is clear: consistency matters more than speed.
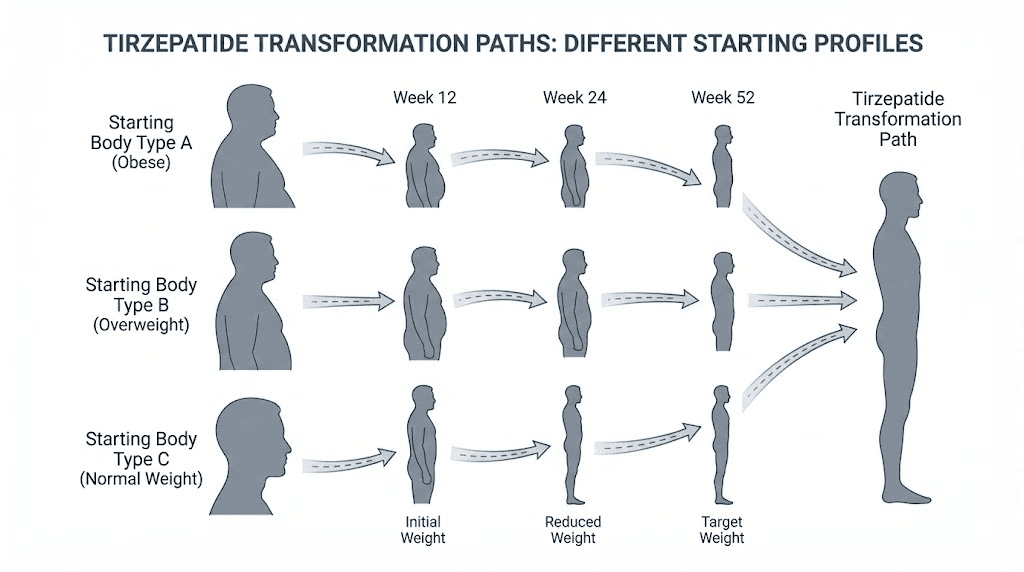
Real-world male transformation patterns
Clinical trials tell one story. Real life tells another. Here is what patterns emerge when you look at men actually using tirzepatide outside of controlled study environments.
The athletic man carrying 30 to 50 extra pounds
This is the man who works out regularly but cannot lose the spare tire. He knows his way around a gym. His diet is not terrible. But years of stress eating, business dinners, and a slowing metabolism have added visceral fat that exercise alone cannot seem to budge.
For this profile, tirzepatide results tend to be particularly striking. The fat burning targets the visceral stores that were most resistant to traditional methods. Because these men already have muscle mass underneath the fat, the reveal is dramatic. By month 3 to 4, they often look like they have been training twice as hard, when in reality the medication simply removed the layer that was hiding years of consistent gym work.
Weight loss: typically 15 to 20% of starting weight. Body composition shift: dramatic improvement in waist-to-hip ratio. Subjective experience: these men often describe it as finally seeing the body they knew was under there.
The significantly overweight man (BMI 35 plus)
For men with BMI above 35, the transformation follows a different arc. Early weight loss is faster in absolute terms because there is more to lose. A man starting at 320 pounds might drop 30 pounds in the first 3 months. The percentage is similar to lighter men, but the raw numbers are more dramatic.
The health markers often improve before the aesthetic changes become obvious. Blood pressure drops. Fasting glucose normalizes. Sleep apnea symptoms reduce or resolve. Joint pain decreases. These invisible transformations often mean more to quality of life than the visible ones.
The challenge for this group is duration. Reaching goal weight may require 18 to 24 months or longer. The before-and-after at 72 weeks is impressive but may still show significant remaining weight to lose. Setting intermediate milestones, every 25 pounds, every pants size, every health marker improvement, prevents the discouragement that comes from only measuring against a distant final goal.
The middle-aged man with metabolic syndrome
Men in their 40s and 50s with the classic pattern of elevated blood sugar, high triglycerides, low HDL cholesterol, high blood pressure, and central obesity represent a significant portion of tirzepatide users. For these men, before and after is not just about appearance. It is about reversing a cascade of metabolic dysfunction that was heading toward serious health consequences.
The SURMOUNT trials included men with these profiles, and the results were consistent. Weight loss in the 15 to 22% range. Improvements in all metabolic markers. And critically, the body composition changes showed that the fat loss was preferentially coming from the most dangerous depots, the visceral fat around organs that drives metabolic syndrome.
These men often report the most dramatic quality-of-life improvements. Not because the scale shows the biggest numbers, but because the metabolic improvements cascade into energy levels, sleep quality, sexual function, and mental clarity. The before-and-after for this group is measured in blood panels as much as photographs.
The muscle preservation protocol for men on tirzepatide
Losing fat is the goal. Losing muscle is the tax. For men, minimizing that tax is not optional, it is the difference between looking lean and looking depleted.
Here is the evidence-based approach to preserving as much muscle as possible while maximizing fat loss on tirzepatide.
Protein: the non-negotiable foundation
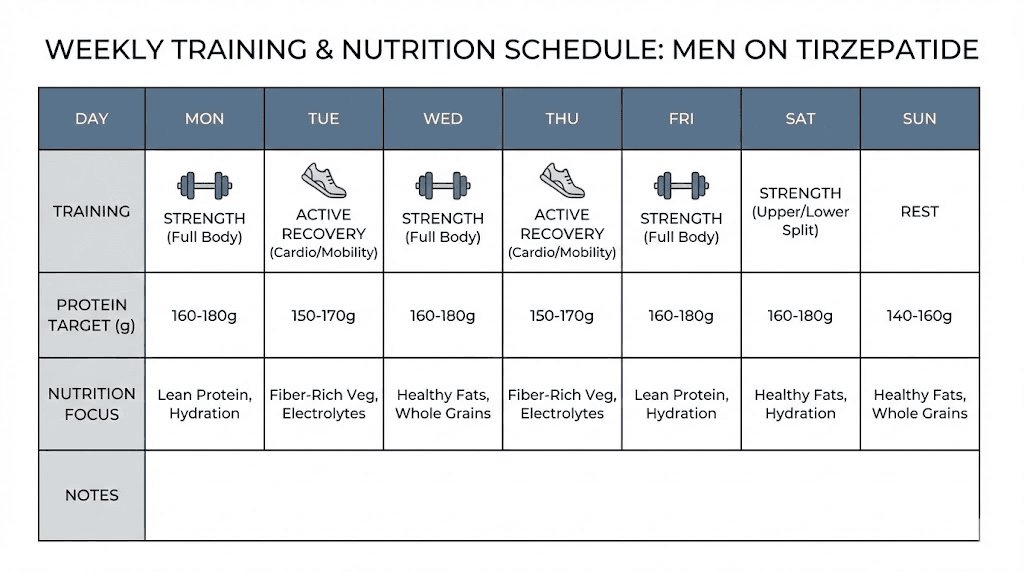
Research on weight loss and muscle preservation consistently points to protein intake as the single most important variable. During caloric restriction, protein requirements increase, not decrease. The current evidence supports 1.6 to 2.2 grams of protein per kilogram of body weight daily for men trying to preserve muscle during weight loss.
For a 220-pound man (100 kg), that means 160 to 220 grams of protein per day.
Here is the problem. Tirzepatide suppresses appetite. Eating 200 grams of protein when you are not hungry is genuinely difficult. This is where strategy matters.
Prioritize protein at every meal. Eat protein first before any other macronutrient. If your total food intake has dropped to 1,500 calories, 600 to 800 of those calories need to come from protein. That leaves limited room for fats and carbohydrates, which is exactly the right ratio for body recomposition.
Protein timing also matters. Spreading intake across 4 to 6 eating occasions throughout the day maximizes muscle protein synthesis. A 40-gram protein breakfast, 40-gram lunch, 40-gram dinner, and two 20-gram protein snacks hits the target more effectively than two 100-gram meals.
Leucine-rich protein sources, whey protein, eggs, chicken breast, lean beef, fish, provide the strongest muscle protein synthesis signal. Supplemental amino acids can help bridge gaps when whole food intake is limited by appetite suppression.
Resistance training: the muscle-saving insurance policy
If protein is the foundation, resistance training is the frame. Without the mechanical stimulus of progressive overload, the body has no reason to preserve muscle during caloric restriction. With it, you send a clear signal: this tissue is being used, do not break it down for energy.
The research is unambiguous. Resistance training during weight loss with GLP-1 medications significantly reduces lean mass loss compared to medication alone.
A practical resistance training protocol for men on tirzepatide should include three to four sessions per week, each lasting 45 to 60 minutes. Focus on compound movements: squats, deadlifts, bench press, rows, overhead press, pull-ups. These exercises recruit the most muscle mass and provide the strongest preservation signal.
Training volume does not need to be extreme. Two to three sets of 8 to 12 repetitions per exercise, taken close to failure, provides sufficient stimulus. The goal during a caloric deficit is not muscle growth, though some beginners will experience that. The goal is muscle retention. That requires less volume than building but more consistency than most men maintain.
Expect some strength decreases during the initial weight loss phase. This is normal and does not necessarily indicate muscle loss. As your body weight drops, your absolute strength may decrease while your relative strength improves. A man who benched 225 at 250 pounds and now benches 210 at 215 pounds is actually relatively stronger.
The complete male optimization protocol
Combining tirzepatide with the right lifestyle approach creates results that exceed what either component achieves alone. Here is the framework.
Daily nutrition targets:
Protein: 1.6 to 2.2 g/kg body weight (prioritize at every meal)
Total calories: let appetite guide, but aim for minimum 1,200 for men under medical supervision
Hydration: 3 to 4 liters of water daily (GI side effects improve with hydration)
Fiber: 25 to 35 grams daily (supports gut health during GI adjustment)
Weekly training schedule:
3 to 4 resistance training sessions (compound movements, progressive overload)
2 to 3 sessions of moderate cardio (walking, cycling, swimming)
Daily step count target: 8,000 to 10,000 steps
Recovery priorities:
7 to 9 hours of sleep (critical for muscle preservation and hormone optimization)
Stress management (elevated cortisol promotes muscle breakdown)
Rest days between resistance sessions for the same muscle groups
Monitoring schedule:
Weekly: body weight (same time, same conditions)
Bi-weekly: waist circumference, progress photos
Monthly: body composition measurement (DEXA if available)
Quarterly: blood work (metabolic panel, hormones, inflammatory markers)
Tirzepatide dosing: what men need to know
The tirzepatide dosage protocol follows a standardized escalation schedule, but understanding the rationale behind each step helps men make informed decisions with their providers.
The standard escalation timeline
Tirzepatide starts at 2.5 mg once weekly. This is not a therapeutic dose for weight loss. It is an introductory dose designed to acclimate the gastrointestinal system. After a minimum of 4 weeks, the dose increases to 5 mg.
From there, the dose can increase by 2.5 mg every 4 weeks until reaching the target dose. The available doses are 2.5, 5, 7.5, 10, 12.5, and 15 mg. The maximum approved dose is 15 mg weekly.
Most men find their effective maintenance dose between 10 and 15 mg. However, some respond well to lower doses. The microdosing approach has gained traction among men who want appetite suppression without the GI side effects that higher doses can produce.
Clinical trial results at 72 weeks showed dose-dependent results. Men on 5 mg lost approximately 15% of body weight. Those on 10 mg lost 19%. And the 15 mg group achieved approximately 21% reduction. Each 5 mg increase translated to roughly 2 to 3 percentage points of additional weight loss.
Injection technique and timing
Tirzepatide is administered as a subcutaneous injection once weekly. The injection should be given on the same day each week, though the specific day and time can be chosen based on personal preference and lifestyle.
Common injection sites include the abdomen (avoiding a 2-inch radius around the navel), the front of the thigh, and the back of the upper arm. Rotate injection sites with each dose to minimize injection site reactions.
Many men find that injecting in the evening reduces the impact of nausea, as they sleep through the peak GI effects. Others prefer morning injections so they can take advantage of the appetite suppression during waking hours. There is no wrong answer, only personal preference.
For men using compounded tirzepatide, reconstitution becomes a relevant skill. Understanding the unit-to-milligram conversion ensures accurate dosing. Using the peptide calculator at SeekPeptides simplifies this math and reduces the risk of dosing errors.
When to hold versus escalate
Not every man needs to reach 15 mg. The decision to escalate should be based on three factors.
First, is weight loss continuing at the current dose? If you are losing 1 to 2 pounds per week consistently, there may be no reason to increase. Higher doses bring higher side effect potential without guaranteed proportional benefit.
Second, are side effects manageable? If nausea, constipation, or fatigue are significantly impacting quality of life, holding the current dose or even temporarily reducing can allow the body to adapt before moving forward.
Third, what does the overall trajectory look like? A man who has lost 18% of body weight on 10 mg over 40 weeks is on an excellent trajectory. Pushing to 15 mg for an additional 2 to 3 percentage points may not be worth the side effect trade-off for every individual.
The dose chart provides a framework, but individualization matters. Work with a provider who understands that the goal is sustainable fat loss, not maximum dose.
Managing side effects: the male experience
Side effects are the price of admission, and being prepared for them makes the difference between powering through and quitting prematurely.
Gastrointestinal effects
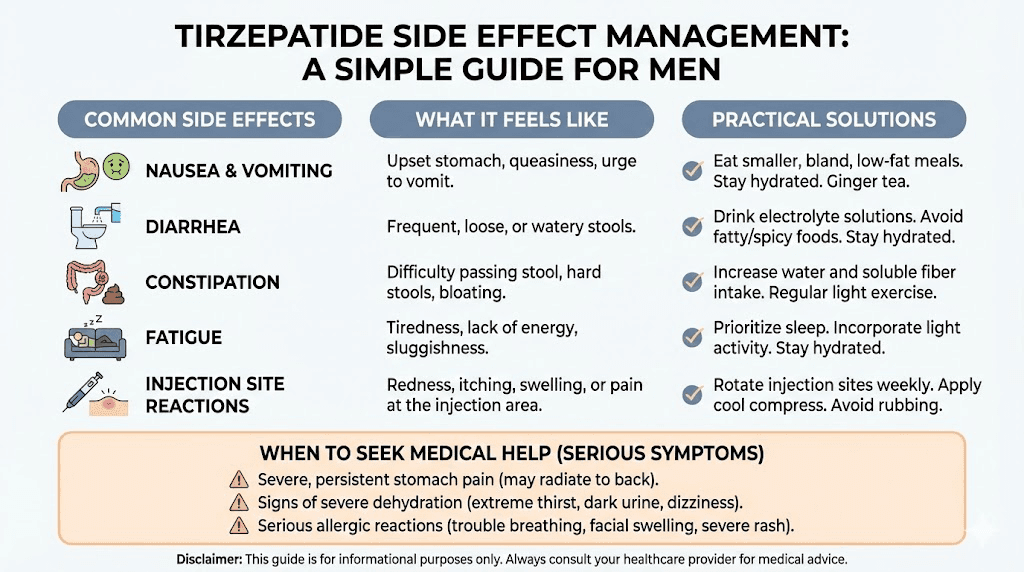
Nausea is the most common side effect, affecting 15 to 33% of users depending on dose. For men, the practical impact often hits hardest at social meals. Business dinners, weekend barbecues, and family gatherings become complicated when your stomach rebels against normal-sized portions.
Strategies that work: eat smaller meals more frequently. Avoid high-fat foods, which slow gastric emptying and worsen nausea. Stay hydrated, dehydration amplifies GI symptoms. Consider timing injections 2 to 3 days before social events so the peak GI effects have passed.
Constipation affects some men and responds to increased fiber, adequate hydration, and gut-supportive strategies. Diarrhea affects others and typically resolves as the body adjusts to each dose level.
The pattern most men report is 3 to 7 days of increased GI symptoms after each dose escalation, followed by gradual improvement. By the third or fourth week at any given dose, most men have adapted and symptoms have minimized.
Fatigue and energy fluctuations
Some men experience fatigue, particularly during the first 4 to 8 weeks. This can result from reduced caloric intake, metabolic adjustment, or both. The tiredness associated with tirzepatide usually resolves as the body adapts to burning fat more efficiently for fuel.
Counterintuitively, maintaining exercise during fatigue phases often helps. Light activity, even a 20-minute walk, can improve energy more than resting. The metabolic shift from primarily glucose-burning to increased fat oxidation creates a temporary energy dip before the body upregulates fat metabolism pathways.
Adequate sleep becomes even more critical. Men on tirzepatide who sleep less than 6 hours show poorer weight loss outcomes and more muscle loss than those getting 7 to 9 hours. Sleep is not a luxury during this process. It is a performance requirement.
Psychological effects men rarely discuss
The reduction in food noise is liberating for most men. But it can also create unexpected challenges.
Social identity tied to eating habits may shift uncomfortably. The guy who always ordered the biggest steak, who could eat a whole pizza, who bonded with friends over massive meals, suddenly does not want those portions. Social dynamics change. Some men report feeling disconnected from social rituals they previously enjoyed.
Relationship dynamics shift when one partner is on tirzepatide and the other is not. Shared meals look different. Restaurant choices change. The partner not on medication may feel judged for their eating habits, even when no judgment is intended.
Body dysmorphia can emerge or intensify. Some men who have been overweight for years struggle to see their changing body accurately. They look in the mirror and still see the old version. Progress photos become essential, not for social media, but for accurate self-perception.
These psychological dimensions are real, common, and worth discussing with a provider or mental health professional. Physical transformation without psychological adaptation is incomplete.
Comparing tirzepatide to other options for men
Men researching weight loss peptides inevitably compare options. Here is how tirzepatide stacks up against the alternatives, with specific attention to male outcomes.
Tirzepatide versus semaglutide for men
The head-to-head data is now available. A New England Journal of Medicine study directly compared tirzepatide to semaglutide for obesity treatment. The results were decisive.
Tirzepatide produced greater weight loss than semaglutide across all dose comparisons. The semaglutide versus tirzepatide comparison shows that the dual GIP/GLP-1 mechanism of tirzepatide consistently outperforms the GLP-1-only approach of semaglutide.
For men specifically, the visceral fat reduction advantage of tirzepatide is particularly relevant. Men carry more visceral fat, and tirzepatide targets it more aggressively. The testosterone recovery benefit, driven by greater total fat loss, also favors tirzepatide in male populations.
However, semaglutide has a longer track record and more long-term safety data. Some men and their providers prefer the known quantity, especially for men who respond well to semaglutide at lower doses with minimal side effects.
The semaglutide dosage calculator can help men understand the differences in dosing between the two medications.
Tirzepatide versus retatrutide
Retatrutide is the emerging triple agonist, targeting GIP, GLP-1, and glucagon receptors. Early trial data shows even greater weight loss potential, with some participants losing over 24% of body weight.
For men, the added glucagon receptor activation in retatrutide may provide enhanced visceral fat targeting, though the long-term data is still limited. The retatrutide comparison is compelling but based on earlier-stage research.
Tirzepatide currently offers the best combination of robust data, proven efficacy, and established safety profile among the multi-agonist weight loss peptides. Retatrutide may eventually prove superior, but the evidence base is not yet mature enough for definitive comparison. Understanding retatrutide availability remains important for men evaluating future options.
Tirzepatide versus traditional approaches
Men often ask whether tirzepatide is worth it compared to just dieting harder or training more. The honest answer: it depends on history.
For men who have successfully lost and maintained significant weight through lifestyle alone, tirzepatide may be unnecessary. But that population is small. Research consistently shows that only 5 to 10% of people who lose significant weight through diet and exercise alone maintain that loss long-term. The biology of weight regain, driven by hormonal adaptations and metabolic slowdown, works against sustained success.
Tirzepatide changes the biological equation. It does not just reduce appetite temporarily. It alters the hormonal signals that drive weight regain. For men who have repeatedly lost and regained weight, this represents a fundamentally different tool, one that addresses the biological drivers of regain rather than just willpower.
The best peptide stack for weight loss article covers additional options for men who want to explore combination approaches.
Tirzepatide and men over 40
Age changes the tirzepatide equation in several important ways. For men in their 40s, 50s, and beyond, the benefits extend well past the scale.
The metabolic reset advantage
Men over 40 face a metabolic headwind that younger men do not. Testosterone naturally declines at approximately 1 to 2% per year after age 30. Muscle mass decreases at 3 to 8% per decade after 30. Basal metabolic rate drops accordingly. And visceral fat tends to accumulate preferentially, driven by declining hormones and changing stress patterns.
Tirzepatide works against all of these trends simultaneously. The fat loss improves testosterone. The improved testosterone supports muscle preservation. The muscle preservation supports metabolic rate. And the reduced visceral fat improves insulin sensitivity, creating a positive feedback loop that counteracts the negative spiral of aging-related metabolic decline.
For men using anti-aging peptides or considering longevity protocols, tirzepatide addresses perhaps the single largest modifiable risk factor for age-related disease: excess body fat.
Joint relief and mobility
Every pound of body weight places approximately 4 pounds of force on the knees during walking. A 50-pound weight loss reduces knee forces by 200 pounds with every step. For men over 40 with joint wear, this is transformative.
Men frequently report that the most life-changing benefit of tirzepatide is not how they look. It is how they move. Knees that ached every morning feel better. The back pain that had become a constant companion eases. Activities that were abandoned years ago, playing basketball, hiking, wrestling with the kids, become possible again.
The joint health benefits compound over time. Less weight means less joint inflammation. Less inflammation means less pain. Less pain means more activity. More activity means more caloric expenditure and better muscle preservation. The virtuous cycle accelerates.
Cardiovascular and metabolic markers
Men over 40 carrying excess weight are in the highest risk category for cardiovascular events. The metabolic improvements from tirzepatide, reduced blood pressure, improved lipid profiles, better glycemic control, and reduced inflammation, directly address the leading cause of death in men.
The before-and-after for this demographic is measured in numbers that do not show up in photos. Triglycerides dropping from 300 to 150. HbA1c falling from 7.2% to 5.6%. Blood pressure normalizing from 145/95 to 120/78. These invisible transformations may add years to a man life and life to a man years.
Peptide protocols for aging adults address additional strategies for men and women navigating the metabolic changes of midlife.
Common mistakes men make on tirzepatide
Knowing what to do is half the battle. Knowing what NOT to do is the other half. These are the most common errors men make, drawn from real-world reports and clinical observations.
Mistake 1: skipping the strength training
This is the biggest and most consequential mistake. Men who rely solely on tirzepatide for weight loss, without resistance training, lose significantly more muscle than those who lift. The medication handles the fat. You handle the muscle. Skip the gym, and you are paying for accelerated aging in exchange for a lower number on the scale.
The fix is simple, though not easy. Three to four resistance training sessions per week, focusing on compound movements, with progressive overload. This is not optional for men who want to look good after weight loss, not just lighter.
Mistake 2: not eating enough protein
Appetite suppression makes it easy to undereat protein. Men who default to whatever sounds palatable, which is often carb-heavy comfort foods in smaller portions, miss the muscle preservation window. Every gram of protein you do not eat during caloric restriction is a gram of muscle that becomes vulnerable to breakdown.
The fix: track protein for at least the first 3 months. Not calories necessarily. Just protein. Hit the 1.6 to 2.2 g/kg target daily, and the rest of the diet tends to sort itself out.
Mistake 3: chasing the scale instead of the mirror
Men who weigh themselves daily and panic over fluctuations make poor decisions. They increase doses prematurely. They cut calories further when the body needs fuel. They interpret a 2-pound overnight increase as failure when it was just water retention from a high-sodium meal.
The fix: weigh weekly under consistent conditions (morning, after bathroom, before food). Track waist circumference biweekly. Take progress photos monthly. Trust the trend, not the daily noise.
Mistake 4: escalating doses too quickly
Impatient men push for faster dose escalation, wanting to get to 15 mg as quickly as possible. This approach increases side effects, makes adherence harder, and does not necessarily improve long-term outcomes.
The tirzepatide dosage guidelines specify minimum 4-week intervals between dose increases for good reason. Each dose level requires physiological adaptation. Rushing through the titration schedule often means more severe GI symptoms, worse adherence, and sometimes temporary discontinuation, which ultimately slows progress.
Mistake 5: stopping cold turkey after reaching goal weight
This might be the most dangerous mistake of all. Men who reach their goal weight and abruptly stop tirzepatide without a tapering plan or maintenance strategy typically regain weight rapidly. The hormonal and neurological adaptations that drove the weight loss reverse. Appetite signals return to pre-treatment levels. And the weight comes back, often with additional fat and less muscle than before.
Maintenance strategies include gradual dose reduction, continuing at a lower maintenance dose, lifestyle modifications that have been established during treatment, and ongoing monitoring. The withdrawal and discontinuation experience is similar across GLP-1 class medications and requires planning.
Combining tirzepatide with other peptides: what men are exploring
Men in the peptide research community often investigate combination approaches. While tirzepatide handles fat loss, other peptides may address complementary goals.
Tirzepatide and BPC-157
BPC-157 is researched for its tissue repair properties and gut protective effects. Some researchers combine it with tirzepatide to potentially mitigate GI side effects, though this combination has not been studied in clinical trials. The theoretical rationale involves BPC-157 protective effects on gastric mucosa, which could offset the GI disturbance that tirzepatide produces.
Using the BPC-157 dosage calculator can help researchers determine appropriate amounts for their protocols.
Tirzepatide and growth hormone secretagogues
Men concerned about muscle preservation sometimes explore ipamorelin or CJC-1295 alongside tirzepatide. The rationale is that enhanced growth hormone release could support muscle preservation during caloric restriction. Some clinics offer combination protocols, particularly for men over 40 where natural GH production has already declined.
The sermorelin ipamorelin blend is one such combination that some male researchers explore for its potential synergistic effects on body composition.
The peptide stack calculator helps researchers plan multi-peptide approaches, and the stacking guide covers compatibility considerations. However, combining any medications or research compounds should only be done under qualified medical supervision.
Tirzepatide and testosterone optimization
For men with documented low testosterone, the combination of tirzepatide-driven fat loss and appropriate hormonal support can produce remarkable results. The fat loss raises natural testosterone while exogenous testosterone (if indicated) supports muscle preservation and energy during the weight loss phase.
This is not a DIY protocol. It requires monitoring of estradiol, total and free testosterone, hematocrit, PSA, and metabolic markers. But when properly managed, the synergy between fat loss and hormonal optimization produces body composition changes that exceed what either intervention achieves alone.
The testosterone boosters versus peptides comparison provides additional context for men evaluating their options. For those exploring research peptides that support male hormonal health, the enclomiphene guide covers another approach to supporting natural testosterone production.
Tracking your transformation: what to measure and when
Men who track their progress systematically get better results than those who rely on subjective assessment. Here is the measurement protocol.
Essential measurements
Body weight: Weekly, same day, same time, same conditions. Monday morning after using the bathroom, before eating or drinking, works for most men. Record the number without judgment. Look at the 4-week trend, not the weekly fluctuation.
Waist circumference: Bi-weekly, at the navel, standing relaxed (not sucking in). This is the most meaningful single measurement for men on tirzepatide because visceral fat loss shows here first.
Progress photos: Monthly, same lighting, same poses, same time of day. Front, side, and back. These photos are not for social media unless you choose to share them. They are for accurate self-assessment, because the mirror lies when you see yourself every day.
Body composition: Monthly if using a bioimpedance scale (understanding its limitations), or quarterly via DEXA scan for the most accurate fat and lean mass measurement. The cost analysis tools can help evaluate whether regular DEXA scans fit your budget.
Performance metrics
Strength levels: Track your main lifts (squat, bench, deadlift, row) weekly. A declining trend indicates potential muscle loss that needs to be addressed through nutrition or programming changes.
Endurance markers: Track resting heart rate, walking speed, or distance. These typically improve steadily as weight drops.
Daily steps: Track via phone or watch. A consistent upward trend in daily movement often correlates with improved energy and reduced pain.
Health markers
Blood work at baseline and quarterly:
Complete metabolic panel (fasting glucose, HbA1c, kidney function, liver function)
Lipid panel (total cholesterol, LDL, HDL, triglycerides)
Hormone panel (total testosterone, free testosterone, estradiol, SHBG)
Inflammatory markers (hsCRP, ESR)
Complete blood count
Thyroid function (TSH, free T3, free T4)
These numbers tell the story the mirror and scale cannot. A man whose weight loss has stalled but whose HbA1c dropped from 6.8 to 5.4 has achieved something profoundly important, even if the before-and-after photos look similar over that period.
Setting realistic expectations: what the data actually says
The internet is full of dramatic before-and-after photos. These are real but represent the best outcomes, not the average. Here is what the clinical data actually predicts for men at different starting points.
Expected weight loss by starting weight
Based on SURMOUNT-1 data showing 15 to 21% body weight reduction over 72 weeks:
Starting at 200 pounds: Expected loss of 30 to 42 pounds over 72 weeks (ending at 158 to 170 pounds).
Starting at 250 pounds: Expected loss of 37 to 52 pounds (ending at 198 to 213 pounds).
Starting at 300 pounds: Expected loss of 45 to 63 pounds (ending at 237 to 255 pounds).
Starting at 350 pounds: Expected loss of 52 to 73 pounds (ending at 277 to 298 pounds).
These ranges reflect the dose-dependent response (5 mg versus 15 mg) and individual variation. Genetic factors, adherence to lifestyle modifications, baseline metabolic health, and age all influence where within this range a man falls.
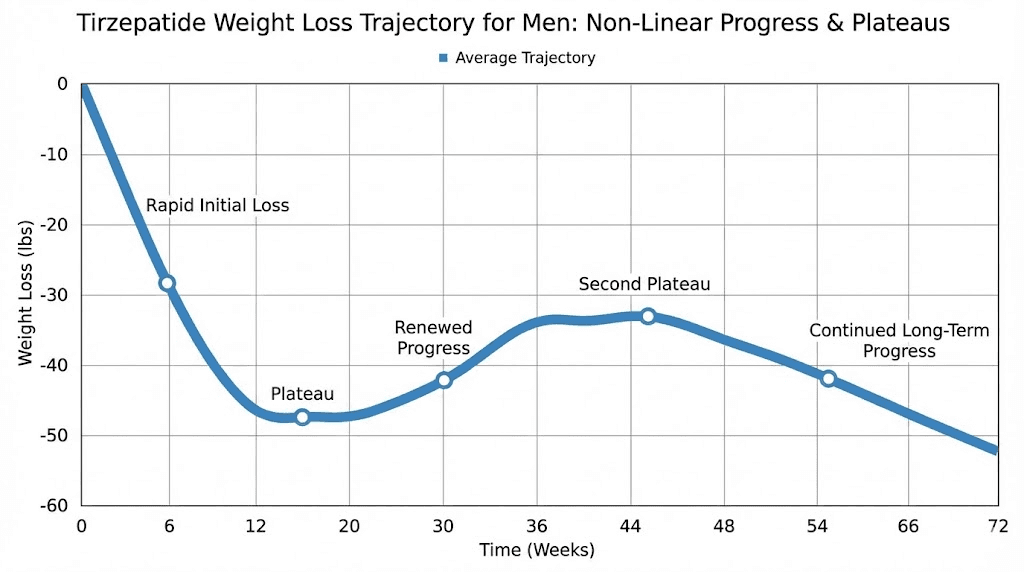
Rate of loss patterns
Weight loss is not linear. The typical male pattern shows rapid initial loss (weeks 1 to 12), gradual deceleration (weeks 12 to 36), and potential plateaus with resumed loss (weeks 36 to 72). Understanding this pattern prevents the discouragement that causes many men to quit during the deceleration phase.
Late responders, men who show minimal response in the first 12 weeks, should not panic. The SURMOUNT-1 post hoc analysis showed that 90% of late responders still achieved at least 5% body weight reduction by week 72, and most achieved significantly more. Patience is not just a virtue here. It is a strategy.
What before and after photos do not show
Transformation photos capture a moment. They do not capture the journey between those moments. They do not show the plateaus that lasted 3 weeks and tested every ounce of resolve. They do not show the morning the scale spiked 4 pounds for no apparent reason. They do not show the social dinners where ordering salad instead of steak felt isolating.
Real transformation is not a straight line from before to after. It is a jagged, frustrating, occasionally exhilarating process that trends in the right direction when you zoom out far enough. The men who succeed are not the ones who lost weight fastest. They are the ones who kept going during the weeks when nothing seemed to be happening.
Tirzepatide storage and handling for men using compounded versions
Many men access tirzepatide through compounding pharmacies. Proper storage and handling directly impacts efficacy, and getting it wrong means wasting both money and time.
Reconstituted tirzepatide must be stored in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Understanding how long tirzepatide lasts in the fridge prevents using degraded product. Most compounded versions maintain potency for 28 to 30 days after reconstitution when properly refrigerated.
Refrigeration requirements are strict. Room temperature exposure degrades the peptide. If your vial has been left out for more than 48 hours, its potency is compromised. When traveling, use an insulated cooler with ice packs, not the car cup holder.
For reconstitution specifics, the peptide reconstitution guide covers the general process, while the reconstitution calculator ensures accurate mixing ratios. Using bacteriostatic water rather than sterile water extends shelf life and reduces contamination risk.
Proper peptide storage is not glamorous but it is the difference between a protocol that works and one that delivers inconsistent results. Men who invest in proper storage practices protect their investment and ensure consistent dosing throughout their treatment.
The financial reality of tirzepatide for men
Cost is a real factor in tirzepatide use, and men deserve an honest discussion about the financial commitment involved. Without insurance coverage, brand-name tirzepatide (Zepbound or Mounjaro) can cost $1,000 to $1,500 or more per month.
Compounded tirzepatide represents a more accessible option for many men, typically costing $200 to $500 per month depending on the pharmacy and dose. The peptide cost calculator can help estimate monthly expenses based on your specific protocol.
When evaluating cost, consider what you are currently spending on the consequences of excess weight. Gym memberships, diet programs, supplements, larger clothing sizes, higher insurance premiums, increased medical visits, and medications for weight-related conditions all carry costs that decrease as weight decreases.
The long-term cost-benefit analysis favors treatment for men with significant obesity-related health risks. Preventing a cardiovascular event, avoiding type 2 diabetes, or eliminating the need for CPAP therapy has value that far exceeds the medication cost.
Frequently asked questions
How much weight can men realistically lose on tirzepatide?
Clinical trial data shows men lose 15 to 21% of their starting body weight over 72 weeks. For a 250-pound man, that translates to 37 to 52 pounds. Individual results vary based on dose, lifestyle modifications, and starting metabolic health.
The tirzepatide before and after results guide covers detailed outcome data.
Does tirzepatide affect testosterone levels in men?
Research shows tirzepatide-driven fat loss can increase endogenous testosterone by 84 to 130 ng/dL in men with obesity-related low testosterone. The mechanism is indirect: less fat means less aromatase activity converting testosterone to estrogen. Men on TRT may need dose adjustments as their body composition changes.
Will I lose muscle on tirzepatide?
Some lean mass loss is expected, approximately 25 to 26% of total weight lost. However, this proportion is identical to weight loss without medication. Resistance training 3 to 4 times per week and protein intake of 1.6 to 2.2 g/kg body weight significantly reduce muscle loss. The muscle growth and preservation guide covers strategies in detail.
How long does it take to see visible results?
Most men notice visible changes by weeks 8 to 12. Waist circumference changes first, followed by face and neck. Significant visible transformation typically occurs between months 3 and 6. Late responders may take longer but still achieve meaningful results by week 72.
Can I drink alcohol on tirzepatide?
Alcohol is not contraindicated with tirzepatide, but it can worsen GI side effects and provides empty calories that slow progress. Many men find that alcohol tolerance decreases on tirzepatide, meaning fewer drinks produce stronger effects. Moderation is advisable, and some men choose to eliminate alcohol entirely during active weight loss phases.
What happens when I stop tirzepatide?
Weight regain is common after discontinuation if lifestyle modifications are not maintained. Studies show that gradual dose tapering produces better long-term outcomes than abrupt cessation. Maintaining the exercise and nutrition habits developed during treatment is critical for sustained results. The discontinuation guide covers this topic comprehensively.
Is tirzepatide safe for men with high blood pressure?
Tirzepatide has been shown to reduce blood pressure in clinical trials. For men with hypertension, the weight loss and metabolic improvements often lead to blood pressure reductions that allow medication adjustments. Always discuss with your prescribing provider, as blood pressure medications may need dose changes during treatment.
How does tirzepatide compare to surgery for men?
Bariatric surgery typically produces 25 to 35% body weight loss, exceeding tirzepatide average of 21%. However, surgery carries higher immediate risk, requires permanent anatomical changes, and has its own long-term complications. For men who prefer a non-surgical approach or do not qualify for surgery, tirzepatide represents the most effective pharmaceutical alternative currently available.
External resources
New England Journal of Medicine: Tirzepatide Once Weekly for Treatment of Obesity
PMC: Body Composition Changes During Weight Reduction with Tirzepatide (SURMOUNT-1)
PMC: Short-term Impact of Tirzepatide on Metabolic Hypogonadism
For men serious about optimizing their tirzepatide results, SeekPeptides provides the most comprehensive resource available, with evidence-based protocols, proven dosing strategies, body composition tracking tools, and a community of thousands of men who have navigated this exact transformation.
In case I do not see you, good afternoon, good evening, and good night. May your visceral fat stay shrinking, your testosterone stay climbing, and your transformation stay on track.