Mar 16, 2026

A 128.5% increase in total testosterone. In two months. Without a single testosterone injection.
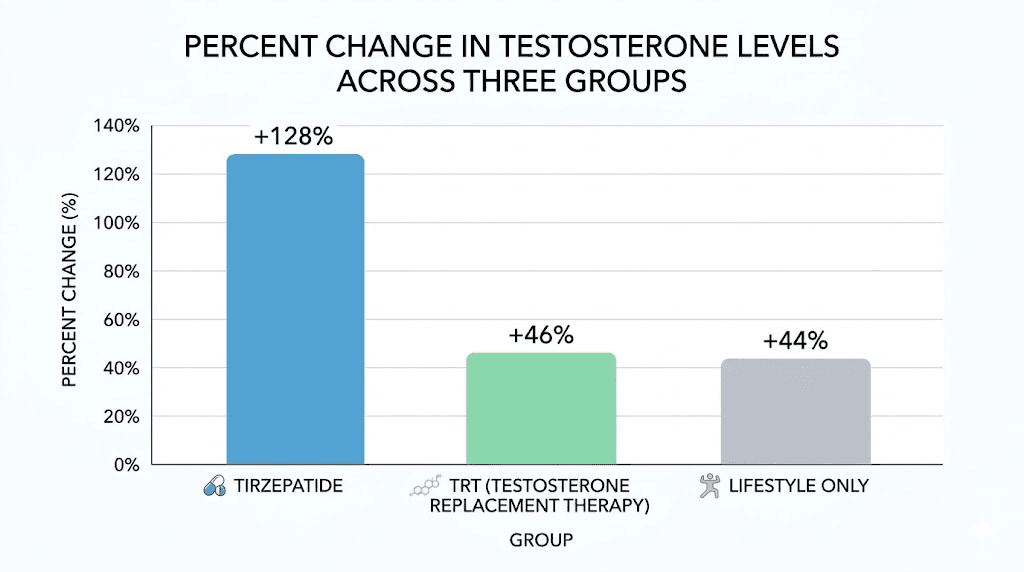
That is not a typo. A controlled pilot study published through the National Institutes of Health followed 83 men with obesity and low testosterone, and the group receiving tirzepatide saw their levels climb from 186 ng/dL to 424 ng/dL. The men on actual testosterone replacement therapy only managed a 46.2% increase over the same period. The lifestyle-only group? Just 44.3%.
Something unexpected is happening at the intersection of tirzepatide and male hormones. And most men have no idea.
For years, the conversation around low testosterone followed a predictable script. Levels drop. Symptoms appear. Doctor prescribes TRT. End of story. But emerging research is rewriting that narrative entirely, revealing that the relationship between obesity, insulin resistance, and testosterone levels is far more intertwined than most protocols account for. And tirzepatide, a medication designed primarily for weight loss and blood sugar management, appears to address the root cause rather than masking symptoms with exogenous hormones.
This guide covers everything researchers need to know about how tirzepatide affects testosterone production, why fat loss restores hormonal function, how it compares to traditional TRT, whether the two can be combined safely, and what the latest clinical data actually shows. Whether you are a man struggling with both weight and low testosterone, or someone on TRT wondering if a GLP-1 medication could reduce your dependence on hormone replacement, the evidence is worth understanding.
The obesity and low testosterone connection most men miss
Low testosterone in men does not exist in a vacuum. In most cases, it is not a standalone condition that appeared randomly. It developed because something else went wrong first.
That something is usually obesity.
Researchers call it metabolic hypogonadism, a form of low testosterone caused directly by excess body fat, insulin resistance, and chronic inflammation. It affects an estimated 30-50% of men with obesity, and the mechanism behind it creates a vicious cycle that becomes progressively harder to break without intervention. Understanding this cycle is essential because it explains exactly why tirzepatide works where other approaches often fail.
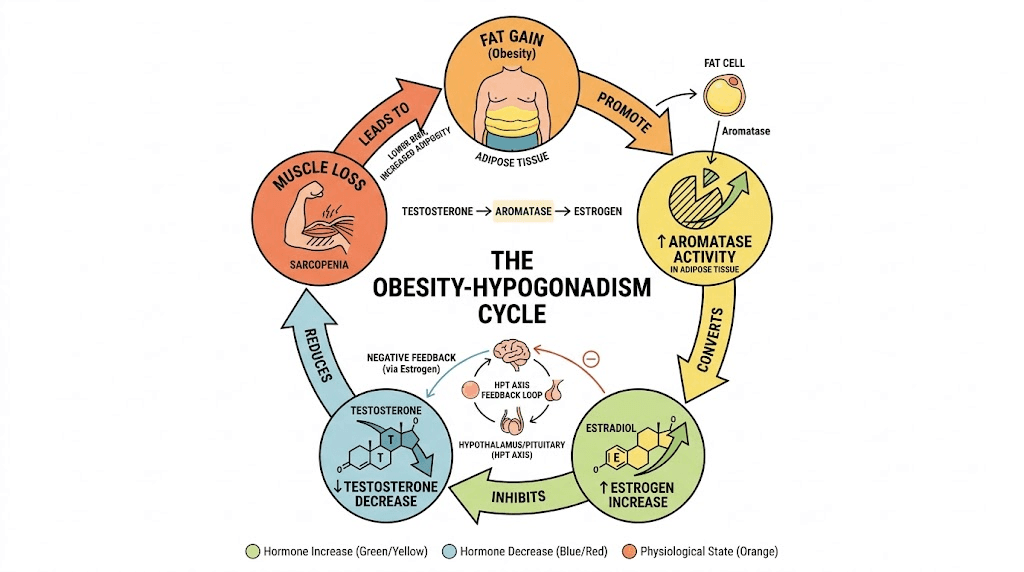
How excess fat destroys testosterone production
Fat tissue is not passive storage. It is an active endocrine organ that produces enzymes, hormones, and inflammatory signals. One enzyme in particular, aromatase (CYP19A1), sits at the center of the obesity-testosterone problem.
Aromatase converts testosterone into estradiol (a form of estrogen). The more fat tissue a man carries, the more aromatase he produces. The more aromatase activity, the more testosterone gets converted into estrogen. This creates a measurable hormonal shift where testosterone drops and estradiol rises simultaneously.
But it does not stop there.
Rising estradiol levels send a signal to the hypothalamus and pituitary gland, the control center that tells the testes how much testosterone to make. Elevated estrogen suppresses the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), the two messenger hormones responsible for triggering testosterone production in the Leydig cells of the testes. Less LH means less stimulation. Less stimulation means less testosterone.
Meanwhile, insulin resistance, which accompanies obesity in the vast majority of cases, reduces sex hormone-binding globulin (SHBG) production in the liver. SHBG is the protein that carries testosterone through the bloodstream. When SHBG drops, the total circulating testosterone decreases further. Hyperinsulinemia also directly suppresses gonadotropin-releasing hormone (GnRH) neurons in the hypothalamus, adding another layer of suppression to the entire hormonal cascade.
Inflammatory cytokines produced by visceral fat, including TNF-alpha and IL-6, compound the problem by directly impairing testicular function and further suppressing the hypothalamic-pituitary-gonadal (HPG) axis. The result is a self-reinforcing downward spiral. Low testosterone promotes more fat storage (particularly visceral fat), which increases aromatase activity, which converts more testosterone to estrogen, which further suppresses production.
Why TRT alone does not fix the underlying problem
Traditional testosterone replacement therapy addresses the symptom, not the cause. It floods the body with exogenous testosterone, which relieves symptoms like fatigue, low libido, and reduced muscle mass. That matters. Those symptoms are real and debilitating.
But TRT does not reduce body fat meaningfully on its own. It does not fix insulin resistance. It does not reduce aromatase activity in adipose tissue. And critically, exogenous testosterone actually suppresses natural LH and FSH production through negative feedback, effectively shutting down the body's own testosterone manufacturing. This creates dependence. Stop the TRT, and levels crash even lower than before because the HPG axis has been suppressed.
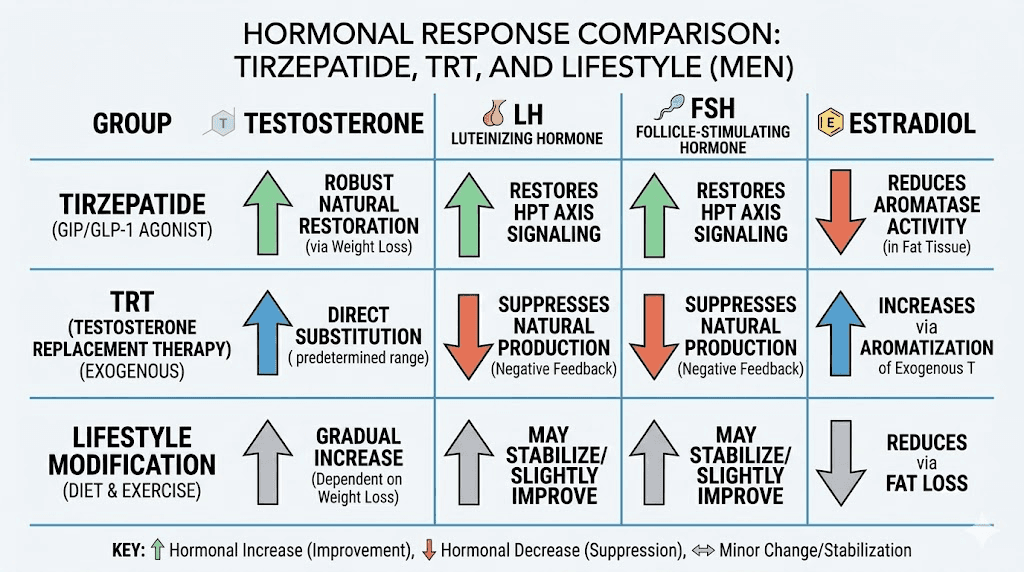
The pilot study data illustrates this perfectly. Men on transdermal testosterone saw their LH levels drop by 23.8% and their FSH drop by 25%. Their bodies were producing less of the hormones needed to make testosterone naturally. In contrast, the tirzepatide group saw LH increase by 80% and FSH increase by 72.2%. Their bodies were producing more of both.
That distinction matters enormously for long-term outcomes.
How tirzepatide increases testosterone levels
Tirzepatide is a dual GIP/GLP-1 receptor agonist. It mimics two natural gut hormones that regulate blood sugar, slow digestion, and reduce appetite. It was developed primarily for type 2 diabetes and weight management, not for testosterone optimization.
Yet it appears to optimize testosterone more effectively than the medication designed specifically for that purpose.
The mechanism is indirect but powerful. Tirzepatide does not stimulate testosterone production directly. Instead, it removes the barriers that were preventing the body from producing adequate testosterone on its own. Think of it as clearing a blocked pipe rather than pouring more water through the clog.
Fat loss reduces aromatase activity
The most significant pathway is straightforward. Tirzepatide produces substantial weight loss, particularly from visceral and subcutaneous fat stores. In the pilot study, the tirzepatide group lost 8.1% of body weight in just two months, with a 42.3% reduction in fat mass. Less fat means fewer adipocytes. Fewer adipocytes means less aromatase enzyme. Less aromatase means less testosterone-to-estradiol conversion.
The numbers in the study confirm this directly. Estradiol dropped by 60% in the tirzepatide group, from 33 pg/mL to 11 pg/mL. The lifestyle-only group saw just a 12.1% estradiol reduction. The TRT group actually saw estradiol increase by 21.2%, rising from 33 pg/mL to 40 pg/mL, because exogenous testosterone provided more substrate for aromatase to convert.
This single finding explains much of the testosterone difference between groups.
Improved insulin sensitivity restores the HPG axis
Weight loss from tirzepatide also improves insulin sensitivity significantly. The HOMA index (a measure of insulin resistance) dropped 13.4% in the tirzepatide group. Improved insulin sensitivity means less hyperinsulinemia, which means less suppression of GnRH neurons and better SHBG production from the liver.
The upstream effect is that the entire HPG axis begins functioning more normally. The hypothalamus sends stronger GnRH signals. The pituitary releases more LH and FSH. The testes respond by producing more testosterone naturally. This is not a temporary boost from an external source. This is the body restoring its own endocrine function.
Reduced inflammation lifts hormonal suppression
Visceral fat produces a steady stream of pro-inflammatory cytokines that directly suppress testicular function. Tirzepatide reduces visceral fat stores aggressively, and the resulting decrease in systemic inflammation removes yet another barrier to testosterone production. Multiple studies have shown that inflammatory markers like C-reactive protein, TNF-alpha, and IL-6 decrease significantly with GLP-1 receptor agonist treatment, each of which has been independently linked to improved gonadal function in men.
The compounding effect
None of these mechanisms work in isolation. They compound. Less fat means less aromatase and less inflammation. Less aromatase means less estrogen conversion and more free testosterone. Less inflammation means better HPG axis signaling. Better insulin sensitivity means more SHBG and stronger GnRH pulses. Each improvement amplifies the others, creating an upward spiral that mirrors the downward spiral that caused the problem.
This is why the tirzepatide group in the study saw total testosterone more than double in just eight weeks, an outcome that surprised even the researchers.
The landmark study: tirzepatide versus TRT head-to-head
The controlled pilot study published through the National Institutes of Health (PMC12220628) deserves a detailed examination because it is the first direct comparison of tirzepatide and testosterone replacement therapy in men with metabolic hypogonadism.
Study design and participants
Researchers enrolled 83 men between October and December of 2024. All participants had obesity (mean BMI 34.9 kg/m2), metabolic hypogonadism (total testosterone below 300 ng/dL), and insulin resistance. The average age was 55.3 years, ranging from 44 to 63.
Three groups were formed. Twenty-eight men received tirzepatide (2.5 mg weekly for month one, escalating to 5 mg weekly for month two). Thirty men received lifestyle modifications only (a 20% caloric deficit plus 20 minutes of daily brisk walking). Twenty-five men received transdermal testosterone therapy (starting at 23 mg daily, titrated based on serum levels).
All groups followed the same lifestyle protocol in addition to their assigned treatment.
Testosterone results
The headline numbers are striking. After two months:
Tirzepatide group: Total testosterone rose from a median of 186.5 ng/dL to 424.0 ng/dL, an increase of 128.5%. Free testosterone and bioavailable testosterone increased proportionally. These men went from clinically hypogonadal to solidly within the normal range, entirely through their own endogenous production.
TRT group: Total testosterone rose from 186.0 ng/dL to 272.0 ng/dL, an increase of 46.2%. While this represents meaningful improvement, the final levels remained in the lower portion of the normal range. And critically, this increase came from an external source, not from restored natural production.
Lifestyle-only group: Total testosterone rose from 192.0 ng/dL to 266.0 ng/dL, an increase of 44.3%. Diet and exercise alone produced nearly identical results to TRT, confirming that weight loss is the primary driver of testosterone recovery in metabolic hypogonadism.
Hormonal cascade improvements
The downstream hormonal changes tell an even more compelling story. In the tirzepatide group, LH surged by 80% (from 2.6 to 4.5 mIU/mL) and FSH by 72.2% (from 1.8 to 3.2 mIU/mL). Both are gonadotropins, the pituitary hormones that directly stimulate testosterone production. Their increase means the HPG axis was actively recovering.
Compare that to the TRT group, where LH dropped 23.8% and FSH dropped 25%. Exogenous testosterone was shutting down the body's own signaling system. When these men eventually discontinue TRT, their HPG axis will need time to recover, a process that can take weeks to months and sometimes requires additional medications like clomiphene or hCG to restart.
Estradiol changes were equally dramatic. A 60% reduction in the tirzepatide group versus a 21.2% increase in the TRT group. The tirzepatide group was making more testosterone while simultaneously having less converted to estrogen. The TRT group was doing the opposite.
Body composition changes
Beyond hormones, the body composition changes in the tirzepatide group were remarkable. Fat mass decreased by 42.3% while lean mass increased by 17.9%. For context, the TRT group, which is specifically known for promoting lean mass, saw a 15% fat mass reduction and 10.5% lean mass increase. The lifestyle group saw essentially no change in either parameter.
Waist circumference, a proxy for visceral fat, dropped 8.2% in the tirzepatide group versus 1.8% in the TRT group. Since visceral fat is the primary source of aromatase activity and inflammatory cytokines, this reduction directly explains the superior hormonal outcomes.
Erectile function improvements
Baseline IIEF-5 scores (the International Index of Erectile Function) were low across all groups, with 64.3% of the tirzepatide group and 52% of the TRT group classified as having severe erectile dysfunction. After two months, the tirzepatide group showed significantly greater improvement in erectile function compared to the lifestyle-only group, and comparable improvement to the TRT group.
This matters because erectile dysfunction is often what drives men to seek testosterone treatment in the first place. The finding that tirzepatide improves sexual function, likely through a combination of improved testosterone levels, better blood flow from weight loss, and psychological benefits of body composition changes, expands its relevance beyond metabolic health.
A separate analysis of electronic health records found that tirzepatide was associated with a 30-45% lower risk of erectile dysfunction compared to other diabetes medications like sitagliptin and dulaglutide, suggesting the benefits extend beyond the study population.
Study limitations to consider
No study is perfect. This was a pilot study with 83 participants, not a large randomized controlled trial. There was no placebo group. The study lasted only two months, so durability of benefits remains uncertain. Participants were not randomized. And the tirzepatide dose was relatively low (5 mg, versus the 10-15 mg doses used in many weight loss protocols), meaning the full potential may not have been captured.
These limitations are real. But the effect sizes were large, statistically significant, and mechanistically plausible. More extensive research is underway.
Who benefits most from tirzepatide for testosterone optimization
Not every man with low testosterone will see these results. The benefits are most pronounced in specific populations where the underlying cause of hypogonadism is metabolic rather than primary testicular failure.
Men with obesity-related hypogonadism
This is the primary target population. If a man has a BMI above 30 and testosterone levels below 300 ng/dL, there is a high probability that the two conditions are causally linked. The obesity is causing the low testosterone through the aromatase, inflammation, and insulin resistance pathways described above.
These men stand to benefit enormously from tirzepatide because addressing the obesity addresses the hormonal dysfunction simultaneously. The study specifically enrolled men in this category, and the results speak clearly.
Signs that low testosterone may be obesity-related include gradual onset of symptoms coinciding with weight gain, no history of testicular injury or disease, relatively preserved LH levels (suggesting the testes can still respond to stimulation), and improvement in symptoms with even modest weight loss.
Men on TRT who want to reduce dependence
Some men have been on testosterone therapy for years and would prefer to restore natural production if possible. For men whose hypogonadism was initially driven by obesity, adding tirzepatide while gradually tapering TRT could allow natural production to recover as weight decreases and metabolic health improves.
This approach requires careful medical supervision. Testosterone levels need monitoring throughout the transition, and the taper must be gradual to avoid symptomatic crashes. But the study data suggests that tirzepatide-induced weight loss can stimulate enough endogenous production to compensate for reduced exogenous dosing, at least in men whose hypogonadism is metabolic in origin.
Men with prediabetes or type 2 diabetes and low testosterone
Type 2 diabetes and low testosterone share insulin resistance as a common root cause. Tirzepatide is FDA-approved for type 2 diabetes management, and the hormonal benefits come as a secondary effect of improved metabolic function. Men in this category may see improvements in both conditions simultaneously.
Who will NOT benefit
Men with primary hypogonadism, where the testes themselves are damaged or dysfunctional, will not see testosterone improvements from weight loss alone. Primary hypogonadism is caused by testicular injury, genetic conditions like Klinefelter syndrome, chemotherapy, radiation, or surgical removal of the testes. In these cases, the HPG axis is functioning properly (LH and FSH are typically elevated, trying to stimulate nonresponsive testes), and weight loss will not restore production that the testes cannot deliver.
Men with normal weight and low testosterone should investigate other causes before assuming tirzepatide will help. Age-related decline, medications, pituitary tumors, and chronic illness can all cause hypogonadism independent of body composition.
Combining tirzepatide and testosterone therapy
For some men, the answer is not tirzepatide or TRT. It is both.
No formal contraindication exists for concurrent use. The two medications operate through entirely distinct mechanisms without documented direct pharmacokinetic interactions. Tirzepatide works through GIP and GLP-1 receptors in the gut, pancreas, and brain. Testosterone works through androgen receptors throughout the body. They do not interfere with each other's absorption, metabolism, or activity.
When combination therapy makes sense
Combination therapy is most appropriate for men with severe symptoms who need immediate testosterone relief while simultaneously addressing the underlying metabolic dysfunction. Starting TRT provides quick symptomatic improvement in energy, libido, and mood while tirzepatide begins the slower process of restoring endogenous production through weight loss.
The goal in these cases is often to use TRT as a bridge. As weight drops and natural testosterone production recovers, TRT can be gradually reduced and potentially discontinued entirely. This requires patience, typically over six months to a year, and close monitoring of hormone levels throughout.
Other scenarios where combination therapy makes sense include men with very high BMI (above 40) where natural recovery will take considerable time, men with both primary and secondary hypogonadism (where weight loss can partially improve levels but not fully normalize them), and men with severe erectile dysfunction or sexual dysfunction who need faster symptom relief.
How they complement each other
The combination creates several synergistic effects. Testosterone promotes lean mass retention during the caloric deficit that tirzepatide induces. More lean mass means higher resting metabolic rate, which accelerates fat loss. Meanwhile, the fat loss from tirzepatide reduces aromatase activity, meaning less of the exogenous testosterone gets converted to estrogen, improving the efficiency of the TRT itself.
Testosterone also provides psychological benefits, improved motivation, better exercise tolerance, and enhanced recovery, that support the lifestyle modifications needed to maximize tirzepatide results. Men who feel better are more likely to exercise, eat well, and stay compliant with their protocols.
Critical monitoring requirements
Combined therapy demands more frequent monitoring than either treatment alone.
Baseline testing before starting: Total and free testosterone, LH, FSH, estradiol, SHBG, complete blood count (especially hematocrit), comprehensive metabolic panel, HbA1c, lipid panel, and PSA for men over 40.
At 3 and 6 months: Repeat testosterone levels (timed appropriately for the TRT formulation being used), hematocrit, estradiol, and metabolic panel. If endogenous testosterone production has increased substantially due to weight loss, the TRT dose may need reduction to avoid supraphysiological levels.
Ongoing: Hematocrit monitoring is particularly important. Both testosterone and the metabolic changes from weight loss can affect red blood cell production. Hematocrit exceeding 54% warrants dose reduction of testosterone. PSA should be checked annually. Blood pressure monitoring throughout is essential since both weight changes and hormone fluctuations can affect cardiovascular parameters.
Estradiol monitoring becomes especially important in this combination. As fat decreases, aromatase activity drops, and the amount of testosterone being converted to estrogen changes. If estradiol drops too low, side effects like joint pain, poor sleep, and dry symptoms can emerge. If it remains elevated despite weight loss, additional investigation may be warranted.
Contraindications for the combination
Men with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome should not use tirzepatide. Men with polycythemia (elevated red blood cell count), untreated sleep apnea, or uncontrolled heart failure should not use testosterone. Elevated PSA (an increase of more than 1.4 ng/mL in 12 months) warrants stopping TRT and investigating further.
Tirzepatide dosing for testosterone optimization
The pilot study used a conservative dosing protocol: 2.5 mg weekly for the first month, increasing to 5 mg weekly for the second month. Even at this relatively low dose, the testosterone results were dramatic. Standard tirzepatide dosing for weight loss goes up to 15 mg weekly, suggesting that higher doses (with correspondingly greater weight loss) could produce even more pronounced hormonal improvements.
Starting protocol
The recommended approach mirrors standard tirzepatide initiation:
Weeks 1-4: 2.5 mg subcutaneously once weekly. This is an initiation dose designed to assess tolerance and minimize gastrointestinal side effects. Testosterone changes will be minimal at this point.
Weeks 5-8: 5 mg weekly. The study showed significant testosterone increases at this dose. Most men will begin noticing improved energy and mood around this phase as weight loss accelerates.
Weeks 9-12: 7.5 mg weekly if tolerated and additional weight loss is desired. Greater fat reduction at this dose should further enhance testosterone recovery.
Weeks 13+: 10-15 mg weekly as the maintenance dose for continued weight loss. The full hormonal benefits typically become apparent after 2-3 months of sustained fat loss.
Injection technique follows standard subcutaneous protocol. Rotate between the abdomen, thigh, and upper arm. Use a 31-gauge insulin syringe for minimal discomfort. Inject at the same time each week for consistency.
When to expect testosterone changes
Based on the study timeline and clinical reports:
Weeks 2-4: Minimal hormonal changes. Weight loss is just beginning, and the metabolic improvements that drive testosterone recovery have not yet accumulated sufficiently. GI side effects are most common during this period as the body adjusts.
Weeks 4-8: First measurable testosterone increases. The study showed significant changes by the two-month mark. LH and FSH begin rising as estrogen drops and the HPG axis starts recovering. Energy and mood may improve noticeably.
Weeks 8-16: More substantial gains as cumulative weight loss deepens. Men losing 10-15% of body weight can expect meaningful testosterone recovery. Libido and sexual function typically improve during this window.
Months 4-6+: Peak effects for men continuing to lose weight. Those reaching 15-20% weight loss from baseline may see testosterone levels normalize entirely without any exogenous hormone support.
Factors that influence the response
Not every man will see a 128% increase. Several variables affect outcomes. Starting BMI matters: men with more fat to lose have more aromatase to eliminate and more metabolic dysfunction to reverse, meaning their potential improvement is greater. Baseline testosterone levels matter: men starting at 150 ng/dL have more room for improvement than those starting at 280 ng/dL.
Age plays a role. Younger men typically have more HPG axis plasticity and may recover faster. Older men may see improvements but potentially to a lesser degree. Duration and severity of obesity matters too. A man who gained weight over 2-3 years may recover faster than someone who has been obese for two decades, though both can improve.
Diet quality during tirzepatide use significantly impacts outcomes. Adequate protein intake (1.2-1.6 g per kg of body weight daily) preserves lean mass and supports overall metabolic function. Zinc and vitamin D supplementation support testosterone synthesis directly. Regular resistance training amplifies both the body composition and hormonal benefits.
Tirzepatide versus TRT: a comprehensive comparison
Understanding the differences between these approaches requires looking beyond just the testosterone numbers. Each has distinct advantages, limitations, and implications for long-term health.
Factor | Tirzepatide | TRT |
|---|---|---|
Testosterone increase | 128.5% (study data) | 46.2% (study data) |
Source of testosterone | Endogenous (body produces it) | Exogenous (external supply) |
LH/FSH effect | Increases (+80%/+72%) | Decreases (-24%/-25%) |
Estradiol effect | Decreases (-60%) | Increases (+21%) |
Fat loss | Significant (-42% fat mass) | Modest (-15% fat mass) |
Lean mass | +17.9% | +10.5% |
Weight loss | -8.1% body weight | -3.0% body weight |
Insulin sensitivity | Improves significantly | Modest improvement |
Fertility impact | Preserves/improves | Impairs (suppresses sperm) |
Dependency risk | Low (restores natural function) | High (creates dependence) |
Discontinuation | Gradual testosterone decline possible if weight regained | HPG axis suppression, recovery needed |
Speed of symptom relief | Slower (weeks to months) | Faster (days to weeks) |
Side effects | GI (nausea, diarrhea) | Polycythemia, acne, mood swings |
Additional benefits | Weight loss, diabetes management, cardiovascular | Bone density, direct muscle anabolism |
Cost | Variable (compounded vs brand) | Generally lower |
The fertility consideration
One of the most significant differences that many men overlook is the impact on fertility. TRT suppresses spermatogenesis. The exogenous testosterone sends feedback to the pituitary that reduces FSH, the hormone that drives sperm production. Many men on TRT become functionally infertile within months. Recovery after discontinuation is possible but not guaranteed, and it can take 6-12 months or longer.
Tirzepatide does the opposite. By increasing FSH by 72.2%, it actually supports the hormonal environment needed for healthy sperm production. For men who want to optimize testosterone while preserving or improving fertility, this distinction is potentially decisive.
The cardiovascular angle
Tirzepatide has demonstrated cardiovascular benefits in large clinical trials, including reductions in blood pressure, inflammatory markers, and cardiovascular event risk. TRT has a more complicated cardiovascular profile, with some studies suggesting increased risk and others showing neutral or beneficial effects. For men with existing cardiovascular disease or significant risk factors, tirzepatide may be the safer choice on multiple levels.
Practical protocols for testosterone optimization with tirzepatide
Based on the available evidence, here are three evidence-based protocols for men seeking to use tirzepatide for testosterone optimization.
Protocol 1: Tirzepatide monotherapy for metabolic hypogonadism
Goal: Restore natural testosterone production through weight loss and metabolic improvement.
Who it is for: Men with BMI above 30, testosterone below 300 ng/dL, no primary testicular pathology, and willingness to wait 2-4 months for full hormonal effects.
Approach:
Tirzepatide: Start 2.5 mg weekly, escalate monthly to 5 mg, then 7.5 mg, up to 10-15 mg based on tolerance and response
Diet: 500-750 calorie deficit with emphasis on high protein (1.4 g/kg body weight minimum)
Exercise: Resistance training 3-4 times weekly plus 150 minutes of moderate cardio
Supplements: Zinc (30 mg daily), vitamin D (4000 IU daily), magnesium (400 mg daily), vitamin B12
Sleep: 7-9 hours nightly (critical for testosterone production)
Monitoring schedule:
Baseline: full hormone panel, metabolic panel, CBC
Month 2: testosterone, LH, FSH, estradiol, body composition
Month 4: repeat full panel
Month 6: comprehensive reassessment
Expected timeline:
Weeks 4-6: initial energy improvements, early weight loss
Weeks 8-12: measurable testosterone increase, improved mood and motivation
Months 3-4: significant testosterone recovery, noticeable body composition changes
Months 5-6: approaching normalized levels if weight loss is substantial
Protocol 2: Tirzepatide plus TRT bridge (severe symptoms)
Goal: Immediate symptom relief via TRT while tirzepatide restores natural production, then gradual TRT withdrawal.
Who it is for: Men with severe symptoms (extreme fatigue, complete loss of libido, significant depression) who cannot wait months for improvement, combined with BMI above 30 and metabolic dysfunction.
Approach:
Tirzepatide: Standard escalation as above
Testosterone: Start at standard dose, plan reassessment at 3 months
At month 3: if endogenous LH/FSH are recovering and weight loss exceeds 8%, begin reducing TRT dose by 25%
At month 4-5: if testosterone levels remain adequate at reduced TRT dose, reduce another 25%
At month 6+: reassess whether TRT can be fully discontinued
Critical rules:
Never discontinue TRT abruptly, always taper
Monitor testosterone levels 2-3 weeks after each dose reduction
If symptoms return during tapering, hold at current dose for 4-6 weeks before attempting further reduction
Some men may need to maintain low-dose TRT indefinitely, that is acceptable
Protocol 3: Tirzepatide for TRT optimization
Goal: Improve TRT effectiveness by reducing aromatase activity, not necessarily discontinuing TRT.
Who it is for: Men currently on TRT who experience high estradiol conversion, poor body composition despite testosterone therapy, or who need an aromatase inhibitor and want a natural alternative.
Approach:
Continue current TRT regimen
Add tirzepatide at standard escalation
As fat mass decreases, expect estradiol to decrease proportionally
May need to reduce or eliminate aromatase inhibitor if currently using one
May need to reduce TRT dose if combined testosterone (exogenous + recovering endogenous) becomes supraphysiological
This protocol is particularly useful for men who have been told they need an aromatase inhibitor (like anastrozole) alongside their TRT. By reducing fat mass and therefore aromatase activity naturally, tirzepatide can eliminate the need for AI medications, which carry their own side effect profiles including joint pain, reduced bone density, and mood changes.
Side effects and safety considerations
Combining metabolic and hormonal interventions requires awareness of potential side effects from both angles.
Tirzepatide side effects
The most common tirzepatide side effects are gastrointestinal: nausea, diarrhea, constipation, and bloating. These are most pronounced during dose escalation and typically improve within 2-4 weeks at each dose level. Eating smaller, more frequent meals helps. Avoiding high-fat foods during dose changes reduces nausea.
Less common but more serious risks include gallbladder disease (rapid weight loss increases gallstone risk), pancreatitis (rare but requires monitoring), and the theoretical risk of medullary thyroid carcinoma based on animal studies.
In the pilot study, none of the 28 men on tirzepatide experienced side effects severe enough to require discontinuation. At the 2.5-5 mg doses used, tolerability was good.
Testosterone-related considerations
As testosterone levels rise, whether from endogenous recovery or exogenous supplementation, some men experience:
Acne: Increased androgen levels stimulate sebaceous glands. Usually mild and manageable with topical treatments.
Hair changes: Men genetically predisposed to androgenic alopecia may notice accelerated thinning. This is a consideration worth discussing before starting treatment.
Mood and energy fluctuations: Rising testosterone levels can cause temporary mood swings, increased irritability, or heightened emotional states during the adjustment period. These typically stabilize within weeks.
Sleep changes: Testosterone influences sleep architecture. Some men report improved sleep quality, while others initially experience disruption. Sleep apnea should be monitored, as testosterone can worsen existing obstructive sleep apnea.
Prostate considerations: Testosterone does not cause prostate cancer, but it can stimulate growth of existing prostate tissue. PSA monitoring is standard practice for any man experiencing rising testosterone levels.
The muscle preservation question
One concern with any significant weight loss is the loss of lean muscle mass alongside fat. GLP-1 medications have been criticized for causing excessive muscle loss in some patients. However, the pilot study showed the opposite, the tirzepatide group gained 17.9% lean mass while losing 42.3% fat mass.
This favorable body composition shift is likely due to the simultaneous testosterone increase. Rising testosterone is strongly anabolic, promoting protein synthesis and muscle preservation even during caloric deficit. Combined with adequate protein intake and resistance training, the concern about muscle loss with tirzepatide appears less relevant in men who are also experiencing testosterone recovery.
That said, resistance training is not optional. It is essential. Men using tirzepatide for testosterone optimization should train with weights at least 3-4 times weekly, focusing on compound movements (squats, deadlifts, bench press, rows) that maximally stimulate both testosterone production and muscle retention.
The role of diet and lifestyle in maximizing results
Tirzepatide is not a magic solution. It is a powerful tool that works best within a comprehensive approach. The men in the study who saw 128% testosterone increases were also following a hypocaloric diet and exercising daily. The medication amplified their efforts enormously, but those efforts still mattered.
Nutritional priorities
Protein: Aim for 1.2-1.6 grams per kilogram of body weight daily. Protein supports testosterone synthesis, preserves lean muscle during weight loss, and enhances satiety. Good sources include lean meats, fish, eggs, and dairy. For men on tirzepatide who experience reduced appetite, protein shakes can help meet targets.
Healthy fats: Testosterone is synthesized from cholesterol. Extremely low-fat diets can impair production. Include moderate amounts of monounsaturated fats (olive oil, avocados, nuts) and omega-3 fatty acids (fatty fish, fish oil). Aim for 25-35% of calories from fat.
Zinc-rich foods: Zinc is directly involved in testosterone synthesis and is one of the most common micronutrient deficiencies in men. Oysters, beef, pumpkin seeds, and chickpeas are excellent sources. A daily zinc supplement of 30 mg provides insurance.
Vitamin D: Low vitamin D is independently associated with low testosterone. Most men, especially those with obesity, are deficient. Supplement with 4000-5000 IU daily unless blood levels are already optimal (50-80 ng/mL).
Magnesium: Involved in over 300 enzymatic reactions including testosterone production. Most men do not consume enough. Supplement with 400 mg of magnesium glycinate or citrate before bed (also improves sleep quality).
Foods to emphasize: cruciferous vegetables (broccoli, cauliflower, Brussels sprouts) contain compounds that help metabolize estrogen more efficiently. This supports the estradiol reduction that tirzepatide is already driving through fat loss.
Exercise strategy
Resistance training is the single most impactful exercise intervention for testosterone. Heavy compound lifts directly stimulate acute testosterone release, and the progressive overload principle builds the lean mass that supports higher baseline levels. Train 3-4 days per week minimum, focusing on progressive overload.
High-intensity interval training (HIIT) also stimulates testosterone release more effectively than steady-state cardio. Two to three 20-minute HIIT sessions per week complement resistance training well without the cortisol-elevating effects of prolonged endurance exercise.
Avoid overtraining. Excessive exercise, particularly high-volume endurance training, increases cortisol and can suppress testosterone. More is not always better. Recovery days matter.
Sleep optimization
Testosterone production peaks during deep sleep. Men who sleep fewer than 5 hours per night have testosterone levels 10-15% lower than those sleeping 7-8 hours. This is a massive, easily addressable variable that many men ignore.
Prioritize 7-9 hours of quality sleep. Keep the bedroom cool and dark. Avoid screens for 30-60 minutes before bed. Magnesium supplementation before bed can improve both sleep quality and testosterone. Address sleep apnea if present, as it independently suppresses testosterone and is common in obese men.
Stress management
Chronic stress elevates cortisol, which directly antagonizes testosterone production. The relationship is inverse: as cortisol rises, testosterone falls. Finding effective stress management strategies, whether meditation, walking, hobbies, or social connection, has measurable effects on hormone levels.
What the research says about GLP-1 medications and male hormones broadly
Tirzepatide is not the only GLP-1 medication showing testosterone benefits. The pattern appears consistent across the class.
Semaglutide and testosterone
A large analysis of electronic health records examined 110 adult men with obesity or type 2 diabetes being treated with semaglutide, dulaglutide, or tirzepatide. Along with 10% weight loss, the proportion of men with normal levels of both total and free testosterone rose from 53% to 77%. This confirms that the testosterone benefit is a class effect related to weight loss rather than a unique property of any single medication.
The Endocrine Society presented data showing that anti-obesity medications can normalize testosterone levels in men, with semaglutide showing similar but slightly less pronounced effects compared to tirzepatide. The difference is likely attributable to tirzepatide dual mechanism producing greater weight loss.
The GLP-1 and testosterone connection
GLP-1 receptor agonists may have effects on testosterone beyond just weight loss, though this remains an area of active research. GLP-1 receptors have been identified on Leydig cells in animal studies, suggesting a potential direct effect on testosterone production. However, human studies have not yet confirmed whether this direct pathway is clinically significant or whether the observed benefits are entirely attributable to weight loss and metabolic improvement.
The honest answer is that we do not know yet whether tirzepatide has testosterone-enhancing effects independent of weight loss. What we do know is that the weight loss it produces is substantial enough to dramatically reverse metabolic hypogonadism, and for most men, that distinction may be academic.
Retatrutide and emerging compounds
Retatrutide, a triple-agonist (GLP-1/GIP/glucagon) currently in late-stage clinical trials, produces even greater weight loss than tirzepatide in preliminary data. If the testosterone benefits scale with weight loss as the evidence suggests, retatrutide could produce even more dramatic hormonal improvements. Studies specifically examining its effects on male hormones are anticipated.
Common questions men ask about tirzepatide and testosterone
The intersection of these two topics generates significant confusion. Here are the most searched questions with evidence-based answers.
Does tirzepatide lower testosterone?
No. The evidence consistently shows the opposite. Tirzepatide increases testosterone in men with obesity-related low testosterone by promoting fat loss, reducing aromatase activity, improving insulin sensitivity, and restoring HPG axis function. The pilot study showed a 128.5% increase, and broader analyses of GLP-1 medications show similar patterns.
The concern likely stems from the fact that rapid weight loss from any cause can temporarily affect hormone levels. During very aggressive caloric restriction, testosterone can dip temporarily. But with tirzepatide, the metabolic improvements appear to outweigh any temporary suppressive effects of caloric deficit, resulting in net testosterone increases even during active weight loss.
Can I take tirzepatide and testosterone together?
Yes. No formal contraindication exists. The two medications work through entirely different mechanisms and do not interact pharmacologically. Many clinicians now prescribe both concurrently, particularly for men with severe symptoms who need immediate relief while working toward metabolic improvement.
The key consideration is monitoring. As tirzepatide-induced weight loss restores natural testosterone production, the exogenous testosterone dose may need reduction to avoid supraphysiological levels. Regular blood work every 2-3 months during the first year of combined therapy is essential.
Will my testosterone drop when I stop tirzepatide?
This depends on whether weight regain occurs. If a man stops tirzepatide and maintains his weight loss through diet and exercise, his testosterone levels should remain improved because the metabolic dysfunction that caused the hypogonadism has been corrected. The body does not need the medication to maintain production, it needs to maintain the healthier body composition.
However, if weight regain occurs after stopping, as it does in many cases, the aromatase activity, inflammation, and insulin resistance will return, and testosterone will likely decline again. This is not a failure of the medication. It is the natural consequence of the obesity-hypogonadism cycle re-establishing itself.
This is why long-term weight maintenance strategies are critical for men using tirzepatide for hormonal optimization.
How long does it take for tirzepatide to increase testosterone?
The study showed statistically significant increases at 2 months, even at a low 5 mg weekly dose. Clinically meaningful improvement (where men notice changes in energy, mood, and libido) typically begins around weeks 6-8. Full optimization may take 4-6 months depending on the amount of weight loss achieved and the starting degree of metabolic dysfunction.
Is tirzepatide better than TRT for low testosterone?
For men with obesity-related hypogonadism, the evidence suggests tirzepatide may be more effective at restoring testosterone than TRT, while also addressing the underlying cause, preserving fertility, and providing additional metabolic benefits. The study showed higher final testosterone levels, better body composition, and restored HPG axis function in the tirzepatide group compared to TRT.
For men with primary hypogonadism (testicular failure), TRT remains necessary because no amount of weight loss will restore function that the testes cannot provide.
For many men, the answer may be both initially, transitioning to tirzepatide alone as natural production recovers.
Frequently asked questions
Does tirzepatide affect testosterone in women?
The hormonal effects discussed in this article are specific to men with obesity-related hypogonadism. In women, tirzepatide may affect hormonal balance differently, including potential effects on estrogen, progesterone, and androgens. Women with PCOS may see reduced androgen levels with weight loss, which is typically beneficial. The testosterone-boosting effects described here apply to men.
Can tirzepatide replace clomiphene for low testosterone?
Clomiphene citrate works by blocking estrogen receptors at the pituitary, tricking the body into producing more LH and FSH. Tirzepatide achieves a similar upstream effect through a completely different mechanism, reducing actual estrogen production rather than blocking its receptors. For men with obesity-related hypogonadism, tirzepatide addresses the root cause more comprehensively while providing significant additional health benefits that clomiphene does not.
Will insurance cover tirzepatide for low testosterone?
Currently, tirzepatide is FDA-approved for type 2 diabetes (as Mounjaro) and obesity (as Zepbound). It is not approved specifically for hypogonadism. Insurance coverage depends on whether a man qualifies under the approved indications. Men with BMI above 30 or above 27 with a weight-related comorbidity may qualify for the obesity indication. Compounded tirzepatide is available as a more affordable alternative for those without insurance coverage.
Should I stop TRT before starting tirzepatide?
No. Do not stop TRT abruptly. If the plan is to transition from TRT to tirzepatide monotherapy, start tirzepatide while continuing TRT at the current dose. After 2-3 months, once weight loss is established and testosterone levels can be reassessed, begin a gradual taper under medical supervision. Abrupt TRT discontinuation causes symptomatic hormone crashes that are unnecessary and avoidable.
What testosterone level can I expect from tirzepatide?
The study showed men going from approximately 186 ng/dL to 424 ng/dL (well within the normal range of 300-1000 ng/dL). Individual results will vary based on starting weight, amount of fat lost, baseline metabolic dysfunction, age, and genetic factors. The correlation with weight loss percentage is strong: greater fat reduction generally produces greater testosterone recovery.
Does microdosing tirzepatide affect testosterone?
Microdosing tirzepatide (using lower than standard doses) may produce smaller testosterone improvements due to more modest weight loss. The hormonal benefits appear to be dose-dependent through the weight loss pathway. That said, even the study's conservative 5 mg dose produced dramatic results, so standard therapeutic doses should be sufficient for most men.
External resources
NIH PMC: Short-term impact of tirzepatide on metabolic hypogonadism
Endocrine Society: Anti-obesity medications can normalize testosterone levels
NIH PMC: Impact of Weight Loss on Testosterone Levels review
European Journal of Endocrinology: Hypogonadism and metabolic health in men
For researchers serious about optimizing both metabolic health and hormonal function, SeekPeptides provides the most comprehensive resource available. Members access evidence-based protocols for tirzepatide dosing, TRT management, and hormonal optimization, along with dosing calculators, detailed guides, and a community of thousands who have navigated these exact decisions. Whether you are exploring tirzepatide as an alternative to TRT, combining the two for maximum effect, or simply trying to understand how your weight loss medication is affecting your hormones, SeekPeptides has the resources to support informed, evidence-based decisions.
In case I do not see you, good afternoon, good evening, and good night. May your testosterone stay optimal, your metabolism stay efficient, and your protocols stay evidence-based.