Mar 23, 2026

Some people start semaglutide and lose 15 pounds in the first two months. Others lose 4. Same drug, same starting dose, wildly different results. The difference is often what they eat. And among the dietary strategies people pair with GLP-1 medications, keto generates more debate than almost anything else. Some researchers call it the perfect pairing. Others warn it amplifies every side effect you are already trying to manage. Both camps have a point.
The ketogenic diet and semaglutide work through completely different mechanisms, but they share a common downstream goal: forcing your body to burn fat as its primary fuel. Semaglutide slows gastric emptying, activates GLP-1 receptors in the brain, and reduces appetite signaling. Keto eliminates glucose as an energy source, shifts metabolism toward ketone production, and restructures the hormonal environment around insulin. When these two approaches work in the same direction, fat loss can accelerate considerably. When they conflict, usually through poor timing, inadequate protein, or mismanaged electrolytes, the combination can make you feel significantly worse than either approach alone.
This guide covers everything you need to know before combining these two strategies. You will find the exact macros that work, a week-by-week protocol for transitioning safely, a detailed breakdown of side effects and how to manage them, the specific muscle preservation problem that neither approach fully solves on its own, and the honest list of people who should not try this combination at all. The research data here comes from clinical trials, emerging endocrinology findings, and the practical experience of people who have navigated this exact combination.
How semaglutide and ketosis work together
To understand why this combination works, you need to understand what each approach actually does inside the body. They are not redundant. They target fat loss from different angles, and those angles are surprisingly complementary.
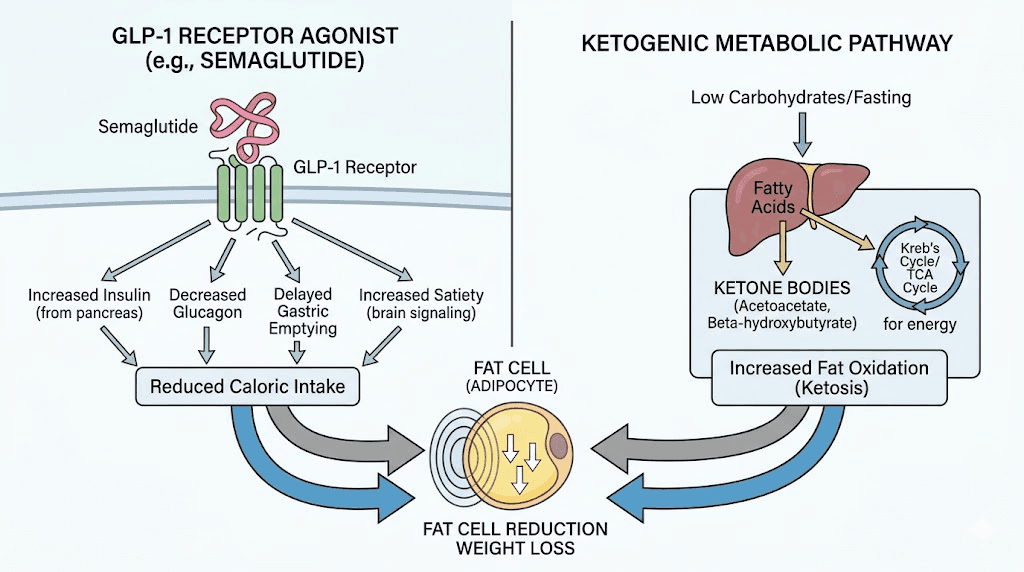
Semaglutide is a GLP-1 receptor agonist. It mimics a naturally occurring hormone called glucagon-like peptide-1, which your gut releases after eating. When semaglutide activates GLP-1 receptors in the hypothalamus, it tells your brain you are full, even when your stomach is not. It also slows gastric emptying significantly, which means food moves out of your stomach more slowly, keeping you feeling full longer and blunting post-meal blood sugar spikes. The result is a consistent reduction in caloric intake driven not by willpower but by altered appetite signaling. People following semaglutide diet plan protocols typically see a natural reduction in portion sizes and frequency of eating without consciously trying to restrict. If you want to understand the full mechanism, the how peptides work guide covers GLP-1 receptor biology in depth.
Ketosis works completely differently. When you restrict carbohydrates below roughly 20 to 50 grams per day, your liver begins converting stored fat and dietary fat into ketone bodies, primarily beta-hydroxybutyrate, acetoacetate, and acetone. Your brain, heart, and muscles shift to burning these ketones as their primary fuel source instead of glucose. This metabolic shift has several downstream effects. Insulin levels drop substantially. Glucagon rises. Fat oxidation increases at the cellular level. And perhaps most relevant to this combination, hunger hormones, particularly ghrelin, tend to decrease in ketosis, reinforcing the appetite suppression that semaglutide is already creating through a completely separate pathway.
This is the key insight. Semaglutide suppresses appetite through GLP-1 receptor activation in the central nervous system. Keto suppresses appetite partly through ketone production, partly through lowered insulin, and partly through the hormonal shifts that accompany fat-adapted metabolism. When you combine them, you have dual-pathway appetite suppression working simultaneously. People who track their food on this combination often report eating 800 to 1,100 calories without feeling deprived, not because they are starving themselves, but because the hunger signal has been genuinely reduced through two independent biological mechanisms. Those wondering how fast semaglutide works often find the timeline accelerates when dietary carbohydrates are also removed.
What semaglutide does and does not do to ketone production
This is worth addressing directly because there is a persistent misconception. Semaglutide does not directly stimulate ketone production. It does not make your liver produce more ketone bodies, and it does not accelerate the transition into ketosis. What it does do is reduce appetite and carbohydrate cravings, which makes adhering to a ketogenic diet considerably easier than it would be otherwise.
People who have tried keto without semaglutide know the hardest part: the first two to three weeks. Carbohydrate cravings are intense. Blood sugar fluctuations make you irritable. The transition period before ketosis is fully established feels genuinely uncomfortable. Semaglutide reduces the severity of these cravings through its effects on the reward pathways in the brain. Research on semaglutide appetite suppression shows it dampens the dopaminergic response to food, particularly processed, high-carb foods. So while semaglutide is not creating ketosis, it is removing one of the primary obstacles to achieving and maintaining it.
Once you are in ketosis, your ketone levels are determined by your carbohydrate intake, your fat intake, your protein intake, and your individual metabolic rate. Semaglutide does not interfere with any of these variables. You can measure your ketones normally and adjust your diet normally. The two approaches operate on separate tracks, which is precisely what makes them stackable.
The insulin connection
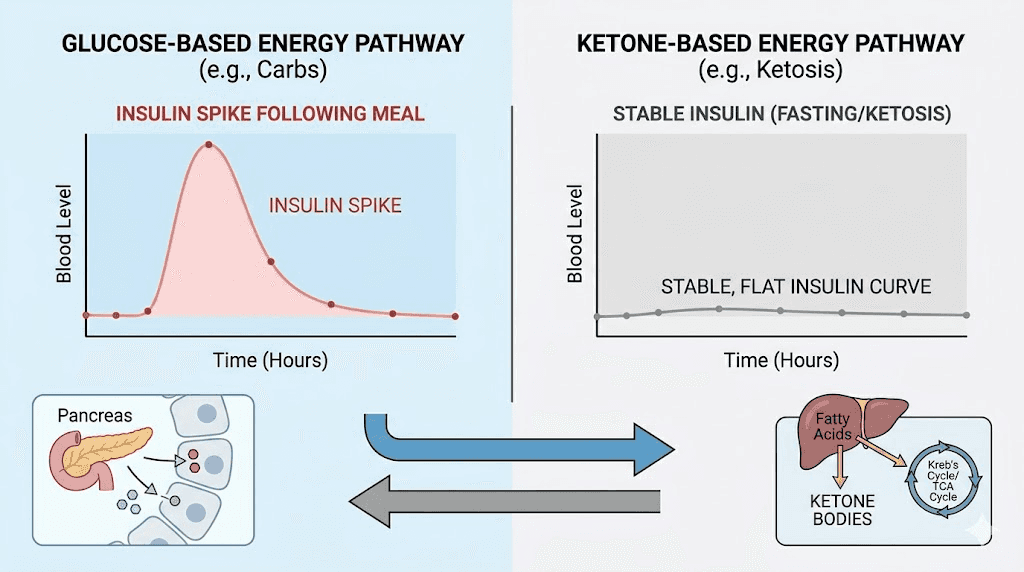
Both semaglutide and the ketogenic diet have significant effects on insulin. Semaglutide stimulates glucose-dependent insulin secretion, meaning it triggers insulin release when blood glucose is elevated but does not cause problematic hypoglycemia in people without diabetes because it stops working when glucose normalizes. The ketogenic diet, by eliminating carbohydrates, dramatically reduces the insulin demand on the pancreas. Fasting insulin levels fall substantially in most people within a few weeks of starting keto.
The downstream effect of lower circulating insulin is important for fat loss. Insulin is a storage hormone. When it is elevated, fat cells preferentially store fatty acids rather than release them. When insulin is low, as it is in nutritional ketosis, fat cells are more accessible for mobilization. This is why people following peptides for fat loss protocols that include dietary strategies often emphasize insulin management. Semaglutide improves insulin sensitivity through its mechanisms. Keto reduces insulin demand through macronutrient restriction. Together, they create a hormonal environment that strongly favors fat oxidation over fat storage.
People managing type 2 diabetes who are considering this combination should be especially careful and work closely with their prescribing physician. The combined glucose-lowering effects of semaglutide, keto-induced insulin reduction, and any other diabetes medications taken concurrently can produce hypoglycemia, and the situation requires careful monitoring. This is covered in more detail in the contraindications section below.
Benefits of combining keto and semaglutide
The research on this specific combination is still emerging, but the mechanistic rationale is strong and the clinical observations from practitioners managing patients on GLP-1 medications are consistent. Here is what the evidence suggests.
Enhanced and accelerated fat loss
The STEP UP trial demonstrated that 7.2mg semaglutide led to approximately 19 percent body weight reduction over the trial period. Those numbers were produced with dietary counseling but not specifically a ketogenic diet. The SELECT trial confirmed significant cardiovascular benefits alongside the weight loss. When ketosis is added to semaglutide treatment, the theoretical and observed weight loss rate tends to increase because both approaches are simultaneously reducing caloric intake through appetite suppression, shifting metabolism toward fat oxidation, and improving insulin sensitivity. People documenting their semaglutide results week by week on keto often report steeper early declines compared to those on semaglutide with a standard low-calorie diet.
This acceleration matters most in the early months when motivation is high and adherence is strongest. Faster visible results reinforce the behavioral changes needed to sustain long-term success.
Reduced carbohydrate cravings
One of the underappreciated benefits of this combination is how semaglutide makes keto adherence dramatically easier. The hardest part of a ketogenic diet is not the fat or the protein, it is eliminating bread, pasta, rice, sugar, and processed snacks that most people have eaten daily for years. Semaglutide specifically blunts the reward response to these foods. People report that pasta no longer calls to them the way it once did. Bread feels less compelling. The craving architecture that makes keto feel like deprivation softens considerably on a GLP-1 medication.
This is a real, biologically grounded effect, not just motivation. Semaglutide modulates dopamine pathways involved in food reward. The result is that high-carbohydrate foods become less appealing at a neurochemical level. For someone attempting keto, this represents a significant reduction in the friction of adherence. Reviews of how semaglutide makes you feel consistently note reduced desire for sweets and processed carbohydrates within the first few weeks.
Potential cardiovascular and metabolic improvements
Both semaglutide and the ketogenic diet have independent evidence for cardiovascular benefit in people with obesity or metabolic syndrome. Semaglutide reduces cardiovascular event risk as shown in the SELECT trial. The ketogenic diet has demonstrated reductions in triglycerides, improvements in HDL cholesterol, and reductions in small dense LDL particles, the type most associated with cardiovascular risk. Whether the combination produces additive cardiovascular benefit beyond either approach alone remains to be studied definitively, but the mechanistic case is reasonable.
Metabolic improvements on the combination are also notable. Blood pressure tends to fall as weight drops. Fasting blood glucose normalizes more rapidly. Inflammatory markers like C-reactive protein decrease. People exploring peptides for anti-aging and longevity often focus on these same metabolic parameters, and the keto-semaglutide combination addresses several simultaneously.
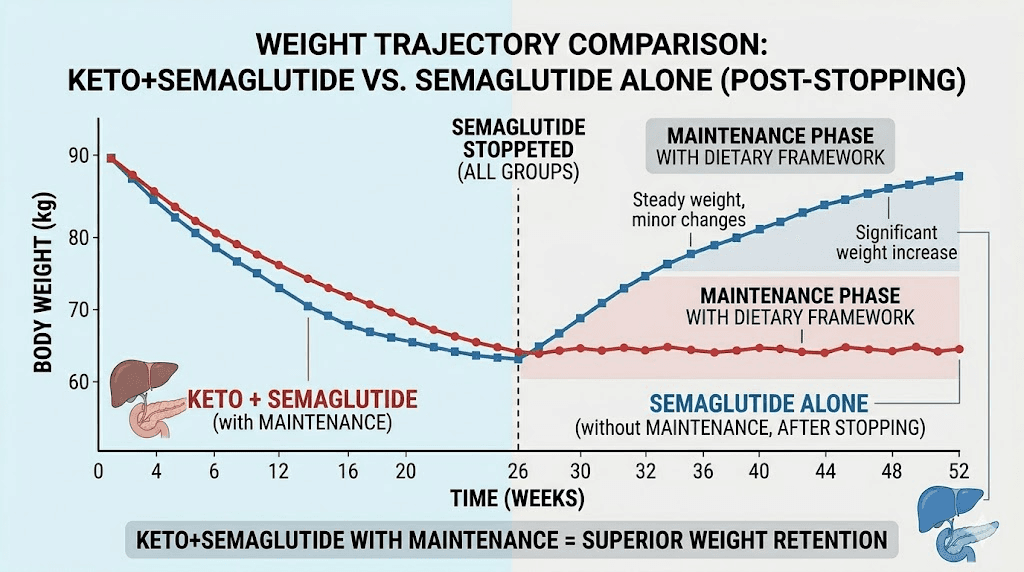
Improved weight loss sustainability
Perhaps the most significant long-term benefit is what happens when semaglutide is eventually stopped. This is covered in detail in the maintenance section, but briefly: people who have established ketogenic metabolic adaptation while on semaglutide appear better positioned to maintain their weight loss after discontinuation than people who relied purely on drug-mediated appetite suppression. They have a dietary framework, fat-adapted metabolism, and reduced dependence on carbohydrate-driven hunger cycles. Understanding semaglutide withdrawal symptoms and how to maintain weight loss after stopping GLP-1 medications both emphasize the importance of having a dietary strategy in place before discontinuation.
The muscle preservation problem
This is where the conversation gets uncomfortable, and most guides about semaglutide skip it entirely.
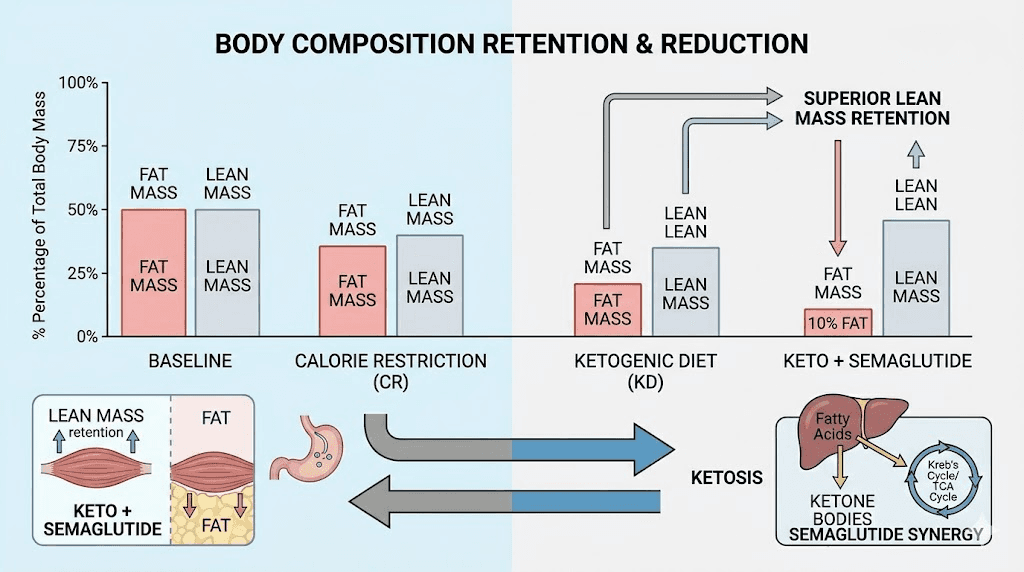
Approximately 40 percent of the weight lost on semaglutide comes from lean mass, not fat. That number comes from body composition analysis in clinical populations, and it is significantly higher than the lean mass loss associated with moderate caloric restriction alone. The mechanism is partly the speed of weight loss, which outpaces the body regulatory mechanisms for muscle preservation. It is partly the reduction in total protein intake that naturally accompanies the appetite suppression. And it is partly the absence of sufficient resistance training in most study populations.
Forty percent lean mass loss is not a small problem. If you lose 50 pounds on semaglutide and 20 of those pounds are muscle, you have reduced your resting metabolic rate, weakened your frame, and set yourself up for weight regain the moment appetite suppression stops. This is why the protein shakes for GLP-1 users topic has become critical, and why creatine and GLP-1 combinations are increasingly discussed among informed researchers.
How keto can help preserve muscle on semaglutide
The ketogenic diet has a specific mechanism that offers meaningful protection against muscle catabolism during caloric restriction. It involves the glucose-alanine cycle.
Under normal conditions, when you are in a caloric deficit and muscle protein begins breaking down, the amino acid alanine is released from muscle tissue and converted to glucose in the liver through gluconeogenesis. This is the body fallback system for maintaining blood glucose when dietary carbohydrates are low. The problem is that this process consumes branched-chain amino acids, specifically leucine, which is the primary driver of muscle protein synthesis. Muscle breakdown feeds the glucose production machine.
In nutritional ketosis, this dynamic changes. When the liver is producing ketone bodies from fat, the demand for glucose from gluconeogenesis drops substantially. The glucose-alanine cycle slows. Muscle tissue is less likely to be cannibalized for glucose production because the brain and other glucose-dependent tissues have ketones available as an alternative fuel. Branched-chain amino acids, particularly leucine and isoleucine, are spared. The body preferentially burns fat-derived ketones and dietary fat rather than pulling down muscle protein for energy.
This is a genuine mechanistic advantage of keto for people on semaglutide. It does not completely solve the muscle loss problem, but it meaningfully reduces it, particularly when combined with adequate protein intake. Data presented at the Endocrine Society ENDO 2025 meeting confirmed that higher protein intake on semaglutide preserves significantly more lean mass, and keto provides a dietary framework that naturally prioritizes protein and fat while eliminating the carbohydrates that tend to displace protein in most diets. Those tracking peptides for muscle growth alongside their GLP-1 protocol understand that protecting existing muscle is just as important as losing fat.
The numbers behind lean mass loss
Consider the math on this problem. A 250-pound person who loses 60 pounds on semaglutide without addressing muscle preservation loses approximately 24 pounds of lean mass based on the 40 percent figure. That 24 pounds of muscle represents a reduction in basal metabolic rate of roughly 144 calories per day. Over a year, that lost muscle accounts for approximately 52,000 fewer calories burned at rest. That is the metabolic hole many people fall into after stopping GLP-1 medication, and it helps explain why regain rates are so high.
Now consider the same person who prioritizes protein at 1.4 grams per kilogram, maintains resistance training, and uses the ketogenic glucose-alanine cycle advantage. If lean mass loss drops to 25 percent of total weight lost instead of 40 percent, the muscle loss is 15 pounds rather than 24. The metabolic rate difference is roughly 54 calories per day. That sounds small in isolation. Over a year, it is nearly 20,000 additional calories burned, which translates to roughly 5 to 6 pounds of fat that get burned rather than stored. People who track how fast you can lose weight on semaglutide understand that the speed of loss matters less than what you lose. Pure fat loss beats rapid total weight loss every time. The best peptides for weight loss guide emphasizes body composition outcomes over scale numbers for this exact reason.
The protein target on keto with semaglutide
The recommended protein intake for people on semaglutide is 1.2 to 1.6 grams per kilogram of body weight per day. This is higher than general population recommendations because of the elevated muscle loss risk associated with GLP-1-driven caloric restriction. For a 200-pound person (about 91 kilograms), this translates to roughly 109 to 146 grams of protein daily.
Here is the challenge. Semaglutide suppresses appetite significantly. Eating 130 grams of protein when you are not hungry is genuinely difficult. Many people on semaglutide naturally drift toward grazing on small amounts of whatever is convenient, which rarely adds up to adequate protein. The best foods to eat on semaglutide guide addresses this directly, and the consistent recommendation is protein-first eating at every meal, however small that meal may be.
The ketogenic diet structure supports this goal because keto naturally emphasizes animal proteins and fat as the foundation of each meal. A keto plate centers on meat, fish, eggs, or dairy, all of which are dense protein sources. You are not filling up on bread, rice, or pasta before getting to the protein. This makes hitting the protein target somewhat more natural within a keto framework than within a standard calorie-restricted diet that includes carbohydrates. Using the semaglutide dosage calculator for your medication and a simple macro tracker for your protein is a reasonable starting point for building your protocol.
Resistance training: the missing piece
Neither semaglutide nor keto can fully replace the muscle preservation signal provided by resistance training. Mechanical loading, specifically the process of lifting weights and causing micro-tears in muscle fiber, triggers a hormonal and cellular response that prioritizes muscle repair and growth over breakdown. Without this signal, even optimal protein intake and ketogenic metabolic conditions cannot fully counter the lean mass loss that accompanies rapid weight reduction.
The practical recommendation is two to three sessions of resistance training per week during a semaglutide course. They do not need to be long or intense. Even 30-minute sessions focused on compound movements, squats, deadlifts, rows, presses, produce meaningful muscle-preservation signals. People who find exercise difficult due to fatigue may find the semaglutide fatigue guide helpful, as fatigue management often comes down to electrolytes and meal timing rather than the medication itself. People interested in peptides for weight loss and muscle gain can find additional strategies for simultaneously protecting lean mass while in a fat loss phase.
Macros and nutrition on keto with semaglutide
Standard ketogenic macro ratios are approximately 55 to 60 percent of calories from fat, 30 to 35 percent from protein, and 5 to 10 percent from carbohydrates. The carbohydrate target is under 20 to 50 grams of net carbohydrates per day depending on individual metabolic flexibility. However, when semaglutide is part of the picture, these ratios need some adjustment.
Protein: the most important variable
Standard keto often runs protein at a moderate level to avoid gluconeogenesis disrupting ketosis. The concern is that excess protein gets converted to glucose and kicks you out of ketosis. This concern is real but often overstated, particularly in people who are insulin sensitive or adapting to fat burning, and it becomes secondary to the muscle preservation imperative when semaglutide is involved.
On this combination, protein intake should be higher than a standard keto protocol. Target 1.2 to 1.6 grams per kilogram of body weight. For most people, this will land protein at 35 to 40 percent of total calories, which is higher than typical keto recommendations. Will this push you toward the lower edge of ketosis? Possibly. For some people, higher protein mildly raises blood ketone levels rather than reducing them. For others, very high protein does produce enough gluconeogenesis to reduce ketone production. The practical answer is: optimize for muscle first, ketosis second. Modest ketosis with adequate protein is more valuable for body composition than deep ketosis with inadequate protein. Track your protein with a food logging app and use the peptide cost calculator to ensure you are accounting for all your supplement costs if you are adding protein powder to hit your targets.
Protein sources that work well in this combination: eggs, salmon, sardines, ground beef, chicken thighs, cottage cheese (check for carb content), Greek yogurt (check for carb content), whey protein isolate, beef liver. The list of foods to eat while on semaglutide includes many of these with specific preparation notes.
Fat: focus on quality, not quantity
Fat makes up the majority of calories on keto, but the "eat all the fat" approach common in some keto communities requires modification when semaglutide is slowing gastric emptying. High-fat meals sit in the stomach longer. Combined with semaglutide gastric emptying delay, very high fat intake can cause nausea, bloating, and reflux that makes eating feel genuinely unpleasant. People who have experienced this often describe the feeling as food just sitting in their stomach for hours.
The adjustment is to use fat as the dietary lever you reduce when appetite is already suppressed, rather than forcing fat intake to hit macro targets. Eat fat to satiety. Do not force-feed butter and cream when semaglutide is already making you feel full. The semaglutide bloating guide and semaglutide acid reflux article both identify high-fat meals, particularly combined with delayed gastric emptying, as a primary trigger. Practical adjustments include choosing leaner proteins more often, using olive oil rather than added butter for cooking, and keeping fat sources concentrated and small rather than spread across large meals.
Prioritize these fat sources: olive oil, avocado, fatty fish, nuts and seeds in moderate portions, coconut oil in small amounts. Minimize: heavy cream in large quantities, butter added liberally to everything, processed keto snacks marketed as fat bombs.
Carbohydrates: the 20-gram target and why it matters
For the combination to provide the muscle-preservation benefits of ketosis, actual ketosis needs to be maintained. This means staying under approximately 20 to 30 grams of net carbohydrates per day for most people. Some metabolically flexible individuals can maintain ketosis at up to 50 grams, but in the context of semaglutide-driven caloric restriction, erring toward the lower end is advisable.
The foods to avoid are the obvious ones: bread, pasta, rice, potatoes, sugar, fruit juice, most fruit, and all processed carbohydrates. But the less obvious sources trip people up. Onions, tomatoes, and peppers contain enough carbohydrates to matter if eaten in quantity. Most sauces and condiments have added sugar. Flavored nuts often have sugar coatings. The foods to avoid on semaglutide guide covers many of these hidden carbohydrate sources in detail. Reading labels and tracking net carbs for the first few weeks until you develop intuition for portion sizes is strongly recommended.
Allowable carbohydrates come primarily from non-starchy vegetables: leafy greens, broccoli, cauliflower, zucchini, asparagus, green beans, cucumbers, celery. These provide fiber for gut health, vitamins and minerals that are critical when calories are reduced, and modest amounts of net carbs that keep you well within ketosis range.
Electrolytes: the non-negotiable addition
Both the ketogenic diet and semaglutide create electrolyte management challenges that compound when combined. Keto increases renal excretion of sodium because low insulin reduces sodium reabsorption in the kidneys. The result is that sodium, potassium, and magnesium are all lost more rapidly in ketosis. The classic keto flu, with its headaches, fatigue, dizziness, and muscle cramps, is primarily an electrolyte depletion phenomenon. The semaglutide dizziness article also identifies electrolyte imbalance as a common contributing factor to dizziness on GLP-1 medications.
Semaglutide adds to this challenge through reduced food intake. When you are eating less overall, you are taking in less of every mineral. If your primary electrolyte source has been food rather than supplementation, reduced intake will amplify the keto-induced losses.
The practical protocol: supplement sodium (2,000 to 3,000mg above dietary intake), potassium (1,000 to 2,000mg), and magnesium (300 to 400mg, preferably glycinate or malate form). Electrolyte drinks can help, particularly ones without added sugar. Salt your food generously. Bone broth is an excellent sodium and electrolyte source that also provides gelatin for gut health. The best fiber supplement for GLP-1 users guide also touches on mineral balance as part of the broader supplementation strategy.
Supplements worth adding to the combination
Beyond electrolytes, several supplements have strong rationale for people combining keto and semaglutide. Creatine monohydrate (3 to 5 grams daily) is probably the single most evidence-supported supplement for preserving lean mass on a GLP-1-driven caloric deficit, and the creatine and GLP-1 guide makes a compelling case for its inclusion. B12 deficiency is more common than people realize on restrictive diets, and the semaglutide with B12 complete guide and methylcobalamin guide both recommend B12 supplementation. L-carnitine supports fatty acid transport into mitochondria, which is directly relevant when fat oxidation is the primary energy pathway, and the semaglutide L-carnitine guide covers this combination in depth.
For gut health, which is stressed by both keto and semaglutide, a quality probiotic is worth including. The best probiotic for semaglutide guide identifies specific strains with evidence for GLP-1 tolerance improvement. Fiber supplementation helps with constipation, which is a genuine problem in this combination as covered in the side effects section.
Those interested in additional support for the fat loss phase can also review the supplements to take with GLP-1 guide and the best peptide stack for weight loss resource, which covers how different compounds can be combined with GLP-1 medications for enhanced outcomes. The peptide stack calculator helps with planning dosing across multiple compounds.
What to eat: practical meal planning
Abstract macros are one thing. Actual meals are another. Here is a practical framework for eating on keto with semaglutide, keeping in mind that portion sizes will be smaller than what most people expect given the appetite suppression.
Breakfast: two to three eggs scrambled in olive oil with spinach and half an avocado. Or a protein shake with whey isolate, almond milk, and a tablespoon of almond butter if solid food is unappealing in the morning. Many people on semaglutide find appetite is lowest in the morning. The GLP-1 breakfast ideas page has additional options designed for low-appetite mornings.
Lunch: a large portion of leafy greens with salmon or chicken, olive oil dressing, cucumber, and a handful of walnuts. Soups work well because they are easier to eat when appetite is reduced. A broth-based soup with ground beef, zucchini, and spinach provides protein, fat, electrolytes, and minimal carbs. The GLP-1 recipes for weight loss collection includes several high-protein, keto-compatible options.
Dinner: the largest meal of the day for most people on semaglutide, since appetite tends to build throughout the day. Ground beef or fatty fish with non-starchy vegetables roasted in olive oil. The GLP-1 dinner ideas guide includes specific recipes designed for GLP-1 tolerability.
Snacks, if needed: hard-boiled eggs, a handful of almonds, cheese in small portions, or Greek yogurt (full-fat, plain, watch carb count). The goal is protein-forward snacking rather than keto fat bombs, which tend to displace protein calories. For calculating specific caloric and macronutrient targets, the how many calories should I eat on semaglutide guide provides personalized frameworks, and there is a parallel resource for how many calories on tirzepatide if you are considering switching between GLP-1 agents.
Week-by-week protocol for combining keto and semaglutide
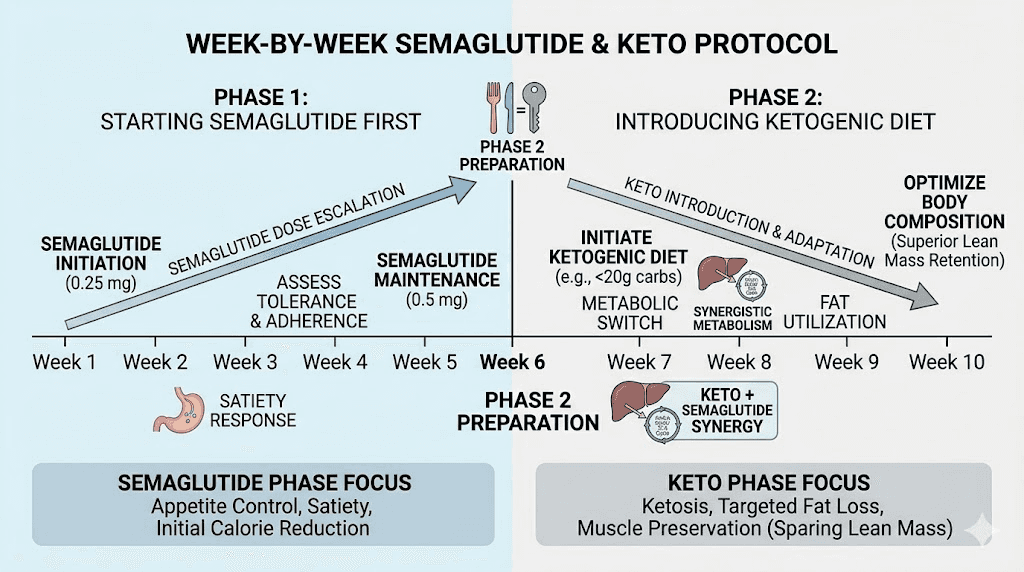
The sequencing of these two interventions matters enormously. Trying to start both simultaneously creates a perfect storm of side effects: keto flu symptoms colliding with semaglutide adjustment symptoms, each amplifying the other. The recommended approach is to start semaglutide first, allow 4 to 6 weeks for the initial adjustment period to pass, and then transition into ketosis.
Phase 1: semaglutide introduction (weeks 1-6)
During this phase, focus exclusively on tolerating the medication and establishing dietary habits that support the eventual keto transition. Do not attempt keto yet.
Week 1 to 2: Start at the standard beginning dose (typically 0.25mg weekly for pharmaceutical semaglutide, or the equivalent compounded dose as outlined in your compounded semaglutide guide). Expect nausea, reduced appetite, and possibly fatigue. Eat whatever you can tolerate that provides adequate protein. This is not the time for dietary restriction. The first week on semaglutide guide sets accurate expectations for what to experience. Review best time of day to take semaglutide to minimize nausea through timing optimization.
Week 3 to 4: Nausea typically eases. Appetite suppression is more consistent. Begin reducing refined carbohydrates and sugar without enforcing strict keto limits yet. Move toward a low-glycemic diet: eliminate bread, pasta, rice, and sugar. Keep carbohydrates from whole foods only. This preparatory phase reduces the shock of full keto transition later. Read the semaglutide one month results guide for realistic expectations at this point. Some people notice their natural semaglutide-driven eating already looks close to moderate-carb without conscious effort, which is common given the reduced carbohydrate cravings.
Week 5 to 6: Continue reducing carbohydrates toward the 50-gram range. Begin introducing ketogenic food patterns: prioritizing fatty proteins, adding avocado, reducing fruit consumption. Start the electrolyte supplementation protocol during this week, before full ketosis, because the electrolyte demands increase as carbohydrates drop even before ketosis is fully established. Review semaglutide tips for optimizing the overall protocol at this stage.
Phase 2: keto transition (weeks 7-10)
This is when you drop carbohydrates under 20 to 30 grams of net carbs daily and enter nutritional ketosis. Having four to six weeks of semaglutide adaptation behind you makes this significantly more manageable.
Week 7: Implement full keto macros. Carbohydrates under 25 grams net. Protein at 1.2 to 1.4 grams per kilogram body weight. Fat to satiety. Expect some keto flu symptoms even with electrolyte supplementation, but they will be milder than starting keto from scratch. Energy may dip for three to five days. This is normal and temporary. If fatigue is severe, the GLP-1 fatigue guide and semaglutide fatigue article both provide management strategies. Some people find taking semaglutide with glycine helps with sleep and recovery during this transitional period.
Week 8: Ketosis should be established if carb restriction has been maintained. Test with urine ketone strips or a blood ketone meter. Target blood ketones of 0.5 to 2.0 mmol/L for nutritional ketosis. Appetite suppression from both semaglutide and ketosis should now be evident simultaneously. Many people report this as the week when the combination starts feeling effortless rather than effortful. Fat loss typically accelerates noticeably. Check the GLP-1 average weight loss per month guide for benchmarking your progress against typical trajectories.
Week 9 to 10: This is the maintenance phase of the transition. The goal is consistent adherence rather than continued tightening. Do not reduce carbohydrates further below 20 grams unless ketosis is not being maintained. Do not reduce protein below 1.2 grams per kilogram. Resistance training should be well established by now. Consider adding creatine if not already included. The semaglutide plateau guide is relevant here if progress stalls, as early plateaus on this combination are often electrolyte or protein-related rather than metabolic adaptation.
Phase 3: optimized combination (week 11 onward)
At this point the combination is running smoothly and the focus shifts to optimization and sustainability.
Dose management: Follow your physician prescribed semaglutide dose escalation schedule. The semaglutide dosage chart in units and semaglutide dosage guide provide reference points. Do not escalate dosage faster than prescribed. The combination of keto appetite suppression and semaglutide appetite suppression means that some people find lower doses sufficient for their goals. The semaglutide 5mg dosage chart and chart semaglutide syringe dosage guide are practical references for those using injectable compounded formulations.
Protein cycling: Some people find that having two or three higher-protein days per week, while staying within keto, helps with muscle maintenance and performance. This does not mean carb cycling, just protein cycling within the ketogenic framework. Leucine-rich protein sources, specifically meat, eggs, and whey, are most effective for triggering muscle protein synthesis.
Monitoring: Weigh yourself weekly, measure body composition monthly if possible. Track protein intake daily until you have strong intuition for hitting targets. Monitor blood ketones weekly if optimization is a priority. The glp-1 monitoring tools for home use guide covers practical home monitoring options. The semaglutide before and after documentation guide provides frameworks for tracking progress meaningfully over time.
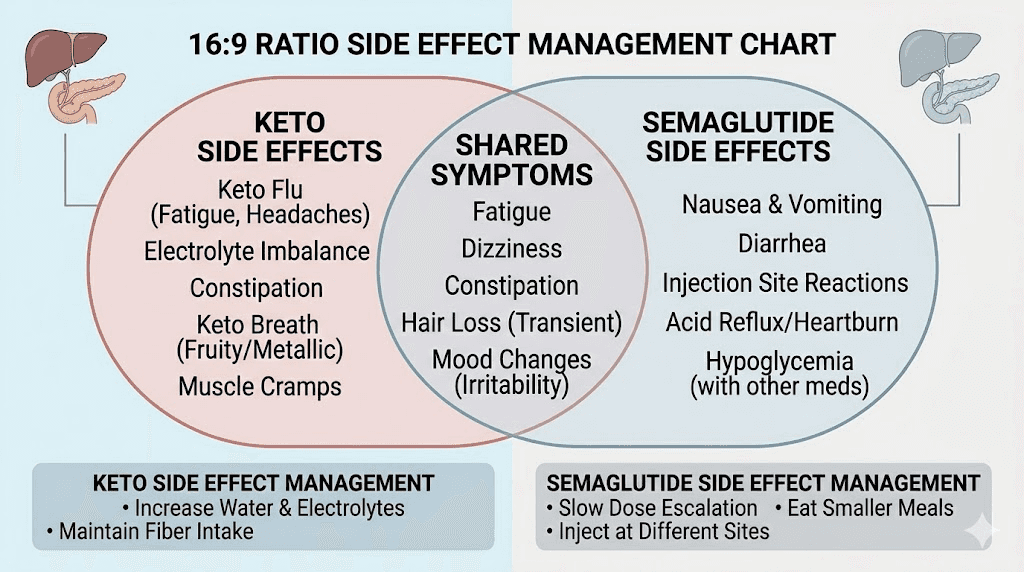
Side effects and how to manage them
Both semaglutide and the ketogenic diet have well-documented side effect profiles. Combining them creates a situation where some of these overlap, some cancel each other out, and some amplify each other. Understanding which is which is critical for managing the combination safely.
Nausea
Nausea is the most common side effect of semaglutide, reported by 15 to 44 percent of users in clinical trials. It is typically worst in the first two months and improves significantly as the body adjusts. High-fat meals, which are central to keto, can trigger or worsen nausea on semaglutide because fat further slows gastric emptying beyond what semaglutide is already doing. This is the main reason the recommended protocol delays keto implementation until after the initial semaglutide adjustment period.
Management strategies: eat smaller, more frequent meals. Avoid very large boluses of fat at any one meal. Ginger tea, ginger chews, and peppermint have modest evidence for nausea relief. The semaglutide burping guide and semaglutide acid reflux guide both cover related gastrointestinal symptoms with practical management approaches. If nausea is severe enough to prevent adequate protein intake, prioritize protein powder shakes over solid food during the worst periods, as discussed in the protein shakes for GLP-1 guide.
Constipation
Constipation is both a keto side effect and a semaglutide side effect. Combined, it becomes a significant issue for many people. Semaglutide slows gut motility through its GLP-1 receptor effects throughout the gastrointestinal tract. Keto reduces fiber intake compared to a carbohydrate-inclusive diet (since most fiber-rich foods also contain carbs) and can reduce bowel movement frequency. Together, these mechanisms create persistent constipation that some people describe as their most disruptive side effect.
The semaglutide constipation treatment guide and GLP-1 constipation relief article both cover this extensively. The essential strategies: adequate hydration (2 to 3 liters of water daily), fiber supplementation from keto-compatible sources (psyllium husk adds fiber with minimal net carbs), magnesium supplementation (magnesium citrate or oxide can have laxative effects and addresses the electrolyte needs simultaneously), and maintaining movement rather than sedentary behavior throughout the day. The best fiber supplement for GLP-1 guide provides specific product recommendations and dosing.
Fatigue and energy dips
Fatigue has three potential sources in this combination. First, the initial keto adaptation period where the brain and muscles are learning to use ketones instead of glucose, typically lasting 7 to 14 days. Second, semaglutide-related fatigue, which is reported by roughly 10 to 15 percent of users and tends to be most prominent in the first month. Third, inadequate caloric or electrolyte intake when semaglutide is significantly suppressing appetite and food intake drops below sustainable levels.
The GLP-1 fatigue guide identifies electrolyte depletion as the most common correctable cause. Sodium deficiency produces fatigue, brain fog, and dizziness that feels like exhaustion but responds rapidly to salt supplementation. If fatigue is persistent after the adaptation period, check whether total caloric intake has dropped below approximately 1,200 to 1,400 calories per day (the minimum for most people to maintain energy and lean mass). Does semaglutide give you energy in the longer term? The semaglutide energy guide addresses this question with nuance.
During the keto transition weeks, temporarily increasing sodium intake to 4,000 to 5,000mg per day can meaningfully reduce keto adaptation symptoms. Broth, salted foods, and an electrolyte supplement taken twice daily are the practical approach. Once adaptation is complete, drop back to 2,000 to 3,000mg additional sodium above dietary intake.
Hypoglycemia risk
For people without diabetes, true hypoglycemia (blood glucose below 70 mg/dL) is uncommon on semaglutide because the drug stimulates insulin secretion in a glucose-dependent manner. However, the combination of semaglutide and keto does create a lower baseline blood glucose environment. Blood sugar readings of 65 to 75 mg/dL are more common in ketosis even without any medication. Semaglutide on top of this can occasionally push readings lower, particularly after intense exercise.
For people with type 2 diabetes who are also taking insulin or sulfonylureas, the risk is substantially higher and requires active monitoring and likely dose reductions of the diabetes medications as weight and blood glucose improve. The can you take metformin with semaglutide guide addresses multi-drug interactions. Symptoms of low blood sugar: shakiness, sweating, heart palpitations, confusion, and irritability. Having a small keto-compatible glucose source available (a few dextrose tablets) is prudent even if you are not diabetic.
Euglycemic ketoacidosis: rare but serious
This deserves specific attention because it is both rare and potentially dangerous, and the combination of GLP-1 medications and very low carbohydrate eating has been associated with it in small numbers of cases.
Euglycemic diabetic ketoacidosis (euDKA) occurs when ketone levels rise dangerously high while blood glucose remains normal or only mildly elevated. It is most associated with SGLT2 inhibitors (a different class of diabetes drug) but has been reported with GLP-1 medications in the context of very low carbohydrate intake, particularly during illness, fasting, or periods of very low food intake. The danger is that normal blood glucose creates a false sense of safety, so the condition can progress undetected.
Risk factors: type 1 or type 2 diabetes, concurrent SGLT2 inhibitor use, prolonged fasting or illness while on keto, very strict carbohydrate restriction below 20 grams during acute illness. Symptoms to watch for: nausea, vomiting, abdominal pain, difficulty breathing, confusion. If you have these symptoms while on GLP-1 and keto, seek medical attention promptly and request ketone testing. For most non-diabetic people on standard nutritional ketosis (under 3 mmol/L blood ketones), the risk is low but worth knowing about.
Hair loss
Both rapid weight loss and nutritional restriction can trigger telogen effluvium, a type of temporary hair loss caused by metabolic stress. The GLP-1 hair loss guide documents this as a real concern in people losing weight rapidly on GLP-1 medications. Keto, particularly in its restrictive early phase, can also trigger hair shedding through micronutrient deficiencies, specifically inadequate zinc, biotin, and iron.
Mitigation: adequate protein intake (this protects against protein deficiency-related hair loss), zinc supplementation, biotin supplementation, iron monitoring particularly in women (the semaglutide and menstrual cycle guide covers hormonal and nutritional considerations for women). The hair loss is almost always temporary and resolves as weight loss slows and nutrition stabilizes.
Sleep disruption
Some people report insomnia or disrupted sleep during keto transition and on semaglutide. The semaglutide insomnia guide covers the mechanisms. Keto can initially disrupt sleep through the metabolic transition period. Magnesium glycinate supplementation (300 to 400mg before bed) consistently helps with sleep quality on keto. Glycine supplementation has evidence for sleep improvement as well, which is why the semaglutide with glycine guide is relevant here.
Who should not combine keto and semaglutide
This combination is not appropriate for everyone. Some conditions create enough additional risk that the combination requires physician supervision at minimum, and in some cases should be avoided entirely.
Absolute contraindications
People with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 should not use semaglutide at all, as these are contraindications for the medication itself regardless of diet. People with severe pancreatitis history require physician guidance before using GLP-1 medications. These are drug-level contraindications that keto does not change.
People with a history of disordered eating, particularly restrictive eating disorders such as anorexia or orthorexia, should be cautious about both semaglutide-driven appetite suppression and the rigid food rules inherent in ketogenic eating. This combination can reinforce unhealthy relationships with food and eating restriction in vulnerable individuals. A mental health professional should be involved in this decision.
High caution: active diabetes on multiple medications
People with type 2 diabetes who are actively taking insulin, sulfonylureas, or SGLT2 inhibitors alongside semaglutide face significantly elevated hypoglycemia and euDKA risk when adding keto. This is not an absolute contraindication but requires close physician involvement, likely dose adjustments of other medications as glucose improves, and frequent monitoring. The can you take phentermine and semaglutide together guide illustrates the general principle of needing physician guidance for any multi-drug combination.
High caution: gallbladder disease
Rapid weight loss increases gallstone risk, and both semaglutide and keto can individually accelerate this. The ketogenic diet dramatically increases fat intake through the gallbladder, which can worsen existing gallbladder disease or precipitate acute events in people with existing gallstones. If you have known gallbladder issues, a history of gallstones, or have had your gallbladder removed and experience digestive difficulty with fat, this combination requires physician guidance and potentially modified fat intake protocols.
Moderate caution: chronic kidney disease
The higher protein recommendations appropriate for semaglutide users may not be appropriate for people with chronic kidney disease, as high protein intake can accelerate kidney function decline in this population. The semaglutide and kidney stones guide and semaglutide and liver enzymes article address organ-level considerations. If you have reduced kidney function, protein targets should be determined by your nephrologist, and standard keto protein recommendations may need downward adjustment.
Pregnancy and breastfeeding
Semaglutide is contraindicated in pregnancy. The ketogenic diet is generally not recommended during pregnancy due to the energy and nutrient demands of fetal development. Both categories apply here. Women who may become pregnant should discuss contraception with their physician before starting semaglutide. The semaglutide sex drive women guide and related guides cover hormonal considerations for women on GLP-1 medications.
Underweight individuals or those with very low BMI
People who are at or below normal body weight should not use this combination. Semaglutide is indicated for people with obesity (BMI over 30) or overweight with weight-related comorbidities (BMI over 27). Adding significant additional caloric restriction through keto in a person without significant fat stores creates genuine risk of lean mass loss, nutritional deficiency, and metabolic disruption. The how to qualify for semaglutide guide covers eligibility criteria in detail.
Common mistakes people make with keto and semaglutide timing
The most frequent mistake is not eating enough total calories. This sounds counterintuitive for a weight loss combination, but there is a floor below which the body stops cooperating. When semaglutide suppresses appetite and keto eliminates an entire macronutrient category, some people end up eating 600 to 800 calories per day without realizing it. At that intake level, metabolic adaptation kicks in aggressively. Thyroid function can downregulate. Cortisol rises. The body shifts into conservation mode that actually slows fat loss and accelerates muscle breakdown. If you have been on the combination for several weeks and weight loss has stalled despite strict adherence, the why not losing weight on semaglutide guide and the 4 weeks on semaglutide no weight loss article both identify undereating as a paradoxical but common cause of plateau.
The second mistake is obsessing over ketone depth rather than protein adequacy. Blood ketone readings of 3.0 or 4.0 mmol/L look impressive but they often indicate either fasting or undereating rather than optimal nutritional ketosis. The ideal range for body recomposition is 0.5 to 2.0 mmol/L. Higher readings are not better for fat loss and may indicate that protein is being sacrificed to maintain deep ketosis, which defeats the entire purpose of combining these approaches. SeekPeptides members who track their protocols consistently report that moderate ketosis with adequate protein produces better body composition outcomes than deep ketosis with inadequate protein.
The third mistake is neglecting to track anything. The combination of keto and semaglutide involves enough variables, protein grams, net carbs, electrolytes, ketone levels, body weight, that flying blind leads to suboptimal results. A food tracking app used for at least the first 8 to 12 weeks builds the intuition needed to eventually eat without tracking. The diet on semaglutide guide and the semaglutide diet plan resource both recommend tracking during the initial establishment phase even if you plan to stop later.
Keto as a maintenance strategy after stopping semaglutide
Weight regain after stopping GLP-1 medications is a real and well-documented phenomenon. Studies show that people who stop semaglutide without maintaining lifestyle changes regain a substantial portion of lost weight within 12 months. The mechanism is straightforward: the drug was suppressing appetite. Without the drug, appetite returns. Without a dietary framework to manage food intake, calories return to pre-treatment levels and weight follows.
This is the most compelling long-term argument for establishing ketogenic eating habits while on semaglutide rather than simply using semaglutide as a passive appetite suppressant. People who develop fat-adapted metabolism, learn keto food preparation, and build sustainable ketogenic eating patterns during their semaglutide course have a functional maintenance strategy available when they eventually taper off. The semaglutide withdrawal symptoms guide and can you stop semaglutide cold turkey guide both address the transition off medication and what to expect.
The fat-adapted advantage after stopping
People who have spent several months in ketosis develop metabolic flexibility that persists after they transition off strict keto. Their mitochondria have upregulated fat oxidation capacity. Their hormonal systems have adapted to lower insulin environments. They have effectively retrained their metabolic preference. While this does not provide permanent protection against weight regain if dietary habits completely revert, it does mean that keto-adapted people who maintain even moderate carbohydrate restriction after stopping semaglutide can often maintain significantly more of their weight loss than those who have no dietary strategy at all.
The GLP-1 maintenance dose guide covers the medical approach of maintaining a low dose of semaglutide long-term. Some people combine both strategies: a low maintenance dose of semaglutide with continued loose keto eating. This represents the most comprehensive maintenance approach currently available. The GLP-1 reset complete guide and restarting semaglutide after 3 months guide are also relevant for people who stop and restart.
Transitioning from strict keto to maintenance carbohydrates
When semaglutide is stopped, some people find strict keto too difficult to maintain indefinitely without the appetite suppression the drug was providing. A reasonable transition approach is to move from strict keto (under 25 grams net carbs) to a low-carbohydrate diet (50 to 100 grams net carbs) that is less restrictive but still meaningfully below the carbohydrate intake that drove the original weight gain.
Whole food carbohydrate sources like legumes, sweet potatoes, and whole fruit can be reintroduced gradually while monitoring weight and metabolic markers. The key is avoiding the full return to processed carbohydrates, refined sugar, and high-glycemic eating patterns that characterized the pre-treatment diet. Those monitoring long-term results can review how long to stay on semaglutide for weight loss for guidance on treatment duration, and how to maintain weight loss after tirzepatide for strategies that translate across GLP-1 medications.
The role of resistance training in post-semaglutide maintenance
The muscle preserved during semaglutide treatment through adequate protein and resistance training becomes a significant metabolic advantage after stopping. Each pound of muscle tissue burns approximately 6 calories per day at rest. For someone who preserved 10 additional pounds of muscle compared to a person who lost the same body weight but with higher lean mass loss, that represents roughly 60 extra calories burned per day, or over 20,000 extra calories per year, without any additional effort. Over time, this compounds into a meaningful metabolic protection against weight regain.
Continuing resistance training after stopping semaglutide is arguably more important than during treatment. The drug is no longer suppressing appetite. The metabolic protection of maintained muscle mass becomes the primary defense against the caloric surplus that drives weight regain. People interested in how peptides can support the post-GLP-1 phase can review peptides for fat loss and the broader peptides for weight loss guide for strategies that support the transition. SeekPeptides members access comprehensive post-GLP-1 protocols developed by experienced researchers who have navigated this exact transition, including guidance on peptide combinations, dietary frameworks, and long-term maintenance strategies.
Frequently asked questions
Can you start keto and semaglutide at the same time?
It is possible but not recommended. Starting both simultaneously amplifies side effects from both approaches, including nausea, fatigue, constipation, and dizziness. The standard protocol is to start semaglutide first, allow 4 to 6 weeks of adjustment, and then introduce keto. This sequencing keeps side effects manageable and makes it far easier to identify which approach is causing any specific symptom. The first week on semaglutide guide gives a clear picture of what the initial semaglutide period involves before adding dietary complexity.
Does keto make semaglutide work better or faster?
Keto does not directly enhance the pharmacological action of semaglutide, but it does amplify the weight loss outcomes through complementary mechanisms. The dual appetite suppression from both approaches typically produces faster and more pronounced fat loss than semaglutide alone with a standard diet. People who wonder when they start losing weight on semaglutide generally find that keto accelerates the timeline for visible body composition changes.
How much protein should I eat on keto with semaglutide?
Target 1.2 to 1.6 grams of protein per kilogram of body weight daily. For a 180-pound person (approximately 82 kg), this is 98 to 131 grams of protein per day. This is higher than standard keto recommendations but necessary to counter the elevated lean mass loss associated with GLP-1-driven caloric restriction. Protein-first eating at every meal is the practical strategy for hitting this target despite reduced appetite. The protein shakes for GLP-1 guide covers liquid protein options when solid food is unappealing.
Will keto kick me out of ketosis on semaglutide?
Semaglutide does not directly interfere with ketone production. Your ketosis depth is determined by carbohydrate intake, protein intake, and individual metabolic factors, not by semaglutide. The medication may indirectly support ketosis by reducing carbohydrate cravings, which makes strict carb restriction easier to maintain. You can test ketones normally with blood or urine strips regardless of semaglutide status. The semaglutide dosage guide and compounded semaglutide guide both confirm that the drug mechanism does not include any interference with ketone metabolism.
What happens to weight after stopping semaglutide if I am on keto?
People who have established fat-adapted metabolism through keto while on semaglutide generally maintain more weight loss after discontinuation than those without a dietary framework. However, keto is not a complete substitute for the appetite suppression the drug was providing. Expect some increased hunger after stopping semaglutide, which keto will partially manage but not fully replicate. Having a maintenance dietary plan, ideally transitioning from strict keto to low-carbohydrate eating, is critical for long-term success. The semaglutide withdrawal symptoms guide covers what to expect physiologically when stopping.
Is the keto and semaglutide combination safe for people with diabetes?
It can be, but it requires significantly more medical supervision than for people without diabetes. The combination of GLP-1-mediated insulin effects, keto-induced glucose reduction, and any other diabetes medications creates real hypoglycemia risk that needs active management. The rare risk of euglycemic ketoacidosis, while low, is higher in diabetic populations, particularly those also on SGLT2 inhibitors. Work closely with your prescribing physician before combining these approaches, and monitor blood glucose and ketone levels regularly. The can you take metformin with semaglutide guide is a relevant reference for people managing multiple diabetes medications.
What supplements help the most with keto and semaglutide?
The non-negotiable supplements are electrolytes: sodium (2,000 to 3,000mg extra daily), potassium (1,000 to 2,000mg), and magnesium (300 to 400mg). Beyond these, creatine monohydrate for muscle preservation, B12 for energy metabolism, and a probiotic for gut health have the strongest combined rationale. L-carnitine and niacinamide round out the support stack for people optimizing fat oxidation. The full case for each of these is made in the supplements to take with GLP-1 guide, the semaglutide niacinamide guide, and the semaglutide L-carnitine guide.
Can I drink alcohol on keto with semaglutide?
Alcohol complicates both keto and semaglutide management. Even low-carb alcoholic beverages can disrupt ketosis in sensitive individuals, and alcohol interacts with semaglutide-mediated nausea in ways that most people find unpleasant. The can you drink on semaglutide guide covers the specific interactions in detail. The general guidance is that occasional low-carb alcohol consumption is not catastrophic but frequent drinking significantly undermines both the fat loss and the tolerability of this combination.
How does tirzepatide compare to semaglutide when combined with keto?
Tirzepatide is a dual GIP and GLP-1 agonist that generally produces greater weight loss than semaglutide alone. The principles of combining it with keto are similar, but the stronger appetite suppression means calorie intake can drop even further, making protein adequacy an even larger challenge. The semaglutide vs tirzepatide comparison and semaglutide vs tirzepatide side effects guide cover the specific differences. People considering switching can review the switching from tirzepatide to semaglutide guide and the semaglutide to tirzepatide conversion chart. The tirzepatide diet plan guide and tirzepatide foods to avoid article provide parallel nutritional guidance for that medication.
What is the best injection site for semaglutide when doing keto?
Injection site does not change based on dietary approach. The standard recommendations apply: abdomen, upper thigh, or upper arm, rotating sites to prevent lipodystrophy. The best injection site for semaglutide guide and how to give semaglutide injection guide cover technique in detail. The best GLP-1 injection site for weight loss guide addresses whether injection location affects outcomes. Proper storage during keto travel (since keto people often travel with meal prep) is covered in the semaglutide shelf life guide and how long semaglutide lasts in fridge.
External resources
STEP 1 Trial: Semaglutide and Weight Loss - New England Journal of Medicine
SELECT Trial: Cardiovascular Outcomes with Semaglutide in Obesity - New England Journal of Medicine
ENDO 2025 Conference: Emerging Data on GLP-1 and Body Composition - Endocrine Society
Ketogenic Diet and Diabetes Management - American Diabetes Association
For anyone navigating the combination of keto and semaglutide, the evidence points toward a protocol that is genuinely more effective than either approach in isolation, provided it is implemented thoughtfully and sequenced correctly. The muscle preservation challenge is real but manageable. The side effects are manageable with proper electrolyte and supplement protocols.
The long-term maintenance benefit is perhaps the most underappreciated advantage of building fat-adapted metabolism while pharmaceutical appetite suppression is supporting adherence. SeekPeptides provides members with detailed, evidence-based protocols for GLP-1 optimization, including keto integration guides, body composition tracking frameworks, and access to a community of researchers who have documented their exact experiences with this combination.
People exploring the broader landscape of GLP-1 and peptide combinations for fat loss and body recomposition can review the best peptide for fat loss guide, the fat burning peptides for men guide, the peptides for belly fat article, and the comprehensive best peptide for visceral fat loss guide. For those considering retatrutide as a next step, the semaglutide vs tirzepatide vs retatrutide comparison and the retatrutide dosage calculator are useful resources. The peptide safety and risks guide and getting started with peptides guide round out the foundational education for anyone new to this space. SeekPeptides remains the most trusted resource for this category of research, with guides built on actual clinical data and reviewed protocols rather than speculation.
In case I do not see you, good afternoon, good evening, and good night. May your ketones stay optimal, your muscle mass stay protected, and your weight loss stay permanent.