Mar 18, 2026

Before you skip your next injection and call it done, you need to understand exactly what happens inside your body when tirzepatide disappears from your system. Because stopping cold turkey is not the same as stopping safely. And the difference between the two could mean keeping your results or watching months of progress unravel in weeks.
The question itself sounds simple enough. Can you stop tirzepatide cold turkey? Technically, yes. Unlike benzodiazepines or corticosteroids, tirzepatide does not create the kind of physical dependence that makes abrupt cessation dangerous. There is no seizure risk. No withdrawal syndrome that sends you to the emergency room. The FDA prescribing information does not require a taper protocol.
But "can you" and "should you" are very different questions. The SURMOUNT-4 trial, one of the largest studies on tirzepatide weight loss outcomes, found that 82.5% of participants who stopped the medication regained at least 25% of their lost weight within a year. Some regained far more. The mechanisms behind this, the appetite changes, metabolic shifts, and hormonal recalibrations, deserve a thorough explanation before you make any decisions about discontinuation. This guide covers everything: what the research actually shows, a detailed week-by-week timeline of what to expect, the critical difference between cold turkey and gradual tapering, and a complete strategy for protecting your results if you do decide to stop. SeekPeptides has compiled the most comprehensive breakdown of tirzepatide discontinuation available, drawing from clinical trial data, real-world experiences, and evidence-based maintenance protocols.
What happens when you stop tirzepatide cold turkey
Stopping tirzepatide abruptly triggers a cascade of physiological changes. Not all at once. Not overnight. But steadily, predictably, and for most people, noticeably.
The first thing to understand is how tirzepatide works in the first place. It is a dual GIP and GLP-1 receptor agonist that slows gastric emptying, reduces appetite signaling in the brain, and improves insulin sensitivity. When you stop the medication, all of those effects begin to reverse. Not immediately, because tirzepatide has a long half-life of approximately five days. But the reversal is inevitable.
Here is what happens in sequence.
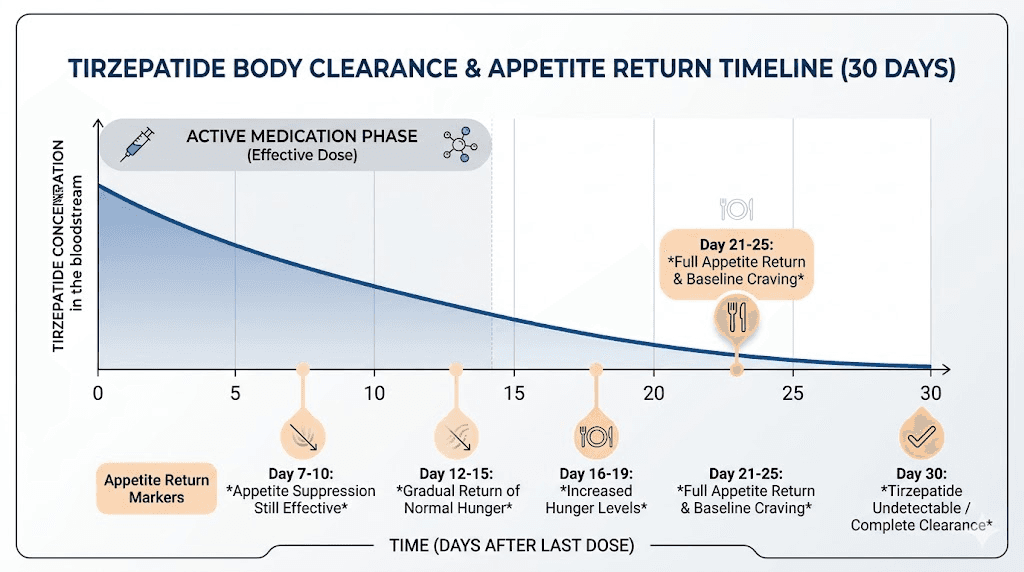
Your appetite starts returning. The appetite suppression that tirzepatide provides does not switch off like a light. It fades gradually as drug levels decline. Most people notice increased hunger within 7 to 10 days of their last injection. Food begins occupying more mental space. Portions that felt satisfying start feeling inadequate. The phenomenon researchers call "food noise," that constant background hum of thinking about your next meal, returns with force around weeks two and three.
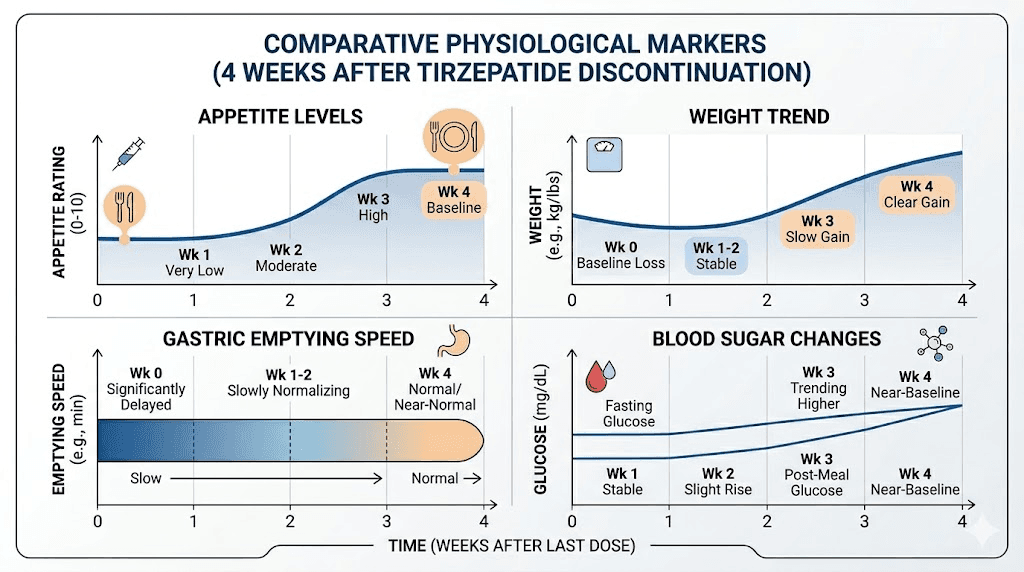
Gastric emptying speeds up. One of the reasons you felt full on smaller meals was that tirzepatide dramatically slowed how fast food moved through your stomach. Without the medication, your digestive system returns to its previous pace. Meals pass through faster. Satiety after eating does not last as long. This is not a side effect of stopping. It is simply your body returning to its baseline function.
Blood sugar regulation shifts. If you were using tirzepatide for metabolic benefits, the improvements in insulin sensitivity and glucose control begin to deteriorate. Blood sugar levels may rise, particularly after carbohydrate-heavy meals. For people with type 2 diabetes, this requires careful monitoring and potentially adjusting other medications.
Weight regain begins. This is the change that concerns most people, and it is the most well-documented. The timeline varies, but research suggests measurable weight regain can begin as early as eight weeks after your last dose. Without the medication supporting reduced calorie intake and improved metabolic function, the body starts trending back toward its previous set point.
The gastrointestinal reset
There is one upside to stopping. If you experienced constipation on tirzepatide, that typically resolves. The bloating that some users report also tends to improve. Gastrointestinal side effects generally clear within one to two weeks as the medication leaves your system. Nausea fades. Acid reflux settles. Your digestive system finds its natural rhythm again.
But make no mistake. The comfortable side effects leaving does not mean everything returns to a better version of normal. It means your body is losing the therapeutic support that was driving your results.
Psychological and behavioral changes
This part gets less attention than it deserves. Many people on tirzepatide describe a fundamentally different relationship with food. Reduced cravings. Less emotional eating. The ability to walk past a bakery without a second thought. When the medication leaves your system, those old patterns do not just return as habits. They return as biology. The neurological pathways that tirzepatide was modifying in the brain, particularly in the hypothalamus and reward centers, revert to their previous state.
Some people describe it as losing a superpower they did not realize they had until it was gone. The mental effort required to make food decisions increases dramatically. This is not a failure of willpower. It is a pharmacological reality that anyone considering cold turkey discontinuation needs to understand.
Hormonal cascades after discontinuation
The endocrine system responds to tirzepatide withdrawal in several measurable ways that go beyond simple appetite changes. Ghrelin, often called the hunger hormone, is produced by cells in the stomach lining. While tirzepatide suppresses ghrelin signaling through its GIP and GLP-1 receptor activity, stopping the medication allows ghrelin levels to normalize. For most people, this means ghrelin rises back to pre-treatment levels within two to three weeks. The practical effect is unmistakable: your stomach starts sending hunger signals with a frequency and intensity that feels almost aggressive after months of pharmaceutical quiet.
Leptin, the satiety hormone produced by fat cells, tells your brain how much energy you have stored. Here is where it gets complicated. When you lose significant weight on tirzepatide, your fat cells shrink. Smaller fat cells produce less leptin. Less leptin means your brain receives weaker "you have enough energy" signals. This creates a biological drive to eat more and restore fat stores, completely independent of anything tirzepatide was doing. It is a survival mechanism that evolved over millions of years, and no amount of motivation overrides it without deliberate strategies.
Insulin sensitivity, which improved during tirzepatide treatment, begins to decline. This affects how efficiently your body processes carbohydrates and stores energy. Fasting glucose levels rise. Post-meal blood sugar spikes become more pronounced. For people without diabetes, these changes are subtle. For those with metabolic concerns, they require monitoring.
GLP-1 levels produced naturally by your body do not change because of tirzepatide discontinuation. Your body was still producing its own GLP-1 throughout treatment. The medication was supplementing that natural production, not replacing it. So when you stop, you still have your baseline GLP-1 activity. It is simply no longer augmented to therapeutic levels.
The metabolic adaptation problem
Weight loss itself, regardless of how it was achieved, triggers metabolic adaptation. Your body becomes more efficient, burning fewer calories at rest and during activity than would be predicted based on your new weight alone. This phenomenon, sometimes called "metabolic adaptation" or "adaptive thermogenesis," is well-documented in weight loss research and affects everyone who loses significant amounts of weight.
On tirzepatide, this metabolic adaptation is partially offset by the medication continued effects on insulin sensitivity, energy expenditure, and appetite regulation. When you stop, the full weight of metabolic adaptation hits you without pharmaceutical buffering. Your resting metabolic rate may be 100 to 300 calories per day lower than expected for someone of your current weight who never lost weight. That deficit, small as it sounds daily, compounds to significant weight regain over months if calorie intake is not carefully managed.
This is why people who have lost 50 pounds on tirzepatide cannot simply eat what a person who naturally weighs their current weight eats. Their metabolism is running at a discount. The body remembers its previous weight and, in many biological respects, is working to return to it. Understanding this reality is essential for anyone considering cold turkey discontinuation.
The science behind tirzepatide clearance
Understanding how tirzepatide leaves your body helps explain why the effects do not vanish overnight, and why the changes that follow are so predictable.
Tirzepatide has a half-life of approximately five days. That means five days after your last injection, roughly half the medication remains in your bloodstream. After 10 days, about a quarter remains. After 15 days, roughly an eighth. Complete clearance, the point at which the drug is functionally eliminated from your system, takes approximately 25 to 30 days.
This extended half-life is actually a double-edged sword when it comes to stopping. On one hand, it means the transition is gradual rather than sudden. You are not going from full therapeutic effect to zero overnight. On the other hand, it creates a deceptive window where everything feels fine, your appetite is still controlled, your weight is stable, and you might think stopping was no big deal. Then week three arrives and the real changes begin.
How tirzepatide differs from other GLP-1 medications
Not all GLP-1 receptor agonists behave identically when discontinued. Semaglutide, for comparison, has a half-life of about seven days, meaning it lingers slightly longer. People who have stopped semaglutide cold turkey report similar patterns but sometimes on a slightly extended timeline. The semaglutide withdrawal experience shares many features with tirzepatide discontinuation, though the dual receptor activity of tirzepatide means some effects may be more pronounced.
The side effect profiles differ between the two medications as well, which means the recovery experience after stopping also differs. Tirzepatide users who experienced more headaches or body aches on the medication may find faster relief after stopping. Those who benefited from stronger appetite suppression may notice a more dramatic return of hunger.
If you are considering switching from tirzepatide to semaglutide rather than stopping entirely, the conversion charts can help determine equivalent dosing. This is a fundamentally different decision from stopping cold turkey, and one that preserves many of the therapeutic benefits while changing the specific medication.
Week-by-week timeline after stopping tirzepatide
Knowing what to expect removes the element of surprise. Here is a detailed breakdown of what most people experience after their last tirzepatide injection, based on the medication half-life, clinical data, and documented patient experiences.
Week 1: the quiet period
Very little changes. Tirzepatide levels are still high enough to maintain most therapeutic effects. Appetite remains suppressed. Food choices still feel manageable. Weight stays stable. You might wonder what all the fuss was about.
Do not let this fool you.
This is the half-life working in your favor. Approximately 50% of the medication remains active. Your body has not yet registered that resupply is not coming. Use this week wisely. Establish the habits and structures that will support you once the medication fully clears.
Week 2: the first signs
Around day 10, subtle changes emerge. Hunger between meals increases slightly. You might find yourself snacking when you previously did not feel the need. Meals that used to keep you satisfied for five or six hours now leave you thinking about food after three or four. These changes are mild but noticeable if you are paying attention.
Gastrointestinal side effects from the medication, if you had any, start improving. Dry mouth resolves. Anxiety that may have been medication-related begins to ease.
Weeks 3-4: the transition
"Food noise" returns in earnest. This is when most people feel the most dramatic shift. The mental quiet that tirzepatide provided around food decisions is gone. Cravings for specific foods, particularly high-calorie and high-carbohydrate options, become more frequent and more intense. The persistent hunger that the medication was designed to address comes back, and it often feels stronger than before simply because of the contrast with how things felt on the medication.
This is also when emotional eating patterns tend to resurface. Food becomes comforting again in ways it had not been while on the medication. Stress, boredom, loneliness, celebration, all the emotional triggers that drive eating independent of physical hunger, return to their pre-treatment intensity. People who did not address these patterns during treatment often find this the most challenging aspect of discontinuation.
If you were taking your injections at a specific time of day or on a particular day of the week, those routine markers can trigger awareness of the medication absence. Some people find it helpful to replace the injection routine with a different health-supporting habit, like a weekly meal prep session or a specific workout, to maintain the sense of structure.
By the end of week four, tirzepatide is essentially cleared from your system. You are operating without pharmacological support for the first time in however long you were on the medication.
Weeks 5-8: the new normal
Your body has fully adjusted to life without tirzepatide. Appetite has settled at its pre-medication baseline, or close to it. For some people, appetite actually feels stronger than it was before starting tirzepatide, though research suggests this is more perception than reality. After months of reduced appetite, normal hunger signals feel overwhelming by comparison.
Weight changes become measurable. The scale starts moving in the wrong direction for many people. How much and how fast depends on multiple factors: how much weight you lost on the medication, how long you were on it, your diet plan, your exercise habits, and your individual metabolic profile.
Months 3-6: the critical window
This is where the SURMOUNT-4 data becomes most relevant. The trajectory established in these months often determines long-term outcomes. People who have built strong nutritional habits, maintained consistent exercise, and addressed the behavioral components of weight management tend to retain more of their weight loss. Those who relied primarily on the medication for appetite control without building supporting habits tend to see more substantial regain.
The strategies for maintaining weight loss after tirzepatide become absolutely critical during this period.
Weight regain: what the SURMOUNT-4 trial reveals
The SURMOUNT-4 trial is the definitive study on tirzepatide discontinuation outcomes, and its findings are sobering.
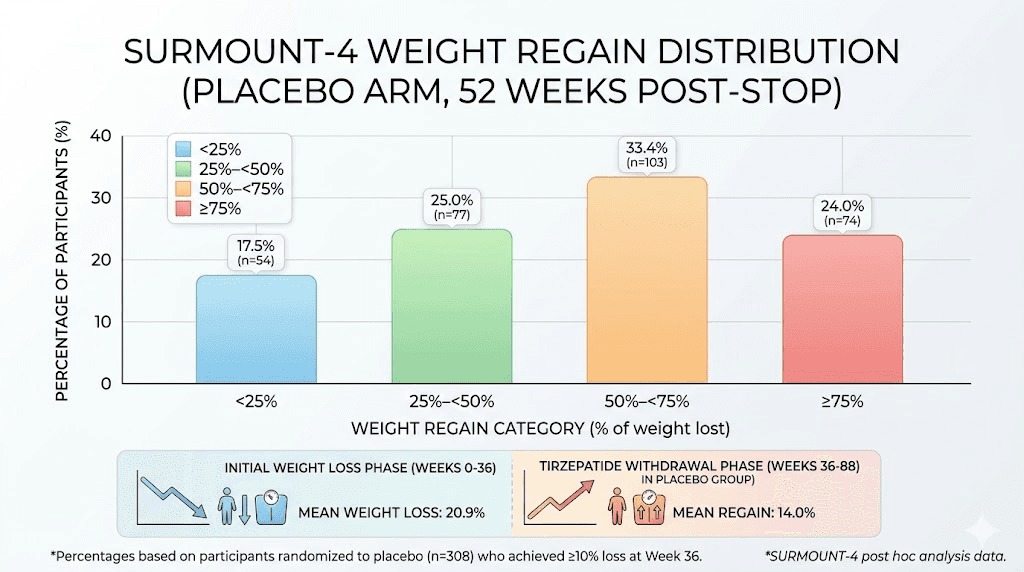
Here is the study design. Adults with obesity achieved at least 10% body weight reduction over 36 weeks of tirzepatide treatment. They were then randomized: some continued the medication, others switched to placebo (effectively stopping cold turkey under controlled conditions). Both groups were followed for an additional 52 weeks.
The results tell a clear story.
Among those who stopped tirzepatide, 82.5% regained at least 25% of the weight they had initially lost. The breakdown was even more revealing: 77 participants regained 25% to less than 50% of their lost weight. 103 participants regained 50% to less than 75%. And 74 participants regained 75% or more of the weight they had worked so hard to lose.
Only 54 out of 308 participants managed to keep their weight regain below 25%.
That last number is the important one. It means roughly 17.5% of people who stopped tirzepatide maintained most of their results. They exist. It is possible. But they are the exception, not the rule.
What separated the 17.5% from the rest
The trial data, combined with post-hoc analyses, suggests several factors that predicted better outcomes after discontinuation:
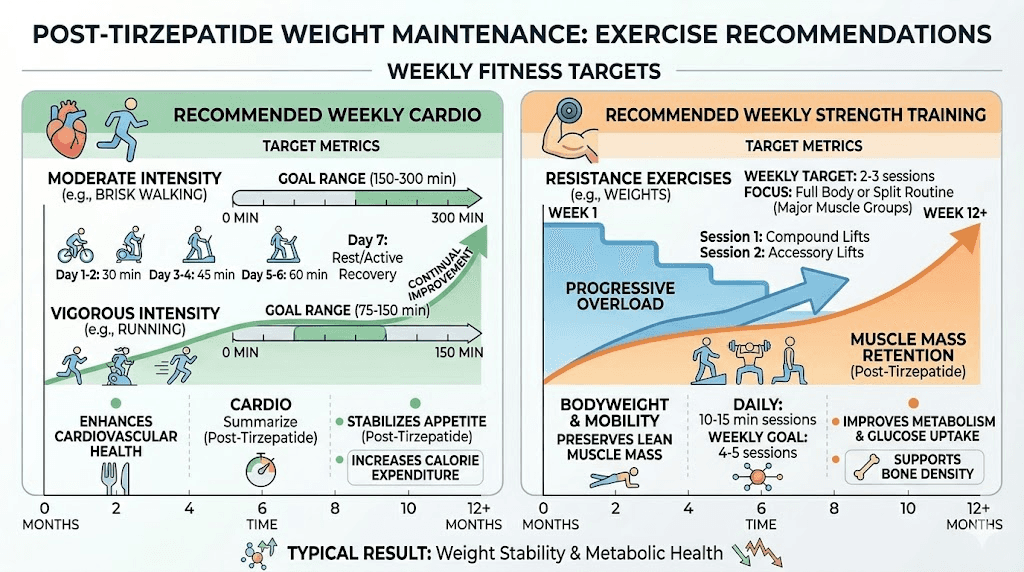
Physical activity levels. Participants who maintained higher levels of exercise, particularly resistance training combined with aerobic activity, retained more weight loss. The American College of Sports Medicine recommends 200 to 300 minutes of moderate-intensity activity weekly for weight loss maintenance. That is significantly more than the 150 minutes recommended for general health.
Dietary adherence. Those who maintained structured meal plans with adequate protein intake (1.2 to 1.6 grams per kilogram of body weight daily) fared better. Protein shakes formulated for GLP-1 users can help hit these targets. Fiber supplementation also appeared to support satiety after medication cessation.
Duration on medication before stopping. Interestingly, there is some evidence that the length of time spent on tirzepatide before discontinuation may influence outcomes, though this remains an active area of research.
Cardiometabolic consequences of weight regain
Weight regain after stopping tirzepatide does not just affect the number on the scale. A post-hoc analysis of the SURMOUNT-4 data, published in JAMA Internal Medicine, found that weight regain was associated with reversal of cardiometabolic improvements. Waist circumference increased. Triglycerides rose. Non-HDL cholesterol worsened. Fasting insulin levels climbed. HOMA2-IR, a measure of insulin resistance, deteriorated.
The one encouraging finding: participants who kept their regain below 25% did not show significant worsening of these markers. Their waist circumference, lipid profiles, and insulin sensitivity remained relatively stable despite stopping the medication. This reinforces the idea that partial maintenance, even if you regain some weight, still provides meaningful health benefits compared to full regain.
Does stopping tirzepatide cause withdrawal symptoms
No. Not in the clinical sense of the word.
Withdrawal, in medical terminology, refers to a specific set of symptoms that occur when a drug the body has become physiologically dependent on is suddenly removed. Benzodiazepine withdrawal can cause seizures. Opioid withdrawal causes intense physical symptoms. Alcohol withdrawal can be life-threatening. Tirzepatide causes none of these.
There is no evidence that tirzepatide creates physical dependence. No documented withdrawal syndrome. No rebound effects that are medically dangerous. The FDA does not require tapering, and emergency departments do not see patients in tirzepatide withdrawal.
However.
The changes that follow discontinuation can feel like withdrawal to the person experiencing them. The return of intense hunger after months of easy appetite control. The psychological shift of losing that food decision support. The creeping weight gain that feels relentless. These are real experiences. They are just not withdrawal in the pharmacological definition.
Some people report specific symptoms after stopping:
Increased appetite and food cravings. This is the most universal experience. It is not a rebound effect but rather the removal of active appetite suppression, combined with the psychological contrast of remembering how things felt on the medication.
Mood changes. Some users report irritability or mild mood shifts, though it is difficult to separate this from the frustration of dealing with returned hunger and potential weight gain.
Digestive changes. As gastric emptying normalizes, some people experience temporary digestive shifts. These typically resolve within one to two weeks.
Fatigue. Some people who experienced fatigue on tirzepatide find it resolves after stopping, while others who felt energized on the medication report decreased energy levels once it clears. GLP-1 related fatigue is a complex topic that varies significantly between individuals.
Cold turkey vs tapering: which approach is safer
This is the central question, and the answer depends on what you mean by "safer."
From a medical safety standpoint, stopping cold turkey is not dangerous. There is no risk of a medical emergency. Your body will adjust. You will not need emergency intervention.
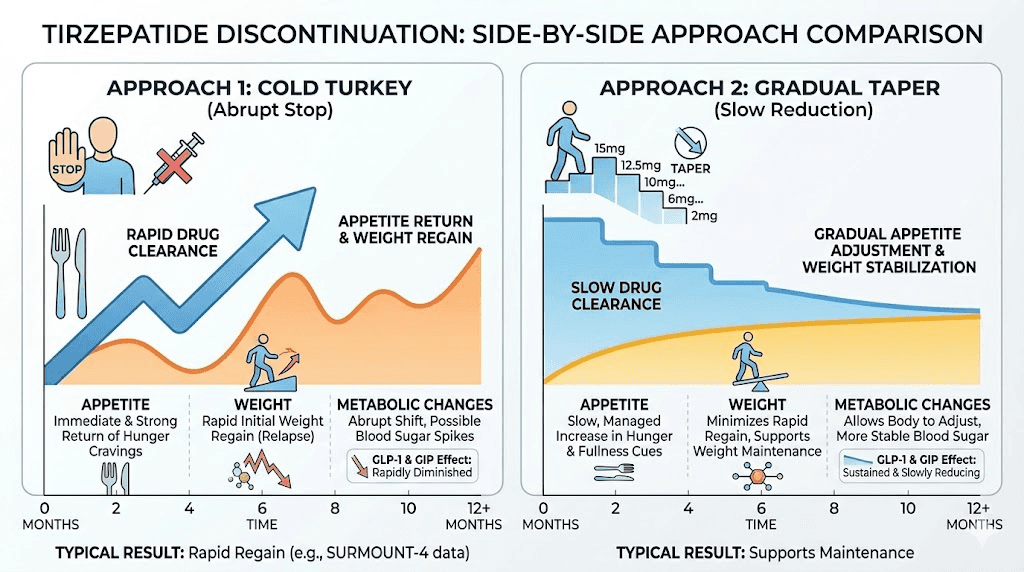
From an outcome standpoint, tapering appears to produce better results for weight maintenance. And this is where the distinction matters most for the majority of people considering discontinuation.
The case for cold turkey
Some situations make abrupt discontinuation the practical choice:
Cost constraints. If you can no longer afford the medication and have no access to affordable tirzepatide options or cheaper compounded alternatives, a gradual taper may not be financially feasible. In this case, stopping is stopping, regardless of how you frame it.
Side effect intolerance. If you are experiencing severe muscle pain, persistent joint pain, or other side effects that significantly impact quality of life, your healthcare provider may recommend immediate discontinuation rather than prolonged exposure at lower doses.
Medical necessity. Certain situations, such as pregnancy, upcoming surgery, or newly discovered contraindications, may require stopping without the luxury of a taper period.
Personal choice. Some people simply prefer a clean break. They want to know exactly when they stopped and deal with the consequences directly rather than dragging out the process over weeks or months. There is something psychologically appealing about drawing a clear line between "on medication" and "managing independently." If that mindset motivates better adherence to maintenance strategies, the psychological benefit of a clean break may outweigh the physiological advantage of tapering.
Travel or lifestyle changes. Extended international travel, particularly to locations where traveling with tirzepatide presents logistical challenges around refrigeration and customs, sometimes makes temporary discontinuation practical. Similarly, major life transitions like relocations, career changes, or relationship upheavals can disrupt the consistency required for ongoing injection therapy.
The case for tapering
The evidence, while limited, favors gradual discontinuation for several reasons:
Appetite adjustment. Tapering allows your body to gradually recalibrate its hunger signals rather than experiencing a sudden shift. At each reduced dose level, you can develop coping strategies for the incrementally increased appetite before reducing further.
Behavioral adaptation. Each step down gives you a window to test and refine the habits that will need to carry the load once the medication is completely gone. You discover which meal timing works, which supplements help with satiety, and which exercise patterns manage hunger most effectively.
Psychological preparation. The gradual nature of tapering allows for mental adjustment. Rather than waking up one day without the support you have relied on, you ease into increasing self-reliance.
Evidence from clinical experience. While there are no large randomized trials specifically comparing cold turkey to tapering for tirzepatide, clinicians who work with these medications consistently report better outcomes with gradual discontinuation. Patients who taper tend to maintain more of their weight loss compared to those who stop abruptly.
The complete guide to weaning off tirzepatide covers tapering strategies in detail.
How to taper off tirzepatide properly
If you decide that gradual discontinuation is the right approach, here is what an evidence-informed taper looks like.
The standard step-down protocol
The general approach is to reduce your dose every two to four weeks, staying at each new dose level until your appetite, energy, and weight feel stable before reducing further. This is not a race. Rushing the taper defeats the purpose.
If you are currently on 15 mg, a typical taper might look like this:
Step 1: Reduce to 10 mg. Stay here for two to four weeks. Monitor your appetite, weight, and energy levels daily. Use the tirzepatide unit conversion guides to ensure accurate dosing during the transition. Your dosage calculator can help determine the exact syringe measurements needed.
Step 2: Reduce to 7.5 mg. Another two to four weeks. This is often where people notice the first real change in appetite, because you are now below the dose that was providing full therapeutic effect. Adjust your meal plan to emphasize protein and fiber.
Step 3: Reduce to 5 mg. Two to four more weeks. At this dose, the appetite suppression effect is noticeably reduced. This is a critical period for solidifying the habits that will support you post-medication.
Step 4: Reduce to 2.5 mg. The standard starting dose becomes your final step. Two to four weeks here, and then discontinuation.
Optional extension: Some people benefit from dropping to 2.5 mg every other week, or even every two weeks, before stopping entirely. This ultra-low-dose approach provides a gentler transition but extends the total taper time significantly.
The microdosing approach
An alternative gaining attention is the microdosing approach. Rather than following the standard dose tiers, some people reduce to very small doses, well below the standard 2.5 mg minimum. The microdosing tirzepatide chart provides guidance on sub-therapeutic doses that may still provide partial appetite support. The microdose schedule typically involves weekly injections at 0.5 to 1.5 mg, doses that would be insufficient for initial weight loss but may help maintain results during the transition off medication.
This approach has theoretical appeal but limited clinical evidence. It is worth discussing with your healthcare provider, particularly if you have had success with lower doses in the past.
Adjusting injection frequency instead of dose
Another strategy is keeping the same dose but extending the interval between injections. If you normally inject weekly, you might try injecting every 10 days, then every two weeks, then every three weeks, before stopping. Some people find this approach more manageable because each individual injection still provides a meaningful therapeutic effect, just spread further apart. Splitting your dose across the week is another variation, though this is more commonly used for managing side effects than for tapering.
Protecting your weight loss after stopping tirzepatide
Whether you stop cold turkey or taper gradually, the strategies for preserving your results are the same. The difference is that tapering gives you more time to implement them before the medication fully clears.
Protein: your most important macronutrient
Research consistently identifies adequate protein intake as the single most important dietary factor for weight loss maintenance. The target is 1.2 to 1.6 grams per kilogram of body weight daily. For a 180-pound person, that translates to approximately 98 to 131 grams of protein per day.
Why protein matters so much after stopping tirzepatide:
It is the most satiating macronutrient. Protein keeps you fuller longer than equivalent calories from carbohydrates or fat. When tirzepatide is no longer providing pharmacological appetite suppression, dietary protein becomes your primary tool for managing hunger between meals.
It preserves muscle mass. Weight loss, whether on medication or not, always includes some loss of lean tissue. Adequate protein minimizes this, which is critical because muscle mass drives metabolic rate. Losing muscle means burning fewer calories at rest, which accelerates weight regain.
It requires more energy to digest. The thermic effect of protein, the energy your body uses to process it, is roughly 20 to 30% of the calories consumed. This means eating 100 calories of protein costs your body 20 to 30 calories just to digest it, compared to only 5 to 10 calories for carbohydrates and 0 to 3 calories for fat.
Practical sources: lean meats, fish, eggs, Greek yogurt, cottage cheese, legumes, and protein shakes designed for GLP-1 users. The specific foods that work best during GLP-1 treatment often remain your best choices after stopping as well.
Exercise: non-negotiable for maintenance
Exercise serves multiple critical functions after tirzepatide discontinuation. It helps manage appetite. It preserves muscle mass. It improves insulin sensitivity independently of the medication. And one study found that participants who exercised four times per week while on a GLP-1 medication maintained their weight loss for a full year after stopping.
The evidence-based recommendations:
Aerobic activity: 200 to 300 minutes per week of moderate-intensity cardio. Walking counts. So does cycling, swimming, elliptical training, or any activity that elevates your heart rate consistently. This is more than the general health recommendation of 150 minutes, and there is a reason for that. Weight loss maintenance requires more movement than prevention.
Resistance training: At least two sessions per week targeting all major muscle groups. This is not optional. Muscle mass is your metabolic insurance policy. Every pound of muscle burns approximately 6 to 7 calories per day at rest. That might sound small, but the cumulative effect of maintaining 10 to 15 extra pounds of lean tissue is significant over months and years.
Daily movement: Beyond structured exercise, non-exercise activity thermogenesis (NEAT), the calories burned through fidgeting, walking, standing, and general daily movement, plays a surprisingly large role in total energy expenditure. People who maintain weight loss tend to be more active throughout their day, not just during workouts.
Fiber and meal structure
Fiber acts as a natural appetite suppressant. It slows gastric emptying (partially replicating one of tirzepatide mechanisms), adds volume to meals without adding significant calories, and feeds beneficial gut bacteria that influence satiety signaling. The target is 25 to 35 grams daily from whole food sources: vegetables, fruits, legumes, whole grains.
Fiber supplements designed for GLP-1 users can help bridge the gap if whole food intake falls short, though whole food sources are always preferable.
Meal timing also matters. Eating at consistent times helps regulate hunger hormones. Front-loading calories earlier in the day, a larger breakfast and lunch with a lighter dinner, aligns with circadian biology and may support better weight maintenance. Your tirzepatide diet plan can be adapted for post-medication use by keeping the protein-heavy structure while gradually increasing total calories to a maintenance level.
Sleep and stress management
Sleep deprivation increases ghrelin (the hunger hormone), decreases leptin (the satiety hormone), and impairs decision-making around food. Seven to nine hours of quality sleep is not a luxury recommendation. It is a physiological necessity for weight maintenance. If insomnia was an issue on tirzepatide, the good news is that sleep quality often improves after discontinuation.
Chronic stress elevates cortisol, which promotes fat storage, particularly visceral fat, and increases cravings for calorie-dense foods. Stress management, whether through meditation, exercise, therapy, or other approaches, directly supports weight maintenance.
Supplements that support the transition
While no supplement replaces the effect of tirzepatide, several may provide modest support during the transition. Key supplements to consider include:
Fiber supplements for satiety support. Probiotics for gut health, particularly those formulated for GLP-1 users. Magnesium for sleep quality and stress management. Omega-3 fatty acids for their anti-inflammatory effects and potential metabolic benefits. Berberine, which some research suggests has modest effects on blood sugar regulation, though you should discuss this with your healthcare provider, especially if you are already taking metformin or other glucose-lowering medications.
When stopping tirzepatide makes sense
Discontinuation is not always a negative event. There are several legitimate and even positive reasons to consider stopping.
You have reached your goal weight
If you have achieved your target weight loss results and want to attempt maintaining them without medication, stopping is a reasonable next step. The key word is "attempt." Go in with eyes open about the statistics, a solid maintenance plan in place, and a willingness to restart if needed.
Side effects outweigh benefits
For some people, the gastrointestinal effects never fully resolve. Persistent headaches, chronic bloating, unmanageable constipation, or muscle pain that does not improve with dose adjustment may make continued use untenable. Quality of life matters, and a medication that makes you miserable is not serving its purpose regardless of the weight loss it provides.
Financial considerations
The cost of tirzepatide is substantial. Even with more affordable compounded options, the ongoing expense is significant. If the medication is creating financial stress, that stress itself can undermine health goals. Stopping, implementing the maintenance strategies above, and potentially restarting later if budget allows is a pragmatic approach.
Pregnancy planning
Tirzepatide is not approved for use during pregnancy. If you are planning to conceive or have become pregnant, discontinuation is necessary. The same applies if you are breastfeeding or plan to breastfeed.
Transitioning to a different approach
Some people stop tirzepatide not because they are giving up on pharmacological support, but because they are switching to something else. Alternatives to tirzepatide include semaglutide, retatrutide, and other emerging options. The three-way comparison between the major GLP-1 options can help inform this decision. Phentermine is another option some people consider, though it works through a completely different mechanism.
What to do if you need to restart tirzepatide
Here is the reality that the cold turkey crowd needs to hear: restarting is always an option, and there is no shame in it.
Weight management for many people is a chronic condition that benefits from ongoing treatment, just like hypertension, diabetes, or depression. No one criticizes a person with high blood pressure for continuing to take their medication. The same principle applies here.
Restarting after a break
If you stopped tirzepatide and weight regain has become significant, restarting is straightforward but requires attention to dosing. You should not resume at your previous dose. The standard recommendation is to restart at the initial starting dose of 2.5 mg and titrate back up following the same escalation schedule you used initially.
Why? Two reasons. First, gastrointestinal tolerance diminishes during the break. Jumping back to a high dose will likely cause significant nausea, vomiting, and other GI effects. Second, gradual re-titration allows your body to readjust to the medication effects progressively, producing a smoother and more comfortable restart.
The first dose experience will likely mirror your initial start, though some people find the gastrointestinal effects are more predictable the second time around simply because they know what to expect.
The maintenance dose approach
Rather than stopping entirely, some healthcare providers recommend transitioning to a lower maintenance dose. Instead of the full therapeutic dose that drove weight loss, you continue on a reduced dose that provides partial appetite support at lower cost and with fewer side effects. This is a middle ground between cold turkey and full-dose continuation.
The microdosing protocol is one version of this approach. The standard dosing guidelines provide the therapeutic range, but maintenance dosing often falls below these targets. The unit-based dosing charts make it easier to calculate these sub-standard doses accurately. Working with your dosage calculator ensures precision at every step of the taper.
The appeal of maintenance dosing is significant. It costs less than full-dose treatment. Side effects are minimal or absent at lower doses. And the partial appetite support, while not as robust as full therapeutic dosing, may be enough to prevent the kind of weight regain documented in the SURMOUNT-4 trial. Some clinicians compare it to a maintenance dose of an antidepressant: you may not need the full therapeutic dose once you have achieved stability, but some pharmacological support prevents relapse.
If you are using compounded tirzepatide with B12 or other compound formulations with glycine and B12, discuss with your compounding pharmacy whether lower-concentration vials are available for maintenance dosing. This avoids the inaccuracy of trying to draw extremely small volumes from high-concentration vials.
Switching medications instead of stopping
If cost is the primary driver for stopping, switching to semaglutide may provide continued benefits at a different price point. The dosage conversion chart helps ensure an appropriate transition dose. Retatrutide is another option for those interested in triple-receptor agonists. Ultimately, the comparison between these medications should involve your healthcare provider to determine the best fit.
Some people also explore oral tirzepatide options or tirzepatide drops as alternatives to injectable forms. The comparison between oral and injectable delivery methods shows different bioavailability profiles, which may allow for continued treatment at reduced cost or greater convenience. Tablet formulations are another emerging option, though availability varies.
The decision tree looks something like this. Can you afford to continue on any form of tirzepatide? If yes, consider adjusting your dose downward for maintenance rather than stopping. If not, can you afford a different GLP-1 medication? If yes, the conversion charts guide the switch. Semaglutide may or may not provide the same level of efficacy, but it maintains pharmacological support. If no medication is financially feasible, then and only then should cold turkey discontinuation be the plan, with all the maintenance strategies discussed in this guide implemented aggressively.
One additional consideration: retatrutide pricing may offer a different cost structure as the market evolves. The three-way comparison between semaglutide, tirzepatide, and retatrutide provides a comprehensive overview of how these medications differ in efficacy, side effects, and mechanism. Even if you cannot continue tirzepatide specifically, staying within the GLP-1 agonist family of medications provides substantially better outcomes than stopping pharmacological support entirely.
Special considerations for different populations
Type 2 diabetes patients
Stopping tirzepatide cold turkey when you have type 2 diabetes carries additional considerations beyond weight management. Blood glucose control will deteriorate as the medication clears. If you are not on other glucose-lowering medications, blood sugar spikes can become significant. If you are on other medications, dosage adjustments may be needed as tirzepatide effects wane. Close monitoring of blood glucose for at least four to six weeks after discontinuation is essential, and this decision should always involve your endocrinologist or prescribing physician.
People on combination therapy
If you are taking tirzepatide alongside other medications, whether phentermine, metformin, or other treatments, stopping tirzepatide requires a comprehensive medication review. Drug interactions change when one component is removed. Doses of remaining medications may need adjustment.
Long-term users
People who have been on tirzepatide for a year or more may have a more significant adjustment period compared to those who used it for only a few months. The body has had more time to adapt to the presence of the medication, and the habits of eating with pharmacological appetite support are more deeply ingrained. These individuals may benefit most from a slower, more deliberate taper.
People with a history of weight cycling
If you have a history of repeated weight loss and regain (sometimes called "yo-yo dieting"), your body may be more efficient at regaining weight after tirzepatide discontinuation. Research suggests that each cycle of loss and regain can make subsequent weight loss harder and regain faster. This does not mean stopping is impossible, but it does mean the maintenance strategy needs to be more aggressive and the decision to stop should be made carefully.
The role of body composition in discontinuation outcomes
Not everyone who stops tirzepatide has the same experience, and body composition plays a larger role than most people realize.
Muscle mass as metabolic insurance
People who maintained or built muscle during their tirzepatide treatment have a significant advantage when stopping. Every pound of lean muscle tissue burns approximately 6 to 7 calories per day at rest, but the indirect metabolic effects are even larger. Muscle tissue improves insulin sensitivity, increases glucose disposal, and raises non-resting energy expenditure during daily activities. A person who lost 40 pounds but preserved their muscle mass is in a fundamentally different metabolic position than someone who lost 40 pounds but lost 10 of those pounds from muscle.
This is why resistance training is not just recommended but essential, both during treatment and after stopping. The peptides that support muscle growth and the best peptides for weight loss are relevant considerations for people who want to optimize their body composition during and after GLP-1 treatment.
Where you carry your remaining fat matters
Visceral fat, the metabolically active fat surrounding your organs, responds differently to tirzepatide discontinuation than subcutaneous fat. Research suggests that visceral fat loss may be partially preserved even after stopping GLP-1 medications, particularly if exercise is maintained. This is encouraging because visceral fat is the type most strongly associated with metabolic disease, cardiovascular risk, and insulin resistance.
Subcutaneous fat, the kind you can pinch, tends to return more readily. This means the scale might move upward while some of the most important health-related fat loss is preserved. Waist circumference measurements can be a more meaningful tracking metric than body weight alone during the post-discontinuation period.
Age-related considerations
Older adults who stop tirzepatide face additional challenges. Metabolic rate naturally declines with age. Muscle loss accelerates. Hormonal changes affect fat distribution and appetite regulation independently of any medication effects. For people over 50 who are considering discontinuation, the exercise and protein recommendations become even more critical. The peptide protocols for women over 40 and related resources address some of these age-related considerations.
Sarcopenia, the age-related loss of muscle mass, combines with weight-loss-induced muscle loss to create a compounding problem. An older adult who stops tirzepatide without maintaining a robust resistance training program may find their metabolic rate drops further than expected, accelerating weight regain beyond what younger individuals experience.
Understanding the set point theory and tirzepatide
The concept of a body weight "set point" helps explain why maintaining weight loss after stopping tirzepatide is so challenging. Your body has a weight range that it defends through multiple feedback mechanisms. Hormonal signals, metabolic adjustments, appetite changes, and even behavioral drives all work to return your weight to this defended range after perturbation.
Tirzepatide, while active in your system, effectively lowers this defended weight by altering the hormonal and neural signals that maintain the set point. Your body adapts to a new, lower weight while on the medication. But when the medication is removed, the original set point defense mechanisms reactivate. This is not a flaw in the medication. It is a fundamental aspect of how the human body regulates weight.
Some researchers believe that prolonged treatment, staying on tirzepatide or similar medications for years rather than months, may gradually shift the set point downward in a more permanent way. This is one argument for considering tirzepatide as long-term or indefinite treatment rather than a short-term intervention with planned discontinuation. The data on this is still evolving, but it adds important context to any decision about stopping.
The question of how long to stay on GLP-1 medications is central to this discussion. There is growing consensus in the medical community that obesity, like hypertension or diabetes, may require ongoing pharmacological management for many people. Stopping the medication is not failure. But understanding that it may require restarting is part of making an informed decision.
Real-world discontinuation patterns
Clinical trial data tells one story. Real-world experiences add nuance.
The planned discontinuation
People who plan their discontinuation, setting a date, building habits in advance, establishing monitoring systems, and having a restart threshold, consistently report better outcomes than those who stop impulsively. The act of planning itself creates accountability and structure that supports maintenance.
A common successful pattern: reach goal weight, maintain on medication for an additional three to six months to allow habits to solidify, then begin a gradual taper while intensifying exercise and dietary structure. This "stabilization plus taper" approach gives the best chance at long-term maintenance.
The forced discontinuation
Insurance changes, supply shortages, cost increases, and medication expiration sometimes force unplanned discontinuation. These situations are stressful and often produce worse outcomes because the preparation phase is compressed or eliminated. If you find yourself in this situation, prioritize the basics: protein intake, exercise, and weight monitoring. Accept that some regain is likely and focus on minimizing rather than preventing it.
Storage issues can also force unexpected discontinuation. If your medication was improperly stored or you are unsure about the remaining shelf life of refrigerated tirzepatide, you may need to make sudden decisions about continuing treatment. The shelf life guide helps with these determinations.
The gradual drift
Perhaps the most common real-world pattern is the unintentional drift away from medication. You miss one injection because life got busy. Then another because refilling the prescription slipped your mind. Before you know it, you have been off the medication for three weeks without ever making a conscious decision to stop. This unplanned cold turkey scenario often produces the worst outcomes because it comes with zero preparation, zero planning, and often zero monitoring until significant regain has already occurred.
If you recognize this pattern, treating it as a wake-up call rather than a failure is productive. Resume the medication if you can. If you cannot, immediately implement the maintenance strategies outlined earlier. The sooner you take deliberate action, the better your outcomes.
Common mistakes when stopping tirzepatide cold turkey
Understanding what goes wrong helps you avoid the same pitfalls.
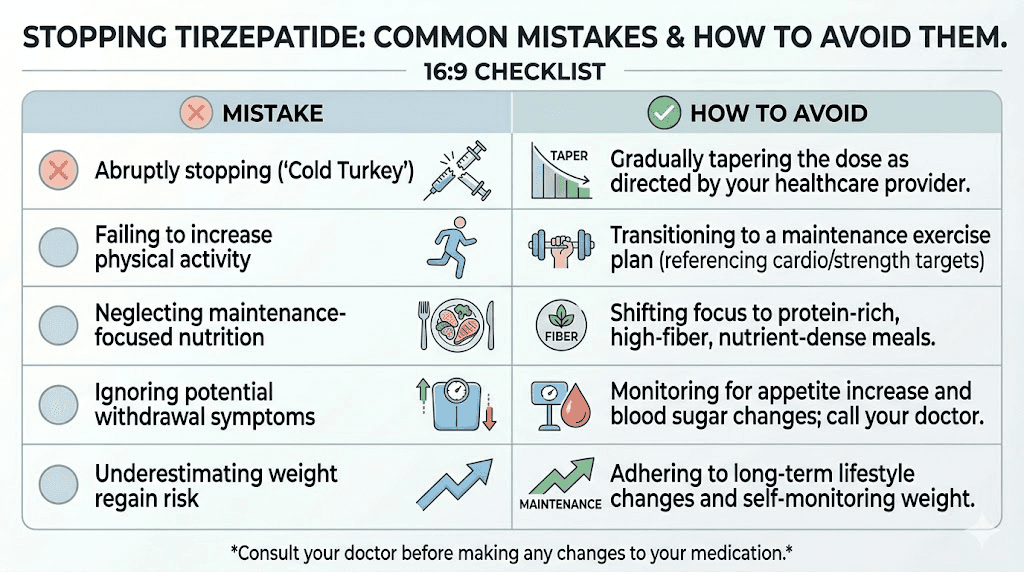
Mistake 1: no plan in place
The single biggest predictor of weight regain is stopping without a comprehensive maintenance plan. This means stopping the injections without having established your calorie targets, meal prep routines, exercise schedule, and accountability systems. The medication was doing heavy lifting. Something needs to replace that support.
Mistake 2: assuming willpower will be enough
Willpower is a limited resource. The appetite changes after stopping tirzepatide are biological, driven by hormones and neurotransmitter shifts, not character flaws. Planning to "just eat less" without structural support is setting yourself up for exactly the kind of regain the studies document.
Mistake 3: ignoring the scale
Some people stop weighing themselves after discontinuation, either because they are afraid of what they will see or because they want to focus on "how they feel." But regular monitoring, at least weekly, provides early warning signals. A two-pound increase in a week can be addressed with minor adjustments. A twenty-pound increase discovered months later requires starting over from scratch.
Mistake 4: cutting calories too aggressively
In an attempt to prevent weight regain without the medication, some people drastically restrict calories. This backfires. Severe caloric restriction triggers metabolic adaptation (your body reduces its energy expenditure in response to low food intake), increases muscle loss, amplifies hunger hormones, and ultimately makes weight regain more likely and more severe when the restriction inevitably breaks.
Mistake 5: not having a restart threshold
Before stopping, establish a clear weight threshold at which you will restart the medication. For example, "If I regain more than 10 pounds, I will contact my provider about restarting." Having this predetermined removes the emotional decision-making from the equation and prevents the kind of gradual, unchecked regain that leads to full reversal of progress.
Building your discontinuation plan
Whether you stop cold turkey or taper, the preparation is the same. Start building this plan at least four weeks before your intended last injection.
Phase 1: assessment (weeks 4-3 before stopping)
Calculate your current daily calorie needs using the total daily energy expenditure formula. Track your actual food intake for one week to see where you stand. Determine your protein intake, your current activity level, your sleep patterns, and your stress management practices. This is your baseline. Every gap you identify now is one you can close before the medication support disappears.
Review your current diet plan and decide what needs to change for maintenance. The calorie deficit you needed for weight loss is different from the calorie balance you need for maintenance. Calculate the adjustment now.
Phase 2: habit building (weeks 3-1 before stopping)
Establish your exercise routine at the maintenance level (200 to 300 minutes of cardio, two to three resistance sessions per week) while you still have medication support. Starting a new exercise program while simultaneously losing appetite suppression is much harder than maintaining one you have already built.
Master four to five high-protein meal prep recipes that you enjoy and can prepare quickly. Stock your kitchen. Remove food triggers. Set up your environment for success.
Phase 3: discontinuation and monitoring (weeks 1-8 after stopping)
Weigh yourself daily at the same time. Track your food intake. Monitor your hunger levels on a 1-to-10 scale. Note your energy, mood, and sleep quality. This data helps you identify problems early and make targeted adjustments rather than waiting until changes become overwhelming.
Schedule check-ins with your healthcare provider at weeks two, four, and eight. If you have type 2 diabetes, more frequent monitoring may be needed for blood glucose.
Phase 4: long-term maintenance (month 3 onward)
Transition from daily tracking to weekly monitoring. Continue exercise at maintenance levels. Maintain protein targets. Stay engaged with whatever accountability system works for you, whether that is a SeekPeptides membership community, a support group, a nutritionist, or a training partner.
For researchers serious about maintaining their results after tirzepatide discontinuation, SeekPeptides offers evidence-based protocols, maintenance planning tools, and a community of experienced individuals who have navigated this exact transition. The combination of structured guidance and peer support can make the difference between the 17.5% who maintain their results and the 82.5% who do not.
Monitoring your health after stopping tirzepatide
Whether you stop cold turkey or taper, monitoring is not optional. It is the early warning system that prevents small problems from becoming big ones.
Weight tracking protocol
Weigh yourself daily, at the same time, under the same conditions (morning, after bathroom, before eating). Daily weigh-ins provide more useful data than weekly ones because they reveal the trend beneath normal day-to-day fluctuations. A three-day moving average is even more useful than individual data points. Weight can fluctuate 2 to 4 pounds daily due to water retention, sodium intake, and bowel contents. Looking at the trend over weeks tells you what is actually happening with fat mass.
Set a clear "action threshold." A common approach is the 5-pound rule: if the three-day average exceeds your target weight by 5 pounds, implement corrective measures immediately. A 10-pound threshold triggers discussion with your healthcare provider about restarting medication. Having these numbers predetermined removes the emotional negotiation that leads to inaction while regain accelerates.
Blood work monitoring
For anyone who was using tirzepatide for metabolic health, blood work at specific intervals post-discontinuation provides objective data on how your body is responding. Recommended testing schedule:
Baseline (at time of last injection): Fasting glucose, HbA1c, lipid panel, fasting insulin. This gives you the "best case" numbers while medication effects are still active.
Week 6: Repeat fasting glucose and lipid panel. By this point, tirzepatide is fully cleared and you are seeing your unmedicated metabolic profile.
Month 3: Full panel including HbA1c (which reflects 3-month average blood sugar). This is the most informative check because HbA1c now reflects your post-medication glucose control.
Month 6: Repeat full panel. If numbers have worsened significantly, this is a strong signal that medication may need to be resumed.
Appetite and hunger journaling
Rating your hunger and fullness on a simple 1-to-10 scale before and after each meal creates a dataset that reveals patterns. You might discover that mornings are manageable but evenings are challenging. Or that certain foods keep you satisfied for hours while others leave you ravenous within 90 minutes. These patterns inform targeted adjustments to your meal plan and eating schedule.
Track "food noise" separately from physical hunger. Physical hunger is a body sensation. Food noise is mental, the constant thinking about food, planning meals, craving specific items. Both increase after stopping tirzepatide, but they respond to different interventions. Physical hunger responds to protein, fiber, and meal timing. Food noise responds more to behavioral strategies, distraction techniques, and environmental management.
Exercise and activity monitoring
Track both structured exercise and daily movement. A fitness tracker or pedometer provides objective data on your activity levels. Aim for a minimum of 8,000 to 10,000 steps daily in addition to structured workouts. Research suggests that people who maintain higher daily step counts after stopping weight loss medications retain more of their results, likely due to the cumulative calorie expenditure and the appetite-regulating effects of movement.
The injection site considerations become irrelevant once you stop, but the exercise routine you built around your injection schedule should continue. If you timed your injections around workouts, redirect that scheduling energy toward planning your exercise sessions with the same intentionality.
Frequently asked questions
Can I stop tirzepatide cold turkey without any medical risk?
Yes. There is no medical danger in stopping tirzepatide abruptly. Unlike medications that cause physical dependence, tirzepatide does not produce a withdrawal syndrome that requires medical intervention. However, if you have type 2 diabetes, you should coordinate with your healthcare provider to monitor blood glucose and potentially adjust other medications as tirzepatide clears your system.
How long until tirzepatide is completely out of my system?
Tirzepatide has a half-life of approximately five days, meaning it takes about 25 to 30 days for the medication to be functionally eliminated from your body. Most people begin noticing changes in appetite around days 7 to 10, with the full return of pre-medication hunger levels by weeks three to four. The complete duration guide covers this timeline in detail.
Will I gain back all the weight I lost if I stop cold turkey?
Not necessarily, but the odds are not in your favor without active effort. The SURMOUNT-4 trial found that 82.5% of participants regained at least 25% of their lost weight within a year of stopping. However, 17.5% managed to keep their regain below 25%, primarily through consistent exercise, high protein intake, and structured eating patterns. Your outcome depends largely on the maintenance habits you establish.
Is it better to taper off or stop cold turkey?
Tapering generally produces better weight maintenance outcomes because it allows your body and habits to adjust gradually. However, cold turkey is medically safe and may be the only practical option in some situations, such as cost constraints or medical necessity. The weaning guide outlines specific tapering protocols.
What dose should I restart at if I stop and then decide to go back on tirzepatide?
Always restart at the initial dose of 2.5 mg and titrate up following the standard dose escalation schedule. Jumping back to your previous dose will likely cause significant gastrointestinal side effects because your tolerance has diminished during the break.
Can I switch to semaglutide instead of stopping entirely?
Yes. Switching from tirzepatide to semaglutide is a common approach for people who want to continue pharmacological support with a different medication. Use the conversion chart to determine the appropriate starting dose for the new medication.
Will stopping tirzepatide affect my period?
Some women notice changes in their menstrual cycle after stopping tirzepatide, just as some experienced period changes while on the medication. Rapid weight changes, whether loss or regain, can affect hormonal balance and menstrual regularity. These changes typically normalize within two to three cycles.
Can microdosing tirzepatide help maintain weight loss better than stopping completely?
There is growing interest in microdosing tirzepatide as a maintenance strategy. The theory is that very low doses, below the standard therapeutic range, may provide partial appetite support at lower cost and with fewer side effects. While clinical evidence is limited, some practitioners report success with this approach. The microdosing chart provides dosing guidance for this strategy.
External resources
SURMOUNT-4 Trial: Continued Treatment With Tirzepatide for Maintenance of Weight Reduction (PubMed)
Cardiometabolic Parameter Change by Weight Regain on Tirzepatide Withdrawal (JAMA Internal Medicine)
The Endocrine Society - Obesity and Weight Management Resources
American College of Sports Medicine Physical Activity Guidelines
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay manageable, your habits stay strong, and your progress stay protected.